
Abstract
Evidence suggests increased mortality rates among autistic individuals. However, risks of mortality, including natural-cause, suicide, and accident mortalities, among autistic individuals remain unclear. Among the entire Taiwanese population (N = 29,253,529), between 2003 and 2017, 45,398 autistic individuals were identified and 1:4 matched to 181,592 non-autistic individuals based on birth year and sex. All-cause mortality, including natural-cause, accident, and suicide mortalities, was assessed from 2003 to 2017 between the two cohorts. Cox regression models were used to investigate the mortality risk between autistic and non-autistic individuals. Autistic individuals had increased likelihoods (hazard ratio, 95% confidence interval) of all-cause mortality (3.43, 3.00–3.92), natural-cause mortality (4.73, 3.99–5.60), and suicide mortality (3.67, 2.37–5.68) compared with non-autistic individuals. In particular, autistic males were more likely to die by suicide (hazard ratio: 3.81, 95% confidence interval: 2.37–6.13), and autistic females were more likely to die of accident (hazard ratio: 5.07, 95% confidence interval: 2.54–10.13) compared with non-autistic individuals. Appropriate and effective medical and mental health care is recommended for autistic individuals.
Lay abstract
Our study was the first population-based study in an Asian country to investigate the mortality rates among autistic individuals. Among the entire Taiwanese population (N = 29,253,529), between 2003 and 2017, 45,398 autistic individuals were identified and 1:4 age-/sex-matched to 181,592 non-autistic individuals. We found that autistic individuals had increased risks of all-cause mortality, natural-cause mortality, and suicide mortality compared with non-autistic individuals. Furthermore, autistic males were more likely to die by suicide, and autistic females were more likely to die of accident compared with the non-autistic individuals.
Introduction
Autism is a common, highly heritable, and heterogeneous neurodevelopmental condition and occurs along a broad continuum of severity with persistent deficits in social communication and social interaction, and restricted, repetitive patterns of behavior, interests, or activities (L. C. Chen et al., 2020; Lord et al., 2018, 2020). Evidence has indicated a consistent and significant rise in autism prevalence worldwide (approximately 0.6%–0.7%) in the recent decades (Lord et al., 2018, 2020). The definite neuromechanisms of autism remains unclear, and its etiology appears to be complex. Multiple genetic and environmental factors act together to develop a spectrum of neurobiological vulnerability to autism (Kim et al., 2019; Lord, 2019).
Increasing evidence has revealed the increased risk of all-cause mortality and cause-specific mortality (i.e. suicide) in autistic individuals (Jokiranta-Olkoniemi et al., 2021; Schendel et al., 2016; Smith DaWalt et al., 2019). Schendel et al. analyzed a Denmark database of 1,912,904 individuals born between 1980 and 2010 and revealed that 20,492 (1.1%) had autism, and 68 (0.3%) autistic individuals died (hazard ratio (HR): 2.2, 95% confidence interval (CI): 1.8–2.8) during the follow-up to the end of 2013 (Schendel et al., 2016). They demonstrated that the rates of natural-cause (HR: 2.2, 95% CI: 1.5–3.2) and suicide (HR: 4.6, 95% CI: 2.7–8.0) mortalities, but not that of accident mortality (HR: 1.4, 95% CI: 0.8–2.3), were significantly higher in autistic individuals than in non-autistic individuals (Schendel et al., 2016). By analyzing the Utah surveillance data obtained between 1998 and 2017, Kirby et al. (2019) identified a higher cumulative incidence of suicide (0.17%) in autistic individuals than in non-autistic individuals (0.11%, p < 0.05). Jokiranta-Olkoniemi et al. followed a Finnish cohort of children born between 1987 and 2005, including 4695 autistic individuals and 18,450 non-autistic individuals, until 2015 for mortality and found increased risks of natural-cause (HR: 7.1, 95% CI: 3.8–13.4) and suicide (HR: 2.1, 95% CI: 1.02–4.1) mortalities in autistic individuals (Jokiranta-Olkoniemi et al., 2021).
Furthermore, a joinpoint regression analysis study of the worldwide suicide mortality trends between 2000 and 2019 discovered a rise in suicide mortality in many countries, including the United States, Australia, Greece, Mexico, and Paraguay (Ilic & Ilic, 2022). The rise in suicide deaths was particularly pronounced among adolescents and young adults (Miron et al., 2019). The parallel rise in global prevalence of autism and suicide may underscore the importance of research at the intersection of autism and suicide for research, clinical, and public policy efforts (Ilic & Ilic, 2022). In addition, a 20-year follow-up study of 406 autistic adolescents and adults demonstrated that 26 individuals died at an average age of 39 years by various causes of death, including chronic physical conditions (i.e. epilepsy and heart disease) and accidents (i.e. choking on food and accidental poisoning) (Smith DaWalt et al., 2019). However, the above-mentioned studies only included Caucasians, which may confound the generality to other ethnicities (i.e. Asians) and racial minorities (i.e. American Indian).
