
Abstract
This study builds on existing literature on autism spectrum disorder (autism) and sexual and gender minority (SGM) identities and is the first to examine self-declared frequency rates, associated functional impairments, and treatment engagement levels for sexual minority (SM) and non-SM populations with and without autism cross-sectionally via a large nationwide college-student sample across 3 years. Using data from the American College Health Association-National College Health Assessment (ACHA-NCHA) III, we analyzed data from 81,286 college students (ages 18–25 years old) randomly selected from 75 U.S. colleges and universities. Included ACHA-NCHA-III measures consisted of self-reported demographics, SM and gender minority (GM) identities, autism diagnosis, stress, academic impairment, mental health symptoms, and treatment engagement. We found a 2.8% self-declared frequency of autism in the SM group, compared with 0.9% self-declared frequency among the non-SM sample. Autistic college students with both SM and GM identities had the greatest levels of reported adverse stress and the most negative academic and mental health outcomes (i.e., suicidality), followed by college students with two minority identities (i.e., Autism and SM, SM and GM), across all groups. These findings emphasize the need for mental healthcare providers to consider SM and GM identities in non-autistic and, especially, in autistic college students to assess suicide risk and inform treatment.
Lay abstract
Autistic individuals and those who identify with a sexual and/or gender minority are both at risk for various mental health concerns and related impairments. However, the connection between autism and sexual and/or gender minorities and mental health and functional outcomes is not clear. Here, we provide evidence of these connections by analyzing data from a large nationally representative dataset from the American College Health Association-National College Health Assessment III. We found that autistic college students who identify with both sexual and gender minorities reported the highest rates of stress, academic, and mental health concerns including suicidality when compared with autistic college students with or without a sexual and/or gender minority. In addition, college students with at least two identities, such as autism and a sexual minority identity or both a sexual and gender minority identity, reported the next highest rates of concern. These findings affirm the need for mental healthcare providers to consider the intersections of a sexual and gender minority identities in non-autistic and, especially, in autistic college students to develop and provide better support and resources.
Autism spectrum disorder (autism) is a neurodevelopmental disorder characterized by deficits in social communication and the presence of restricted/repetitive behaviors, interests, or activities (American Psychiatric Association (APA), 2022). The prevalence rate of autism is approximately 2% in both adults (Dietz et al., 2020) and college students (White et al., 2011). The number of autistic young adults attending college is increasing steadily (Bakker et al., 2019; Volkmar et al., 2017).
Students who identify with sexual and gender minority (SGM) identities are also increasingly prevalent on college campuses (American College Health Association (ACHA), 2020). Briefly, sexual minority (SM) groups may include individuals who identify as lesbian, gay, bisexual, asexual, or other non-heterosexual sexual orientations, while gender minority (GM) groups may include individuals who identify as transgender, non-binary, intersex, or other non-cis-gender identities (U.S. Department of Health and Human Services, 2021).
While autism, SM, and GM identities are increasingly prevalent on college campuses, research focusing on the intersection of autism, SM, and GM in college students has been very limited. Autistic adults with both SM and GM identities face more barriers to healthcare access compared with autistic individuals without SGM identities (Hall et al., 2020). These findings are unsurprising given the increased healthcare accessibility barriers faced by individuals with SM and/or GM identities (e.g., concerns of experiencing prejudice and/or discrimination from providers due to their SM and/or GM identities leads to avoidance of services; Batza, 2018; Simpson et al., 2013; Streed et al., 2019). Taken together, minority stress theory (Meyer, 2003) and intersectional stigma (Maroney & Horne, 2022) predict that autistic individuals belonging to minority groups will experience higher rates of mental health problems due to compounding stressors that may be further exacerbated in the presence of two or more intersecting minority identities. This study seeks to expand on the existing literature on autism and SGM by specifically examining self-declared frequency rates, functional outcomes, mental health correlates, and mental health treatment patterns for autistic and non-autistic college students with non-SM, SM, and both SM and GM identities. This study incrementally advances the field by using a large nationally representative college student sample, examining SM populations with and without GM identities separately, and assessing important mental health factors (e.g., suicidality) and functional outcomes that have never been previously considered.
Autism spectrum disorder (Autism)
Approximately 70% of autistic individuals experience at least one co-occurring psychiatric disorder and approximately 40% experience two or more co-occurring psychiatric disorders (APA, 2022; Simonoff et al., 2008). The most common co-occurring conditions in autistic college students are anxiety, depression, attention-deficit/hyperactivity disorder (ADHD), and learning disorders (Anderson et al., 2018; McMorris et al., 2019). Autistic college students also experience difficulties with activities of daily living, social perception, executive functioning, and emotion regulation (Baribeau et al., 2015; Gobbo & Shmulsky, 2012; Hewitt, 2011; White et al., 2016). Many of these associated features of autism are further exacerbated by autism stigma and accompanying stress (Botha & Frost, 2020). Importantly, autistic college students are less likely to seek out and engage in mental health treatments compared with individuals with mental health conditions other than autism (Chandrasekhar, 2020).
Likely due to the compounding effects of these associated features and stigma, autistic college students face additional academic and social challenges. Only 17%–35% of autistic individuals attend 2- or 4-year colleges (Newman et al., 2011; Roux et al., 2015; Shattuck et al., 2012). Among those who attend college, autistic individuals tend to underachieve academically (Kapp et al., 2013) and experience difficulties forming social relationships (Sasson et al., 2013; Test et al., 2014). For example, graduation rates for autistic college students are 38.8% as compared with 52.4% in the general population (Newman et al., 2011).
Autistic college students are also at increased risk of engaging in risky behaviors. Systematic reviews and meta-analytic evidence indicate substance use (particularly alcohol, cannabis, and nicotine use) may be more prevalent in adult autism populations compared with non-autism populations (Haasbroek & Morojele, 2021; Lugo-Marin et al., 2019). However, autism is associated with lower rates of substance abuse (i.e., clinically impairing levels of substance use) among college students compared with those without autism (Kuder et al., 2021; Yule et al., 2021), though autistic individuals are nearly nine times more likely to engage in substance use to self-manage mental health symptoms compared with those without autism (Weir et al., 2021). In addition to substance use, young adults with autism have higher rates of suicide attempts (Kirby et al., 2019) and deaths by suicide (Chen et al., 2017) compared with the general population. However, to the best of these authors’ knowledge, no studies todate have examined the prevalence of suicidality in autistic college students within the United States specifically.
Sexual and gender minorities
Much like autism, college students who hold an SGM identity are at higher risk for psychiatric disorders, such as anxiety and depression, compared with students without an SGM identity (Busby et al., 2020). SGM college students experience both proximal stressors, such as rejection sensitivity and internalized homonegativity, and distal stressors, such as discrimination, physical victimization, and verbal harassment. These stressors, in turn, increase the risk for the development of psychiatric conditions (Meyer, 2003; Pachankis et al., 2018; Rosendale et al., 2021).
SM college students are at higher risk for substance abuse as compared with non-SM individuals (Rice et al., 2019). Similar to autism, SGM individuals have higher prevalence rates of suicide attempts and deaths by suicide than non-SGM individuals (Hatzenbuehler & Keys 2013), with 11% of individuals with SM identities (Hottes et al., 2016) and 40% of individuals with GM identities (Marshall et al., 2016) reporting at least one suicide attempt throughout their lifetime, compared with 4% in the general population. Both SM and GM college students are more likely to seek out mental health treatments than non-SGM college students but are also more likely to discontinue treatment prematurely due to feeling that their treatment needs are not being met by providers (Burgess et al., 2007; Dunbar et al., 2017). In addition, both SM and GM individuals engage in more non-suicidal self-injurious (NSSI) behaviors compared with individuals without an SGM identity (Bretherton et al., 2021; Frisell et al., 2010) and SM individuals are three times more likely to engage in NSSI behaviors compared with same-aged heterosexual peers (Batejan et al., 2015).
