
Abstract
Gastrointestinal disturbances (GIDs) are relatively common in children diagnosed with autism spectrum disorder (ASD). This study assessed associations between maternal obesity, diabetes, preeclampsia, and asthma and likelihood of ASD with GIDs. This retrospective cohort study included 308,536 mother–child pairs of singletons born between 2001 and 2014 in a single integrated health care system. Social demographics, maternal health conditions during pregnancy, and child’s ASD and/or GID diagnosis by age 5 were extracted from electronic medical records. Child’s outcome was classified as: no ASD no GIDs; no ASD with GIDs; ASD no GIDs; and ASD with GIDs. Multinomial logistic regression was used to estimate odds ratios of child’s outcomes associated with maternal exposures, adjusting for covariates. Compared to children with neither disorder, each maternal condition was associated with higher odds of no ASD with GIDs, ASD no GIDs, and ASD with GIDs. Association was greatest for likelihood of ASD with GIDs (Maternal obesity odds ratio (95% confidence interval): 1.37 (1.22–1.54); Diabetes: 1.50 (1.28–1.76); Preeclampsia: 1.63 (1.36–1.95); Asthma: 1.39 (1.17–1.67); relative to no ASD no GIDs). Associations were robust to mutual adjustment for all maternal exposures. Maternal obesity, diabetes, preeclampsia, and asthma exposure during pregnancy may increase likelihood of both GIDs and ASD with or without co-occurring GIDs in offspring. This association was greatest in children diagnosed with ASD with co-occurring GIDs.
Lay abstract
Autism spectrum disorder is heterogeneous and often accompanied by co-occurring conditions. Previous studies have shown that maternal health conditions during pregnancy including obesity, diabetes, preeclampsia, and asthma were associated with increased likelihood of autism. However, little has been done examining the likelihood associated with autism with co-occurring conditions. This study assessed these maternal health conditions in relationship to autism and gastrointestinal disturbances, a common co-occurring condition in children diagnosed with autism. Data included 308,536 mother-child pairs from one integrated health care system with comprehensive electronic medical records. Among the study cohort, 5,131 (1.7%) children had a diagnosis of autism by age 5. Gastrointestinal disturbances were present in 35.4% of children diagnosed with autism and 25.1% of children without autism diagnoses. Our results showed that each of the four maternal health conditions during pregnancy was associated with increased likelihood of gastrointestinal disturbances, autism without gastrointestinal disturbances, and autism with gastrointestinal disturbances. For all four maternal health conditions, the association was greatest for likelihood of autism with gastrointestinal disturbances. Given that children diagnosed with autism are more likely to have gastrointestinal disturbances and over 80% of gastrointestinal disturbances in this cohort were diagnosed prior to autism diagnosis, this study suggests that there may be common biological pathways between autism and gastrointestinal disturbances impacted by these maternal exposures. Future studies are warranted to assess associations between different exposures and autism with other co-occurring conditions to increase our understanding of autism heterogeneity.
Keywords
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by impaired social communication, repetitive behaviors and restricted interests, and disturbances in sensory processing (Maenner et al., 2020). ASD has multifactorial etiology (Geschwind, 2011; Hallmayer et al., 2011; Wang et al., 2017) and heterogeneous presentation (Masi et al., 2017), with symptoms and severity varying widely between individuals. Diagnoses are frequently accompanied by co-occurring medical conditions, including gastrointestinal disturbances (GIDs) (Aldinger et al., 2015; Leader et al., 2022). These are broadly characterized by chronic gastroesophageal reflux (GERD) and bouts of diarrhea or constipation with encopresis (Ristori et al., 2019), affecting approximately 40% of children diagnosed with ASD (Aldinger et al., 2015; Chaidez et al., 2014; Gorrindo et al., 2012; Restrepo et al., 2020). Children diagnosed with ASD and co-occurring GIDs exhibit increased rigid-compulsive behaviors (Marler et al., 2017), higher levels of oxidative stress (Gorrindo et al., 2013; Osredkar et al., 2019), and neuroimmune and microbiome disruptions (Luna et al., 2017). As the gastrointestinal tract is an immune and stress-sensitive organ (Takiishi et al., 2017), ASD and GIDs may be linked by complex common etiology and symbiotic presentation.
