
Abstract
The mediators of real-world executive functions in autism during the transition into adulthood are mainly unknown. This study aimed to identify the mediators for the behavioral and cognitive domains of real-world executive functions in late adolescent and young adult autistic populations. We followed up 289 autistic children (aged 11.6 ± 3.8, male 82.2%) and 203 non-autistic controls (10.7 ± 2.9, 66.5%) to their ages of 16.9 ± 4.7 and 15.8 ± 3.9, respectively. The Behavior Rating Inventory of Executive Function, comprising two global scales (Behavioral Regulation Index and the Metacognitive Index), was used to assess real-world executive functions at Time 2. Mediators of behavior regulation and metacognition were explored among a wide range of clinical correlates and parental bonding. We found that the autistic group had lower executive functions than the non-autistic group with lower behavior regulation and metacognition subscores. Several childhood factors were significant mediators. Multiple mediation analyses revealed that childhood inattention remained a significant mediator for both behavior regulation and metacognition in late adolescence, and peer problems were the specific mediators of metacognition. Our findings suggest several childhood factors may mediate real-world executive functions during late adolescence. Treating common mediators such as inattention may improve real-world executive functions in autistic individuals during adulthood.
Lay abstract
Childhood factors that predict real-world executive function in autism spectrum disorder during the transition into adulthood are largely unknown. This study aimed to identify the predictors for the behavioral and cognitive aspects of real-world executive function in late adolescent and young adult autistic populations. We followed up 289 autistic youth (mean age 11.6 years) and 203 non-autistic controls (10.7 years) to their ages of 16.9 and 15.8, respectively. The Behavior Rating Inventory of Executive Function scale was used to measure the real-world executive function at late adolescence and young adulthood at follow-up. Potential predictors such as autistic symptoms, inattention or hyperactivity symptoms, peer relationship, emotional symptoms, and parenting styles were assessed in childhood at first enrollment. The results showed that childhood inattention, withdrawn behaviors, social communication difficulties, and child-reported emotion and inattention/hyperactivity may predict real-world lower executive function in late adolescence and young adults with autism. When separating executive function into behavioral and cognitive aspects, we found that oppositional behaviors and peer problems were specific predictors for behavioral regulation and cognitive function, respectively. Our findings suggested that treating common predictors in childhood, such as inattention, may potentially improve real-world executive function in autism during the transition into adulthood.
Introduction
Executive functioning difficulties have been observed in people with autism. Using laboratory-based neurocognitive tasks such as the Wisconsin Card Sorting Test, the Go–no-Go task (Bölte et al., 2009; Happé et al., 2006), and the Cambridge Neuropsychological Test Automated Battery (Chen et al., 2016; Chien et al., 2015; Craig et al., 2016; Seng et al., 2020), studies have demonstrated that autistic people were more likely to have impaired executive functions on various tasks than the non-autistic controls with moderate overall effect sizes (Demetriou et al., 2018). However, although executive functions measured by standardized procedures help understand cognitive function in autism, these tasks may not capture real-world difficulties with planning, organization, and self-regulation (Ng et al., 2019; Van Eylen et al., 2015). Thus, the findings might not directly translate to daily life function or implicate intervention (Ng et al., 2019; Van Eylen et al., 2015). The behavioral aspect of executive dysfunction is more strongly associated with everyday functioning than standardized assessments of executive functions (Barkley & Murphy, 2010), partly because it may capture extraneous cognitive abilities beyond an isolated executive domain targeted by a standardized assessment (Udhnani et al., 2020). For clinical practice, a measure based on more representative environmental situations must be considered when assessing areas of executive dysfunction.
Scales rating executive functions observed in daily life have been developed, such as the Behavior Rating Inventory of Executive Function (BRIEF) (Gioia et al., 2000). A recent meta-analysis (Demetriou et al., 2018) supported that BRIEF achieved clinical utility in differentiating autistic and non-autistic groups. Several studies have adopted the BRIEF to investigate everyday executive functions in autism (Blijd-Hoogewys et al., 2014; Gilotty et al., 2002; Gioia et al., 2002; Kenworthy et al., 2005; Lawson et al., 2015; Rosenthal et al., 2013; Smidts & Huizinga, 2009; van den Bergh et al., 2014). Most studies reported elevated scores on almost all BRIEF subscales in support of everyday executive dysfunction in autistic children. Two studies further indicated that autistic children had the most difficulty shifting but the least in organizing materials in daily life (Blijd-Hoogewys et al., 2014; Smidts & Huizinga, 2009). Not only autistic children but autistic adults may also show difficulties in flexibility and metacognition (Wallace et al., 2016), suggesting that a lower everyday executive function may be a lifelong condition in some autistic individuals.
Assessment of executive functions is critical during late adolescence to understand how autistic people manage their daily lives in adulthood. Evidence suggested an age-related increase in real-world executive dysfunctions from childhood to late adolescence (Pugliese et al., 2015; Rosenthal et al., 2013). Nearly two-thirds of autistic adults (64.2%) still suffer from executive dysfunction (Johnston et al., 2019), with significant inter-individual variability (Demetriou et al., 2019). They have difficulties compensating for increasing demands on executive functions to behave age-appropriately (Chen et al., 2016; Happé et al., 2006). In thinking of ameliorating real-world executive dysfunction in late adolescence, identifying trainable or manageable mediators before adolescence is valuable for improving adaptive function and life quality in adulthood (Gardiner & Iarocci, 2018; Pugliese et al., 2015). Suppose executive dysfunction in daily life is associated with the factors that could be detected earlier and treated effectively. Such intervention may result in real-world gains for later study or work (Lee et al., 2021). Despite this critical implication, the mediators of real-world executive dysfunction are largely unknown in autism. In typically developing children, executive function has been shown to relate to the development of emotion regulation (e.g. cognitive reappraisal) (Mohammed et al., 2022; Sudikoff et al., 2015), academic achievement (Cortés Pascual et al., 2019), oppositional behaviors (Chen et al., 2019; Jiang et al., 2016; Pijper et al., 2018), and school readiness (Pellicano et al., 2017). Parenting behaviors (e.g. parental involvement and inconsistent discipline) and parent–child relationships also influenced the development of executive function in school-age children (Fay-Stammbach et al., 2014; Sosic-Vasic et al., 2017). Identifying childhood factors that influence executive functions differently in autistic and non-autistic groups within the transition period is particularly interesting to this study.
