
Abstract
Moderate feeding problems affect many children with autism spectrum disorder and often co-occur with disruptive mealtime behaviors. Although parent-mediated interventions have shown promise to support feeding problems, research has primarily occurred within randomized controlled trials when delivered by highly trained clinicians in specialty clinics. Thus, the alignment of these approaches within community settings is unclear. To address this limitation, this study explored adaptations to a parent-mediated intervention, Managing Eating Aversions and Limited Variety (i.e. MEAL Plan), to enhance its adoption, implementation, and sustainment within community settings, including factors that may support or hinder its translation. Participants were 14 multidisciplinary providers who attended one of the three workgroups that included semi-structured focus groups regarding the fit of MEAL Plan in their practice setting. Thematic analysis was used to determine emergent themes, which fell into the domains of content, contextual considerations, and training needs. Specific themes included the appropriateness MEAL Plan for autistic and non-autistic children, adaptations to MEAL Plan delivery, billing considerations, agency-level support, and the format of ongoing training and consultation. By proactively responding to these factors, it may be possible to enhance the implementation and sustainability of parent-mediated interventions, including MEAL Plan, within community practices that support autistic children.
Lay abstract
Moderate feeding problems and disruptive mealtime behaviors are common in children with autism spectrum disorder. Although parent-mediated interventions are able to support feeding problems in autistic children, most research has occurred within specialty clinics when delivered by highly trained clinicians. Thus, the fit of these interventions within community settings is not clear. To address this limitation, this study explored adaptations to a parent-mediated intervention, Managing Eating Aversions and Limited Variety (i.e. MEAL Plan), to improve its fit and use within community settings. Participants were 14 multidisciplinary providers who attended one of the three intensive workgroups that included focus groups about the fit of MEAL Plan in their practice setting. Qualitative analysis was used to determine the main themes that came up within the focus groups. Specific themes included the appropriateness MEAL Plan for autistic and non-autistic children, how providers might adapt their delivery of MEAL Plan, billing and insurance considerations, administrator support for MEAL Plan, and the content and format of ongoing training and consultation. By proactively considering and responding to these factors, it may be possible to enhance MEAL Plan so that it is better able to be delivered and sustained within community practices that support autistic children.
Keywords
Introduction
The detected prevalence of children with autism spectrum disorder (ASD) has steadily increased over the past two decades to the current estimate of 1 per 44 children with a male-to-female ratio of 4.2 to 1 (Maenner et al., 2020; Yeargin-Allsopp et al., 2003). Over this period, the evidence base for supporting the core features of autism and common co-occurring challenges has also expanded (Hume et al., 2021; Sandbank et al., 2020). Despite advances in intervention efficacy, access to high quality treatments remains a challenge for autistic children and their families (Drahota et al., 2020; Lord et al., 2022; Pickard et al., 2018). Against the backdrop of challenges accessing quality services, there is mounting interest in translating evidence-based practices (EBPs) for ASD into community settings (Boyd et al., 2022; Dingfelder & Mandell, 2011; Lord et al., 2022). As in many other health fields, there is a significant lag between the empirical support for autism interventions and their eventual translation to community settings (Bauer & Kirchner, 2020; Boyd et al., 2022). Moreover, even with concerted translation efforts, EBPs may not be sustained following community training efforts (Barnett et al., 2021).
Within the autism field, there are several known challenges to implementing EBPs in community settings. These challenges include provider shortages and turnover, inconsistent fidelity in treatment delivery, inadequate administrative support in community agencies, and broader systemic barriers such as insurance coverage (Boyd et al., 2022; Brookman-Frazee et al., 2020; Melgarejo et al., 2020; Pickard et al., 2023; Suhrheinrich et al., 2021). These challenges underscore the importance of careful attention to the feasibility, acceptability, and scalability of EBPs prior to investing the time and resources needed to implement them in community settings (Bauer & Kirchner, 2020; Boyd et al., 2022). Attention to the factors that promote or hinder translation efforts in partnership with community providers may expedite the implementation and sustainment of evidence-based interventions for children with ASD in community settings. To date, most community implementation efforts for autistic children have centered on interventions that support the core features of ASD, including social and communication skills (Melgarejo et al., 2020; Rieth et al., 2022; Stahmer et al., 2020), and common co-occurring mental and behavioral health challenges (Brookman-Frazee et al., 2021; Reaven et al., 2022). There is also growing need and demand for access to EBPs that support other co-occurring problems such as feeding problems in children with ASD.
Autistic children have an estimated fivefold increased likelihood of feeding problems than children in the general pediatric population (Sharp et al., 2013). Across a range of mild to severe, the most common feeding problem in children with ASD is food selectivity. Severe food selectivity in autistic children, characterized by refusal to eat one or more food groups, warrants intensive intervention in day hospital or inpatient settings due to the adverse effects on growth, nutrition, and overall health (Sharp et al., 2017; Volkert et al., 2021). By contrast, moderate food selectivity, characterized by limited intake of items in one or more food groups (e.g. eating two or fewer fruits), which elevates the risk for nutrient deficiency if further restriction occurs (Sharp & Postorino, 2017). Thus, although children with moderate food selectivity may not have urgent nutrition related medical problems, the low intake of nutrient-dense foods may have short- and long-term adverse health effects. In addition, parental efforts to expand the child’s diet almost invariably results in disruptive mealtime behavior that may include verbal protest, crying, pushing away food and tantrums (Burrell et al., 2023; Johnson et al., 2019; Sharp et al., 2019). In the absence of intervention, moderate food selectivity can persist into adolescence and adulthood (Kuschner et al., 2015).
