
Abstract
We examined the association of socioeconomic status with the diagnosis of autism during 16–30 months of age. Using data from a national survey in China, we included 6049 children (55.6% male) in the final analysis, among which 71 of them were clinically diagnosed with autism. Adjusted for covariates, the odds ratios for having the diagnosis of autism (2.46, 95% confidence interval: [1.32, 4.59]) among children whose mother’s level is “junior middle school or below” were significantly higher than children whose mother’s level is “college or above.” Among children of lower educated mothers, there is a higher risk of being diagnosed with autism at a young age. We recommend more support for families with a low socioeconomic status to early detect, diagnose, and manage autism.
Lay abstract
Does being born in a family of high socioeconomic status mean a higher risk of being diagnosed with autism? The evidence from the Asian area is lacking. This research was conducted among 6049 toddlers who went through an evaluation–diagnose procedure of autism and whose parents were surveyed during the national survey of China, 2016–2017. Parents reported their education levels, occupations, family income, and ethnic background. We recruited the toddlers and parents from kindergartens, communities, and hospitals in five geographically representative areas of China. On average, these toddlers were 23 months of age. We found toddlers whose mothers had less than 9 years of education (junior middle school or below) had 2.46 times the chance to get a diagnosis of autism, compared with toddlers whose mothers had more than 15 years of education (college or above). We also found that 1.17 toddlers could be diagnosed with autism in each 100 Chinese toddlers. These findings have important implications for providing support to families that have low socioeconomic status, especially families with a mother who did not complete 9 years of education. Early detection programs focused on children from low socioeconomic backgrounds should be promoted.
Introduction
Early detection, diagnosis, and management of autism in childhood are crucial to offering timely support (Lai et al., 2014). For this, full and equal access to high-level autism evaluation services is necessary (Lai et al., 2014). The challenge of early identifying children with autism is behavior assessment; only high-quality services could provide precise and cautious evaluation, which parents from low socioeconomic status (SES) might have less access (Lord et al., 2018).
The association between SES and autism has been discussed for years. Although most SES factors, such as maternal/paternal age, education, occupation, family income, ethnicity, race, and residence, have been addressed, the results remain inconclusive. For instance, although research indicated higher parental education level was associated with a higher rate of autism (Durkin et al., 2017; Kelly et al., 2019; Lung et al., 2018; Rosenberg et al., 2018), there were opposite results published as well (Abdullahi et al., 2019; Fujiwara, 2014; He et al., 2018; Rai et al., 2012; Rosenberg et al., 2018; Zablotsky et al., 2019). In addition, two studies found no association between SES and autism (Larsson et al., 2005; Giserman-Kiss & Carter, 2020).
In Supplemental Table S1, we listed the previous epidemiological studies of SES and autism. It shows most SES-autism studies were conducted by developed countries, including the United States, United Kingdom, Australia, Sweden, and Denmark. There were only four studies that represented the population of Asian origin (Fujiwara, 2014; He et al., 2018; Lung et al., 2018; Zhang et al., 2010), but a relatively small sample size (Zhang et al., 2010), regional sample (Fujiwara, 2014; Zhang et al., 2010), and the variety of autism inclusion criteria (He et al., 2018; Lung et al., 2018) limited the generalization of the results.
On the contrary, the availability of autism-related health services, including diagnosis services, is highly SES-dependent (Cantor et al., 2021). The poor in low- and middle-income countries are consistently at a disadvantage in each of the dimensions of health service access (Peters et al., 2008). As a low-middle income country with a huge population basis and regional developmental differences, the barriers to accessing health services in China could be higher from Western countries (Jacobs et al., 2012). For instance, although China promoted a universal health care policy, a child may be undiagnosed due to the less educated mother lacking knowledge of autism and failing to get the child screened. However, the potential barriers can hardly be tackled, due to a lack of autism-SES evidence from the Chinese context. In this case, research that addresses the relationship between autism and SES in the Chinese context as well as the prevalence of autism among young-aged children is urgent to support policy-making and promote regular screening among vulnerable populations.
