
Abstract
Parent training (i.e. group-based supports and psychoeducation aimed at parent as primary agent of change) in Autism Spectrum Disorders (autism) is well-documented as an Evidence-Based Intervention designed to increase advocacy, knowledge, and empowerment. While research on Parent Training acknowledges the cultural limitations, the field lacks culturally grounded models. Furthermore, barriers in diagnosis, service acquisition, and inclusion of under-represented populations including Black families have been established; however, research programs have traditionally failed to include these families. This study aims to provide a first toward addressing the lack of inclusion. We describe the practice-based implementation of a culturally concordant Parent Training program (Spectrum of Care) developed by a community organization (the Color of Autism) as well as feedback from parents after the implementation process. The findings indicate that culturally grounded strategies could promote engagement and empowerment of Black families. There, however, is still a need for research that attends to parental mistrust and examines culturally grounded strategies more closely.
Lay abstract
Parent training programs have been well-studied in Autism Spectrum Disorders and shown to increase a parent’s feeling of empowerment, advocacy skills, and treatment enrollment for their child. The majority of parent training interventions have been developed without considering the unique needs of under-represented communities, such as the Black community. Black children with autism are not only misdiagnosed or not diagnosed at all, but are not accessing services equally compared to their White peers. There is an urgent need for culturally adapted interventions in order to decrease the disparity gap. The Color of Autism Foundation developed and ran a parent training program for Black parents of children with autism. The program was grounded in two key features: (1) creating a circle of support for parents to connect and heal from ongoing and historical racial trauma and (2) using parents of Black children with autism as the main facilitators. We believe this increased parent’s ability to engage in the educational aspects of the training. Overall, parents reported high levels of satisfaction with the training were highly engaged (attended an average of five of six sessions) and reported high levels of empowerment. Parents also reported continued mistrust in the medical and research community and a need for more Black providers. Further work should examine the relationship of the parent and provider in autism treatment and study the impact of circles of healing for Black families.
Keywords
For over two decades, we have described the ever widening racial, ethnic, and geographic disparities in Autism Spectrum Disorders (autism) (Wallis, 2021). Yet, to date, sociodemographic factors have only partially accounted for increasing inequities and a few systemic solutions have been implemented that significantly narrow the disparity gap. History has taught us that meaningful systemic change is multifaceted and occurs slowly over time; perhaps too slowly to yield any meaningful difference to significantly impact those in the system in need of services now. It is well-established that Black 1 and minoritized families with autism are not as quickly enrolled in services in the first years of life following a diagnosis (Mandell et al., 2002, 2007). Nor are they being diagnosed, referred, or screened as early as their White peers, resulting in delayed onset of treatment (Zuckerman et al., 2017). However, more recent data on prevalence estimates suggest that Black children are being diagnosed closer to 4-year-old in more recent years, which is similar to their White peers (Patrick et al., 2020). While such delays certainly play a role, it also is reported that families report hesitation and distrust in treatment for autism and providers (Burkett et al., 2015; Locke et al., 2020; Magaña et al., 2015). Furthermore, minority families are consistently under-represented in evidence-based treatments and services in autism (Broder-Fingert et al., 2020; Imm et al., 2019; Koh et al., 2011; Liptak et al., 2008; Mandell et al., 2002). Novel and expedient solutions are required to increase the support available to all families impacted by autism, which will require culturally competent researchers to partner with and gain the trust of communities (Maye et al., 2021). We describe a novel practice-based evidence approach to the development of autism interventions by the Black community and for the Black community.
Practice-based research
The use of evidence-based practices, or “practices and programs shown by high-quality research to have meaningful effects on outcomes” (Cook & Odom, 2013, p. 136) has become the standard of care for autistic youth and their families (Steinbrenner et al., 2020; Wong & Singhal, 2014). However, there are many challenges and limitations of evidence-based practices especially for historically marginalized and minoritized populations. Many evidence-based practices that have been proven efficacious in traditional research settings have inadequate or no inclusion of racial, ethnic, or cultural variables of autistic youth (Jones & Mandell, 2020) and do not examine the impact of culture, local context, or environment on outcomes (Isaacs et al., 2005). The concept of practice-based evidence, intervention approaches, and supports that are derived from, supportive of, and embedded in the local cultural context and traditions may be more appropriate for historically marginalized and minoritized populations (Isaacs et al., 2005). Although these practices do not have as strong a research base in the traditional sense, there is much to learn from them, and documenting culturally grounded intervention approaches may be how we build a stronger evidence base.