In autism, cross-sectional studies have examined the relationship between executive functions and autistic traits or symptoms of attention-deficit/hyperactivity disorder (ADHD) (Kenworthy et al., 2009; Kenworthy et al., 2005). Social communication symptoms in autism were associated with weakness in executive dysfunction (e.g. working memory or flexibility) (Gilotty et al., 2002; Gioia et al., 2000; Hill, 2004). A national survey of 6832 children also found that autistic traits were significantly associated with executive dysfunction measured by the BRIEF (Tsai et al., 2021). Besides, executive functions on the inhibition, planning, switching, and working memory tasks were correlated with ADHD symptoms in autistic adolescents (Lukito et al., 2017). A recent study on autistic children (n = 64, aged 6.7–13.5 years old) showed that executive dysfunction was related to ADHD symptoms but not to autistic traits (Lee et al., 2021). Other than autistic traits and ADHD symptoms, the mediating roles of other clinical correlates of executive functions were also uncertain. Evidence suggested that executive function was closely related to emotional and cognitive regulation strategies necessary for social interactions (Fong & Iarocci, 2020; Lantrip et al., 2016) and was associated with adaptive functioning, particularly communication and daily living skills (Udhnani et al., 2020). Middle-childhood executive functions could influence the associations between early-childhood autistic symptoms and behavioral problems, academic performance, or adaptive functioning in early adolescence (at 10–11.8 years) (Ameis et al., 2021; St. John et al., 2018). Longitudinal studies also implied that early-childhood executive functions predicted social communication 3 years later (Pellicano, 2013) and were associated with autistic features and adaptive functioning in autistic young people (Kenny et al., 2019), particularly in daily living skills and socialization (Pugliese et al., 2016). In addition, specific parenting styles observed in videotaped standardized play and clean-up sessions might predict executive functions on the BRIEF at ages 6 to 10 years (Halse et al., 2019). Taken together, executive functions in autism may not only relate to autistic traits and ADHD symptoms; still, they may also link to emotional/behavioral problems, academic performance, adaptive functioning, and parenting style in childhood. Whether these childhood factors mediated the diagnosis of autism established in early childhood to everyday executive functions in late adolescence waits to be examined in longitudinal studies. Of note, studies examining autistic traits or ADHD symptoms often summed up all symptoms as total severity. It is unclear which specific symptom domain (e.g. inattention vs. hyperactivity/impulsivity) correlates with executive dysfunction. In addition, most studies focused on one or two factors (e.g. autistic traits or ADHD symptoms) rather than a comprehensive set of measures. Furthermore, several factors may be highly correlated with each other (e.g. emotional symptoms vs. behavioral problems). Therefore, it is essential to consider all potential factors to detect important mediators for executive functions.
The BRIEF scale measures two major domains of executive functions. Behavioral regulation reflects the ability to modulate behavior and emotion by exerting appropriate inhibitory control. Meanwhile, metacognition demonstrates the ability to manage tasks by effectively initiating, planning, organizing, and monitoring goal-oriented behaviors (Tsai et al., 2019). Metacognition was found to be associated with social functioning in autistic children (Torske et al., 2017), as well as social skills (Gardiner & Iarocci, 2018); behavior regulation, instead, was significantly associated with depressive symptoms for children with and without autism (Gardiner & Iarocci, 2018). In addition, a recent study demonstrated that polygenic scores of autism were associated with behavioral regulation aspects of everyday executive functions in children admitted for clinical assessment, suggesting that common risk gene variants of autism had a stronger association with behavioral regulation than metacognition (Torske et al., 2020). Together, these studies suggested distinct correlates between behavioral regulation and metacognition. Hence, we separated these two domains to identify specific mediators for each domain.
Instead of using executive functions assessed by neuropsychological tests as outcome measures (Kenny et al., 2019; Pugliese et al., 2016; Udhnani et al., 2020), this study aimed to focus on deficits in the behavioral regulation and cognitive aspects of everyday executive functions in autistic youth in late adolescence upon transitioning into adulthood. It investigated the predictors in childhood using a prospective follow-up design. First, we comprehensively assessed potential mediators of everyday executive dysfunction, including autistic traits, ADHD symptoms, behavior problems (e.g. oppositional, aggressive, or withdrawn behaviors, etc.), school behaviors (e.g. academic performance, peer problems, etc.), and parenting style. Then, we examined whether these clinical correlates in childhood mediated the relationship between autism diagnosis at baseline and everyday executive dysfunctions in late adolescence and young adulthood. As an exploratory study, we separately selected significant mediators from single mediation analyses for multiple mediation analyses to detect the most important mediators for behavior regulation and metacognition. Finally, based on previous evidence in cross-sectional associations, we explored whether childhood autistic and inattention/hyperactivity symptoms, social/peer functions, emotional/behavioral characteristics (e.g. externalizing behaviors), and parenting styles mediate behavior and cognition domains of executive dysfunctions (or both) in late adolescence.
Methods
Participants and procedure
This study recruited 319 Han Chinese autistic children, aged 11.7 ± 4.1 (mean ± standard deviation), and 237 non-autistic controls, aged 10.7 ± 2.6 at the first enrollment. The inclusion criteria for the autistic and non-autistic groups were children with and without a diagnosis of autism spectrum disorder (ASD), respectively. The exclusion criteria of both groups were: having major neuropsychiatric disorders (e.g. schizophrenia, bipolar disorder, or organic mental disorder) or intelligence quotient (IQ) lower than 70. Autistic participants were referred from the Department of Psychiatry outpatient clinics at the National Taiwan University Hospital, Taiwan. Board-certified child psychiatrists diagnosed ASD based on the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013). The diagnosis of ASD was further confirmed by the Chinese versions of the Autism Diagnostic Interview–Revised (ADI-R) (Gau et al., 2011; Lord et al., 1994) at first enrollment (Time 1) and follow-up (Time 2) and the Autism Diagnostic Observation Scale (Gau et al., 2011; Lo et al., 2019) at follow-up. Non-autistic participants were recruited via advertisements and received a clinical assessment to exclude those with a diagnosis of ASD. Both autistic children and their parents also received the Kiddie Epidemiologic Version of the Schedule for Affective Disorders and Schizophrenia (Puig-Antich & Chambers, 1978) for other psychiatric disorders to screen for any major neuropsychiatric disorders. Eventually, 289 autistic (aged 11.6 ± 3.8, male n = 255, 82.2%) and 203 non-autistic participants (aged 10.7 ± 2.9, male n = 100, 66.5%) completed the follow-up assessment. The follow-up ages were 16.9 ± 4.7 and 15.8 ± 3.9 in the autistic and non-autistic groups, respectively.
All the participants completed IQ assessments using the Wechsler Intelligence Scale for Children-IV (Wechsler, 2004) and reported on the Strength and Difficulty Questionnaire (SDQ) (Goodman, 1999). In addition, their parents completed the clinical measures to quantify autistic symptoms (Social Responsiveness Scale, SRS) (Constantino et al., 2003), behavior problems (Child Behavior Checklist, CBCL) (Achenbach, 1991), ADHD symptoms (the Swanson, Nolan, and Pelham–Version IV Scale, SNAP-IV) (Swanson et al., 2001), parenting style (Parental Bonding Instrument, PBI) (Cox et al., 2000), and school function (Social Adjustment Inventory for Children and Adolescents, SAICA) (John et al., 1987) at the first enrollment. At follow-up (around 5–8 years after the initial evaluation), the parents of all the participants completed the BRIEF scale for their real-world executive functions.
