
Abstract
Autistic children commonly experience mealtime difficulties; however, it is unknown what makes an effective transdisciplinary mealtime service for autistic children. This study used a realist evaluation framework to explore caregivers’ and therapists’ perceptions of the contexts, mechanisms and associated outcomes of a transdisciplinary mealtime management service for autistic children. Semi-structured interviews were conducted with six caregivers of autistic children engaged in a transdisciplinary mealtime service and 10 therapists providing the service, with interview data analysed using a realist evaluation approach. Four-context (child factors, family factors, therapist factors and institutional parameters), three-mechanism (transdisciplinary collaboration, child-centred approach and managing caregiver expectations) and two-outcome (impact on the child and impact on the caregiver) themes were identified. Findings highlighted that transdisciplinary collaboration, a child- and family-centred approach and managing caregiver expectations are key mechanisms providing a foundation for the development of evidence-based mealtime services for autistic children.
Lay abstract
Mealtimes and eating can be difficult for autistic children. A service where different professions work together is required to address the varied and complex mealtime difficulties of autistic children. Little is known about what is needed for such services to be effective. We interviewed six caregivers of autistic children who were engaged in a mealtime service and 10 therapists who are involved in delivering the service to understand their perspectives on the factors that were driving the effectiveness of the mealtime service. We found that different health professionals from different disciplines working together, focusing on adapting intervention to the child and family and managing expectations of the caregiver were important in contributing to outcomes of the mealtime service. The findings of this study can be used to inform the development of more effective interventions and services to support the well-being and development of autistic children.
Eating is a meaningful occupation, essential not only to sustain life but also in promoting development and social connectedness (Absolom & Roberts, 2011). Mealtimes can be particularly challenging for autistic children, with some estimates suggesting that over 80% of autistic children experience difficulties during mealtimes (Leader et al., 2020). Food selectivity and food refusal are among some of the most commonly documented feeding difficulties experienced by autistic children (Leader et al., 2020; Ledford & Gast, 2006; Page et al., 2022).
Mealtimes are complex multi-sensory experiences involving various textures, tastes, smells, appearances of food and auditory input from the environment (Nadon et al., 2011). Sensory experiences associated with mealtimes may be particularly challenging for autistic children, who can experience differences in sensory modulation (Cermak et al., 2010; Nadon et al., 2011; Page et al., 2022), that can result in avoidance or preference for particular foods or textures (Cermak et al., 2010; Nadon et al., 2011; Page et al., 2022). Motor dysfunction, another feature associated with some autistic children (Ozonoff et al., 2008), can impact swallowing and chewing and contribute to distressing mealtime experiences such as choking, gagging and vomiting (Manno et al., 2005). Autistic children may also show a preference for sameness, which may also act to restrict food preferences (Marí-Bauset et al., 2014). Autistic children may manage these feeding difficulties (i.e. sensory, motor and preference for sameness) by limiting the variety of foods consumed or by refusing food through behaviours such as food expulsion, displaying physical aggression, attempts to leave and/or verbal refusals such as crying and shouting (Provost et al., 2010; Volkert et al., 2016; Williams et al., 2010). Not only are the mealtime difficulties experienced by autistic children distressing, these difficulties can also result in nutritional deficiencies, which can hinder the child’s physical and psychosocial development (Graf-Myles et al., 2013; Zimmer et al., 2012). Furthermore, these persistent mealtime difficulties can also contribute to mealtimes being a source of family stress (Curtin et al., 2015), as mealtimes are important for maintaining (and strengthening) relationships within the family (Curtin et al., 2015; Lawrence & Plisco, 2017).
A variety of interventions exist to support autistic children during feeding (Ledford et al., 2018). Examples include systematic desensitisation (Galpin et al., 2018), escape extinction and reinforcement (Ledford & Gast, 2006). While these approaches can be valuable, they often target only singular aspects of the mealtime difficulties that may be faced by an autistic child, and may not capture and address the multiple and varied factors that may contribute to mealtime difficulties for autistic children (Leader et al., 2020). Given the complexities of Autism Spectrum Conditions and the mealtime difficulties experienced by autistic children, we propose adopting a holistic, transdisciplinary approach of delivering mealtime services, consistent with recommendations by others (Laud et al., 2009; Owen et al., 2012). Unlike a uni-disciplinary approach to mealtime service delivery, where each discipline works in disciplinary-silos to deliver a mealtime service (Khalli et al., 2019), the transdisciplinary approach emphasises boundary working, where different disciplines work at role boundaries to share discipline-specific expertise and work interdependently with one another and with the client, to provide a client-centred service (Bowman et al., 2021).
Although Bowman et al. (2021) recommended transdisciplinary service provision, reviews of the literature on mealtime approaches for autistic children (Diaz & Cosbey, 2018; Ledford et al., 2018; Ledford & Gast, 2006) suggest this is currently an under-researched area. Specifically, scant studies exist that explores the mechanisms that influence the effectiveness and outcomes of transdisciplinary services addressing mealtimes for autistic children. To address this knowledge gap, this study aimed to explore caregiver and therapist perceptions of the contexts, mechanisms and outcomes of a transdisciplinary mealtime service for autistic children.
Methods
Design
A qualitative approach guided by the realist evaluation framework (Pawson & Tilley, 1997) was used to determine the active ingredients of atransdisciplinary mealtime management service. A realist evaluation approach is concerned with answering the question ‘‘what works for whom in what circumstances . . . and why’ (Pawson, 2013, p. 15). Unlike other evaluation methods, realist evaluations acknowledge that contextual elements can influence interventions and their outcomes (Gilmore et al., 2019). Through a realist evaluation, the mechanisms (what works), contexts (the conditions and circumstances) and outcomes of a service are identified, and context–mechanism–outcome configurations are explored to understand the interconnectedness of the contexts and mechanisms of a service associated with the outcomes observed (Pawson, 2013). A realist evaluation approach was selected due to its particular utility in evaluating complex interventions. The mealtime service met several criteria for a complex intervention (Craig et al., 2008), being tailored to individual children and their families and containing multiple interacting components. It also involved various participants (i.e. the child, families), and had variable target behaviours and outcomes. Through the realist evaluation, those particular factors contributing to the outcomes mealtime service could be disentangled, supporting knowledge translation and service provision (Salter & Kothari, 2014).