Practice-based research has been previously used in healthcare as a method for expediting novel therapeutic approaches (Pirotta & Temple-Smith, 2017) and more recently in adult autism research methods as a way for increasing inclusion in research participation and designs (Nicolaidis et al., 2019). One potential pathway to address service gaps in healthcare is to develop programs in partnership with families and communities rather than solely relying on researcher-driven methods of intervention development and testing. This approach is critical to ensure that programs and services meet the needs of families. This means that practice-based interventions may require a shift from traditional university- or clinic-developed research interventions to treatments that can feasibly and meaningfully be implemented in everyday practice (Weisz, 2004; Weisz et al., 2004). Culturally grounded interventions that are developed for and by Black communities and other communities of color may ultimately have a better chance of being used and sustained than those developed in university-based research settings, which are primarily grounded in Eurocentric and middle-class standards (Boyd et al., 2018). Interventions that emerge from practice may have an advantage compared to university-developed interventions, in that much of the work of fitting the treatment to the setting has already been done, so the intervention is more appropriate and relevant to the community (Weisz, 2004; Weisz et al., 2004). Practice-based research increases the likelihood that resulting interventions will be more culturally relevant, tailored, and actionable than if they were developed in a laboratory or university-based setting without attention to community (Green, 2008; Green et al., 2009).
Specifically, Parent Training (PT) (i.e. group-based supports and psychoeducation aimed at parent as primary agent of change) (Bearss et al., 2015) in autism is well-documented as an Evidence-Based Intervention (EBI) designed to increase advocacy, knowledge, and empowerment (Brookman-Frazee & Koegel, 2004; Zwaigenbaum et al., 2015). Parent training interventions in autism have proven to be highly effective in terms of improving child outcomes (Deb et al., 2020; Nicolaidis et al., 2019). Traditional parent training programs focus on child symptom severity and skill outcomes in young children or children with behavior challenges (Weisz, 2004). While much of the prior research has focused on child outcomes in younger children, parent training studies have explored parental outcomes such as stress and community engagement (Weisz et al., 2004) or more recently resilience (Schwartzman et al., 2021); however, these studies have failed to include culturally diverse populations. A single PT program, FACES, which was implemented in the Black community, has pointed toward the feasibility of implementing PT in the Black community successfully while demonstrating improvements in parental empowerment and advocacy (Pearson & Meadan, 2021; Pearson et al., 2020). However, no PT program to date has directly addressed the challenges in healthcare engagement specific to the Black community including acknowledging ongoing and historical trauma and engagement in medical research. Thus, community organizations such as The Color of Autism (CoA) have led the way in developing such culturally grounded interventions for the Black community.
Meeting the needs of Black families
Black families live under the constant weight of systemic racism and inequities from inequitable access to services and opportunities to low quality and ineffective services (Iruka et al., 2021; Shonkoff et al., 2021; Structural Racism is a Public Health Crisis: Impact on the Black Community, 2020). This is pervasive across every sector of society from health, education, to economic opportunities. Of particular note is the race-based trauma that Black people experience that remains invisible, unaddressed, and unacknowledged in clinical research (French et al., 2020; Williams & Cooper, 2020). This is important because the Black community needs to utilize safe spaces to speak their truth and through peer support be guided on how to build a system of care using from their own lens with the support of those with similar lived experiences including historical trauma, poverty, and other presenting challenges that historically have either prohibited or inhibited their ability to walk in their truth. This approach is consistent with the psychological framework of radical healing by French and colleagues (2020) that is defined as,
being able to sit in a dialectic and exist in both spaces of resisting oppression and moving toward freedom [that] includes both acknowledgment of and active resistance from oppression, as well as a vision of possibilities for freedom and wellness. Moreover, the act of being in that dialectic is, in and of itself, a process of healing (p. 24).