We conducted the study after approval by the Research Ethics Committee at the National Taiwan University Hospital (approval no. 201201006RIB; ClinicalTrials.gov no., NCT01582256 for Time 1; approval no. 201403109RINC, ClinicalTrials.gov no. NCT02233348 for Time 2 follow-up). In addition, written informed consent was obtained from all the participants and their parents after a detailed explanation of the objective and procedures of the study.
Measures
This study adopted the original versions of the SRS and BRIEF rather than the latest versions (e.g. SRS-2 and BRIEF-2) because only earlier versions had been translated into Chinese at the time of study implementation.
BRIEF
The BRIEF (Gioia et al., 2000) is an 86-item parent rating scale to assess daily, real-world executive function abilities in children ages 5–18 years. The measure comprises eight empirically derived scales, two global scales (the Behavioral Regulation Index [BRI] and the Metacognitive Index [MI]) based on factor analysis, and a composite score (Global Executive Composite [GEC]). The BRI includes Inhibit, Shift, and Emotional Control subscales, and the MI comprises the Initiate, Working Memory, Plan/Organize, Organization of Materials, and Monitor subscales. The BRIEF has good psychometric properties, high inter-rater, retest reliability, good face validity, and predictive validity. This study used the Chinese version of the parent-report BRIEF (Tsai et al., 2021) to assess everyday executive dysfunction.
SRS
The SRS is a 65-item self-rating scale that quantifies social deficits (Constantino et al., 2003). It measures the level of autistic symptoms in natural settings over the past 6 months (Constantino & Gruber, 2005). Items were rated on a 4-point Likert-type scale from “0” (not true) to “3” (almost always true). The Chinese version has adequate reliability and validity (Gau et al., 2013), with a four-factor structure including Social Communication, Stereotyped Behaviors/Interest, Social Awareness, and Social Emotion (Cronbach’s α, 0.94–0.95). The SRS in Chinese has been widely used in assessing autistic trait/symptoms in Taiwan (e.g. Chen et al., 2020; Lo et al., 2019; Tsai et al., 2021).
SNAP-IV
Parents reported the ADHD and oppositional defiant symptoms on the SNAP-IV (Swanson et al., 2001), a 26-item scale rating on a 4-point Likert-type scale (0 = “at all,” 1 = “just a little,” 2 = “quite a bit,” and 3 = “very much”). Eighteen items parallel to the diagnostic symptoms of ADHD (Items 1–9 for inattention symptoms; Items 10–18 for hyperactivity/impulsivity symptoms), and 8 items correspond to oppositional defiant disorder. The psychometric properties of the Chinese SNAP IV-Parent form are satisfactory (Gau et al., 2008), showing the same three-factor structure as its original version. The SNAP-IV Parent form in Chinese has been widely used in assessing ADHD/oppositional defiant symptoms in Taiwan (e.g. Chiang et al., 2022; Lin et al., 2023; Lin & Gau, 2019; Tung et al., 2021).
CBCL
The CBCL (Achenbach, 1991) is a parent-report questionnaire to screen for behavioral symptoms in youths aged 4–18 years, including withdrawal, somatic complaints, anxious/depressed symptoms, social problems, thought problems, attention problems, delinquent behaviors, and aggressive behaviors. Items are rated on a 3-point scale from “0” (not true) to “2” (very true or often true). The subscores were calculated by summing up the item responses of each construct described previously (Achenbach, 1991). The translation procedure and psychometric properties of Chinese CBCL have been documented (Yang et al., 2001).
SAICA
The SAICA is a semi-structured interview that assesses social functions in children aged 6–18 years using a 4-point Likert-type scale. The Chinese SAICA was a reliable and valid instrument for evaluating youth’s social functions (Gau et al., 2015)—parental reports on the school function and peer relations. The school function domains include academic grades (5 items), attitude toward school (4 items), social interactions at school (3 items), and behavioral problems at school (11 items). The peer relation subscale consists of interactions with peers (5 items) and problems with peers (12 items) (John et al., 1987). A higher score represents more severe problems. The SAICA in Chinese has been used in Taiwan’s research (e.g. Chiang & Gau, 2016; Chiang et al., 2018; Lin et al., 2021).
PBI
The PBI is a 25-item instrument measuring the parenting style during the child’s first 16 years. The PBI consists of two principal dimensions: Care (12 items) and Protection (13 items, including Authoritarianism and Overprotectiveness). Each item has a 4-point Likert-type scale from “very likely” to “very unlikely” to evaluate parenting styles. A high score on the Care scale reflects affection and warmth, whereas a low score indicates rejection, coldness, or indifference. The Authoritarianism subscale reflects either discouragement or encouragement of a child’s behavioral freedom, and the Overprotectiveness subscale reflects overprotective parenting and denial of the child’s psychological autonomy (Cox et al., 2000). The Chinese PBI is a reliable and valid instrument (Cronbach’s α 0.75–0.84) (Gau et al., 2010). The PBI in Chinese has been used to assess parenting in Taiwan’s research (e.g. Chang & Gau, 2017).
SDQ
The SDQ, a 25-item self-report screening questionnaire, was developed to assess a broad spectrum of psychological adjustments in children and adolescents (Goodman, 1999). Each behavioral item is rated on a 3-point Likert-type scale (“0,” not true; “1,” somewhat true, and “2,” certainly true). Factor analysis supported a five-factor structure, including emotional problems, prosocial behaviors, hyperactivity/inattention, conduct problems, and peer relationship problems. In addition, the Chinese version had good psychometric properties (Liu et al., 2013).
Statistical analysis
Statistical analysis was conducted using SAS program 9.4 (SAS Institute Inc., Cary, NC, USA). First, the demographics and subscores of clinical measures (i.e. SRS for autistic traits, SNAP-IV for ADHD symptoms/attention deficits, CBCL for behavior problems, SAICA for school behaviors, and PBI for parental bonding) were compared between autistic and non-autistic groups by independent t-test or chi-square test. Then, in variable selection, we used multiple regression to select significant subscales within each scale associated with executive dysfunction (on BRI and MI, respectively) at follow-up, controlling sex, age, full-scale IQ, and follow-up duration. For the significant subscales (p < 0.05), we then used mediation analysis to examine whether it mediated the relationship between diagnosis status and executive dysfunction (i.e. BRI or MI) at follow-up, with sex, age, full-scale IQ, and follow-up duration controlled in the model. Finally, all the significant mediators were included in a final multiple mediation analysis to test their mediation effects between the ASD diagnosis at baseline and executive dysfunction in late adolescence, controlling for sex, age, full-scale IQ, and duration of follow-up. The mediation analysis was performed on the Statistical Package for the Social Sciences (SPSS v.23) using the PROCESS macros (Hayes et al., 2017). In addition, a bootstrapping procedure with 5000 bootstrap samples was used to test the significance of the indirect effects (Preacher & Hayes, 2008). Using G*power 3.1.9.7 for power analysis of a statistical test on multiple linear regression (fixed model, single regression coefficient), the total sample 492 had 0.8 power to detect a mediator with effect size 0.016. We did not correct for multiple comparisons in single mediation analyses but adopted multiple mediation analyses to confirm the robustness of the findings.
