
Abstract
Measurement-based care is an approach to clinical care that involves systematically evaluating patient-reported outcomes to guide clinical decision making with a strong evidence base in the general population; however, its use in autism is limited. As autistic people are more likely to be diagnosed with psychiatric disorders (e.g. depression, anxiety) and to use psychiatric services (e.g. psychotherapy) than the general population, efforts to enhance clinical care for this population are critical. The current proof-of-concept study presents the development and pilot administration of an autism-adapted measurement-based care (MBC-AUT) system for psychotherapy designed for and with autistic people, as well as preliminary data on the feasibility, acceptability, benefits, and barriers to the adoption of the system for clients and clinicians. Findings from the first 18 youth and adult clients to use the system suggest that the MBC-AUT system is feasible and acceptable. Important benefits of the MBC-AUT system for clients and clinicians were identified through semi-structured interviews, and some barriers to the use of the MBC-AUT system were raised. Potential solutions are presented to address these barriers and to reduce the client and clinician burden. As autistic clients continue to seek psychological services, efforts to enhance the delivery and quality of psychotherapy for this population are essential.
Lay abstract
Autistic youth and adults are more likely to experience psychiatric symptoms (e.g. depression, anxiety) and to use psychiatric services than non-autistic people, yet research on evidence-based approaches to enhance psychiatric care for autistic people is limited. Measurement-based care is an evidence-based approach to psychotherapy that improves outcomes for clients, clinicians, and organizations by routinely administering and evaluating measures to clients. Despite this, research on measurement-based care systems for autistic clients is sparse. To address this gap, we developed an autism-adapted measurement-based care (MBC-AUT) system for and with autistic people and pilot tested the system in an outpatient psychiatry clinic to investigate the preliminary feasibility, acceptability, benefits, and barriers to this system for clients and clinicians. Findings suggested that the MBC-AUT system was a feasible and acceptable system for the first 18 autistic youth, their caregivers, and autistic adults to use the system. In semi-structured interviews, clients and clinicians discussed the benefits of the MBC-AUT system to various therapeutic processes, as well as several important barriers to the use of the system. We offer potential solutions to address these barriers and to reduce client and clinician burden, and propose future directions for this line of research to increase access to more autistic people. As autistic clients continue to seek psychological services amid social landscapes of increasing complexity (e.g. COVID-19 pandemic), efforts to enhance the delivery of psychotherapy for this population are critical.
Measurement-based care (MBC) is an evidence-based approach to clinical care that involves systematically evaluating patient-reported outcomes prior to and during clinical encounters to guide clinical decision making (Fortney et al., 2017; Lewis et al., 2019; Scott & Lewis, 2015). The MBC approach has been primarily tested in general psychiatric services (Bickman et al., 2011), and specifically in psychotherapy, MBC has been associated with direct benefits to clients (e.g. symptom improvement), clinicians (e.g. empirically-based decision making), and organizations/clinics (e.g. quality improvement efforts; Bickman et al., 2011; Carlier et al., 2012; Kearney et al., 2015). In particular, the personalized approach of MBC may be critical for improving clinical care and outcomes for heterogenous populations, including autistic 1 youth and adults. Despite the promise of MBC systems for autistic clients accessing mental health services, to our knowledge, no MBC system has ever been specifically developed both for and with autistic people, and the literature evaluating MBC in the autistic population is limited to a single study (McFayden et al., 2021). The current conceptual overview will discuss MBC (i.e. design, clinical use, benefits, challenges) in non-autistic and autistic clients, followed by a description of the design and initial implementation of the first MBC system designed for autistic clients (i.e. autism-adapted measurement-based care (MBC-AUT)), including data on initial feasibility and acceptability of MBC-AUT among clients and clinicians.
Autism is a neurodevelopmental disability characterized by social communication differences and the presence of restricted, repetitive behaviors and/or interests (American Psychiatric Association, 2022). Autistic youth and adults are more likely to experience depression (Hollocks et al., 2019; Hudson et al., 2019; Lai et al., 2019; Schwartzman et al., 2022), suicidal thoughts and behaviors (Blanchard et al., 2021; Hedley & Uljarević, 2018; O’Halloran et al., 2022), and anxiety (Hollocks et al., 2019; Lai et al., 2019; White et al., 2009) than the general population (Joshi et al., 2010; Mutluer et al., 2022). Relatedly, autistic people are more likely to use psychiatric services than non-autistic people (Narendorf et al., 2011). As autism is characterized by heterogeneity across people (Georgiades et al., 2013), it is likely that the personalized approach of MBC may be critical for guiding clinical care and improving outcomes. Although MBC is considered an evidence-based approach to psychotherapy in the general population (Fortney et al., 2017; Lewis et al., 2019; Scott & Lewis, 2015), its research base in autism is limited to a single study (McFayden et al., 2021). Furthermore, the prospective development, implementation, and evaluation of a MBC system designed for and with autistic people have not been conducted.
In the following sections, an overview of standard MBC in clinical services for non-autistic clients will be presented, followed by a review of the only study of standard MBC in autistic clients, to lay the foundation for developing a system for and with autistic clients in the present study.
MBC: Improving clinical services
A substantial gap between treatment outcomes in randomized controlled trials (RCTs) and routine mental health care settings has been frequently documented, with superior outcomes observed in controlled, experimental settings (Fortney et al., 2013; Roy-Byrne et al., 2010; Wang et al., 2003). Two components of RCTs that contribute to their enhanced efficacy include: (1) systematic measurement of symptom severity and other treatment factors (e.g. therapeutic alliance, demographic factors) and (2) adjusted treatment approaches when clients do not respond or progress (Fortney et al., 2017). To fill these gaps in routine mental health care settings, researchers and clinicians have emphasized the feasibility, acceptability, and utility of MBC (Aboraya et al., 2018; Fortney et al., 2017; Lewis et al., 2019; Scott & Lewis, 2015).
MBC is an approach that utilizes self- and/or proxy-report measures to monitor client symptomatology and treatment progress over time (de Beurs et al., 2011), and may resemble the process of obtaining vital sign measurements or routine laboratory tests in a medical setting. Additional benefits of MBC include the integration of data into patient care such that clinicians and clients work collaboratively to address symptom progression, focus on improving outcomes, and make decisions regarding treatment termination (Carlier et al., 2012). For clients, MBC promotes awareness and knowledge about their symptoms and diagnoses, thereby fostering a sense of power and collaboration in diagnostic decisions and treatment planning (Fortney et al., 2017). Importantly, MBC has been successfully applied in both adult and pediatric client populations (Bickman, 2008; Bickman et al., 2011). At the same time, barriers to MBC adoption and implementation in community mental health settings have been identified across the U.S., with continued efforts to close this research-to-practice gap (Kruk et al., 2017; Pincus et al., 2016). Although MBC has been established as an evidence-based approach to optimizing psychotherapy for non-autistic clients, limited research has been conducted on MBC with autistic clients. Thus, given that adaptations to standard-of-care mental health treatments are often necessary to maximize efficacy in autistic children and adults (see Bal et al., 2022; Brosnan & Adams, 2022; Cooper et al., 2018), additional work specifically examining MBC in autistic people is warranted to potentially determine the need for autism-specific modifications and protocols that optimize care delivery in this population.
MBC for autistic clients
Limited research on MBC systems with autistic clients has been conducted, which is surprising as autism prevalence rates are on the rise (Maenner et al., 2021), psychiatric disorders are commonly experienced by autistic people (Joshi et al., 2010), and treatment personalization is a preferred approach for this population (Georgiades et al., 2013; Sherer & Schreibman, 2005). Complicating matters, the majority of mental health providers report greater uncertainty in treating autistic clients compared to non-autistic clients (Jager-Hyman et al., 2020; Maddox et al., 2019, 2020). As the use of MBC has been linked to a higher sense of efficacy among mental health providers (Scott & Lewis, 2015), a better understanding of MBC with autistic clients may be one avenue to increase provider certainty.