This process includes critical consciousness, cultural authenticity and self-knowledge, hope, emotional and social support, and strength and resilience. A critical and missing component of EBI in autism for the Black community is acknowledging this history and process.
The CoA believed that in order to create a safe space, Black parents of children with autism would be the most appropriate facilitators of the program. Research has shown that the provider–patient relationship is a critical component in healthcare engagement and culturally concordant relationships are more likely to result in patient-centered care. Spectrum of Care (SoC) parent training programs are culturally concordant as the facilitators are themselves, Black parents of children with autism. With provider characteristics, Cooper and her colleagues found that when physicians and patients were of the same race (i.e. there was racial concordance), patients were more satisfied with services (Cooper-Patrick et al., 1999; Stevens et al., 2003; Street et al., 2008). Through a line of research on minority health disparities, she has found that Black patients’ perceptions of racism or discrimination from their physicians as well as the physicians’ implicit attitudes on race and class can lead to less patient-centered care. This is important because better patient-centered care has been linked to improved patient perceptions of their providers (Saha et al., 2003; Stevens et al., 2003; Street et al., 2008) and health outcomes for minorities. For example, Latinos with Spanish as their primary language receive less family-centered care for autism (Liptak et al., 2008; Magana et al., 2012) and are less likely to receive care consistent with families’ values (Magaña et al., 2015). In autism, we know so little about how issues of parent–provider cultural concordance (e.g. racial and ethnic match) affect family or child outcomes, or the ways in which this cultural concordance (or discordance) facilitate or inhibit the ability of families to access appropriate services for their children. Yet, such information could be critical for the development of culturally tailored interventions, and play a pivotal role in improving Black families’ access to services and children’s outcomes. The purpose of this article is to describe the practice-based implementation of a culturally concordant PT program (SoC) developed by a community organization (the CoA) as well as feedback from parents after the implementation process.
Methods
The CoA: program description
Founded in 2009, The Color of Autism Foundation (CoA) is a non-profit (501 c3) organization committed to educating and assisting Black families affected by Autism Spectrum Disorders. The goal of CoA is to help all families identify the warning signs of autism early on by providing culturally competent support and training, which will lead to better outcomes for children in underserved communities on the autism spectrum. They believe an informed parent is an empowered parent. The goal for parents is to exit their training with the confidence and ability to lead at home, become a more effective advocate for their children, and be empowered to support their community.
SoC program: intervention description
CoA developed SoC specifically for parents of children with autism in communities of color. The CoA developed and implemented a PT program, SoC, that not only directly addressed the historical trauma of the Black community but also created a safe environment for parents of children with autism to heal. Similar to other evidence-based PT programs, SoC ultimately aims to increase empowerment, parental knowledge, and service utilization. CoA’s foundation for SoC is based on the tenets of the Peer Support Movement which has informed family and youth driven care. Using the Family-Driven Care Principles (FPA Code of Ethics—Appendix B Family-Driven Care Principles). CoA began creating this program at the intersection of both these principles and the Black lived experience and culture.
In order to meet these aims, the CoA team focused on acknowledging the trauma that many Black people and their ancestors have experienced and continue to experience through the medical and research community, creating a healing circle (Pearpoint et al., 2015) that allow participants to share their pain, trauma, and challenges with engaging with the medical and research community, and providing knowledge and insights on how parents can advocate for themselves and their children to access the highest quality care. CoA therefore focused on ensuring that SoC incorporated a safe space and culturally congruent/competent environment so as to foster healing and affirm experiences, which is a critical step in the process of helping parents to better engage in autism services.
Parents attended six weekly sessions as part of a 14-h program facilitated in person (Years 1 and 2) and online (Year 3) due to the pandemic. The program was implemented in parent groups and each cohort included a maximum of 20 parents (range = 15–20; M = 18). In-person trainings were held at a local community center. Each session was 1–2 h in duration and focused on psychoeducation and efficacy skill building. Parents met with a Peer Support Specialist and co-facilitator individually no less than three times over the course of the program (prior to attending, week 3, and upon completion). The program was run by culturally concordant facilitators who were Certified Family Peer Support Specialists and parents of Black children with autism. Peer Support entails training for individuals with lived experience within a variety of systems that encompass disability, child welfare, substance use, or mental illness. Family Peer Support training requires completion of a Parent Empowerment Program (PEP) or other Peer Support Training that introduces individuals to their role and to the skills they will need to effectively engage and empower parents. A sample outline of a session is provided in Figure 1.

