
Abstract
Best-practice recommendations for young children at high likelihood of autism include active involvement of caregivers in intervention. However, the use of evidence-based parent-mediated interventions in community practice remains limited. Preliminary evidence suggests that Project ImPACT for Toddlers demonstrates positive parent and child outcomes in community settings. Project ImPACT for Toddlers was adapted specifically for toddlers and teaches parents of young children strategies to build their child’s social, communication, and play skills in daily routines. This study reports implementation outcomes from the initial community rollout of Project ImPACT for Toddlers and examines the system-wide intervention reach, with the goal of informing continued community sustainment and scale-up. Participants include 38 community providers who participated in a Project ImPACT for Toddlers’ training study who completed an implementation survey and semi-structured interviews after approximately 3 months of community implementation. Participants perceived the training model as acceptable and appropriate, and identified several strengths of the approach. Interview themes also supported the feasibility, acceptability, and utility of the intervention in community settings. Quantitative findings complemented the thematic results from interviews. Intervention reach data indicate an increasing number of agencies delivering and families receiving Project ImPACT for Toddlers. Efforts to scale-up evidence-based interventions in early intervention should continue to build upon the model of the Bond, Regulate, Interact, Develop, Guide, and Engage Collaborative.
Lay abstract
Expert recommendations for toddlers who are likely to develop autism include caregivers being actively involved in the services children receive. However, many services available in the community may not follow these recommendations. Evidence suggests that an intervention named Project ImPACT for Toddlers demonstrates positive parent and child outcomes for families in the community. Project ImPACT for Toddlers was designed specifically for toddlers by a group of parents, clinicians, researchers, and funders. It teaches parents of young children strategies to support their child’s development in daily routines. This study reports the perspectives of early intervention providers who learned to use Project ImPACT for Toddlers on whether the intervention was a good fit for their practice and easy to use. The study also examines how many agencies are using Project ImPACT for Toddlers and how many families have received the intervention in the community. The goal of the study is to inform the continued use of Project ImPACT for Toddlers in the community and support offering the intervention in other regions. Participants include 38 community providers who participated in a training study of Project ImPACT for Toddlers and completed a survey and semi-structured interview after approximately 3 months of using Project ImPACT for Toddlers with families. Participants perceived the training model as acceptable and appropriate, and identified the group-based model of training, comprehensive materials, and agency support as strengths of the approach. Survey findings complemented the results from the interviews. Data indicate an increasing number of agencies and families accessing Project ImPACT for Toddlers. Efforts to expand evidence-based intervention in early intervention should continue to build upon the model used for Project ImPACT for Toddlers.
Keywords
It has been long established that parent involvement in early intervention is crucial for optimal child outcomes (Maglione et al., 2012; National Research Council, 2001). In early parent-implemented autism interventions, parents learn to use techniques and to integrate evidence-based strategies into their daily routines with their young child. While efficacy data for early parent-implemented autism interventions are promising (e.g. Kasari et al., 2014; Rogers et al., 2014; Sandbank et al., 2020; Solomon et al., 2014; Wetherby et al., 2014), there are currently no parent-implemented autism interventions for toddlers with demonstrated effectiveness in large community-based trials. According to local agencies, providers, and parents, there continues to be limited capacity to effectively serve families of toddlers at high likelihood of having autism in the community and available services often lack quality. Services are highly variable based on geographic location, cultural fit, community resources, and provider training (Drahota et al., 2020).
To remedy these service gaps, systematic efforts to deliver evidence-based intervention (EBI) specifically designed to meet the needs of toddlers with or at high likelihood for autism and to be feasible within existing community early intervention services are needed. A review by experts in the field led to recommendations for best practice care for young children with and at high likelihood of having autism included ensuring: (1) a combination of developmental and behavioral strategies, delivered as early as possible; (2) active involvement of caregivers as part of the intervention; (3) a focus on core autism symptoms, such as social communication; and (4) individualization based on family needs and culture (Zwaigenbaum et al., 2015). These recommendations are consistent with community-focused recommendations for the use of family-centered help-giving practices in early intervention broadly (Dunst et al., 2007) and fit with the mission of the federally funded early intervention (i.e. under age 3) services which is to enhance the development of infants and toddlers with disabilities and the capacity of families to meet the needs of their young children with disabilities (Individuals With Disabilities Education Act (IDEA), 2004).