In the current 15-year follow-up study, we investigated the all-cause mortality, natural-cause mortality, and unnatural-cause mortality, including accident and suicide, in autistic individuals by using data from the Taiwan National Health Insurance Research Database (NHIRD) that covered almost the entire population (N = 29,253,529). We hypothesized elevated risks of all-cause mortality, natural-cause mortality, and suicide mortality in autistic individuals compared with non-autistic individuals.
Methods
Data source
The Taiwan NHIRD, which consists of health care data of >99.6% of the entire Taiwan population, is audited and released by Health and Welfare Data Science Center of Ministry of Health and Welfare, Taiwan, for research purposes. This database includes comprehensive (outpatient, inpatient, and emergency department settings) data of insured individuals, which include demographics, clinical visits (dates), and disease diagnoses. Individual medical records included in the NHIRD are anonymous to protect individual privacy. In the current study, the Longitudinal Health Insurance Database of the NHIRD, which includes all medical records between 2003 and 2017 of the entire Taiwanese population (N = 29,253,529), was linked to the Database of All-cause Mortality, which includes all-cause mortality records between 2003 and 2017 of the entire Taiwanese population for the analyses of mortality risk in autistic individuals. In the Database of All-cause Mortality, natural death and mortality due to physical diseases (natural cause) were coded as 1; accidental death as 2; suicide as 3; homicide as 4; and mortality with uncertain cause as 5. NHIRD has been used in numerous epidemiological studies in Taiwan (M. H. Chen et al., 2016; M. H. Chen et al., 2019; Cheng et al., 2018; Hsu et al., 2023; Huang et al., 2020). The diagnostic codes used in the present study are based on the International Classification of Diseases, 9th or 10th Revision, Clinical Modification (ICD-9-CM (2003–2014) or ICD-10-CM (2015–2017)). The institutional review board of our Hospital approved the study protocol and waived the requirement for informed consent because deidentified data were used in this study, and no participants were actively enrolled.
Inclusion criteria for autistic individuals and non-autistic individuals
Individuals diagnosed as having autism (ICD-9-CM codes: 299.0, 299.8, 299.9 or ICD-10-CM codes: F84.0, F84.5, F84.8, F84.9) by board-certified psychiatrists at least twice were included as the autism cohort. In Taiwan, children aged <6 years who had any developmental concern, including language and social development, would be taken by their parents to a psychiatric, pediatric, or rehabilitation medicine outpatient for the developmental evaluation. If children aged between 6 and 17 years had social communication problems, their parents may take them to a psychiatric outpatient for the social communication assessment. Those aged ⩾18 years can consult psychiatrists on their own if they have social communication problems. During the psychiatric assessment, a comprehensive diagnostic interview was performed by the board-certified psychiatrists to achieve a diagnosis, including autism. To reduce the confounding effects of age and sex, because autism is predominant in males and infrequently diagnosed in middle-aged to older Taiwanese adults (Lai & Baron-Cohen, 2015), a 1:4 autism–non-autism matched analysis was conducted based on birth year and sex. Non-autistic individuals were randomly identified from the entire Taiwanese population after those who had been diagnosed with autism (ICD-9-CM code: 299 or ICD-10-CM codes: F84) were eliminated at any time in the database. The urbanization level of residence (levels 1–4, most to least urbanized) was assessed as a proxy for health care availability in Taiwan (Liu et al., 2006). Autism develops in early childhood, and the time of diagnosis varies across individuals; therefore, individuals’ data from their birth or 1 January 2003 to death or 31 December 2017, were collected in the present study. The diagnosis of autism was regarded as a time-dependent variable. All-cause mortality, natural-cause mortality (natural death and mortality due to physical diseases), and unnatural-cause mortality (accident mortality and suicide mortality) were identified between 2003 and 2017 from the Database of All-cause Mortality. For autistic individuals and matched non-autistic individuals, Charlson Comorbidity Index (CCI) scores were calculated. The CCI comprising 22 physical conditions was also assessed to determine the systemic health conditions of all enrolled subjects (Charlson et al., 1987). The 22 physical conditions included myocardial infarct, congestive heart failure, peripheral vascular disease, dementia, cerebrovascular disease, chronic lung disease, connective tissue disease, ulcer, chronic liver disease, diabetes, hemiplegia, moderate or severe kidney disease, diabetes with end organ damage, tumor, leukemia, lymphoma, moderate or severe liver disease, malignant tumor, metastasis, and AIDS. On the basis of individuals’ CCI scores, diseases such as liver cirrhosis or leukemia were diagnosed (at least twice) by the relevant specialists, such as a gastroenterologist (including pediatric gastroenterologists) or a hematologist (including pediatric hematologists). Furthermore, because autism may be comorbid with intellectual disability, attention-deficit hyperactivity disorder (ADHD) (ICD-9-CM codes: 314 or ICD-10-CM codes: F90), schizophrenia (ICD-9-CM codes: 295 or ICD-10-CM codes: F20, F25), bipolar disorder (ICD-9-CM codes: 296 except 296.2, 296.3, 296.9, and 296.82 or ICD-10-CM codes: F30, F31), major depressive disorder (ICD-9-CM codes: 296.2, 296.3, 300.4, and 311 or ICD-10-CM codes: F32, F33, F34, and F39), and intellectual disability (ICD-9-CM codes: 317, 318, 319 or ICD-10-CM codes: F70, F71, F72, F73, F78, F79) (Hossain et al., 2020; Mutluer et al., 2022), which are also associated with an increased mortality rate (Laursen et al., 2007; Lomholt et al., 2019), these comorbidities also were investigated during the follow-up period for further evaluation of the effect of comorbidities on the risk of mortality. These psychiatric disorders were diagnosed at least twice by board-certified psychiatrists (Figure 1).