Exposures during pregnancy may play an important role in the development of both ASD and GIDs. Maternal obesity (Li et al., 2016), diabetes mellitus (Xiang et al., 2015), preeclampsia (Maher et al., 2020), and asthma (Bilbo et al., 2018) have been associated with childhood ASD diagnosis. These pregnancy health conditions can impact fetal brain development by exposing the fetus to higher levels of pro-inflammatory cytokines and greater oxidative stress (Smith et al., 2007). The disruption of cytokine and chemokine expression modulates microglial function, which can impact neurodevelopment (Bilbo et al., 2018). These four maternal health conditions have also been associated with offspring GIDs and changes to the gut microbiome in children (Chong et al., 2018; Dreisbach et al., 2020; Leybovitz-Haleluya et al., 2019; Ponzo et al., 2019; Ristori et al., 2019; Vandenplas et al., 2020). Together, studies suggest that maternal conditions during pregnancy may impact biological mechanisms essential for brain and gut development in offspring.
Few epidemiological studies have examined indicators of ASD with co-occurring conditions. Although maternal obesity, diabetes, preeclampsia, and asthma are associated with both ASD and GIDs, there has been no previous population study examining their associations with the ASD phenotype with co-occurring GIDs. We hypothesize that maternal obesity, diabetes, preeclampsia, and asthma will increase the likelihood of children developing ASD and co-occurring GI conditions. We tested this hypothesis by assessing the associations of these four common conditions during pregnancy (Alexopoulos et al., 2019; Catalano & Shankar, 2017; Perez-Crespo et al., 2019; Shebl & Chakraborty, 2021) with ASD, GIDs, and ASD with GIDs. In addition, previous studies have reported increased likelihood of co-occurring conditions in girls with ASD diagnoses, compared to boys with ASD diagnoses (Angell et al., 2021; Rodgaard et al., 2021; Supekar et al., 2017). As a secondary objective, we explored potential sex differences in the associations.
Materials and methods
Study population
This population-based retrospective birth cohort study included 308,536 mother–child pairs of singletons born at Kaiser Permanente Southern California (KPSC) hospitals between 1 January 2001 and 31 December 2014 (Supplemental eFigure 1). Children were followed through KPSC comprehensive electronic medical records (EMR) from birth until age 5. The KPSC healthcare system serves a diverse population of 4.5 million members throughout Southern California, with member social and demographic data reflecting regional census tracts (Koebnick et al., 2012). Maternal social and demographic information and pregnancy health data as well as child’s ASD and/or GIDs diagnoses were extracted from KPSC’s integrated EMR system.
Outcomes: ASD and/or GIDs
Outcomes were whether a child had a diagnosis of ASD and/or GIDs by age 5. KPSC moved from International Classification of Diseases, 9th Revision (ICD-9) codes to International Classification of Diseases, 10th Revision (ICD-10) on 1 October 2015. For EMR entries dated before 1 October 2015, ASD diagnoses were identified by ICD-9 codes 299.0, 299.1, 299.8, and 299.9. After that date, ASD diagnoses were identified by ICD-10 codes F84.0, F84.3, F84.5, F84.8, and F84.9. Codes included autistic disorders, Asperger’s syndrome, and pervasive developmental disorder not otherwise specified (PDD-NOS). Codes did not include Rett’s syndrome or childhood disintegrative disorder. For this analysis, ASD case definition required that relevant codes were recorded in EMR for at least two separate health visits. This approach was previously validated with a positive predictive value of 88% (Coleman et al., 2015; Jo, Eckel, Wang, et al., 2019; Xiang et al., 2015, 2018).
GIDs included a diagnosis of GERD, diarrhea, constipation, ulcers, or disorders of the esophagus (Alexeeff et al., 2017; Leybovitz-Haleluya et al., 2019) and were defined based on an ICD-9 (or ICD-10) code for the condition recorded at two or more health visits. ICD-9 and ICD-10 codes for each of these conditions are listed in Supplemental eTable 1.
