
Abstract
Emerging evidence suggests that physical activity may be associated with improved sleep in autistic children. We aimed to determine whether physical activity associated with sufficient sleep duration in children and whether this association was modified by reported autism spectrum disorder (ASD) status. We analyzed existing data of children 6–17 years old whose caregivers completed the 2018 National Survey of Children’s Health (nonautistic N = 20,845; ASD N = 681). Logistic regression determined whether physical activity (days active in the past week) associated with sufficient sleep duration. Physical activity-by-ASD interactions were included to determine whether the association differed for autistic children. Physical activity-by-ASD-by-sex and physical activity-by-ASD-by-age-group interactions were also modeled. Physical activity was associated with increased odds of sufficient sleep duration (e.g. 0 days vs 4–6 days: odds ratio (OR) = 1.85; 95% confidence interval (CI): 1.48–2.32). We did not observe an overall statistically significant interaction between physical activity and reported ASD status; however, the positive association between physical activity and sufficient sleep duration was weaker in autistic children, especially those with more severe ASD, female autistic children, and autistic children ages 6–12 years old. In conclusion, physical activity is a promising approach to improve sufficient sleep duration but with nuanced findings in autistic children.
Lay abstract
Higher levels of physical activity may be associated with improved sleep in children, but this relationship is still being determined, especially in autistic children. In this study, we used existing data from the 2018 National Survey of Children’s Health. Caregivers of children 6–17 years old, including caregivers of autistic children, completed a questionnaire that included questions about physical activity (days active in the past week) and sleep duration. We then determined if children were obtaining the recommended hours of sleep for their age (i.e. sufficient sleep). We found that higher physical activity levels were associated with sufficient sleep duration, but this finding was weaker in autistic children. In particular, this association was not observed in autistic children with more severe autism spectrum disorder, female autistic children, and autistic children 6–12 years old. In conclusion, physical activity is a promising approach to help children obtain sufficient sleep duration. However, more personalized approaches to improving sleep may be needed for certain groups of autistic children.
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by difficulties with social interactions and communication as well as restricted and repetitive behaviors (American Psychiatric Association, 2013). In the United States, 1 in 54 children are diagnosed with ASD with a male predominance (Maenner et al., 2020). Importantly, an estimated 44%–86% of autistic children have sleep problems, such as difficulties initiating and maintaining sleep and shorter sleep duration (Carmassi et al., 2019; Fletcher et al., 2017; Goldman et al., 2017; Healy et al., 2019; Jovevska et al., 2020; Liu et al., 2006; Richdale & Prior, 1995). Furthermore, there is an indication of sleep problems being more common among female autistic children (Angell et al., 2021; D’Agati et al., 2020; Hartley & Sikora, 2009; Masi et al., 2017; Mazurek & Sohl, 2016; Petrou et al., 2018; Wang et al., 2016). Given that poor sleep can affect daytime functioning, it is critical to identify effective strategies to improve sleep in autistic children (Allik et al., 2006; Veatch et al., 2017). Interestingly, there are emerging data supporting an association between physical activity and improved sleep in children.
Among nonautistic children, higher levels of physical activity have been associated with improved sleep metrics, including increased sleep duration, lower wakefulness after sleep onset, shorter sleep onset latency, lower nighttime awakenings, and increased sleep efficiency (Brand et al., 2010; Ekstedt et al., 2013; Kalak et al., 2012; Khan et al., 2015; Lang et al., 2013). There are also data supporting the benefits of physical activity on sleep among autistic children, such as increased sleep duration, lower wakefulness after sleep onset, shorter sleep onset latency, increased sleep efficiency, and decreased daytime sleepiness (Brand et al., 2015; Lawson & Little, 2017; Narasingharao et al., 2017; Oriel et al., 2016; Samanta et al., 2020; Tatsumi et al., 2014; Tse et al., 2019; Wachob & Lorenzi, 2015). While this is encouraging, these studies involving autistic children were relatively small and did not always include both sexes. Large-scale studies are needed to better understand whether physical activity can improve aspects of sleep health in male and female autistic children and whether any benefits are comparable to nonautistic children. Furthermore, studies reporting positive associations between physical activity and sleep outcomes have tended to be more commonly reported among adolescents (Brand et al., 2010; Kalak et al., 2012; Lang et al., 2013, 2016) and so age differences also warrant further investigation.
To address these gaps in knowledge, we analyzed existing data from the 2018 National Survey of Children’s Health (NSCH) that included 20,845 nonautistic children and 681 autistic children. The aim was to determine whether there was an association between physical activity and age-specific sufficient sleep duration in American children ages 6–17 years old and whether the association was modified by reported ASD status. We hypothesized that higher levels of physical activity would be associated with sufficient sleep duration, and this association would be consistent in autistic and nonautistic children. In exploratory analyses, we tested for sex and age-group differences with respect to the association between physical activity and sufficient sleep duration in autistic and nonautistic children.