This study aimed to gain an understanding of potential inequalities in the toddlers with autism in China and examine the association of SES (maternal/parental education level, occupation, ethnic background, and household income per year) with the prevalence of autism during 16–30 months of age. We chose the age range because it is the time that Chinese children were recommended to undergo developmental surveillance at a primary care pediatric visit (China, 2009) and the earliest time that a child could be diagnosed with autism (Miller et al., 2021). Besides, the prevalence of autism in the age range in China remains unknown. We hypothesize maternal education level is associated with the risk of autism diagnosis. This study adds to the literature by studying the association between socioeconomic factors and autism, using data from a national survey in China. To our best knowledge, this is the first research to assess the association between SES and early clinical diagnosis of autism spectrum disorder (ASD) by considering comprehensive SES factors in the Asian area. In addition, we used child psychologists/psychiatrists to diagnose child autism, to obtain a reliable prevalence of autism among Chinese children at a young age. Apart from maternal original factors, paternal education and occupation, ethnicity, and household income per year are studied.
Method
Study population and design
This cross-sectional study was a part of the national validation study for the Chinese version of the Modified Checklist for Autism in Children–Revised with Follow-Up (M-CHAT-R/F), which was conducted between August 2016 and March 2017. The details of the validation study are published (Guo et al., 2019). Briefly, using a convenience cluster sampling strategy, five cities (Guangzhou, Foshan, Hangzhou, Guiyang, and Wuhan) from four provinces (Guangdong, Zhejiang, Guizhou, and Hubei) and two municipalities (Beijing and Chongqing) were selected as the study sites. At each study site, one or two tertiary hospitals were randomly selected as the collaboration hospitals, which is, one way, responsible for sample recruiting and, in another, randomly selecting their affiliated communities and kindergartens. In addition, for those children recruited from hospitals, only those children who came to the hospital with the purpose of (a) general health care, (b) prophylactic vaccination, or (c) physical examination before entering the kindergarten would be recruited, to avoid potential selection bias. According to economic development level, these regions were further classified as eastern, southern, and capital regions (Beijing, Zhejiang, and Guangdong) and middle and western regions (Hubei, Guizhou, and Chongqing). Finally, a total of 7928 children aged 16–30 months (and their parents) were recruited from seven tertiary hospitals, 21 communities, and seven kindergartens. Among these children, the origin from hospitals, communities, and kindergartens was 62.18%, 30.92%, and 6.17% respectively. The study was approved by the Ethical Review Committee for Biomedical Research of the institution where the corresponding authors work. All caregivers of children were informed of the purpose of the study by researchers. Signed written informed consent was obtained before the questionnaire was completed. In total, 6049 parents completed the survey via parent-reported questionnaires (the participation rate was 76.3%). The questionnaire assessed socioeconomic characteristics, autism-related symptoms of children, as well as age, gender, maternal health behavior, and clinical issues during pregnancy. On the contrary, 1879 parents only finished the M-CHAT-R screening procedure but either refused or lost follow-up. These parents only provided SES information of the child’s gender, age, and if the only child in the family. Figure 1 shows the flowchart of sample enrollment, the questionnaire survey, and the diagnosis procedure of autism.

Flowchart of sample enrollment, questionnaire collection, and autism diagnosis.
Socioeconomic characteristics
Information on socioeconomic factors was collected via a questionnaire. We included ethnic background, maternal/paternal education level, and occupation as well as household income.
Ethnic background was assessed by the question, “What is the ethnic background of your children? Please specify.” Parents would write down the ethnic background of the child. Ethnic background was categorized as “Han ethnic background vs Other ethnic backgrounds.”
Maternal/paternal education level was assessed by the question, “What is the mother’s/father’s education level?” The response options were as follows: (a) primary school or below, (b) junior middle school, (c) high school/vocational high school, (d) college, or (e) graduate school or above. Education level was grouped into three categories: “Junior middle school or below, high school, college or above.”
Maternal/paternal occupation was assessed with the question, “What is the mother’s/father’s current occupation?” Response options were as follows: (a) principal of government offices, business or public institutions; (b) professional and technical staff; (c) office clerks or related personnel; (d) sales and service personnel; (e) production personnel in agriculture, forestry, animal husbandry, fishing and water conservancy; (f) operation personnel of production, transportation, equipment; (g) soldiers; or (h) others. The response options were based on the Chinese Standard Classification of Occupation (CSCO, 2015). We further grouped occupation into “Higher managerial, administrative or professional (A&B), Intermediate, routine and manual occupation (C, D, E&F) and others (G&H),” by the National Statistics Socioeconomic Classification (2020).