Exposures during pregnancy
Exposures of interest were maternal obesity, diabetes mellitus, preeclampsia, or asthma during pregnancy. Maternal obesity was defined as pre-pregnancy body mass index (BMI) ⩾ 30 kg/m2 (Centers for Disease Control and Prevention, 2021). Maternal obesity was associated with likelihood of ASD in previous research as well as in a previous study that included births prior to 2010 from this study population (Li et al., 2016; Xiang et al., 2015). Maternal pre-pregnancy BMI was calculated using maternal height and weight measurements recorded in EMR that were closest to the date of last menstrual period between a window of 6 months before and 3 months after last menstrual period (Xiang et al., 2019). Recording of height and weight at each clinical visit in EMR at KPSC was not implemented until late 2006. Thus, maternal height and weight was missing for mothers of children born from 2001 to 2006. Maternal pre-pregnancy BMI was categorized as obese (BMI ⩾ 30 kg/m2), non-obese (BMI < 30 kg/m2), and unknown (including mothers for whom BMI data was unavailable). Diabetes during pregnancy included pre-existing Type 1 or Type 2 diabetes and gestational diabetes mellitus diagnosed before 26 weeks, as all were reported to be associated with likelihood of ASD in this study sample (Xiang et al., 2015, 2018). Preeclampsia during pregnancy was identified by ICD-9 codes 642.40-642.44, 642.50-642.54, and 642.60-642.64, and included eclampsia and HELLP syndrome (Miller et al., 2020). Preeclampsia was associated with ASD in previous studies that included births prior to 2010 in this population (Xiang et al., 2015). Asthma during pregnancy was identified by ICD-9 code 493 and at least one prescription for an asthma-specific medication (Huang et al., 2021). Maternal asthma was associated with increased likelihood child ASD diagnosis in previous studies (Bilbo et al., 2018).
Covariates
Covariates included to adjust for potential confounding were maternal age, parity, self-reported race/ethnicity and education, census tract-level household income at child’s first birthday, maternal smoking during pregnancy, maternal mental health conditions during pregnancy (any anxiety, depression, or use of selective serotonin reuptake inhibitors), and history of comorbidity (⩾1 diagnosis of heart, lung, kidney, liver disease, or cancer); all were associated with likelihood of childhood ASD in this study population (Jo, Eckel, Chen, et al., 2019; Xiang et al., 2015) and differed by maternal exposures. Birth year was included as a covariate to account for increasing ASD diagnosis trends over the study period (Jo, Eckel, Wang, et al., 2019). KPSC medical centers of birth were also included to control for possible geographic differences in diagnosis. Gestational age was not included as a covariate as it could be on the causal pathway from preeclampsia onset and ASD diagnosis.
Statistical analyses
Outcomes were child’s ASD and/or GIDs diagnosis by age 5 grouped into four categories: (1) no ASD no GIDs; (2) no ASD with GIDs; (3) ASD no GIDs; and (4) ASD with GIDs. Exposure variables were maternal obesity, diabetes, preeclampsia, and asthma during pregnancy. Maternal and child characteristics by the four outcome groups were presented using descriptive statistics where median and interquartile range (IQR) were used for continuous variables and total number (N) and proportion (%) were used for categorical variables. Kruskal–Wallis rank-sum test and Pearson’s chi-square test were used to assess differences in characteristics among the groups.
Multinomial regression models were used to assess associations between maternal exposure variables and child’s ASD/GID outcomes. Results were presented as odds ratios (ORs) and 95% confidence interval (CI) of children having (a) GIDs with no ASD, (b) ASD no GIDs, or (c) ASD with GIDs associated with each maternal exposure, relative to children having no ASD and no GIDs. Data analysis began by assessing exposure variables one at a time in single exposure models. Maternal obesity was examined by including the entire cohort with unknowns treated as a separate category. Sensitivity analysis was performed excluding the birth cohort with missing data on maternal obesity. Results were nearly identical across both obesity models. Since mothers with one condition during pregnancy are more likely to have other conditions, subsequent data analysis was performed for the entire cohort including all four exposures in one model to assess independent associations between exposures, including the unknown category for maternal obesity. We also assessed whether associations with maternal exposures were significantly greater for ASD with GID than ASD without GIDs. This was done by specifying ASD no GIDs as the reference group within the multinomial regression models. All models were adjusted for birth year, maternal age, self-reported race/ethnicity, parity, census tract household income (per $10k) at child’s first birthday, maternal education, history of comorbidity, smoking during pregnancy, mental health diagnoses in pregnancy, KPSC medical center, and child’s sex. Birth year was modeled as a penalized spline to account for non-linear relationship between birth year and outcomes. Sex differences were assessed through testing for interaction between child’s sex and maternal exposures and stratification by child’s sex. Child’s sex was not adjusted in sex-stratified models.