Despite wide agreement on how to best support toddlers with or at high likelihood of autism, however, meeting these recommendations can be challenging. Family involvement strategies are not widely implemented in community settings, despite being a value and mandate of publicly implemented early intervention systems (Grygas-Coogle et al., 2013; Hume et al., 2005). For example, data indicate that the parent plays a passive rather than active role in a majority of Part C early intervention sessions (Aranbarri et al., 2017; Campbell & Sawyer, 2007). Training for early intervention providers equips them to work directly with children with general developmental delays, but not to build parent capacity or coach parents effectively (Fleming et al., 2011), or to address autism symptoms specifically (Ingersoll et al., 2012). The field of early intervention has begun to focus more strongly on how to optimally coach parents (Fettig & Barton, 2014; Friedman et al., 2012; Pellecchia et al., 2020) as well as how to address symptoms related to autism in the context of early intervention (Aranbarri et al., 2017; Stahmer et al., 2017), but considerable work is needed in these areas to effectively move these skills to day-to-day, community practice. This study describes the nature and impact of one such long-standing community-partnered effort aiming to translate and implement evidence-based, parent-mediated interventions for young children at high likelihood for autism in community agencies delivering early intervention services to children under 3 years old.
Community involvement: the BRIDGE collaborative
The BRIDGE Collaborative is a group of early intervention stakeholders who came together to address the need for high-quality early intervention within their community. The BRIDGE Collaborative was founded in the principles of community-partnered participatory research (CPPR; Israel et al., 2005), with the goal that community partners and researchers engage as equal partners in the research process. The BRIDGE (Bond, Regulate, Interact, Develop, Guide, and Engage) name is comprised of shared early intervention values and represents the connection the group aims to build between research and practice, as well as between parents and children (see Brookman-Frazee et al., 2012). The group includes clinical providers, funding agency representatives, parents of individuals with autism, and autism services researchers. The goals and activities of the BRIDGE Collaborative, including the research detailed here, involves stakeholders to provide direction, inform methods, and ensure acceptability and appropriateness. Over the last 15 years, this community-academic partnership (Brookman-Frazee et al., 2012) has utilized a range of implementation strategies to improve early intervention for children with social communication challenges and their families in their local community (Rieth, Stahmer, & Brookman-Frazee, 2018).
Project ImPACT for Toddlers
After a discussion of shared goals and values, the initial work of the BRIDGE Collaborative centered on the selection of an intervention model to promote in community practice. The Collaborative conducted local needs assessments and consensus discussions (Powell et al., 2015) to choose an evidence-based practice with potential to support a broad range of providers and families in early intervention in our community. The selection process and guiding values are detailed in Brookman-Frazee et al. (2012). The group used consensus-based decision-making to ultimately identify Project ImPACT (Improving Parents as Communication Teachers; Ingersoll & Dvortcsak, 2019) as the best fit. Project ImPACT is a parent-mediated, naturalistic, developmental, behavioral intervention that is identified as an EBI for children with autism (Steinbrenner et al., 2020). The intervention aims to teach parents strategies to promote their child’s social engagement, communication, imitation, and play skills in daily routines.
After selection, however, initial pilot testing of Project ImPACT by providers and families in the community revealed several areas of needed adaptations to improve its fit for toddlers and the agencies that serve them in service of maximizing community sustainment and uptake. Iterative adaptations to the intervention and training materials were made through pilot testing, expert and clinician feedback, and consultation with Project ImPACT developers to ultimately develop a targeted version of the intervention, known as Project ImPACT for Toddlers (PIT; Haine-Schlagel et al., 2020; Stahmer et al., 2020). Final products of the adaptation process included both a revised parent coaching manual and full interventionist training materials with flexible delivery options (e.g. in-person and online didactic options, and structured coaching procedures) to match the variable needs across community agencies. Following the adaptations, a quasi-experimental pilot test comparing PIT to usual care early intervention services demonstrated more positive outcomes after receiving PIT for both parents and children, including greater changes in parent interaction style and promising impacts on children’s social communication skills (Stahmer et al., 2020). In addition, providers trained in PIT had moderate to strong adherence to intervention fidelity, and fidelity to the model predicted parent outcomes.
Community uptake of PIT was initially supported through a series of research studies designed to build local capacity for the intervention, including a train-the-trainer effort implemented across 12 early intervention agencies. To facilitate implementation, the Collaborative designed educational materials and a dynamic training for PIT involving both didactic instruction and hands-on-practice with feedback that prepared clinical providers to utilize PIT. Simultaneous with the training effort, a specific contract for funding was first offered to early intervention agencies to deliver PIT to families by San Diego Regional Center (SDRC), the local funder of public early intervention services. This contract was discussed and developed via the Collaborative, which includes several key members of the Early Start administration. Taken together, these factors represent multiple strategies known to facilitate community EBI implementation (Powell et al., 2015).
Implementation outcomes framework
In the current analyses, we applied the Proctor et al. (2011) taxonomy to guide evaluation of implementation outcomes realized as part of the community-partnered effort to train agencies in PIT. Implementation outcomes are important to consider as they are a necessary precondition for clinical or treatment outcomes (Proctor et al., 2011). This framework has been successfully applied to interventions for autism within public schools (Locke et al., 2016) as well as mental health interventions used with individuals with autism (Dickson et al., 2021). The Proctor and colleagues (2011) taxonomy specifies eight distinct outcomes: (1) acceptability (satisfaction); (2) adoption (intervention use or intention to try); (3) appropriateness (intervention relevance or usefulness); (4) feasibility (or intervention fit or utility); (5) fidelity (adherence and delivery quality); (6) implementation cost (cost-benefit and cost-effectiveness); (7) penetration (proportion of clients with whom the intervention is used); and (8) sustainability (continued use and routinization). Four of these outcomes are directly addressed through secondary data analyses in this study, including appropriateness, acceptability, feasibility, and sustainability. Intervention reach is examined via the penetration of the intervention at the agency level and the volume of families receiving PIT in the community 5 years after the training study.