Over the past decade, there has been growing interest in the application of parent-mediated approaches to manage food selectivity in autistic children (Aponte et al., 2019). The rationale for parent-mediated intervention in managing food selectivity in autistic children is supported by the large body of evidence confirming the efficacy of parent-mediated interventions for disruptive behavior in young children with ASD (Postorino et al., 2017; Tarver et al., 2019). In a previous study, our team developed and evaluated a structured, parent-mediated intervention for children with ASD and moderate food selectivity. In that study, 38 children (ages 3 to 8) were randomly assigned to Managing Eating Aversions and Limited Variety (i.e. MEAL Plan) or a parent education program for 16 weeks. Treatments were delivered in a group format that included 4–5 parents per group. MEAL Plan was deemed acceptable as evidenced by low attrition (i.e. 16%) and high attendance (i.e. 87%). In addition, MEAL Plan was superior to Parent Education in reducing disruptive mealtime behavior and expanding dietary variety in children with ASD and moderate feeding problems (Sharp et al., 2019). Our findings were consistent with other reports on parent-mediated intervention for moderate feeding problems in autistic children (Johnson et al., 2019).
Although the efficacy of structured, parent-mediated interventions for food selectivity is promising, research to date has exclusively occurred in randomized controlled trials by highly trained clinicians in specialty clinics (Johnson et al., 2019; Sharp et al., 2019). Thus, the fit of these approaches in community settings where many children with ASD and moderate feeding problems are served, is not clear. In a survey of 419 providers that included speech language pathologists, occupational therapists, psychologists, Board Certified Behavior Analysts and registered dietitians, 90% of respondents indicated that they treat children with ASD and feeding problems (Burrell et al., 2021). Respondents also reported using a variety of behavioral, sensory, oral-motor, and nutritional approaches to manage feeding problems in this population. A high percentage of respondents indicated willingness to try a structured, parent-mediated intervention for co-occurring feeding problems (Burrell et al., 2021).
Taken together, available research suggests that translating a parent-mediated intervention into community practice may be timely. However, implementing psychosocial and behavioral interventions in community settings is a complex process requiring proactive attention to support intervention fit and adaptation (Aarons et al., 2012; Stirman et al., 2019). Moreover, when guided by implementation science frameworks (e.g. PRISM, Feldstein & Glasgow, 2008), this pre-implementation effort can align EBPs with community practice and identify key factors that may help or hinder implementation. Factors that may be important to consider within frameworks such as PRISM, include the community demand for the intervention, organizational/agency support for adopting new interventions, the insurance landscape for the intervention, provider attitudes toward the intervention, and intervention feasibility and acceptability (Feldstein & Glasgow, 2008). Finally, proactive efforts to plan for community implementation are maximized when conducted in partnership with community stakeholders, including providers representing diverse practice settings. These partnerships have the potential to increase the external validity and relevance of research findings to community settings (Hursting & Chambers, 2021).
Here, we present qualitative study results on the fit of a parent-mediated intervention for children with ASD and moderate food selectivity (i.e. MEAL Plan) in an interdisciplinary sample of community providers. This study explored adaptations to MEAL Plan that could enhance its adoption, implementation, and sustainment within these settings. A second aim was to examine factors that may support or hinder the translation of MEAL Plan into community practice. This second aim, grounded in the PRISM framework (Feldstein & Glasgow, 2008), considered how factors, such as community demand, provider background, and agency support, might affect the translation of MEAL Plan into community practice.
Methods
Design
This study was part of a larger project approved by the Emory Institutional Review Board (IRB). This larger project began with a national, web-based survey of providers who treat children with ASD and feeding problems (Burrell et al., 2021). The survey included an invitation to attend a 3-h virtual seminar on feeding problems in children with ASD. Interested survey respondents who provided an email address indicating interest in the virtual seminar, were sent registration information. The 3-h seminar provided background information on food selectivity in children with ASD, an overview of MEAL Plan and the results of the randomized trial of MEAL Plan.
Upon conclusion of the virtual seminar, attendees were invited to participate in this study, which included an intensive 10- to 12-h workgroup that included a detailed review of the MEAL Plan. In addition to MEAL Plan review, each workgroup included a pre and post focus group session to gather insights from participants on translating MEAL Plan into community settings. A total of three intensive workgroups were conducted virtually over Zoom with a total of 14 providers (i.e. 4–6 providers per group). Purposive sampling was used to ensure that each workgroup included a mix of providers who reported in our previous research to support autistic children with feeding challenges, including speech language pathologists (SLPs), occupational therapists (OTs), psychologists, board certified behavior analysts (BCBAs), and registered dieticians (RDs). Figure 1 presents a flow diagram of participation.