Sample outline of parent training session.
SoC is grounded in two key features as follows: (1) The circle of support/team building and (2) parent–provider cultural concordance.
Circle of support and team building
Both lie at the intersection of the Principles of the Family Peer Code of Ethics. Circle of support was adapted from Circle of Friends (Pearpoint et al., 2015) by CoA specifically for Black parents of children with autism in order to help parents build community and supports around themselves as they are finding their own identity as a parent of a child with autism. A key component to engagement is the team building exercises utilized during each session. Specifically, circle of support helps parents/caretakers develop their own system of care for themselves and their children using both natural (family, friends, partners, neighbors) Spiritual/Self Care as well as community based and professional supports, activities, and tools to use when there are social/emotional, educational, spiritual, medical, or behavioral challenges. Each circle is person/family centered and strength based. In SoC, the circle of support is created after the assessment of needs session and the advocacy training module (see Figure 1). At this point, parents/caretakers know where their efficacy, knowledge, and advocacy goals intersect with what they have determined are the support needs for themselves and their children. The circle of support helps to create a visual understanding that they are not alone in this journey (see Figure 2).
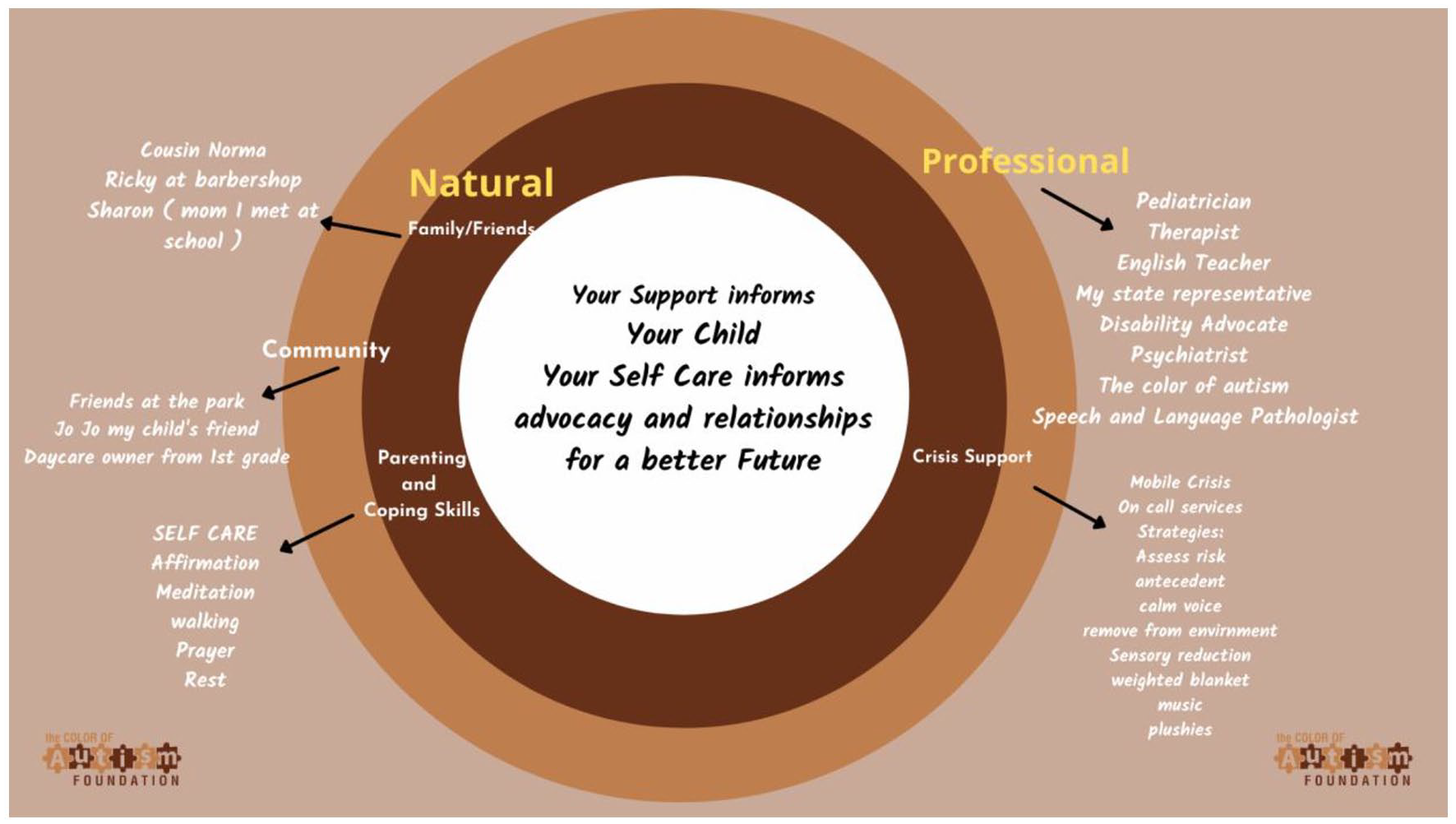
Circle of support path map.