Household income data were collected by the question, “What is your household income per year? Household income was defined as income of all family members who live together, including salary, bonus, and income from investment.” Response options were as follows: (a) 50,000 yuan or below, (b) 50,000–100,000 yuan, (c)100,000–150,000 yuan, (d) 150,000–200,000 yuan, (e) 200,000–300,000 yuan, (f) 300,000–400,000 yuan, (g) 400,000 yuan or above, or (h) I do not know. Household income was further categorized as “100,000 yuan or below, 100,000-299,999 yuan, 300,000 yuan or above, not reported.”
Autism evaluation and diagnosis
During the child health care visit, caregivers completed the M-CHAT-R/F. This questionnaire consists of 20 questions about autism behavior. Behavior including social communication dysfunction and restricted repetitive behavior were evaluated (e.g. if you point to an object in the room, would your child look at it? Please choose yes or no). Children with positive screening further underwent a face-to-face Childhood Autism Rating Scale (CARS) performed by trained psychometrists and/or licensed psychologists in tertiary hospitals in the study area. The diagnostic process also included 30 min of parent interviews and interactions with children. The final diagnosis was made according to the 30-min interaction and the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) diagnostic criteria. All evaluations were performed no longer than 1 week after the M-CHAT-R/F was completed.
Potential cofounders
The following characteristics were included as potential confounders: maternal age, child sex, child age, the only child in the family (yes or no), maternal overweight or obesity before pregnancy (China, 2013; yes or no), preterm birth (yes or no), pregnancy complications (such as gestational diabetes mellitus and gestational hypertension, “yes” or “no”), secondhand smoking exposure (yes or no), and depressed mood during pregnancy (assessed by a question, “if the mother once experienced lasting low mood or down in spirit during pregnancy,” “yes” or “no”; Breider et al., 2021).
Statistical analysis
Data analyses were conducted during April and May 2021. Continuous variables and categorical variables are presented as either mean (SD) values or percentages, respectively. T-tests (continuous variables) or chi-square tests (categorical variables) were used to explore differences between children with or without an autism diagnosis, regarding socioeconomic characteristics.
Generalized linear models with a logit link function were applied to explore the associations between socioeconomic factors and child autism diagnosis.
Statistical analyses were conducted with Statistic Package for Social Science 25.0 (SPSS 25.0, IMB, U.S. 2017), except Firth’s bias reduction regression, which was conducted by R (version 4.0.5). The results were presented as odds ratios (ORs) with a 95% confidence interval (95% CI). All applicable tests were two-sided tests and p < 0.05 was considered statistically significant. Sensitivity analysis was conducted by analyzing basic characteristics of the research population according to paternal education level (Supplemental Table S3) and research area level (Supplemental Table S4), as well as the associations between socioeconomic factors and child autism diagnosis that only included term children (Supplemental Table S5), boys (Supplemental Table S6), and all children with a Firth-based logistic regression model (Supplemental Table S7).
There was no community involvement in the reported study.
Results
Children without data (n = 1879) were not included in the analysis. We compared children with and without data (Supplemental Table S2). No differences in age, gender, or being an only child between the two groups were observed.
There were 6049 infants and children in the final analysis (area distribution: Beijing, 21.6%; Guangdong, 42.9%; Zhejiang, 15.3%; Chongqing and Guizhou, 18.1%; and Hubei, 2%), of which 1.17% got an autism diagnosis. The mean age of the children was 22.68 (SD = 4.11) months. The majority of children were boys (55.6%), with Han ethnic background (93.8%), living in an urban area (57.4%), and coming from a one-child family (70.7%). Almost half of the children had a mother aged 24–29 years (52.7%). For education level, most mothers (67.5%) and fathers (65.9%) reported having finished college or higher. Children from families with a 300,000 yuan/year household income were rare (7.7%). The most common occupation type was intermediate, routine, and manual for the father (39.8%) and others for the mother (41.5%). Pregnancy and perinatal issues were commonly reported, including complications of pregnancy (14.2%), depressed mood during pregnancy (24.6%), maternal prepregnancy overweight/obesity (7.8%), secondhand smoking during pregnancy (13.9%), and preterm birth (8.4%; Table 1).