Autism and SM and GM identities
Very few studies have examined the intersectionality of autism, SM, and GM despite findings that adolescents and adults (ages 16–70 years old) with autism are seven to eight times more likely to identify as belonging to an SM group (Weir et al., 2021). The prevalence of autism within GM youth (ages 14–25 years old) is approximately 23% (Strauss et al., 2021). Furthermore, one recent study found approximately 41% of autistic adults (ages 18–83 years old) reported identifying with an SM group (McQuaid et al., 2023). However, no study to date has examined the prevalence rates of autism specifically within SM college students, which is perhaps surprising given the independently increasing rates of both autistic students and students with SGM identities pursuing higher education. One study considered mental health symptoms in a broader age range (ages 18–42 years old) of autistic adults stratified by sexual orientation (George & Stokes, 2018). Results indicated that mental health symptoms were not different between autistic heterosexual adults and autistic non-heterosexual adults; however, these relations have yet to be examined specifically in college populations. Another study found higher rates of autism along with other mental health conditions in individuals (ages 16–90 years old) identifying as transgender (Warrier et al., 2020). While these few studies have independently examined autism within SM and GM separately, the rates of functional impairments, additional mental health correlates (e.g. loneliness and suicidality), and rate of mental health treatment engagement within autistic SM college student populations with and without GM identities have largely been unexamined despite each identity being associated with significant societal barriers that impact functioning. Addressing these gaps in the literature using samples that include autistic SM college students with and without GM identities is necessary to inform our understanding and treatment of difficulties experienced by autistic college students with SM identities.
Better understanding of autism in SGM college students is a clinically significant topic for several reasons. First, as noted above, both SGM identities and autism are increasingly prevalent among college students. Second, as predicted by both minority stress and intersectionality theories, negative outcomes may be more common in college students with two or more intersecting minority identities. Third, individuals belonging to two minoritized groups tend to be marginalized by members in one or both of their identified minority groups (Purdie-Vaughns & Eibach, 2008). Thus, autistic SM and GM college students are more likely to experience increased stigma and more negative functional and mental health outcomes than SGM college students without autism, non-SGM autistic individuals, and non-SGM individuals without autism. Despite seeming intuitive, this hypothesis has never been empirically tested.
Current study
This study is the first to investigate the self-declared frequency rates, functional outcomes, and treatment engagement levels for autistic and non-autistic college students with non-SM and SM identities with and without GM identities via a large nationally representative college-student sample. As such, this study fills in notable gaps in the literature by providing a comprehensive examination of treatment engagement levels and functional outcomes reported by both autistic and SGM college students across six distinct groups (i.e., Autism-only, SM + Autism, SM + GM + Autism, SM + GM, SM-only, and Comparison) to examine the effects of having multiple minority identities. In addition, this study improves our understanding of potential differences experienced by SM individuals with and without GM identities. In the originally submitted version of this article (pre-print link: https://doi.org/10.31234/osf.io/8bxfq), the primary hypothesis included examining these factors more broadly within autistic SGM and non-SGM college students. However, these initial hypotheses shifted during the course of the peer-review process given compounding evidence that SM and GM groups should be examined separately (Bouzy et al., 2023; National Academies of Sciences, Engineering, and Medicine, 2022). Accordingly, our revised current first aim is to determine the self-declared frequency rates among the intersections of autism and SM. We predicted (1) higher self-declared frequency rates of autism among SM college students compared with non-SM college students. Second, in line with prior literature demonstrating functional and psychiatric impairments for both autism and SM groups independently, we aimed to investigate academic, social, and mental health correlates across autism and SM groups (SM with and without GM identities). Specifically, we hypothesize that (2) autistic individuals with both SM and GM identities (SM + GM + Autism) will have higher reported rates of academic, functional, and mental health impairments, followed by autistic individuals with SM identities (SM + Autism), compared with SM individuals without autism (SM-only, SM + GM), non-SGM autistic individuals (Autism-only), and non-SGM individuals without autism (Comparison). Finally, consistent with empirical work highlighting stigma and barriers to receiving care, we hypothesize that (3) autistic individuals with both SM and GM identities (SM + GM + Autism) would report the lowest mental health treatment engagement rates.
Methods
A secondary analysis of data from the American College Health Association-National College Health Assessment (ACHA-NCHA) III (ACHA, 2019–2022) was conducted for this study. The ACHA-NCHA III survey was administered through 75 participating colleges and universities during both fall and spring semesters. Each campus followed their respective institutional policies and distributed the survey in-person on campus or online. Data were collected from randomly selected students or collected from surveyed students in randomly selected classrooms from participating colleges/universities. These random sampling techniques and this large reference group obtained have contributed to the ACHA-NCHA being considered to be a useful study design for understanding contemporary trends in college student health (Kerr et al., 2021).
Participants and group assignment
This study sample consisted of 81,286 self-reported full-time or part-time enrolled college/university students between the ages of 18–25 years old (M = 20.40, SD = 1.89). Most participants self-identified as women (68.6%), were full-time students (95.0%), were not in a current romantic relationship (56.9%), were living on-campus or within university housing (44.3%), and were covered by their parents’ health insurance (75.1%). The total sample ethnicity was 68.2% White, 13.5% Asian/Asian American, 13.5% Hispanic/Latino, 7.5% Black/African American, 4.2% Biracial/Multiracial, 2.2% American Indian/Native Alaskan, and 1.4% Middle Eastern/North African or Arab Origin. Consistent with this study’s aims, participants were assigned into one of six mutually exclusive groups based on autism status and SM identity with and without GM identities: Autism-only (n = 565), SM + Autism (n = 290), SM + GM + Autism (n = 187), SM-only (n = 14,871), SM + GM (n = 1988), and Comparison (n = 63,385). While the original intention was to study Autism in GM students, the number of GM participants who identified as autistic (n = 9) was too small to permit inclusion.
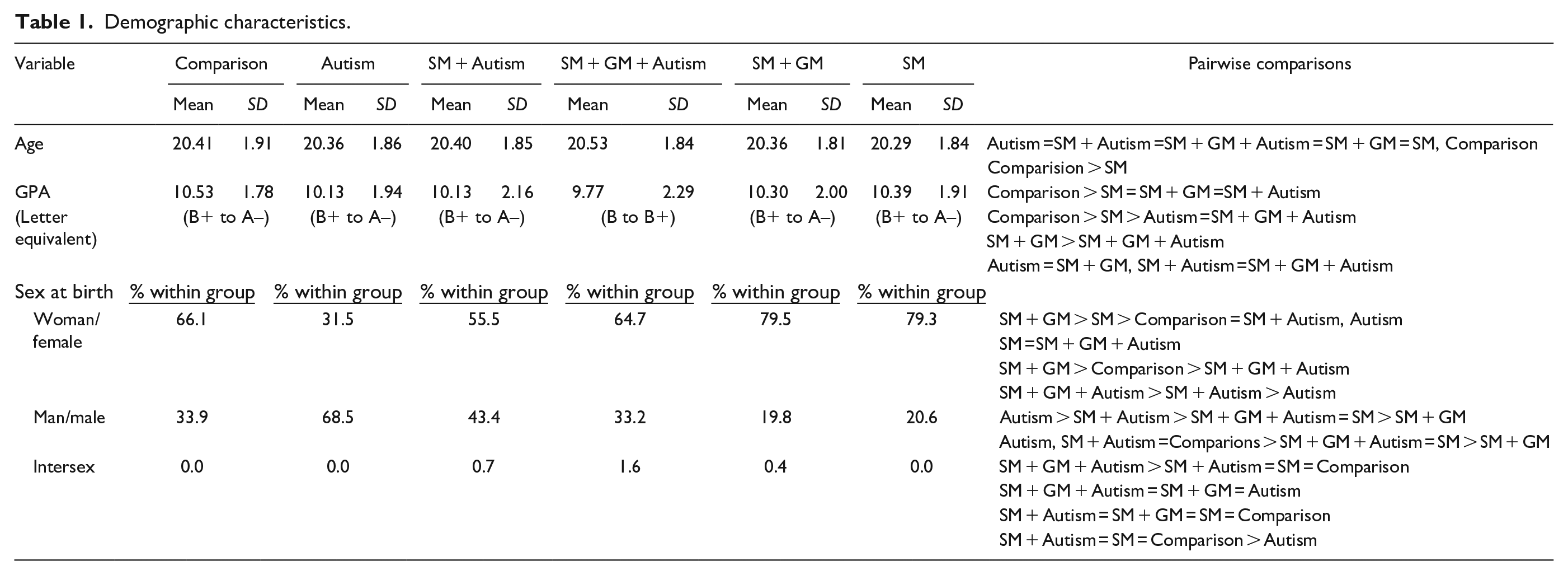
Descriptive statistics for all demographic variables are presented in Table 1 and Supplemental Table 1. The mean age of participants significantly differed among the six groups, F(5, 81,286) = 9.25, p < .001, η2 < .001, such that participants in the SM-only group were younger than the other five groups. Given that age was associated with several of the outcome variables (see Supplemental Table 2), age was statistically controlled for in all analyses.
