
Abstract
Early support should help autistic children lead flourishing lives. We sought to understand parents’ experiences of their children’s involvement in early intervention and associated research, through focus groups with 23 parents (of 22 children) enrolled in a university-affiliated service. Reflexive thematic analysis revealed four themes. Parents conveyed a strong sense of gratitude (Theme 1) arising from their perceptions of the importance of early intervention and feelings of having ‘hit the jackpot’ to secure access to the service from which they perceived their children ‘gained so much’. They valued the service and staff expertise which made them feel secure (Theme 2). University affiliation and the associated research also contributed to parents’ sense of safety, from perceived ‘accountability’ and ‘integrity’. Parents conveyed deep commitment to the service (Theme 3) but shared often-negative experiences as their child’s enrolment came to an end (Theme 4) and they expressed feelings of abandonment and disempowerment, being confronted with the reality of needing to secure next-stage support for their children and of perceived critical need for ‘conversion of research into practice’. These parents’ accounts offer insights into the benefits and ongoing challenges of achieving truly effective supports for autistic preschoolers and their families.
Lay abstract
Support for autistic children early in life should help them to lead flourishing lives. However, many of the early intervention programmes for young autistic children are time-consuming and costly for families. These programmes are also often conducted in settings that are not closely matched to real life. We spoke to 23 parents (of 22 autistic children) to understand their experiences of their children’s involvement in early intervention. Parents told us they were grateful for the opportunity, that they had ‘hit the jackpot’, and their children had ‘gained so much’ from the programme. They seemed to value the service because it made them feel safe and secure during an uncertain time in their children’s lives. Parents told us they trusted staff, felt that they weren’t ‘doing it alone’, and this ‘took that pressure off’ and helped them feel empowered. They also spoke of feelings of safety from being linked to the university research programme which offered ‘accountability’ and ‘integrity’. Parents’ comments showed a strong commitment to the early intervention model and staff – but also common feelings of abandonment and disempowerment as their child’s time with the programme came to an end and they went ‘back to the real world’ and needed to find new supports for their children. These parents’ insights should help to inform the design and delivery of community supports for preschool-aged autistic children and their families, which match the reality of their lived experiences.
Keywords
Many autistic children require early-life supports to facilitate learning and development, enable community participation and ultimately lead fulfilling and happy lives. Early intervention research often employs controlled efficacy trials – long considered the gold standard health programme evaluation method – seeking evidence about precisely which supports will give young autistic children the best chance in life (Vivanti et al., 2018). Yet, there is growing acknowledgement that programmes developed and evaluated in highly controlled environments may not translate readily to real-world settings (Nahmias et al., 2019). Furthermore, selection among the numerous available early intervention options is likely determined by cost, time commitment and delivery setting (Miller et al., 2012; Mire et al., 2017). One way to bridge what has been promoted as evidence-based versus pragmatically determined early intervention is through the conduct of community-based research, seeking to examine the effectiveness of interventions as delivered within settings where they will eventually be implemented (Vivanti et al., 2018), through partnership between formally trained researchers and key community stakeholders (e.g. service managers and providers).
Parents also are key stakeholders in the development, evaluation and implementation of effective early childhood supports. Yet, comparatively little attention has been given to their experiences with autism services (Wainer et al., 2017). This lack of research attention is notable given that parental perceptions and engagement are key to intervention effectiveness: – improved child and family outcomes, and better generalisation across learning contexts are achieved when parents are equal partners in early childhood support programmes (Brookman-Frazee et al., 2020; Wainer et al., 2017). Professional–parent partnership models aim to empower parents to be equal players in collaborations that support their child’s intervention, such that they can be effective and confident in teaching their child, managing daily routines and interacting with services for enduring improvements in family quality of life (Brookman-Frazee & Koegel, 2004; Heflinger et al., 1997; Resendez et al., 2000).
Existing research addressing parent perspectives has focused primarily on exploring their roles in mediating early intervention approaches. For example, in one such study, Freuler et al. (2014) interviewed 14 parents of children at increased likelihood of autism who had been randomised to a relationship-focused intervention (adapted responsive teaching (ART); n = 10) or advised to seek community intervention (n = 4). Participants reported benefits from education about available community services and what to expect from future interventions/service providers, and that the personal relationships built with professionals – both within community services and those associated with the research – were key to their investment in intervention and overall positive experience of support. Parents randomised to ART also reported relief in having access to an intervention without the responsibility of navigating community services, while those randomised to seek community intervention reported ‘stress and strain’ (p. 525) from having to identify and make decisions about appropriate services (despite receiving information, referrals and weekly check-in calls; Freuler et al., 2014).