The service
Therapy Focus is a disability service provider based in Perth, Western Australia (WA) and is the organisation in which this research was conducted. The Mealtime Eating Allied Health Liaison Service (MEAHLS) at Therapy Focus is one of the many therapy services provided by the organisation (Therapy Focus, 2022). MEAHLS is a transdisciplinary specialist mealtime service that aims to provide client-centred solutions to address the mealtime needs of children with disabilities including autism (Therapy Focus, 2022). Clients who access this service typically have complex mealtime needs (Therapy Focus, 2022). A proposed definition of complex mealtime needs is, mealtime needs that arise from multiple, interacting factors (e.g., physiological, socio-cultural, and/or psychological) that, consequently, require therapists from different professions to contribute profession-specific knowledge, skills, and expertise, in collaboration with the client and their caregiver(s), to achieve shared, context-dependent mealtime goals.
This proposed definition aligns with the therapy service provision approach of Therapy Focus (2022) and recommendations from key health bodies (Institute of Medicine, 2015; World Health Organization, 2016) on the importance of ensuring a collaborative approach to deliver client-centred healthcare.
Given the complex nature of clients’ mealtime needs, mealtime service delivery typically encompasses mealtime assessments and interventions that involve collaboration among the client (person with mealtime difficulty), their caregivers, therapists from the client’s broader therapy team (from the same organisation that may be addressing other needs of the child and family) and MEAHLS therapists (Therapy Focus, 2022). For example, a mealtime assessment involves MEAHLS therapists working collaboratively with caregivers, the client and therapists from the client’s therapy team to gain insight into the client’s mealtime concern and current mealtime capability. Therapists then complete mealtime evaluations and make individualised recommendations for interventions that meet the needs of the autistic children and their caregivers (Therapy Focus, 2022).
It should be noted that therapists within the service play a crucial role in guiding caregivers and clients to prioritise mealtime interventions by supporting service recipients (i.e. clients, caregivers) to identify functional outcomes associated with the mealtime intervention (e.g. for the autistic client to have a meal at the dining table, together with family); set specific, measurable, achievable, realistic and time-bound (SMART) intervention goals associated with the desired functional outcome of intervention; and finally, ensure caregivers are equipped with strategies that align with the SMART goals and outcomes (Therapy Focus, 2022).
In line with an individualised approach to mealtime interventions, therapists use a combination of tools and strategies such as food desensitisation, oral-motor therapy and behavioural management to improve functional outcomes and social engagement during mealtimes. Therapists in the service include occupational therapists, physiotherapists, dieticians and speech pathologists who bring profession-specific expertise to create person-centred mealtime interventions (Therapy Focus, 2022). The hours of service delivery is dependent on the goals identified and the number of therapists involved in delivering the service (Therapy Focus, 2022).
Participants
A total of six caregivers of autistic children accessing the mealtime service and 10 therapists delivering the service were purposively recruited to participate in this study. Caregiver participants were required to have a child under 16 years of age, with a diagnosis of autistic disorder, Asperger’s disorder or pervasive developmental disorder – not otherwise specified, according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed. text rev.; DSM-IV-TR; American Psychiatric Association, 2000), or a diagnosis of autism according to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-V; American Psychiatric Association, 2013). Their child was required to be currently participating, or have previously participated, in at least two sessions with the mealtime service. Therapist participants were required to be practicing occupational therapists, speech pathologists, physiotherapists and dieticians who were part of the mealtime service and had autistic clients under 16 years of age.
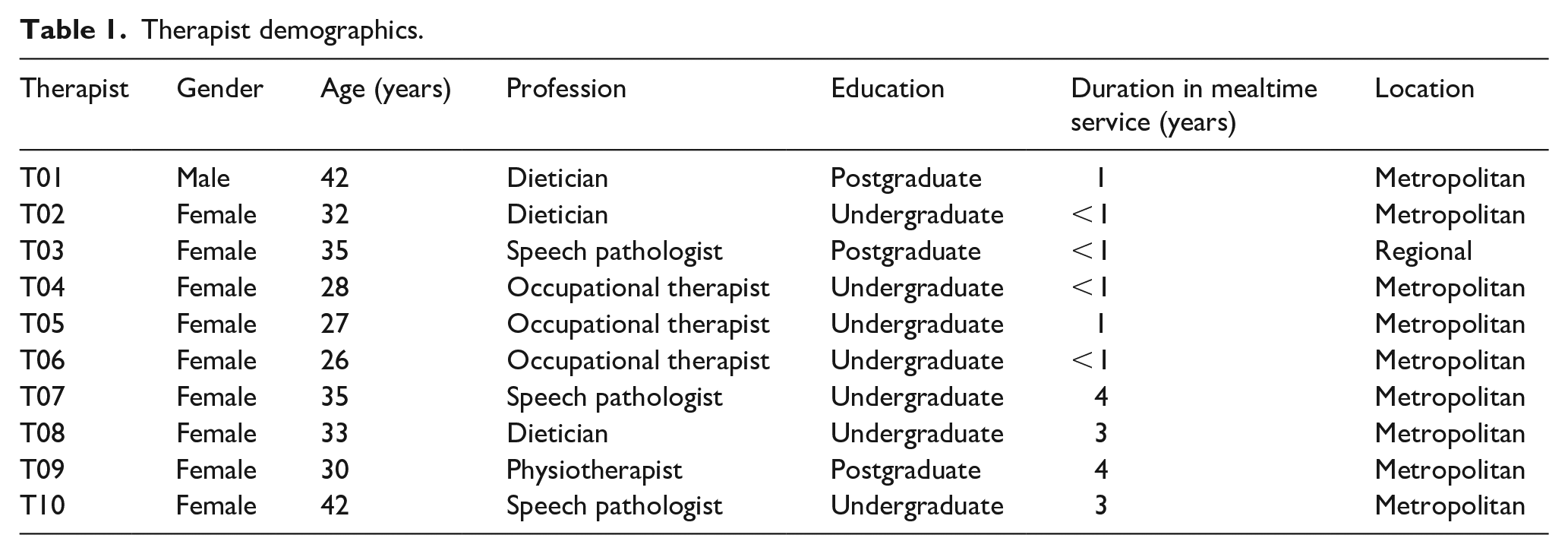
The socio-demographic characteristics of therapists, caregivers and their child are outlined in Tables 1 to 3, respectively. Therapists were occupational therapists (n = 3), speech pathologists (n = 3), dieticians (n = 3) and a physiotherapist (n = 1). The majority of therapists had been delivering the mealtime service for up to 1 year (n = 6). The remaining four therapists had been in the team for 3 to 4 years (n = 4). Most therapists worked in the metropolitan area (n = 9), with one therapist working regionally. Caregivers had a mean age of 36.8 years (SD = 4.22, range = 32–42 years). One male and five females were interviewed. Caregivers’ main education was a Technical and Further Education/Diploma equivalent (n = 5) and majority were located in the metropolitan area (n = 5). Each caregiver had a child aged between 5 and 11 years (mean age 9.7 years), who had been accessing the service for up to 3 years.