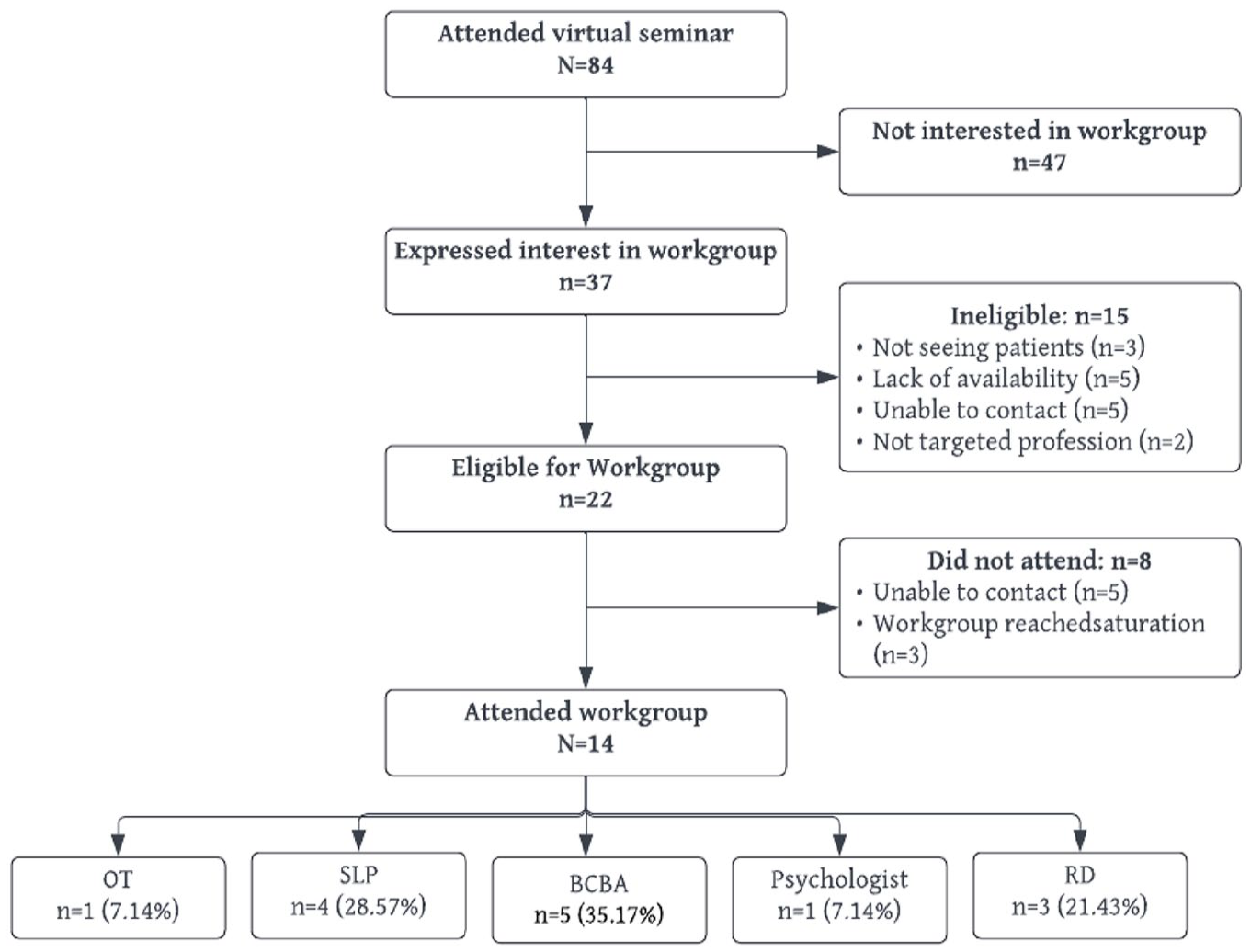
Diagram depicting study flow and participation.
Participants
Eligibility for the intensive virtual workgroups included prior participation in a MEAL Plan seminar, self-reported experience in providing services to children with ASD and feeding problems, ability to read and write in English, and availability for one of the three planned 10- to12-h workgroups (spread over three sessions). Clinicians who did not have an active caseload or who did not independently bill for services, such as Registered Behavior Technicians or Speech Language Pathology Assistants, were not included. Fourteen providers participated, including five BCBAs, four SLPs, one psychologist, three RDs, and one OT. Participating providers resided in eight states including California, Florida, Georgia, Louisiana, Missouri, Ohio, South Dakota, and Washington.
Intervention
MEAL Plan is a structured, 10-session, 16-week, parent-mediated intervention designed to reduce disruptive mealtime behavior and expand dietary diversity in autistic children (ages 3–8 years) with a limited dietary variety. The 10 sessions focus on three core areas: foundational feeding behaviors, disruptive mealtime behavior, and food selectivity. The manual includes therapist scripts, caregiver handouts and in-session activities, and homework assignments. Sessions include didactic content with the parent-only in the first four sessions followed by instruction and live coaching with parent and child in sessions 5–10.
Approximately 1 week before the first workgroup session, participants received an electronic copy of the MEAL Plan manual used in the prior randomized trial. This draft version included a table of contents, an introduction describing the structure of the program and the patient population. As noted, the manual also included therapist scripts, parent handouts, and examples of in-session activities and homework. Participants were asked to review subsections of the manual (e.g. the introduction and the first two sessions prior to the first meeting) prior to each meeting.