Study aims
The purpose of this study is to: (1) utilize mixed qualitative and quantitative methods to characterize the short-term, provider-level implementation outcomes from the initial community training effort in PIT, including determinants of outcomes and (2) identify the long-term, system-level sustainment outcomes of PIT (penetration and reach) in publicly funded early intervention services. The overall goal of these aims is to inform scale-up and further sustainment of evidence-based early intervention.
Method
Implementation outcomes (Aim 1)
Training study context
This study reports implementation outcome data from a PIT community training effort (Rieth, Stahmer, Dickson, et al., 2018). The training study evaluated a train-the-trainer approach of PIT via a multiple probe design (Horner & Baer, 1978). Participating agencies identified individuals as “agency trainers,” who then participated in PIT training with the clinical research team. Each agency trainer then provided training on PIT content and delivery to direct service providers at their agency, with support from the research team. Feedback was solicited from both agency trainers and service providers on their perspectives via both qualitative (interview) and quantitative (survey) methods. The current analyses combine these sources to examine implementation outcomes of the training effort and initial intervention rollout.
Training study data
Mixed qualitative and quantitative methods were used to examine implementation outcomes related to PIT and the training process via quantitative feedback surveys and qualitative interviews. Data were solicited from providers after they received training and had delivered PIT to families for at least 3 months in their usual clinical practice. All data collection procedures were approved by the University of California, San Diego Institutional Review Board and relied on by participating institutions. All study procedures conformed to the US Federal Policy for the Protection of Human Subjects.
The participant sample and training process is briefly described below. A full description of the methods and sample from which participants were drawn is available in Haine-Schlagel et al., (2020).
Participants
Agencies providing early intervention services in two counties were identified based on their involvement and prior participation with the BRIDGE Collaborative or via recommendation of a BRIDGE member. Participants were recruited from 12 community agencies that provide early intervention services through California Early Start, the program for public funding of early intervention (IDEA, 2004). Publicly available data indicate that race/ethnicity for families receiving California Early Start services are as follows: 10% Asian, 5% Black or African American, 58% Hispanic/Latino, 3% two or more races, and 25% White. Although these data are on the demographics of families receiving early intervention services broadly, we expect that these demographics roughly parallel the populations served by participating agencies.
A total of 59 providers enrolled in the train-the-trainer study as either agency trainers (n = 14) or therapists (n = 45), with 38 total providers contributing feedback data in the current sample (agency trainers n = 14, 100% response rate; therapists n = 24, 53% response rate; 64% response rate overall). Given the moderate response rate for therapists, responders and non-responders for the implementation measures reported here were compared on baseline demographic characteristics of race, ethnicity, primary discipline, age, and caseload (chi-square) as well as years of experience with early intervention, autism spectrum disorder (ASD), and parent coaching (t-tests). All tests revealed no significant differences between groups (p < 0.05). Eligibility criteria included (1) a master’s degree or equivalent degree or credentials in a relevant field or specialty; (2) agency employment for at least 6 months; and (3) provision of direct services to infants and toddlers with social communication concerns. Providers invited to participate were selected by each agency and then enrolled on a first come, first serve basis. Participants did not have prior experience with the PIT intervention specifically. Full demographics for those in the current sample are displayed in Table 1.
Participant demographics.

M: mean; SD: standard deviation; ASD: autism spectrum disorder.
Procedures
ImPACT training
All participants received training in PIT from either members of the research team (n = 14) or agency trainers at their own agencies (n = 24). Training took place over a period of approximately 6 months in groups of three to five individuals. For all participants, training involved (1) a 12-week PIT training period with alternating didactic and in vivo coaching sessions with feedback on working directly with families and (2) a 12-week period of PIT implementation and ongoing coaching with clients on their current caseload. Expert mentors from the research team provided ongoing consultation and coaching to all trainers throughout as needed/requested by the trainer. A full discussion of the training model is available in Rieth, Stahmer, Dickson, et al. (2018) and Rieth, Stahmer, & Brookman-Frazee (2018). In addition, implementation checklists for the didactic workshops, live coaching, and ongoing coaching portions of the model are available from the authors.
Implementation feedback
A follow-up assessment was completed 3 months after completion of training (both the initial training and implementation/coaching phases), during which participants had been utilizing PIT in routine clinical care. The follow-up assessment included an implementation survey and a brief phone interview to gather feedback on the intervention itself as well as the training process for PIT. Both measures are described in detail below.