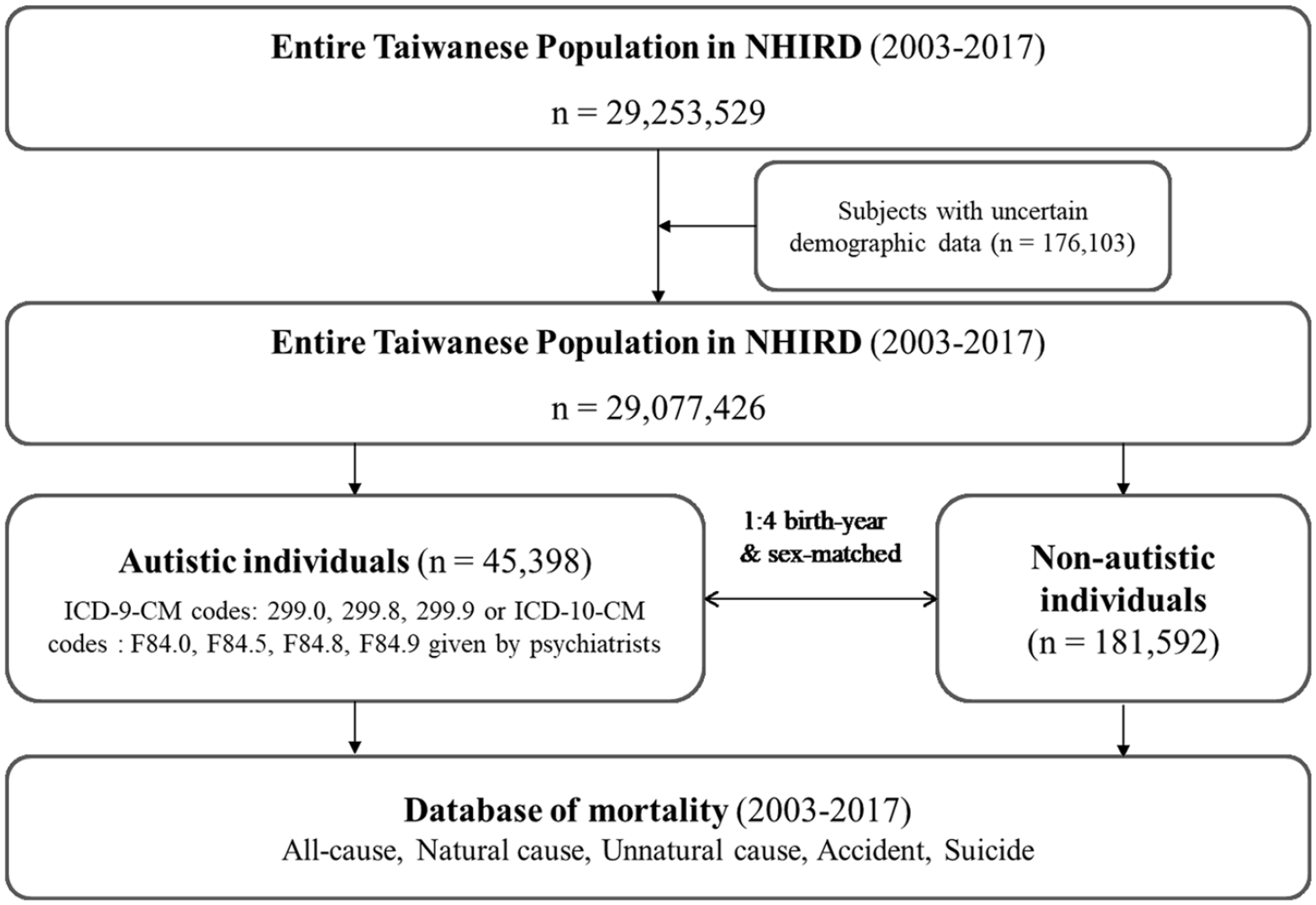
Study flowchart.