Procedures
Prior to the virtual workgroups, all participants completed a demographic and clinical questionnaire. All intensive workgroups were structured in the same manner such that they began with informed consent, followed by a semi-structured focus group regarding providers’ current practice setting and openness to adopting new empirically supported treatments. After the first focus group, providers participated in a detailed review of the MEAL Plan protocol and concluded the virtual workgroup with a second semi-structured focus group regarding translating a structured intervention such as MEAL Plan into their practice setting.
Demographic and Clinical Questionnaire
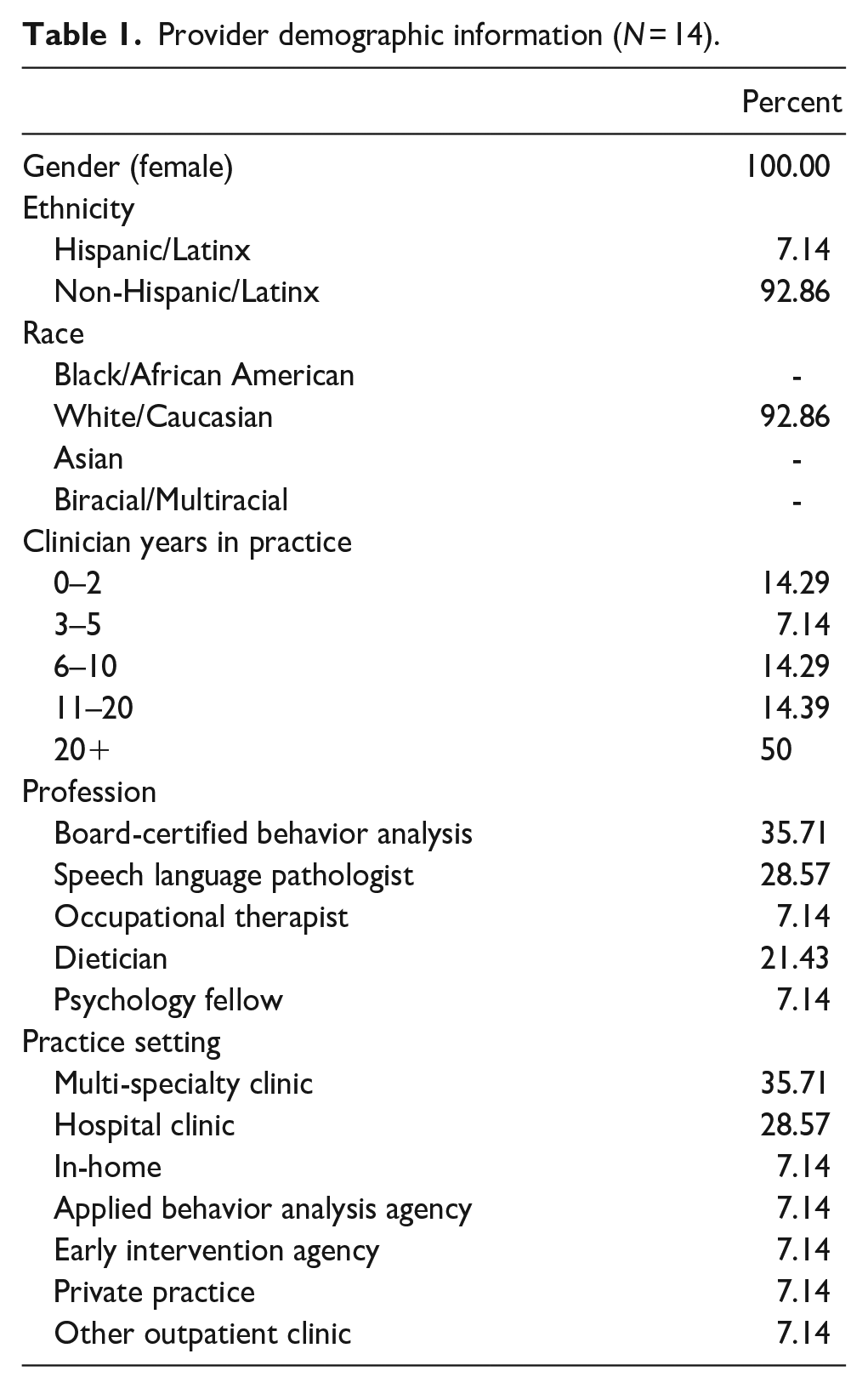
Prior to the workgroup session, participants completed a 10-item survey developed for the study. This form included items on gender, race, ethnicity, professional discipline, and years in practice. It also included questions about age range of patient population, number of active patients with ASD, number with ASD and feeding problems, types of feeding problems, treatment modality (e.g. therapist-led and parent-led), and treatment approach (e.g. behavioral, nutrition, and oral-motor). Table 1 presents demographic characteristics reported by participants.
Provider demographic information (N = 14).
Semi-structured focus group guides
An IRB-approved semi-structured interview guide was used to facilitate focus group discussions (see Supplemental Material). As noted, focus groups were held at the open and close of each workgroup. This structure was intentional so that descriptive data could be gathered from providers in the first focus group, with allotted time for a much deeper discussion of MEAL Plan implementation after the manual had been reviewed. Each focus group lasted approximately 60 min. The opening focus group introduced study team and focus group members, reviewed focus group guidelines, explored participants’ practice setting, discussed provider experience and approaches to management of feeding problems in children with ASD. For example, we asked participants to describe their practice setting (e.g. academic, hospital-based, and community clinic), practice size (e.g. number of patients/therapists), provider types within the practice settings (e.g. single discipline vs multiple disciplines), the patient population (e.g. ASD only vs mixed population), and the practice billing structure (e.g. self-pay, private insurance, and Medicaid). Participants were also asked about models of treatment used in the practice, approach to treatment planning, and openness to learning new treatments for feeding problems in children with ASD.
