
Abstract
The capacity of the workforce lags behind the current demand for timely autism diagnostic assessment. Primary care providers (PCPs) are well-positioned to diagnose autism at earlier ages than providers from other disciplines. Thus, bolstering PCPs’ diagnostic capabilities has been the focus of many recent capacity-building initiatives. Using data from the National Survey of Children’s Health, this study aimed to evaluate whether diagnosis of autism in primary care has changed over time and whether diagnosis in primary care relates to age at autism diagnosis. Results indicated that the likelihood of being diagnosed with autism by a PCP decreased by about 2% with every passing year from 2004 to 2019 when controlling for demographic characteristics. PCPs diagnosed children approximately 1 year earlier than non-PCPs (e.g., psychiatrists and psychologists), which supports the critical role PCPs can play in timely diagnosis. Further research is needed to understand why the proportion of children diagnosed by PCPs has decreased over time; however, these findings suggest that capacity-building initiatives have not yet reached community practice. Future research should focus on the dissemination and implementation of training initiatives in community-based primary care practices.
Lay abstract
The current demand for autism diagnostic services exceeds the ability of the workforce to assess and diagnose children in a timely manner. One solution may be to equip primary care providers (PCPs) with the tools and expertise needed to diagnose autism within their practice. PCPs are often trusted professionals who have many touchpoints with children during early development, in which they can identify early signs of autism. Recent initiatives have focused on bolstering PCPs’ diagnostic capabilities; however, no studies have examined how the rates of autism diagnosis in primary care have changed over time. We aimed to evaluate whether autism diagnosis in primary care has changed over time and how diagnosis in primary care relates to a child’s age at the time of diagnosis. We found that the likelihood of a child being diagnosed by a PCP decreased by about 2% with every passing year from 2004 to 2019 when accounting for demographic characteristics. In our sample, PCPs diagnosed children approximately 1 year earlier than non-PCPs (e.g., psychologists and psychiatrists). Further research is needed to understand why the proportion of children diagnosed by PCPs decreases over time. However, this decrease suggests more work is needed to get capacity-building initiatives into community primary care practice. Though we must continue to find effective ways to build community PCPs’ ability to diagnose autism, the present findings support the crucial role PCPs can play in early autism diagnosis.
There is considerable heterogeneity among the 1 in 36 children with autism spectrum disorder (hereby referred to as “autism”) in the United States (American Psychiatric Association, 2022; Maenner et al., 2023) with respect to core diagnostic features, communication style, adaptive functioning, intellectual functioning, and co-occurring conditions (Masi et al., 2017; Rosen et al., 2018). This hallmark heterogeneity presents clinical challenges to the diagnostic process, as there is no one sole autism presentation. Thus, detection and diagnosis of autism requires expertise.
Best practice protocols for autism diagnosis recommend the use of a multidisciplinary team to aid in the diagnostic process by allowing for multiple lenses through which a presenting child’s unique profile can be viewed (Penner, Anagnostou, Andoni, et al., 2018). While ideal, multidisciplinary teams are resource-intensive, and clinicians often must assess children independently (Penner, Anagnostou, & Ungar, 2018). When assessing for autism, clinicians primarily use The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria, expert clinical judgment, and, in many cases, standardized diagnostic tools such as the Autism Diagnostic Observation Schedule (Lord et al., 2012) and the Autism Diagnostic Interview-Revised (Lord et al., 1994). Many of these diagnostic tools require extensive training to reach clinical proficiency and reliability, often limiting their use to professionals practicing in specialized autism centers or academic medical settings. Thus, the traditional diagnostic process is time- and resource-intensive. Compounding this problem is a widespread shortage of clinicians with expertise in autism diagnosis, including developmental-behavioral pediatricians and psychologists specializing in autism (Bridgemohan et al., 2018; Ning et al., 2019).
The high level of resources needed to effectively diagnose paired with the rising prevalence of autism has contributed to the “waitlist crisis” in which many families find themselves (Kanne & Bishop, 2021; Makino et al., 2021; Siklos & Kerns, 2007; Wong et al., 2017). This crisis is characterized by the extensive waitlists in the United States to receive a diagnostic evaluation from a provider (Kanne & Bishop, 2021). Caregivers describe the service navigation process as a “diagnostic odyssey” that begins with the identification of autism symptoms (Lappé et al., 2018), requires multiple appointments with providers, and results in a considerable gap between caregiver’s first concern and the receipt of a diagnosis (MacKenzie et al., 2022). Both the researcher-deemed “crisis” (Kanne & Bishop, 2021) and caregiver-deemed “odyssey” (Lappé et al., 2018) result from the same fundamental challenge: The capacity of autism specialists lags far behind the demand for timely diagnoses.