Parent–provider cultural concordance
The program was implemented and developed by Black parents of children with autism. Culturally, the facilitators had similar life experiences as the parents attending the group. Furthermore, the majority of the speakers brought in for the psychoeducational components were from the Black community. This ensured that parents were receiving information from sources with similar lived experiences who understand the shared collective history of Black families. SoC also includes a psychoeducational component in each session. The psychoeducational component presented by an expert in the field who was also from the Black community. Topics are presented in lifespan relevant order, for example, early intervention, applied behavior analysis (ABA) therapies in the beginning and transition, and mental health issues in the last 2 weeks (see Figure 3).

Spectrum of care session list.
Study design
This study used a practice-based research approach wherein an intervention developed in and implemented in the Black autism community is described. Retrospective data from parent surveys and interviews to collect feedback on their experiences were used.
Participants
The study included 147 parents over the course of a 3-year period who participated and completed SoC. The CoA is connected with numerous local and national community organizations that serve families of color. Through the relationships CoA developed with these organizations, they used electronic messaging, social media, and personal recommendations to share the program information and invite families to sign up. Once a family completed an interest form on the website, a facilitator called the parent and reviewed their information to determine whether they met eligibility criteria. Once a family was enrolled, they were asked to complete a basic demographic form either via interview or paper. While additional demographic data were requested from parents, few chose to share (see section “Results”). In order to build trust with the families and prioritize engagement, further requests for demographic data were not made at this time.
Eligibility criteria
Parent inclusion in SoC was based on the biological or non-biological parent(s) or legal guardian being Black, and the family having one Black or biracial child, who met diagnostic criteria for autism. We did not exclude non-traditional families, such as those headed by grandparents, because we do not have enough information about how family constellations affect service access for children with autism. Having older or younger children with other types of disabilities is not an exclusion criterion. A member of the household was required to speak English to participate in interviews and complete the program, although we did work with families who needed interpreters (n = 2). Peer support was utilized for interpretation as parents who previously completed the program volunteered to be available for interpretation. Families who are Black and Latino were included because we wanted to offer the program to all families who are interested and meet basic criteria listed above.
Measures and procedures
Parent survey
Parents were administered the SoC follow-up survey 30 days after completion of the program. The survey (see Table 1) assessed parent satisfaction with the program, empowerment, and advocacy and was developed by CoA. The survey was administered by an SoC facilitator electronically; if it was not completed by the parent, a facilitator would call and talk through the questions with the parent over the phone.
Outcome survey results.

Parent interviews
Upon completion of the program, facilitators would contact each parent attendee to inform them of the survey and complete a set of interview questions. Interview questions are open-ended and broad and meant to be an informal “check-in” with the family. Questions were asked around general themes of empowerment, advocacy, healthcare/services engagement, and interests in autism research (e.g. “What are your current feelings around autism research or engaging with autism services for your child?”). Parents were asked five specific questions about each area by a facilitator using a semi-structured protocol, which were then followed up on for further information.