Statistical significance was set at p < 0.05. All statistical analyses were performed in R (version 3.6).
Results
Among 308,536 children included in the study, 5131 (1.7%) were diagnosed with ASD and 77,846 (25.2%) had GIDs. GIDs were present in 35.4% of children diagnosed with ASD and in 25.1% of children without ASD diagnoses. Of the total sample, 1814 (0.6%) of children were diagnosed with ASD with GIDs, 3317 (1.1%) were diagnosed with ASD without GIDs, and 76,032 (24.6%) without ASD diagnoses had GIDs. Among children diagnosed with ASD and GIDs, 79.9% had GIDs diagnosed before ASD diagnosis. Mean age of GID diagnosis was lower for children diagnosed with ASD compared to children without ASD diagnoses (1.1 years vs 1.3 years). Mean age of ASD diagnosis was slightly lower in children with GIDs than in children without GIDs (2.5 years vs 2.6 years).
Table 1 displays participant characteristics by child’s ASD/GID diagnosis. Sex was approximately equally (~50%) distributed among children without ASD. However, boys accounted for 82% of children diagnosed with ASD only, and 80% of children diagnosed with ASD and GIDs. Gestational age at delivery was comparable across the four groups. Greater proportions of children diagnosed with ASD (with or without GIDs) had older mothers and mothers reporting college or higher educational qualifications than children without ASD diagnoses. Children diagnosed with ASD and GIDs had the largest proportions of nulliparous mothers and mothers with mental health conditions and histories of comorbidities. For the four maternal exposures, the highest proportions of maternal obesity, diabetes mellitus, preeclampsia, and asthma diagnoses were observed in children diagnosed with ASD and GIDs. All tests for differences in characteristics among the groups were statistically significant at p < 0.001.
Cohort characteristics by child’s ASD and GIDs status. a

ASD: autism spectrum disorder; GIDs: gastrointestinal disturbances; IQR: interquartile range; BMI: body mass index; API: Asian/Pacific Islander.
All tests for difference in each characteristic among the four groups were statistically significant at p < 0.001.
Maternal comorbidity was defined as ⩾1 diagnosis of heart, lung, kidney, liver disease, or cancer.
Proportions calculated with 118,299 unknown BMI cases excluded.
Table 2 presents covariate-adjusted ORs associated with each of the four maternal exposures, comparing odds of ASD and/or GIDs diagnoses relative to children with no ASD no GIDs. In single exposure models, maternal obesity was associated with increased likelihood of GIDs without ASD (OR = 1.09; 95% CI = 1.06–1.11). However, likelihood was greater for ASD no GID (1.25, 1.13–1.37) and greatest for ASD with GIDs (1.37, 1.22–1.54). After excluding children with maternal obesity unknown, ORs remained similar to models including unknown maternal obesity. The corresponding ORs (95% CI) were 1.08 (1.06–1.11) for no ASD with GIDs; 1.25 (1.13–1.38) for ASD no GIDs; and 1.38 (1.22–1.56) for ASD with GIDs. For maternal diabetes, a similar pattern of increasing OR across outcome categories was observed. The corresponding ORs (95% CI) were 1.15 (1.11–1.19), 1.26 (1.11–1.43), and 1.50 (1.28–1.76) for no ASD with GIDs, ASD no GIDs, and ASD with GIDs, respectively. For maternal preeclampsia, associations were comparable for no ASD with GIDs (1.19, 1.14–1.24) and ASD no GIDs (1.18, 1.00–1.38); however, the OR was much greater for ASD with GIDs (1.63, 1.36–1.95). Finally, for maternal asthma exposure, increasing OR across outcome categories was observed where corresponding ORs (95% CI) were 1.13 (1.09–1.17), 1.15 (0.98–1.34), and 1.39 (1.17–1.67) for no ASD with GIDs, ASD no GIDs, and ASD with GIDs, respectively. It must be noted that the statistical power was smaller in ASD no GIDs than for other groups.