In an effort to curb this crisis, there have been growing calls to expand the capacity of a broader range of professionals and disciplines to identify autism (Gordon-Lipkin et al., 2016; Zwaigenbaum & Warren, 2021). While psychologists continue to diagnose autism at greater rates than other providers (MacKenzie et al., 2022), many recent capacity-building initiatives focus on leveraging the diagnostic capabilities of primary care providers (PCPs) to identify autism rather than the traditional pathway of referring children to a specialty clinic with lengthy waitlists (Mazurek et al., 2019; Wieckowski et al., 2022; Zuckerman et al., 2021). PCPs are well-positioned to identify autism, as they are trusted community-based healthcare professionals who have ongoing and regular opportunities to monitor a child’s development across infancy, toddlerhood, and early childhood. In fact, studies from the United States and other Western countries highlight that caregivers often express their first concern to a physician, such as a pediatrician or general practitioner (Chamak & Bonniau, 2013; Chamak et al., 2011; Karim et al., 2014; MacKenzie et al., 2022). In addition, the American Academy of Pediatrics (AAP) released guidance in 2007 that recommended routine surveillance and standardized universal screening for autism-related symptoms during well-child visits, or visits with a pediatrician in which developmental progress is monitored at regular intervals (Myers et al., 2007). This guidance was reiterated and updated in 2020 (Hyman et al., 2020); however, these practices are implemented inconsistently (Mazurek et al., 2021; Wallis et al., 2020).
Findings from a systematic review suggest that capacity-building initiatives centered around training PCPs to use standardized screening or diagnostic protocols can promote the implementation of screening and diagnostic practices in routine primary care and bolster provider self-efficacy in identifying autism (Guan et al., 2022). Examples of such initiatives include programs such as START-ED (Warren et al., 2009), ECHO Autism (Bellesheim et al., 2020; Mazurek et al., 2017), and ECHO Autism STAT (Mazurek et al., 2019) that train PCPs to use standardized screening or diagnostic tools and employ diagnostic decision-making frameworks (Guan et al., 2022). Most evidence from these and related initiatives suggests that, in the majority of cases, PCP-provided diagnoses were consistent with the diagnostic decision of a multidisciplinary team or independent evaluation using standardized tools (Ahlers et al., 2019; Guan et al., 2022; Mcclure et al., 2010; Sohl et al., 2023). However, findings from one capacity-building initiative indicated that pediatricians may misclassify individuals without ongoing support and training (Warren et al., 2009). Evaluation of the effectiveness of these training initiatives to date has been based on pilot studies; thus, more research in this area is needed.
In addition to improved provider self-efficacy and diagnostic accuracy, outcomes from studies of physician training indicate an approximate 50% reduction in time to diagnosis (Ahlers et al., 2019; Harrison et al., 2017). The reduction in time from first concern to diagnosis does more than just alleviate pressure on the current diagnostic system. Timely receipt of an autism diagnosis is crucial to optimize developmental and mental health outcomes. A formal diagnosis is often required for access to treatment services (Jacobs et al., 2018; Lappé et al., 2018), and receiving autism treatment services within the first few years of life enhances positive developmental outcomes (Dawson, 2008; Zwaigenbaum et al., 2015). Though diagnoses can be made beginning at around 18 months of age (Hyman et al., 2020), the mean diagnostic age in the United States is around 4 years of age (Maenner et al., 2023). Many factors contribute to later diagnosis including being assigned female at birth, presenting with a more nuanced phenotypic profile (e.g., better social skills and higher verbal IQ), or being of lower socioeconomic status (Daniels & Mandell, 2014; Loubersac et al., 2023).
Conversely, one factor contributing to earlier diagnosis is attendance at primary care appointments. Attendance at well-child visits (Daniels & Mandell, 2013; DeGuzman et al., 2022) and being screened in primary care relates to an earlier age at diagnosis (Carbone et al., 2020; Hine et al., 2020) and thus swifter entry into treatment, like the early intervention system in the United States. The AAP recommends 14 well-child visits before the age of 4 years old, which provides numerous opportunities for the early identification of autism (Committee on Practice and Ambulatory Medicine & Bright Futures Periodicity Schedule Workgroup, 2023). Taken together, primary care is a vital setting to understand in relation to autism diagnosis.