To date, only one retrospective study compared outcomes (i.e. weekly MBC use, psychotherapy course and trajectory) between 20 autistic and 20 non-autistic clients receiving psychotherapy in a community-based psychology training clinic (McFayden et al., 2021). Important differences between autistic and non-autistic clients were observed including lower weekly MBC compliance among autistic clients relative to non-autistic clients (60% vs 78% compliance), more therapy sessions among autistic clients (31.7 sessions) than non-autistic clients (20.2 sessions) for the same presenting problem, and smaller treatment gains among autistic clients (10.4% average symptom reduction) than non-autistic clients (22.4% average symptom reduction; McFayden et al., 2021). Client experiences in using the MBC system were not measured, which may highlight barriers to use and lower compliance in autistic clients than in non-autistic clients. Initial findings from MycFayden and colleagues (2021) suggest that MBC can be used to track outcomes and to understand psychotherapy processes in autism.
As autistic clients spent more time in therapy and made less progress than non-autistic clients (McFayden et al., 2021), continued efforts to develop and implement MBC systems are needed in autism. Additional information on feasibility (e.g. user experience, provider utility) and acceptability of MBC from clients and providers alike may improve our understanding and implementation for autistic clients. Furthermore, it is likely that a system designed both for and with autistic people may increase feasibility, acceptability, and efficacy. The importance of participatory design in research and clinical projects will be presented in the next section, including specific methods used in the present study to co-design a psychotherapy MBC system for autistic people (MBC-AUT) alongside members of the autistic community.
Participatory design for MBC
Participatory research enables researchers to connect with community members (i.e. self-advocates, caregivers, professionals) to design programs and deliver results in alignment with shared goals (Cornwall & Jewkes, 1995). In autism research, a growing emphasis is placed on participatory research methods to understand implementation challenges, address community dissatisfaction, and deliver a high standard of research to enhance clinical translation and overall outcomes for autistic people (Fletcher-Watson et al., 2019; Keating, 2021). Importantly, participatory methods have become more prevalent in autism research; however, such methods in clinical care for autistic clients are limited. Theoretical examples of participatory clinical care in autism have been proposed and include components such as incorporating autistic perspectives on intervention development and implementation (Schuck et al., 2022). Translation of this theoretical approach into clinical services for autistic people is an important next step. Though opportunities to develop more effective health and social care services in partnership with the autism community is a key area of interest among autistic people (Fletcher-Watson et al., 2019; Shaw et al., 2022), efforts to design clinical systems for and with autistic people have not advanced.
Present study
The current study presents a psychotherapy MBC system (i.e. MBC-AUT) designed for and with autistic people and preliminary data on the feasibility, acceptability, benefits, and barriers of the MBC-AUT system to a pilot sample of clients and clinicians. Three autistic adults of the Neurodivergent Advisory Team at Vanderbilt University Medical Center guided the development of the MBC-AUT including design, measurement selection, and review of implementation in clinical practice. Additional feedback on the initial design of the MBC-AUT system was collected from six members of the broader autism community (i.e. psychologists, psychiatrists, researchers). Data on the feasibility, acceptability, benefits, and barriers to the MBC-AUT were collected from the first 18 autistic youth and adult clients to use the system. Given community-guided design and the known benefits of MBC in improving clinical care, we hypothesized that the MBC-AUT would be feasible and acceptable to autistic clients and that the benefits of the MBC-AUT to both clients and clinicians would be greater than the barriers.
Methods
Participants
The MBC-AUT was designed and implemented in a psychiatry outpatient clinic at the Vanderbilt University Medical Center that provides multidisciplinary psychiatric care to youth (9–17 years old) and adults (18 years and older). This care included individual and group cognitive behavioral therapy (CBT; Beck, 1991). Preliminary data on the feasibility, acceptability, benefits, and implementation barriers of the MBC-AUT were collected from the first 10 autistic clients receiving individual CBT (five adolescent clients and their caregivers, as well as five adult clients), and the first group of autistic adolescents (n = 8) participating in a 12-week CBT group program. Demographic information on the adolescent and adult clients is provided in Table 1. Although the sample was not racially diverse, it reflected the demographics of the general region of the outpatient clinic.
Demographic statistics.
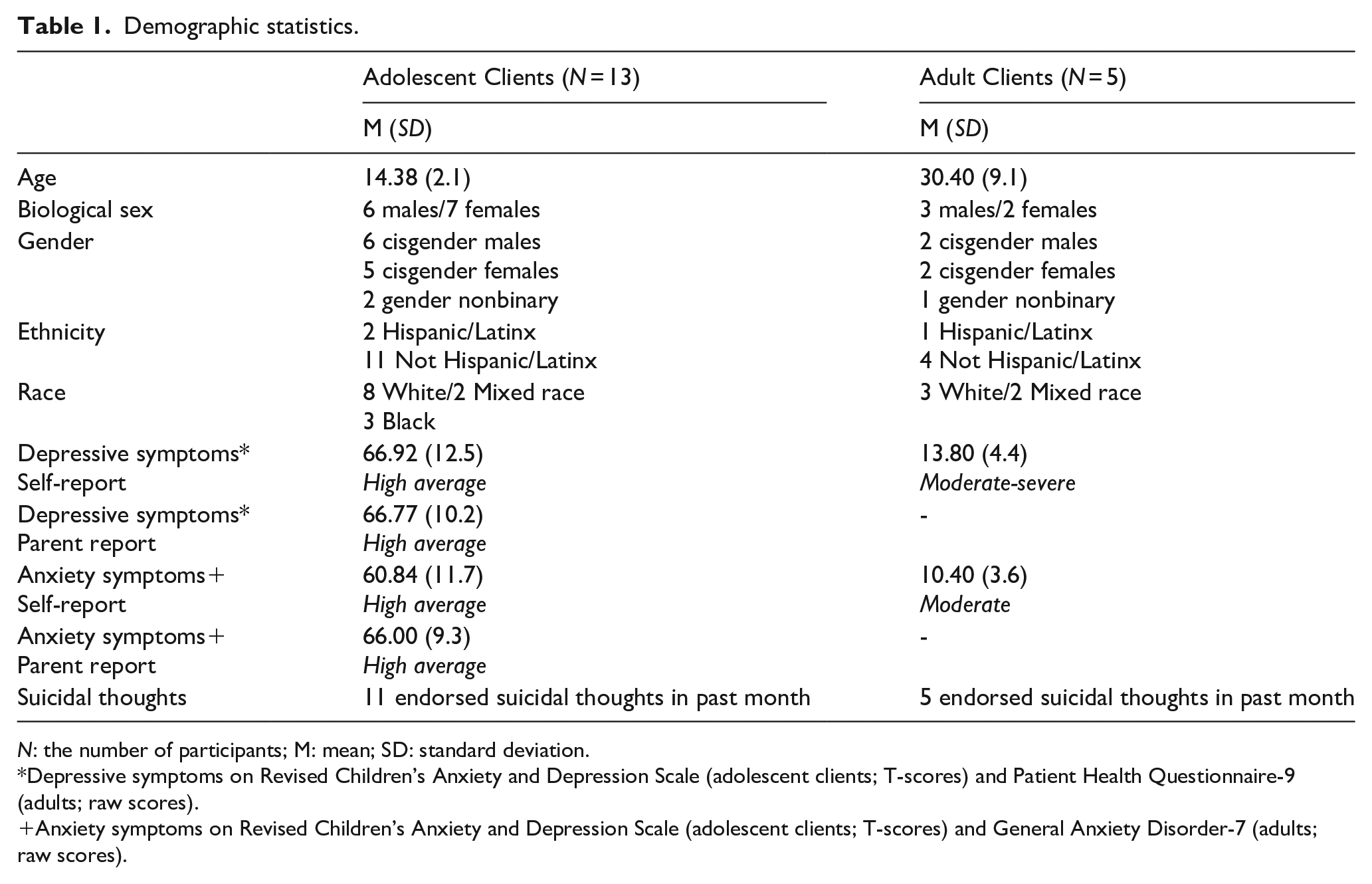
N: the number of participants; M: mean; SD: standard deviation.
Depressive symptoms on Revised Children’s Anxiety and Depression Scale (adolescent clients; T-scores) and Patient Health Questionnaire-9 (adults; raw scores).
Anxiety symptoms on Revised Children’s Anxiety and Depression Scale (adolescent clients; T-scores) and General Anxiety Disorder-7 (adults; raw scores).