Basic characteristics of the study population according to autism diagnosis (M (SD) values or case number (%)).
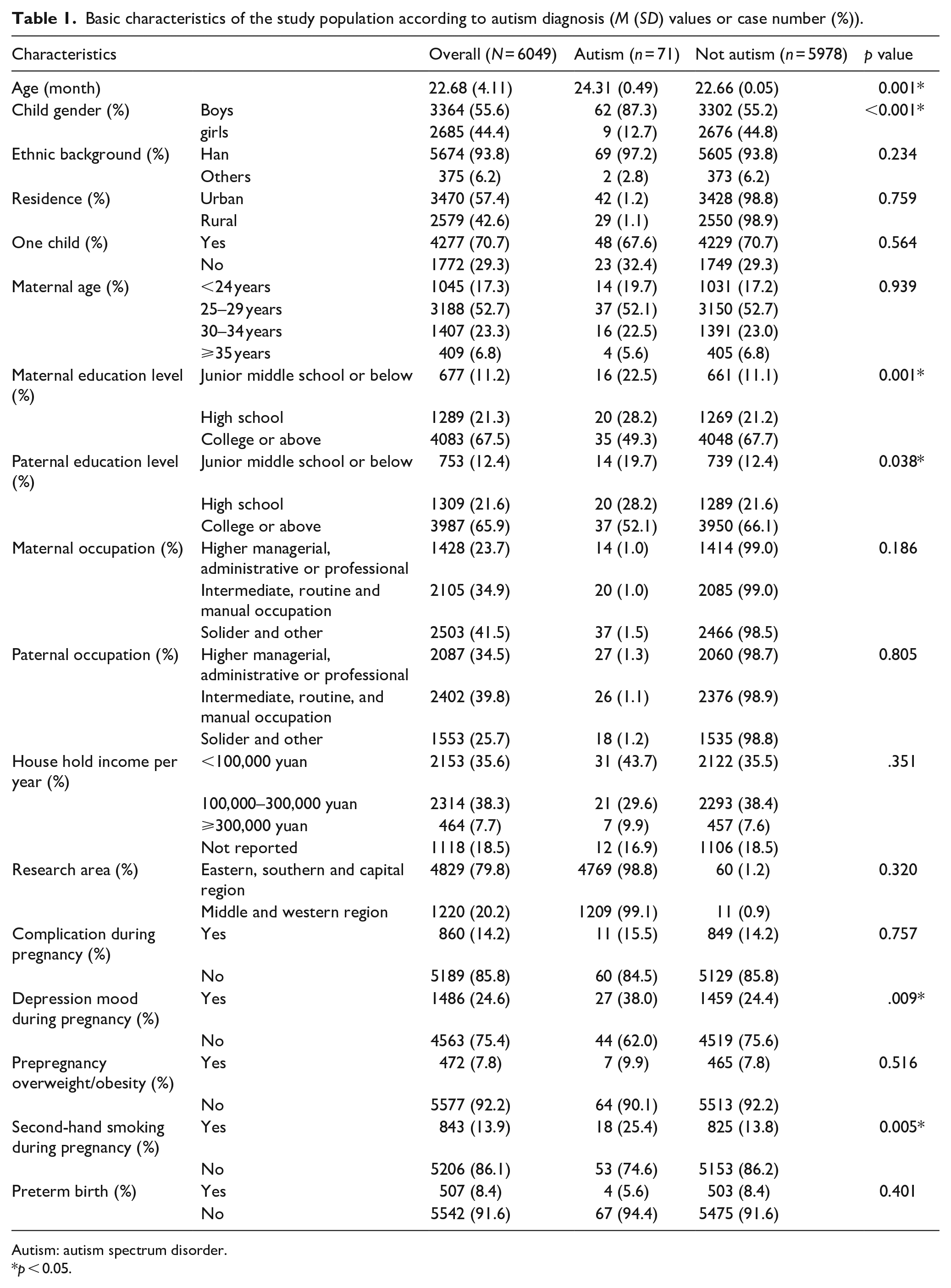
Autism: autism spectrum disorder.
p < 0.05.