Methods
Participants
This study used existing data from the 2018 NSCH (Child and Adolescent Health Measurement Initiative, 2019e). Overall, 176,052 American households were randomly selected, and a total of 30,530 questionnaires were completed (weighted completion rate of 36.9%) (Child and Adolescent Health Measurement Initiative, 2019c, 2019d, 2019e). Caregivers filled out a screener survey to capture basic information (e.g. age, sex, and race/ethnicity) (Child and Adolescent Health Measurement Initiative, 2019e). After completion, one child from each household was randomly selected for caregivers to report upon in a detailed, age-specific questionnaire. We included survey data from 6- to 11-year-old and 12- to 17-year-old age-groups; children under 5 years old were excluded because daytime naps are common (Iglowstein et al., 2003) and their motor skills are incomplete (Malina, 2004). All participants were informed that participation in the survey was voluntary and that their answers would be kept confidential per U.S. laws that allowed the U.S. Census Bureau to conduct the NSCH on the behalf of the Department of Health and Human Services. The Census Disclosure Review Board approved the public de-identified data release (Child and Adolescent Health Measurement Initiative, 2019d).
Sleep outcome
Children (6–12 years old) are recommended to sleep 9–12 hours, while adolescents (13–18 years old) are recommended to sleep 8–10 hours in a 24-hour period (Paruthi et al., 2016). In the NSCH, caregivers were asked, “During the past week, how many hours of sleep did this child get on most weeknights?” (Child and Adolescent Health Measurement Initiative, 2019a, 2019b). The answer choices were <6, 6, 7, 8, 9, 10, or ⩾11 hours per weeknight (Child and Adolescent Health Measurement Initiative, 2019a, 2019b). We categorized children as meeting or not meeting age-specific recommended sleep duration (0 = insufficient sleep duration and 1 = sufficient sleep duration).
Autism spectrum disorder
Caregivers were asked, “Has a doctor or health care provider ever told you that this child has Autism or Autism Spectrum Disorder? Include diagnoses of Asperger’s Disorder or Pervasive Developmental Disorder (PDD)” (Child and Adolescent Health Measurement Initiative, 2019a, 2019b). Caregivers reporting a prior diagnosis of ASD were asked if their child currently has ASD and to classify the severity (Child and Adolescent Health Measurement Initiative, 2019a, 2019b). We therefore created an ASD variable (0 = no ASD; 1 = ASD) and an ASD severity variable (0 = no ASD; 1 = mild ASD; 2 = moderate ASD; 3 = severe ASD). We also categorized children as having ASD with or without intellectual disability (ID; 0 = no ASD; 1 = ASD without ID; 2 = ASD with ID). This was achieved by pairing the ASD status responses with responses to the question, “Has a doctor, other health care provider, or educator ever told you that this child has Intellectual Disability (formerly known as Mental Retardation)?” and the follow-up question asking if the child currently has ID (Child and Adolescent Health Measurement Initiative, 2019a, 2019b).
There were instances where discrepant responses were provided for past and present ASD and ID diagnoses. We categorized children as having reported ASD and ID if the caregiver answered “yes” to ever having ASD and ID, respectively, but had missing data regarding current ASD and ID diagnoses. If caregivers reported “yes” to ever having ASD and ID but reported that their child did not currently have an ASD or ID diagnosis, we categorized these children as not having reported ASD and ID (Healy et al., 2019; Must et al., 2017).
Physical activity
Children are recommended to accumulate at least 60 minutes of moderate-to-vigorous physical activity per day (Piercy et al., 2018). In the NSCH, physical activity levels were captured using the question, “During the past week, on how many days did this child exercise, play a sport, or participate in physical activity for at least 60 minutes?” (Child and Adolescent Health Measurement Initiative, 2019a, 2019b). Children were categorized as followed based on caregiver responses: 1 = 0 days, 2 = 1–3 days, 3 = 4–6 days, and 4 = every day.