Clients were referred for individual or group psychotherapy from providers at the Vanderbilt University Medical Center, local schools, and regional autism/disability organizations. The first iteration of MBC-AUT uses caregiver- and self-report questionnaires to measure various domains of client functioning (see the next section) and thus, inclusion criteria included clients: (a) 11–17 years old (youth) or 18–60 years (adult), (b) without an intellectual disability, (c) with a third-grade reading level or higher for comprehension of survey items, (d) who are English speaking, and (e) who can complete measures online (i.e. access to computer, smartphone, tablet). The assessment battery of the current iteration of the MBC-AUT system includes measures not validated for individuals with intellectual disabilities; however, potential suggestions for this population are included in section “Discussion.” Additional inclusion criteria for psychotherapy in the clinic included some willingness/buy-in to participate in therapy and appropriateness of outpatient care for presenting problems (i.e. youth with severe suicidal intent and plan referred to higher-level care). For the current iteration of the MBC-AUT system, the following exclusion criteria were applied to clients: (a) with an intellectual disability, (b) with a reading level lower than the third grade, (c) who were not confident in their English-language reading abilities, and (d) who were not able to complete measures online. To preserve the safety of adolescents in group therapy, an additional exclusion criterion included adolescents with aggression toward others in the past 6 months. Informed consent and assent for psychotherapy and the use of the MBC-AUT to guide clinical care were collected in writing from caregivers and clients during the intake appointment. To utilize de-identified clinical data for research purposes, the first author completed an application to the Institutional Review Board (IRB) at the Vanderbilt University Medical Center (#211870), and all procedures were approved by the IRB in accordance with the 1964 Helsinki Declaration and its later amendments.
Community involvement statement
To design the MBC-AUT, three autistic adults (including an autistic parent) provided feedback on various aspects (e.g. functionality, implementation) of the MBC-AUT. Specifically, autistic adults were engaged in the project as part of the Neurodivergent Advisory Team at the Vanderbilt University Medical Center given their interests in participatory research and clinical service, as well as personal and/or family experiences of psychiatric disorders and psychotherapy. On several occasions, the Neurodivergent Advisory Team provided feedback on various domains of the MBC-AUT including administration, measure selection, and/or considerations of benefits and barriers to the system for autistic clients. All members of the Neurodivergent Advisory Team were compensated financially for their feedback, participated in the writing and review of the present article, and are included as co-authors. In addition, the first author collected feedback on the initial design of the MBC-AUT system from six other members (i.e. two psychologists, three psychiatrists, one researcher) in the autism community with familiarity of outpatient systems and services at the Vanderbilt University Medical Center.
Procedures
The present section will review a series of procedures used in the current study to design and implement the MBC-AUT with autistic clients. Although MBC systems can be applied to other psychiatric services (e.g. psychopharmacology), the first iteration of MBC-AUT presented here was designed for measuring psychotherapy processes.
Construction of the MBC-AUT
The MBC-AUT was built in REDCap (Research electronic data capture; Harris et al., 2009), which is an online metadata-drive methodology and workflow process developed at Vanderbilt University for providing translational research informatics support. Some of the measures (e.g. Patient Health Questionnaire-9; (Kroenke et al., 2001) selected for the MBC-AUT battery were available in REDCap, whereas other measures (e.g. Comprehensive Autistic Trait Inventory; (English et al., 2021) were not and had to be created by the first author. To reduce risks to confidentiality, all data collected in the MBC-AUT were de-identified and only the treating clinicians had access to client email addresses used to administer the surveys. Community members suggested the following modifications to ease clients’ burden of completion: (1) “save and return” capability to allow clients to complete surveys in multiple attempts, (2) automatic, one-time email reminders to complete surveys, and (3) an open text box at the end of each measure for clients to write additional notes or clarifications as desired (i.e. to make the system more user-friendly).
Measure selection for the MBC-AUT
Measure criteria
Measurement challenges in autism research and clinical practice are common (Loth et al., 2016) as many measures have not been carefully validated in autistic people. Therefore, a review of the existing literature was used to develop the following criteria for measures of the MBC-AUT: (a) validated in autistic people (e.g. Revised Children’s Anxiety and Depression Scale, RCADS; Chorpita et al., 2005), when available, (b) brief, when possible, to reduce client burden (e.g. PHQ-9 in lieu of the BDI-II), and (c) free and publicly-available to reduce clinic costs. As needed, permission from measure authors was obtained (e.g. author permission to use the RCADS). In particular, the use of free and publicly available measures may enhance the generalization and feasibility of the MBC-AUT to other clinical settings with limited funds and/or resources available.
Domains of interest
Although psychotherapy is a dynamic, multifaceted process, the following five domains were consistently measured to inform case conceptualization and treatment planning: symptom severity, client safety, risk and protective factors, therapeutic alliance, and functional outcomes. A list of the measures administered in the MBC-AUT to clients is available in Supplemental Tables 1 and 2. Symptom severity measures provide information about symptom type (e.g. depression, anxiety) and severity (i.e. average, mild, moderate, severe), and are often included in treatment plans as an index of therapeutic progress (i.e. decreased symptom severity). Client safety measures monitor potential harms to self (e.g. suicidal thoughts, self-injurious behaviors) or others (e.g. homicidal thoughts, aggression) and provide data for crisis assessments and safety planning. Risk and protective factor questionnaires assess risk (e.g. substance use, bullying, insomnia) and protective (e.g. social connectedness, family cohesion) factors to monitor as clients engage in therapy and/or identify additional areas for intervention. Therapeutic alliance measures determine client–therapist fit and can pinpoint any barriers to a client’s therapeutic progress, an essential component of therapeutic change (Horvath & Luborsky, 1993). Functional outcome indices assess global functioning in various domains (e.g. quality of life, daily activity, social engagement).
Despite a robust evidence base of risk and protective factors to psychiatric disorders in the general population, the evidence base in autism is limited. Several risk factors were measured in the MBC-AUT based on a review of literature and feedback from community members: cognitive rigidity (Zimmerman et al., 2017), low social connectedness (Diendorfer et al., 2021), poor sleep quality (Jovevska et al., 2020), emotion dysregulation (Mazefsky et al., 2014), distress intolerance (Boulter et al., 2014), negative self-esteem (Cooper et al., 2017), and camouflaging (i.e. behavioral and cognitive strategies by autistic people to adapt to or cope within the predominately non-autistic social world; see review by Cook et al., 2021). These risk factors are not specific to autistic people but have been endorsed more frequently by autistic people than non-autistic people. Although these eight risk factors are comprehensive, they are not an exhaustive list and thus, clinicians, community members, and researchers may consider other risk/protective factors in designing and implementing a system of MBC for a given setting. In autistic youth, inter-rater discrepancies between youth and their caregivers on adolescent psychiatric symptoms have been documented (Schwartzman & Corbett, 2020). Therefore, the MBC-AUT included caregiver- and self-report versions of several measures (e.g. Revised Children’s Anxiety and Depression Scale, Caregiver and Youth Versions) to obtain multiple perspectives of an adolescent’s symptoms and severity.
Caregiver-specific measures
Community members suggested the inclusion of several caregiver-specific measures in the MBC-AUT to understand and monitor caregiver experiences as youth participate in therapy. Certain caregiver factors (e.g. depressive symptoms, anxiety) have been associated with youth psychopathology and may be critical to monitor as youth engage in psychotherapy (Marmorstein & Iacono, 2004; Schwartzman et al., 2021; Zhou & Yi, 2014). In addition, caregivers are critical treatment partners who often increase the efficacy of therapy (e.g. generalization of skills, safety monitoring). Therefore, a consideration of caregiver-specific measures is critical to understanding treatment engagement and progress among autistic youth. In the MBC-AUT, the following measures were administered to caregivers once a month: depression symptoms (PHQ-9; Kroenke et al., 2001), anxious distress (GAD-7; Spitzer et al., 2006), stress (10-item Cohen Perceived Stress Scale; Cohen et al., 1994), and quality of life (PROMIS Global–10; Hays et al., 2009).