Odds ratios (95% CI) for the associations between maternal exposures and risk of (1) no ASD with GIDs (N = 76,032), (2) ASD no GIDs (N = 3317), and (3) ASD with GIDs in children (N = 1814), relative to children with no ASD no GIDs (N = 227,373). a .

ASD: autism spectrum disorder; GIDs: gastrointestinal disturbances; OR: odds ratio; CI: confidence interval; BMI: body mass index
Adjusted for birth year, maternal age, parity, maternal race/ethnicity, maternal educational qualifications, smoking in pregnancy, history of comorbidity, maternal mental health issue, income (per 10k), and child’s sex.
Not adjusted for the three other maternal pregnancy exposures.
Simultaneously adjusted for the three other maternal pregnancy exposures.
Across the four maternal exposures, among mothers with known maternal obesity status, mothers with pre-pregnancy obesity had greater proportions of diabetes (14% vs 4.6%), preeclampsia (6.1% vs 3.2%), and asthma (10% vs 6.8%) than mothers who were not obese before pregnancy. Rates of preeclampsia (8.9%) and asthma (11%) were highest in mothers with both diabetes and pre-pregnancy obesity and lowest in mothers who were not obese and did not have diabetes (preeclampsia: 3.1%; asthma: 6.7%). Mutually adjusting by putting all four exposures into one model slightly reduced ORs for each ASD and/or GIDs outcome associated with maternal obesity, diabetes, and preeclampsia, but did not change the overall conclusion. These mutual adjustments had little effect on ORs associated with maternal asthma (Table 2).
Table 3 presents ORs comparing likelihood of children diagnosed with ASD and GIDs relative to children diagnosed with ASD without GIDs. The OR was significantly greater for maternal preeclampsia (OR = 1.38; 95% CI = 1.09–1.75). ORs for the other three maternal exposures were also greater although not statistically significant (obesity: 1.10 (0.95–1.28); diabetes: 1.19 (0.98–1.45); asthma: 1.21 (0.96–1.53)) (Table 3). The presence of any four of the maternal conditions was associated with an OR (95% CI) of 1.21 (1.07–1.38) for children diagnosed ASD with GIDs relative to children diagnosed with ASD but no GIDs (Table 3).
Odds ratios (95% CI) for the associations between maternal exposures and risk of children with ASD and GIDs (N = 1814) relative to children with ASD no GIDs (N = 3317). a .

ASD: autism spectrum disorder; GIDs: gastrointestinal disturbances; OR: odds ratio; CI: confidence interval; BMI: body mass index.
Adjusted for birth year, maternal age, parity, maternal race/ethnicity, maternal educational qualifications, smoking in pregnancy, history of comorbidity, maternal mental health issue, income (per 10k), and child’s sex.
Not adjusted for the three other maternal pregnancy conditions exposures.
Any known exposure to maternal obesity, diabetes, preeclampsia, or asthma in utero.
Figure 1 displays sex-stratified results. Patterns of associations were generally similar for both boys and girls, and no significant interactions with sex were observed except for maternal obesity (p = 0.04). Each of the four maternal exposures was significantly associated with the odds for children having ASD with GIDs in both sexes, except for maternal asthma in girls. Note that the small sample size for girls diagnosed with ASD (n = 613 for girls diagnosed with ASD no GIDs; n = 359 for girls diagnosed with ASD and GIDs) possibly limits the ability to detect sex differences.