Despite the crucial position of primary care in autism identification and recent efforts focused on increasing autism screening and diagnostic practices among PCPs, to date, no studies have characterized how the rate of PCPs diagnosing autism has changed over time. In turn, this study aimed to understand how diagnosis of autism in primary care has changed over time and how diagnosis in primary care relates to age at diagnosis. We hypothesized:
Given recent capacity-building initiatives, the rate of PCPs diagnosing autism has increased over time.
PCPs diagnose autism at earlier ages than non-PCPs.
Methods
Participants
Data from the 2016–2021 waves of the National Survey of Children’s Health (NSCH) were used (U.S. Census Bureau, 2016, 2017, 2018, 2019, 2020, 2021) for secondary analysis in the current study. The NSCH is a nationally representative caregiver-report survey of the health and well-being of children (birth to 17 years) in the United States. Each wave of the NSCH weights survey data to represent the population of noninstitutionalized children who live in housing units in each state and nationally. While 225,443 caregivers completed the NSCH over the 6 waves, the present sample (n = 5296) is limited to children with a caregiver-reported diagnosis of autism who met the inclusion criteria outlined below.
Children were excluded if their caregiver did not list a provider who first diagnosed their child’s autism (e.g., “don’t know”) and/or were unable to provide an age at which their child was first diagnosed. Due to the rapidly changing diagnostic landscape as a result of the COVID-19 pandemic (see Zwaigenbaum et al., 2021), children were excluded if their autism diagnosis took place after 2019. See Table 1 for the final sample’s full demographic information.
Sample demographic information (n = 5171).

Note. This table shows demographic characteristics for the final sample used in analyses. Group differences between those diagnosed by a primary care provider (PCP) and non-PCP were analyzed by demographic characteristics.
p < 0.05. **p < 0.01. ***p < 0.001.
Measures
Demographic information
Caregiver-reported child demographic information and relevant caregiver demographic information were collected through the NSCH (see Table 1), including child race, ethnicity, and sex. 1
Autism diagnosis
Caregiver respondents were asked if a healthcare professional had ever told them that their child had autism spectrum disorder, Asperger disorder, autistic disorder, or pervasive developmental disorder not otherwise specified (PDD-NOS) (hereafter, “autism”). Children of caregivers who responded affirmatively were included in the present sample.
Diagnostic professional
Caregivers who responded affirmatively to their child having an autism diagnosis were asked to retroactively report on the type of doctor or other health care provider who was the first to tell them their child had autism. Response options were PCP, specialist, school psychologist/counselor, other psychologist (non-school), psychiatrist, other, or don’t know. For this study, responses were collapsed into PCP and non-PCP (encompassing all other response options, excluding “don’t know”).
Age of child and year at diagnosis
Consistent with previous research using the NSCH (Emerson et al., 2016; Goldblum et al., 2023; Hanley et al., 2021; Jo et al., 2015), age at diagnosis was determined by caregiver report of their child’s age when a doctor or health care provider first told them their child had autism. Year at diagnosis was computed by first calculating the difference between the child’s age when their caregiver completed the NSCH and the age at which they were diagnosed. This difference was then subtracted from the year at which their caregiver completed the NSCH survey.
Data analytic plan
Data were analyzed in SPSS, v27. Descriptive statistics were generated for the total sample. A preliminary review of these data indicated certain years at diagnosis had high leverage points, which coincided with years in which there were fewer than 100 respondents from analyses (years 2000–2003). These years were removed from analyses, and the sample size for analyses reported is 5171 (125 children less than the original sample; years at diagnosis range: 2004–2019). Removal of these cases did not change the trends of results.
Binary logistic regression was used to test the first hypothesis, in which the dependent variable was a binary variable of diagnostic provider (PCP vs. non-PCP), and the predictor variable was year at diagnosis; covariates included indicator variables for child race, ethnicity, and sex. Due to the nature of data collection being nonconcurrent with the time of diagnosis, the inclusion of meaningful covariates was limited to those that remain the same across time, specifically the aforementioned demographic characteristics. Inclusion of other covariates was not possible because of the possibility that participant characteristics may have changed from the time of diagnosis to the time of survey completion. For example, participants may have moved from the location in which they were first diagnosed, changed insurance plans, or experienced changes in autism characteristics due to maturity or receipt of services. Pearson χ2 goodness-of-fit test was conducted to investigate model fit for binary logistic regression. For the second hypothesis, an independent samples t-test was used to assess group differences in age at diagnosis.