The majority of autism diagnoses were among boys (87.3% vs 12.7%, boys vs girls, in children who got autism diagnosis, p < 0.001) and older aged children (24.32 (0.49) months vs 22.66 (0.05) months, p = 0.001). Children with an autism diagnosis more often had a mother or father with a low education level (e.g. junior middle school or below 22.5% (autism) vs 11.1% (not autism), p < 0.001 and 19.7% vs 12.4%, p = 0.038, respectively). During pregnancy, mothers of children diagnosed with autism had more depressed mood (38.0% vs 24.4%, p = 0.009) and secondhand smoking exposure (25.4% vs 13.8%, p = 0.005; Table 1).
Compared with mother with college or above degree, primary or high school education group showed more boy gender (54.3%, 58.9%, and 58.0%, college or above, primary, high school, respectively, p = 0.011), more rural area residence (37.9%, 50.1%, 57.9%, college or above, high school, junior middle school or below, respectively, similarly hereinafter, p < 0.001), proportion of only one child (77.1%, 47.7%, and 62.7%, p < 0.001), younger age (<24 years, 11.2%, 32.3%, and 28.6%, p < 0.001), and lower household income (<100,000 yuan/year, 29.0%, 52.9%, and 47.5%, p < 0.001). Relative to mother with college or above degree, primary or high school mother experienced more depression mood (22.9%, 31.0%, and 26.3%, p < 0.001) and secondhand smoking (11.6%, 19.2%, and 18.5%, p < 0.001) during pregnancy, prepregnancy overweight/obesity (6.7%, 10.3%, and 10.1%, p < 0.001; Table 2).
Basic characteristics of research population according to maternal education level (M (SD) values or case number (%)).
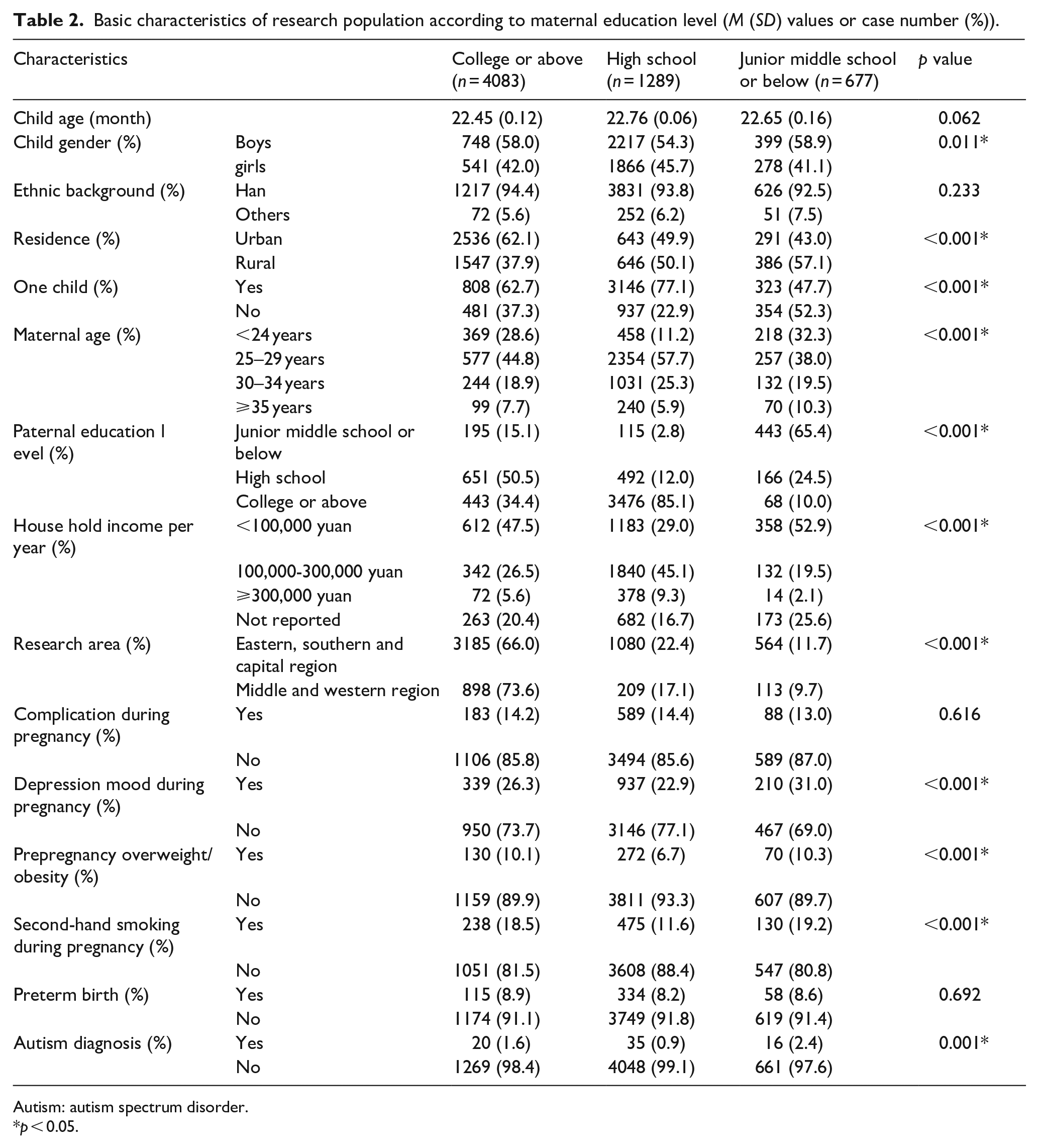
Autism: autism spectrum disorder.