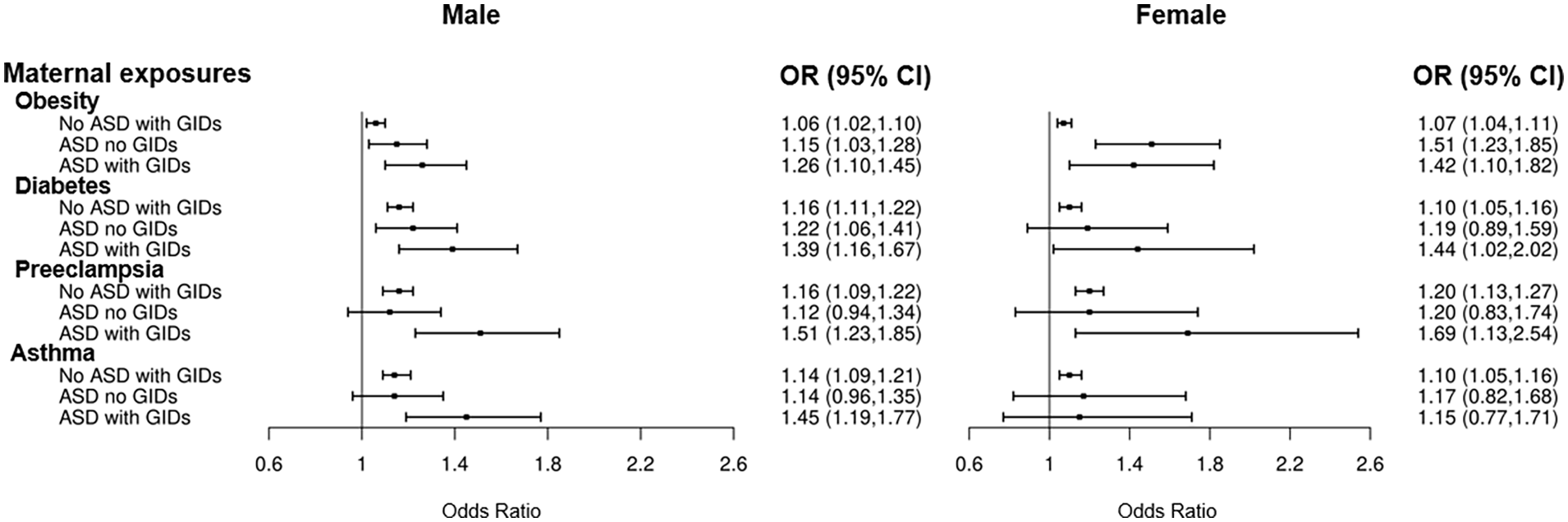
Sex stratified odds ratios for associations between maternal exposures and risk of specific ASD phenotypes.a,b
Discussion
To our knowledge, this is the first study assessing the likelihood of ASD with co-occurring GIDs in children associated with maternal obesity, diabetes, preeclampsia, and asthma during pregnancy. GIDs are common medical conditions, occurring in 35% of children diagnosed with ASD and 25% of children without ASD diagnoses in this study cohort. Obesity, diabetes, preeclampsia, and asthma are common medical conditions during pregnancy, each affecting 26.2%, 6.3%, 4.0%, and 6.8% of mothers, respectively, in this study cohort. Exposure to each of these conditions was associated with increased likelihood for GIDs and ASD with or without GIDs in children. Importantly, associations appeared greatest for ASD with GIDs for all four exposures and significantly greater than ASD without GIDs for preeclampsia. Associations were independent from each other as overall conclusions remained when mutually adjusting for other exposures in the models. When stratified by sex, similar patterns of associations were observed in boys and girls. However, the small sample size of girls diagnosed with ASD limited the ability to detect small differences.
Results from this study suggest that maternal obesity, diabetes, preeclampsia, and asthma during pregnancy each not only increases likelihood of ASD in children, as shown in previous studies (Bilbo et al., 2018; Li et al., 2016; Maher et al., 2020; Xiang et al., 2015), but also increases likelihood of specific medical conditions, leading to even greater likelihood for children diagnosed with ASD and co-occurring GIDs. Each of the four maternal health conditions has been linked to increased maternal immune activation (MIA; Aneman et al., 2020; Donath et al., 2019; Maurizi et al., 2018; Peebles & Aronica, 2019). Thus, our findings are consistent with previously published child neurodevelopment studies reporting the influence of MIA, defined as elevated systemic immune responses during pregnancy (Han et al., 2021). Associations between MIA exposures and ASD with GIDs may be due to the prenatal influence of heightened maternal immune response on fetal brain development directly, or on infant gut microbiota that may contribute to severity of ASD with co-occurring GIDs. MIA during pregnancy exposes the fetus to higher levels of pro-inflammatory cytokines and greater oxidative stress (Smith et al., 2007), which in turn affect neurodevelopment (Bilbo et al., 2018). Studies have shown that cytokine disequilibrium, and the challenge it presents to developing microglia and neurons, is associated with GIDs in children (Ristori et al., 2019). The consistent associations of these four exposures with ASD and GIDs suggest that these maternal conditions can affect the development of multiple organ systems. Interestingly, associations between ASD and childhood obesity, diabetes, and asthma have been reported, indicating that children diagnosed with ASD may be at greater risk of several different inflammatory co-occurring conditions (Cortese et al., 2022; Kaas et al., 2021; Sammels et al., 2022).
