
Abstract
Studies are emerging documenting the experience of fatigue, exhaustion and loss of functioning that has long been described by autistic adults as autistic burnout. New assessment tools are needed to enable identification and diagnosis. Here, we sought to identify factors associated with severity, develop an autistic burnout assessment and test the prepublication AASPIRE Autistic Burnout Measure tool. A co-produced survey of 141 autistic adults with experience of autistic burnout (98% above cut-off for depression) was subjected to exploratory factor analysis and scale reduction to identify a grouping of Autistic Burnout Severity Items. Autistic Burnout Severity Items showed strong overall internal consistency and acceptable internal consistency across four factors. Masking and depression were associated with the Autistic Burnout Severity Items, once variation in alexithymia, interoception, repetitive behaviours, sensory sensitivities and autism severity had been adjusted for. There is some suggestion that the Autistic Burnout Measure may not be as robust as the Autistic Burnout Severity Items, particularly as it showed a significant relationship with depression but not masking. Our findings alongside recent literature highlight a core phenomenon, comprising exhaustion, withdrawal and cognitive overload, associated with stressors potentially unique to autistic people. Further disambiguation from autistic shutdown and other conditions is needed in work towards the measurement of autistic burnout.
Lay abstract
Autistic burnout has been talked about by autistic adults for some time on blogs and in social media. Now, research describes fatigue, exhaustion and other related symptoms experienced by autistic people. We need new ways to help identify autistic burnout. In this study, we tested a new questionnaire called the AASPIRE Autistic Burnout Measure, and we investigated things that are linked to worse autistic burnout. We also trialled a group of Autistic Burnout Severity Items that we made. Working with an autistic researcher, we made the Autistic Burnout Severity Items based on published definitions of autistic burnout. Autistic adults (n = 141) who had experienced autistic burnout completed an online survey. We found that autistic burnout was connected to masking and depression. The Autistic Burnout Measure tool was associated with depression but not with masking. It was not very accurate in telling apart participants who were currently experiencing burnout versus those who were reporting on their past experience. The Autistic Burnout Severity Items might have problems with subscales adding together to measure autistic burnout. More work is needed on how to measure autistic burnout. Our research and other recent studies show autistic people experience a combination of exhaustion, withdrawal and problems with their concentration and thinking. Burnout seems to be linked to the stress experienced by autistic people in their daily lives. We need more research to understand the difference between autistic burnout and other conditions and experiences. We need to develop assessment tools that can help identify this burnout.
Introduction
Research on autistic burnout is only just emerging in the literature, despite being discussed by autistic adults online for more than a decade. Terminology, and to a degree the formulation, is derived from occupational burnout, defined in the International Classification of Diseases, 11th Revision (ICD-11) (World Health Organization, 2019) as a condition characterised by exhaustion, perceived reduced professional efficacy and mental distance from one’s job, although this conceptualisation is not uncontested (Hillert et al., 2020). To our knowledge, only four studies have focused specifically on autistic burnout (Higgins et al., 2021; Mantzalas et al., 2021; Phung et al., 2021; Raymaker et al., 2020), although studies on the related phenomena such as fatigue in autistic children (Keville et al., 2021), experiences of autistic students during COVID-19 (Cage & McManemy, 2022) and experiences of masking (or ‘camouflaging’) in autism (Pearson & Rose, 2021) have referenced autistic burnout. All four studies on autistic burnout, despite some differences, have largely described core elements of exhaustion, withdrawal, a heightening of autistic traits and reduced functioning. The emerging literature arguing for the existence of an autistic burnout syndrome, and its devastating impacts, highlights the need for further research and development.
All studies to date have identified characteristics that they argue distinguish autistic burnout from depression and occupational burnout. Raymaker et al. (2020) were the first to publish a definition of autistic burnout. They gathered data from (n = 10) interviews as well secondary analysis of (n = 19) social media accounts and (n = 9) interviews on employment. Their definition included reduced tolerance of stimuli alongside the typical burnout characteristics of exhaustion and reduced function. Higgins et al. (2021), based on the findings from a grounded Delphi method study of autistic adults (N = 23) positioned as experts by lived experience, derived a somewhat different definition. Higgins et al. (2021) argued for interpersonal withdrawal as an essential feature, alongside exhaustion as the core characteristics of autistic burnout, with reduced function, confusion or problems with executive function, and increased intensity of autistic traits, including sensory sensitivities.
Subsequent studies have proposed a variety of potential risk factors. Mantzalas et al. (2021), analysing 1127 posts from Twitter and the Wrong Planet website, endorsed the findings of earlier studies, though also highlighted the potential roles of alexithymia (i.e. problems identifying emotions) and interoception (i.e. sensing of internal body states). Mantzalas et al. (2022) further put forward a theoretical framework intending to provide a holistic perspective outlining potential measurable direct and indirect pathways to autistic burnout. This framework drew from the social-relational model of disability, the neurodiversity paradigm, the job demands-resources model and the conservation of resources theory relating to burnout and stress. Previously, masking and unaccommodating neurotypical environments primarily were the proposed contributing factors, but Mantzalas et al.’s framework attempted to identify multiple potential social, environmental, psychological and individual risk and protective factors, including satisfaction with life, stigma and stimming. In their review and conceptual analysis of masking, Pearson and Rose (2021) discussed social context and stigma driving the need to mask autistic behaviours, such as stimming, and the role alexithymia plays in not being able to identify when stressors are accumulating. The impact of masking on overall mental well-being is a focus of several recent studies (e.g. Cage & Troxell-Whitman, 2019; Cassidy & Rodgers, 2017; Hull et al., 2019). All studies on autistic burnout have highlighted the role of masking.