p < 0.05.
The likelihood of autism diagnosis was higher among lower maternal education levels (junior middle school or below: OR = 2.80, 95% confidential interval (CI) = [1.54, 5.09], high school: OR = 1.82, 95% CI = [1.05, 3.17], Table 3, crude model), compared with maternal education that college or above. After adjusting for child age, gender, maternal age, and other socioeconomic factors in the analysis, children from mothers in junior middle school or below group were more likely to have an autism diagnosis (OR = 2.61, 95% CI = [1.36, 5.03], Table 3, adjusted Model 1), but not high school group (OR = 1.72, 95% CI = [0.95, 3.66], Table 3, adjusted Model 1). Additional adjusted prenatal and perinatal factors as well as odds of autism diagnosis were higher among children whose mother got junior middle school or lower education level (OR = 2.41, 95% CI = [1.25, 4.66]).
Odds ratio and 95% confidence interval of autism prevalence among different socioeconomic levels.

Autism: autism spectrum disorder.
p < 0.05.
Crude model had no adjustment.
Adjusted child age, gender, one child, maternal age, maternal occupation, household income, residence, research area, and ethnic background in maternal/paternal education–level analysis.
Adjusted variants in adjusted Model 1 plus preterm birth, gestational complications, depression mood during pregnancy, prepregnant overweight/obesity, and secondhand smoking during pregnancy.
Discussion
This study gained an understanding of potential social inequalities in the diagnosis of autism in China by examining the association of SES with the prevalence of autism among children 16–30 months of age. First, an up-to-date prevalence of autism in Chinese toddlers was obtained. Second, using cross-sectional data from a national multicenter study, we confirmed that low maternal education level was associated with autism among Chinese toddlers. No association was observed for the indicators of paternal education level, maternal and paternal occupation, household income, residence, and ethnic background.
This study adds to the literature by providing an updated autism prevalence from a national sample of Chinese toddlers, which could guide early screening, diagnosis, and intervention in young children with autism. Second, the results of this study ascertained a vulnerable group of toddlers, namely, toddlers from lower educated mothers who had an increased risk of getting an autism diagnosis. Thus, policy regarding autism screening, diagnosis, and intervention could be further targeted toward this specific population. Third, in a broader view, this study also provided evidence for potential social inequalities with regard to accessibility of Chinese health care services.
The prevalence of autism in our study is much higher than data reported in China in 2018 (He et al., 2018). This can be attributed to the different sampling methods and data collection time in the two studies. Data reported by He et al. came from the Second National Sample Survey on Disability in 2006. The limited diagnosis skill and tools, awareness of parents, and pediatricians 10 years ago in China may relate to a missed diagnosis. On the contrary, The authors also indicated that autistic children without mental retardation might have been excluded from the survey, which is another reason for the low rate of prevalence (He et al., 2018).