Demographic characteristics.
Community involvement
No members of the autism community were involved in the original study research question, study design, measures, implementation, or interpretation of these findings as this is a secondary analysis of data from the ACHA-NCHA III survey. As such, interpretations of results may not be fully reflective of those of the autism community. The authors will discuss the results of this study with members of the public via conference and poster presentations.
Measures
Autism diagnostic status
Autism diagnostic status was a dichotomous variable (Yes/No) determined by participants who endorsed “yes” to whether they have ever been diagnosed with autism by a healthcare or mental health professional. The autism diagnostic status variable was used in all hypothesis tests.
SM and GM identities
SM and GM identities were coded as two separate dichotomous variables (SM/non-SM; GM/non-GM, respectively) derived from participant responses to questions about their sexual orientations and gender identities. Individuals who endorsed a sexual orientation other than straight/heterosexual (i.e., bisexual, gay, lesbian, pansexual, queer, or “other sexual orientation identities not listed”; Supplemental Table 3) were coded as having an SM identity. Similarly, individuals who endorsed any gender identity other than woman or man (i.e., trans woman, trans man, genderqueer, agender, gender fluid, intersex, non-binary, and “other gender identity not listed”; Supplemental Table 3) were coded as having a GM identity.
The SM variable was used for hypothesis 1. Both the SM and GM variables were used to determine the group assignment to be used for all other hypotheses. Participants with overlapping SM and GM identities were classified as the SM + GM group, while participants with only SM identities were classified in one of the two SM groups (i.e., SM-Autism and SM-only).
Past year stress and distress
Participants were asked to rate their level of general past-year stress using a Likert-type scale (1 = No Stress to 4 = High Stress). In addition, participants rated their level of domain-specific past-year distress using a Likert-type Scale (1 = No Distress to 4 = High Distress) for six domains: academics, faculty relationships, family relationships, intimate relationships, roommates/housemate relationships, and peer relationships. For past-year stress and all six past-year distress domain variables, higher scores indicated more self-reported stress/distress. The stress/distress variables were included in analyses for Hypothesis 2.
Academic performance and impairment
Academic performance
Academic performance was measured using self-reported cumulative grade point average (GPA). Participants rated their approximate cumulative GPA on a scale such that lower values represent poorer academic performance (i.e., F = 1, D–= 2, D = 3, D+= 4, C– = 5, C = 6, C+= 7, B–= 8, B = 9, B+= 10, A–= 11, A = 12, and A+= 13).
Academic impairment
Academic impairment related to mental health factors and interpersonal factors were also measured. Academic impairment was defined as class performance being negatively impacted and/or progress toward degree being delayed. To assess academic impairment, the extent to which four mental health factors (i.e., anxiety, depression, posttraumatic stress disorder (PTSD), and stress) and five interpersonal factors (i.e., intimate, faculty, family, roommates/housemates, and peer relationships) affected academic performance was collected for participants who indicated those factors had been a problem for them within the previous 12 months. Participants rated impacts on academic performance using a Likert-type scale (0 = I did not experience this issue/Not Applicable; 1 = This issue did not affect my academic performance; 2 = This issue negatively impacted my performance in a class; 3 = This issue delayed progress toward my degree) for each of the four mental health and five interpersonal factors. Higher scores represent increased perceived academic impairment related to these factors. The academic performance and impairment variables were examined in Hypothesis 2 analyses.
Mental health correlates
All nine mental health correlate variables were included in analyses for Hypothesis 2.
Connor-Davidson Resilience Scale – two-item version (CD-RISC 2)
The CD-RISC 2 (Vaishnavi et al., 2007) is a two-item scale that measures an individual’s ability to adapt and bounce back after experiencing hardships. Participants rated the extent to which a statement applies to them (e.g., “I am able to adapt when changes occur” and “I tend to bounce back, after illness, injury, or other hardships”) using a 5-point Likert-type scale (0 = Not at all true to 4 = True nearly all the time). Total CD-RISC 2 scores ranged from 0 to 8 with higher scores indicating greater perceived resilience. Cronbach’s alpha for the current sample was .76, indicating acceptable internal consistency. While longer versions of the CD-RISC have been used with autistic adult populations (Hwang et al., 2020), the CD-RISC-2 has not been used with autistic college students or college students with SM and/or GM identities.
Diener-Flourishing Scale (FS)
The FS (Diener et al., 2010) is an eight-item scale designed to measure an individual’s self-perceived achievement in categories such as optimism, purpose, relationships, and self-esteem. Participants rated the extent to which each item statement applies to them (e.g., “I am a good person and lead a good life”) using a 7-point Likert-type scale (1 = Strongly Disagree to 7 = Strongly Agree). Total FS scores range from 7 to 56 with higher scores indicating greater perceived psychological resources and strengths. Cronbach’s alpha for the current sample was .93, indicating excellent internal consistency. The FS has been previously used to assess positive mental health within SGM college students (Parchem et al., 2024) but has not been used with college student autistic populations.
UCLA Loneliness Scale (ULS)
The ULS measures an individual’s subjective feelings of social isolation and loneliness (Russell et al., 1978). For this study, the short form consisting of three items from the ULS was used given its strong correlation (r = .81) with the longer ULS and strong convergent and divergent validity (Hughes et al., 2004). Participants reported the frequency of the experience (e.g., “How often do you feel left out?”) using a 3-point Likert-type scale (1 = Hardly Ever; 2 = Some of the Time; 3 = Often). Total ULS scores ranged from 3 to 9 with higher scores indicating greater perceived loneliness. Cronbach’s alpha for the current sample was .83, indicating good internal consistency. Both longer and short forms of the ULS have been used to assess loneliness in adult autistic populations (Ee et al., 2019; Jobe & White, 2007) and adult SGM populations (Busby et al., 2020).
Global Distress (Kessler-6)
The Kessler-6 is a six-item global distress measure based on symptoms of anxiety and depression over the past month (Kessler et al., 2003). Participants reported the past-month frequency of the experience (e.g., “How often have you felt nervous?”) using a 5-point Likert-type scale (0 = None of the Time to 4 = All of the Time). Total Kessler-6 scores ranged from 0 to 24 with higher scores reflecting greater perceived past-month distress. Cronbach’s alpha for the current sample was .88, indicating good internal consistency. The Kessler-6 has been used to assess psychological distress in autistic adults (Vogan et al., 2017) and adult SGM populations (Gonzales et al., 2016; Wilson & Liss, 2022).