Where other studies have focused on adult samples, Phung et al. (2021) interviewed eight autistic children and youth (aged 8–18 years, median 14 years) about experiences of autistic burnout, shutdown, meltdown and inertia using definitions based on previous studies (Belek, 2019; Raymaker et al., 2020; Welch et al., 2021). They defined autistic burnout as a state of ‘severe and chronic exhaustion’ (p. 2), inertia as a state of being ‘stuck’ (p. 2) and unable to physically engage in desired activities, meltdowns as a state of being ‘entirely overwhelmed’ (p. 2), expressed externally with a lack of control and cumulative stress, and shutdowns being ‘internal expressions’ of ‘emotional pain’ precipitating withdrawal from surrounding environments (p. 2). Using the language of the autistic children and youth, the phenomena were renamed with burnout as feeling exhausted, inertia as feeling stuck, meltdown as feeling out of control and shutdowns as feeling frozen. Autistic young people used metaphors such as a ‘heavy blanket’, ‘hard piece of dough’ or ‘old computer’ to describe their burnout experiences in particular: ‘a slow old computer that’s trying to run Google Chrome . . . it just uses up a lot of RAM’ (p. 7). Yet, Phung et al. (2021) also found that participants’ descriptions were unclear in distinguishing burnout from shutdown and inertia, though cautioned that young people may not have had the vocabulary needed for clearer delineation and were more commonly exposed to specific terms such as ‘meltdown’.
All four studies to date (Higgins et al., 2021; Mantzalas et al., 2021; Phung et al., 2021; Raymaker et al., 2020) have identified characteristics suggesting a distinction of autistic burnout from depression and occupational burnout. Given the ongoing debate in the literature outside of autism regarding the separation, or lack thereof, of occupational burnout from depression (e.g. (Bianchi et al.,2020, 2021; Parker & Tavella, 2021; Tavella et al., 2020, 2021; Tavella & Parker, 2020; Verkuilen et al., 2021), this is of particular importance. These authors have used various meta-analytic, structural equation and factor analytic approaches, and argued on both sides of a problematic overlap of depression and burnout. In autistic burnout research, one participant in Higgins et al. (2021) reported ‘depression is the side effect with burnout being the cause’ (p. 2362). Studies emerging on autistic burnout, together, propose the existence of a potentially unique autistic burnout syndrome and further suggest that existing measures of occupational burnout may not be suitable in this context, or at least, would not address the full range of symptomatology.
The current study
In the current study, we sought to (1) determine indicators of autistic burnout severity and validity of the Academic Autism Spectrum Partnership in Research and Education (AASPIRE) group Autistic Burnout Measure (AABM) and (2) investigate conceptually related factors that might be associated with autistic burnout severity. To achieve these aims, we conducted an online mixed-methods Autistic Burnout Survey, combining items based on emerging definitions with standardised measures. To measure autistic burnout severity itself, we used a prepublication version of the AASPIRE AABM. The AABM was developed from a sample of 80 participants, with details forthcoming. Given some discrepancies between the Raymaker et al.’s and Higgins et al.’s definitions of burnout, we also constructed our own measure of autistic burnout severity. The findings of Mantzalas et al. (2021) and hypothesising of Higgins et al. (2021) and others (Pearson & Rose, 2021) suggest high-incidence stressors in autism may drive autistic burnout. Hence, we included measures of camouflaging (masking), difficulties with interoception, alexithymia, repetitive behaviours and sensory sensitivities, as these characteristics are amplified in autistic people. We also included a measure of depression, given questions around differential diagnosis in both the autistic and non-autistic burnout literature.
Methods
Participants
Volunteer participants were recruited through advertisement distributed by social media, the Australian Longitudinal Study of Autism in Adulthood (ALSAA; Arnold et al., 2019) newsletter, autism organisation websites and newsletters. As an incentive, participants could enter a prize draw for one of four US$100 gift cards. Participants had an independent clinical diagnosis of autism and self-identified an episode of autistic burnout. The consent form made reference to the definition of autistic burnout by Raymaker et al. (2020) and the survey included a screening question ‘Have you had an experience of autistic burnout?’. The survey was anonymous, and N = 141 participants provided useable data, that is, more complete responses beyond the opening demographic questions. Only a small proportion of males participated (16%, n = 22; n = 3 missing), with higher numbers of females (64%, n = 88) and participants reporting another gender (20%, n = 28). The mean age was 40.2 years (SD = 10.8, range: 20.3–71.0; n = 8 missing). Two participants (1%) scored 64 and 65 on the Autism Spectrum Quotient-28 (AQ-28), just below the >65 cut-off which has a sensitivity of 97%, but were nevertheless included in the analysis.
Approximately half of the participants were employed, with the majority having completed high school and gaining a bachelor’s degree or higher (see Table 1). The majority of the sample were diagnosed recently in adulthood: the mean age at diagnosis was 36.9 years (SD = 12.4, range: 3.4–67.1), and the mean years since diagnosis were 3.4 years (SD = 5.3, range: 0–27). Current co-occurring mental health conditions were common, with 113 participants (78%) reporting an internalising mental health condition (i.e. mental health conditions where people internalise their problems, such as depression or anxiety). Responses were collected from October 2020 to April 2021, during which time COVID-19 related lockdowns were occurring. Further demographics and co-occurring mental health conditions are presented in Table 1.
Demographics and mental health conditions (N = 141).

SD: standard deviation.
Other conditions reported more than once included premenstrual dysphoric disorder and dissociative identity disorder.
Measures
Two unvalidated measures of autistic burnout were employed alongside several standardised measures of conceptually related constructs in the Autistic Burnout Survey. This article reports on a portion of the survey findings focused on the measurement of autistic burnout. We attend to participants’ responses to the open-ended questions in a separate paper (Arnold et al., in press).
Autistic burnout
We employed two measures of autistic burnout, one that we developed and the second created by Raymaker et al. (2020). In our Autistic Burnout Survey, led by autistic peer researcher J.M.H., we developed a series of items based on a combination of the Higgins et al.’s (2021) and Raymaker et al.’s (2020) definitions. Forty-eight of these items questioned participants on ‘During my most recent (or current) autistic burnout experience’ and were related to elements in one or both definitions (e.g. exhaustion, withdrawal, executive functioning, masking), including items relating to meltdowns for the purpose of determining divergent validity (see Table 2). All quantitative survey items were scored on 7-point Likert agreement scale ranging from ‘1’ (strongly agree) to ‘7’ (strongly disagree) with an additional ‘not applicable’ (NA) option. Each question block was followed by open-ended items probing for additional detail or missing concept coverage. J.M.H. determined agreement scale design with open-ended follow-up questions to allow autistic participants a full range of response options and the ability to explain their responses. J.M.H., S.R.C.A. and A.D. developed items, which were then reviewed by all co-authors. For example, given that interpersonal withdrawal was a central characteristic in the Higgins et al.’s (2021) definition, Item 7 asked ‘During my most recent (or current) autistic burnout experience . . . I withdrew from social situations’. Exploratory factor analysis (EFA) and iterative scale reduction applied to these items revealed a grouping of 20 Autistic Burnout Severity Items (ABSI) across four factors (see Table 2). The process to identify the ABSI is described subsequently. These items showed good overall internal consistency (Cronbach’s α = 0.88) with acceptable internal consistency for each factor (range: 0.73–0.86). However, internal consistency at the subscale level was questionable (α = 0.66), which cautions against assuming unidimensionality of the scale. NA responses were set to missing, and those participants who had more than two NA or missing items, were excluded from ABSI total score (n = 2). In subsequent analyses, an average score across answered items was taken to maximise total observations, giving a possible total score ranging from 1 (most severe) to 7 (least severe).