Measures
Demographics
At baseline, all participants reported on their sociodemographic characteristics, including age, race, ethnicity, and professional history.
Implementation survey
A 41-item questionnaire was utilized to examine implementation outcomes across six subscales including training acceptability, training appropriateness, training feasibility, intervention appropriateness, intervention acceptability, and sustainability. Using a 5-point Likert-type scale (1 = strongly disagree to 5 = strongly agree), participants rated both the training they received in PIT as well as the intervention itself. This survey was adapted from several sources examining implementation of evidence-based practices in other disciplines (Halliday-Boykins et al., 2005; Haug et al., 2008; Lehman et al., 2002). Example questions included (1) “I am satisfied with the PIT training materials” (Training Acceptability); (2) “I have space and equipment needed to participate in PIT Training effectively” (Training Appropriateness); (3) “PIT training provided me with the skills needed to implement PIT effectively” (Training Feasibility); (4) “I feel comfortable using the PIT materials in my program” (Intervention Appropriateness); (5) “I would want to invite other staff from my agency to receive PIT training” (Intervention Acceptability); and (6) “Therapists at our agency will now be trained in PIT as part of the general training process” (Sustainability). Alpha values for subscales ranged from 0.36 to 0.87. Table 2 shows the number of items and alpha values for each scale. All subscales with an alpha value below 0.60 were dropped from further analyses (i.e. Training Acceptability and Training Appropriateness), resulting in a total of 23 items utilized in current analyses. Implementation surveys were available for 32 providers (84%).
Implementation survey subscales, item information, and reliability.
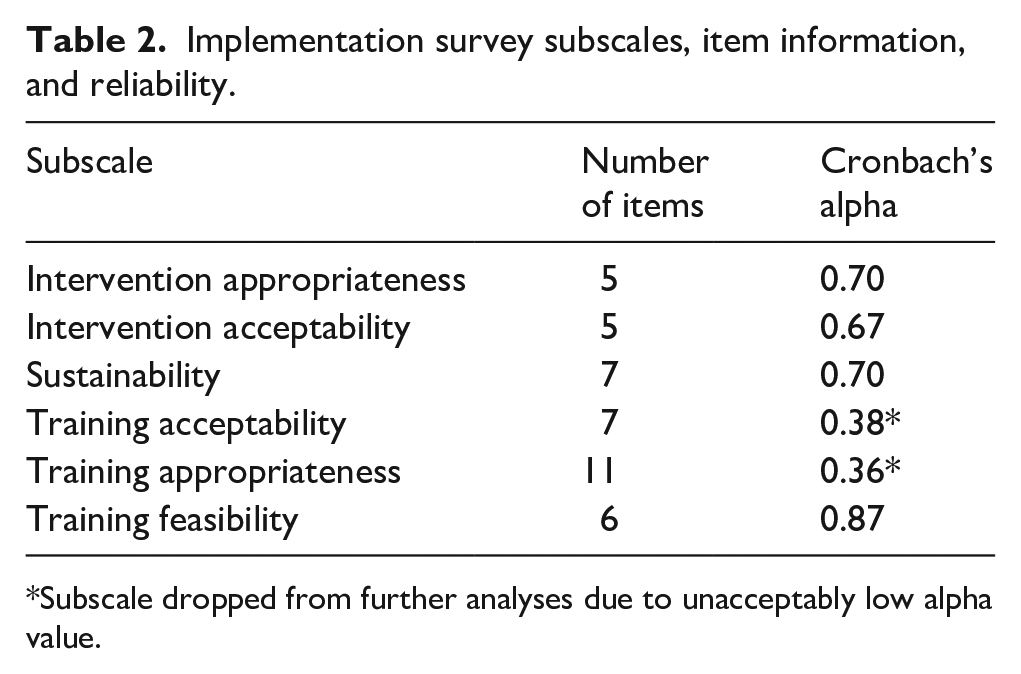
Subscale dropped from further analyses due to unacceptably low alpha value.
Semi-structured interview
A brief semi-structured interview was conducted with all interested participants. All interviews were conducted by a trained member of the research team who was not involved in the training of participants. Interviews were guided by a series of questions related to implementation outcomes, including feasibility, acceptability, appropriateness, and sustainability. All interviews were recorded and transcribed for later analyses. The interview guide questions were developed simultaneously with the survey. Interviews were available for 26 providers (68%). The average duration of the interviews was 17.36 min.