Community involvement
The Black Autism Community was directly involved in all aspects of this article. The CoA is founded by and serves Black families with autism. Ms Kaiser and Ms Proctor worked directly with the community to develop the intervention program and design this article. The community was directly involved in the developing the research question, study design, measures, implementation, or interpretation and dissemination of the findings. For the purposes of gaining trust with the community, the CoA decided in advance they would not require socioeconomic information from parents. The goal of the program was to create a safe for Black families and in order to do so, only basic information was required to attend the trainings. The program is now in its fourth year and has begun collecting this information as trust has been established with the community.
Analyses
Survey results were analyzed using descriptive statistics from Likert-type scale ratings. Parent interviews responses were grouped based on interview questions of empowerment, advocacy, healthcare/services engagement, and interests in autism research. Parent interview responses were recorded by hand by the facilitators conducting the interviews. While audio recordings would have been preferred, CoA made the decision to earn family and community trust first. As community trust and engagement was the goal of this study, we did not utilize in depth qualitative analysis. Data analyses were performed by the first authors.
Results
Findings from surveys and interviews all indicated that SoC was positively received, parents felt empowered and with a sense of support and advocacy. Overall parents attended an average of five out of six sessions. Approximately, six parents per year missed a session with their original cohort but returned to complete the training later in the year.
Parent survey
Survey data (Table 1) were available for 94% (n = 138) of parents who completed the program (Year 1 = 28; Year 2 = 43; Year 3 = 76). Of the 147, 97% of parents identified themselves as Black, three parents also identified as Hispanic and Other. Two males and 145 females attended the trainings. Approximately 84% of families lived in urban areas and 26% rural or suburban. We found that all participants completing the survey reported they were confident they could replicate the skills learned at home and 88% were implementing efficacy building skills. Over 92% rated the training as “exemplary” indicating that the training was acceptable to the target population.
Interview responses
Parent interviews were conducted with each parent over the 3 years. Facilitators collected interview responses from each parent. Responses were chosen from each year to represent the entire sample.
Empowerment
Parents were asked in the follow-up interview and in the survey about how empowered they felt following the program. The majority of parents (76%) reported feeling “extremely empowered” and 22% reported feeling “somewhat empowered.” When parents were asked if the training allowed them to feel more empowered to care for their child with autism, parents reported not only that they felt more confident but also they were able to support their child better. For example, one mother stated: “I feel like I found my power. I am more confident now with my skills to help my daughter.” Another mother commented on how the training empowered her to understand her child better: “Autism for me was a White American male disease that meant you were smart and quirky. After this training I know my child was not only misdiagnosed, my child was underestimated in his abilities. Thank you.”
Advocacy
Parents were asked how comfortable and confident they felt in their ability to advocate for their child following the training. The majority of parents felt as though they were better able to advocate for their children (88%). These parents also reported that the team building and circle of support exercises allowed them to heal and want to share their experiences with others in their community:
This training just made it real for me because I could cry and share things that we as people of color share, I never knew I could have this and now I want to help other parents in my neighborhood. You helped calm my fear, use my voice and advocate for my child. I was alone in spaces where no one understood the fear . . . Now I am not afraid and I have a plan, resources and confidence. Thank you.
Engagement in research
Parents expressed concerns about participating in research broadly, sharing private demographic information and around engaging with autism organizations following the training. While parents were comfortable providing anonymous responses about their experiences during SoC and providing feedback on satisfaction of services, most parents did not feel comfortable sharing personal information for the purposes of research including demographics, which CoA chose not to require for this portion of the study. The following quotes describe the overlying apprehension many Black families feel about research and trust in the medical field broadly:
No one understands why we can’t trust, its real, its history and time after time they wonder why we won’t just give them information or answer questions we don’t relate to, but some Black folks want that iPad or gift card. So, they just mail in answers; there’s no truth. Because we know it’s all Tuskegee all the time. It’s a game to check the box after you already decided your course of action. My grandmother died from high blood pressure right before we realized the research was wrong on treating blood pressure in Black folks. The default person is the White male. We are different, we live different, we process different. No one cares, so we keep dying—I won’t be part of a study that uses me not to improve my community but to objectify my community. They used Henrietta Lacks cells without permission because we are not valued. They ripped uteruses out of slaves to advance gyn research and tortured young Black girls to advance their cause . . . and then they continued doing just that with all the hysterectomies done for tiny little fibroids. That is what research does to us. Where are the Black doctors and research folks who really know us? There has to be someone who can help us get what we really need to make a change in how we treat Black children with autism and how we educate ourselves and do what CoA has taught us over the last 6 weeks.
