
Abstract
Despite an estimated population of 10 million autistic individuals, there is still a significant lack of research on autistic adults in China. This study aimed to investigate the extent and factors influencing community integration (employment, independent living and friendship) and life satisfaction among young autistic adults in China, and compare them with an autistic adult sample with similar characteristics (58%–63% with a reported IQ below 70) from the Netherlands. Data were collected via online surveys to the caregivers of 99 young autistic adults (18–30 years) in China and 109 in the Netherlands, because the autistic adults were not able to fill in the survey independently. Autistic adults in both countries were reported to have limited community integration, as indicated by low rates of employment, limited independent living and few close friendships. Proxy-reported life satisfaction of autistic adults seemed relatively low in both countries, but even lower in Chinese adults, possibly due to limited awareness and acceptance of autism in China, inadequate or inaccessible support services, higher parenting stress, or general cross-country differences in well-being. In general, the findings indicate a common challenge faced by autistic adults with high support needs in both China and the Netherlands.
Lay abstract
Even though there are about 10 million Chinese autistic individuals, we know little about autistic adults in China. This study examined how well young autistic adults in China integrate into their communities (such as having a job, living independently and having friends) and how satisfied they are with their lives as reported by their caregivers. We compared them to autistic adults with similar characteristics (such as high support needs) from the Netherlands. We included 99 autistic adults in China and 109 in the Netherlands (18–30 years). In both countries, autistic adults were reported to have a hard time fitting into their communities. They often had no work, did not live on their own and had few close friends. Also, in both countries, caregivers reported that autistic adults felt low satisfaction with their life. Chinese adults were less satisfied with their life than Dutch adults, as indicated by their caregivers. This could be because of a lack of support for autistic adults in China, higher parental stress in Chinese caregivers, or general cross-country differences in happiness. Only in the Dutch group, younger compared with older adults fitted better into their communities, and adults without additional psychiatric conditions were reported to have higher life satisfaction. Country was a significant predictor of independent living only, with Dutch participants more likely living in care facilities than Chinese participants. In conclusion, our study shows that autistic adults with high support needs generally face similar challenges in both China and the Netherlands.
Keywords
Introduction
While there is a growing focus of autism research on adults (Howlin, 2021), it is striking how little is known about one of the largest populations of autistic adults: the estimated 10 million individuals living with autism in China (Zhou et al., 2020). Studies on autistic adults are mostly based in Western high-income countries like the U.S. and European countries (Sáez-Suanes & Álvarez-Couto, 2022; Scheeren et al., 2022) generally showing reduced community integration (Mason et al., 2021) and lower life satisfaction (Lord et al., 2020) compared with non-autistic adults. A fundamental question regarding autistic adults in Mainland China is the integration within their communities (employment, independent living and having friends) and their life satisfaction, as well as potential distinctions between Chinese and Western European autistic adults.
Previous research on autism in China indicated limitations in the health, social care and educational services for individuals with autism throughout the country, despite increased attention for more inclusive education (Fisher et al., 2010; Xiao, 2023). Relatively many families with an autistic member experience financial burden and psychological stress (Baker et al., 2020; Clark et al., 2019; Huang et al., 2013; Sun et al., 2013). Studies from China and Japan also suggest that autistic adults experience a lower quality of life (physical health, psychological health and environment) compared with neuro-typical adults (Kamio et al., 2013; Lin, 2014; Lin & Huang, 2019). The available information on living situations of autistic adults in Mainland China is mainly derived from parent reports surveys in locally published books and research. Furthermore, a limited number of parent report studies have indicated that the employment rate among a group of autistic adults in China was below 10%, and 95% of them lived with their parents (Hua, 2017; Jia, 2022). Most of these adults have what is called ‘high support needs’(Lord et al., 2022), including a constant need for an adult caregiver for assistance, being unable to be left alone, and an inability to independently manage basic daily tasks. Many autistic adults in China have difficulty in communicating their needs and preferences effectively (Zhou et al., 2023). Chinese parents play a central role in the lives of their autistic children (Lei & Kantor, 2021) even after they become adults. In groups with communication difficulties proxy-reports can be employed as an alternative source of information on an individual’s quality of life (Clark et al., 2014; Egilson et al., 2017).
Community integration generally involves three primary areas: employment or other productive activity, independent living and social engagement (Sander et al., 2010; Scheeren & Geurts, 2015). Many autistic adults face challenges in these domains (Mason et al., 2021; Wickstrom et al., 2021). Cultural and contextual backgrounds may affect community integration of autistic adults across the globe. Western individualistic countries, such as the Netherlands, have a longer history of autism awareness as well as active self-advocacy movements for autistic individuals (Waltz et al., 2015), promoting their empowerment and potentially creating an environment more accepting of neurodiversity (Szlamka et al., 2022). The majority of more recently diagnosed adults with autism in Western countries have average to high intellectual abilities (Brugha et al., 2016; Christensen & Zubler, 2020) and an increasing number of people are diagnosed in adulthood (Begeer et al., 2013; Lai & Baron-Cohen, 2015). In Mainland China, autism is generally considered a disorder rather than a form of neurodiversity. Autistic behaviours may be perceived more strongly as non-conforming in Chinese society (Mak & Kwok, 2010; Zhou et al., 2020). Individuals with high intellectual ability and fewer autism traits are less likely to be recognized as autistic or formally diagnosed (Huang et al., 2013). The majority of individuals with formal autism diagnoses tend to have moderate to severe intellectual disabilities (ID), have limited functional communication and/or are unable to advocate for themselves (Huang et al., 2013), similar to how it was in Western countries about 30 years ago. Chinese families with an autistic member may face a high degree of stigma and discrimination (Chan & Lam, 2018; Mak & Kwok, 2010). Therefore, some Chinese parents may choose to conceal the autism condition of the autistic family member (Luo et al., 2022; Su et al., 2019), contributing to a heavy dependence of Chinese adults with autism on their families (Baker et al., 2020).