Therapist demographics.
Caregiver demographics.

TAFE: technical and further education.
Child demographics.
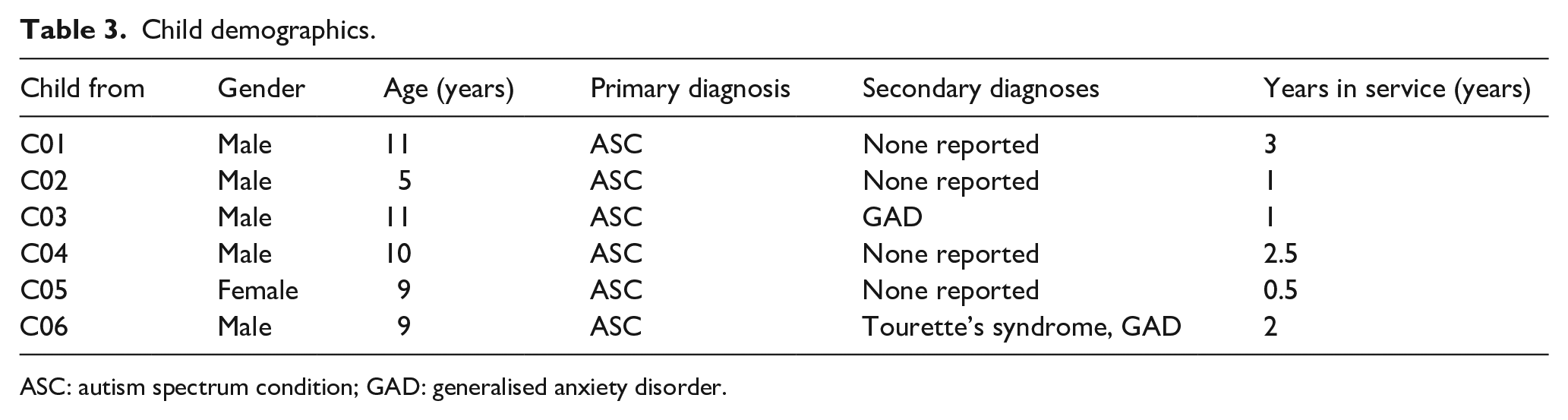
ASC: autism spectrum condition; GAD: generalised anxiety disorder.
All children had received a diagnosis of autism prior to their participation in the study, which requires children to be evaluated by a trained multidisciplinary team (Whitehouse et al., 2018). Two children had co-occurring conditions, and no child had a co-occurring intellectual disability.
Materials
Socio-demographic questionnaire
Socio-demographic questionnaires were delivered to participants via Qualtrics (2020), which is an online survey platform. Questionnaires collected the socio-demographic information (such as age and gender) of caregivers and therapists, as well caregiver educational background, the child’s specific autism diagnosis and the therapist’s length of practice experience.
Semi-structured interview guide
Semi-structured interview guides gathered participants’ perceptions of factors that influence the outcomes of the mealtime service. Separate interview guides were developed for caregivers and therapists (Supplementary File 1). The caregiver interview guide explored their child’s engagement in the mealtime programme, their expectations and perspectives of the service and the perceived outcomes of the service for their child and family. A pilot test of the interview guide was completed with a caregiver of an autistic child prior to data collection, with amendments implemented prior to its use. The therapist interview guide explored their role in the service, the strategies they used, their perspectives on the participation of the child and family and the observed outcomes.
Procedure
Participants were provided with an information sheet and were required to provide written informed consent. To accommodate caregiver participants’ schedules, they were provided with the option to participate in online, telephone or face-to-face interviews. They were also provided with the opportunity to provide written responses. Prior to the interviews, each participant received a link to the questionnaire via email and was provided with the interview guide. Interviews were audio-recorded and had an average duration of 1 h and were conducted either online, through phone calls or in person. Each participant participated once, either during or after their involvement in the mealtime service. All interviews were conducted by researchers independent of the therapy service, and individual results were not shared with researchers from the organisation.
Ethical considerations
Ethical approval was obtained from the Curtin University Human University Human Research Ethics committee (HRE2020-0769). All participants provided individual written informed consent prior to participating in the study. Caregivers who participated in interviews were provided with a US$10 retail gift voucher. Participants were informed that their responses would not impact the services that they or their child receive through the organisation.
Community involvement
Caregivers of autistic children were involved in this study as participants. Autistic individuals were not directly involved in the design, implementation, analysis or interpretation of this study.