Covariates
Age, sex, race/ethnicity, and highest adult level of education in the household were included to describe the sample. These demographic variables were also included as covariates. Shorter sleep duration is more common among older children (Iglowstein et al., 2003; Leger et al., 2012), Black and Hispanic children (Combs et al., 2016; Matthews et al., 2014; Mitchell et al., 2020), and children living in households with lower caregiver education levels (Jarrin et al., 2014; Marco et al., 2011). With respect to sex, male children have a higher prevalence of ASD diagnosis than female children (Maenner et al., 2020); and sleep duration has been reported to be shorter among male children in some studies (Bagley et al., 2015; Matthews et al., 2014; Mitchell et al., 2020) but female children in other studies (Jiang et al., 2015; Lewin et al., 2017; Nuutinen et al., 2013). The same demographic associations hold for physical inactivity, except, female children are more likely to be physically inactive (Cooper et al., 2015; Pate et al., 2019). ASD diagnoses are most common around age 4 years old (Maenner et al., 2020), among male children (Maenner et al., 2020) and among children living in households with higher caregiver education levels (Durkin et al., 2017). ASD diagnoses also vary by race/ethnicity (Durkin et al., 2017; Maenner et al., 2020). In addition, we controlled for being overweight because this has been associated with shorter sleep duration (Mitchell et al., 2013; Padez et al., 2009), physical inactivity (Miller et al., 2018), and ASD diagnosis (Must et al., 2017).
Statistical analyses
Study sample characteristics are presented overall and by reported ASD diagnosis (yes/no). To determine if physical activity level associated with achieving age-specific sufficient sleep duration, multivariate logistic regression was used adjusting for age, sex, race, Hispanic ethnicity, highest household adult education level, overweight, and autism diagnosis. We next tested if the association between physical activity and sufficient sleep duration was modified by reported ASD diagnosis by adding a physical activity-by-ASD interaction term to the model. This interaction analysis was repeated using an ASD variable accounting for reported severity and an ASD variable accounting for reported ASD diagnosed with or without ID. Finally, for exploratory purposes, we tested for a sex difference and an age-group difference by adding the following interaction terms separately: physical activity-by-ASD-by-sex and physical activity-by-ASD-by-age-group. For these three-way interactions, the lower-order two-way interactions were included in the model. Stata 16.1 was used for statistical analyses (StataCorp, College Station, TX). The data set was declared survey data prior to executing logistic regression models, with sampling weights included. We used the margins and marginsplot commands to visually present the findings from the models with two-way and three-way interactions.