In another study, Stahmer et al. (2017) spoke to 13 parents about their perspectives of the Improving Parents as Communication Teachers (Project ImPACT; Ingersoll & Dvortcsak, 2010) – a programme implemented through community-research partnership and focused on children with a formal autism diagnosis or showing early signs. Parents described strong buy-in to the intervention, in which community practitioners coached them to use naturalistic developmental and behavioural intervention (NDBI) strategies intended to build child’s social, language and play skills. Parents believed their involvement was key to their children’s learning outcomes, which fostered feelings of self-empowerment and reduced stress. Akin to Freuler et al. (2014), Stahmer et al. (2017) identified strong parent–professional relationships as critical to perceived programme success, with parents expressing the value of working with and learning from their coach. Parents also valued the approach of embedding intervention strategies within daily routines (rather than during isolated intervention sessions), but experienced difficulties generalising the use of the taught strategy from the intervention setting to the home environment. Other challenges identified by parents were a lack of flexibility in session scheduling, desire for longer session duration and limited opportunity to engage with other families accessing the programme.
Both studies highlight the value of engaging parents as key stakeholders within early childhood autism service provision and understanding how the extent and nature of their involvement can contribute to the ‘success’ of an intervention. They also offer valuable insight into the experiences of parents with recently or not-yet diagnosed children early in their journeys seeking and accessing targeted supports for autism, whether through research participation in controlled settings or community–research partnership. Limited research, however, has considered the experiences of families accessing centre-based early intervention services within community or university settings, especially those who may not be directly involved in delivering the intervention. Such, centre-based group supports reflect an emerging model often presented as the aspirational ideal, mirroring the early childhood education provision commonly accessed by families with young children in their local communities (e.g. Vivanti et al., 2019). In the current study, we sought to address this particular gap by examining parents’ perspectives of experiences of their autistic children’s year-long enrolments at a university-affiliated centre-based service.
Methods
Context
This research was conducted within a university-affiliated community children’s centre, which offers services for preschool-aged autistic children following a particular NDBI approach either within a regular childcare programme (i.e. alongside primarily non-autistic peers) or in autism-specific playrooms (i.e. exclusively among other autistic children). The autism-specific playrooms were located in a separate wing of the community children’s centre alongside a dedicated office for the onsite allied health team (including psychology, speech and occupational therapy) and certified training staff. Inclusive playrooms were located in the same building, among several regular childcare rooms that were accessible to families in the local community. Families accessed the autism intervention service through various pathways, including recommendation from healthcare professionals, local autism information and/or diagnostic services, and local word-of-mouth and self-referral. The service was initially funded by the Australian Government Department of Social Services, such that fees to attend the service were substantially subsidised (with parents contributing the cost of childcare and intervention costs covered by the government grant). From 2017, the centre transitioned to a new funding model (the National Disability Insurance Scheme (NDIS) 1 ), whereby parents could apply for funding towards the cost of intervention, while continuing to self-fund childcare fees as usual.
Families attending the service are routinely invited to participate in research to evaluate the feasible implementation and effectiveness of the NDBI programme, delivered across autism-specific and inclusive settings. On an average day, up to 10 autistic children attended each of the autism-specific playrooms, while 1–3 autistic children attend several inclusive playrooms with an average of 12 non-autistic children. In each setting, autistic children typically attend 3 days per week (for between 5 and 8 h) and there is a 1:4 staff-to-child ratio. One certified therapist is trained to deliver the intervention within each of the autism-specific and inclusive playrooms, while early childhood educators in each setting also attend training workshops and receive ongoing coaching from certified staff and the onsite allied health team. Each child/family is allocated a primary and secondary keyworker (usually a member of the allied health team or a playroom teacher) responsible for liaising with families, developing and reviewing children’s goals and modifying their individual programme as required. The same NDBI programme is implemented in both the autism-specific and inclusive settings, with the manualised programme implemented throughout daily routines and group activities that target children’s individual learning goals. Goals are developed collaboratively with parents following an initial assessment with each child, across relevant curriculum domains, including communication, play, social engagement and cognition. Intervention data are collected daily by staff in each playroom to monitor children’s goals and reviewed weekly by the child’s keyworker, to allow individualised support and adjustments to the programme as appropriate. Parent workshops were also conducted throughout the year which provided an overview of the intervention approach and strategies, as well as education around common topics such as toileting, sleep, mealtimes and behaviour management.
Participants
Parents invited to participate in the current study had a young autistic child enrolled at the service between 2015 and 2019 and had participated in associated research evaluating the manualised NDBI delivered within the inclusive and autism-specific settings. Among 80 eligible families contacted, 38 (48%) expressed interest and 23 parents/caregivers (of 22 children; 29%) participated in focus groups held in 2019. Participants were predominantly mothers, almost all reported some university qualification and family income ranged from <AU$25,000 to >AU$115,000 (see Table 1). Many self-identified as culturally/linguistically diverse, with 35% of Central or South East Asian ethnicity, and 26% reporting speaking a language other than English at home.
Sociodemographic characteristics of participating parents.