Suicide Behavior Questionnaire-Revised (SBQ-R)
The SBQ-R is a five-item measure surveying suicidality (Osman et al., 2001). Participants reported the lifetime frequency of suicidal ideation and suicide attempts (e.g., “How often have you thought about killing yourself in the past year?”) using 5- and 7-point Likert-type scales. Total SBQ-R scores were used for this study with higher scores indicating higher endorsement of past suicidal behaviors and higher risk of suicide. Consistent with prior literature (Osman et al., 2001), total scores were dichotomized to indicate > 7 as positive suicidality. Cronbach’s alpha for the current sample was .80, indicating good internal consistency. The SBQ-R has been used to assess suicidal behaviors in autistic adult populations (Cassidy et al., 2021; Hedley et al., 2021) and SGM populations (Chu et al., 2019).
Non-Suicidal Self Injury (NSSI)
Past year engagement with NSSI behaviors was assessed for using the following question: “Within the last 12 months, how often have you intentionally cut, burned, bruised, or otherwise injured yourself?” Participants responded on a 5-point Likert-type scale (1 = Never to 5 = Daily or Almost Daily).
Past year suicide attempts
Past year history of suicide attempts was assessed using the following question: “Within the last 12 months, have you attempted suicide?” Participants responded either “Yes” or “No.”
Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST)
The ASSIST (WHO ASSIST Working Group, 2002) is an eight-item measure that assesses for various substances and substance use over the lifetime and last 3 months, frequency of use, and consequences of use (e.g., “During the past 3 months, how often has your use of the following substance(s) led to health, social, legal or financial problems?”). Notably, and in line with the “skip-out” survey structure of the ACHA-NCHA III survey, participants were only administered the ASSIST measure for substances they had endorsed using. Substances assessed included alcohol, tobacco, cocaine, cannabis, prescription stimulants, methamphetamine, inhalants, sedatives, hallucinogens, heroin, opioids, and “other.” Prescription stimulant-use scores were adjusted for students with prescriptions so that participants with prescriptions only reported when they took their stimulants “just for the feeling or experience they caused or taking them more often or at higher doses than prescribed.” Adhering to ASSIST guidelines (WHO ASSIST Working Group, 2002), risk levels were categorized for each substance as (1 = Low Risk; 2 = Moderate Risk; 3 = High Risk). Each of the 12 substance groups was considered individually for analysis. The ASSIST has been used to assess self-reported substance usage in autistic adult populations (Kunreuther, 2021) but has not been used with college SGM student populations.
Mental health treatment status
Mental health treatment status over the past year was assessed from participants that had indicated they had spoken with a healthcare or mental health care professional within the last year about any of 13 mental health conditions (i.e., ADHD, substance-related abuse or addiction, gambling disorders, anxiety disorders, autism spectrum, bipolar disorders, personality disorders, depressive disorders, eating disorders, insomnia, obsessive-compulsive disorders, trauma disorders, and psychotic disorders; Supplemental Table 4). For each condition endorsed by the participant, participants were asked to denote the types of treatment received as “No treatment,” “Medicine only,” “Therapy only,” “Both medicine and therapy,” and “Other treatment.” The Mental Health Treatment Status variable was derived by collapsing responses across all endorsed mental health conditions for each participant and recategorized into “No treatment,” “Medicine only,” “Therapy only,” “Both medicine and therapy,” and “Only other treatment.” The Mental Health Treatment Status variable was only included in analyses for Hypothesis 3.
Data analysis overview
This study examines self-declared frequency rates, associated mental health correlates, functional impairments, and treatment engagement levels for SM and non-SM college-student populations with and without autism. To test Hypothesis 1, we examined the self-declared frequency rates of autism between SM identity (SM-only and non-SM) using chi-square tests. To test Hypothesis 2, we investigated associated functional outcomes and mental health correlates between our groups (i.e., Autism-only, SM + autism, SM + GM + Autism, SM-only, SM + GM, and Comparison) using multivariate analyses of covariance (MANCOVA) for continuous variables while covarying for age. Significant findings were followed up with analyses of covariance (ANCOVA) with Bonferroni post hoc analysis performed for significant models. Effect size estimates for comparisons are reported as partial eta square (ηp2) for continuous variables. Effect sizes were considered to be small at approximately ηp2 = .01, medium at approximately ηp2 = .06, and large at approximately ηp2 = .14. To test Hypothesis 3, we examined mental health treatment engagement levels for students within each group by using chi-square tests.
Analyses were conducted using SPSS version 23. Participants missing > 25% of data were excluded from analyses. Little’s MCAR (missing completely at random) test concluded that missing data were random. Missing cases were addressed using pairwise deletion across all analyses. Given the large sample size of this study and its associated power, an alpha level of .001 was chosen for demonstrating statistical significance to reduce the risk of a Type I error. Effect size will be reported for all analyses so that the reader can review the magnitude of the differences.
Results
Hypothesis 1: self-declared frequency rates of autism among SM groups
In the total sample, the self-reported lifetime frequency rate of autism was 1.3%. Self-reported autism frequency rates were significantly higher in the SM group (2.8%) compared with the non-SM group (0.9%), χ2(1) = 376, p < .001, Φ = 0.07. Rates of college students identifying with an SM identity were also significantly higher in the autism group (45.8%) as compared with the comparison group (21.0%), χ2(1) = 376, p < .001, Φ = 0.07. These results support Hypothesis 1; there is a higher self-declared frequency rate of autism among SM college students compared with non-SM college students.
Hypothesis 2: associated functional impairments and mental health correlates
Past year stress and distress
Differences in general past-year stress levels were found among the six groups, F(3, 81,135) = 322.0, p < .001, ηp2 = .02. As demonstrated in Table 2, pairwise comparisons indicated that all the SM (SM + GM + Autism, SM + Autism, SM + GM, and SM) groups similarly reported the highest levels of general stress over the past year, followed by the Autism group, while the Comparison group reported the lowest.
Mean levels of general stress and specific domain distress.
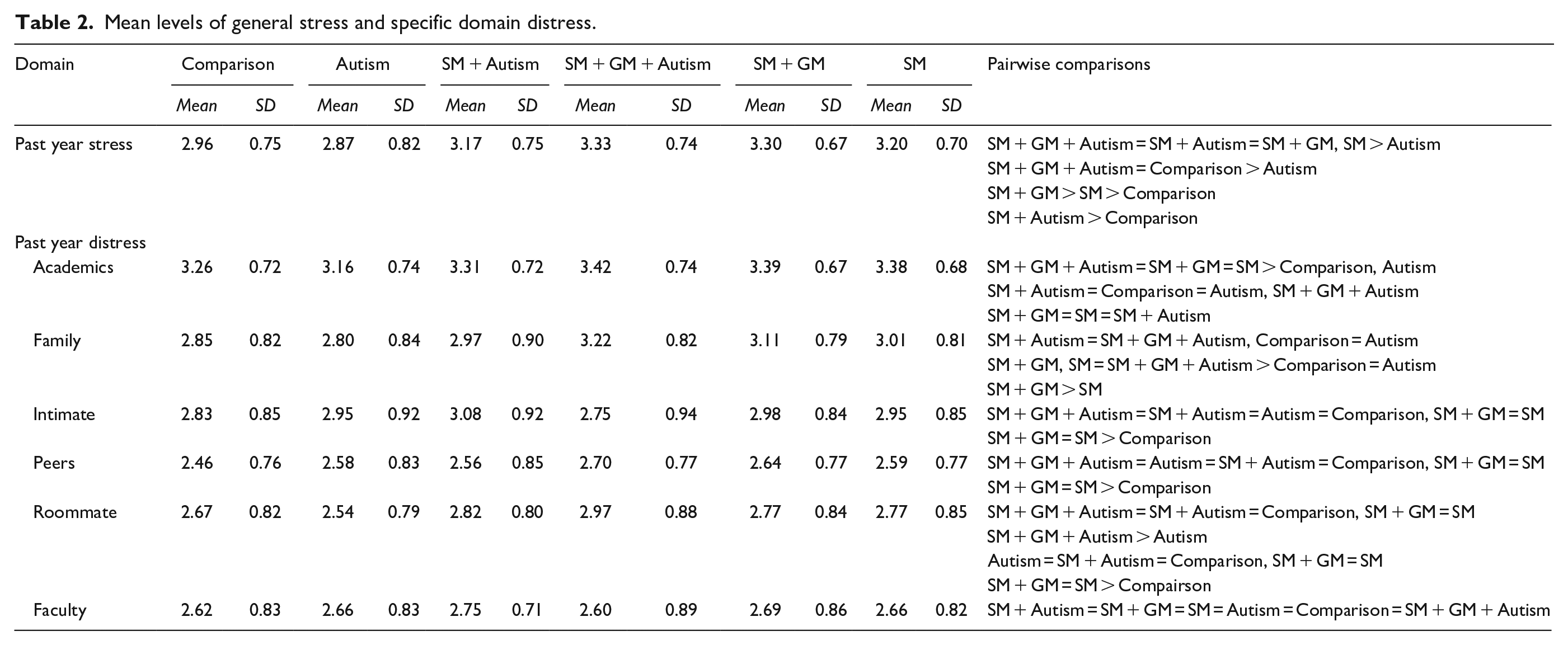
With regard to domain-specific past-year distress, the omnibus MANCOVA was statistically significant, Wilk’s λ = 0.94, F(30, 6,186) = 3.2, p < .001, ηp2 = .010. Follow-up analyses indicated past-year distress differences among the six groups for the following domains: academics F(5, 37,875) = 43.1, p < .001, ηp2 = .006, family relationships F(5, 27,399) = 58.1, p < .001, ηp2 = .01, intimate relationships, F(5, 30,448) = 25.1, p < .001, ηp2 = .004, peer relationships, F(5, 20,168) = 26.4, p < .001, ηp2 = .006, and roommate relationships domains, F(5, 22,780) = 14.8, p < .001, ηp2 = .003. In general, pairwise comparisons indicated that the SM + GM + Autism and SM + Autism groups reported the highest levels of domain-specific distress, while the Comparison group reported the lowest levels of distress across most domains, except the academic domain. The Autism-only and SM-only groups were comparable with the SM + GM + Autism and SM + Autism groups on academic, intimate, and peer relationship domains and lower on the family domain. No between-group differences emerged for faculty relationships.