The focus group conducted after the conclusion of the virtual workgroup explored the feasibility and acceptability of implementing MEAL Plan in community practice settings. Providers were asked to reflect on prior experience with adopting new treatment approaches and attitudes toward structured, parent-mediated interventions such as MEAL Plan. Consistent with the PRISM framework, group discussions included consideration of factors that could influence the success or breakdown of implementing a program such as MEAL Plan. These factors included the perceived demand for a program like MEAL Plan, goodness of fit (e.g. treatment duration, treatment modality), requirements for provider training and supervision, and billing (Feldstein & Glasgow, 2008). Providers were also asked to offer modifications in MEAL Plan or the manual that could improve its alignment in community practice.
Data analysis
All focus groups were audio recorded and transcribed verbatim. Transcripts were reviewed by qualitative experts on the study team (S.B. and K.P.) using an initial conventional content analysis approach to identify codes from the data followed by a directed content analysis approach (Hsieh & Shannon, 2005). Consensus coding was used for reliability with a third qualitative expert available to resolve any discrepancies in coding. Thematic analysis of focus group material was also informed by field notes taken during the MEAL Plan workgroup that added nuance to identified themes. Peer debriefing sessions were held after each work group with all members of the research staff to discuss preliminary themes and allow reflection. These peer debriefing sessions continued throughout the data analysis phase and later served as a way to confirm data saturation was achieved. The focus group material and field notes were organized under three major themes: content, context and training (Stirman et al., 2019).
Following analysis, we engaged participants in virtual member-checking sessions to review the validity of our findings through (Elliott et al., 1999). During member-checking sessions, participants were presented with main qualitative themes, exemplar quotes representing these themes, and possible groupings of themes (Table 2). Over three member-checking sessions, workshop participants offered feedback on the qualitative themes. Participants concurred with the content and interpretation of identified themes and provided additional feedback on identified themes. For example, participants offered suggestions on the format of training and comments on essential content of the training. These impressions were incorporated into the results.
Primary themes and definitions.
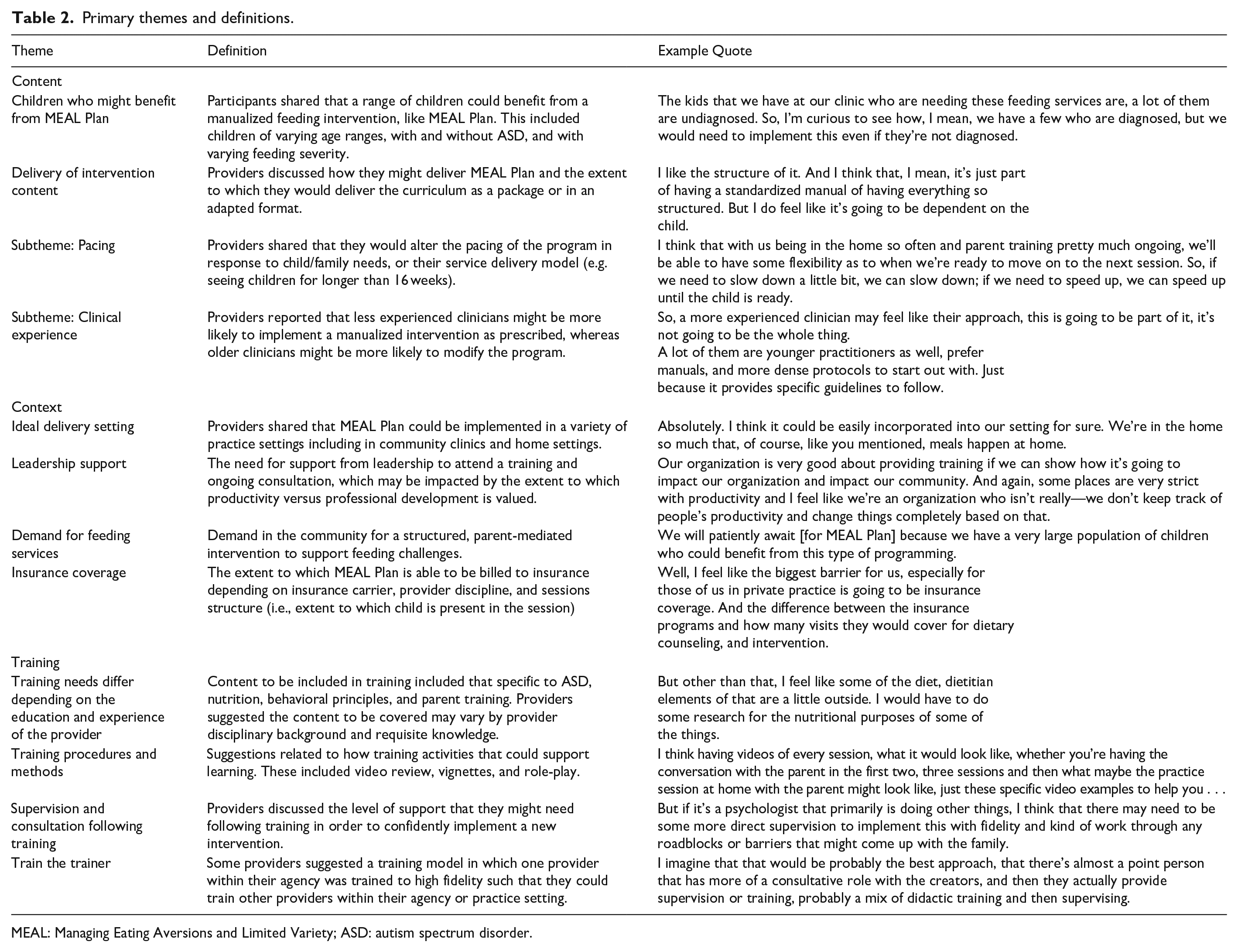
MEAL: Managing Eating Aversions and Limited Variety; ASD: autism spectrum disorder.