Participants’ children (16 male, 6 female) had typically attended 3 days per week across one school year, enrolled in either the autism-specific (n = 14) or inclusive (n = 8) settings. Table 2 shows that children varied in age and developmental/communicative abilities at service intake, with moderate- to high-level autistic features.
Characteristics of autistic children of participating parents, at intake into the intervention programme.
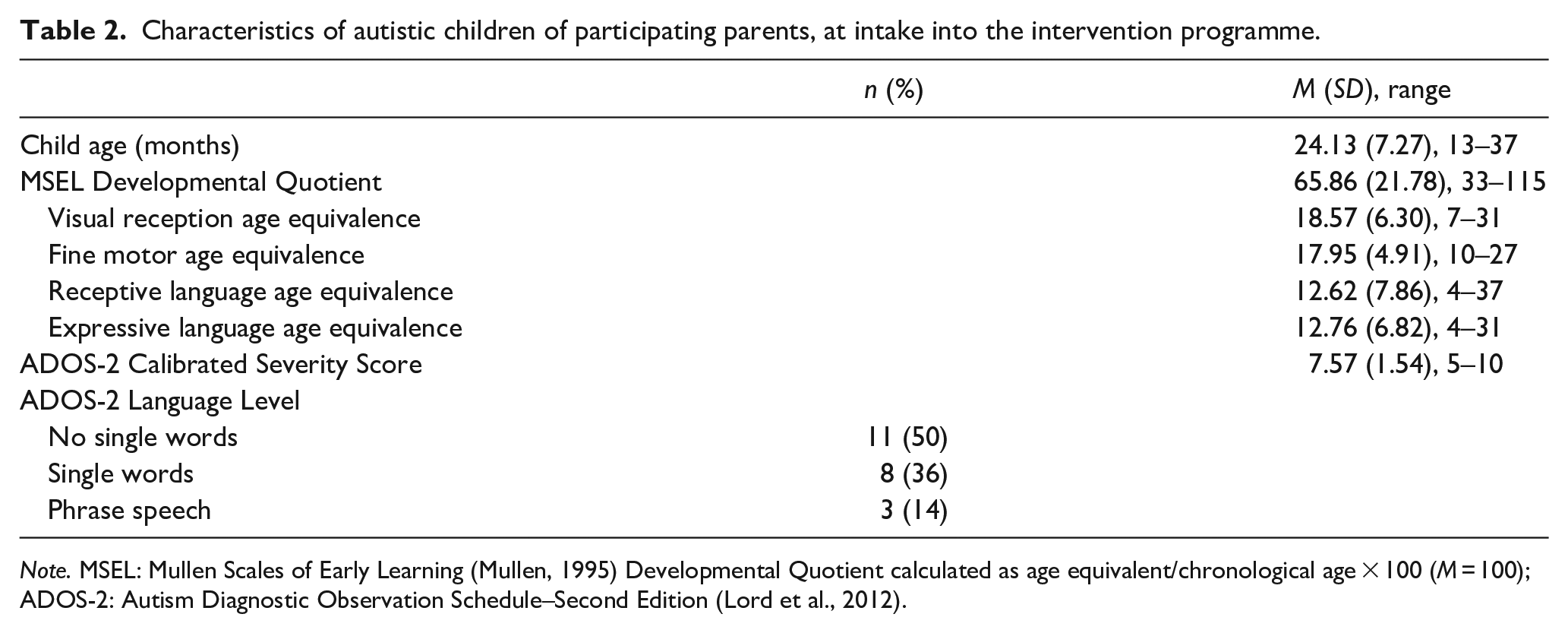
Note. MSEL: Mullen Scales of Early Learning (Mullen, 1995) Developmental Quotient calculated as age equivalent/chronological age × 100 (M = 100); ADOS-2: Autism Diagnostic Observation Schedule–Second Edition (Lord et al., 2012).
Procedure
Ethical approval for this qualitative study was obtained from La Trobe University Human Ethics Committee (Reference Number: HEC18514) and participants provided signed informed consent for participation (including audio-recording and verbatim transcription), as well as access to data from assessments completed when their children attended the service (e.g. Mullen Scales of Early Learning (Mullen, 1995); Autism Diagnostic Observation Schedule–Second Edition (ADOS-2; Lord et al., 2012); see Table 2). Four in-person focus groups were conducted at the centre, and two via online web conferencing, with one further individual telephone interview conducted with a participant who needed to leave their focus group session early. Each session included two facilitators and from two to nine parents. The lead facilitators were neither affiliated with the centre nor known to the participating parents. Facilitators introduced the project, obtained verbal confirmation of consent and posed a series of open-ended questions about parents’ experiences of the centre-based service, perceived impact on their child’s development and well-being, and their experiences of associated research participation. Parents were sent a written topic guide in advance and facilitators encouraged discussion, including helping to structure the conversation, support equitable participation and offer summaries to ensure accurate interpretation.