Community involvement statement
As these were secondary data analyses, there was no community involvement in this study.
Results
Rate of PCPs diagnosing autism over time
From 2004 to 2019, 14.3% of the sample was first diagnosed as having autism by their PCP. Results of the binary logistic regression to predict the likelihood of being diagnosed by a PCP over time, when controlling for demographic characteristics, suggest the year at which a child was diagnosed with autism was a negative and significant predictor of the probability of being diagnosed by a PCP (β = –0.02, Wald χ2 = 5.17, p = 0.02). The odds of being diagnosed by a PCP decreased by about 2% with every passing year from 2004 to 2019 (odds ratio (OR) = 0.98, 95% confidence interval CI (0.96, 1.00)). See Figure 1.
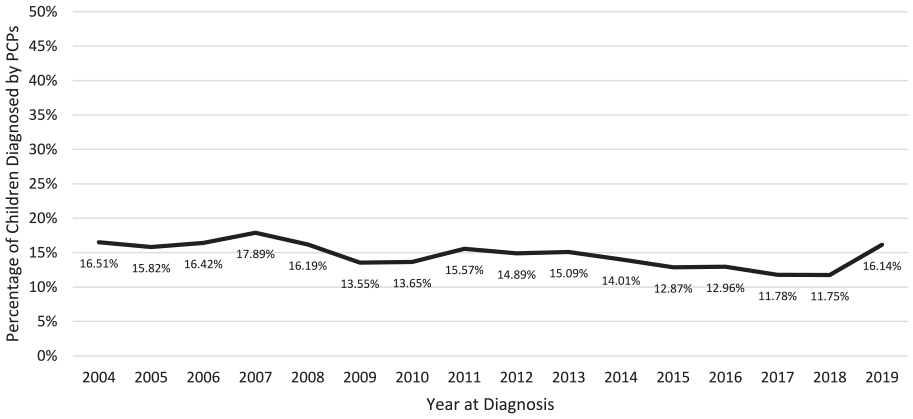
Proportion of children diagnosed by a primary care provider from 2004 to 2019 (n = 5171).
Relationship between diagnosing professional and age at diagnosis
Children whose autism was first diagnosed by a PCP were approximately 1 year younger at the time of diagnosis (MPCP = 4.10, SD = 2.67) than those whose autism was first diagnosed in non-primary care settings (Mnon-PCP = 5.30, SD = 3.38; t(1174.04) = 10.87, p < .001). See Figure 2.

Age at autism diagnosis by provider type.
Discussion
To date, there has been no literature documenting how the types of providers diagnosing autism may have changed over time in the United States. Given burgeoning attention to the role PCPs can play in early autism diagnosis, the present study focused on how autism diagnosis in primary care has changed over time and how diagnosis in primary care relates to children’s age at autism diagnosis in the United States. Findings indicated a small but significant decrease in the likelihood of autism being first diagnosed by a PCP over time between 2004 and 2019. Though over one-tenth of caregivers reported their child was first diagnosed by a PCP, the proportion waxed and waned greatly from 2004 to 2019. Importantly, the present findings support the role PCPs play in early access to diagnosis, as age at first diagnosis of autism was approximately one year earlier among children whose autism was first diagnosed by their PCP as compared with non-PCPs.
This was the first study to describe changes in autism diagnosis in primary care over time. Results indicate about one-tenth of children with autism were first diagnosed by their PCP over the past 15 years. The proportion of children whose autism was diagnosed by PCPs in the present community-based sample is similar to that in a research-ascertained sample diagnosed within the past few years (MacKenzie et al., 2022). Over the past 15 years, guidance from the AAP has attempted to embed autism screening and surveillance into routine clinical practice, and more recent training initiatives have focused on increasing workforce knowledge and capacity to diagnose autism in primary care settings. However, the present findings suggest that these initiatives may not have yet achieved their goal.