Clinical caution
It is important to note that measures of some client experiences (e.g. gender dysphoria, trauma exposure) may be stressful and potentially harmful to clients if administered in a MBC system (Machtinger et al., 2019). To protect client safety, careful consideration of measures in collaboration with clients is needed. Therefore, certain experiences that have been found to occur more frequently among autistic people (Corbett et al., 2023; Lai et al., 2019) were not selected in the MBC-AUT. Instead, measures were available to clinicians for use during sessions. Similarly, additional measures of suicide risk (e.g. Columbia Suicide Severity Rating Scale; Posner et al., 2011) were administered in person, and answers were entered into the REDCap system during sessions. Of note, clinicians, community members, and researchers may consider other client experiences to monitor sensitively to uphold client confidentiality, safety, and well-being in a given setting.
MBC-AUT implementation in clinical practice
Establishing care
For new clients to the Vanderbilt University Medical Center, clients were asked to arrive 30 min early to complete consent and assent forms for psychotherapy. Clients were not charged for their time in completing consent/assent processes and MBC-AUT surveys. In the consent/assent process, clients received brief psychoeducation about the role of the MBC-AUT in clinical care and were provided with opportunities to ask questions. Following consent/assent, clients completed the online surveys of the MBC-AUT. For clients established at the Vanderbilt University Medical Center with completed consent/assent on file, clients were contacted over the phone and notified that they would receive an online survey approximately 3–4 days before their intake appointment. Clients and caregivers were provided with psychoeducation about the role of the MBC-AUT in clinical care over the phone and during the intake appointment, and clients and caregivers were provided with opportunities to ask questions.
Intake appointments and diagnostic decisions
During the intake appointment, clinicians used a computer to review survey responses with clients (and caregivers) including symptom endorsement, any safety risks, and initial diagnostic impressions. By doing so, clients and caregivers clarified their responses (if desired) and contributed to diagnostic decisions. In addition, a review of responses enabled clinicians to provide clients with psychoeducation about psychiatric symptoms (e.g. loss of interest in activities is a symptom of depression). For youth clients, a review of responses often highlighted caregiver-youth discrepancies in ratings and provided an opportunity for group discussion and consensus. Although the focus of discussions was on diagnostic clarity, it also afforded opportunities for youth and caregivers to learn about each other’s perspectives and to discuss ways to monitor symptoms throughout treatment.
Treatment planning
Following diagnostic decision making, clinicians used client responses to discuss initial treatment goals with clients and to collaboratively develop an initial treatment plan. Data from the MBC-AUT were used to inform a client’s progress toward their treatment goals and to adapt treatment plans over time.
Individual psychotherapy
In alignment with feedback from community members, surveys were emailed to clients once a month throughout treatment to reduce client burden. A consistent battery of measures (see Supplemental Tables 1 and 2) was sent each month, with opportunities to customize certain measures (e.g. Columbia Suicide Severity Rating Scale; Posner et al., 2011). For patients with significant safety risks, clinicians administered some measures (e.g. C-SSRS; Posner et al., 2011) during each session to monitor safety and to review and reinforce safety plans. Once per month, clinicians reviewed the MBC-AUT data with clients in session to facilitate discussions about symptom severity, safety (if applicable), risk and protective factors, and functional outcomes (e.g. quality of life). By doing so, clients directly engaged in their care to identify progress and barriers to be addressed in session. In addition, clients and clinicians could discuss areas for potential referrals to other providers to enhance care (e.g. referral to neurology for chronic migraines). Clinicians discussed data on therapeutic alliance in an open, curious, and collaborative manner with clients to isolate areas of clinician adaptation needed to support client progress toward treatment goals. Furthermore, discrepancies in caregiver-youth ratings could be identified and discussed in session.
The decision to administer measures monthly was influenced by previous studies on MBC systems and feedback from autistic community members. Weekly administration is a common, but not required, format for MBC systems that is associated with certain advantages (e.g. frequent estimates of psychiatric symptoms) and disadvantages (e.g. significant time, lower compliance, diluted responses; Scott & Lewis, 2015). Community guidance in developing and implementing a system of MBC is a critical component of this work (Lewis et al., 2019), and thus, we relied on feedback from community members to guide the default frequency of assessment used in the MBC-AUT system (i.e. monthly administration). Of note, measures were available to administer more frequently if clinicians noted substantial changes in client presentation and/or changes or concerns were reported by clients or caregivers that may warrant additional assessment.
Group therapy
Although group-based therapy is associated with benefits (e.g. increased access to care, reduced clinic costs; Churchill et al., 2001), it provides a less tailored approach than individual therapy. To address this challenge, the MBC-AUT was used to monitor symptom severity, patient safety, risk and protective factors, therapeutic alliance, and functional outcomes of all clients throughout the 12-week CBT group program. At the midpoint (week 6) session, each family received a report of youth and caregiver scores from the MBC-AUT to summarize symptom severity and to provide recommendations (e.g. individual therapy) for discharge planning. Reports were provided to families directly and families were encouraged to contact the clinicians with any questions or concerns. At the graduation (week 12) session, each family received an updated report of additional scores from the MBC-AUT to summarize the youth’s engagement in treatment, areas of continued intervention, and recommendations for future care. Families were again encouraged to contact the clinicians with any questions or concerns and to share the reports with other providers to guide continued care.
For clients in individual or group therapy, the MBC processes were identical in the intake appointment (e.g. case conceptualization, treatment planning). In lieu of monthly score review, group therapy clients received several reports of MBC-AUT scores with clinical summaries and recommendations, and were repeatedly encouraged to contact clinicians with any questions or concerns. While this approach may not be as individualized as individual therapy, it nevertheless afforded some opportunity to personalize the group therapy approach for clients.
Treatment decisions
The MBC-AUT guided treatment decisions between clients and providers including session frequency, therapy graduation, and additional services that may be beneficial to clients. Individual therapy clients who demonstrated consistent progress toward their selected goals often chose to reduce session frequency over time to increase independence and to advance toward therapy graduation. The individualized approach of the MBC-AUT enabled clients and clinicians to personalize benchmarks for therapy graduation and to visualize client changes over time. Clients who demonstrated limited progress toward their selected goal and/or exhibited worsening symptoms based on scores in the MBC-AUT typically elected for more frequent sessions, greater caregiver involvement (if applicable), and/or alternative care options (e.g. medication management, intensive outpatient program).
Measures of the feasibility, acceptability, benefits, and barriers to the MBC-AUT
A questionnaire assessing the feasibility and acceptability of the MBC-AUT was administered to the 18 autistic clients at three timepoints: at the end of the intake appointment (T1), after 6 weeks of using the system (T2), and after 12 weeks of using the system (T3). The questionnaire included the following items: (1) “Completing the surveys was difficult for me”; (2) “Completing the surveys was a good use of my time”; (3) “Completing the surveys was helpful to my experience in therapy”; and (4) “Completing the surveys interfered with my experience in therapy.” Items were rated on a 7-point Likert-type scale from 1 = Very Much Disagree to 7 = Very Much Agree. For youth clients, an identical questionnaire was administered to caregivers. As another index of feasibility, the consistency of MBC-AUT completion throughout therapy was monitored for each client.
To assess the benefits and barriers of the MBC-AUT, clients and their caregivers participated in a brief, semi-structured interview at T3. The following questions were asked of clients and caregivers: (1) “Are there benefits to completing the surveys and reviewing them with your therapist? If so, what are the benefits?”; (2) “Are there difficulties in completing the surveys and reviewing them with your therapist? If so, what are the difficulties?”; and (3) “Is there anything else that you would like to share about your experience with the surveys throughout therapy?” Notes were taken as clients provided answers to these questions, and the main points were recorded in REDCap.
Results
Feasibility and acceptability
Client ratings of the feasibility and acceptability of the MBC-AUT are presented in Table 2. Average ratings from adolescent clients reflected neutral attitudes about the difficulty of completing surveys and their use of time at T1; however, ratings in both areas improved over time at T2 and T3. On average, ratings from adolescent clients indicated slight agreement about the helpfulness of the MBC-AUT to therapy at T1, with ratings improving over time at T2 and T3. Importantly, average ratings from adolescent clients indicated that the use of the MBC-AUT did not interfere with therapy across the three timepoints.
Means and standard deviations of feasibility and acceptability ratings of MBC-AUT from autistic clients.

MBC-AUT: autism-adapted measurement-based care; SD: standard deviation.
Completing the surveys was difficult for me.
Completing the surveys was a good use of my time.
Completing the surveys was helpful to my experience in therapy.
Completing the surveys interfered with my experience in therapy.