Academic performance and impacts
Differences in academic performance using self-reported GPA were found among the six groups, F(5, 79,159) = 31.2, p < .001, ηp2 = .002. Pairwise comparisons indicated that both the SM + GM + Autism and Autism-only groups reported lower GPAs, followed by the SM + GM and then SM-only groups. The Comparison group reported the highest GPA (Table 1).
Regarding academic impairment related to mental health factors, the omnibus MANCOVA was significant, Wilk’s λ = 0.90, F(20, 265,702) = 422.8, p < .001, ηp2 = .020. Differences in the extent that mental health factors negatively impacted academic performance were found among the six groups: depression, F(5, 80,986) = 1427.0, p < .001, ηp2 = .080, anxiety, F(5, 80,662) = 873.0, p < .001, ηp2 = .051, PTSD, F(5, 80,917) = 520.0, p < .001, ηp2 = .031, and stress, F(5, 80,897) = 551, p < .001, ηp2 = .033. As seen in Table 3, across nearly all mental health domains, the SM + GM + Autism, SM + Autism, and SM + GM groups reported the most significant negative academic impacts, followed by the SM-only group, then the Autism-only group, and the Comparison group reporting the least academic impacts from mental health conditions.
Academic impairment caused by mental health and interpersonal factors.
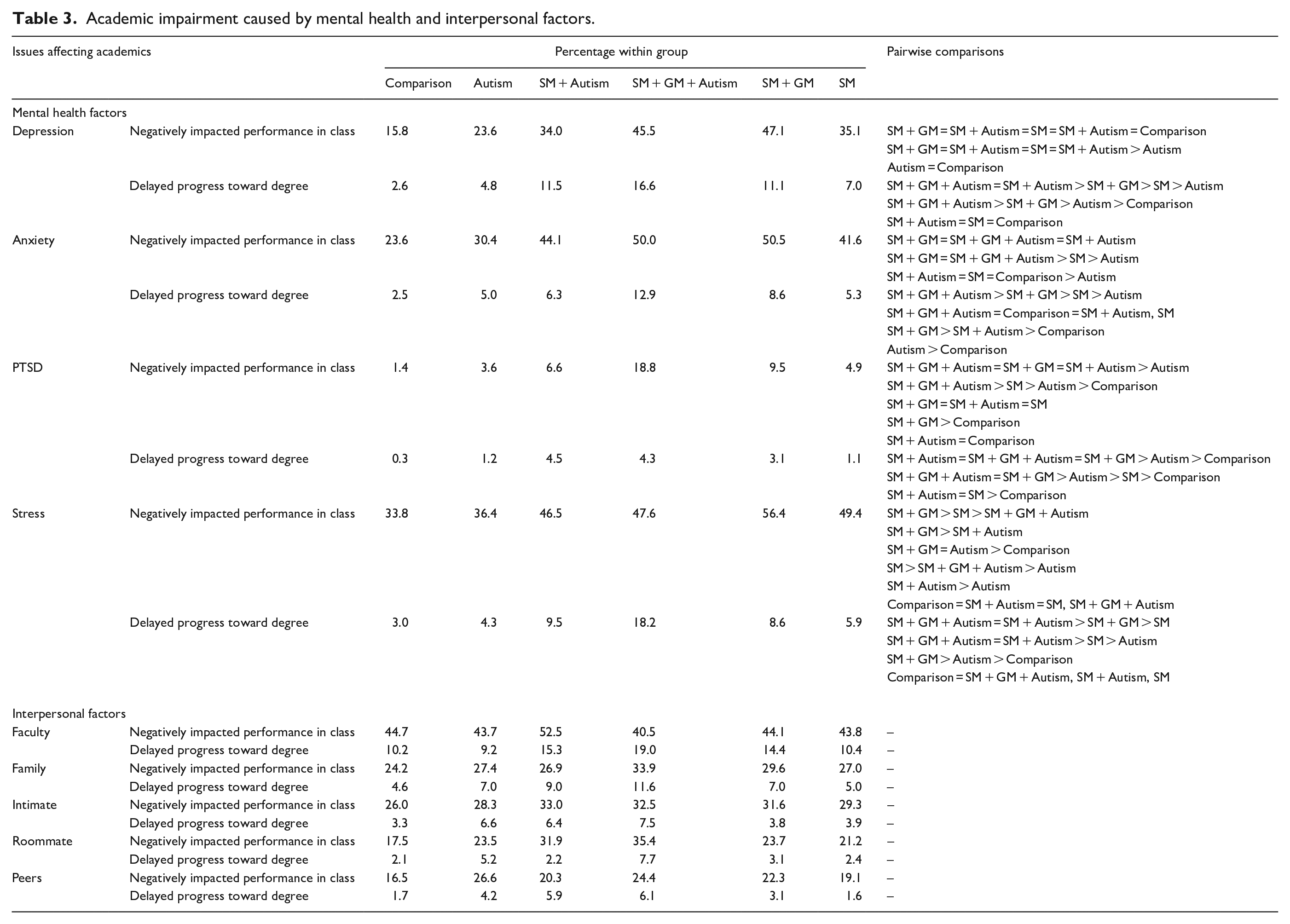
In terms of academic impairment related to interpersonal factors, the omnibus MANCOVA for interpersonal problems within the last 12 months was not significant, Wilk’s λ = 0.98, F(25, 6346.4) = 1.4, p = .08, ηp2 = .004.