Statistical analysis
For between-group comparisons, the independent t test was used for continuous variables and Pearson’s χ2 test was used for nominal variables. Time-dependent Cox regression models with adjustment for sex, birth year, income, level of urbanization, and CCI were used to calculate HR and 95% CI of subsequent mortality, including all-cause, natural-cause, and unnatural-cause (accident, and suicide) mortalities between autistic individuals and non-autistic individuals. Sub-analyses stratified by sex and CCI (0, 1–2, >2) were further performed. Additional time-dependent Cox regression models with adjustment for sex, birth year, income, level of urbanization, and CCI were performed to investigate the mental comorbidities, including intellectual disability, ADHD, schizophrenia, bipolar disorder, and major depressive disorder, on the mortality risk between autistic (without vs with each comorbidity) and non-autistic individuals. The comorbid conditions were accounted for separately in the Cox regression models, which meant that an autistic individual with ADHD and major depressive disorder was treated separately as an autistic individual with ADHD and an autistic individual with major depressive disorder in the models. Finally, because each subject may experience different age stages (childhood, adolescence, young adulthood, or later adulthood) as he or she grew, sensitivity analyses based on age as a time-dependent variable (0–6 (reference group), 7–12, 13–17, 18–29, and 30– years) in the Cox regression models were performed (Somerville, 2016). Such analyses would clarify the age effect on the mortality risk. A two-tailed p value of <0.05 was considered statistically significant. All data processing and statistical analyses were performed using the Statistical Analysis Software Version 9.1 (SAS Institute, Cary, NC, USA).
Community involvement
Not applicable.
Results
In all, 45,398 autistic individuals and 181,592 age-/sex-matched non-autistic individuals were included in the current study, with a male predominance (83.1%; Table 1). A greater proportion of people in the autism cohort resided in the urban region (p < 0.001) and had higher income (p < 0.001) compared with non-autistic individuals (Table 1). In addition, autistic individuals were more likely to have higher CCI scores compared with non-autistic individuals (p < 0.001; Table 1).
Demographic characteristics of autistic individuals and non-autistic individuals.

USD: US dollar; CCI: Charlson Comorbidity Index; ADHD: attention-deficit hyperactivity disorder.
Cox regression analyses with adjustment for sex, birth year, income, level of urbanization, and CCI revealed that autistic individuals had increased risks (HR, 95% CI) of all-cause mortality (3.43, 3.00–3.92), natural-cause mortality (4.73, 3.99–5.60), unnatural-cause mortality (2.33, 1.87–2.90), accident morality (1.96, 1.47–2.63), and suicide mortality (3.67, 2.37–5.68) compared with non-autistic individuals (Table 2).
Mortality risk between autistic individuals and non-autistic individuals.
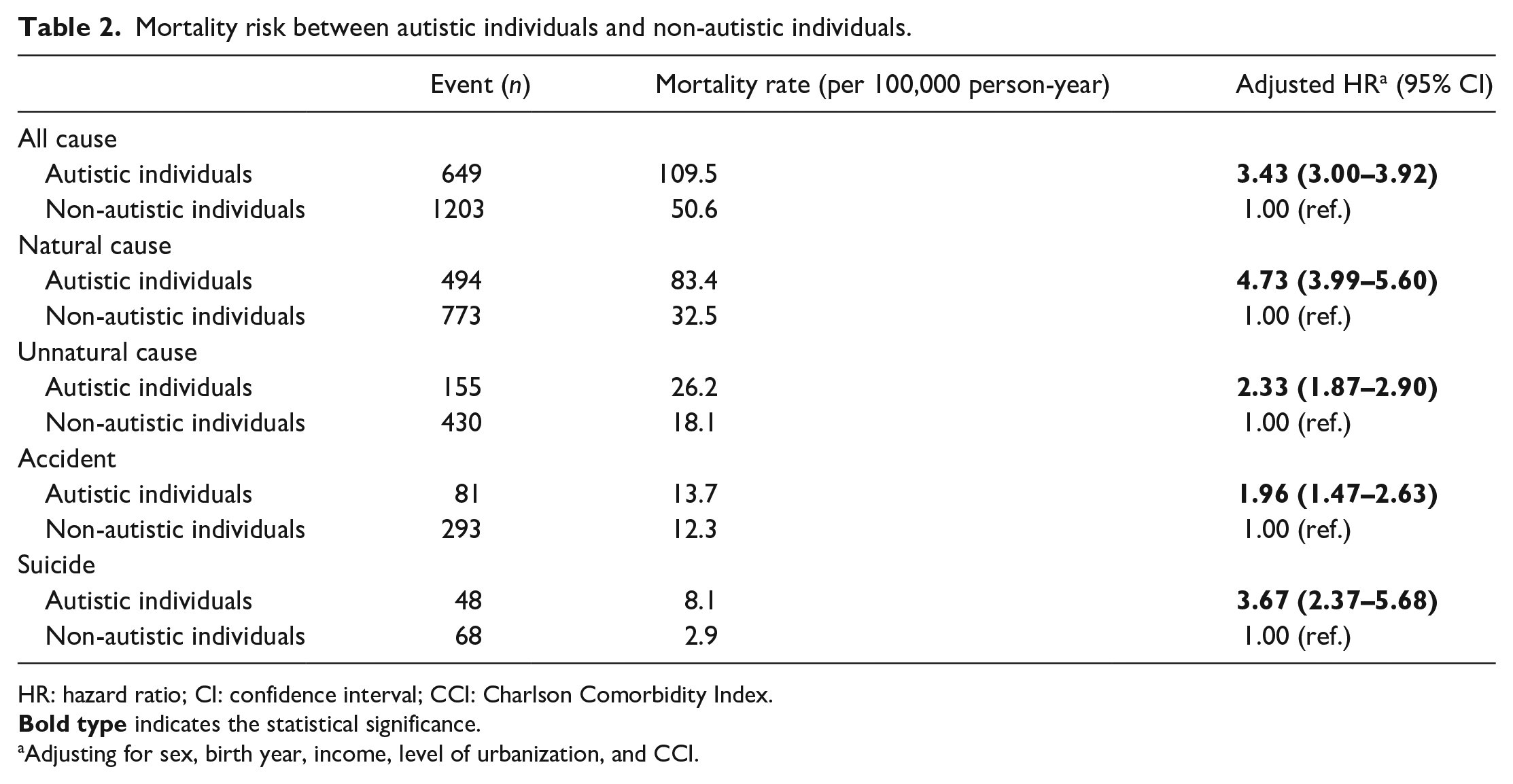
HR: hazard ratio; CI: confidence interval; CCI: Charlson Comorbidity Index.