Autistic burnout experience items ordered by highest mean agreement.

SD: standard deviation; ABSI: Autistic Burnout Severity Items.
Item included in the ABSI Exhaustion factor.
Item included in the ABSI Overwhelm and Withdrawal factor.
Item included in the ABSI Heightened Autistic Self-Awareness factor.
Item included in the ABSI Cognitive Disruption factor.
Second, we gathered data using a prepublication version of the AASPIRE Autistic Burnout Measure (AABM) with permission from Raymaker and colleagues. Building on work conducted by Raymaker et al. (2020), this 27-item tool asked participants to rate items on a 5-point Likert scale, ranging from ‘0’ (strongly agree) to ‘4’ (strongly disagree), 1 yielding a total possible score range of 0–108. Participants respond to items in reference to ‘the past three months’ with item content such as ‘I’ve wanted to isolate myself from others more often than I usually do’ and ‘I’ve felt more mentally exhausted than I usually do’. Lower total sum scores are indicative of greater risk of being in autistic burnout.
Autism severity and screening
The widely used 50-item AQ tool (Baron-Cohen et al., 2001), originally developed to identify autistic traits in adults of at least average intelligence, uses a 4-point Likert scale, ranging from ‘1’ (definitely agree) to ‘4’ (definitely disagree). The AQ-50 has been critiqued on several grounds, including its length, factor structure and whether it is suitable to use as an autism severity measure (Lundqvist & Lindner, 2017). In this study, we gathered subsets of the original 50-item AQ. This included the 28 items selected by Hoekstra et al. (2011) in creating the abridged AQ-28, which we used to determine whether participants met cut-off for autism. The AQ-28 using a cut-off of >65 demonstrates high sensitivity (97%) and specificity (82%) for distinguishing between autistic and non-autistic participants. We also gathered the 12 items (4 not included in the AQ-28) identified by Lundqvist & Lindner, (2017) as having utility to measure autism severity. Good internal consistency was evident in this sample for both the 28-item (α = 0.82) and 12-item (α = 0.81) extracts.
Autistic dispositions
A range of measures were gathered to identify potential unique stressors correlated with autistic burnout, including the Adult Repetitive Behaviour Questionnaire-2 (RBQ-2A). Adapted from the Repetitive Behaviours Questionnaire-2 designed for children, the RBQ-2A (Barrett et al., 2015) is a 20-item tool scored on 4- and 3-point frequency or severity scales, with higher scores indicating greater severity. Following previous studies (Barrett et al., 2015, 2018), the 4-point scaled items were collapsed to a 3-point scale, then a total sum score was used giving a possible score range of 20–60. The RBQ-2A also provides two factor scores of repetitive motor behaviour and insistence of sameness, although only the total score indicating levels of repetitive behaviours was used in this study. It has shown convergent validity with the AQ-50, and good internal consistency in non-autistic (α = 0.73) and autistic samples (α = 0.91), which was replicated in the current sample (α = 0.90).
The Glasgow Sensory Questionnaire (GSQ) (Robertson & Simmons, 2013) is a 42-item tool assessing hyper- and hypo-sensitivities. Items are scored on a 5-point frequency scale, ranging from ‘0’ (never) to ‘4’ (always), giving a maximum total sensory score of 168, with higher scores indicating higher amounts of sensitivities. A single-factor total sensory score has strong internal consistency (α = 0.94), which we replicated in the current sample (α = 0.91).
The Camouflaging Autistic Traits Questionnaire (CAT-Q) (Hull et al., 2019) is the first measure of social camouflaging / masking behaviours, that is, the strategies and actions used by autistic individuals to reduce their autistic characteristics in the context of social interactions. This 25-item scale is scored on a 7-point Likert scale, ranging from ‘1’ (strongly disagree) to ‘7’ (strongly agree) with five reverse-scored items, given a possible score range of 25–175, with higher scores indicating higher amounts of camouflaging. It has shown acceptable test–retest reliability (r = 0.77) and good internal consistency (α = 0.94), replicated in our sample (α = 0.90). The total sum score was used in our study, although subdomains of compensation, masking and assimilation can be calculated. Convergent validity has been tested in autistic (N = 306) samples in comparison with autistic traits (r = 0.34; p < 0.001) using the Broad Autism Phenotype Questionnaire (BAPQ; Hurley et al., 2007), well-being (r = −0.16; p < 0.05) using the Warwick–Edinburgh Mental Well-being Scale (WEMBS; Tennant et al., 2007), anxiety (r = 0.35; p < 0.001) using the Generalised Anxiety Disorder-7 (GAD-7; Spitzer et al., 2006), social anxiety (r = 0.44; p < 0.001) using the Liebowitz Social Anxiety Scale (LSAS; Liebowitz, 1987) and depression (r = 0.28; p < 0.001) using the Patient Health Questionnaire-9 (PHQ-9).