Mental health correlates
The omnibus MANCOVA that included the mental health correlate measures related to flourishing, resilience, loneliness, internalizing symptoms, NSSI, and suicide risk was significant, Wilk’s λ = 0.87, F(35, 318,309) = 294.8, p < .001, ηp2 = .030. Follow-up analyses for each of these measures are presented in Table 4. For flourishing, differences in the FS were found among the six groups, F(5, 80,738) = 774, p < .001, ηp2 = .046. The SM + GM + Autism group reported the lowest levels of flourishing, followed by SM + Autism and SM + GM groups reporting similar levels, then the SM-only and Autism-only groups reporting similar levels, and the Comparison group reported the highest levels of flourishing. For resilience, differences in the CD-RISC-2 were found among the six groups, F(5, 80,926) = 244, p < .001, ηp2 = .015. In general, the SM + GM + Autism group reported the lowest level of resilience, followed by the Autism-only, SM + Autism, and SM + GM groups, and finally the Comparison group reported the highest level of resilience. For loneliness, differences in the ULS were found among the six groups, F (5, 81,019) = 539.0, p < .001, ηp2 = .033. The SM + GM + Autism, SM + Autism, and SM + GM groups reported the highest level of loneliness, followed by both the Autism-only and SM-only groups reporting similar levels of loneliness, and finally the Comparison group reporting the lowest level of loneliness. Next, for psychological distress as measured by the Kessler-6 Scale, differences were found among the six groups, F(5, 80,395) = 1067.0, p < .001, ηp2 = .063. The SM + GM + Autism group reported the highest level of psychological distress, followed by the SM + GM and SM + Autism groups reporting similar levels, then the SM-only group, and then the Autism-only group. Finally, the Comparison group reported the lowest level of psychological distress.
Mental health means.
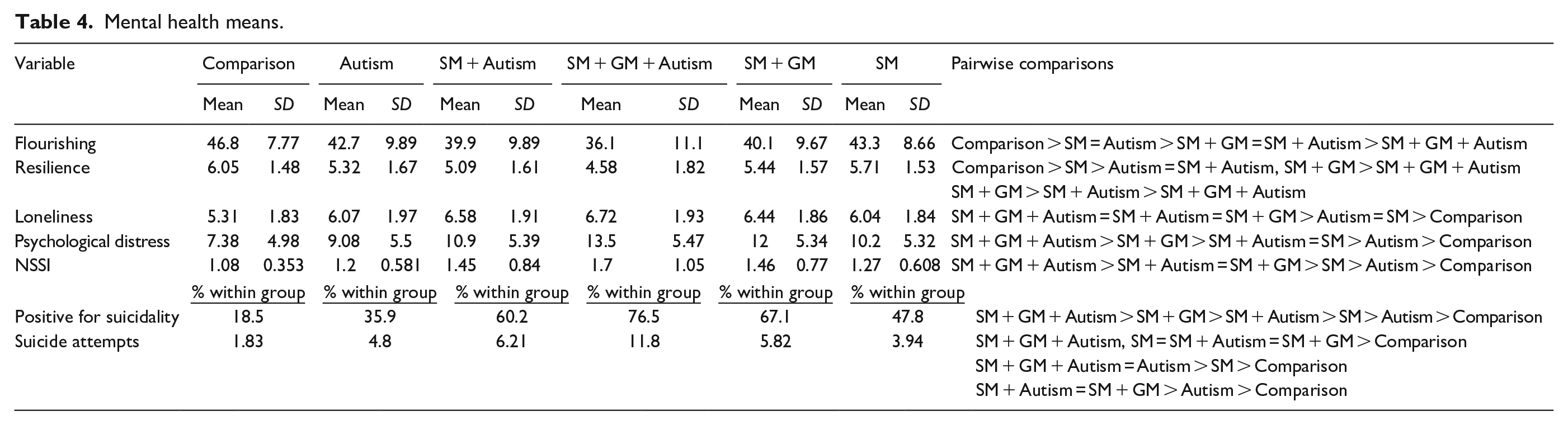
For suicidality, differences with screening positive for suicidal risk on the SBQ-R screening were found among the six groups, χ2(5) = 7,779, p < .001, Φ = 0.31. The SM + GM + Autism group reported the highest risk, followed by SM + GM, SM + Autism, SM-only, Autism-only, and then the Comparison group reported the lowest risk. For NSSI, differences in the frequency of engagement in NSSI were found among the six groups, F(5, 77,965) = 747.0, p < .001, ηp2 = .046. The SM + GM + Autism group reported the highest frequency of NSSI engagement, followed by the SM + GM and SM + Autism groups reporting similar levels, then the SM-only group, and then the Autism-only group. Finally, the Comparison group reported the lowest frequency of NSSI engagement. For suicide attempts, differences in suicide attempts over the past year were found among the six groups, χ2(5) = 445.0, p < .001, Φ = 0.074. More specifically, the SM + GM + Autism (11.8%), SM + Autism (6.2%), and SM + GM (5.8%) groups had the highest endorsement of attempting suicide over the past year, followed by the Autism-only group (4.8%), the SM-only group (3.9%), and finally the Comparison group (1.8%).
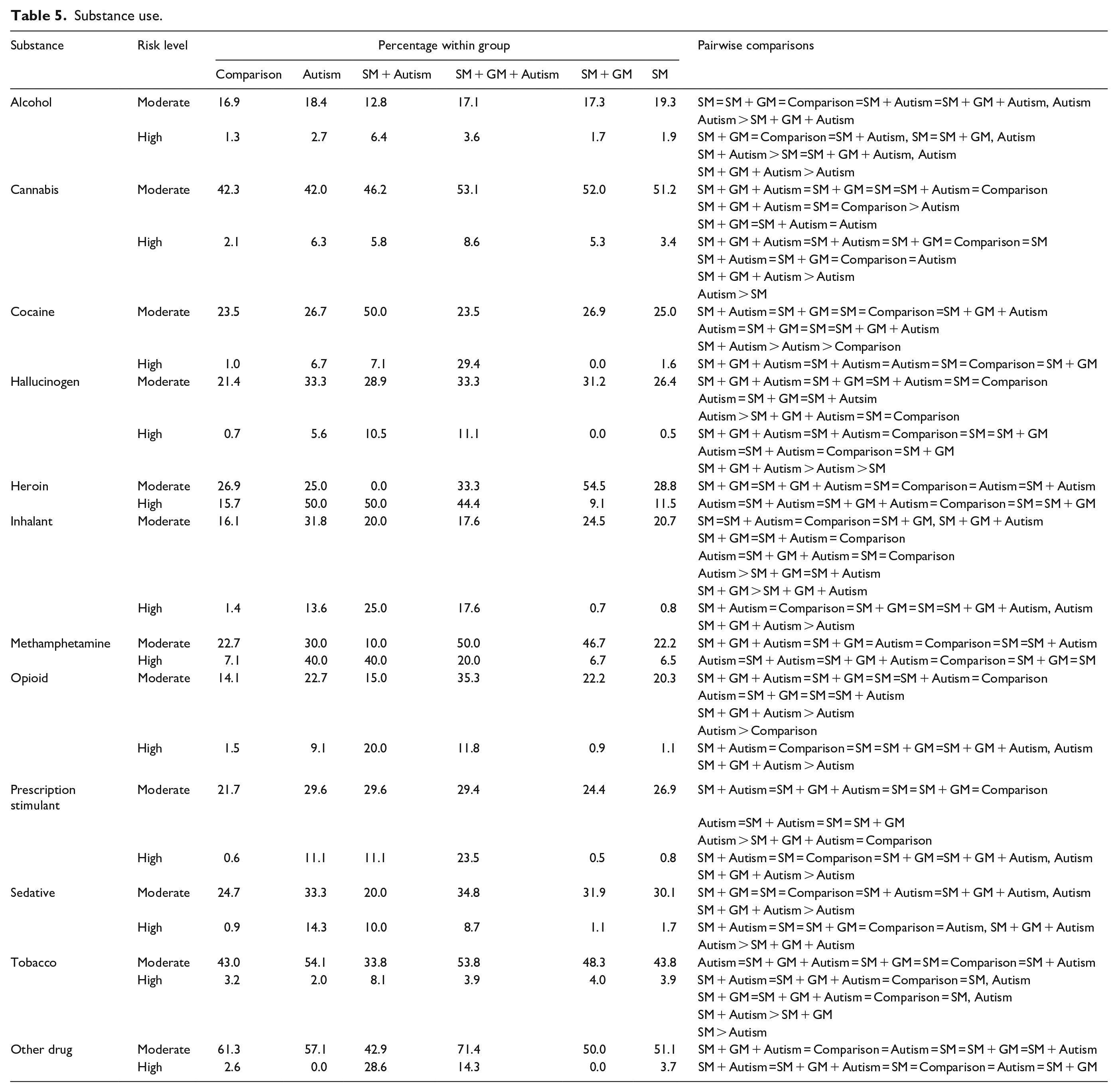
Regarding high-risk substance use, differences in various individual substance use categories were found among the six groups in nearly all substance categories (ps < .001). As seen in Table 5, across nearly all substances, the SM groups (i.e., SM + GM + Autism, SM + Autism, SM-GM, and SM-only) had a greater risk for high-risk substance use as compared with the Autism-only and Comparison groups, with the SM + GM + Autism groups typically showing the greatest high-risk. No between-group differences emerged for cannabis, methamphetamine, or “other” drugs.