Community involvement statement
This study involved qualitative interviews with community providers serving young children with feeding problems across a range of practice settings. Member checking was conducted to ensure the accuracy of study findings. Other aspects of the study (e.g. study design, qualitative analysis, and manuscript writing) were not conducted with involvement from community stakeholders or participants.
Results
Content
Participants affirmed the value of delivering the MEAL Plan manual as a structured intervention and suggested expanding the protocol to include a clinically more diverse group of children than the strictly defined sample in the original randomized trial. For example, participants suggested that the MEAL Plan manual could support children without a confirmed medical diagnosis of ASD. Clinicians also often described key factors, including a clinician’s level of experience and differences in child and family’s specific needs that could influence the delivery of a structured intervention such as MEAL Plan.
Children who might benefit from MEAL Plan
The original randomized trial of MEAL Plan included children 3–8 years with a confirmed diagnosis of ASD and carefully defined moderate food selectivity. In contrast to the strictly defined sample in the randomized trial, workgroup participants expressed that MEAL Plan would be relevant to children without a diagnosis of ASD and children below age 3: The kids that we have at our clinic who are needing these feeding services are, a lot of them are undiagnosed. So, I’m curious to see how, I mean, we have a few who are diagnosed, but we would need to implement this even if they’re not diagnosed.
Participants also recommended a broader definition of moderate feeding problems. For example, the randomized trial excluded children on feeding supplements (e.g. PediaSure®). Participants noted that because this product and other similar products are commonly used in community practice, children on supplements should not be categorically excluded from MEAL Plan.
Delivery of intervention content
Most providers agreed that a structured, empirically supported program such as MEAL Plan should be delivered as intended. Although some providers predicted that they would deliver the entire program as intended, others suggested that clinical characteristics of the child and family might call for adaptations in program delivery.
Pacing
Several workgroup participants proposed greater flexibility in the pacing of the 16-week MEAL Plan program based on child- and family-specific needs. For example, some parents might need one or more MEAL Plan sessions repeated to learn and apply specific behavioral techniques. This may be especially important for foundational sessions such as strategies designed to keep the child at the table. Pacing could also be affected by the need to integrate the feeding intervention with the child’s ongoing treatment plan, which may include other therapeutic goals. Providers anticipated that the need to repeat sessions or intersperse MEAL Plan with ongoing treatment would likely extend the program beyond the 16-week duration: I think the clinician needs to have the ability to be flexible with the sessions, and how fast or slow that you might move through it. And I like that [MEAL Plan] has the option of slowing down or speeding up depending on the child.
Clinician experience
Clinicians indicated that level of experience with ASD and feeding problems could affect delivery of MEAL Plan. Specific areas mentioned included prior experience with parent-mediated interventions for disruptive behavior, feeding interventions, and experience with nutritional guidance. Participants noted that clinical experience could also influence the level of flexibility in the delivery of MEAL Plan. For example, clinicians with less experience might be more likely to deliver MEAL Plan as intended with minimal adaptation. By contrast, more experienced clinicians might be more likely to modify MEAL Plan pacing and session sequence, and, perhaps, more likely to blend MEAL Plan with other oral-motor approaches: . . . younger, less-experienced clinicians who are interested in working with feeding and swallowing, . . . they do want something that says, “Step 1, do this; Step 2, do this.” So, it’s nice for them to have a guidebook like that. Some of your more seasoned therapists, they’re going to be resistant to it.
Context
Participants cited information on the community practice setting and institutional factors that might influence the feasibility and acceptability of adopting a structured feeding intervention such as MEAL Plan. Recurring themes included (1) Ideal MEAL Plan delivery settings; (2) level of leadership support within a practice setting; (3) demand for feeding services in the community; and (4) insurance coverage.
Ideal delivery settings
Providers consistently described a variety of practice settings that could support the delivery of a structured feeding intervention such as MEAL Plan. These included outpatient clinics, early intervention systems (e.g. Birth-to-Three), schools, and telehealth. BCBAs also indicated that MEAL Plan could be nested in home-based applied behavior analysis (ABA) services.
Leadership support
Workgroup participants acknowledged the importance of solid administrative support to introduce and maintain the delivery of a structured intervention for feeding problems in children with ASD. Leadership support essentials included approving provider training and ongoing consultation. Some participants noted that the administrative tension between productivity and professional development could affect the level of support for training and supervision on adoption of an evidence-based intervention: Our organization is very good about providing training if we can show how it’s going to impact our organization and impact our community . . . some places are very strict with productivity and I feel like we’re an organization who isn’t really—we don’t keep track of people’s productivity and change things completely based on that.