Adjusting for sex, birth year, income, level of urbanization, and CCI.
Stratified by sex, autistic males and females exhibited elevated risks (HR, 95% CI) of all-cause mortality (2.81, 2.39–3.29; 6.00, 4.63–7.77), natural-cause mortality (4.08, 3.31–5.02; 6.68, 4.93–9.05), and unnatural-cause mortality (2.06, 1.62–2.63; 4.30, 2.54–7.25) compared with non-autistic individuals (Table 3). In particular, autistic males were more likely to die by suicide (HR: 3.81, 95% CI: 2.37–6.13), and autistic females were more likely to die of accident (HR: 5.07, 95% CI: 2.54–10.13) compared with non-autistic individuals (Table 3).
Mortality risk between autistic individuals and non-autistic individuals, stratified by sex and CCI.

HR: hazard ratio; CI: confidence interval; CCI: Charlson Comorbidity Index.
Furthermore, stratified by the level of physical illness severity based on CCI, autistic individuals with CCI scores of 0 or 1–2 had significantly increased risks (HR, 95% CI) of natural-cause mortality (15.38, 7.13–33.16; 7.97, 5.1–12.45) and suicide mortality (7.29, 2.53–20.97; 6.17, 2.04–18.69) compared with non-autistic individuals (Table 3). However, autistic individuals with CCI scores of >2 only exhibited higher risks of natural-cause mortality (HR: 2.22, 95% CI: 1.67–2.94) than non-autistic individuals (Table 3).
The presence of comorbidities of ADHD (HR: 4.66, 95% CI: 1.89–11.51), schizophrenia (4.32, 2.30–8.12), bipolar disorder (6.46, 2.19–19.02), and major depressive disorder (3.97, 2.10–7.50) with autism was associated with substantially higher risks of suicide mortality (Table 4). The presence of intellectual disability (HR: 1.77, 95% CI: 