Considering the sex and age difference between the autistic and non-autistic groups, we performed the above variable selection and mediation analyses again in a subsample matched on sex and age (ASD subgroup: n = 203, mean age, 16.4 ± 4.34 years, males n = 173 (85.2%) non-ASD subgroup: n = 174, mean age 15.9 ± 3.80 years, males n = 135 (77.6%)). The age (t = −1.13, p = 0.261) and sex (χ2 = 3.65, p = 0.056) were not statistically different between the two subgroups.
Community involvement
There is no community involved in this study.
Results
Comparisons between the autistic and non-autistic groups
At the first entry, the autistic group was 1 year older than the non-autistic group (Table 1). The autistic group had more males and lower full-scale IQ than the non-autistic group. At baseline, the autistic group had more autistic symptoms (SRS), more ADHD symptoms (SNAP) (Table 1), lower school function (SAICA), and more behavioral problems (parent-report CBCL and self-report SDQ) compared to the non-autistic group (Table 1). As for BRIEF, the autistic group scored higher on all the subscales (effect sizes ranging from 0.66 [for Task monitor] to 1.49 [for Shift]), BRI, MI, and GEC at follow-up than the non-autistic group (Table 2). The ASD diagnosis at Time 1 was significantly associated with the BRI and MI subscales.
Demographics and sample characteristics at Time 1 for the autism spectrum disorder (ASD) and non-autistic comparison (NAC) groups.
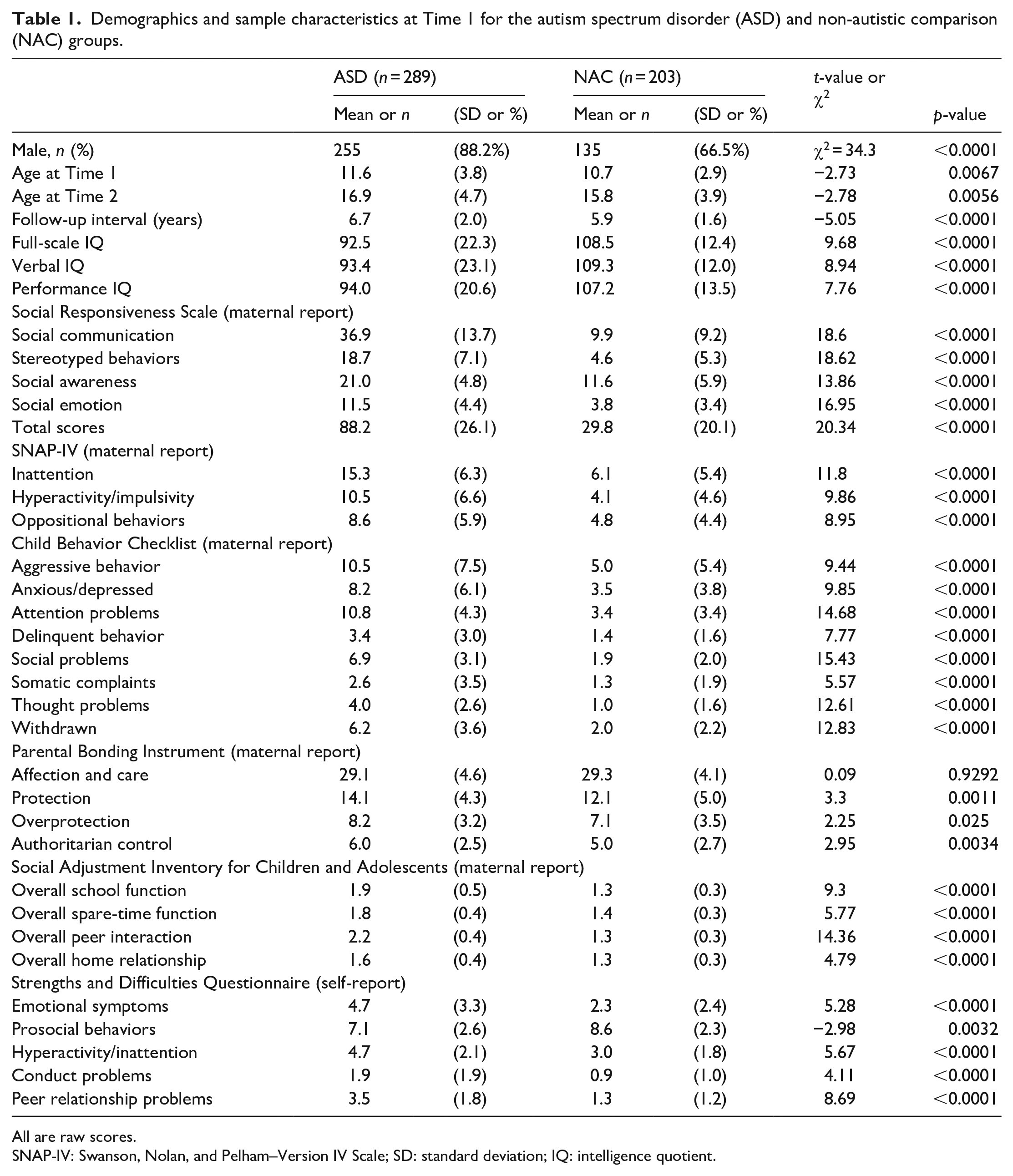
All are raw scores.
SNAP-IV: Swanson, Nolan, and Pelham–Version IV Scale; SD: standard deviation; IQ: intelligence quotient.
Real-world executive functions at Time 2 presented by the raw scores of BRIEF subscales for the autism spectrum disorder (ASD) and non-autistic comparison (NAC).