Though the first AAP guidance for autism identification in pediatric primary care was published in 2007, this guidance was primarily focused on screening and surveillance. Although this is a first step toward a formal diagnosis, positive screening results require further diagnostic assessment. Findings from a systematic review highlight that four out of six PCP diagnostic trainings or initiatives were published in 2014 or after, and all published initiatives were in the pilot stage (Guan et al., 2022). The lag between research to clinical practice in health sciences is approximately 17 years to reach routine clinical practice (Morris et al., 2011). Though research on diagnostic training initiatives was conducted in community settings (Ahlers et al., 2019; Swanson et al., 2014), the present findings suggest that these initiatives have not yet been widely implemented or disseminated and have had limited reach to everyday clinical practice (as of 2019).
Patient-level factors may account for the decrease in the likelihood of being diagnosed by a PCP in everyday clinical practice. From 2004 to 2019, autism awareness and healthcare professionals’ understanding of different phenotypes has dramatically changed. In turn, PCPs in recent years may be more likely to refer subtle phenotypic presentations to other providers for autism evaluation than they would have in the past; however, due to the limitations of the present dataset, this hypothesis could not be formally tested. Increased awareness may also lead caregivers to pursue specialty autism centers rather than consultation with a PCP. However, PCP referrals are often required by autism clinics prior to scheduling diagnostic evaluations, and there is literature spanning across time to support that caregivers often voice their first concerns to their PCP (Chamak & Bonniau, 2013; Chamak et al., 2011; Karim et al., 2014; MacKenzie et al., 2022). It may be that caregivers voicing concerns to a PCP and making an appointment at a specialty center are not mutually exclusive. For instance, caregivers with a greater awareness of autism may make an appointment at a specialty autism center for a comprehensive evaluation and consult their PCP in their interim, given their accessibility.
Provider-level factors such as lack of autism-related knowledge and self-efficacy may have also contributed to the limited scope of autism diagnosis in primary care over time. A recent systematic review revealed that providers across disciplines show low levels of knowledge and self-efficacy in working with autistic individuals (Corden et al., 2022). Specifically, PCPs report low self-efficacy in working with autistic children (Mazurek et al., 2020), and limited autism training in medical school, which in turn makes many feel unqualified to make a diagnosis (Finke et al., 2010). Alternatively, in cases where PCPs felt qualified to diagnose autism, they felt the current system of care prevented them from making the diagnosis, coining the opaque system as a “black box” (Hamp et al., 2022). Future qualitative research is needed to better understand both patient- and provider-level factors contributing to autism diagnosis in primary care.
Enhancing self-efficacy and knowledge of autism and the complex system of care may be essential for scaling up the identification and diagnosis of autism in primary care. Prior studies have demonstrated the impact of provider self-efficacy on autism identification practices in primary care. In a study focused on screening practices, PCPs with prior autism training and greater self-efficacy in screening and identification were more likely to implement autism screening in their practice (Mazurek et al., 2021). In addition, one study found the use of a PCP learning community effectively increased provider self-efficacy and provider implementation of high-fidelity autism identification (Carbone et al., 2016). The same learning community was also effective at reducing the common barriers to screening that many providers cite, namely, the lack of time and resources to screen in primary care.
Screening is the first step in the diagnostic process and a critical step for PCPs in tiered diagnostic models. In such models, a PCP screens for autism as they would in routine practice, diagnoses clear-cut cases of autism, and refers more complex cases to specialty providers (Hyman et al., 2020; Wieckowski et al., 2022). Cases in which a PCP feels comfortable diagnosing autism without referral to a specialty provider are likely cases who have explicit diagnostic features of autism, also conceptualized as “frank” autism in the literature (de Marchena & Miller, 2017). On the contrary, pediatricians in a Canadian study found it more difficult to diagnose children with a milder presentation of autism, who were older, or who had co-occurring conditions (Penner et al., 2017), all of which are also contributors to being diagnosed later with autism (Daniels & Mandell, 2014). Consequently, through tiered diagnostic models, PCPs can confidently diagnose those with clear autism features, who are likely to present with less diagnostic challenges than those with more subtle or complex profiles. Such diagnoses in primary care could reduce the waitlist crisis by using referral pathways for more complex cases.
Diagnostic models such as the tiered approach may lead to increased capacity and its downstream benefits, namely, shorter time from first concern to a diagnosis, younger age at diagnosis, timely access to treatment services, and alleviation of pressure on the current diagnostic system by letting specialists focus on more complex diagnostic profiles. However, increasing the diagnostic workforce also requires careful consideration of the potential concern in expanding the diagnostic workforce to professionals without specialized expertise in autism. The largest concern is the potential for PCPs to misclassify autism, which was seen in previous trainings or initiatives (e.g., Warren et al., 2009). However, a recent prospective study of the concordance between diagnoses made by community pediatricians and multidisciplinary teams demonstrated a high concordance between the two groups and highlighted that the accuracy of diagnoses related to clinician certainty (Penner et al., 2023). These disparate findings highlight the need for training initiatives to investigate how and when PCPs can make a diagnosis of autism, and under what conditions that diagnosis is accurate.