1.23–2.56) and bipolar disorder (HR: 2.65, 95% CI: 1.21–5.79) in addition to autism was associated with a substantially high risk of accident mortality (Table 4). Furthermore, the presence of intellectual disability (HR: 3.69, 95% CI: 2.98–4.57), schizophrenia (HR: 3.47, 95% CI: 2.47–4.88), or bipolar disorder (HR: 3.68, 95% CI: 2.29–5.92) in addition to autism was associated with a considerably high risk of natural-cause mortality (Table 4).
Mortality risk between autistic individuals and non-autistic individuals, stratified by mental comorbidities. a
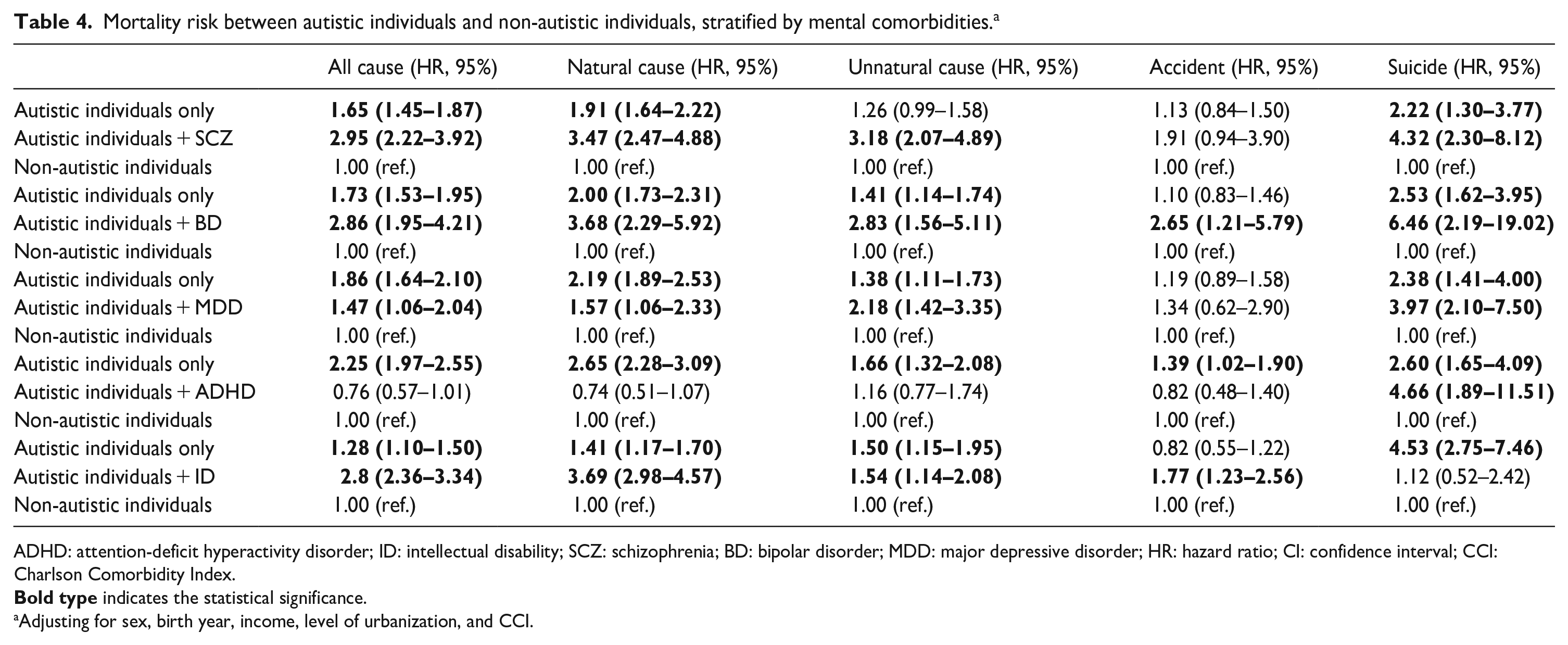
ADHD: attention-deficit hyperactivity disorder; ID: intellectual disability; SCZ: schizophrenia; BD: bipolar disorder; MDD: major depressive disorder; HR: hazard ratio; CI: confidence interval; CCI: Charlson Comorbidity Index.
Adjusting for sex, birth year, income, level of urbanization, and CCI.
Finally, Table 5 showed that compared with age 0–6 years, only age ⩾ 30 years (HR: 2.89, 95% CI: 2.46–3.61) was associated with the increased risk of natural-cause morality (Table 5). Ages after 18 years (18–29, ⩾30 years) were linked to unnatural-cause mortality (HR, 95% CI: 5.19, 3.95–6.82; 7.77, 5.75–10.52); ages after 13 years (13–17, 18–29, ⩾30 years) were associated with accidental mortality (1.9, 1.29–2.79; 5.64, 4.04–7.87; 6.60, 4.47–9.75) (Table 5). Perhaps because the number of suicides was too small, age as a time-dependent variable was divergent in the Cox regression models.
Age as a time-dependent variable on the morality between groups.
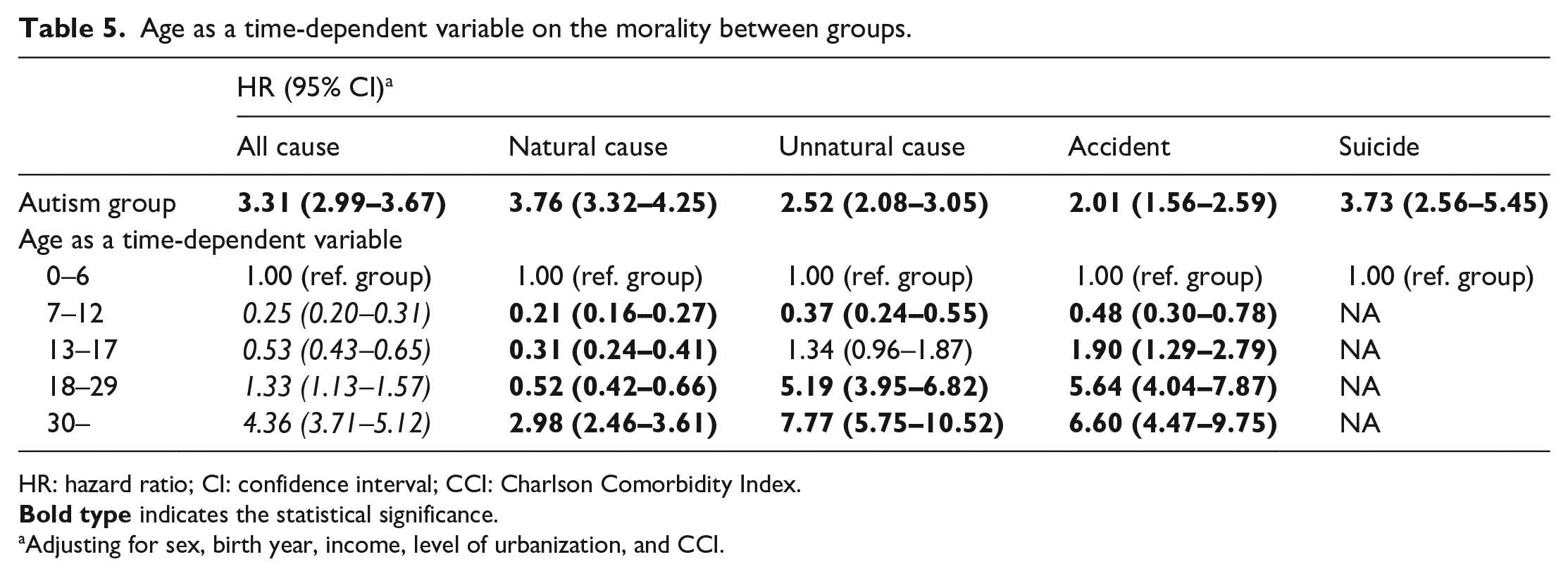
HR: hazard ratio; CI: confidence interval; CCI: Charlson Comorbidity Index.