On average, caregivers endorsed slight disagreement about the difficulty of completing surveys at T1; however, caregiver ratings improved across timepoints. Average ratings from caregivers indicated that the MBC-AUT was a good use of time and helpful to therapy at T1, with improved ratings in both areas across timepoints. Importantly, caregivers did not report that the MBC-AUT interfered with therapy.
Average ratings from autistic adult clients indicated slight disagreement about the difficulty of completing surveys at T1; however, ratings improved over time at T2 and T3. Autistic adults reported that the MBC-AUT was a good use of time and helpful to therapy at T1, with ratings in both areas increasing across the timepoints. On average, autistic adults did not report that the MBC-AUT interfered with therapy.
Of all 18 clients, 14 clients (77.7%) completed the MBC-AUT consistently and on-time throughout the course of psychotherapy. Of the remaining four clients, three clients (16.7%) did not complete one administration of the MBC-AUT due to illness or forgetting, and only one client (5.6%) did not complete two administrations of the MBC-AUT.
Benefits of MBC-AUT for clients and clinicians
Implementation of the MBC-AUT in an outpatient setting highlighted benefits to clients and clinicians (see Table 3).
The benefits of the MBC-AUT for autistic clients and clinicians.
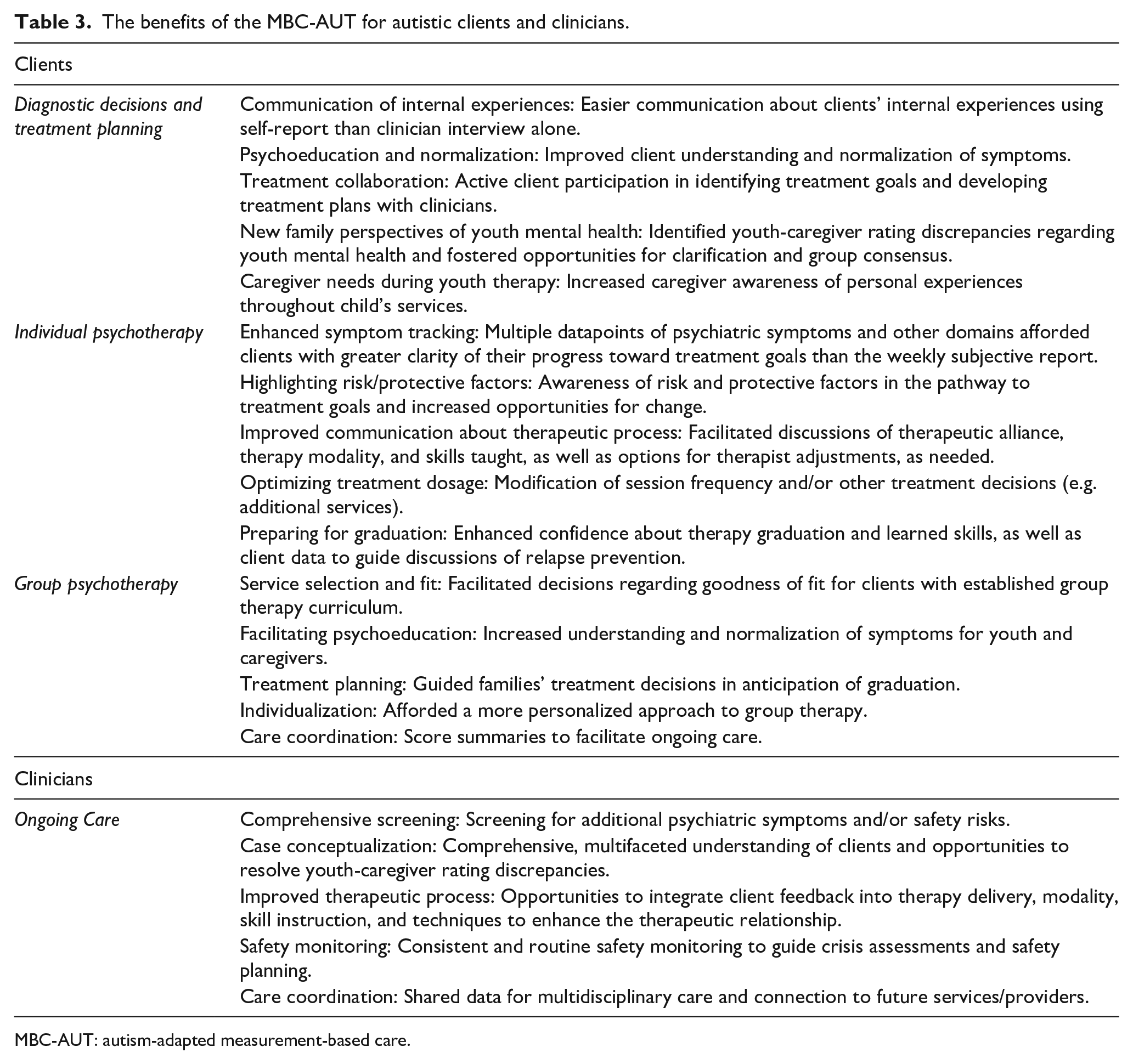
MBC-AUT: autism-adapted measurement-based care.
Benefits for clients: Diagnostic decisions and treatment planning
First, the theme of Communication of Internal Experiences emerged across multiple youth and adult clients who shared that self-report measures were “easier to do” than semi-structured, clinician-administered interviews. Second, the theme of Psychoeducation and Normalization was identified as a review of responses in the intake appointment provided clients with a better understanding of their symptoms and some normalization (e.g. “I realized there isn’t something wrong with me. . .depression makes me less interested in things”). Third, the theme of Treatment Collaboration was mentioned by multiple clients as a review of responses with clinicians fostered collaborative discussions of treatment goals and plans (e.g. “I knew what we would work on and why, like it made sense to me”). Fourth, for caregivers, the theme of New Family Perspectives of Youth Mental Health emerged as a review of responses/scores highlighted youth-caregiver rating discrepancies (e.g. “I never realized that he (child) thought so negatively of himself”). Finally, caregivers noted the theme of Caregiver Needs During Youth Therapy as they identified benefits to monitoring their own experiences (e.g. “I could see that my stress was really high at times when my son was also really stressed—we affect each other”).
Benefits for clients: Individual psychotherapy
First, the theme of Enhanced symptom tracking emerged as clients noted that multiple datapoints of symptom severity, rather than their subjective opinion each week, clarified their progress toward treatment goals (e.g. “I knew my sadness was getting better, but it really helped to see it go down (in the surveys)”). Second, the theme of Highlighting risk/protective factors was mentioned by several clients who commented that data on risk/protective factors fostered open discussions of ways to problem solve for risk factors (e.g. “I needed help with bullying—it was making me sad”) or consider ways to increase protective factors (e.g. “I realized that spending time with friends is really important for me and my mental health stuff”). Third, the theme of Improved communication about therapeutic process was identified as many clients commented on the benefits of openly discussing components of therapy (e.g. therapeutic alliance, therapy modality; “My therapist didn’t get mad or something when I told her that some things she taught didn’t work for me”).
Fourth, the theme of Optimizing treatment dosage was identified as a review of responses fostered conversations about modifying session frequency (e.g. weekly to bimonthly, monthly to bimonthly) or care options (e.g. initiating medication management). Finally, the theme of Preparing for graduation emerged as clients noted that ongoing data collection improved confidence in therapy graduation (e.g. “I could pause or stop therapy and probably continue to do well”), and facilitated discussions of relapse prevention (e.g. “Good sleep is something that I need to continue to focus on for my mental health”).
Benefits for clients: Group psychotherapy
First, the theme of Service selection and fit emerged as the review of data facilitated families’ decisions to join the group program or not (e.g. “If other kids also have depression stuff on these questions then we might understand each other or something”). Second, the theme of Facilitating psychoeducation was identified as a review of data that provided clients with a better understanding of their symptoms (e.g. “I was not excited about my future, but it wasn’t my fault—just a depression thing”). At the midpoint (week 6; T2), the theme of Treatment planning emerged as caregivers commented that a review of scores guided families’ treatment decisions in anticipation of group graduation (e.g. “It was clear that her depression was getting better, but that getting more therapy would help her”). The theme of Individualization emerged as several families noted that the MBC-AUT provided a more personalized approach to group care than typical group therapy formats (e.g. “I could see how they were doing even if they were in a group with other kids”). In the final summary report (week 12; T3), the theme of Care coordination was identified as caregivers shared that the report was helpful in guiding future care (e.g. “I can take his scores to the next therapist to give us a starting point”).