Community involvement
There is no community involved in this study.
Results
The sample comprised 20,845 nonautistic and 681 autistic children (Table 1). For the latter, 670 participants had reported autism severity data (53.9% had mild ASD, 36.6% had moderate ASD, and 9.6% had severe ASD) and 679 participants had ID data (15.9% had reported ASD with ID). Among nonautistic children, there was a near equal proportion of each sex. In contrast, autistic children were more likely to be male (77.8%). For autistic and nonautistic children, the average age was 12 years old, the majority identified as White and non-Hispanic or Latino ethnicity, and more than half of caregivers reported the highest household adult education level as college degree or higher. In nonautistic children, 8.3% were overweight while 16.7% of autistic children were overweight. Nonautistic children were more physically active than autistic children. For example, 22.0% of nonautistic children versus 15.3% of autistic children were physically active every day in the past week (Table 1).
Characteristics of study sample by autism spectrum disorder diagnosis.
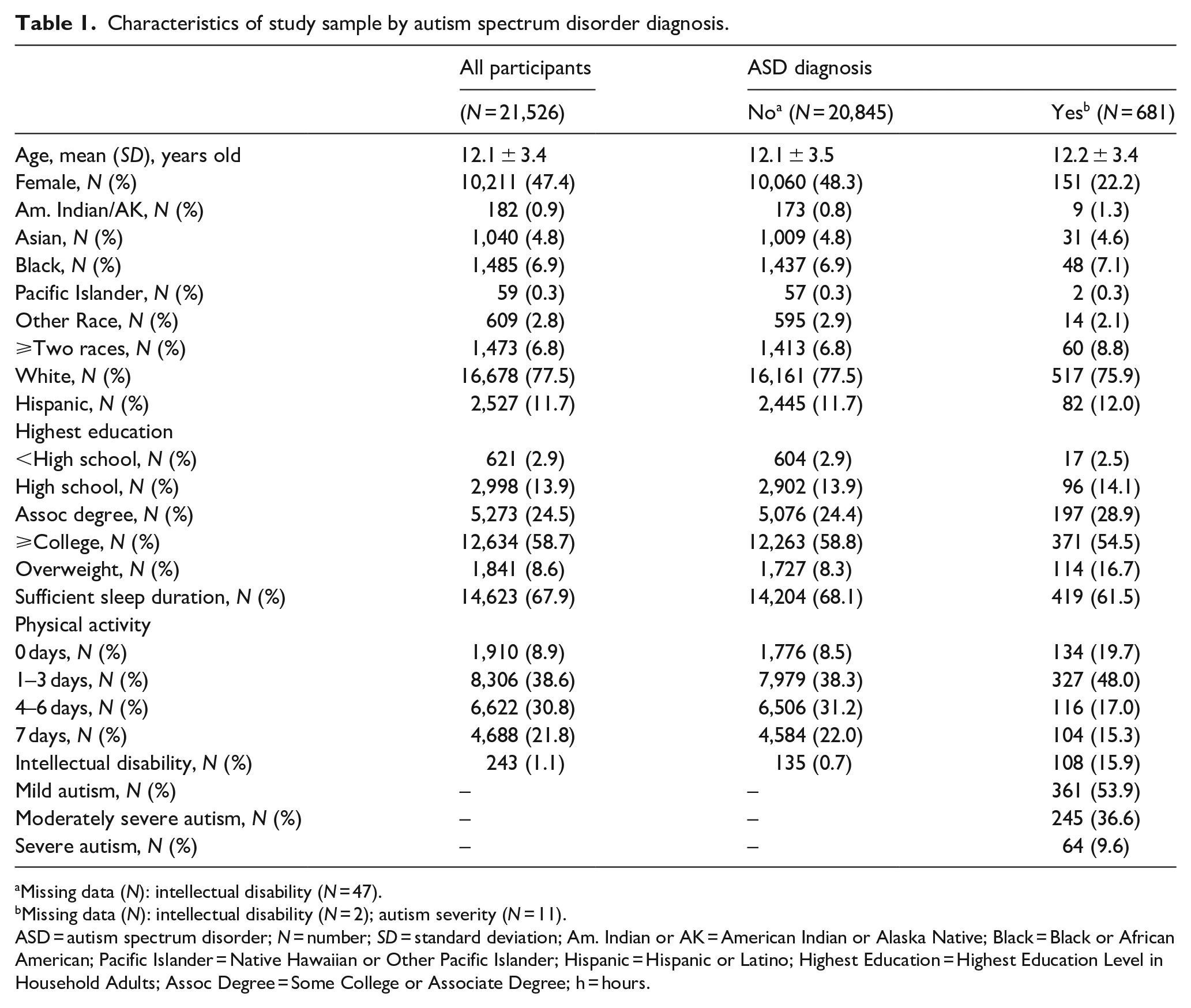
Missing data (N): intellectual disability (N = 47).
Missing data (N): intellectual disability (N = 2); autism severity (N = 11).
ASD = autism spectrum disorder; N = number; SD = standard deviation; Am. Indian or AK = American Indian or Alaska Native; Black = Black or African American; Pacific Islander = Native Hawaiian or Other Pacific Islander; Hispanic = Hispanic or Latino; Highest Education = Highest Education Level in Household Adults; Assoc Degree = Some College or Associate Degree; h = hours.
We first determined if physical activity level associated with achieving age-specific sufficient sleep duration in the full sample (i.e. nonautistic and autistic children combined) adjusting for covariates and reported ASD diagnosis. Compared to zero days of physical activity in the past week, being physically active on 1–3 days, 4–6 days, and 7 days was associated with increased odds of sufficient sleep duration in a dose-response manner that plateaued at 4–6 days (Table 2). Specifically, compared to zero days of physical activity in the past week, the odds of sufficient sleep duration increased 1.43, 1.85, and 1.77-fold for children who were physically active 1–3 days, 4–6 days, and all 7 days in the past week, respectively.
Physical activity and the odds of sufficient sleep duration.
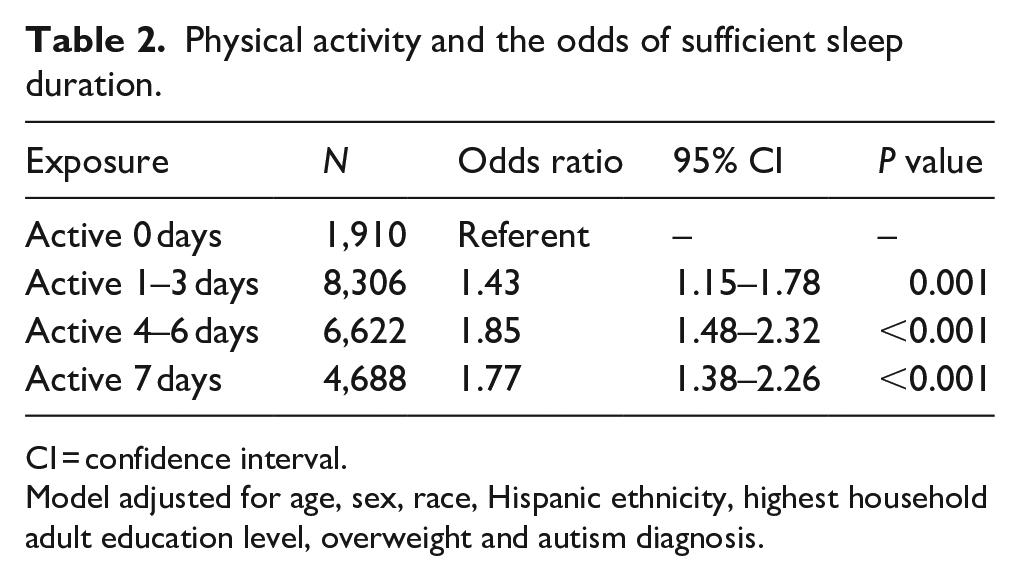
CI = confidence interval.