Data analysis
All recorded interviews were transcribed verbatim. Transcriptions were checked for accuracy and imported into NVivo 12 Pro (QSR International Pty Ltd., 2020) for analysis. Using the realist evaluation framework, transcribed data were initially coded into each of the context, mechanism and outcome categories. Analyses were undertaken across all interviews with data from different participant groups (caregivers and therapists) treated as one dataset. These codes were subsequently organised into themes to explore the key contexts, mechanisms and associated outcomes of the service. Contexts referred to factors outside the parameters of the service that could affect how autistic children and their caregivers engage in the service (Pawson & Tilley, 1997). Mechanisms referred to how the service was run and outcomes referred to the expected or unexpected consequences of the service (Pawson & Tilley, 1997). The relationships between the contexts, mechanisms and outcomes were then identified by the research team by examining transcripts and the links made between contexts, mechanisms and outcomes by the participants. The analysis process is illustrated in Figure 1.
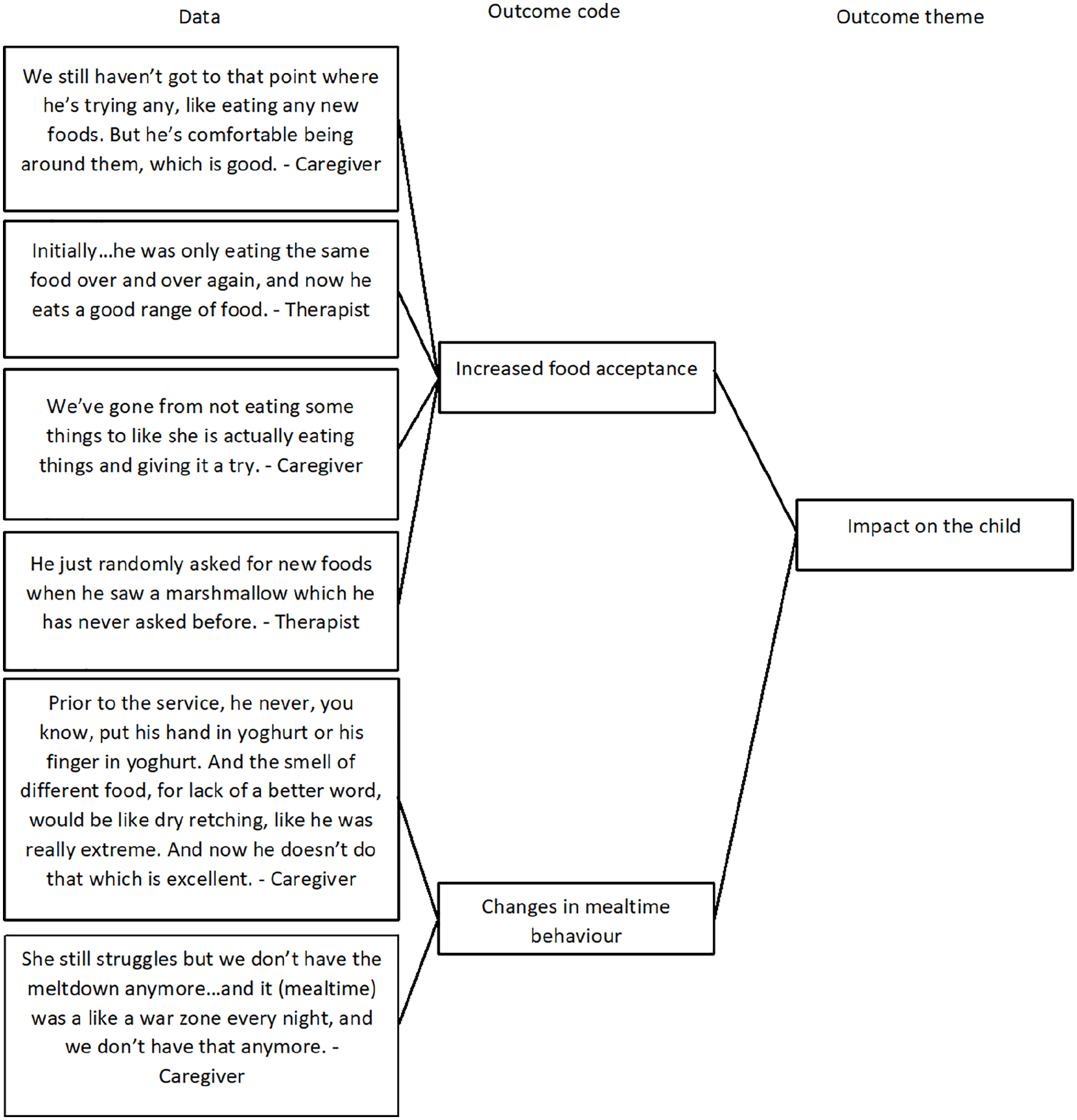
Thematic analysis process example.
Each group member kept a reflexive journal and discussed themes within the research team to resolve any discrepancies, which increased confirmability by minimising bias of a single interviewer (Krefting, 1991). Debriefing sessions with the research team were conducted to ensure team accountability throughout data collection and analysis (Krefting, 1991). To improve transferability of the findings, a thick description of the participants experiences and the data collection process was provided (Krefting, 1991). An audit trail was created to increase dependability and ensure transparency in the research process (Krefting, 1991).
Results
Analysis resulted in 9 context codes, 7 mechanism codes and five outcome codes, which were organised into four context themes, three mechanism themes and two outcome themes.
Context
The four context themes identified included child factors (C1), family factors (C2), therapist factors (C3) and institutional parameters (C4).
Child factors (C1)
Child-related factors captured children’s interests (C1.1), as well as the characteristics and challenges faced by autistic children during mealtimes (C1.2). Caregivers and therapists indicated that autistic children receiving the mealtime service often presented with challenging mealtime behaviours and risks of choking due to low muscle tone, poor interception (the ability to accurately identify internal sensations such as satiation or hunger), slow oral-motor development, poor breath control, difficulty following mealtime routines and varying sensory preferences. Some children were also reported to experience anxiety around mealtimes from past negative experiences with food and feeding: . . . potentially they’ve had. . . this long journey when it comes to mealtimes and maybe have had some previous mealtime experiences that were quite negative. So when it comes to working with us, they’ve already built up a huge anxiety around mealtimes too. (T08)
Family factors (C2)
Family factors included caregiver stress related to mealtimes (C2.1) and family capacity (C2.2). Caregivers experienced stress related to mealtimes (C2.1) and concerns about their child’s nutrition, growth and feeding. A caregiver (C05) reported that ‘when [her kids] weren’t eating, it stressed [her] out a lot’.