The Interoception Sensory Questionnaire (ISQ) (Fiene et al., 2018) was developed to measure autistic adults’ perception and interpretation of interoceptive sense. The original 20-item tool had a 7-point Likert scale response option, ranging from ‘1’ (not at all true of me) to ‘7’ (very true of me), and showed strong internal consistency (Cronbach’s α = 0.96) for a single factor, strong correlations with a measure of alexithymia (r = 0.76) and significant correlations with a measure of interoceptive awareness (range: −0.28 to −0.15). Subsequently, Suzman et al. (2021) developed a revised 8-item version using a condensed 5-point Likert scale response option and noted multiple redundant item pairs. They also developed an online scoring calculator (https://asdmeasures.shinyapps.io/ISQ_score/) to facilitate the use of latent trait scores. Due to clerical error, we did not gather Item 20 of the original ISQ; however, we substituted the redundant paired Item 19 and calculated ISQ-8 latent trait scores using the online calculator from Suzman et al. (2021). Suzman found strong internal consistency of the ISQ-8 using coefficient omega (ω = 0.90), which was replicated in the eight items from our sample (ω = 0.92)
The recently developed Perth Alexithymia Questionnaire (PAQ) (Preece et al., 2018) is a 24-item tool using a 7-point Likert scale, ranging from ‘1’ (strongly disagree) to ‘7’ (strongly agree) giving a possible score range of 24–168; higher scores indicate higher levels of alexithymia – an inability to identify and describe one’s emotions. Its four subscales and all composite scores show good internal consistency (α = 0.87–0.95), which was replicated in this sample (0.90–0.97). It has shown good convergent validity with expected relationships with emotional regulation measures and measures of depression and anxiety, as well as divergent validity from overall distress. It has also shown good convergent validity (Preece et al., 2020) with the widely used 20-item Toronto Alexithymia Scale (TAS-20).
Depression
The PHQ-9 (Kroenke et al., 2010) measures the severity of depressive symptoms and is used to identify clinical levels of major depressive disorder. Each of its nine items is scored on a 4-point frequency scale: ‘0’ (not at all), ‘1’ (several days), ‘2’ (more than half the days) and ‘3’ (nearly every day). When summed, the scale generates a continuous score ranging from 0 to 27, with higher scores indicating greater depression severity (Kroenke et al. 2010). The PHQ-9 demonstrates excellent internal consistency (α = 0.89) and test–retest reliability (r = 0.84) (Kroenke et al. 2001), and acceptable sensitivity and specificity (>79%) in detecting depressive disorder (Cassidy et al. 2018). It showed good internal consistency in this sample (α = 0.90). It has been previously validated in an autistic sample (Arnold et al., 2019).
Data analysis
All quantitative data were analysed using Stata 15, with a web-based version of the R cocor package (Diedenhofen & Musch, 2015) used for correlation comparisons. Survey item responses are presented ordered by highest mean scores. To identify the ABSI, EFA using the principal factors method and Pearson’s correlations with promax rotation was used. Factor retention decisions were based primarily on parallel analysis with 1000 repetitions using 95th percentile eigenvalues (using the STATA ‘paran’ command), though multiple criteria (Izquierdo et al., 2014), including visual inspection of eigenvalues, review of the scree plot, Velicer’s minimum average partial and clinical judgement of resulting structure were considered. Criteria for item retention were <0.3 for low loading and <0.2 difference for high cross-loading. Items were removed sequentially as described below.
After checking for collinearity and normality, regression models examined associations with the ABSI and the AABM as dependent variables. Given the limited observations available, only total scores from assessment tools were used to contain the total number of predictor variables within regression models. We repeated these analyses limiting the sample to participants who were currently experiencing or who had experienced burnout in the past 3 months (n = 103; 73%) to align with the scoring of the AABM. We also completed a receiver operating characteristic (ROC) analysis of AABM scores versus participants who reported burnout within the past 3 months.
Community involvement
This project was co-led with autistic peer researcher J.M.H., who has lived experience of autistic burnout. In relation to this article, J.M.H. co-produced the research questions, funding application, survey tool, named factors resulting from the EFA, reviewed all interpretations of findings and co-authored outputs. J.M.H.’s major impact on the conduct and outcomes of the study are acknowledged with her position as joint first author.
Results
Identifying the ABSI
To create an indicator of severity of autistic burnout, we applied EFA to the 48 items from the Autistic Burnout Survey (see Table 2). Immediately, items that were included relating to meltdown grouped together (Item 38 onwards) and were dropped from further rounds of factor analysis. Items 10 and 11 were related to school or academic tasks and were not included in the analysis due to the lower number of observations. The Kaiser–Meyer–Olkin (KMO) test (KMO = 0.80) and Bartlett’s test of sphericity (χ2(595) = 2246.05, p < 0.001) indicated data for the remaining items that were acceptable for factor analysis. A four-factor solution was evident subsequently and confirmed at each round of analysis, with items dropped sequentially (37, 35, 25, 13, 14, 20, 6, 9, 23, 32, 36, 28, 30) if they did not load (>0.3) on any factor (37, 35, 25, 32), had high cross-loading (<0.2 difference) (13, 14, 20, 6, 9, 23), or low loadings (<0.3) after removing cross-loading items (36, 28, 30). Factors were named Exhaustion, Cognitive Disruption, Heightened Autistic Self-Awareness, and Overwhelm and Withdrawal and together explained 95% of variance in the reduced item set. Heightened Autistic Self-Awareness encompassed both increased sensory sensitivity and increased self-awareness of autistic characteristics, and Cognitive Disruption encompassed memory problems and confusion. Remaining items and factor loadings are reported in Table 2. There was a moderate significant correlation between the ABSI and the removed meltdown items (r = 0.42, p < 0.001). Initial factor loadings for all 48 items are reported in Supplementary Table 2, and factor loadings across all factors for the final 20-item solution in Supplementary Table 3.
Relationships with ABSI
Across the sample, very high rates of depression were evident, with 98% (n = 131) of the complete responses (n = 7 missing) above cut-off for clinical depression on the PHQ-9. Many participants (n = 60, 44%) endorsed the PHQ-9 item relating to suicide ideation or self-harm. Similarly, 53% (n = 69) reported high levels of alexithymia on the PAQ, while a minority (12%; n = 12) had low levels of alexithymia (n = 10 missing). Descriptive statistics for standardised tool and burnout indicators are presented in Table 3.
Descriptive statistics.