Model adjusted for age, sex, race, Hispanic ethnicity, highest household adult education level, overweight and autism diagnosis.
We next determined if the association between physical activity and sufficient sleep duration was modified by reported ASD status. Overall, we did not observe a statistically significant interaction between physical activity and reported ASD status with respect to sufficient sleep duration (P interaction = 0.57), indicating that the positive association between physical activity and sufficient sleep duration applied to autistic and nonautistic children (Figure 1). However, it should be noted that confidence intervals (CIs) for the physical activity associations with sufficient sleep duration were wider for autistic children, and point estimates were less pronounced (Figure 1). For example, while not statistically significant, the positive effect of 4–6 days of physical activity in the last week on the probability of achieving sufficient sleep duration was 14 percentage points less among autistic children compared to nonautistic children (β = −0.14; 95% CI: −0.30, 0.02; p = 0.09).
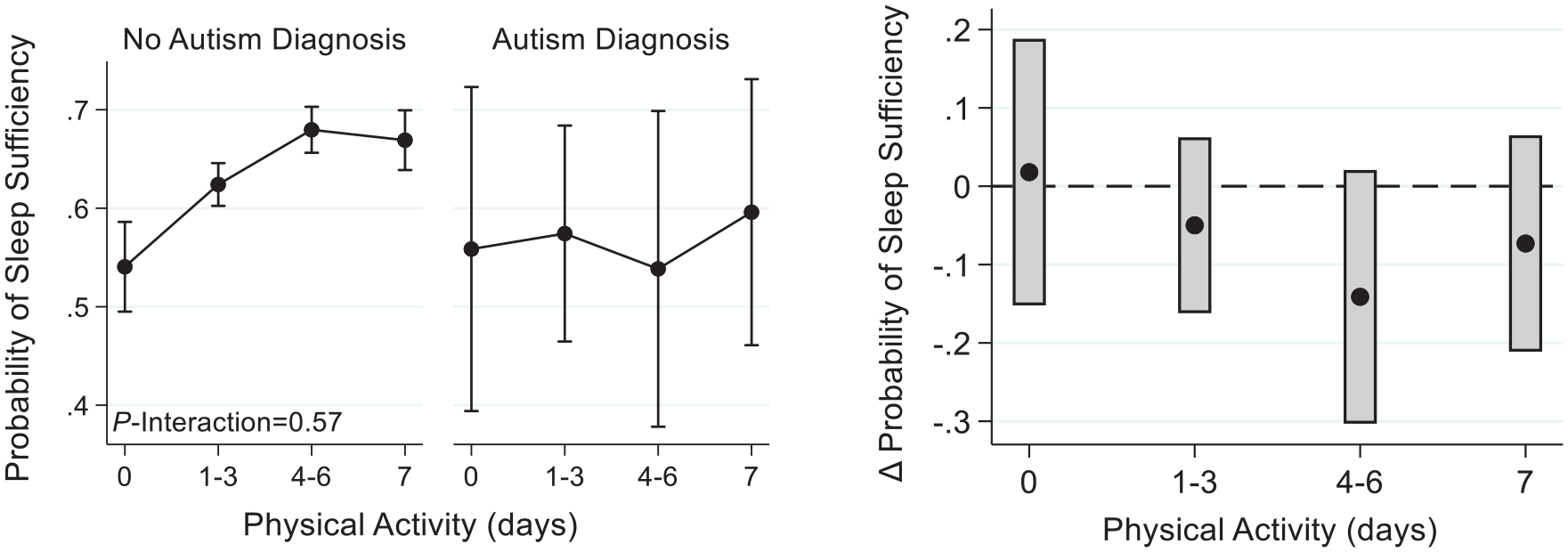
Physical activity-by-ASD interaction results. Left panel: the probability of sufficient sleep duration by physical activity level and reported ASD diagnosis. Right panel: the difference in the probability of sufficient sleep duration by physical activity level for autistic children versus nonautistic children.