Data analyses
The mixed-methods complementarity approach was used in which the qualitative interview data and quantitative survey data were compared side by side to determine commonalities and/or differences across the two methods (Palinkas et al., 2011). Qualitative interview data were analyzed using content analysis concerned with manifest constructs (Bengtsson, 2016). Interview transcripts were entered, coded, and analyzed in QSR-NVivo 2.0, a program frequently used in qualitative research (Tappe, 2002). After transcription, two interviews were randomly selected and examined jointly by two members of the research team to elicit a priori and emergent codes within the interviews and generate a codebook. Segments of the texts, ranging from sentences to paragraphs, were assigned specific codes that enabled members of the research team to consolidate interview data into analyzable units. A senior member of the research team reviewed the codes for accuracy and comprehensiveness relative to the interviews. Two members of the research team then independently coded one additional transcript and codes were checked for consensus and accuracy by a senior team member. Following this process, all interviews were coded, with 27% of interviews coded by both team members and checked for agreement. A review of double coded transcripts was conducted whereby members of the research team reached consensus as to which codes should be applied to specific segments of text. Adjustments were made to independently coded transcripts based on consensus discussions, and any areas of discrepancy or concern were discussed with the team. Emergent themes were identified and assigned a code by considering the frequency of and salience with which (i.e. importance or emphasis) a participant discussed it. Quantitative survey analyses primarily consisted of descriptive statistics to characterize implementation outcomes.
Intervention reach (Aim 2)
To identify the reach of PIT in the local community, data were solicited directly from SDRC. The director of Autism Services at SDRC, a member of the BRIDGE Collaborative, facilitated data collection from agency records. Data requested included (1) the number of early intervention agencies with active vendor contracts to provide PIT services through SDRC and (2) the number of SDRC consumers (families) receiving PIT funded by SDRC across the years 2016–2020. These years were selected based on the conclusion of the community training study and the start of PIT contract availability from SDRC (2016) and the end date of available compiled data in the SDRC system (2020). Data solicited from SDRC referred to any agency with a contract to provide PIT, independent of past involvement in any research or training studies. This broad net was cast to capture the extent to which PIT is integrated into the service system after its initial rollout supported by the research team (in 2016). Descriptive statistics were calculated to describe the reach data solicited from SDRC about the extent of PIT use in the community by SDRC contracted agencies.
Results
Implementation outcomes (Aim 1)
Themes regarding participants’ perception of PIT and the training were distilled from both the qualitative and corresponding quantitative data. Outcomes revealed no major differences between agency trainers and therapists in the interview or survey data, and thus, the groups were collapsed for reporting. The results are presented as the implementation outcomes related to PIT training (acceptability, appropriateness, and feasibility) and those related to the intervention (acceptability, appropriateness, and sustainment; Aarons, Sklar, et al., 2017; Proctor et al., 2011). Initial themes are presented, with corresponding sample quotes from our qualitative interviews for each theme included in parentheses. When available from the qualitative data, facilitators and barriers to each outcome are discussed, with sample corresponding quotes also included in parentheses. Quantitative data follow for each theme, although data for two subscales are not reported due to low alpha values (training acceptability and training appropriateness, see Table 2).
Training acceptability
Our qualitative results indicate high training acceptability, with participants indicating that they found it engaging and acceptable (“[PIT] was one of the best trainings I’ve ever had.”). Primary facilitators that emerged around training acceptability included the group-based model for training (“Really enjoyed having kind of that sense of a cohort. You’re working together, you’re learning together.”), the training materials themselves (“It was very, very well laid out and all of the materials were easily accessible, easy to use, you know very user friendly.”), and agency support for participating in the training (“Our director was . . . very open to us doing this and happy that we had gotten trained . . . We set up the consistent room and place every other week for our training. So that was like, our organization making sure we had the computer and putting it up on the screen and everything.”). However, agency policies also emerged as a barrier to providers’ availability to participate in training (“I’m trying to advocate for my therapists to have time allocated for them to do Project ImPACT.”).
Training appropriateness
Participants reported the training experience as relevant or practical and fit their needs and values (“[PIT] was explained in a way that I was able to learn and understand.”). A key facilitator of the appropriateness of training included the model of providing in vivo coaching with feedback (“Really helpful in the process was getting that hands-on experience . . . having the feedback from (a coach).”). However, a consistent barrier noted by participants was the large amount of content covered in the weekly meetings (“It just felt like it was a lot of information . . . You had good amount of time to go through all the stuff . . . it all felt adequate it’s just a lot of information at once.”).
Training feasibility
In interviews, providers consistently reported that they found PIT training to be helpful in impacting their work with families (“The material presented was really meaningful . . . actually changed my practice with not only the Project ImPACT families I’m working with right now, but also with the other families I was working with in the agency, so it was really eye opening.”). Key facilitators to the utility included the comprehensive and structured nature of the PIT materials (“I liked having kind of the structure for to be able to have that for the parent. To be able to have something to be like okay let’s start with this, let’s look at this.”) and the accountability of in-person meetings with live practice (“It held me accountable . . . being able to you know talk with other people . . . receive feedback from other people and see other people you know go through what I’m going through.”), as well as how the strategies built on their existing knowledge but provided new tools (“Strategies that we’ve already been using but we didn’t really know how to explain it to parents . . . it sort of gives terms and simplifies these strategies that are really easy to explain to family members.”). A primary barrier to the feasibility, however, was the time commitment (“What was challenging for me was just the time commitment . . . I had to you know, reorganize my caseload at that time . . . and really commit to that chunk of time each week.”). Quantitative results for the feasibility of training subscale supported the largely positive qualitative results, indicating that therapists found the training to be practical for their clinical practice (M = 4.29, standard deviation (SD) = 0.48).