Studies also have established that the presence of conditions associated with MIA during pregnancy, including the ones in the present study, can influence the gut microbiota of both mothers and their children (Mulligan & Friedman, 2017). The gut microbiota of infants with mothers diagnosed with gestational diabetes was found to be less diverse than that of infants with mothers who did not have diabetes (Ponzo et al., 2019), exposure to maternal asthma in utero can alter gut microbiota in infants (Chong et al., 2018), and the children of overweight mothers had lower concentrations of Bifidobacterium and Clostridium histolyticum at 6 months old than did infants of women with average weights (Collado et al., 2010). While differences in the gut microbiota of children have been linked to neurodevelopment and behavior (Srikantha & Mohajeri, 2019), evidence for the influence of gut microbiota on development and treatment of ASD remains equivocal (Tan et al., 2021). It is also possible that additional environmental exposures or genetic characteristics increase both these maternal conditions during pregnancy and ASD and GIDs in young children. Further research is needed to understand the links between conditions associated with MIA and the co-development of ASD and GIDs.
The major strength of our study is the diverse and large birth cohort with comprehensive data including social demographics, maternal health conditions during pregnancy, and relatively long-term continuous follow-up of children from birth to obtain clinical diagnosis of ASD and GIDs in children through EMR. The continuity of care at KPSC minimizes ascertainment bias for both exposures and outcomes. We were able to adjust for not only social-demographic confounders but also maternal health conditions other than the four of focus in this study. These data allowed us to reveal novel findings concerning the likelihood of ASD and GIDs associated with exposures to four common maternal health conditions during pregnancy. Our Kaiser Permanente Southern California membership age and race/ethnicity distributions are comparable to its service area – in Southern California, as shown in the comparison with the census tract data in 2010 (Koebnick et al., 2012), and in the American Community Survey in 2020 (data not shown). Thus, the findings presented here are likely to be broadly generalizable to the underlying study population.
This observational study has limitations. Our findings do not establish a causal link between maternal exposures and ASD with co-occurring GIDs. We did not assess severity of ASD, beyond stratifying by co-occurring GIDs. This study considered broad categories of GIDs and did not explore relationships between exposure to maternal conditions of pregnancy and specific types of GIDs. Similarly, maternal diabetes diagnoses (Type 1 diabetes, Type 2 diabetes, and gestational diabetes mellitus) were combined into a single exposure variable, as previous work in this cohort reported significant associations between maternal diabetes and ASD (Xiang et al., 2015). We chose to focus on preeclampsia exposure and offspring ASD to identify links between this discrete maternal hypertensive disorder and offspring ASD with and without co-occurring conditions. Assessment of associations between more specific maternal exposures and offspring ASD outcomes is an avenue for future research. Paternal data and parental genetic information were unavailable; thus, we were unable to control for paternal factors and genetic contributions to likelihood of ASD and GIDs. There may be other potential residual confounders, such as environmental exposures and postnatal risk factors like childhood diet and household exposures, which could not be controlled for in this study. A validation approach led by trained experts found that having two or more diagnoses ICD codes in electronic medical records provided 88% positive predictive value (PPV) for an ASD diagnosis, which suggests that there may be outcome misclassification. There may also be exposure misclassification in the electronic medical records. However, misclassification of exposure is not likely different for kids with or without ASD, and misclassification of ASD is not likely different for different levels of exposure; thus, misclassification is potentially non-differential for both exposure and outcome. Thus, the likelihood that our significant findings are due to misclassification bias is small.