Similar observations were made when using reported ASD severity and ASD with and without ID variables (Figures 2 and 3). For example, the positive effect of 4–6 days of physical activity in the last week on the probability of sufficient sleep duration was 42 percentage points lower for children with reported severe ASD compared to nonautistic children (Figure 2; β = −0.42; 95% CI: −0.77, −0.07, p = 0.02) and was 32 percentage points lower among autistic children with ID compared to nonautistic children (Figure 3; β = −0.32; 95% CI: −0.66, 0.002; p = 0.05).

Physical activity-by-ASD severity interaction results. Top panel: probability of sufficient sleep duration by physical activity level and reported ASD severity. Bottom panel: difference in probability of sufficient sleep duration by physical activity level for autistic children accounting for severity versus nonautistic children.
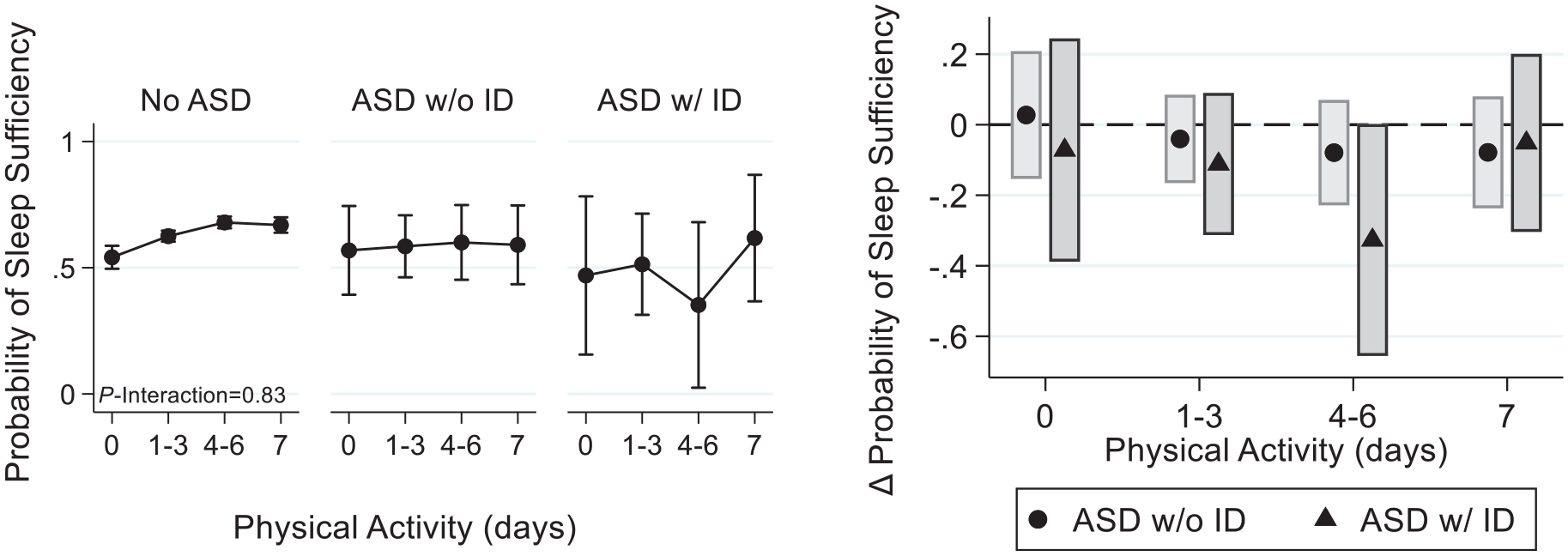
Physical activity-by-ASD with ID interaction results. Left panel: probability of sufficient sleep duration by physical activity level and reported ASD status accounting for ID. Right panel: difference in probability of sufficient sleep duration by physical activity level for autistic children accounting for ID versus nonautistic children.
For exploratory purposes, we tested sex and age-group differences with respect to the association between physical activity and sufficient sleep duration in autistic and nonautistic children. We detected a statistically significant three-way interaction for physical activity, reported ASD status, and sex (P-interaction = 0.03), indicating that the positive association between physical activity and achieving sufficient sleep duration was different for male and female autistic and nonautistic children (Figure 4). Indeed, the positive effect of 4–6 days of physical activity in the last week on the probability of sufficient sleep duration was 43 percentage points lower in autistic female than nonautistic female children (β = −0.43; 95% CI: −0.63, −0.23; p < 0.001). There was no difference in the association between physical activity and sufficient sleep duration for autistic and nonautistic male children (Figure 4).