Demand for feeding services in the community
Participants uniformly confirmed ample need and demand for a structured feeding intervention. Participants described high demand of structured feeding interventions in their practice given the high frequency of requests for feeding services and the scarcity of tested interventions indicated the need.
Insurance coverage
Despite the demand for a structured feeding intervention, participants noted that insurance coverage could influence the accessibility of a feeding intervention such as MEAL Plan in some practice settings. For example, SLPs noted that several MEAL Plan sessions described in the manual were delivered to caregivers without children present. This format was not consistent with usual speech therapy billing, which requires the presence of the child in treatment sessions: The biggest barrier for me being in a clinic that is only speech therapy, occupational therapy, and physical therapy is going to be reimbursement with those first four sessions being . . . so heavy on parent coaching. If there’s not an optional piece or a very clear way for therapists to incorporate working with the child in some way where we can document what we were doing, it’s going to be hard for people to use it if they may not get reimbursed for it.
Although billing requirements could affect the feasibility of delivering MEAL Plan, participants offered adaptations to meet these requirements. For example, speech language pathologists noted that the child and parent could be included in all sessions consistent with billing conventions.
Training
Participating providers were asked about the ideal training methods and format for a structured, parent-mediated feeding intervention. In addition to initial training, participants also considered the role of ongoing supervision and consultation to support program implementation.
Training needs differ depending on the education and experience of the provider
Participants acknowledged that the ideal content for training included content specific to ASD, nutrition, behavioral principles and techniques, and parent coaching strategies. However, the focus of training would almost certainly vary by provider discipline and clinical experience. For example, BCBAs might have a solid foundation in application of behavioral techniques, but perhaps less experience on parent coaching and nutrition. By contrast, SLPs noted that colleagues in their discipline would likely need training on behavioral principles and techniques to deliver MEAL Plan successfully: I agree that speech pathologists and occupational therapists . . . would need some more background and more emphasis on some of those behavioral principles; that might be a little bit boring for some of the BCBAs in the room or psychologists.
Training procedures and methods
In addition to training differences by discipline, participants offered suggestions on a range of specific activities that could enhance training on MEAL Plan. Suggestions included interactive activities such as video review of common challenges in the application of MEAL Plan, inclusion of illustrative case vignettes in the manual, and role-play to test drive specific techniques. Despite recognition that providers may have different training needs, participants expressed preference for interdisciplinary training to promote exchange across disciplines (as implied in the above quotation). This theme was reiterated in member-checking sessions.
Supervision and consultation following training
To foster the successful implementation of MEAL Plan in community practice settings, participants, without exception, expressed the need for supervision and consultation following training on MEAL Plan. Participants predicted that community providers would require practical advice on how to deliver specific behavioral or parent training techniques. This post-training supervision could be provided by an external MEAL Plan expert or a clinician in the practice setting who achieved deeper experience with the intervention: They’re still learning, they’re not experts and they’re not comfortable doing feeding therapy on their own. So, it’s now getting their feet wet and getting support while doing it.
Train the trainer
To support the sustained use of a structured intervention such as MEAL Plan in community practice, several participants suggested a train-the-trainer model. In this model, one clinician in the practice would acquire high proficiency on the intervention and then serve as a resource for other clinicians in the practice.
Discussion
The heightened risk of feeding problems such as food selectivity in autistic children underscores the need to translate EBPs into community practice settings. To do so, early attention to factors that influence the feasibility, acceptability, and appropriateness of these programs within community practice is essential (Boyd et al., 2022; Dingfelder & Mandell, 2011; Feldstein & Glasgow, 2008). This study presents results from workgroups that included a range of professional disciplines to examine the fit of a structured, parent-mediated intervention for feeding problems (MEAL Plan) in community settings. We conducted three virtual workgroups that opened and closed with focus groups in which participants were invited to describe factors that could help or hinder the implementation and sustainability of MEAL Plan in their practice settings. The focus groups were grounded in the implementation science PRISM framework to explore factors known to influence the implementation of EBPs in community practice, including provider attitudes, intervention compatibility, organizational support, and community demand (Feldstein & Glasgow, 2008).
Qualitative results highlighted the demand for a manualized program like MEAL Plan, as well as factors to consider during community implementation efforts, including (1) how the intervention content might be delivered, (2) the context in which it would be implemented, and (3) and the training necessary to support the implementation and sustained delivery of a program such as MEAL Plan in community settings. These overarching domains corresponded well with frameworks that characterize adaptations that can be made prior to implementation efforts to align an intervention more closely with the systems in which it will be implemented (Aarons et al., 2012), as well as common adaptations that are made to interventions during community implementation (Stirman et al., 2019). Within the overarching domains, specific themes were noted related to the flexibility of MEAL Plan delivery, the target population to receive MEAL Plan, billing and insurance considerations, administrative support for implementing novel interventions, and the requisite knowledge needed within ongoing training and consultation. Considering these factors prior to implementation may support a structured, parent-mediated intervention for feeding challenges in being more effectively delivered and sustained within community settings.