Requests for additional supports
Parents were asked what supports they felt like they needed following the training and if they would be interested in peer supports moving forward. Some of the requests included continued peer support, advocacy assistance, links to Black clinicians, attorneys and education consultants, more parent support groups, and transitional guidance. Many parents reported a desire for additional peer or community supports following the training. Some parents requested specific trainings such as how to navigate police experiences. One parented commented specifically on peer supports. Feedback from parents suggested that utilizing culturally concordant facilitators helped to provide a safe space for parents to learn and develop skills to support their children:
It is so important for us to have this space you provide. We are different in our experiences but we share something deeper as Black people and I am proud to learn and share and grow so I can support my child to be who he wants to be. Handsdown! having another Black parent to vent to and who is trained to redirect me, talk me off the ledge and center my continued fight. Black people are always encountering microaggressions and we do not talk about it but with a Black Peer you can! My son’s therapist looks at me like I have 3 heads when I vent and turns it back on me! Gives excuses! It happens too often!
Discussion
This study is one of the first to describe a PT program specifically developed for and by Black families in autism. We found that culturally grounded strategies such as the circle of support and culturally concordant facilitators may be effective in ensuring the training was successful for Black parents. While this approach was successful at engaging parents in the long-term and they felt the training to be empowering, more rigorous study will be required to measure parental engagement and empowerment in the future. As SoC was implemented by culturally concordant facilitators (i.e. Black parents of children with autism), we believe this was a potential key ingredient to parental engagement. Furthermore, circle of support team building components may have provided a safe space for parents to address the ongoing and historical racial medical trauma. It will be critical to better examine the role of parent–provider concordance and culturally adapted components such as circle of support in autism interventions moving forward in order to better engage and build trust with the Black autism community, and determine if such program results improved parent and child outcomes. In light of the continual trauma of the Black communities, it is important to also examine the length of time. There may be a need to continue providing support to address the mistrust of the medical community, including autism organizations that have not fully addressed the historical racial medical trauma experienced and still being experienced by Black communities including parents with children with autism.
Implementation facilitators
Cultural concordance
Implementation of SoC suggests that cultural concordance may play a role in facilitating treatment engagement. Several studies have shown that racial and cultural concordance is positively associated with aspects of care for adults, such as participatory decision-making, interpersonal respect, and satisfaction (Cooper-Patrick et al., 1999; Ferguson & Candib, 2002; Saha et al., 2003). The physician–patient relationship is strengthened when patients see themselves as similar to their physicians in personal beliefs, values, and communication. Perceived personal similarity is associated with higher ratings of trust, satisfaction, and intention to adhere. Race concordance is the primary predictor of perceived ethnic similarity, but several factors affect perceived personal similarity, including physicians’ use of patient-centered communication (Street et al., 2008). While previous PT studies targeted similar outcomes at SoC, including empowerment, advocacy, and service utilization, SoC focused on creating a circle of support and environment for Black parents to begin engaging. It may be that without this critical step in interventions, we will continue to see a widening disparity gap in service utilization for Black families.
Circle of support and team building
In order to directly address the ongoing and historical trauma the Black community experiences, the SoC shows the importance of creating communities of support that not only have direct experiences due to autism but also have lived experiences that attend to the compounded impact of structural racism and other racialized experiences (Iruka et al., 2021; Shonkoff et al., 2021; Structural Racism is a Public Health Crisis: Impact on the Black Community, 2020). Emerging research is showing the importance of not only having high-quality care but also care from individuals who share similar experiences (French et al., 2020) or at the minimum, understand how biases may impact their provision of quality care (Jones et al., 2021). This study also highlights the importance of community building and peer support to support parents’ understanding about how to support their child with autism.