Physical activity-by-ASD-by-sex interaction results. Left panel: the probability of sufficient sleep duration by physical activity level and sex. Right panel: the difference in the probability of sufficient sleep duration by physical activity level for autistic children versus nonautistic children by sex.
Overall, we did not detect a three-way interaction for physical activity, reported ASD status, and age-group (P-interaction = 0.48), indicating that the positive association between physical activity and sufficient sleep duration applied to younger and older autistic and nonautistic children (Figure 5). However, the positive association of physical activity on sufficient sleep duration may be less pronounced in the 6- to 12-year-old autistic age-group. Notably, the positive effect of 4–6 days of physical activity in the last week on the probability of sufficient sleep duration was 23 percentage points lower in autistic children ages 6–12 years old compared to nonautistic children ages 6–12 years old (β = −0.23; 95% CI: −0.45, −0.02; p = 0.03) (Figure 5).

Physical activity-by-ASD-by-age-group interaction results. Left panel: the probability of sufficient sleep duration by physical activity level by age-group. Right panel: the difference in the probability of sufficient sleep duration by physical activity level for autistic children versus nonautistic children by age-group.
Discussion
A limited number of small-scale studies have investigated the role of physical activity on sleep health in autistic children. We used extensive data from the 2018 NSCH, which was representative of American children and so included autistic children, to determine if there was an association between physical activity and sufficient sleep duration. In general, we found that higher levels of physical activity associated with an increased probability of sufficient sleep duration but associations in autistic children were less pronounced. When we investigated further, we specifically observed no association between physical activity and sufficient sleep duration among children with more severe ASD and autistic children with ID per caregiver report. We also detected sex and age-group differences such that there was no association between physical activity and sufficient sleep duration among female autistic children and autistic children aged 6–12 years. Our findings need to be replicated, especially using objective estimates of sleep duration and physical activity. However, these data suggest that physical activity is a promising approach to improve sufficient sleep duration in childhood but only in certain groups of autistic children.
We found that physical activity was associated with sufficient sleep duration in autistic children with reported mild ASD but not in autistic children with more reported severe ASD and autistic children with reported ID. Limited studies have investigated the association between physical activity and sufficient sleep duration in autistic children with severe ASD and ASD with ID, so direct comparisons to our observations cannot be made. For example, Garcia et al. (2020) found that moderate-vigorous physical activity was associated with higher probability of meeting sleep duration recommendations, but children were recruited from a school that enrolled autistic children with mild severity, without ID. Additional research is needed to replicate our observations and to better understand the relationship between sleep and physical activity in children with more severe ASD. Furthermore, it is possible that physical activity could improve other dimensions of sleep health, other than sufficient sleep duration, warranting additional investigation.
We observed an association between physical activity and increased odds of sufficient sleep duration in male children and nonautistic female but not autistic female children. To our knowledge, this is the first study to demonstrate a sex difference in the context of sufficient sleep duration, physical activity, and reported ASD diagnosis. There is a growing body of evidence that female autistic children may have more sleep difficulties than male autistic children (Angell et al., 2021; D’Agati et al., 2020; Hartley & Sikora, 2009; Mazurek & Sohl, 2016; Petrou et al., 2018; Wang et al., 2016). Therefore, it will be important to understand factors affecting the relationship between sleep and physical activity and if similar findings occur with sleep traits beyond sufficient sleep duration. This could be accomplished by using multilevel socioecological models to consider individual-level factors that could partly explain the sex difference (e.g. sex hormones and pubertal maturation) through to sociocultural factors (e.g. gender-related factors impacting sleep behavior and autism diagnoses) (Billings et al., 2021; Meltzer et al., 2021; Ordway et al., 2021).
We observed an age-group difference whereby no association was observed between physical activity and sufficient sleep duration among autistic children ages 6–12 years old. In a prior study involving 49 autistic children, ages 8–17 years old, with mild severity and without ID, Garcia et al. (2020) reported that the association between moderate-to-vigorous physical activity and longer sleep duration was strongest among younger children (mean age 10.5 years old versus 13.9 years old). Similarly, two other studies that enrolled autistic children under 13 years old found that physical activity interventions (aquatic exercise (Oriel et al., 2016) and basketball skills (Tse et al., 2019)) improved sleep duration. However, adolescents were not enrolled in these studies to directly test for age-group differences. Younger children often have sleep schedules more regulated by caregivers, which could mask the benefits of physical activity on sleep and thus be identified in interventional but not observational studies. In addition, adolescents have increased autonomy and increased sleep regulation by their circadian rhythm making them potentially more sensitive to environmental factors like physical activity (Antczak et al., 2020; Logan & McClung, 2019; Tashjian et al., 2019). Further studies among autistic children are needed that include wider age ranges to determine if the potential positive association between physical activity and sufficient sleep duration is modified by age. This is especially important because physical activity levels are known to decline as children age and mature (Dahlgren et al., 2021; Dumith et al., 2011), and levels of physical inactivity are elevated among autistic children compared to nonautistic children (Gehricke et al., 2020; Healy et al., 2019).