In conclusion, in the multi-ethnic cohort study, maternal obesity, diabetes, preeclampsia, and asthma during pregnancy were each associated with increased likelihood of GIDs and ASD with or without GIDs in offspring. Associations appeared greater for ASD with GIDs for all four maternal exposures. Given the higher prevalence of GIDs in children diagnosed with ASD compared to children without ASD, and that over 80% of GIDs were diagnosed prior to ASD diagnosis, this study suggests there may be common biological pathways between ASD and GIDs impacted by these maternal exposures. The results of this study indicate that prevention or effective management of inflammatory conditions of pregnancy will help to reduce likelihood of children developing GIDS and ASD with or without GIDs. Future studies are warranted to assess associations between other exposures and ASD with co-occurring GIDs to increase our understanding of ASD heterogeneity.
Supplemental Material
sj-docx-1-aut-10.1177_13623613221118430 – Supplemental material for Maternal obesity, diabetes, preeclampsia, and asthma during pregnancy and likelihood of autism spectrum disorder with gastrointestinal disturbances in offspring
Supplemental material, sj-docx-1-aut-10.1177_13623613221118430 for Maternal obesity, diabetes, preeclampsia, and asthma during pregnancy and likelihood of autism spectrum disorder with gastrointestinal disturbances in offspring by Sarah A Carter, Jane C Lin, Ting Chow, Xin Yu, Md Mostafijur Rahman, Mayra P Martinez, Klara Feldman, Sandrah P Eckel, Jiu-Chiuan Chen, Zhanghua Chen, Pat Levitt, Frederick W Lurmann, Rob McConnell and Anny H Xiang in Autism
Supplemental Material
sj-docx-2-aut-10.1177_13623613221118430 – Supplemental material for Maternal obesity, diabetes, preeclampsia, and asthma during pregnancy and likelihood of autism spectrum disorder with gastrointestinal disturbances in offspring
Supplemental material, sj-docx-2-aut-10.1177_13623613221118430 for Maternal obesity, diabetes, preeclampsia, and asthma during pregnancy and likelihood of autism spectrum disorder with gastrointestinal disturbances in offspring by Sarah A Carter, Jane C Lin, Ting Chow, Xin Yu, Md Mostafijur Rahman, Mayra P Martinez, Klara Feldman, Sandrah P Eckel, Jiu-Chiuan Chen, Zhanghua Chen, Pat Levitt, Frederick W Lurmann, Rob McConnell and Anny H Xiang in Autism
Footnotes
Acknowledgements
The authors thank KPSC patients for helping us improve care using information collected via our electronic health record systems.
Author contributions
Sarah A Carter, Xin Yu, Md Mostafijur Rahman, Zhanghua Chen, Pat Levitt, Frederick W Lurmann, Rob McConnell, and Anny H Xiang were responsible for the study concept and design. Rob McConnell and Anny H Xiang obtained funding. Sarah A Carter, Jane C Lin, Ting Chow, Xin Yu, Md Mostafijur Rahman, Mayra P Martinez, Klara Feldman, Sandrah P Eckel, Jiu-Chiuan Chen, Zhanghua Chen, Pat Levitt, Frederick W Lurmann, Rob McConnell, and Anny H Xiang conducted the study. Jane C Lin, Ting Chow, Mayra P Martinez, and Anny H Xiang acquired data. Jane C Lin, Ting Chow, and Anny H Xiang analyzed data. Sarah A Carter, Rob McConnell, and Anny H Xiang drafted the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by National Institutes of Health (R01ES029963 (Xiang, McConnell); R56ES028121 (Xiang); R01DK116858 (Page; Xiang); P30ES007048 (McConnell), Simms/Mann Chair in Developmental Neurogenetics (Levitt) and WM Keck Chair in Neurogenetics (Levitt), and by Kaiser Permanente Southern California Direct Community Benefit Funds. The funding agencies had no role in the design of the study, the analysis or interpretation of data, or the preparation or approval of the manuscript. The other authors received no additional funding.
Ethical approval
This study was approved by KPSC and University of Southern California Institutional Review Boards, with individual subject consent waived. There was no community involvement in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.