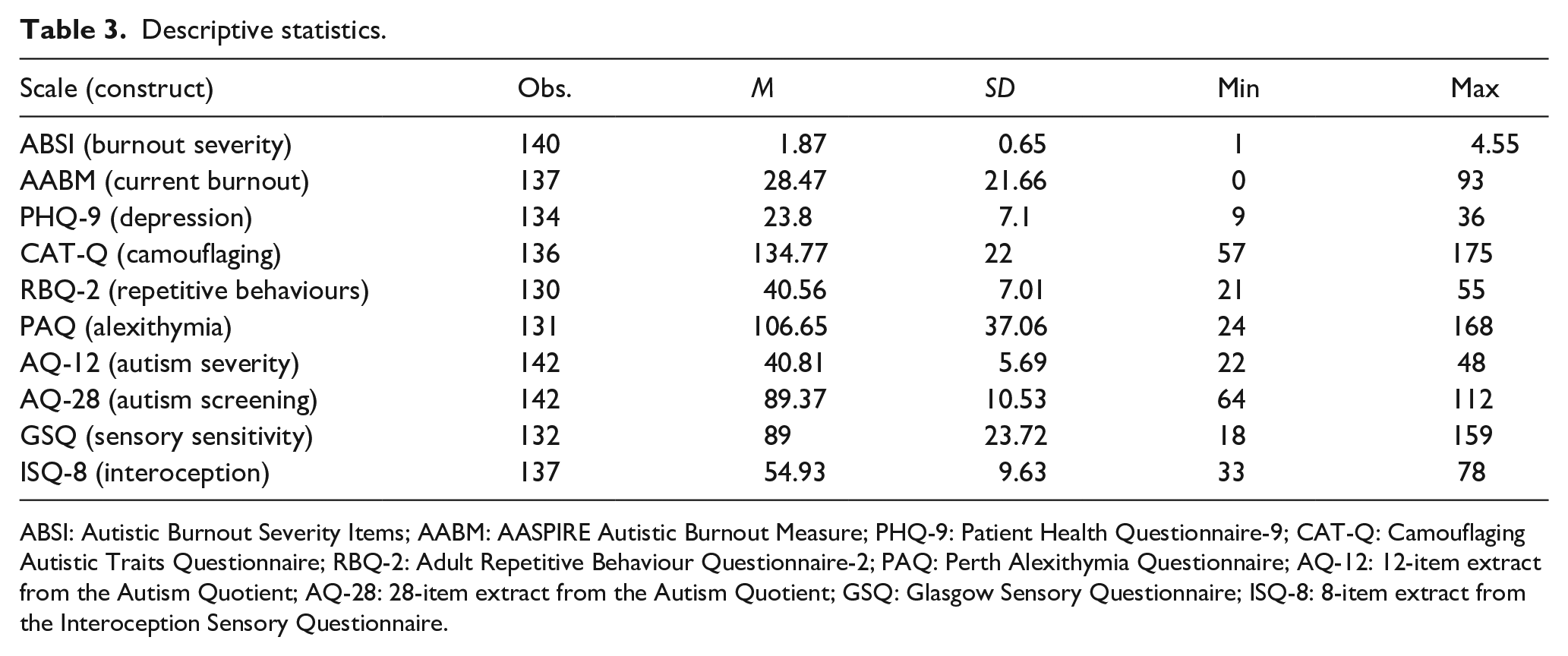
ABSI: Autistic Burnout Severity Items; AABM: AASPIRE Autistic Burnout Measure; PHQ-9: Patient Health Questionnaire-9; CAT-Q: Camouflaging Autistic Traits Questionnaire; RBQ-2: Adult Repetitive Behaviour Questionnaire-2; PAQ: Perth Alexithymia Questionnaire; AQ-12: 12-item extract from the Autism Quotient; AQ-28: 28-item extract from the Autism Quotient; GSQ: Glasgow Sensory Questionnaire; ISQ-8: 8-item extract from the Interoception Sensory Questionnaire.
Correlations between measures are presented in Table 4. Both burnout indicators showed significant correlations across all supplementary measures, except, unexpectedly, the AABM did not correlate with the CAT-Q. We note that the ABSI subdomains showed some marginally stronger correlations with discriminant measures over other ABSI subdomains; however, they were all most strongly correlated with the ABSI total score. These marginally stronger correlations with discriminant measures were not significantly different when analysed with a backtransformed average Fisher’s Z procedure, following Hittner et al. (2003). We also report item-level Spearman’s correlations with the PHQ-9, ABSI meltdown items and Spearman’s item-rest correlations for ABSI domain and total scores in Supplementary Table 4. We note ABSI items were more strongly correlated with ABSI domain and total scores than with the PHQ-9, including for additional partial correlations that were conducted between ABSI domain scores and ABSI total score controlling for variation in PHQ-9 scores.
Pairwise correlations (bottom diagonal) and confidence intervals of correlations (top diagonal).
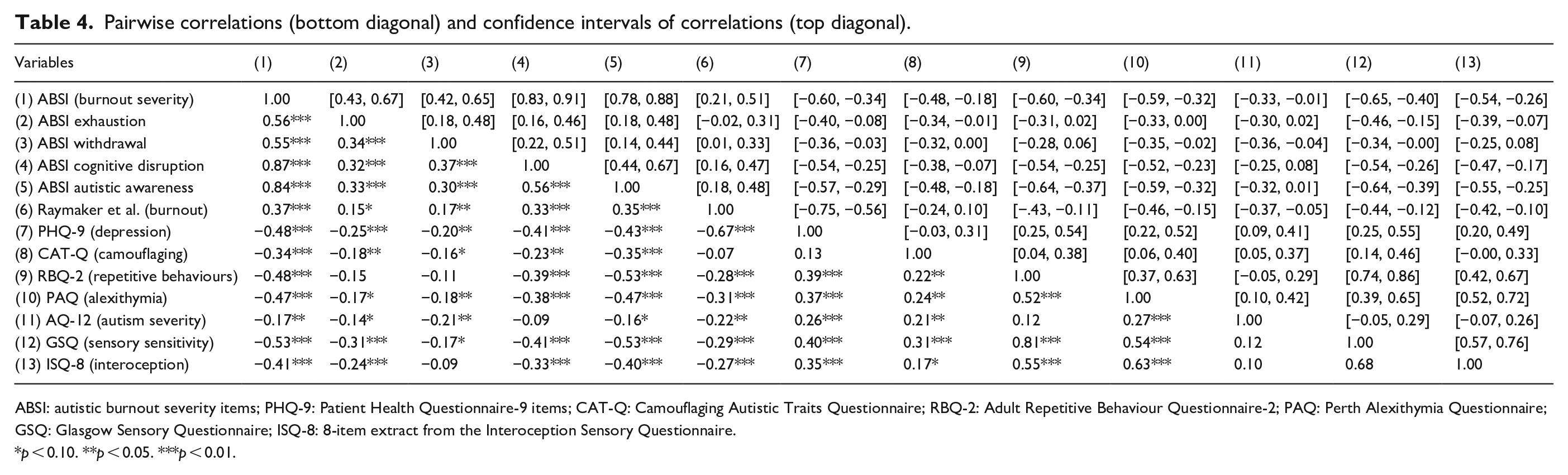
ABSI: autistic burnout severity items; PHQ-9: Patient Health Questionnaire-9 items; CAT-Q: Camouflaging Autistic Traits Questionnaire; RBQ-2: Adult Repetitive Behaviour Questionnaire-2; PAQ: Perth Alexithymia Questionnaire; GSQ: Glasgow Sensory Questionnaire; ISQ-8: 8-item extract from the Interoception Sensory Questionnaire.