Data analysis
We followed Braun and Clarke’s (2006, 2019) method for reflexive thematic analysis, within a critical realist framework (Willig, 2013): acknowledging that everyone has subjective experiences (the empirical); that an objective reality exists outside of direct experience (the actual) and that causal mechanisms lie between and within these (the real). Themes were identified using an inductive (bottom-up) approach (i.e. without integrating the themes within any pre-existing coding schemes or preconceptions of the researchers) to identify patterned meanings within the dataset. Our team members brought a range of perspectives and professional expertise to bear on the analysis, including from psychology/public health (C.A.B. and K.H.), educational psychology (E.P.) and speech–language pathology (T.I.). None identify as autistic, or as parents of autistic children.
The analytic process began during the interview phase, with the lead facilitators meeting regularly to debrief and discuss patterns in parents’ responses, including potential codes and analytic ‘noticings’. Upon transcription, three of the four researchers (including the two lead facilitators) immersed themselves in the data reading and re-reading transcripts, taking reflexive notes on striking and recurring observations and assigning codes (line-by-line) to each transcript. Our team conferred regularly to discuss preliminary codes and especially when reviewing codes and grouping them together to form coherent themes and subthemes. The team liaised several times to review the thematic map and supporting quotations, focusing on semantic features of the data (i.e. staying close to parents’ own language), highlighting contradictory perspectives within and between themes, resolving discrepancies and deciding on final themes and subthemes. The analytic approach was one in which themes and subthemes are seen not to ‘emerge’ on their own but are identified through systematic engagement with the data combined with an active and deeply reflexive approach to analysis, influenced by the researchers’ own aims, positionalities and interpretation of the data. Participating parents also had the opportunity to provide feedback on the results as part of the member-checking process and to be acknowledged as named contributors (with 9 agreeing to be named and 13 electing to remain anonymous).
Community involvement
Autistic adults or their family members were not involved in the design or conduct of this study. Clinicians and educators involved in service management and programme delivery contributed to study development and design. This included individuals being named on a successful funding application that supported external collaborator involvement, reimbursement for parents’ focus group participation time and catering at in-person sessions. Service staff also provided input into, and gave feedback on, draft focus group schedules.
Results
As shown in Figure 1, we identified four themes, each with several subthemes, from parents’ data. We consider these in turn, with illustrative quotes.

Parents’ views on experiences of participation in university-affiliated early intervention service and associated research: themes and subthemes.
Theme 1: grateful for the opportunity
Parents overwhelmingly agreed that ‘early intervention makes a big difference to kids on the spectrum’ (Subtheme 1.1). They wanted their children to show ‘as much independence as possible’, to be able to ‘express their wants and needs’ through spoken language (especially for non-speaking children) and ‘to learn and thrive when they are older’. They perceived early intervention as critical to achieving these goals – important ‘to give it to them now’. Without early intervention, parents were worried their children would ‘slip through the cracks’ or ‘miss the boat’.
Precisely because ‘early intervention’s so important’, parents expressed that securing a place in the programme felt like they had ‘hit the jackpot’ (Subtheme 1.2). They were well aware of ‘not many choices out there’ for early intervention programmes in their communities – ‘there’s really not many places where you can get a really focused 15 to 20 hours [per week]’ – and the few available programmes were described as ‘hugely expensive’ and therefore prohibitive: ‘we did find somewhere that’s right near our house, but it was AUD$75,000 a year’. Feeling fortunate – ‘we just got a lottery ticket, big time’ – was further validated by the perception that ‘[the centre] is just so hard to get into’. One participant said, ‘I just contacted the centre and put his name down without hope because I know that there’s a long waiting list’.
Across the intervention programme, there were parents who reported more reasons to feel grateful for the opportunity. One key reason was that their children had ‘gained so much’ (Subtheme 1.3). According to some parents, improvements were rapid – ‘within about two weeks, he was looking’ – while other children ‘took a while to settle in’, showing progress that ‘was very slow, very steady’. Sometimes, parents reported gains towards specific goals: ‘the most important thing is to get the goals’; ‘she went from the non-verbal to verbal’. The gains that meant the most to parents, however, tended to be much broader, often relating to their child’s happiness, ‘understanding the enjoyment of interacting with people’ and their ability to do ‘everyday tasks’, such as ‘putting on their sunscreen’ and ‘walk[ing] into the shop holding your hand’ – ‘basic things like that’.
Yet, such progress was not the perceived experience for all parents, as not all children progressed towards their specific goals. Some children still had ‘no words at all just yet’ and had made ‘very little’ improvement: ‘we had the last report from his keyworker and it turns out that he did not achieve the goals that he is supposed to achieve’. Even where parents reported seeing ‘huge’ gains, not all attributed these to the programme itself: ‘I know it’s hard because you’ll never know what they would have been if they hadn’t come. How much of that would have happened anyway?’ Despite this handful of dissenting experiences, parents’ overall sentiments towards the programme and centre were unanimously positive.