Intervention acceptability
Interview participants reported that they enjoyed delivering PIT to families, found it easy to put into practice, and thought the materials were simple to follow. The emphasis on parents was particularly a match for providers’ values (“We are teaching the parents to do the work, and so I think that including them and making them feel empowered was probably one of the most important things we can do. Especially with the families that we serve here, we are a disadvantaged community, so we really need to make them feel empowered to make choices.”). Characteristics of parents were also sometimes a barrier to the more structured nature of PIT, however, as some providers found it difficult to manage the parent’s agenda for the session in conjunction with the PIT topic (“It was not always easy to follow the kind of session plan and also like adequately answer all of the parents’ questions too. Because parents also have just, like a lot of questions . . . And sometimes their questions pull us kind of off topic.”). Complementing these findings, quantitative results for the five items on the acceptability of PIT indicated that providers found the intervention and the materials highly acceptable and would recommend the intervention to other clinicians (M = 4.14 and SD = 0.54).
Clinical intervention appropriateness
Providers reported that the materials and structure of PIT were appropriate for their role with families and was a good match with the content and background knowledge that they brought to their role as early interventionists. The ease of use and similarity to other interventions that had previously learned were key facilitators (“That’s one of the nice things about Project ImPACT, it sort of gives terms and simplifies these strategies that are really easy to explain to family members.”). One key barrier that providers discussed was the difficulty in coaching parents if they were not already comfortable with a coaching format (“Like coaching them and maybe some challenges that they are having. That was difficult for me, in the beginning . . . How do I provide feedback to this mom without telling her, hey you know you’re prompting, over prompting . . . you’re not following all the steps for prompting.”). However, the specific strategies incorporated into PIT training to address this need and were valued greatly by providers (“We really need to make (caregivers) feel empowered to make choices and I actually found out my therapists were really receptive to those. They actually really liked the ACEs (parent engagement strategies).”). These specific perceptions related to strategies to engage and coach parents are reported in Haine-Schlagel et al. (2020). The five items of the intervention appropriateness subscale supported the qualitative findings, indicating that providers found the procedures of PIT to be a reasonable match with their existing clinical practice (M = 3.90 and SD = 0.47).
Sustainability
The primary theme that emerged from the qualitative interviews related to sustainability was the way in which PIT strategies and components generalized into therapists’ clinical practice once they had learned the intervention (“[PIT] is really something that is pushing into other areas of work” and “[PIT] actually changed my practice not only with the Project ImPACT families I am working with right now, but also with other families I am working with”). The seven items related to the sustainment of PIT indicated a moderate level of willingness to continue participation in further PIT training and to continue to use the intervention with new families (M = 3.13 and SD = 0.73).
Intervention reach (Aim 2)
In 2016, the first two early intervention agencies were contracted to deliver PIT with SDRC. As of June 2021, a total of 28 agencies were contracted to provide PIT to families in the San Diego and Imperial county regions, demonstrating the growing reach of PIT and PIT training in the local community. These agencies represent 51% of the total number of agencies contracted to provide services to infants and toddlers with developmental disabilities with SDRC (n = 55).
Figure 1 represents the number of children who have received Project ImPACT across the years 2016–2020 as funded by SDRC. As illustrated by the date, there are a steadily increasing number of children receiving Project ImPACT. Children receiving Project ImPACT were an average of 23.31 months old (SD = 5.14) at the start of service.