p < 0.10. **p < 0.05. ***p < 0.01.
Linear regression with ABSI scores as the outcome with all supplementary measures as predictors, showed significant relationships with scores on depression and camouflaging measures (see Table 5). These significant associations remained when the sample was limited to those who reported having experienced a burnout within the past 3 months. To maximise observations, we also repeated the regression using multiple imputation with 20 imputations and obtained similar results (see Supplementary Materials Table 4). Given concerns as to the unidimensionality of the ABSI, we repeated the linear regression predicting ABSI subdomain totals (see Supplementary Materials Tables 5–9). Patterns of associations changed when predicting subdomain scores, with depression only significantly related in the ABSI Cognitive and ABSI Heightened Autistic Self-Awareness models, and camouflaging and repetitive behaviours significant in the ABSI awareness model.
Linear regression predicting ABSI (n = 106).
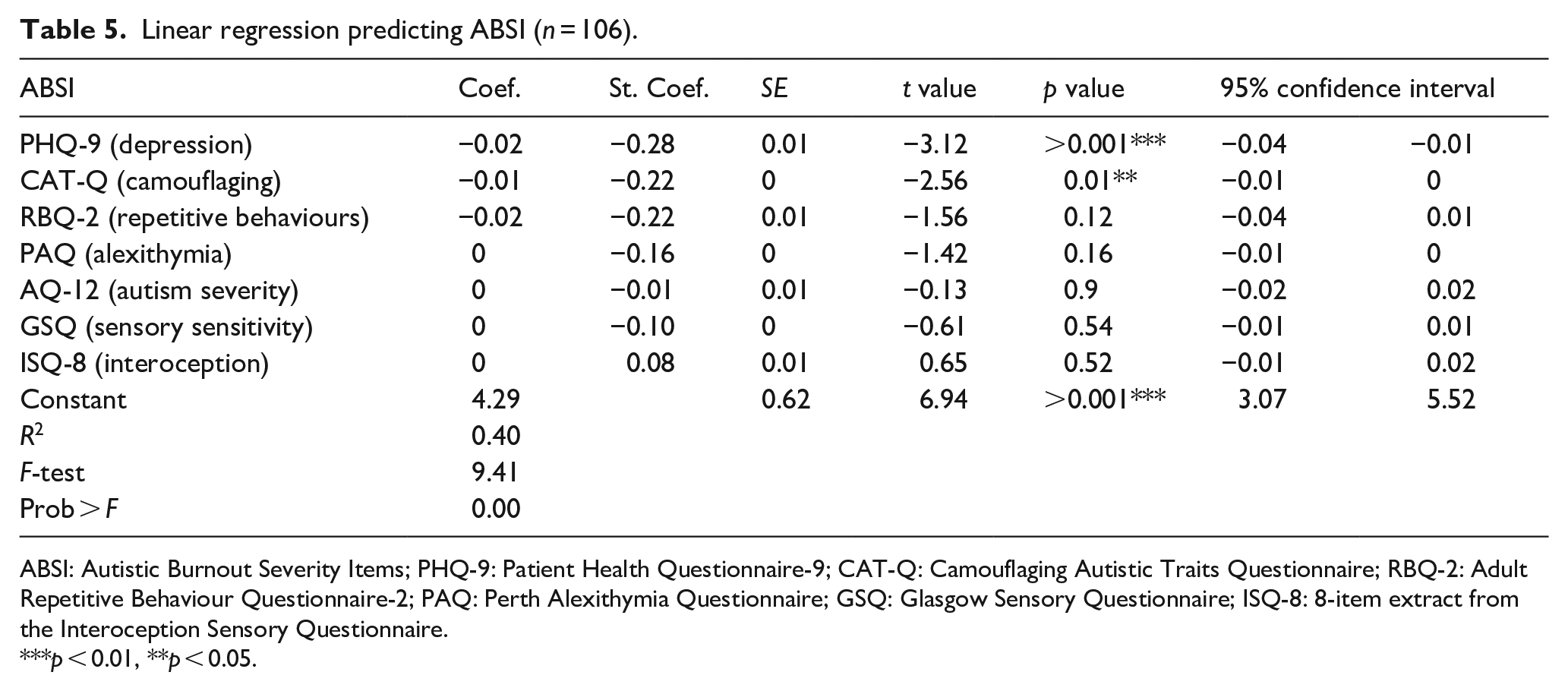
ABSI: Autistic Burnout Severity Items; PHQ-9: Patient Health Questionnaire-9; CAT-Q: Camouflaging Autistic Traits Questionnaire; RBQ-2: Adult Repetitive Behaviour Questionnaire-2; PAQ: Perth Alexithymia Questionnaire; GSQ: Glasgow Sensory Questionnaire; ISQ-8: 8-item extract from the Interoception Sensory Questionnaire.
p < 0.01, **p < 0.05.
Relationships and sensitivity of the AABM
Linear regression with AABM as the outcome variable, limited to those who had experienced burnout in the last 3 months, with all supplementary measures as predictors, showed only depression as a significant predictor (see Table 6). The pattern of findings did not change when all participants were included. To maximise observations, we also repeated the regression using multiple imputation with 20 imputations and obtained similar results (see Supplementary Materials Table 10).
Linear regression predicting AABM for those experiencing burnout within last 3 months (n = 76).