Theme 2: safety and security during an uncertain time
Another key reason for parents’ appreciation was that the programme provided the safety and security they needed during a particularly uncertain time: ‘by making my child safe and secure, it made my family safe and secure’. The trust that parents expressed in the caring, respectful staff (Subtheme 2.1) who supported their children was central to this sentiment, with parents describing the ‘amazing, phenomenal’ support and care that staff provided: ‘They were incredible – they cared, and they took on everything that they could to support him’. They felt that staff had developed deep connections with their children (‘they loved him for him’), were ‘so respectful’ of their children and their needs (‘I just felt like he was treated I don’t know, the way that he should be, like a real person that has their own needs and wants’) and accepting of their family (‘it is such a warm place to be, there was just no judgment’). Parents witnessed and felt greatly reassured by the effects of the ‘amazing amounts of love’ for their children: ‘[child] feels like it’s a second home . . . even driving to the centre, he recognises where we are and he’s not crying. That’s a positive thing for me, to know that he’s happy coming here’.
Parents’ stresses and strains were also eased immensely by the support of empathetic professionals and other parents, resulting in feeling like ‘I wasn’t doing it alone’ (Subtheme 2.2), and that ‘all the staff in that room became [child’s] champion . . . they were so invested’, so much so that ‘they almost become like your extended family’. They felt comforted knowing that there were other parents ‘in the same boat’ with whom they were ‘creating a community, not connected by blood but by the same situation and experiences’. This support was also practical: ‘like the logistics of NDIS, the logistics of networking for therapists, the feedback from different providers’. For parents, drawing on others’ experiences mattered: ‘That’s the best help you could get . . . you don’t have to ask the help of Google now’. That said, those with children enrolled in the inclusive setting specifically felt detached from parents of the neurotypical children: ‘I really felt like it was me and them’.
Parents’ reassurance was also attributable to their deep trust in experts and expertise (Subtheme 2.3): ‘being linked to a university is a big tick’. Parents expressed trust in the university because being ‘couched in the university’ meant the staff were ‘educated in autism’, and therefore ‘aware of children’s needs and helped to support those needs . . . rather than just the regular day carers that don’t have a lot of knowledge about kids on the spectrum’. This institutional trust was unwavering: ‘I always rely on their feedback because they’re professionals . . . So, I believe them’. Parents further described feeling ‘a lot of safety and security’ in the knowledge that ‘there is research ongoing in this bigger centre’ because it ‘makes people more accountable’ and ‘helps maintain the integrity of the program’. They also felt that being involved in research added trustworthiness to the programme and meant better support for their children: ‘I really liked that the research drove the intervention in a way that I knew that they wouldn’t let [child] down because they needed to accumulate research’.
Parents’ deep connections with the staff and other parents, and their strong belief in the expertise and reputation of the centre and university, allowed them to ‘feel safe in the knowledge that she’s getting what she needs’, which, ultimately, ‘took that pressure off’ (Subtheme 2.4): ‘They did some of the hard work for us . . . ’. This reduced parents’ anxiety and allowing them to engage in other life tasks: ‘knowing there was a whole team who was also interested [in child] and concerned about his progress and development allowed me to just relax a little bit, be a mum to my other child, a wife, a student’. One mother observed that her family’s involvement in the programme ‘allowed me to have another child, without absolutely going to pieces’.
Consequently, parents felt empowered during their time in the programme (Subtheme 2.5). The safety of the programme helped them to ‘feel confident as a parent’ and gave them the time and space. With this additional space, they could deal with their child’s diagnosis – ‘I went into overdrive, I didn’t sleep, I would read everything that I could’ – and, importantly, begin to understand their child: ‘I think him being here took a load off while we got to know him and understand what autism really is, and now we’re all the more better for it’. They also gained a better understanding of what good support meant for their child: ‘one thing that I feel like we’ve gotten out of this is knowing what our children deserve and what – the type of care that they deserve’. Some parents also reflected on how they developed ‘trust in ourselves as well’ and were helped to ‘make you really think about things . . . because [the program] asks a lot of questions about what they can and can’t do, it really makes you analyse what it is he can and can’t do . . . [also] how we’re responding to him as parents of an autistic child, what are our coping mechanisms’.
Theme 3: allegiance to the model, staff and research
Parents’ reflections illustrated the deep commitment they had developed to the early intervention model, the educators and the research. This commitment was most evident in the language parents used to describe their own and their children’s experiences, demonstrating that they were strongly wedded to the NDBI approach (Subtheme 3.1). Reiterating some expressions used in the NDBI, they spoke of how the programme had given their child ‘such a great head start’, ‘put those building blocks in place’ and ‘built some really solid foundations for [child] to understand group learning and the enjoyment that he can find with adults and children’. According to parents, developing these skills ‘set him up in the mainstream now’ and meant that ‘he left here with a taste of learning which just kind of opened him up that there’s a world around you’. As one parent explained, All of the therapists and educators in that group would all say to us that, ‘oh you can tell she’s had early intervention’. They would do group work, and [child] knew how to sit down in a group, and how to put her bag away . . . and how to follow instructions. She had already learnt that here. She went into this group, I feel, a step ahead.