Alternative ways to build capacity in primary care should also be considered, including those that do not rely on PCPs acting as the sole diagnostician. For example, another proposed way to build diagnostic capacity employs behavioral health providers embedded within primary care as diagnosticians (Hine et al., 2018, 2020). Within this model, upon positive screening of a child for autism, pediatricians quickly transfer the case to behavioral health providers who conduct further assessment, in effect reducing the time from first concern to diagnosis in primary care without the need for a PCP to be trained in diagnostic assessment. While integrating behavioral health into pediatric primary care holds tremendous promise, the current medical system remains siloed, and such integration requires well-resourced systems of care that may take time to curate.
Limitations
Several study limitations should be noted. First, this study utilized large-scale survey data, which presents unique strengths and limitations. While the sample was nationally representative and large, some of the survey questions lacked specificity. Specifically, caregivers were asked when and by whom they were first told their child had autism rather than asking specific questions about diagnostic evaluation and timing, which is more typical when probing for prior developmental or medical history. Previous research on diagnostic timing using the NSCH has also operationalized these variables as being related to the time of diagnosis; however, due to the wording of the question, it is possible that some caregivers reported the professional and age at the time that their child screened positive for autism or was given a provisional diagnosis to access services. In addition, some of the categories of professionals were opaque, including a “specialist” category without additional criteria. Considering this and the central focus of the study on PCPs, this study did not separate out those in the non-PCP group. Future research is needed to systematically examine how the capacity of all healthcare professions capable of diagnosis has shifted over time.
Due to the nature of the sample, inclusion of meaningful covariates such as whether or not someone lived in a rural area, what insurance type they had, or what diagnostic features they had were not possible, as these factors may have changed from the time of diagnosis to time of survey completion. It is likely the inclusion of these covariates would have had an impact on the present findings (DeGuzman et al., 2021); however, this study offers the first descriptive account of changing autism diagnosis rates in primary care over time. These findings may be useful in providing a baseline and informing more robust prospective studies in the future. In addition, these data were cross-sectional and retrospective, which impeded the ability to draw causal links between time and the likelihood of diagnosis by a PCP.
Finally, other factors changing over the course of 2004–2019 in the field could not be directly tested but should be noted in the interpretation of these results. Namely, the diagnostic criteria, prevalence rates, and understanding of autism have changed drastically over the course of the included 15-year period. With the change from DSM-IV to DSM-5 in 2013, autism diagnoses changed from separate but related diagnoses (e.g., PDD-NOS, Asperger’s, and autistic disorder) to one all-encompassing diagnosis of autism spectrum disorder. The NSCH directly probes for diagnoses listed in both the DSM-IV and DSM-5 (e.g., Asperger’s, PDD-NOS, and autism spectrum disorder), thus children diagnosed using both criteria are included in the present sample. As the diagnostic criteria shifted, so did prevalence rates of autism from 1 in 125 in the year 2004 to 1 in 44 in 2018. The higher prevalence rate may be due to a multitude of factors, such as changes to the diagnostic criteria, more sensitive detection tools, and a better understanding of autism and its many clinical presentations across healthcare disciplines.
Conclusions
From 2004 to 2019, approximately one-tenth of children in the present sample were first diagnosed with autism by a PCP, and PCPs diagnosed autism earlier than their counterparts outside of primary care. The current results suggest a decrease in the likelihood of autism being first diagnosed by a PCP over time between 2004 and 2019. Autism training initiatives that focus on provider knowledge, skill, and self-efficacy may be the key needed to unlock a more expansive workforce, and future research should prioritize hybrid effectiveness-implementation evaluation of these trainings to identify factors that may promote uptake, dissemination, and reduced time from research to practice (Curran et al., 2012). Future research must also continue to monitor the effectiveness of such training models to ensure resultant accurate diagnoses of autism. Overall, the current results indicate that more widespread access to diagnosis in primary care settings may have the potential to greatly reduce diagnostic delays in the years to come.
Footnotes
Data availability statement
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.