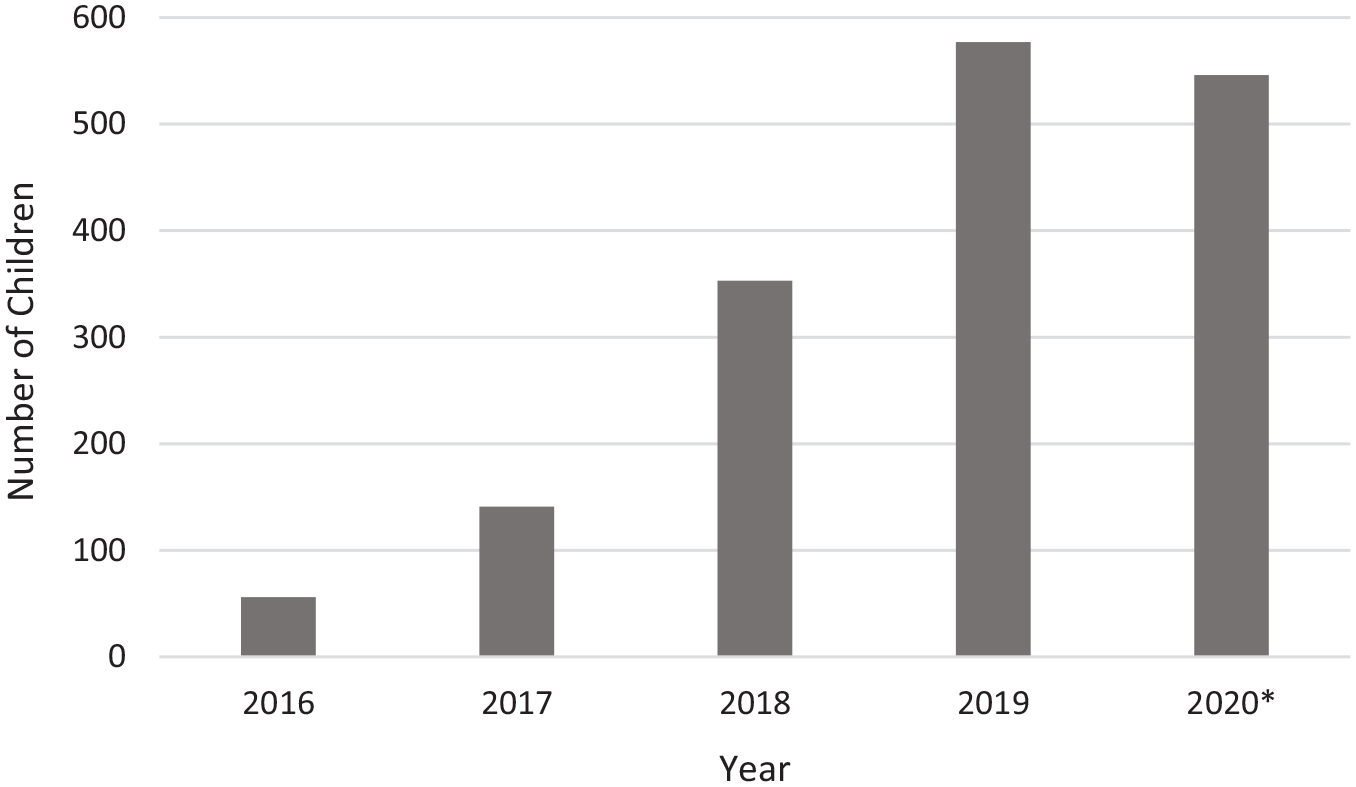
Children receiving Project ImPACT for Toddlers in community services.
Discussion
The implementation outcomes for training efforts in PIT within the local community thus far appear strong, with expanding reach in terms of the number of children receiving the funded service. A growing number of agencies have contracted with the local regional center to provide PIT in the community, illustrating the strong fit of the model for the service system. Findings also extend the literature on key components for effective provider training, with results highlighting the importance of user-friendly materials, group-based trainings, and multiple opportunities for feedback to support provider learning.
The facilitators of positive implementation outcomes identified here represent key recommendations for future implementation efforts within the early intervention service system. Specifically, clear, structured materials that providers view as a match for their clients’ needs and adjacent to their existing clinical skills supported their positive view of the training experience and the intervention itself. Efforts to develop professional and high-quality intervention materials that are easy for providers to access and navigate in a variety of modalities (e.g. book/hardcopy and electronic access) will likely support future scale-up efforts. In addition, the opportunity to receive ongoing in vivo supervision on use of the model was highly valued by therapists. The availability of live feedback is often a costly feature of trainings to implement, especially on an ongoing basis, but these results demonstrate the importance of this approach in supporting positive perceptions. Finally, agency support for training and use of PIT was cited by participants as particularly helpful, supporting recent efforts to approach implementation through intervention at the leadership level (Aarons, Ehrhart, et al., 2017; Green et al., 2014).
It is likely that the iterative, community-informed intervention adaptations and training development greatly facilitated the positive outcomes reported here, and will continue to be important for scale-up of PIT to new regions. The train-the-trainer model resulted in positive perceptions from both groups involved, the trainers and the therapists. Early intervention agencies involved in the BRIDGE Collaborative have repeatedly indicated that intervention models that require each individual provider to be externally certified and trained, often at high monetary and time costs, are not appropriate or sustainable for their companies. The PIT model tested here allowed agencies to develop capacity to train their own staff in a way that was positively received. This success is consistent with the need for context-specific adaptations that consider fit across multiple levels to promote strong implementation outcomes. Since the time this study was conducted, the Project ImPACT developers have created a certification model that continues to allow an individual to train others within their agency after meeting training and fidelity requirements, similar to the model reviewed here.