Adjusting for sex, birth year, income, level of urbanization, and CCI.
Discussion
Our findings support the hypothesis that autistic individuals, particularly children aged 7–12 years, adolescents, and adults, exhibit higher risks of all-cause, natural-cause, and suicide mortalities compared with non-autistic individuals. In addition, we found that autistic adults were more likely to die of accident than non-autistic individuals.
Among the entire population of Taiwan (N = 29,253,529), the prevalence of autism was determined to be only 0.15%, which is much lower than that (0.76%) reported by the World Health Organization (Hodges et al., 2020). Two possible reasons can be highlighted for this low prevalence of autism in Taiwan: underdiagnosis and a lack of autism-related knowledge in the general Taiwanese population. Thus, our study cohort may represent individuals with psychiatric morbidity who had severe autism (Lai & Baron-Cohen, 2015). Shavelle et al. (2001) and Mouridsen et al. (2008) demonstrated that an increased risk of autism-associated mortality is correlated with the presence of a neurological disorder (i.e. epilepsy) or intellectual disability, respectively. An Australian study that included a total of 35,929 autistic individuals who were aged 5–64 years revealed that concurrent intellectual disability, epilepsy, chronic physical health conditions, and history of admission to a psychiatric ward were all associated with a higher risk of all-cause mortality (Hwang et al., 2019). The presence of these comorbidities indicated high-severity autism, which was associated with high mortality (Hwang et al., 2019; Mouridsen et al., 2008; Shavelle et al., 2001). Among the autistic individuals in the present study, approximately 26% had intellectual disability, 20% had severe mental disorders (e.g. schizophrenia, bipolar disorder, and major depressive disorder), and 7.5% had a CCI score of >2; all these imply that our subjects had severe autism.
We further investigated the effect of physical illness severity based on the individuals’ CCI scores—a possible indicator of autism severity—on the morality risk of autistic individuals. Notably, individuals with low-grade (CCI score ⩽ 2) physical illness severity exhibited the most prominent effect of autism on all-cause, natural-cause, and suicide mortalities. The effect of autism on natural-cause mortality, but not on suicide mortality, was maintained in individuals with high-grade (CCI scores > 2) physical illness severity. Our findings may reflect the inconsistent findings reported by Schendel et al. (2016) and Hwang et al. (2019). Schendel et al. (2016) indicated that the presence of neurological comorbidities does not affect autism-associated mortality, whereas Hwang et al. identified neurological comorbidities to be major factors associated with all-cause mortality (Hwang et al., 2019). Jokiranta-Olkoniemi et al. reported an HR of 7.1 for natural-cause mortality, which is higher than that (4.73) determined in our study. Furthermore, autistic females exhibit higher risks of all-cause, natural-cause, and accident mortalities than autistic males, which implies that high-severity autism is diagnosed more commonly in women than in men (Dillon et al., 2023; Lord et al., 2018, 2020), and may also imply that the current diagnostic procedures may be biased to male phenotypes (missing the females with higher ability) in Taiwan. Further studies are warranted to evaluate the effects of sex and physical illness severity on autism-related mortality. Sex-specific and integrated (mental and physical) medical care should be provided to at-risk individuals.
A higher risk of suicide mortality was noted in autistic individuals than in non-autistic individuals. A meta-analysis that included the data of a total of 34,011 autistic youths reported that the pooled prevalence was 25.2% (95% CI: 18.2–33.8) for suicidal ideation, 8.3% (3.6–18.2) for suicide attempts, and 0.2% (0.05–0.52) for suicide mortality (O’Halloran et al., 2022). In their study on the prevalence of confirmed autism in individuals who died by suicide, Cassidy et al. found that the prevalence of autism (10.8%) was significantly higher in these individuals than that (1.1%) expected in the general British population (those alive) (Cassidy et al., 2022). They further determined autistic traits (undiagnosed possible autism) were positively correlated with completed suicide (Cassidy et al., 2022). A population-based cohort study on autistic individuals (n = 27,122) and age- and sex-matched non-autistic individuals (n = 2,672,185) reported that the odds ratio was higher in autistic individuals who died by suicide (odds ratio: 7.55, 95% CI: 6.04–9.44) than in the age- and sex-matched non-autistic individuals (Hirvikoski et al., 2016). Given the compelling evidence of high suicide risk in autistic individuals and the fact that suicide is the second leading cause of mortality among adolescents in the United States, child and adolescent psychiatrists have implored the US government to develop a safety plan for suicidality in autistic individuals (Ruch et al., 2019; Schwartzman et al., 2021). Considering the similarities in the increased likelihood of suicide mortality between Taiwan (3.67 times in our study) and the United States (3.42 times in the study by Kirby et al., 2019), we recommend that a suicide prevention program specific to autistic individuals or those with autistic traits be implemented in Taiwan.