Family capacity (C2.2) also included family readiness for therapy that was often limited by the situation the family was in, such as their finances and availability for services. Families had varying levels of capacity and readiness to engage in mealtime therapy. One therapist (T04) reported that some families in lower socioeconomic areas are ‘quite low capacity’, and have difficulties attending appointments, answering the phone or sending their children to school. Another therapist (T01) reported that there are ‘some parents who just don’t have a lot of capacity’ as they have to manage ‘their own mental health or their own sensory issues around food’. A therapist (T02) commented that ‘. . . success of intervention always comes down to the capacity of the family to make changes. So this is based on what else is happening in their lives’.
Therapist factors (C3)
This theme captured therapist factors such as their clinical experience (C3.1) and caseload duties (C3.2). Therapists offered varying levels of expertise in conducting thorough transdisciplinary assessments and developing highly individualised intervention plans. Therapists reported considering their degree of clinical experience (C3.1) and confidence in providing mealtime services for clients prior to making referrals to other team members or internal specialist services.
Therapists reported that their caseload (C3.2) often limited their availability to engage in upskilling opportunities, contributing to limited confidence particularly in areas where they had less experience. However, therapists reported that they could utilise the expertise of team members who possess more knowledge in specific areas such as enteral feeding, and can provide supervision as required.
Therapists’ full caseloads and clinical responsibilities also impacted communication within the therapy team and with families. Therapists reported that these factors contributed to challenges in ensuring that team members and families were aware of the child’s progress: . . . [therapists are] all open to calling families and having those discussions. The challenging part of that is that working in a community setting, we’re not always available at the same time, or not always at the same place at the same time. (T04)
Institutional parameters (C4)
This theme encompassed institutional factors that influenced therapists’ service provision, including funding systems (C4.1) and organisational processes (C4.2). Funding constraints within the Australian funding system (C4.1) were found to limit families’ access to mealtime services. Several therapists noted that insufficient therapy budgets for some services often led to reduction of therapy hours in other areas or frequency of sessions. Communication times between therapists regarding a child’s progress were also restricted as time spent discussing the child’s case was billable.
Similarly, caregivers reflected that funding reductions and inadequacies had affected the therapy their child receives. A caregiver (C05) recounted that her child’s occupational therapist could only provide therapy strategies for positioning in a chair because their child ‘[did not] have funding to get chairs’. The caregiver resorted to purchasing the recommended equipment out of pocket.
Organisational processes (C4.2) referred to the therapists’ availability and organisation waitlists, geographical location and shadowing opportunities. Multiple therapists highlighted that a shortage of therapists led to larger caseloads for individual therapists and longer waitlists, which was exacerbated by the high demand for the service. Larger caseloads limited therapists’ abilities to address urgent circumstances, such as rapid functional declines, changes to a child’s dietary needs and new equipment requiring immediate reviews, all of which elicited concerns for the child’s safety during mealtimes, if left unaddressed: We’ve just lost our [physiotherapist], and we’ve not had an OT [occupational therapist] in my area for a while . . . if we had more access to multiple therapists, across each discipline, . . . the load would be spread a little bit further . . . that would definitely improve the quality of the mealtime programme. (T10)
Geographical location (C4.3) referred to whether therapists were based in the metropolitan or regional offices, which influenced their access to shadowing opportunities. The regional therapist noted that their district had limited access to colleagues with more knowledge and experience in specific practice areas. Having access to a larger pool of expertise in the metropolitan regions enabled therapists to select referral pathways for the child according to their confidence levels in delivering the service.
Mechanisms
The three mechanism themes identified includes transdisciplinary collaboration (M1), child-centred approach (M2), and managing caregiver expectations (M3).
Transdisciplinary collaboration (M1)
A key mechanism identified by participants was engagement in a transdisciplinary team, which included communication within the team (M1.1), the role of a mealtime service therapist (M1.2), and contribution of expertise to service delivery (M1.3). While each discipline had key roles (M1.2; Supplementary File 2.1), therapists reported that they also adopted a transdisciplinary approach where they might work outside their scope of practice. For example, during a transdisciplinary assessment, therapists are skilled in assessing components of other disciplines that influence a client’s mealtime before making referrals to the corresponding services. Therapists reported that in complex cases, a therapist from all disciplines may attend the assessment, followed by ‘a case discussion’ to determine ‘the priority discipline’ and develop the ‘best’ plan for the child: We’ll look into all the clinicians’ roles that may be impacting [the child’s] feeding . . . regarding oral-motor, a SP [speech pathologist] will be needed. A PT [physiotherapist] for his balance and core for feeding, what he needs for breathing . . . Toileting, that will have an impact as well . . . Really comprehensively figuring out what may be symptoms that are impacting on eating and then going from there. (T05)
Within the transdisciplinary team, therapists reported that they shared their skills and knowledge (M1.3) to work collaboratively through regular discussions within the therapy team about the child’s progress (M1.1) and joint sessions to support a child in achieving therapy goals (Supplementary File 2.2). A therapist (T07) identified that a benefit of the service was that it was ‘the only one’ where therapists could ‘gather the knowledge of that many disciplines to support a family’, which another therapist (T03) also described the service as a ‘brain trust’. This source of information for therapists was reported to provide therapists with opportunities for upskilling and peer learning. Caregivers also reported benefits of the transdisciplinary approach: . . . basically give that holistic approach where everyone could communicate together and . . . have suggestions and input into each of the sessions in each [discipline] . . . staff will also have meetings together . . . it’s a whole team, they work together to support [my son], which has been excellent. (C02)
Child-centred approach (M2)
Adopting and demonstrating a child-centred approach was a key mechanism identified by participants, influencing how therapists delivered their services. Child-centred approach referred to therapists considering the child’s and family’s needs (M2.1) and adapting service provision in the child’s best interests (M2.2) to achieve the best therapy outcomes.