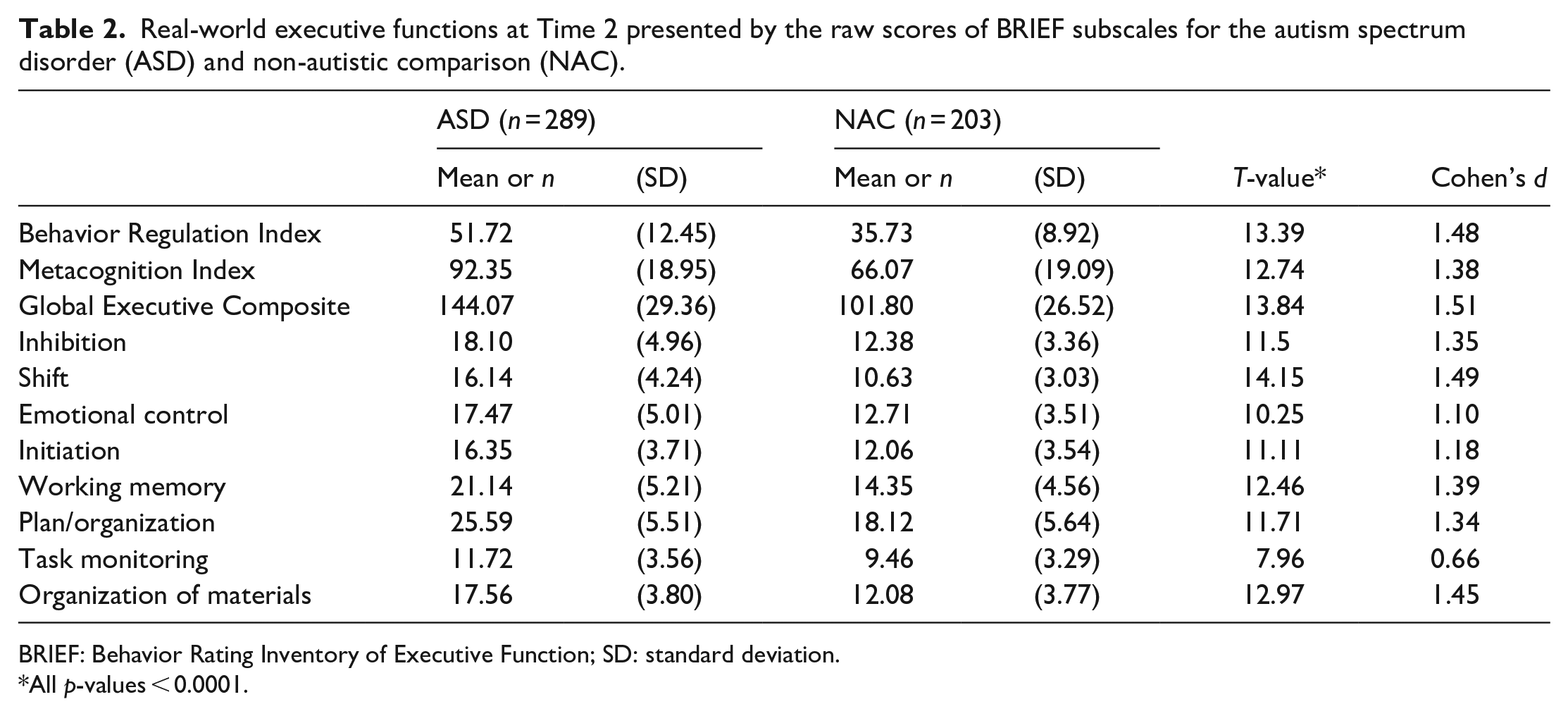
BRIEF: Behavior Rating Inventory of Executive Function; SD: standard deviation.
All p-values < 0.0001.
Variables selected by multiple regression
We performed the multiple regression model for the predictions of Time 1 clinical measures to the follow-up real-world executive functions. We present the model including all the predictors, regardless of the statistical significance of each regression coefficient (Supplementary Table S1), and the model only includes significant variables (Table 3). For the SNAP subscales, inattention and oppositional behaviors were associated with BRI, while inattention symptoms were associated with MI. As for the CBCL subscales, aggressive and withdrawn behaviors were associated with BRI, while inattention symptoms and withdrawn behaviors were associated with MI. Social communication symptoms were associated with both MI and BRI for the SRS subscales. As for PBI, all subscales were associated with BRI, while only the affection and care subscale was associated with MI. For the SAICA, the spare-time function was associated with BRI, and the school function was associated with MI. Finally, for the SDQ subscales, emotional problem and hyperactivity/inattention were associated with both BRI and MI and peer relationship was associated with MI.
Prediction of significant potential mediators at Time 1 to the BRIEF subscales at Time 2: Metacognition Index and Behavior Regulation Index based on multiple regression analyses.
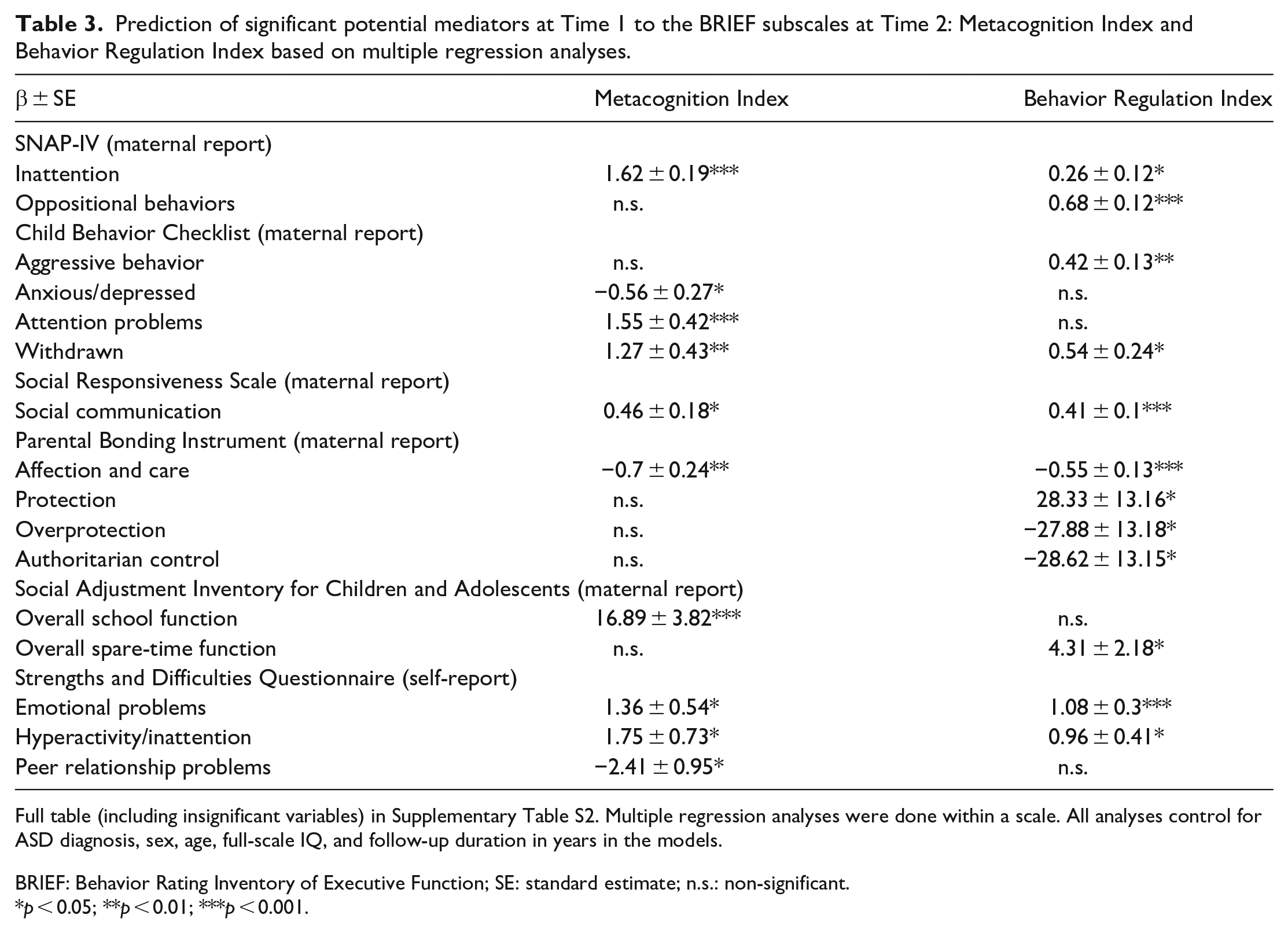
Full table (including insignificant variables) in Supplementary Table S2. Multiple regression analyses were done within a scale. All analyses control for ASD diagnosis, sex, age, full-scale IQ, and follow-up duration in years in the models.