Previous research reported that ethnic background is associated with higher undocumented diagnosed autism among 0–17 years old children (Wiggins et al., 2020) and Black groups showed higher rates of autism (Keen et al., 2010). This was in contrast to the Bradford cohort study, which showed no association between ethnic background and autism (Kelly et al., 2019). Autism is heritable (more than 80%) and suspects genetic-environmental interplay (Lai et al., 2014). It is reasonable that other ethnic background groups had similar autism prevalence to ethnic Han in the Chinese population (He et al., 2018), as our study reported, because most ethnicities are the Mongolian stock and gene-homological with the ethnic Han in China (China, 2010). The findings with regard to the association between low maternal education and autism diagnosis have been reported in studies performed in the United States (Durkin et al., 2010; Rosenberg et al., 2018; Zablotsky et al., 2019), France (Delobel-Ayoub et al., 2015), Japan (Fujiwara, 2014), and Sweden (Fujiwara, 2014). Inline herewith, an association between low SES and psychiatry/developmental disorder, overall developmental disability (Zablotsky et al., 2019), ADHD (Cerrillo-Urbina et al., 2018), and mood disorder in childhood (Guhn et al., 2020) have shown in previous research. A low maternal education level has been reported to be associated with raised maternal stress and immune activation (Maharani, 2019), which are considered two of the pathways to offspring’s neuropsychiatric illness (Brown & Meyer, 2018). In addition, elevated cytokine and chemokine levels in maternal mid-pregnancy serum samples are associated with autism (Lyall et al., 2021). A literature review has shown that maternal immune activation was associated with neuroinflammation in neurodevelopmental disorders (Han et al., 2021); autism may share the same neurological pathway as these neurodevelopmental disorders.
In addition, underdiagnoses among lower educated families long have been suspected as the reason for the association between socioeconomic factors and autism (Avlund et al., 2021). Underdiagnosis might be due to a lack of knowledge among health care professionals in China (Sun et al., 2013); according to a review published in 2013 (Sun et al., 2013), most of the pediatricians in small cities in the east area of China (which is considered a more developed area) knew little about the symptoms of autism. Since then, in 2017, an expert consensus on early screening and intervention for Chinese children with autism was established (Xu, 2017). Interestingly, Sun et al. (2013) also stated that the parents were more knowledgeable about the symptoms of autism compared with pediatricians and physicians. They attributed this parental knowledge to increased access to information about autism diagnosis from the Internet and media coverage about autism (Sun et al., 2013). It was suggested that hospital staff and physicians should engage more in autism-related health education.
Moreover, underdiagnosis might relate to the accessibility parents have to autism-related information. Accessibility to autism-related sources for parents, including health education information, screening, and diagnosis institution, is socioeconomic-dependent (Fombonne, 2018). Families with higher socioeconomic positions might acquire autism-related support easier (Dickerson et al., 2017). For instance, a mother with a higher education level may have a higher chance to obtain knowledge of the developmental disorder, and therefore might be aware of the problem of the child in an earlier stage (Kelly et al., 2019). In the Bradford cohort in the United Kingdom (Kelly et al., 2019), an association was reported between having a higher educated mother and doubled odds of giving birth at a later age for autism-diagnosed children. A similar relationship between parental education and autism was found in study populations from the Taiwan area (Lung et al., 2018), as well as surveillance (Durkin et al., 2017) and regional data (Bhasin & Schendel, 2007) of the United States. Most authors of previous studies attributed the findings to ascertainment bias which was suggested to be caused by social-economic inequality, indicating there were more children, whose parents had relatively low education or economic status, remaining undiagnosed (Kelly et al., 2019).
The undiagnosed speculation is supported by research that found low parental education level or other indicators of SES status were related to a delayed (Jo et al., 2015; Avlund et al., 2021), undocumented autism diagnosis (Wiggins et al., 2020), or late first evaluation (Hrdlicka et al., 2016; Rubenstein et al., 2018). In our study, the participants’ enrollment covered children’s routine care at hospital-based, community-based, and kindergarten-based medical facilities; thus, children from different maternal education populations may have had a relatively equal chance to get the autism screening. Nevertheless, despite near-universal health insurance coverage in China, populations with low incomes may still face barriers to access and utilization of affordable health care (Towne et al., 2021). In 2021, Towne et al. showed more than 36% of Chinese reported forgone medical care due to cost in the past 12 months. In this case, cost-related disparities in the access and utilization of needed medical care persist, maybe due to lower education and being a resident of a province with a lower density of physicians (Towne et al., 2021). Compared with other developed countries such as the United States, China’s health policy is focusing on “disease treatment” rather than “preventive services” (Ma et al., 2008). In this case, a child who has not yet received a diagnosis may not be covered by health insurance. At present, early ASD screening has unfortunately only been implemented in a few large cities through cooperative projects (Zhou et al., 2022). This could impede children from poor families and those living in the rural or underdeveloped regions to get early screening.