Therapists were mindful of the child’s interests and preferences during sessions (M2.1) and tailored the interventions to incorporate the child’s areas of interest to increase engagement in sessions (M2.2). For example, one therapist who knew that the child enjoyed playing Minecraft included Minecraft characters and food in the session. The caregiver reported that the therapist also took time to have conversations with her child about his interests in computers and gaming and commented that this helped with rapport building.
Therapists often considered family capacity and readiness for therapy when developing the child’s therapy plan and would tailor the programme to suit the family’s current level of capacity and involvement in therapy: . . . it can get to the point, trying to increase the parents’ capacity, and they just aren’t ready for that. So being realistic as well, and not bombarding them with too much, but they do get quite a lot of support. (T04)
Therapists also reported accounting for caregivers’ understanding of and experience with mealtime intervention (M2.1) when providing caregiver education and adapted their communication style based on caregiver preferences and learning style to ensure effective communication of ideas. One caregiver (C01) reported that the service therapist always gave clear explanations and ‘lays it out really simple for [her]’ so that it was easier for her to understand the purpose of the programme and what she was doing with the home strategies. Several therapists also shared caregiver coaching processes, and how they built caregiver confidence in implementing home-strategies by modelling strategies in session and providing feedback on their performance.
Therapists selected the service location based on the child’s current abilities, routines and goals to ensure that the child received services in the most appropriate environment (M2.2). One therapist (T09) mentioned that ‘all [her] intervention sessions were at home, because that’s the environment the kids are eating in and it’s very consistent’. Some therapists also reflected that conducting home sessions compelled caregivers to be present and involved in sessions and provided caregivers with opportunities to practice taught strategies in their natural home environment. Therapists also adapted therapy sessions and recommendations based on the amount of available funding. For example, a therapist chose to tape together phone books to make a footrest for a child whose family was unable to afford a specialised chair for mealtimes.
Managing caregiver expectations (M3)
Managing caregiver expectations was identified as a mechanism, which facilitated the way families engaged in the service. Several therapists reported that caregivers may have unrealistic expectations of the mealtime service and their child’s abilities, which contributed to a perception of a lack of progress in caregivers. Therapists provided caregiver education (M3.1) early to ensure that families were aware of what was realistic for their child’s mealtimes, to set ‘reasonable’ and ‘attainable’ goals as therapy is a ‘slow process’. One therapist (T06) reported that she would re-frame caregiver’s unrealistic perceptions of ‘success’ in therapy by explaining the steps involved to achieve their desired goals and that achieving each step is considered a success: So, I do try to set up that expectation fairly early on. If I’ve met a new family and I’m working on a mealtime goal, just letting them know that it’s going to be slow. It’s going to happen, but we do a lot of . . . goal revision that I can show them, ‘Hey look, you know, I’ve actually tried three new foods’ which that’s a wonderful achievement. But just making sure they’ve got those really good expectations. (T03)
A caregiver (C04) reported that she appreciated how therapists did not ‘sugar-coat’ the explanation of the therapy process during the initial consultation, and instead helped her to understand that improvements with mealtime could potentially take years.
One therapist (T08) also mentioned the importance of goal setting and revising goals with caregivers in the early stages of therapy (M3.2), as caregiver’s perspectives and expectations of the service change with more knowledge. Goals were often streamlined into achievable ‘[specific, measurable, attainable, realistic, and timely] goals’ after caregivers have reviewed assessment results and have identified with the therapists the specific skills their child needs to work on to achieve the long-term goals.
Outcomes
Two outcome themes including impact on the child (O1) and impact on the caregiver (O2) were identified.
Impact on the child (O1)
This theme captured outcomes directly related to the child and included developing readiness for mealtimes (O1.1), increased food acceptance (O1.2) and changes in mealtime behaviour (O1.3).
Developing readiness for mealtimes (O1.1) referred to skill development in domains such as oral-motor, gross motor and respiratory control. Therapists emphasised the importance of readiness as a foundation for self-feeding, which can impact on the child’s nutritional intake and growth. Several therapists reported that oral-motor skill development and increase in respiratory control lowered the child’s risk of choking on food and ensured their safety during mealtimes.
Increased food acceptance (O1.2) referred to children increasing tolerance of non-preferred food, and overall food intake and variety. One caregiver (C05), whose child had been accessing the service for 6 months reported that her child has ‘gone from not eating some things’ to ‘actually eating things and giving it a try’. Another caregiver (C02), whose child had been accessing the service for a year, also reported that their child is now comfortable being around non-preferred foods and increased food acceptance has reduced the frequency of meltdowns for their child: [My son has] got quite significant sensory issues when it comes to food, where he sort of becomes unwell, or starts yelling that it smells . . . Anything that he didn’t like, got on him or he touched it, it would trigger a meltdown. So now he’s not doing that that much. (C02)
Both therapists and caregivers observed positive changes in mealtime behaviour (O1.3), including requests for non-preferred foods, increased ability to communicate food refusal appropriately and reduced frequency of meltdowns. Therapists also reported an increase in exposure to different foods, developing positive perceptions and interactions with food.
Impact on the caregiver (O2)
This theme captured outcomes including changes in caregiver perception (O2.1) and reduced family stress around mealtimes (O2.2).
Caregiver perception (O2.1) referred to the caregiver’s understanding of their child’s mealtime behaviours and their expectations of the mealtime programme. Caregivers discovered that mealtimes are complex and formed realistic expectations of the service over time. Therapists commented that caregivers’ acknowledgement of ‘not having instant changes’ made a significant difference to the way they viewed progress. One caregiver (C06) reported she started to celebrate small successes after accepting that therapy is a ‘long process’. Other caregivers recognised small actions such as taking a bite of previously avoided food or touching non-preferred food to be significant gains for their child.