BRIEF: Behavior Rating Inventory of Executive Function; SE: standard estimate; n.s.: non-significant.
p < 0.05; **p < 0.01; ***p < 0.001.
Single mediation analysis adjusting for age, sex, and full-scale IQ
For the selected variables from multiple regression, baseline inattention/oppositional symptoms (SNAP-IV), aggressive and withdrawn behaviors (CBCL), emotional problems, and hyperactive/inattention (self-report on SDQ) significantly mediated BRI at follow-up (Table 4). In contrast, baseline inattention symptoms (SNAP-IV and CBCL), withdrawn behaviors (CBCL), social communication deficits (SRS), emotional and hyperactivity/inattention problems, and overall school function significantly mediated MI at follow-up.
Significant mediators for the BRIEF subscales: Metacognition Index and Behavior Regulation Index.
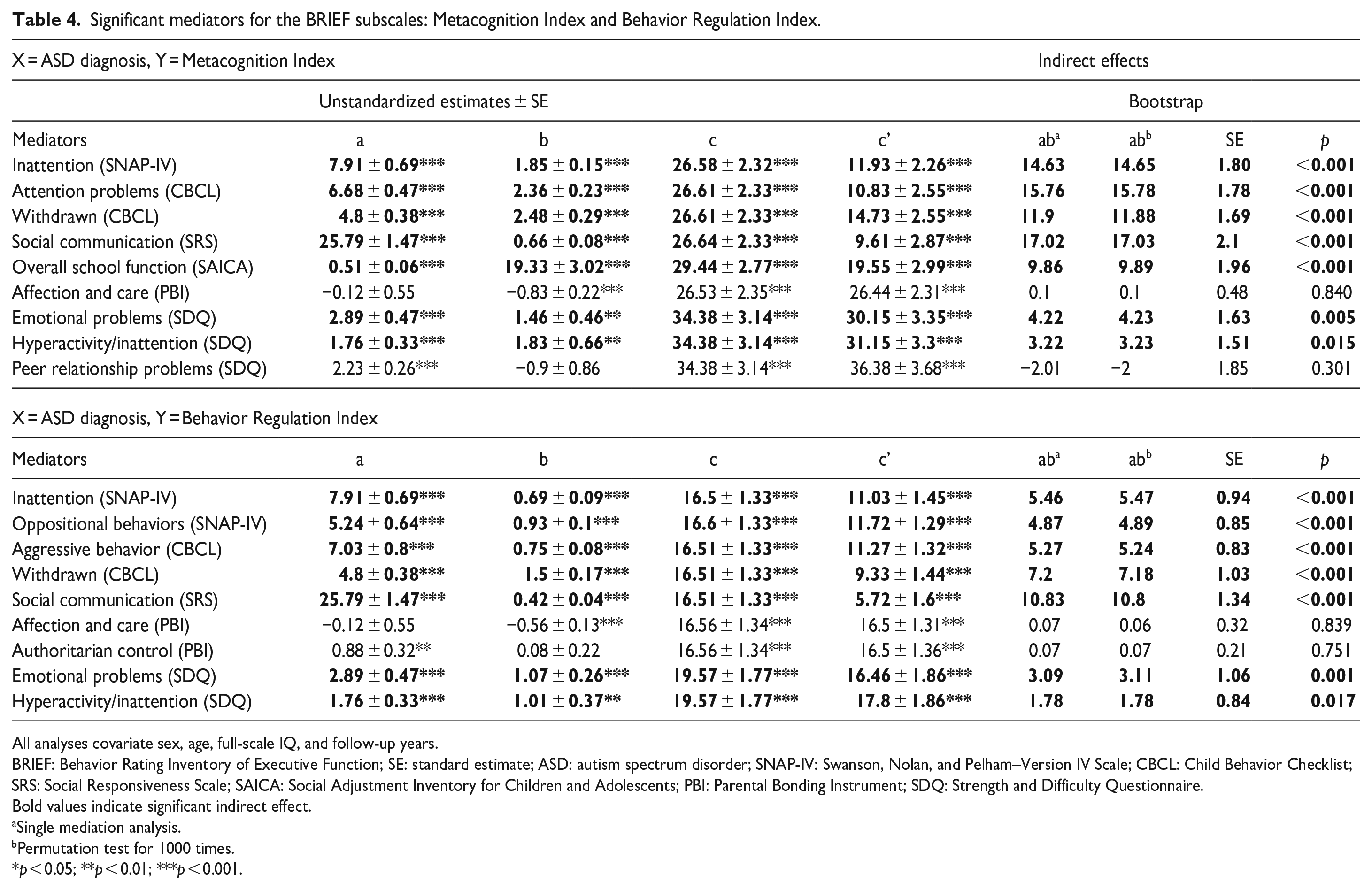
All analyses covariate sex, age, full-scale IQ, and follow-up years.
BRIEF: Behavior Rating Inventory of Executive Function; SE: standard estimate; ASD: autism spectrum disorder; SNAP-IV: Swanson, Nolan, and Pelham–Version IV Scale; CBCL: Child Behavior Checklist; SRS: Social Responsiveness Scale; SAICA: Social Adjustment Inventory for Children and Adolescents; PBI: Parental Bonding Instrument; SDQ: Strength and Difficulty Questionnaire.
Bold values indicate significant indirect effect.
Single mediation analysis.
Permutation test for 1000 times.
p < 0.05; **p < 0.01; ***p < 0.001.
Multiple mediation analysis
In multiple mediation analyses (Figure 1), baseline inattention and oppositional symptoms mediated BRI at follow-up (Figure 1(a)). In contrast, baseline inattention and self-report peer relationship mediated MI (Figure 1(b)) at follow-up. Notably, peer relationship was not significant in a single mediation analysis. Instead, it mediated executive functions while the effects of other mediators were considered.