Substance use.
These results support our hypothesis that autistic SGM individuals would report the highest rates of academic, social, and mental health impairments.
Hypothesis 3: mental health treatment engagement
Differences in the percentage of students receiving mental health treatment were found among the six groups, χ2(20) = 403.7, p < .001, V = .07. Pairwise comparisons for level of engagement for all mental health treatments are shown in Table 6. The Comparison reported the highest level of engagement in medicine-only treatments (27.2%), followed by the Autism-only (24.6%) and SM + Autism (21.4%) groups reporting similar levels, then the SM-only (18.6%), SM + GM (18.6%), and the SM + GM + Autism (11.9%) group reporting the lowest level of medicine-only treatment engagement. The comparison, SM-only, and SM + GM groups similarly reported the highest level of therapy-only treatment engagement (23.7%, 24.5%, and 24.8%, respectively), followed by the Autism-only group, while the SM + Autism and SM + GM + Autism group reported the lowest use of therapy treatment. For treatment with both medicine and therapy, the SM + GM + Autism, SM + Autism, and SM + GM groups similarly had the highest treatment engagement (50.8%–62.9%), followed by SM-only (49.0%), then Autism-only (44.4%), while the Comparison group (39.0%) shows the lowest treatment engagement. Finally, all six groups reported similar rates for both not engaging in any treatment (3.5%–9.1%) or engaging in another (“other,” 1.8%–4.3%) form of treatment for their mental health conditions.
Mental health treatment.
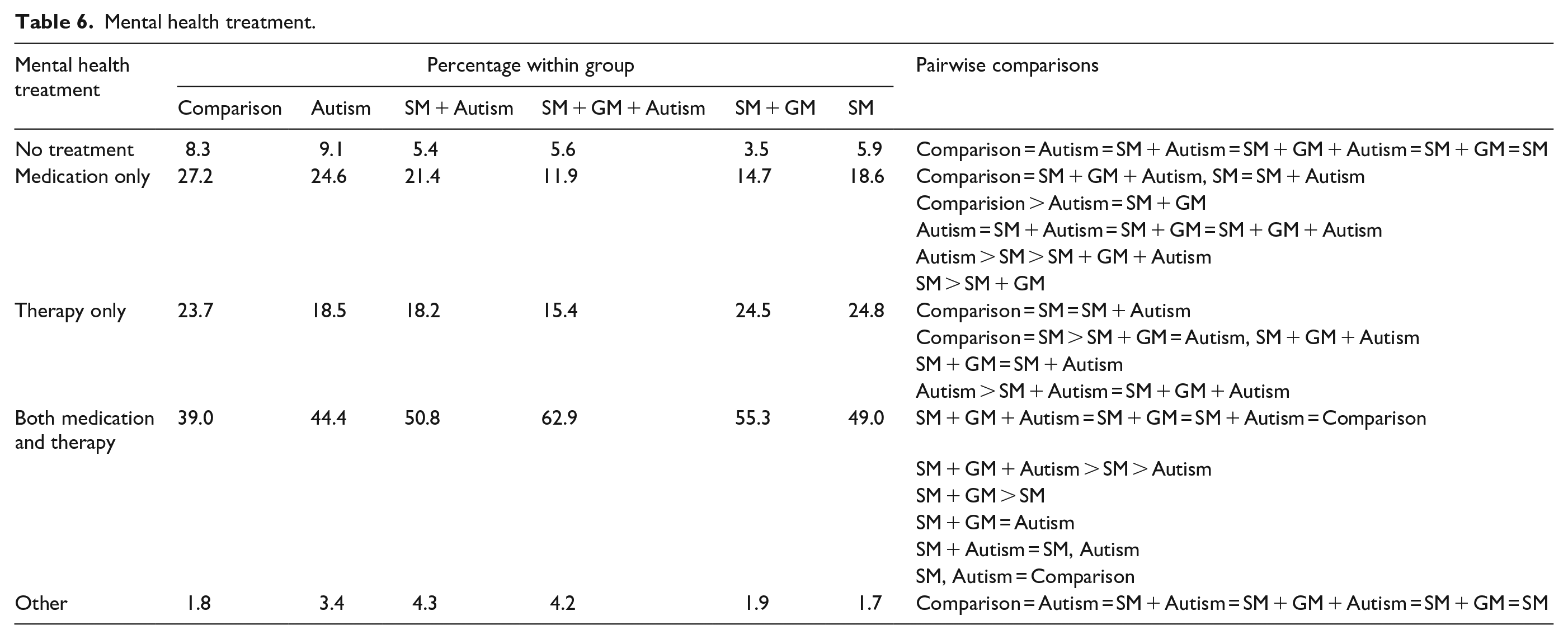
Taken together, these results partially support our hypothesis that SGM autistic individuals would have the lowest reported rates of mental health treatment. SGM autistic individuals engage in combined treatment as often as other groups yet participate in medicine-only and therapy-only at lower rates.
Discussion
This study was the first to examine the self-declared frequency rates, functional and mental health outcomes, and treatment engagement levels for autistic and non-autistic college students with non-SM, SM, and SM + GM identities via a large nationally representative college-student sample. A considerable strength of this study is that results are derived from the ACHA-NCHA-III from 2019 to 2022 and included randomly sampled students from 75 U.S. colleges and universities. Results of this study reflect a self-declared frequency rate of autism as 1.3% and are consistent with extant literature (Baio et al., 2018; Christensen et al., 2018; Maenner et al., 2020). This study builds off existing literature by testing and finding support for the hypothesis that the frequency rates of self-reported autism among SM students would be higher than among non-SM college students (2.8% vs 0.9%).
In general, and in line with our second hypothesis, autistic college students with both SM and GM identities reported the highest rates of academic and functional impairments and mental health concerns across all groups. Furthermore, college students belonging to more than one minority group (i.e., autistic college students with SM identities, non-autistic college students with both SM and GM identities) generally had the next highest rates of academic, functional impairments, and mental health concerns, followed by those belonging to only one (i.e., autistic college students without an SM identity, non-autistic college students with SM identities) or no minority group identity (i.e., non-autistic college students without an SM identity). This pattern of results aligns closely with both the minority stress and intersectional stigma predictions postulating that the presence of two or more intersecting minority identities may create and/or exacerbate mental health problems driven by compounding stressors faced by autistic individuals belonging to other minority groups (Maroney & Horne, 2022; Meyer, 2003). More specific to academic outcomes and expanding on previous literature showing that autistic college students and SGM college students each experience academic difficulties (Kapp et al., 2013; Oswalt & Wyatt, 2011), autistic college students with both SM and GM identities reported the lowest academic performance and the highest academic impairment when related to mental health factors compared across all six groups. Small effects were observed for the majority of these relations, except for the medium effect for academic impairment related to depression. In contrast, academic impairment when related to interpersonal factors did not differ across all six groups, suggesting that all groups experience similar levels of academic impairment attributed to interpersonal conflicts.