Parents did not tend to report many details of the intervention model nor what was involved. Rather, their responses often included broad emotive descriptions that conveyed a strong faith in the methods and in those delivering them (Subtheme 3.2): ‘I used to think it was wonderful magic that went on in [the centre] to produce the tremendous change in [child]’, ‘there is no magic bullet, there is no special diet, we just have to be dedicated and love him and make him happy. Because that’s what they did in there, and he made such great progress’. Parents highlighted that ‘you can really depend on the evidence there’, which was ‘so important when there’s so much rubbish out there about autism’, and this knowledge helped them to ‘learn what best practice is’ (see also Subtheme 2.3). Not all parents, however, were steadfast to the model. Some explicitly emphasised that it was too complicated and that they did not understand exactly what was involved – ‘It’s a beautiful model, but when it started to get into that little bit more detailed ways to go about doing things, I got a bit lost after a while’ – while a few parents’ had come to believe that ‘the [NDBI] model is not the best approach for [my child]’.
Parents’ allegiance to the programme was also demonstrated by their staunch defence of the educators, who needed more support (Subtheme 3.3). Parents were overwhelmingly positive about the educators and staff at the centre (see also Subtheme 2.1). Nevertheless, many parents also stressed that the educators, especially those working in the inclusive setting, needed additional assistance from certified therapists and trainers to implement the programme. Parents whose children attended this setting described how there were ‘a few concerns in our room’ related to a lack of staff stability. Such instability was felt to be linked to high turnover: ‘I can’t remember who we had at first, and then I was devastated when she left and then we got a new one and she seemed really switched on, and then she stayed a really short time, so that was stressful’. Instability in staffing was also perceived by some parents to be due to inconsistent expertise: ‘we were in a room that hadn’t done the program before, so everyone was new to it. So, no-one really knew what they were doing’. They felt that the educators ‘needed a lot more support in the room’ from NDBI certified training staff: ‘even though they’re amazing, they get stuck and then they’re stuck. If there’s no-one coming in, then they’re just stuck’. Another parent explained that this help was not forthcoming, in the case of her child: ‘there were whole fortnights or three-week periods where not one specialist went into that room. Where I thought he was getting maybe a couple of hours a week, he was getting none’.
Theme 4: back to the real world
The three largely positive themes presented so far focused on the period during which parents and their children received support at the centre. The final theme related to parents’ often-negative experiences of navigating the transition out from the programme and into services in their own communities.
Parents spoke of having found this ‘amazing’ programme – whether through serendipity or great determination – which had provided security for themselves, their children and their families during a period of much uncertainty. While parents understood why programme placements were so short-lived ( ‘because the funds were exhausted, and they would like to give other kids on the waiting list a chance’), their responses nevertheless suggested they felt abandoned (Subtheme 4.1) when the programme ceased: ‘You’re no longer eligible to contribute to the research, and they drop you after that . . . off you go to the next thing’. They were deeply disappointed in having to leave – ‘I wish he could stay there for longer, but he can’t’; ‘we hated having to leave’ – and reported a considerable amount of ‘grief’ associated with the loss of support: ‘our hearts were broken’.
Parents felt that the programme had set ‘really high expectations’ in terms of ‘research and evidence-based practices’ and the ‘fantastic’ support they had received: ‘I assumed that that is the norm after coming to [the centre] because everything there was research-based and evidence-based’. Unfortunately, this was not their subsequent experience of other centres, ‘out there’ in the real world. As one parent put it, ‘nowhere is like here’. They described how ‘other centres don’t have the skills/knowledge to support us around autism, they don’t do the research, they don’t understand evidence-based practices’.
Ultimately, transition out of the centre and into local communities meant that the ‘onus is back on you’, ‘Here, they look after you. Once you’re out of the special, lovely cocoon, you’re on your own. You want something to happen, you pay for it yourself, you organise it yourself, otherwise nothing happens’. This transition appeared to result in parents’ feeling ‘really confused’ and suggested that their initial feelings of empowerment appeared not to translate to life after the programme (Subtheme 4.2): ‘one of the things the university was very good at was empowering us as a family. However, we found that once we moved on from there, we really struggled to find our feet’. With scaffolds and supports removed, it was ‘a total struggle’: ‘you’re just not sure whether you’re doing the right thing or not’. Parents described being unsure what type of intensive early intervention they should be doing – ‘should I be doing ABA [applied behaviour analysis], should I be doing ESDM [Early Start Denver Model]?’ – what allied health support (‘speech and OT [occupational therapy]’) they should be engaging and whether they should be ‘picking between mainstream or autism-specific for schooling’. As one parent put it, ‘I don’t know what the answer is’. They reported ‘just second-guessing yourself all of the time’ and had also come to realise there was widespread lack of autism knowledge in the community: ‘we’ll have to educate [people] for the rest of our lives [about autism]’, ‘constantly educating and informing and advocating’.