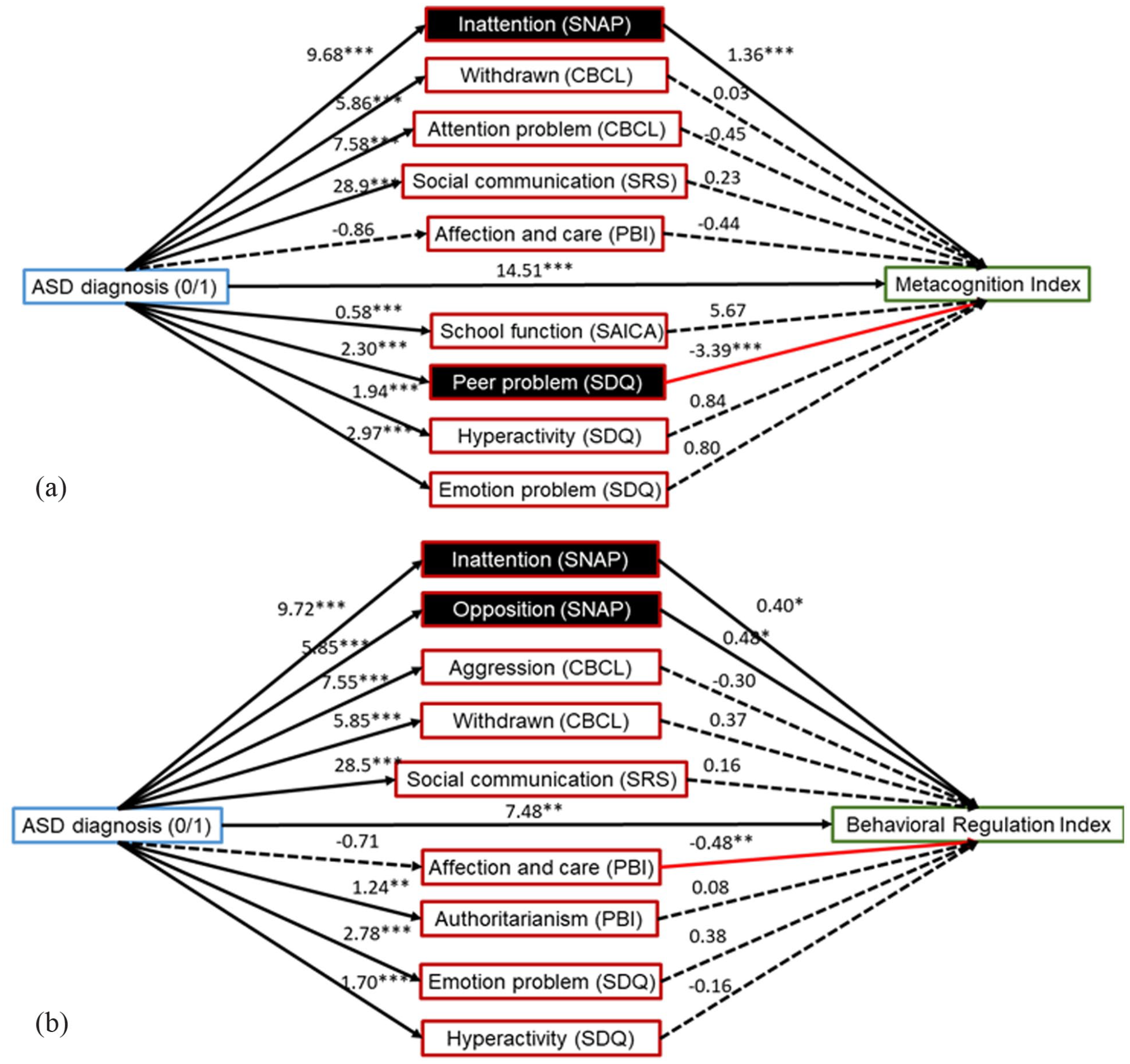
Mediators selected from single mediation analysis were included in the model of multiple mediation analysis for (a) Metacognition Index and (b) Behavior Regulation Index. The black box represents the significant mediators in the multiple mediation model. Solid lines represent the significant association, while dashed lines represent no significant relationship. Numbers were beta estimates.
In the age- and sex-matched subsample, most potential mediators from whole-sample multiple regression analyses remained significant in the subsample analyses (Supplementary Table S2). In multiple mediation analyses, childhood inattention remained a significant mediator for both BRI and MI, while childhood peer problems remained a significant mediator for MI in late adolescence (Supplementary Figure S1).
Discussion
As one of the few longitudinal follow-up studies on real-world executive functions in autism, we have the following findings. First, the autistic group had more severe real-world executive functional impairments, assessed by the BRI, MI, and GEC subscores of BRIEF during late adolescence and young adulthood than the non-autistic group. Second, among several factors hypothesized to mediate real-world executive dysfunctions, parent-reported inattention, withdrawn behaviors, social communication symptoms, and self-reported emotion and inattention/hyperactivity symptoms were significant mediators for both behavior regulation and metacognition, whereas oppositional and aggressive behaviors were significant mediators only for behavior regulation domain, and overall school function only for metacognition. Finally, multiple mediation analyses revealed that inattention remained a significant mediator for both behavior regulation and metacognition. In contrast, oppositional behaviors and peer problems were specific mediators for metacognition. Finally, in age- and sex-matched subsample analyses, childhood inattention remained an important mediator for both behavior regulation and metacognition. In contrast, peer problems remained a significant mediator for metacognition in late adolescence.
Our finding of executive dysfunction in autism was consistent with previous studies in autistic children and adolescents (aged 5–18 years) using the same scale, BRIEF (Blijd-Hoogewys et al., 2014; Gilotty et al., 2002; Gioia et al., 2002; Kenworthy et al., 2005; Rosenthal et al., 2013; van den Bergh et al., 2014), and with a study in autistic children and adult sample using the Dysexecutive Questionnaire (Johnston et al., 2019), supporting that broad-based daily executive dysfunction in autism persisted into young adulthood. Our results further endorsed a wide range of day-to-day executive functional impairments in autistic adolescents and adults with large effect sizes on all BRIEF subscales (all Cohen’s d > 1.0 except Task monitoring (0.66)), consistent with previous studies (Gilotty et al., 2002; Gioia et al., 2002; Kenworthy et al., 2005; Rosenthal et al., 2013). Our finding of the most significant effect size shown on the Shift scale (Cohen’s d = 1.49) of the BRIEF provided substantial evidence to support persistent difficulty in cognitive flexibility in autism (Chen et al., 2016). Training on flexibility appears to be necessary for autistic adolescents when they transit to adulthood. Ecologically based executive function training programs such as Unstuck and On Target! have been validated to improve flexibility, planning, and organization in autistic children aged 7–12 years (Kenworthy et al., 2014). An extended version modified for autistic adolescents will be invaluable.
Common mediators
Our findings supported several mediators for both behavior regulation and metacognitive domains of executive functions, including inattention, withdrawn behaviors, social communication, and emotional difficulties. A cross-sectional study reported that behavior regulation, but not metacognition, was related to depression in autistic and non-autistic children (Gardiner & Iarocci, 2018). Yet, another study reported that lower flexibility and metacognition in autistic adults were associated with anxiety and depression (Wallace et al., 2016). We found that parent-reported withdrawn behaviors and self-reported emotional symptoms in childhood predicted both behavior regulation and metacognition in late adolescence, supporting a dominant effect of internalization symptoms on later executive dysfunction in daily life. It has been proposed that greater reliance on reappraisal as an emotion regulation strategy reserved cognitive resources for attention and self-regulation and was associated with better executive functions in daily life. In contrast, reliance on suppression was related to lower executive functions (Lantrip et al., 2016). By showing that emotional symptoms in childhood may predispose to lower behavioral regulation and overall cognitive performance in late adolescence, our findings supported the link between emotion and executive functions in a developmental approach. In other words, adolescents’ ability to regulate their behaviors and organize their daily life might be enhanced by establishing an effective emotional regulation strategy in childhood.