We further evaluated the additive effects of autism and other mental disorders, such as ADHD, intellectual disability, schizophrenia, bipolar disorder, and major depressive disorder, on the risk of suicide mortality. Autistic individuals who had no intellectual disability, but not those who had intellectual disability, exhibited a higher risk of suicide mortality than non-autistic individuals, which was compatible with Hirvikoski et al.’s (2020) findings that the increase in the risk of suicide mortality was the highest in autistic individuals without intellectual disability. In addition, the comorbidities of bipolar disorder and intellectual disability are associated with an increased risk of accident mortality in autistic individuals, which may suggest a potential role of reckless behaviors shared between three conditions in accident mortality (Dutta et al., 2007; Lie et al., 2017). Finally, autistic individuals with comorbid schizophrenia, bipolar disorder, or intellectual disability exhibit a higher risk of natural-cause mortality than non-autistic individuals; therefore, clinicians should assist these individuals in maintaining healthy lifestyle habits, such as regularly exercising and quitting smoking (Firth et al., 2020).
Age-related differences in natural-cause mortality, unnatural-cause mortality, and accident mortality indicate that clinicians and public health officers should offer age-appropriate medical and mental health services to autistic individuals (Farmer et al., 2014; Powell et al., 2021; Smith DaWalt et al., 2019; Weiss et al., 2018). Our results indicate that the risk of natural-cause mortality appeared since age of 30 years among autistic individuals, but the risks of accidental mortality and overall unnatural-cause mortality have been observed among autistic individuals during adolescence, and further increases when they grew older. Farmer et al. revealed that over 60% of autistic children had unmet medical and mental health service needs (Farmer et al., 2014). Powell et al. (2021) reported that autistic adolescents were more likely to have an unmet medical and mental health service needs (11.0% vs 3.2%) than non-autistic adolescents. Weiss et al. (2020) further concluded that autistic adults were more likely to have almost all the examined clinical health issues and health service use indicators compared with those without developmental disability.
The study has several limitations. First, the prevalence of autism may be underestimated because only those who sought mental health consultation and help were identified in the database. Among individuals with mild autistic condition, autism may be underdiagnosed because of a lack of medical consultation or treatment. Thus, autistic individuals whose cases have been registered in the NHIRD may represent those with psychiatric disorders with severe autism. Nevertheless, the National Health Insurance offers convenient and affordable medical services, which may help reduce this bias. Autism diagnosis was only given by board-certified psychiatrists, which improves the diagnostic validity. Furthermore, whether our findings may be extrapolated to individuals with mild autistic condition must be validated further. Second, information on the severity of autism was unavailable in the NHIRD. The presence of intellectual disability reportedly indicates autism severity (Underwood et al., 2010). As mentioned, our study demonstrated that autistic individuals with intellectual disability exhibited a higher risk of natural-cause mortality and those without intellectual disability exhibited a higher risk of suicide mortality than non-autistic individuals. Further community-based cohort studies are needed to identify the possible association between autism severity and mortality risk. Third, intellectual disability and ADHD have an early-onset and have genetic correlates with autism. All three conditions may require lifelong support related to education and/or labor market. Although there was no information on social support in the database, differences in social support among individuals with intellectual disability, ADHD, and autism may probably confound our findings, which would need further investigation. Fourth, we only assessed the major psychiatric comorbidities, including schizophrenia, bipolar disorder, and major depressive disorder, with autism on the mortality risk in current study. Anxiety disorders were commonly comorbid with autism. Further studies would be necessary to clarify the anxiety comorbidity with autism on the mortality risk, especially suicide. Fifth, data such as information on psychosocial stress, lifestyle, and environmental factors were unavailable in the NHIRD; therefore, we could not investigate their potential influence on the study outcome.
In conclusion, autistic individuals exhibit higher risks of all-cause, natural-cause, and suicide mortalities than non-autistic individuals. Moreover, autistic adults had an elevated risk of accident mortality compared with non-autistic individuals. Our results indicate that clinicians should routinely monitor the physical and mental health of autistic individuals. Furthermore, comprehensive public health policies may be required to provide improved medical and mental health care services to fulfill the unmet needs of high-risk autistic individuals.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by grant from Taipei Veterans General Hospital (V111C-010, V111C-040, V111C-029), Yen Tjing Ling Medical Foundation (CI-109-21, CI-109-22, CI-110-30), Ministry of Science and Technology, Taiwan (MOST110-2314-B-075-026, MOST110-2314-B-075-024 -MY3, MOST 109-2314-B-010-050-MY3, MOST111-2314-B-075 -014 -MY2, MOST 111-2314-B-075 -013), Taipei, Taichung, Kaohsiung Veterans General Hospital, Tri-Service General Hospital, Academia Sinica Joint Research Program (VTA112-V1-6-1) and Veterans General Hospitals and University System of Taiwan Joint Research Program (VGHUST112-G1-8-1). The funding source had no role in any process of our study.