They also (re-)experienced the precarity around funding for their children’s support (Subtheme 4.3), which brought ‘extra stress for us as parents’. Some noted having submitted applications for NDIS funding but accepted they might need ‘to continue to self-fund’ ‘very expensive’ support for their child. Some felt ‘lucky that we got NDIS funding two years now, after going through two reviews’, while others still waited months for application outcomes (‘we had to ask the local MP [Member of Parliament] again for help’) which added ‘real burden’ to an already stressful, uncertain period. Having seen – and been deeply disappointed by – the services available after leaving the centre, parents reported anxiously trying to recreate the programme locally: it was a big transition for us out of [the city] back to home. We were starting from scratch and there’s no centres here that could emulate [it] so then it became a work in progress trying to find a way to build our own [centre]. While we can’t replicate [centre], that’s effectively what we’ve tried to do.
Parents reported wanting to see more conversion of research into practice (Subtheme 4.4) and to make the programme real for their own and others’ children in their local communities. They wanted to know ‘what happens at the end of it all?’, ‘when does the research convert to functional practice within the community, that is funded by the government for all kids on the spectrum everywhere?’
Discussion
We addressed the knowledge gap around parents’ perceptions of early intervention for their autistic pre-schoolers by examining their views and experiences of engagement with a university-affiliated, community children’s centre – offering a group-based NDBI. Within focus groups, we heard parents’ gratitude for the opportunity provided through the offer of, and subsequent participation in, this service. Parents expressed a strong sense of safety and security during their child’s enrolment and, perhaps as a result, were steadfastly committed to centre staff, the NDBI and the associated research programme. Parents also highlighted the time-limited nature of this supportive experience – that the sense of empowerment built with the programme did not endure following transition to other services. These accounts offer insights into the benefits and ongoing challenges of achieving truly effective community supports for autistic pre-schoolers and their families.
Whether parents happened upon or deliberately sought out the service, securing enrolment brought reprieve from the effort and anxiety otherwise associated with seeking reputable, affordable community autism services, and from sole responsibility of caring for their young autistic child. This is consistent with findings from other studies of parents’ experiences of advocating for their children around the time of diagnosis, including to initiate appropriate supports (e.g. Boshoff et al., 2018; Locke et al., 2020). Parents of autistic children repeatedly report increased stress compared to parents of children with other conditions (e.g. Ingersoll & Hambrick, 2011; Mathew et al., 2019), with experiences around seeking a timely diagnosis and gaining rapid access to services key contributors to this stress (Boshoff et al., 2018). A common experience for parents in the current study was of having recently secured a diagnosis around the time of their child’s service enrolment, and they expressed clear gratitude for, and relief from, engagement with this first substantive avenue of autism-specific support – a timely, year-long placement with a programme perceived as trustworthy and evidence-based.
Parents reported strong allegiance to and trust in the service and its staff, in stark contrast to other accounts reported in the literature. Rather, past research suggests parents’ early concerns for their child are often dismissed by professionals, necessitating strong self-advocacy and contact with multiple providers on the early journey to securing a diagnosis and specialised support (e.g. Bent et al., 2020; Crane et al., 2018). Negative experiences around this time have been described as contributing to ongoing professional mistrust (Boshoff et al., 2018; Sperry et al., 1999), and several factors appear to have contributed to a sense of trust in the current sample. First, engagement with the intervention service was designed to mirror the experience of many families who access creche/kindergarten services for young children without disabilities. These parents felt safe and secure leaving their young autistic children at the centre, several days per week, allowing time for their other personal or family activities. Second, perceived ‘trustworthiness’ likely also came from university affiliation of the service and associated research programme. Existing studies suggest that the degree to which a programme is seen as ‘evidence-based’ contributes to parents’ initial selection of services for their autistic children (Bowker et al., 2011; Wilson et al., 2018) and, indeed, programmes delivered through university–hospital partnership have reported larger gains for children’s cognitive abilities and adaptive behaviours, on average, than other community-based programmes (Nahmias et al., 2019), perhaps contributing to likely perceived effectiveness.