In addition, we found that social communication difficulties also mediated both behavior regulation and metacognition in late adolescence. Previous studies regarding the link between autistic traits and executive function were contradictory. Two studies showed correlations between the behavior regulation index and three core symptoms on the ADI-R (Kenworthy et al., 2009) or overall autistic traits on the SRS (Tsai et al., 2021). In contrast, other studies reported no correlation with autistic traits measured by the total scores of the ADI-R (Johnston et al., 2019; Lee et al., 2021), Social Communication Questionnaire (Lee et al., 2021), or SRS (Bednarz et al., 2020). In studies that adopted executive function tasks in the laboratory, performance on task initiation, working memory, monitoring skills, and cognitive flexibility were negatively related to social communication symptoms in autism (Bednarz et al., 2020; Gilotty et al., 2002; Hill, 2004). Moreover, executive function, such as metacognition (Gardiner & Iarocci, 2018), was strongly associated with social and communication skills (Clark et al., 2002; Gilotty et al., 2002; Hutchison et al., 2020; McLean et al., 2014; Pugliese et al., 2015). Among the autistic characteristics, the social communication domain may be more important in mediating everyday executive functions in late adolescence.
Among the common mediators, inattention remained significant in multiple mediation analyses on both behavioral and cognitive executive dysfunction, suggesting that attention was the most important mediator considering all other variables. This finding was consistent with Lee et al. (2021), which suggests a linear relationship between ADHD symptoms (on the Connors’ Rating Scale) and overall executive functions (i.e. GEC) in autism. Evidence from ADHD studies also demonstrated executive dysfunction in each BRIEF domain in children (Gioia et al., 2002), adolescents (Toplak et al., 2008), and adults (Barkley & Murphy, 2010) with ADHD, supporting a close relationship between ADHD symptoms and executive dysfunction (Lukito et al., 2017). Lee et al. (2021) argued that if executive dysfunction was associated with ADHD symptoms, treatment of ADHD might effectively improve daily function. These findings underscore the importance of early intervention in the inattention symptoms in childhood and promise to enhance real-world executive functions later in young adulthood. In addition, psychosocial training on using strategies to keep focus, reduce distractibility, organize things, and make schedules may help improve executive functions in daily life and offset later functional impairment (Jensen et al., 2022; Kajka & Kulik, 2022).
Distinct mediator for metacognition
Metacognition in late adolescence was specifically mediated by parent-reported school function (in single mediation analysis) and child-reported peer problems (in multiple mediation analysis) in childhood. Executive dysfunction was not only related to academic performance (St. John et al., 2018) but also associated with playground isolation and less peer engagement, suggesting that metacognition—such as initiation, working memory, planning, and organization—was highly related to social functioning in autistic children (Freeman et al., 2017; Torske et al., 2017). A recent study has suggested that metacognition and behavioral regulation predicted distinct social functioning domains in autism (Bednarz et al., 2020). Our explorative finding extended the knowledge to a specific relationship on a longitudinal time frame between peer or school problems in childhood and metacognitive dysfunction in late adolescence that warrants further investigation. Peer relational issues and school problems in childhood may already reflect underlying metacognitive dysfunction that requires further assessment and support. Future works may consider providing executive function training in childhood and examine whether such intervention improves peer or school problems in childhood and changes the trajectory of everyday executive function in late adolescence.
Variables without mediation effects
Although parenting styles were correlated with executive dysfunction, they were not significant mediators for behavioral or cognitive executive dysfunction in late adolescence in either single or multiple mediation analyses. Yet, negative findings in this study did not weaken the importance of the parent–child relationship. Adequate resources that support parental mental health and enhance parenting skills may still benefit the development of everyday executive function (Siebelink et al., 2021) and mitigate the adverse effects of early life stress in the family for both autistic and non-autistic children (Kuenzel et al., 2021).
This study had several limitations to be addressed. First, the autistic group had more males, lower full-scale IQ, and longer follow-up years than the non-autistic group. Hence, these covariates were controlled in all statistical analyses. Besides, in the age- and sex-matched subsample, the main findings from the whole-sample analyses remained significant, implying that childhood inattention and peer problems were important mediators for real-world executive functions in late adolescence. Second, we used multiple regression to select significant subscales for further mediation analysis. Subscales less competitive in various regression models were discarded; thus, potential mediators with more minor effects may need to be addressed. Third, our sample included participants with IQ > 70; the results may not be generalized to the subpopulation accompanying intellectual disability. Nevertheless, this study had specific strengths as it adopted a prospective follow-up design to identify childhood mediators for everyday executive dysfunction in late adolescence. Multi-dimensional assessments from parent-report (including the autistic traits, ADHD symptoms, behavioral problems, parenting style, and school function) and child-report (strengths and difficulties) constitute another strength. Besides, both single and multiple mediation analyses were performed to unfold the robustness of the outstanding mediators.
In conclusion, this study demonstrated behavioral and cognitive executive dysfunctions in autistic adolescents approaching adulthood in daily life. Using multiple regression models, we found that social communication symptoms, inattention, internalization symptoms, and school function in childhood were common mediators for everyday executive functions in late adolescence, with oppositional behaviors and school function as specific mediators for behavioral and cognitive domains of executive function, respectively. Inattention demonstrated the most robust effect when other contributory factors were considered. Our findings highlight the importance of timely intervention for inattention and emotional symptoms in childhood, improving executive functions in late adolescence, and preparing autistic youths for adulthood.
Supplemental Material
sj-docx-1-aut-10.1177_13623613231184733 – Supplemental material for The mediators for the link between autism and real-world executive functions in adolescence and young adulthood
Supplemental material, sj-docx-1-aut-10.1177_13623613231184733 for The mediators for the link between autism and real-world executive functions in adolescence and young adulthood by Yi-Ling Chien, Yueh-Ming Tai, Yen-Nan Chiu, Wen-Che Tsai and Susan Shur-Fen Gau in Autism
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Science and Technology (NSC101-2627-B-002-002, NSC101-2314-B-002-136-MY3, MOST 103-2314-B-002-055-MY3), the National Taiwan University Hospital (NTUH101-S1910), and the National Health Research Institute (NHRI-EX104-10404PI, NHRI-EX105-10404PI, NHRI-EX106-10404PI, NHRI-EX107-10404PI, NHRI-EX108-10404PI), Taiwan.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the research committee of National Taiwan University Hospital, Taipei, Taiwan, and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data availability
Data sharing was subject to restriction imposed by the Research Ethics Committee of National Taiwan University Hospital, Taipei, Taiwan. For inquiries regarding the sharing of data, please contact corresponding author (S.S.-F.G).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.