When studying the lower rate of offspring autism among higher educated mothers, which we observed in our study, a potential stigma surrounding autism disorder hypothetically may explain this finding. According to Yu et al. (2020), the Chinese public experiences more stigma related to autism, relative to the U.S. public. In addition, they also found an association between a higher educated background and reporting the stigma of having autism (Yu et al., 2020). Interestingly, Khowaja et al. (2015) showed declining autism screening among highly educated parents, which supported that higher educated parents may be more inclined to resist an autism diagnosis.
Our finding of a lack of association between paternal education, maternal and paternal occupation with autism diagnosis might be due to the former indices’ high correlations with maternal education (Fujiwara, 2014). It appears both parents’ education level is relevant to the child’s diagnosis of autism (Table 2), but the mother’s education level has the highest impact. Parents’ occupation was once reported by Windham et al. (2009), which indicated that parents occupation with highly technical demands had more chance to give birth to autistic children. But we used a different occupation classification, which is more income-dependent.
The strengths of this study included (a) a national sample of Chinese children which added to the literature on SES and autism, (b) a combined sample that came from Kindergarten-community-hospital health care toddlers decreased the ascertainment bias, (c) diagnosis of autism was made by child psychologists/psychiatrists, and (d) an updated prevalence of autism among Chinese toddler was obtained.
This study suffers from some limitations. Although the data came from a national survey, the convenience cluster sampling strategy compromised the national representativeness. The lack of validated assessment instruments in Chinese, such as Autism Diagnostic Observation Schedule, Second Edition (ADOS-2) and Autism Diagnostic Interview–Revised (ADI-R), also limits consistency with the international standards for an autism evaluation. A multistage cluster random sampling in a follow-up national survey, along with validated assessment instruments in Chinese, should be considered in the future.
Conclusion
In this research, the population which is susceptible to autism is addressed. Using national survey data, we confirmed the association between low maternal education levels and the prevalence of autism among toddlers in a Chinese context, in addition, an up-to-date prevalence of autism among Chinese toddlers was obtained. The result showed the necessity to support lower socioeconomic families, especially low educated level mothers, to promote early detection of autism.
This study also provided important evidence in tackling barriers to accessing autism-related health services for Chinese policymakers, including taking autism screening in early childhood primary health care, and launching autism knowledge education programs, to decrease the potential stigma of the general public.
Supplemental Material
sj-docx-1-aut-10.1177_13623613221132743 – Supplemental material for Socioeconomic factors and autism among 16- to 30-month-old children: Evidence from a national survey of China
Supplemental material, sj-docx-1-aut-10.1177_13623613221132743 for Socioeconomic factors and autism among 16- to 30-month-old children: Evidence from a national survey of China by Muqing Cao, Li Li, Hein Raat, Amy Van Grieken, Xin Wang, Lizi Lin, Qiang Chen and Jin Jing in Autism
Footnotes
Acknowledgements
We thank all the participants and families, our autism research group, and all members of the national validation study for the Chinese version of the M-CHAT-R/F research team not otherwise named.
Author contributions
Concept and design: Lin
Acquisition, analysis, or interpretation of data: Li, Wang, Chen
Drafting of the manuscript: Cao
Critical revision of the manuscript for important intellectual content: Raat, Grieken
Statistical analysis: Cao
Obtained funding: Jing
Availability of data and materials
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Key-Area Research and Development Program of Guangdong Province (Grant No. 2019B030335001) and the National Science Foundation of China (Grant Nos. 81872639 and 81903337).
Research involving human participants
This research involved human participants. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
The study was approved by the Ethical Review Committee for Biomedical Research, Sun Yat-sen University. All caregivers of children were informed with the purpose of the study by researchers. Signed written informed consent was obtained before the questionnaire was completed.
Consent for publication
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.