ABSI: Autistic Burnout Severity Items; PHQ-9: Patient Health Questionnaire-9; CAT-Q: Camouflaging Autistic Traits Questionnaire; RBQ-2: Adult Repetitive Behaviour Questionnaire-2; PAQ: Perth Alexithymia Questionnaire; GSQ: Glasgow Sensory Questionnaire; ISQ-8: 8-item extract from the Interoception Sensory Questionnaire.
p < 0.05. ***p < 0.01.
With regard to our final research question on the predictive validity of the AABM, the AABM asks participants to report on their experiences in the past 3 months. Overlaying kernel density estimations of those who had (n = 103) and had not (n = 33) experienced autistic burnout in the past 3 months suggested poor specificity of the AABM (see Figure 1). Receiver operative curve analysis suggested poor specificity (area under the curve (AUC) = 0.661; n = 136).

Kernel density scores on AABM versus have you been burnt out in the last 3 months?
Discussion
Emerging research is investigating the existence of an autistic burnout syndrome. From a survey of autistic adults with experience of autistic burnout, we used EFA to construct a preliminary measure of autistic burnout, the ABSI, and, once controlling for other factors, found masking and depression to be associated with more severe autistic burnout. Our findings must be considered with caution given the potential lack of unidimensionality of the ABSI. The ABSI and AABM total scores were only moderatly significantly correlated. The AABM tool may be problematic in not showing associations with masking in multivariate regression analysis and having poor specificity in determining participants currently or recently in burnout, compared to those who perceive they are not currently in burnout. Our finding of masking associated with the ABSI aligns with the testimonies reported in emerging literature of adults who are compelled to mask their autistic features enduring stressors and fatigue leading to autistic burnout. However, masking being a precursor rather than a feature of autistic burnout experiences may explain its lack of association with the AABM. Work is needed to develop and validate assessment tools in this area, with this study providing potential directions for item development. Longitudinal work is needed to determine causative rather than associative factors, including the interrelationship and divergent validity of burnout and depression in autism, especially considering there were some high correlations between ABSI items and subdomains with depression scores. Of importance, all other measures gathered in this study were significantly correlated with the ABSI, and future research with larger samples is needed to determine the significance of these associations.
The EFA in this study, alongside emerging literature (Higgins et al., 2021; Mantzalas et al., 2021; Phung et al., 2021; Raymaker et al., 2020), highlights the need to further investigate the phenomenon of autistic burnout. Our study, similar to other published literature, suggests that burnout is distinct from meltdowns, although its disambiguation from depression remains currently unclear. Some of the ABSI domains showed marginally stronger correlation with depression than other subdomains, although overall were more strongly correlated with the ABSI total score. Unidimensionality of the ABSI is questionable, and regression models predicting subdomain scores showed varying patterns of relationships. Also not explored in our design is the separation or interrelatedness of autistic burnout, shutdowns, catatonia (i.e. a disorder characterised in the Diagnostic and Statistical Manual of Mental Disorders (5th ed., DSM-5) as the presence of three of the following symptoms: catalepsy, waxy flexibility, stupor, mutism, negativism, agitation, posturing, stereotypes, mannerism, grimacing, echolalia and echopraxia; (Ghaziuddin et al., 2021; Vaquerizo-Serrano et al., 2022) and inertia (Buckle et al., 2021), which appears less clear. Particularly some of our participants’ experiences included changes in motivation, mutism or stupor. The children and youth in Phung et al. (2021) did not report a clear distinction, with burnout, shutdowns and inertia all being thematically grouped as ‘exhausted and/or frozen’ (p. 6). Of interest, there is content alignment between the shutdowns and burnout described by Phung et al.’s (2021) participants with the content of ABSI items. Together with the unclear duration and both chronic and acute experiences of autistic burnout (Arnold et al., in press; Higgins et al., 2021), emerging literature may point towards an overarching autistic exhaustion syndrome which encompasses burnout, shutdown and inertia, occurring across the lifespan, and is possibly related to autistic catatonia, though more research in this area is needed.
Conceptual issues in the criteria for autistic burnout may require more work before the development of autistic burnout measurement tools. The prepublication AABM tool appeared somewhat problematic in two areas. First, it shows no relation to masking, which is indicated in the literature and in our findings with the ABSI. We note that the literature discusses masking as a stressor leading to autistic burnout onset, and it is plausible that masking is a component of a complex causal pathway where it is no longer significant once in the experience of burnout. Second, having poor specificity in determining those who report currently being in autistic burnout, although our sample ideally would have included autistic adults who had never experienced autistic burnout. Although, the identification of the ABSI did not follow all processes ideal in the development of assessment tools (Boateng et al., 2018), it may provide useful material for future assessment tool development in this area. Better conceptualisation and screening tools will help identify autistic burnout sooner, and could, in some instances, prevent misdiagnoses (see Arnold et al., in press). We deliberately refer to autistic burnout as a syndrome, while acknowledging limitations of preliminary findings from emerging studies, and that this terminology is potentially stigmatising and the problematic history of the medical model within autism (Pellicano & den Houting, 2022). We recommend that autistic burnout is considered a diagnosable condition. Doing so may assist in reducing misdiagnoses and in developing validated prevention, treatment and support pathways. This would be particularly important to clinicians without extensive autism knowledge. There are potential risks though situating autistic burnout within the psychiatric nosology, with similarity to the pathologisation of depression (Ratnayake, 2022). Further research is needed with sensitivity to the most beneficial approaches to supporting autistic adults.
Masking and depression being the most predictive factors in regression models give some direction towards supports and prevention of autistic burnout. The significance of masking highlights the locus of stressors driving autistic burnout. This challenges us to promote social change, build more neurodiverse spaces and accommodation within the neurotypical world, reducing the need to mask. Relatedly, encouragement from autistic pride movements and active inclusion (Weaver et al., 2021) from neurotypical people might lead some autistic adults to lessen their masking or unmask.