Benefits for clinicians
In addition to the benefits reported by clients, the use of the MBC-AUT was associated with added benefits to clinicians. First, the theme of Comprehensive screening emerged as clinicians screened for additional psychiatric symptoms (e.g. OCD symptoms, separation anxiety) and/or safety risks (e.g. substance use), many of which were not mentioned by clients, in the intake appointment and throughout therapy. Second, the theme of Case conceptualization was identified as clinicians obtained a comprehensive and multifaceted understanding of clients (e.g. psychiatric symptoms, quality of life, safety concerns). Third, the theme of Improved therapeutic process emerged as clinicians received feedback on the quality of therapeutic techniques and/or alliance, which was reviewed and adjusted collaboratively with clients as needed. Fourth, the theme of Safety Monitoring was identified as clinicians consistently and routinely monitored safety (e.g. suicidal thoughts, substance use), and data could inform crisis assessments and safety planning. For example, routine data collection was leveraged to monitor for any changes in types (e.g. change from previous passive suicidal thoughts to current thoughts of a plan, alcohol consumption to cope) and severity (e.g. passive vs active suicidal thoughts, intent vs no intent, increased number of alcoholic drinks) of safety risks. This updated information could be used to review and reinforce existing safety plans, adapt safety plans (e.g. increase caregiver supervision), or implement greater safety measures (e.g. voluntary hospitalization). Finally, as needed and permitted by clients, clinicians shared data with outside providers (e.g. psychiatrists, primary care physicians, individual therapists) to guide additional care—a theme of Care Coordination.
Of note, the MBC-AUT collects a substantial amount of data from clients that can be de-identified and available for research purposes (e.g. longitudinal risk/protective factors to depression in autism, caregiver-child rating discrepancies throughout therapy). Although contribution to the research was not a primary objective of developing the MBC-AUT, it may enable researchers to advance the study of mental health and psychotherapy for autistic clients.
MBC-AUT barriers for clients and clinicians
Implementation of the MBC-AUT in an outpatient setting highlighted barriers to clients and clinicians (see Table 4).
The barriers and proposed solutions to the MBC-AUT for autistic clients and clinicians.
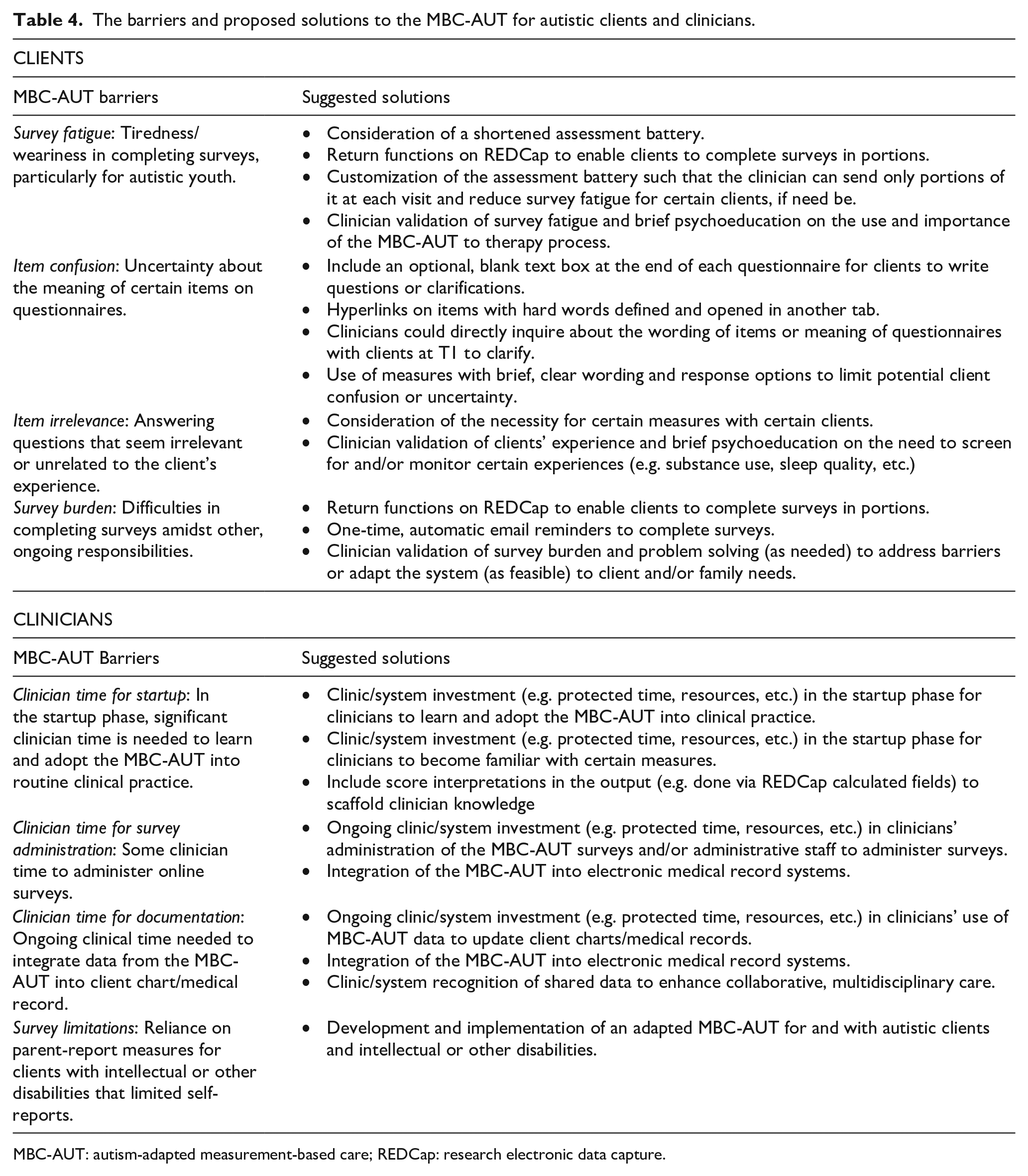
MBC-AUT: autism-adapted measurement-based care; REDCap: research electronic data capture.
Barriers for clients
First, the theme of Survey fatigue emerged as multiple youth clients reported weariness in completing the surveys (e.g. “I got pretty bored sometimes,” or, “Doing the questions made me sleepy and tired”). Some fatigue was reported by caregivers and autistic adults, but this was less in amount than fatigue reported by youth clients. Second, the theme of Item confusion was identified as some youth and adult clients endorsed confusion or uncertainty at the meaning of questions or particular item wording (e.g. “Some questions were confusing like when it said I feel shaky or restless—I don’t know what those mean”). Third, the theme of Item irrelevance emerged as some clients perceived certain questionnaires to be irrelevant (e.g. “I always saw questions about drinking, but I never drink”). Finally, the theme of Survey Burden was identified as some caregivers conveyed some difficulties in completing surveys (e.g. “I get that it is helpful for my kid—but sometimes it was still one more thing on the to-do list”). A similar challenge was reported by a few autistic adults.
Barriers for clinicians
First, the theme of Clinician time for startup emerged as a barrier, as a substantial amount of clinician time was required to initially learn and adopt the MBC-AUT system into routine clinical practice, as well as become familiar with certain measures (e.g. item content, clinical cutoff scores). Second, the theme of Clinician time for survey administration was identified as some clinician time (10–15 min total) was needed once a month to administer online surveys to clients and review responses before sessions. Third, the theme of Clinician time for documentation emerged as clinicians spent some time integrating data from the MBC-AUT into each client’s chart/medical record. Finally, the theme of Survey limitations emerged as the current iteration of the MBC-AUT system was not available for clients with intellectual disability, language barriers, or other disabilities (e.g. blindness).