A therapist (T07) reported that altering caregiver perceptions also alleviated family stress around mealtimes (O2.2) as ‘[caregivers] knowing that what they’re doing is enough’. Caregivers highlighted that reassurance from therapists around their child’s diet helped to reduce their anxiety about their child’s nutrition intake. Lower frequency of meltdowns during mealtimes also contributed to reduced caregiver stress and development of a ‘harmonious environment’ at home. One caregiver (C05) described the difference in her mealtime experience after the mealtime service: There was a lot of fights going on in the house, just getting them to try to eat . . . I don’t have that stress anymore . . . it’s much more pleasant, sitting at a table, than it ever has been. (C05)
Context–mechanism–outcome combinations
The contexts, mechanisms and outcomes identified were closely interlinked. Figure 2 illustrates the relationship between the contexts, mechanisms and outcomes. Therapists provided (M3.1) and modified caregiver education to the families needs (M2.1), and set achievable goals (M3.2) by considering the autistic child’s challenges and characteristics (C1.2) and their family capacity (C2.1), leading to two outcomes. These were changes in caregiver perception (O2.1) and reduced family stress around mealtimes (O2.2). Due to the complexity of characteristics and challenges faced by autistic children during mealtimes (C1.2), therapists communicated closely with each other (M1.1) and contributed their expertise to service delivery (M1.2), producing the outcomes of developed readiness for mealtime (O1.1), increased food acceptance (O1.2) and positive changes in behaviour (O1.3). Therapist accounted for the child’s and family’s needs (M2.1), including the child’s interest (C1.1), characteristics and challenges faced during mealtimes (C1.2), and adapted the service provision into the child’s best interest (M2.2), leading to three outcomes – developed readiness for mealtime (O1.1), increased food acceptance (O1.2) and positive changes in behaviour (O1.3).
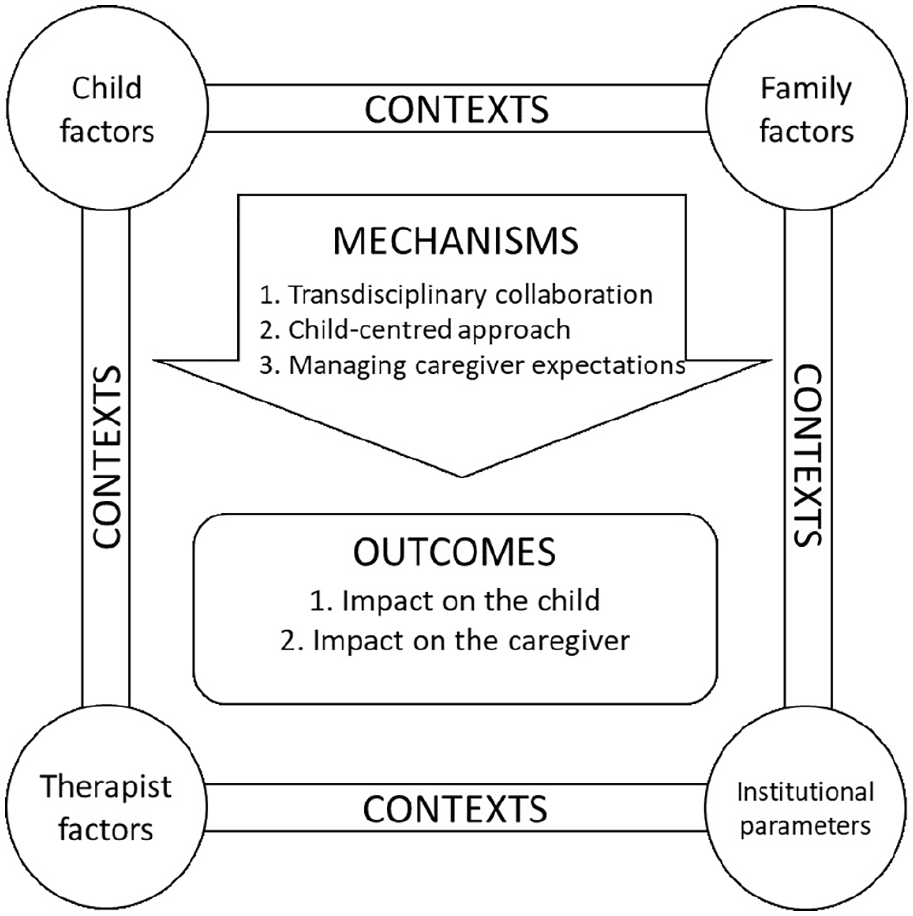
Relationship between the context, mechanism and outcome themes in the transdisciplinary mealtime programme.
Discussion
This study identified the contexts, mechanisms and outcomes operating within the mealtime service for autistic children. Factors related to the child and their needs, the families capacity and therapist and institutional parameters influenced the strategies that therapists implemented including transdisciplinary approaches, child-centred approaches and managing caregiver expectations. The combination of these contexts and mechanisms influenced outcomes of the service for both the child and their family.
Autistic children in this study experienced complex and multifaceted mealtime difficulties such as anxiety during mealtimes, sensory preferences, choking risks and mealtime behaviours of concern. These findings are consistent with previous research in this area (Ledford & Gast, 2006; Page et al., 2022; Provost et al., 2010). To address the complex and varied difficulties of autistic children, a transdisciplinary approach was undertaken by therapists in the mealtime service who worked collaboratively in a child-centred manner to effectively achieve mealtime goals. Under this approach, therapists contributed their unique discipline-specific expertise to the therapy process and were trained to perform duties extending beyond their traditional roles. Through role expansion, discipline-specific boundaries were blurred, resulting in a shared and holistic perspective. This perspective was found to allow the therapy team to develop comprehensive interventions to address complex and multifaceted mealtime difficulties that autistic children experienced. This approach was also reported by caregivers to streamline their access to services and disciplines. Such transdisciplinary approaches have been referred to as best practice for children with disabilities previously (Bowman et al., 2021), however, have been implemented to varying extents.