Findings from this study included considerations for the target population of MEAL Plan that may also be generalizable to other empirically supported parent-mediated interventions for ASD. Although the efficacy trial of MEAL Plan included caregivers of children with a known ASD diagnosis between the ages of 3 and 8 years (Sharp et al., 2019), providers consistently expressed the view that the program would be fitting for a broader group of children and families, including those without a known diagnosis of ASD, those from a slightly older and younger age group, and those with more mild and more severe feeding challenges. Providers’ consistent emphasis on expanding the target audience of MEAL Plan highlights the discrepancy between the inclusion criteria used within intervention development and efficacy trials, which is often narrow and exclusionary (Steinbrenner et al., 2022), and the needs of community practitioners who serve a much larger and more diverse group of children and families.
In addition to the target population, providers discussed whether they anticipated MEAL Plan being delivered as intended or in an adapted format. In general, participants predicted that less experienced clinicians would likely follow the program as intended. By contrast, more seasoned providers might be more selective in the delivery of MEAL Plan. Beyond the matter of following the manual versus selective application, several participants suggested that pacing described in the MEAL Plan manual would likely require adaptation to meet the needs of children and families in clinical practice. This discussion on flexibility in delivering structured interventions reflects the inevitability of adaptation during implementation efforts (Stirman et al., 2019). In this study, anticipated adaptations included those that would maintain (e.g. repeating content) and those would deviate (e.g. selective application of treatment sessions) from the MEAL Plan manual. This finding highlights the need to specify the core elements and acceptable adaptations of structured interventions prior to implementation efforts (Chambers & Norton, 2016). Attention to this matter, may support providers in making adaptations that are responsive to diverse families and children, but also maintain the integrity of structured, parent-mediated interventions (Edmunds et al., 2022).
In addition to discussion on intervention delivery, participants identified several contextual factors that could affect the implementation of MEAL Plan (Feldstein & Glasgow, 2008). For example, insurance and billing considerations, leadership support, and the dedicated time to attend ongoing training and consultation are known factors that impact the quality of intervention implementation (Brookman-Frazee et al., 2020; Melgarejo et al., 2020; Pickard et al., 2023; Suhrheinrich et al., 2021). Although the contextual findings within this study were not necessarily surprising, their known association with implementation outcomes makes them particularly critical to consider. Finally, providers articulated the importance of ongoing training and consultation when learning MEAL Plan and also provided insight into the knowledge that might be necessary for community providers to deliver MEAL Plan. Although participants shared that community providers would likely enter training with diverse baseline knowledge (e.g. knowledge of nutrition vs knowledge of challenging behavior), they also indicated that trainings did not need to be tailored to account for these diverse knowledge sets. Indeed, providers shared that multidisciplinary training permits providers to share their knowledge sets.
The findings of this qualitative study have potentially important implications for future study. Although our findings are specific to the implementation of MEAL Plan, the proactive examination of fit in community settings may be applicable to other structured, parent-mediated interventions. In line with other studies, our findings confirm the importance of assessing provider attitudes toward structured treatment programs and the importance of administrative support for training and supervision (Melgarejo et al., 2020). In addition, implementing MEAL Plan within community practice while also exploring factors reported to impact its implementation and sustainment could inform the design of hybrid implementation trials (Curran et al., 2012; Powell et al., 2015).
Limitations
There are several limitations in this study. First, the study sample was a small and purposively selected group of providers practicing from specific geographic regions in the United States. Saturation was reached within this study; however, it is possible that certain provider disciplines (i.e. occupational therapists) were underrepresented in our sample. Although the study provides insight on the implementation of EBPs in these community settings, the findings may not reflect the wide diversity of community practices serving autistic children. In addition, this study focused on anticipated adaptations for MEAL Plan in community practice. Factors that could influence implementation efforts of other EBPs for children with ASD, however, may not be the same.
Conclusion
Our findings highlight the importance of aligning EBPs into community practice. Early attention to factors that promote or hinder the translation of EBPs into community practice can inform the design of hybrid implementation-effectiveness and reduce the research to practice gap (Curran et al., 2012). For example, future research examining the effectiveness of MEAL Plan within community practice should also intentionally include strategies to ensure that there is administrative and leadership support for MEAL Plan delivery, insurance coverage for MEAL Plan, and sustainable forums for ongoing consultation in MEAL Plan. Given the potentially detrimental effects of food selectivity for children with ASD and the high demand for treatment, the translation of evidence-based interventions into community practice is clearly warranted. This proactive effort to evaluate the adaptations needed to export a structured intervention such as MEAL Plan into community settings may be useful for translating other evidence-based interventions for children with ASD.
Supplemental Material
sj-doc-1-aut-10.1177_13623613231166181 – Supplemental material for Examining adaptations necessary to support the implementation of a parent-mediated intervention for children with autism spectrum disorder and moderate feeding problems
Supplemental material, sj-doc-1-aut-10.1177_13623613231166181 for Examining adaptations necessary to support the implementation of a parent-mediated intervention for children with autism spectrum disorder and moderate feeding problems by Katherine Pickard, T Lindsey Burrell, Susan Brasher, Derianne Buckley, Scott Gillespie, William Sharp and Lawrence Scahill in Autism
Footnotes
Acknowledgements
The authors acknowledge the significant support of the community practitioners who participated within this research project as well as the Marcus Foundation, which funded the research presented in this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.