Regarding mental health, autistic adults with both SM and GM identities reported the highest levels of depression, loneliness, and psychological distress and the lowest levels of flourishing and resilience across all six groups. Notably, medium-sized effects were observed between group membership and flourishing and psychological distress. These results begin to bridge together previous independent autism and SGM literature showing that both groups are at elevated risk for feelings of depression, loneliness, and psychological distress (Suzuki et al., 2021; Wilson & Liss, 2022). Having both minoritized identities seems to increase these mental health concerns.
Perhaps some of the most striking findings from this study were the medium-sized relations between group membership and NSSI (ηp2 = .046) and suicide risk (Φ = 0.31). Importantly, all autism and SM groups showed a higher rate of suicide attempts compared with non-autistic college students without an SM identity, with autistic college students with both SM and GM identities showing nearly six times more suicide attempts than the non-autistic college students without SM identities. Furthermore, autistic college students with and without SM identities reported higher rates of NSSI than non-autistic college students without SM identities. This relation between autism and NSSI is of clinical importance given that it is in line with prior work among autistic adult samples (Maddox et al., 2017) but had not been previously documented in college samples. Furthermore, we continue to expand on these findings by showing that autistic college students with both SM and GM identities reported higher rates of NSSI, followed by college students with at least two group memberships (i.e., autistic college students with SM identities and non-autistic college students with both SM and GM identities), compared with non-autistic college students. These results emphasize the need for autistic college students, non-autistic college students with SGM identities, and especially autistic college students with SGM identities, to have access to and receive support/resources to mitigate suicide risk.
Regarding treatment engagement, autistic college students are less likely to seek out mental health treatments compared with non-autistic college students (Chandrasekhar, 2020), while SGM college students are more likely to seek mental health treatments but are more likely to discontinue treatments prematurely (Dunbar et al., 2017). Given compounding evidence highlighting stigma and barriers to receiving care faced by both autistic college students and SGM college students separately, we hypothesized that autistic college students with both SM and GM identities would report the lowest mental health treatment engagement rates compared with non-autistic college students without SM identities and autistic individuals with SM identities. Interestingly, and only partially supporting our hypothesis, results reflect that autistic college students with both SM and GM identities engage in combined mental health treatment as often as other groups but participate at lower rates in medicine-only and therapy-only treatments. At the same time, the comparison group reported the highest treatment engagement in medicine-only, followed by both autistic college students with and without an SM identity. For therapy-only, the non-autistic college students with SM identities reported the highest treatment engagement, followed by non-autistic college students with both SM and GM identities. One possible explanation for this pattern of results is that a combined treatment approach may be better suited to address exacerbated mental health problems associated with belonging to multiple minority groups, such as having a diagnosis of autism and both an SM and GM identity.
Limitations/future directions
This study has several strengths, including a large nationally randomly selected sample of college students across multiple colleges and universities. However, the following limitations should be considered when interpreting results. Data collection was ongoing before, during, and after the COVID-19 pandemic, which may have had both direct and indirect impact on these findings. Recent work suggests that culminating factors of virtual education, strained interpersonal relationships, and decreased social engagement during COVID-19 increased mental health problems in college students (Lee et al., 2021). Future studies continuing to monitor these trends are needed to determine how COVID-19 may or may not be continuing to impact these relations. Another limitation of this study is that autism diagnostic status was based on one self-reported question for autism rather than best evidence-based assessment practices which include the use of multi-informant and multi-method approaches. One recent study suggests that a diagnosis of autism spectrum disorder may be overestimated within GM populations when assessed for via self-report only (Kallitsounaki & Williams, 2022). At the same time, it is also possible that individuals who both self-identify as autistic and experience similar difficulties as autistic people with a formal diagnosis of autism may not have endorsed having an autism spectrum disorder due to challenges with receiving a formal diagnosis. Often, women, individuals belonging to racial/ethnic minority groups, and individuals identifying as belonging to an SGM group experience the most difficulties with obtaining a formal diagnosis of autism (Driver & Chester, 2021; Tromans et al., 2021). Taken together, clinic-based studies or studies using clinically derived diagnostic groups may provide more accurate prevalence rates for SGM identities in autistic individuals.
Another limitation of this study was our inability to include GM-only and GM + Autism groups, which reduces the generalizability of these findings to specific sexual orientation and/or gender identity minority groups. In addition, this study used only one question asking participants’ gender identity, and items about biological sex were not considered, which means this study may have missed individuals identifying as transgender and/or individuals who were in the process of transitioning in our groupings. Recent studies have shown that adults who identify as transgender are more likely to report a mental health diagnosis and/or a diagnosis of autism comparative to their cis-gender adult peers (Kallitsounaki & Williams, 2022; Warrier et al., 2020).
While this study is an important first step toward understanding the relations among autism, SM and GM identities, and functional statuses; future work using comprehensive, evidence-based assessments of autism and examining SGMs separately is necessary to continue to fill in these notable gaps in the literature. A qualitative study design may permit a deeper consideration of the mental health and functional challenges faced by autistic college students who have SM and/or GM identities. This study examined mental health treatment engagement of non-SM, SM-only, and SM and GM identities in autistic and non-autistic college students; however, more work is needed to determine the efficacy of treatment across these groups and GM groups. Another potential limitation is the method invariance with all data being reported by one person (i.e. college student). Finally, while all the results presented in this study are statistically significant at the .001 level, most of the effect sizes are uniformly small and warrant consideration when interpreting the strength of these findings.
Clinical implications
Taken together, the results that autistic and non-autistic college students with and without SM identities (including SM-only and SM + GM identities) experience unique functional differences and treatment engagement levels provide important implications for both assessment and intervention. Coupled with emerging work showing that sex- and gender-related factors may impact behavioral variabilities in neurodevelopmental disorders (Bölte et al., 2023), the results of this study emphasize the need for mental health providers to inquire about both SM and GM identities when working with autistic college students. Similarly, mental health providers are encouraged to conduct comprehensive assessments that include evaluations of general stress, academic functioning, and mental health factors, especially suicide risk, when working with autistic college students with any SM and GM identities, as well as non-autistic college students with SM and GM identities.
Regarding intervention efforts, the findings of this study demonstrate that each of these groups has difficulties across many domains but experiences them differently, suggesting that supports/resources may be needed at multiple levels (e.g., academic and mental health). Furthermore, given the differences across these groups, it is possible some supports/resources would be more efficacious for some groups and not others. As such, additional research is necessary to examine how these supports may or may not be efficacious across groups. For example, one recent study by McAuliffe and colleagues (2023) shows that SGM autistic individuals identified wanting to be more included within SGM communities in both physical and virtual spaces, wanting to see more SGM autistic role models, and wanting to be more involved in social justice. As such, higher educational settings may be better equipped to support SGM autistic students by creating safe spaces and specific SGM and autism events that focus on themes of suicide risk awareness and social change. In addition, it is imperative that mental healthcare providers are trained to recognize and work with these intersecting identities in supportive ways to increase treatment engagement.
Supplemental Material
sj-docx-1-aut-10.1177_13623613241236228 – Supplemental material for Autism and sexual and gender minority identity in college students: Examination of self-reported rates, functional outcomes, and treatment engagement
Supplemental material, sj-docx-1-aut-10.1177_13623613241236228 for Autism and sexual and gender minority identity in college students: Examination of self-reported rates, functional outcomes, and treatment engagement by Elia F Soto, Destiny Orantes, Natalie Russo and Kevin M Antshel in Autism
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclaimer
The opinions, findings, and conclusions presented/reported in this article/presentation are those of the author(s) and are in no way meant to represent the corporate opinions, views, or policies of the American College Health Association (ACHA). ACHA does not warrant nor assume any liability or responsibility for the accuracy, completeness, or usefulness of any information presented in this article/presentation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.