Discussion
In the present study, we sought to design and implement a MBC-AUT for and with autistic people to enhance psychotherapy services, and to investigate the preliminary feasibility, acceptability, benefits, and barriers to this system. Initial findings suggest that the MBC-AUT is a feasible and acceptable system for autistic youth, their caregivers, and autistic adults that may be associated with greater benefits than costs to clients and clinicians. Client ratings of feasibility and acceptability improved over the course of treatment, and the majority of clients consistently engaged with the MBC-AUT at all timepoints. Data from semi-structured interviews revealed important benefits of the MBC-AUT to clients in enhancing diagnostic decisions, treatment planning, and experiences in individual and group psychotherapy, as well as benefits to clinicians. Importantly, some barriers of the MBC-AUT were identified by clients and clinicians, and proposed solutions (see Table 4) will be provided to advance efforts in MBC for autistic clients.
Prior to this study, only preliminary findings from one study of a standard MBC with autistic and non-autistic clients were available to suggest that the MBC is an important area of investigation for this population (McFayden et al., 2021). The present study expanded upon these findings by co-designing an autism-adapted MBC system with a group of autistic adults and investigating user experiences across clients and clinicians (i.e. feasibility, acceptability, benefits, barriers) to modify practices and to propose a model for future use in clinical settings. Following initial use of the MBC-AUT during the intake appointment, the majority of autistic youth, their caregivers, and autistic clients reported the system to be feasible and acceptable. Importantly, over the course of therapy, client and caregiver ratings improved across the four domains and may suggest that clients perceive the system to be easier to engage with and/or experience greater familiarity with the questions. Improvements in ratings may also encourage clinicians to spend more time during intake appointments discussing the value of MBC to case conceptualization and treatment planning and decisions. An important next step in this line of research is to understand mechanisms of change in acceptability over time in larger and more controlled samples.
The majority of clients and caregivers perceived the system to be a good use of time and helpful to the therapeutic process, which highlights the initial promise of the MBC-AUT system as a critical tool to improve psychotherapy for autistic clients. In the general population, MBC has been associated with direct benefits to clients (e.g. symptom improvement), clinicians (e.g. empirically-based decision making), and organizations/clinics (e.g. quality improvement efforts; Bickman et al., 2011; Carlier et al., 2012; Kearney et al., 2015). It is critical to test whether these benefits can also be realized in autistic clients. A comparison of client experiences with a standard or autism-adapted MBC system is an important next step to advance this line of research, as well as the utilization of the system with other therapy modalities (e.g. family therapy) and/or psychiatric services (e.g. medication management).
The majority of clients completed the MBC-AUT consistently and on-time throughout therapy, which adds support to the preliminary feasibility of the system for autistic clients. The compliance rate among autistic clients in this study (77%) was higher than that reported by McFayden and colleagues (2021; 60%). Potential explanations for these differences may include a smaller sample in the present study, a system designed for and with autistic people in the present study, and/or fewer administrations of surveys in the present study (i.e. once a month compared to weekly). With a limited sample size, it is difficult to robustly investigate differences between clients who did (i.e. responders) or did not (i.e. nonresponders) complete surveys consistently. It would be important to investigate the feasibility and acceptability of the MBC-AUT system with larger samples to identify differences between responders and nonresponders to propose solutions to increase compliance.
Many autistic youth and adults identified important benefits to the MBC-AUT system that may be leveraged to enhance psychotherapy for this population. For some autistic clients, self-report measures of internal experiences were a favored assessment method over clinical interviews. Social interactions and/or generic, open-ended questions (e.g. “How are you feeling?” or, “Describe your mood most days”) inherent to clinical interviews may be interpreted as ambiguous and stressful by some clients. Though some challenges occurred with self-report measures (e.g. confusing item wording), this methodology lacks a social interaction component and is more structured in nature, and thus, it may be a more comfortable assessment method for some clients than clinical interviews. The inclusion of open text boxes at the end of measures to clarify item selection and/or pose questions to clinicians may also facilitate clients’ ease of use. Self-report measures alone do not supersede clinician observation and judgment, but they may nevertheless be a beneficial addition to the assessment of emotional experiences in autistic clients due to their ability to circumvent certain social communication differences between clients and clinicians. Questionnaire scores, particularly in conjunction with an opportunity to review and understand their meaning with clinical judgment, may afford a more concrete and digestible approach to diagnostic decision-making for autistic clients than clinical interviews alone.
Improved client understanding of symptoms and normalization have been associated with the use of MBC in psychotherapy (Bickman et al., 2011; Carlier et al., 2012) and appear to be an important benefit for autistic clients. Similarly, client–clinician collaboration on diagnostic decisions and treatment planning has been documented in non-autistic clients receiving MBC (Fortney et al., 2017), and our findings suggest that client–clinician collaboration is important to autistic clients. Collaboration in therapy to identify effective strategies may be exceptionally valuable to autistic clients who are more likely to be misunderstood, experience miscommunications, and/or engage in masking. A study of client and clinician experiences in therapy collaboration is a critical next step to advance this research. In addition, the benefits of identifying and resolving youth-caregiver rating discrepancies through the MBC-AUT system may be particularly salient in autism as rating discrepancies of adolescent mental health are more common in autism than the general population (Kalvin et al., 2020; Schwartzman & Corbett, 2020).
The caregiver-specific measures of the MBC-AUT system provided clinicians and caregivers alike with information about caregiver well-being, some insights into family history, and potential areas to support caregivers in their role as treatment partners for their child. For example, many caregivers reported depressive symptoms and shared family histories of depression that may contribute to a youth’s depression. Similarly, caregivers acknowledged the role of their own stress, anxiety, or depressive symptoms in interactions with their child. Increased awareness and open conversations about caregiver well-being afforded a more holistic perspective of the family and opportunities to share resources for caregivers themselves. On several occasions, these realizations encouraged caregivers to pursue their own individual therapy. A focus on caregiver well-being in the MBC-AUT system may be a critical benefit for autistic clients, particularly as caregivers of autistic youth frequently endorse higher stress (Bonis, 2016) and more psychiatric symptoms (e.g. depression, anxiety) than caregivers of non-autistic youth (Corbett et al., 2021; Giallo et al., 2013; Schwartzman et al., 2021; Zhou & Yi, 2014).
Of note, adolescent clients were informed that survey responses would be reviewed with caregivers in the intake appointment and in developing treatment plans, which adolescent clients agreed to. However, it is important to consider that a review of responses with caregivers, and/or knowledge that caregivers have access to minors’ health information, may have affected adolescents’ responses to questions (e.g. under-reporting, worry about disappointing caregivers, masking). To address this, suggestions for clinicians include: (a) the option for families to do separate survey reviews with adolescents and caregivers, (b) additional discussions with adolescents about the role of the MBC system in care (e.g. improve care, target distress experienced by clients, not to get youth in trouble), and (c) the option to opt out of completing surveys. If clients elect for the third option, clinicians could qualitatively assess the critical domains of the MBC (e.g. symptom severity, risk/protective factors) in session with the adolescent client, while not reporting scores.
Clinicians reported many benefits to the MBC-AUT system in enhancing clinical care for autistic clients, which supports the feasibility and acceptability of this intervention for clinicians and clients alike. Enhanced screening, case conceptualization, safety monitoring, and care coordination have been associated with MBC systems for non-autistic clients (Bickman et al., 2011), and may be important benefits for clinicians serving autistic clients. Clinicians in the present study were experienced in treating autistic clients and, thus, may not have reported a benefit of increased certainty in treating autistic clients. As many clinicians report uncertainty in treating autistic clients and often refer out (Maddox et al., 2019, 2020), it is possible the systematic administration of the MBC-AUT intervention may increase provider certainty and/or retention of referrals. To test this, it would be important to measure clinician attitudes toward, and certainty in treating, autistic clients before and after the implementation of the MBC-AUT system.