The interrelationship of autistic burnout with depression appears to mirror the relationship of occupational burnout and depression, and the ongoing, years-long conceptual uncertainty between these disorders. Of interest, the Sydney Burnout Measure, which measures occupational burnout, developed by Parker et al. (2021), shows good sensitivity but poor specificity and requires clinical reasoning to exclude depression in diagnosing occupational burnout. Similar to arguments presented by Parker and Tavella (2021), such as differences in precipitant, attribution of causation, severity of depression, primary symptom and anhedonia, we would contend there are important differences between depression and autistic burnout, that they could occur independently, though likely that an autistic person who is experiencing burnout is more at risk of developing depression. For example, many participants highlight an onset associated with stressors, such as masking, with a primary symptom of exhaustion, not depression. This will be another area for future disambiguation. Furthermore, Parker and Tavella (2022) suggest that ‘widespread acceptance by the lay community of burnout as a distinct and relatable syndrome suggest it is worthy of independent designation’ (p. 1065), and we believe this is mirrored in the autistic community for autistic burnout. Future work may benefit from the inclusion of clinical reasoning, as suggested by Parker et al. (2021), to disambiguate autistic burnout from depression and other conditions that could be misdiagnosed. Future research should also consider the various approaches from the occupational burnout literature that have examined the depression and burnout overlap (e.g. Bianchi et al.,2020, 2021; Tavella et al., 2021; Verkuilen et al., 2021). We note that Tavella et al. (2021) argue that the presence of depression symptoms in burnout does not suggest that burnout and depression are synonymous. Tavella et al. (2021) applied bifactor analyses to a set of 137 items generated from existing burnout and depression measures, arriving at a 34-item general burnout factor that included only four depression-related items and may present a model for future autistic burnout work. Also missing from our study and needed in future research is an exploration of the unique stressors arising from an unaccommodating neurotypical systems and structures reportedly leading to autistic burnout, and the relationships of autistic burnout with anxiety and social anxiety.
Limitations
We were unable to screen participants for a confirmed diagnosis of autistic burnout, as there are currently no validated definitions or screening tools for the syndrome. However, we believe there is increasing evidence of an underlying core phenomenon given emerging studies and the strong responses of participants in this study. Given resource constraints and the geographic spread of Australia, we were unable to clinically confirm autism diagnosis, Although all, but two, participants were above cut-off on the AQ-28. The small proportion of male participants is of interest, and although potentially a limitation, larger studies not recruiting specifically for autistic burnout are needed to determine if there are relationships between gender and prevalence of this syndrome. Alternatively, the frequent reports of higher female participation in online autism research may underlie the gender ratio in this study (Arnold et al., 2019). The recency of diagnosis, gender ratios and mean age in this sample may also be a product of the sampling strategy, being an online survey that was promoted via social media. The study was promoted via the ALSAA newsletter, the ALSAA study had an inclusion criterion of age 25+ years. Including promotion through social media, those more recently diagnosed are possibly more likely to be engaged with online autism forums.
Ideally, to identify items that can be used to measure autistic burnout severity, a larger sample and larger item pool would be used. Furthermore, beyond good internal consistency and generally strong item-total correlations, we have limited data to support the use of a single ABSI total score. We attempted to conduct a bifactor analysis, although the model did not converge, likely due to the number of items and sample size (Morgan et al., 2015). Furthermore, calculating overall internal consistency using subscale scores was not strong, questioning the unidimensionality of the scale. Significant correlations between ABSI subscales scores and depression scores raise questions of the inclusion of some ABSI subscales in measuring autistic burnout, although as argued above, further work is needed to understand the depression / autistic burnout phenomenology. Given the limited justification for using the ABSI total score, our findings suggest that factors related with autistic burnout should be considered with some caution. As noted, future work is needed to further validate diagnostic criteria for autistic burnout and to develop reliable and sensitive measurement tools. A particular complexity to be addressed in future research is the both chronic and brief nature of burnout experiences reported by autistic adults (Higgins et al., 2021, under review). Ideally, the ROC analysis of the AABM would have been done in a sample that included autistic adults who report never having experienced autistic burnout and included stronger indicators in addition to the single item asking when the person most recently experienced burnout, acknowledging the impact that alexithymia may have on the recognition of burnout state. However, we posit the findings have sufficient strength to suggest that more work is needed on measurement tool development.
Although many participants endorsed the suicidal ideation item on the PHQ-9, being an anonymous survey, we were unable to reach out and provide support to these participants. Potentially anonymity allows participants to safely reveal their experiences, with more work needed on the known high rates of suicidal ideation in autistic adults (Hedley et al., 2018). Building better understanding of autistic burnout and related phenomena may be one component of these efforts.
Conclusion
Autistic people report that autistic burnout is a debilitating condition. This condition is only recently being investigated in the scientific literature. More work is needed to develop valid screening and measurement tools, including further definitional work around duration and relationships with shutdown and inertia. In common with the occupational burnout construct, further work is needed to disambiguate autistic burnout from depression and other conditions that are potential misdiagnoses. The significant relationship of masking with autistic burnout highlights core phenomena of exhaustion, withdrawal and cognitive overload in autistic people driven by stressors amplified in autistic people. Efforts to reduce the stress and frequency of masking are needed, including acceptance and valuing of autistic people in society, increase in accommodations for autistic people and promotion of autistic pride.
Supplemental Material
sj-docx-1-aut-10.1177_13623613221147401 – Supplemental material for Towards the measurement of autistic burnout
Supplemental material, sj-docx-1-aut-10.1177_13623613221147401 for Towards the measurement of autistic burnout by Samuel RC Arnold, Julianne M Higgins, Janelle Weise, Aishani Desai, Elizabeth Pellicano and Julian N Trollor in Autism
Supplemental Material
sj-docx-2-aut-10.1177_13623613221147401 – Supplemental material for Towards the measurement of autistic burnout
Supplemental material, sj-docx-2-aut-10.1177_13623613221147401 for Towards the measurement of autistic burnout by Samuel RC Arnold, Julianne M Higgins, Janelle Weise, Aishani Desai, Elizabeth Pellicano and Julian N Trollor in Autism
Footnotes
Acknowledgements
The authors thank Dora Raymaker, the Academic Autistic Spectrum Partnership in Research and Education (AASPIRE) group and colleagues for sharing a prepublication version of the AASPIRE Autistic Burnout Measure that was used in this study. They also thank Yunhe Huang for her support in data analysis and discussing concepts.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The authors acknowledge the financial support of the Cooperative Research Centre for Living with Autism (Autism CRC), established and supported under the Australian Government’s Cooperative Research Centres Program.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.