Implementation challenges
Engagement in autism services
Our experiences also suggest that Black parents experience mistrust around research and data collection in autism. While SoC was built by community providers, parents still report hesitancy around such issues. A few studies have focused on collaboration with the Black communities to decrease service gaps. This is despite recent guidance advocating for patient-centered engagement at the onset of research (Gowen et al., 2019):
The recommendations promote effective communication and equal partnerships between the autism and research communities, so that the needs of participants pre-research, during and post-research are taken into account, and so that participants are supported to become involved in research at the level they choose.
Despite substantial documentation that the needs of the Black community are unique and still not well-understood (Scharff et al., 2010), to date research has not prioritized an engagement first approach. We propose prioritizing building trust, collaborating directly with the Black communities and identifying stakeholder-specific research priorities as we work toward eliminating disparity gaps.
Continued supports
Many parents expressed the desire to continue engagement with their peers and support families in their community following the training. Parents also expressed the desire for resources in the Black community, such as Black autism providers and clinicians. This speaks to a well-documented need for autism services and providers in the Black community. Minority populations are consistently under-represented in the development of interventions and the majority of service providers are racially discordant from their patients. While such challenges will take time to address in the field at large, it remains critical for us to increase efforts toward recruiting Black clinicians, scientists, and autistic adults in the field (Jones & Mandell, 2020). Furthermore, in order to begin narrowing the service delivery gaps for Black and minority families with autism, cross-cultural EBIs must be developed and implemented in collaboration with the community. By exploring culturally grounded models of care in the Black community, we can then apply these findings to other minoritized populations (e.g. Hispanic and Native American) and move away from a “one-size fits all” treatment model of autism and effectively tailor services to meet each family’s unique culture subsequently improving child outcomes in the long-term.
Limitations and future directions
While the CoA and the SoC program provide emerging evidence about the importance of culturally relevant adaptations that are meaningful and relevant for Black families of autistic children, we have only described the first stages of this practice-based research model. Furthermore, as we have described this intervention in retrospect, we are limited by the data families were comfortable sharing and lack of rigorous testing at this time. Practice-based methodology has largely been overlooked in autism; however, practice-based designs may present a solution for the immediate need for culturally relevant services. They have the potential to provide us with an overview of a “real world” practice outside of the controlled clinical research setting. Utilizing this methodology for SoC has allowed for us to uncover potential key ingredients in interventions for the Black community; however, interview and survey data are challenging to acquire consistently, and in this study, demographic information was particularly challenging to collect.
Next steps should focus on including strategies for increasing trust and engagement with the Black autism community. Future studies should explore the circle of support exercises and patient–provider cultural concordance to better understand their unique impact on Black parent training program outcomes such as empowerment, advocacy, and service utilization over time. Measuring implementation outcomes related to SoC among Black communities including adoption and fidelity over time will also be critical.
While detection or the existence of disparities has been well-documented, the next stage of research must address the lack of culturally grounded EBIs in autism. Furthermore, EBIs such as parent training have demonstrated high levels of efficacy in the autism population at large but not yet incorporated diverse samples required to understand their efficacy in sub-populations. In order to begin narrowing the service delivery gaps for minority families with autism, cross-cultural EBIs must be tested and implemented in collaboration with the community. By exploring culturally grounded models of care in sub-populations, such as the Black community we can potentially use these processes to support culturally grounded approaches with other ethnic minority communities (e.g. Hispanic and Native American), ensuring that services are effective and meet the wholistic and unique needs of families and their children. It behooves us as researchers and clinicians to follow their lead and expertise while we develop interventions.
Footnotes
Acknowledgements
The authors thank the Color of Autism Foundation for their tireless efforts to support the Black community. The authors also thank all the families who shared their experiences and truth for this paper. The Color of Autism would like to thank Jillian Nathan, Ari Cole, and Brian A. Kaiser for your inspiration, guidance, and hard work in supporting the Foundation’s journey to support and empower Black communities impacted by ASD.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K.K. and C.P. are the founders of the Color of Autism, and do not receive any funding from the Spectrum of Care program. Drs M.E.V., J.L., I.U.I., and B.B. declare that they have no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.