Barriers to implementing MBC systems in healthcare settings are documented in the general population (Carlier et al., 2012) and occur for autistic clients and clinicians alike. Fatigue in completing surveys, confusion about item wording and/or importance, and client burden in completing surveys are challenges to MBC that are noted in non-autistic clients (Bickman et al., 2011; Kearney et al., 2015), and occurred for autistic clients and caregivers in the current pilot study as well. Proposed solutions to the barriers identified by clients are presented in Table 4 and may provide an initial starting point for addressing these barriers. Although these barriers are not specific to our institution and are likely to apply across multiple clinical settings, it is notable that we only explored the potential for implementation barriers to occur at our specific clinical site (i.e. a specialized outpatient psychotherapy clinic within an academic medical center). With the potential adoption of the MBC-AUT system into other clinical settings (e.g. community mental health, partial hospitalization programs), additional barriers may arise for clients and clinicians alike. In order for the MBC to be incorporated into routine clinical practice more widely within the autism field, continued investigations of user experiences (i.e. feasibility, acceptability, benefits, barriers) are essential. Further large-scale data demonstrating the feasibility, acceptability, and cost-effectiveness of MBC-AUT and similar MBC systems are therefore needed to support autism-specific MBC as a truly evidence-based practice within this field of mental health care. However, the preliminary data from our MBC-AUT system and many years of research on MBC in other psychiatric services support this practice in the autistic population and encourage additional research and quality improvement efforts in parallel. As noted previously, it will also be important to design and implement an MBC system that is inclusive of autistic clients with intellectual disability, language disability, or other disabilities (e.g. blindness) to enhance clinical care for the broader spectrum of autistic individuals served at mental health clinics, including our clinic (see Fitzpatrick et al., 2022; Nicolaidis et al., 2020) for examples of adaptations for individuals with more limited cognitive or language abilities).
Importantly, administrative barriers (i.e. clinician time for startup, survey administration, and documentation) were the most common for clinicians using the MBC-AUT system in psychotherapy and point to the importance of support and resources (e.g. protected time, clinician training) from clinics and organizations to adopt this system. It is important to note that researchers, clinicians, and autistic adults dedicated time in the startup phase of MBC-AUT to closely review the literature and select the measures included in the battery. While this effort produced a battery of robust measures that may be used by other clinics, this process highlights the need for more freely available and brief measures to be created and/or validated for autistic people. In the general population, similar barriers are frequently reported by clinicians and healthcare systems attempting to implement MBC into routine clinical care (Fortney et al., 2017). Greater support and resources are needed in the startup phase of MBC (Aboraya et al., 2018; Lewis et al., 2019; Scott & Lewis, 2015), but over time, less support is needed as clinicians become familiar with the system. The initial investment in MBC contributes to long-term benefits to clients (e.g. reduced symptom severity, fewer treatment sessions), clinicians (e.g. empirically-based decision making), and organizations or clinics (e.g. quality improvement efforts; Bickman et al., 2011; Carlier et al., 2012; Kearney et al., 2015) over time and may be important for autistic clients who are more likely to seek psychiatric services than the general population (Joshi et al., 2010). A systematic investigation of the short-term costs and long-term benefits of the MBC-AUT system to clients, clinicians, and organizations is an important extension of this research.
As different clients and clinicians engage with the MBC-AUT system in real-time at the Vanderbilt University Medical Center, the system is constantly being improved and iterated to meet client and clinician needs. Opportunities to personalize the system for clients are underway, including optional add-on modules that are disorder-specific (e.g. OCD, social anxiety) and iterations for clients who cannot complete self-report measures for various reasons (e.g. language barriers, intellectual disability).
Limitations
The present study was the first to design and implement an MBC system for psychotherapy for and with autistic clients; however, there are several limitations that warrant a discussion and may constitute future directions. First, the study included a small sample of autistic clients and caregivers attending one of two psychotherapy services at a single clinic, which limits the generalizability of findings and/or consideration of additional benefits or barriers to the system that may be identified by a greater number of autistic people in multiple environments or accessing a wider range of therapeutic interventions. In addition, between-group differences in adolescent, caregiver, and adult acceptability ratings were not tested given the small sample; however, this is an important area of future investigation. Relatedly, we did not investigate changes in acceptability ratings over time due to the small sample and conceptual focus of the article; however, this may be an important next step in this line of research, particularly in a larger controlled trial. Second, clients in the study were able to access therapy and utilize insurance to pay for sessions, which are two challenges (i.e. access to care, insurance coverage) faced by many autistic people and limit the generalizability of these findings. Third, the clinicians included in the study had expertise in autism and may not represent the majority of clinicians in other settings (e.g. community mental health, general psychiatry clinic). Fourth, the MBC-AUT system was implemented in an outpatient setting, and thus, the feasibility and acceptability of the system may change across settings (e.g. partial hospitalization program, residential care setting) and clients (e.g. significant safety concerns and/or functional impairments that warrant higher-level care). Fifth, the feasibility and acceptability of the MBC-AUT system were not compared to a control condition (e.g. standard MBC or treatment as usual), which limits conclusions. Sixth, the parameters of the MBC-AUT system may still not be optimal as we have not tested all possible iterations of the assessment battery. Seventh, modified approaches to reviewing responses with clients in individual and group therapy were used given the distinct treatment modalities. It may therefore be important to investigate associations between system modifications and client experiences for clients receiving individual or group therapy in larger more controlled trials. Finally, as noted, the MBC-AUT system was implemented within the psychotherapy clinic that primarily serves clients presenting with depressive disorders, anxiety disorders, and/or suicidal thoughts and behaviors and thus, the current iteration of the system does not cover additional psychiatric problems common in autistic people (e.g. PTSD, eating disorders).
Conclusion
With many autistic clients pursuing psychotherapy for psychiatric symptoms, research into MBC to enhance therapeutic processes is critical for this population. Participatory research methods may improve the quality of research projects and clinical services, but the extent to which an MBC system designed for and with autistic people may be feasible and acceptable is unclear. The current findings from autistic clients suggested that the MBC-AUT system was a feasible and acceptable system associated with many benefits to various therapeutic processes. Clinicians also noted the benefits of the implementation of the MBC-AUT system in clinical practice. Notably, important barriers to the use of the MBC-AUT system were raised by clients and clinicians, although several potential solutions were presented to address these barriers and reduce client and clinician burden. As autistic clients continue to seek psychological services amid social landscapes of increasing complexity (e.g. the COVID-19 pandemic), efforts to enhance the delivery of psychotherapy for this vulnerable population are critical.
Supplemental Material
sj-docx-1-aut-10.1177_13623613221143587 – Supplemental material for Community-guided measurement-based care for autistic youth and adults receiving psychotherapy: A conceptual overview and pilot implementation study of MBC-AUT
Supplemental material, sj-docx-1-aut-10.1177_13623613221143587 for Community-guided measurement-based care for autistic youth and adults receiving psychotherapy: A conceptual overview and pilot implementation study of MBC-AUT by Jessica M Schwartzman, Zachary J Williams, Ann V Paterson, Alexandra X Jacobs and Blythe A Corbett in Autism
Supplemental Material
sj-docx-2-aut-10.1177_13623613221143587 – Supplemental material for Community-guided measurement-based care for autistic youth and adults receiving psychotherapy: A conceptual overview and pilot implementation study of MBC-AUT
Supplemental material, sj-docx-2-aut-10.1177_13623613221143587 for Community-guided measurement-based care for autistic youth and adults receiving psychotherapy: A conceptual overview and pilot implementation study of MBC-AUT by Jessica M Schwartzman, Zachary J Williams, Ann V Paterson, Alexandra X Jacobs and Blythe A Corbett in Autism
Footnotes
Acknowledgements
The authors would like to thank the autistic adults of the Neurodivergent Advisory Team for their contributions to the design and interpretation of this project, as well as the autistic clients for their generous participation in this study. In addition, the authors wish to thank Brianna Lewis, Ph.D., Joshua Smith, M.D., Carissa Cascio, Ph.D., Margaret Benningfield, M.D., and Cheryl Cobb, M.D. for their feedback on the initial design of the system. Importantly, the authors acknowledge Dr. Stephan Heckers, M.D., the Chair of the Department of Psychiatry and Behavioral Sciences at VUMC, for his support of the design and implementation of the measurement-based care system in the present study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Zachary Williams has received consulting fees from Roche, Autism Speaks, and the May Institute. He owns stock in Axsome Therapeutics, and he also serves on the family advisory committee of the Autism Speaks Autism Care Network Vanderbilt site and on the autistic researcher review board of the Autism Intervention Research Network on Physical Health (AIR-P). The other authors have no conflicts of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received departmental support from the Department of Psychiatry and Behavioral Sciences at Vanderbilt University Medical Center (VUMC), and core support from the National Center for Advancing Translational Sciences (CTSA UL1TR000445) to utilize the REDCap system.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.