An interesting finding was most caregivers reported that their child required input from the dieticians who were part of the transdisciplinary mealtime service, to address concerns related to feeding difficulties such as fussy eating, playing an essential role in ensuring adequate nutrition. This finding is consistent with current literature estimating that 90% of autistic children may present with selective eating behaviour, which impact their dietary intake (Hyman et al., 2012). Several studies have also emphasised the value of dietetic consultations to provide advice on mealtime interventions and dietary goals for management to alleviate feeding difficulties for autistic children (Huxham et al., 2021; Zhu & Dalby-Payne, 2019). Dietetic services were previously not available through the Australian disability funding scheme, the National Disability Insurance Agency (NDIS, 2020) until recent developments in legislation in late 2019 that allowed children with disabilities to access dietetic services using their funding to meet mealtime needs (Dieticians Association of Australia, 2020). The findings of this study support the need for dieticians to have continued involvement in addressing mealtime difficulties of autistic children.
Our findings demonstrated that working with families was a key factor perceived to lead to clients’ achieving their desired mealtime outcomes. This finding aligns with evidence supporting the benefits of family-centred practice (Kokorelias et al., 2019). Furthermore, therapists in this study recognised that mealtimes were important for family functioning (Lawrence & Plisco, 2017). It can, therefore, be argued that working with families is important for autistic children to achieve their mealtime goals.
Despite therapists’ willingness to involve caregivers in mealtime strategies and interventions, findings from this study indicated that barriers to having caregivers involved in mealtime interventions included limited availability and receptiveness of caregivers to participate in mealtime interventions, and caregivers’ perception of a lack of progress in their child’s mealtime function. According to the caregivers interviewed, caregiver stress during mealtimes was a barrier to consistent participation in mealtime interventions. Specifically, findings from this study indicated that caregiver’s mental health and the family’s finances were two factors that contributed towards caregiver stress during mealtimes. This finding extends previous studies on caregiver stress and feeding issues in autistic children (Şahan et al., 2021; Suarez et al., 2014; Zlomke et al., 2020) by demonstrating that factors beyond the mealtime experience, and/or that are related to the autistic child, influence caregiver involvement in mealtime interventions.
As mentioned earlier, caregivers’ perception of a lack of progress in their child’s mealtime function was the second barrier to caregiver involvement in mealtime interventions. According to the therapists interviewed, this barrier could be due to unrealistic expectations of the therapy and outcomes. Therapists worked to manage these expectations through developing goals that were specific, measurable, attainable, relevant and timely for the child’s engagement and participation in mealtimes (Ogbeiwi, 2021).
Engaging in caregiver education early in the therapy process about their child’s function and engagement during mealtimes were also perceived to be helpful in setting realistic expectations. Providing caregivers’ insight into the level of involvement required for therapy and education around child development can increase active collaboration in goal setting, increasing perceived therapist competence and caregiver satisfaction (Forsingdal et al., 2014; Golnik et al., 2012; Rodger et al., 2012). Engaging in child-centred conversations to determine shared goals and language may also be valuable in improving mealtime outcomes, as families may have their own unique dynamics and needs (Smith & McQuade, 2021).
Therapists delivering the mealtime service adapted their interventions based on the child and their needs. Therapists identified the child’s interests and sought ways to incorporate these into service provision, reporting that such methods increased child engagement and rapport. These findings align with contemporary research that highlights the importance of identifying and harnessing a child’s interests and strengths in service provision (Jones et al., 2022; Mottron, 2017). While such ‘strengths-based’ approaches have been used to inform therapies associated with early intervention, education and employment (Jones et al., 2022; Mottron, 2017), this research suggests that designing a transdisciplinary mealtime service based on the strengths (and needs) of the child may be key to successful mealtime interventions.
Of note, while working with families and undertaking collaborative goal setting were identified by participants as an important mechanism contributing to the success of the mealtime services, collaborative goal setting can take time and potentially detract from time and funding allocated for therapy (Rodger et al., 2012). When funding is limited, caregivers may be hesitant to allocate funding to activities that do not provide direct therapy to the child. Educating families on the benefits of collaborative goal-setting and family-centred practice, alongside adequate funding allocations, may assist in overcoming these barriers.
This study has some limitations. First, the sample size for both groups was small with a greater number of therapists participating. Second, this study did not have a quantitative measure of mealtime outcomes, as this was a qualitative study. Due to the complexity of mealtimes, it is challenging to obtain quantifiable data and this provides a direction for future research. Third, the findings of this study indicated some differences in service provision for regional and metropolitan areas; however, the small number of participants from regional settings limits the interpretation of these results. Despite its limitations, this study is novel in its use of realist evaluation to evaluate a transdisciplinary mealtime service. This approach enables researchers and employers to identify the conditions needed to optimise the success of a transdisciplinary mealtime service. To conclude, this study provides empirical data demonstrating the complexity of delivering a transdisciplinary mealtime service to autistic children. A range of therapist, child and family factors influence how the mealtime service can be tailored to optimise outcomes for autistic children. Collaborative goal setting between therapists and families, combined with a transdisciplinary approach of delivering the mealtime service were perceived to be essential in optimising intervention outcomes for autistic children.
Supplemental Material
sj-docx-1-aut-10.1177_13623613221140717 – Supplemental material for Realist evaluation of a transdisciplinary mealtime management service for autistic children
Supplemental material, sj-docx-1-aut-10.1177_13623613221140717 for Realist evaluation of a transdisciplinary mealtime management service for autistic children by Wai Ting Chan, Christina Li Ern Chong, Zhao Min Goh, Chrystal Xin Xuan Ling, Ruyi Tong, Madeline Davey and Melissa H Black in Autism
Footnotes
Acknowledgements
We thank the participants for their contribution to this study. We are grateful to the Curtin School of Allied Health for the support of the research.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Ruyi Tong and Madeline Davey report a relationship with Therapy Focus that included employment.
Ethical approval
Ethical approval was obtained from the Curtin University Human Research Ethics committee (HRE2020-0769) in Perth, WA. All participants provided individual written informed consent prior to participating in the study. Caregivers who participated in interviews were provided with a US$10 retail gift voucher.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.