Sleep duration is just one marker of sleep health, and other metrics, such as sleep quality, daytime alertness, and sleep efficiency should be considered (Buysse, 2014; Meltzer et al., 2021). Prior studies have investigated associations between physical activity and these other sleep health metrics among autistic children (Brand et al., 2015; Lawson & Little, 2017; Narasingharao et al., 2017; Wachob & Lorenzi, 2015). For instance, Brand et al. (2015) found that on the nights after an aerobic exercise program, 10 autistic children aged 7–13 years old experienced improved sleep efficiency, wake after sleep onset, and sleep onset latency. Narasingharao et al. (2017) found in 68 autistic children aged 5–16 years old that sleep quality measures, such as duration of uninterrupted sleep, improved after completing a 3-month yoga intervention. Lawson and Little (2017) found that the overall sleep quality of 10 autistic boys aged 5–12 years old improved after completing an 8-week swimming intervention. In general, these studies have small sample sizes, narrow age ranges, and a male predominance. Nonetheless, these studies highlight the importance of considering sleep health metrics beyond sleep duration in future studies.
Clinically, pediatric providers should still encourage autistic children to be physically active for the extensive health benefits it provides (Lobelo et al., 2020; Tiner et al., 2021). Regular physical activity benefits cardiovascular health, bone health, mood, and body composition (lean and fat mass) (Lobelo et al., 2020; Mitchell et al., 2017; Ness et al., 2007; Piercy et al., 2018). While our results suggest that physical activity may not always be beneficial for sufficient sleep duration in all autistic children, this does not mean physical activity is not important and should be neglected. It simply means that when treating insufficient sleep duration, a more personalized approach may be needed for female autistic children, adolescent autistic children, and autistic children with more severe ASD.
Strengths of our study include a large, national sample of American children encompassing both school-age children and adolescents. We also evaluated different subpopulations of autistic children based on reported ASD severity and the presence or absence of ID. Limitations include that the data were derived from caregiver recall; the data capture would have been more rigorous if ASD diagnosis, ASD severity, and presence or absence of ID were derived from medical records; and sleep duration and physical activity patterns were derived from actigraphy. Also, caregivers were not explicitly asked about repetitive behaviors commonly seen in autism, such as rocking, which may have limited the measurement of physical activity levels. Sleep duration was restricted to school nights and physical activity in the last week, so we were not able to perform school and non-school night sleep analyses. In addition, residual confounding may remain as we could not adjust for all physical, cultural, and environmental factors that may be associated with sufficient sleep duration and physical activity in childhood. Our study was cross-sectional, so future studies should focus on longitudinal studies designs to measure changes in sleep and physical activity during childhood development as well as account for sleep variability given that our study was only able to evaluate weekday/school night sleep. In addition, our sample from the NSCH was predominantly White highlighting the need for more diverse samples of autistic and nonautistic children.
In conclusion, we found a positive association between physical activity and sufficient sleep duration in children. Among autistic children, this association holds for those with reported mild ASD but not those with reported severe ASD and ASD with ID. Furthermore, a sex difference was detected where the association between physical activity and sufficient sleep duration was apparent in autistic male but not female children. We also found evidence of an age-group difference where the association between physical activity and sufficient sleep duration was detected in autistic adolescents ages 13–17 years old but not autistic children ages 6–12 years old. Physical activity is a promising approach to improving sufficient sleep duration in children, but the nuances observed among autistic children warrant further investigation.
Footnotes
Acknowledgements
The data were obtained from the publicly available National Survey of Children’s Health funded by the Health Resources and Services Administration (HRSA) Maternal and Child Health Bureau (MCHB).
Author contributions
SES, JAM, and NG conceived the study idea. SES and JAM designed the study with support from NG, ESB, and MB. SES and JAM planned and performed the statistical analyses. SES and JAM wrote the initial draft with critical revisions from NG, ESB, and MB.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SES: NIH/NHLBI T32HL07713; Institute for Translational Medicine and Therapeutics at the Perelman School of Medicine at the University of Pennsylvania
MB and ESB: supported by the Autism Spectrum Program of Excellence (Research gift to the University of Pennsylvania, Daniel J. Rader, MB, and ESB, principal investigators).
JAM: NIH/NHLBI K01HL123612 and NIH/NICHD R01HD100421