Finally, parents in the current study indicated strong allegiance with the specific NDBI. Allegiance or ‘buy-in’ to an approach has previously been attributed to strong professional–parent relationships (Freuler et al., 2014), and the parent-mediated nature of certain programmes which involves parents actively in intervention delivery (i.e. learning strategies to promote child development and manage challenging behaviour, and how to implement these within daily routines (Stadnick et al., 2013; Stahmer et al., 2017). Parents here spoke directly of (and signalled indirectly) their strong trust in centre staff, and they used expressions associated with the NDBI. They did not give detailed descriptions of the NDBI, however, and some parents commented on not understanding the complexities of the model. Thus, it seems parents valued staff care for and acceptance of their children, and their sense of centre ‘trustworthiness’ fostered ‘buy-in’ to the NDBI, rather than vice versa. It is unsurprising that many parents expressed only cursory knowledge about the NDBI given the centre-based model encouraged parents to leave children in the educators’ care, unlike other approaches where psychoeducation or parent-mediated delivery are key programme components (e.g. Freuler et al., 2014; Stadnick et al.,2013, 2015; Stahmer et al., 2017).
Parents’ deep commitment to the programme was encouraging, but nevertheless brought difficulties when transitioning away from the centre to other services. Such challenges are not uncommon: many parents of young autistic children face substantial difficulties securing and maintaining access to care, even in high resource countries/communities (e.g. Boshoff et al., 2018). The standard of care and service provided through the research partnership examined here seemed to create an expectation that was unavailable or unattainable elsewhere. Interestingly, while the parents Freuler et al. (2014) interviewed, who had been randomised to receive intervention, similarly reported a sense of relief from relinquished responsibility for navigating community services, those randomised by Freuler et al. to seek community services reported ‘stress and strain’ at having to identify and make decisions about these – a burden which was not alleviated by regular ‘check-in calls’ by and referrals from research staff. These and the current findings highlight the critical difference between simply offering parents information/advice and building genuine empowerment to consider, make decisions about and navigate access to services in ways that transcend relationships with particular professionals/providers.
Combining intervention with centre-based care, which offers parents relief and respite, with psychoeducation and training which may build insights, skills and confidence (e.g. Minjarez et al., 2020), seems key to effectively supporting young autistic children. A service component focused on genuine parent empowerment may benefit families and children beyond what can be achieved through enrolment in child-focused programmes alone. Support as children transition between services, from dedicated outreach staff, may also better prepare parents to critically consider options, facilitate engagement once an appropriate service is identified and empower future navigation through services and funding as children grow (e.g. Olin et al., 2010). Furthermore, helping parents to build deep connections with others in similar circumstances – valued by many of the current participants, and highlighted as missed opportunities where service provision is individualised (Freuler et al., 2014; Stahmer et al., 2017) could also represent a highly effective, low-cost support.
Limitations and future directions
Our study is not without its limitations. First, since we focused on the experiences of parents of autistic children participating in a university-affiliated community children’s centre offering a manualised early intervention programme, we cannot be sure how their insights might reflect parents of children attending other services not affiliated with a university. Given evidence of better gains for children when community-based programmes are delivered through university–hospital partnerships (Nahmias et al., 2019), there may be some differences in the experiences of the parents involved in those programmes compared to those reported here. Future studies will need to examine specifically the experiences of parents whose young autistic children attend community-based intervention programmes. Second, while this study included parents whose children were enrolled in either an inclusive or autism-specific playroom implementing the same NDBI programme, it was not designed to directly compare the experiences of parents across settings nor was such a comparison possible because focus groups included parents from both settings. That said, our analysis revealed some important distinctions between the settings that may be worthy of future investigation. Third, while our parents identified with a range of cultural and linguistic communities, they were nevertheless highly educated, and so it is also unclear how the experiences of parents from groups often underrepresented in research (i.e. such as those experiencing socioeconomic adversity or without English-language proficiency) – might overlap with those of parents in this study (Galpin et al., 2018). Finally, the insights from this study were elicited exclusively from parents, and not professionals and service providers, who will have valuable, alternative perspectives. We intend to address professionals’ views and experiences separately, with interviews and focus groups conducted with intervention staff, management and researchers, to gain a fuller understanding of how key stakeholders can work together as equal partners to deliver the most effective early childhood supports for autistic children and their families.
Footnotes
Acknowledgements
We thank the parents/families for their participation and acknowledge the following individuals who elected to be named: Julia Baird, Rachkrit Chaijaroenswad, Bao Hiep Ly, Joanna Lanaghan, Zhienna Mansfield, Angela Mcilroy, Sarah McKenzie, Sarah Ryan, Jing Su, Quynh Trieu and Yimin Wang. We also thank Cherie Green, Jodie Smith and all staff at the intervention centre for facilitating contact with eligible families and onsite focus group conduct.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Catherine Bent and Kristelle Hudry have previously received salary to conduct research associated with the service provider that is the subject of this study. Elizabeth Pellicano and Teresa Iacono have no conflicts of interest of which they are aware.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was from the La Trobe University Building Health Communities Research Focus Area. Elizabeth Pellicano is supported by an Australian Research Council Future Fellowship (FT190100077). The funders had no role in the study design, manuscript drafting or submission.