Of the implementation outcomes queried, sustainability scored the lowest quantitatively and the qualitative themes were limited. Providers referred to the generalized use of PIT elements within broader practice, but did not speak specifically to their continued or ongoing use of PIT or the PIT training. However, the reach data indicate strong growth in the number of families who are receiving PIT, which indicates that therapists must in fact be using the approach with new families and/or that new therapists are being trained. It may be that the interview questions and sustainability focused survey items did not capture the sustainability outcome accurately, and a later or broader exploration of implementation outcomes for PIT should consider this area more directly and explicitly.
Findings regarding the barriers to PIT training and intervention highlight the need for continued refinement to try to simplify interventions and trainings to aid learning and delivery. Providers found the amount of information in PIT overwhelming and difficult to manage. In a system where providers are likely to have high caseloads and burn out is common, perceptions of this complexity could prevent therapists from selecting to engage in training or continued use. Members of the BRIDGE Collaborative have often debated the balance between wanting to ensure that providers have enough information (e.g. foundational understanding of multiple domains of development, detailed knowledge of the intervention strategies themselves, and techniques to engage parents) while also keeping the content streamlined and accessible. Given that providers likely come to the table with varying levels of knowledge and experience, a modular approach to the content that allows providers to tailor their own training may be optimal. As noted by providers here, clear intervention materials can also be a great facilitator in ensuring learning, so time spent developing quality materials is not misplaced. The focus on balancing the amount of information may be especially relevant for EBIs for autism, where a large portion of recommended EBIs are multi-component and data show poor fidelity of these multi-component interventions in community settings (e.g. Mandell et al., 2013).
Differences in perspective between agency trainers and therapists may have been expected based on previous literature reporting differences in opinions between leadership and direct service providers (Beidas et al., 2018). However, agency trainers were identified by individual agencies rather than by specific leadership criteria in this study, and it is likely that the two groups were not fully distinct in the current sample. This is evident in the demographic information regarding the two groups, which reveals a high degree of overlap in terms of parent coaching experience, specifically, as well as other factors. Given the similarity between the two groups, it is not surprising that their perspectives were similar. Despite the positive implementation outcomes thus far, there remain several critical unknowns and areas for future research regarding the use of PIT in the community. First, the intervention fidelity with which therapists are utilizing PIT was not assessed in the current analyses. Although data available from the pilot study of PIT demonstrate the ability of community providers to implement PIT with fidelity (Stahmer et al., 2020), it could be that some providers feel positively about the training they received and the strategies themselves, but still have difficulty actually implementing the approach with families. It will be important to measure to what extent community providers are able to successfully adhere to the coaching and parent engagement strategies of PIT, as this is a known area of challenge for the early intervention service system broadly. Future work should also systematically explore the remaining aspects of the Proctor et al.’s (2011) implementation taxonomy that were not available from the measures examined here, including adoption, caseload penetration, and cost.
An additional area for future examination is the successful implementation of PIT with early intervention providers with various levels of experience. The BRIDGE Collaborative made intentional decisions in the rollout of PIT training to engage relatively experienced service providers who were likely to be prepared and successful in coaching parents (represented by MA degrees). The average years of experience of the participating sample were over 10 years in EI/ASD/parent coaching, representing a more skilled workforce than many therapists who are providing direct early intervention services to families. While the reach data presented here support the ability of agencies to continue to deliver PIT by providers with the required level of expertise, future research should focus on whether the approach may also be feasible, well-received, and successful when delivered by members of the early intervention workforce with less experience.
A primary limitation of this study is the fact that implementation outcomes were solicited from participants who participated in a training research study and willing to respond to the survey and interview. Although all participants were employed by community early intervention agencies, those willing to engage in training via research participation may be qualitatively distinct from service providers who do not select to participate in such opportunities, and those that chose to respond may have been only those that felt positively. Implementation outcomes regarding PIT from a group of providers who are less eager to be involved in research may reveal different results than those identified here, and further exploration of PIT should attempt to capture perspectives from multiple viewpoints. The early intervention service landscape is comprised of providers with a variety of motivation and skill levels, and it is important that PIT be a good match across the full range of interventionists. Additional limitations include the short period of time from training to assessment (3 months) and the somewhat limited response rate to the surveys and interviews from the full sample of providers who participated in the training study.
In conclusion, early intervention providers who learned PIT in a community training study reported the intervention to be acceptable, appropriate, and feasible for their clinical practice. The growing penetration of the intervention in terms of early intervention agencies contracted with SDRC and the expanding reach of the intervention to a growing volume of families each year indicate the sustainability of the approach. Overall, these illustrate success in the efforts of the BRIDGE Collaborative to ensure access to EBI for families of young children with autism.
Footnotes
Acknowledgements
The authors thank the BRIDGE Collaborative for their tireless and rigorous work toward a better understanding of community-based research, and the community providers who participated in this project. The authors also thank Kassondra Soto and Delia Camacho at the San Diego Regional Center for their support with data collection.
Author Note
Jordan Ko is now affiliated to San Diego State University, USA.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a US Department of Education Grant: R324A140004 and an Autism Speaks Grant: 8136.