Differences in availability, accessibility, affordability and acceptability of autism support services across countries can also serve as contextual facilitators or barriers for community integration (Chiang & Wineman, 2014; de Leeuw et al., 2020). Table 1 shows the comparative healthcare system as well as the basic socioeconomic status of China and the Netherlands. For example, per capita healthcare expenditure in the Netherlands is tenfold that of China. These differences may indicate a more robust mental health care infrastructure and support system in the Netherlands, which may potentially lead to greater community inclusion and more opportunities to live an independent life for autistic individuals. In China, despite policies and guidelines promoting the inclusion of autistic individuals in schools (Fisher et al., 2010; Xiao, 2023), challenges persist, such as financial problems in families with autism, services inequality between urban and rural areas and lack of healthcare and educational professionals (Clark et al., 2019; Li & Qi, 2023; Sun et al., 2013). Some Dutch young autistic adults with high support needs live with their parents but a larger proportion lives in residential care facilities (Barneveld et al., 2014; Scheeren et al., 2021) compared with Chinese adults. In China, especially in urban cities where the cost of living and purchasing a house is high, autistic adults remain living with their parents, as care facilities are scarce and government support for residential care is only provided when there are no family members available (Fisher & Jing, 2008).
Comparative information on the background status of China and the Netherlands.
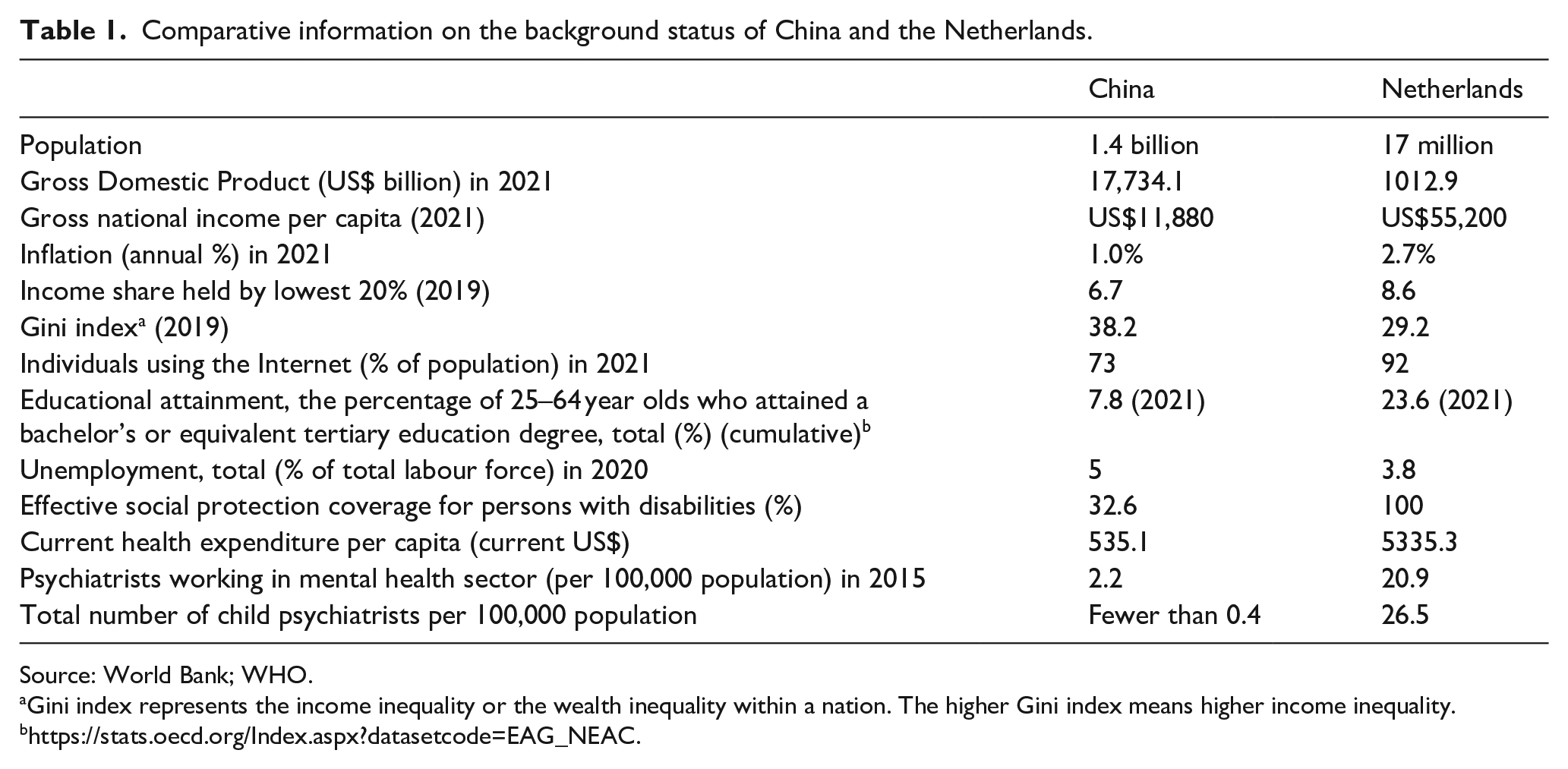
Source: World Bank; WHO.
Gini index represents the income inequality or the wealth inequality within a nation. The higher Gini index means higher income inequality.
To fully understand the outcomes for autistic adults, besides their community integration, we should also take into account their overall well-being, such as happiness and life satisfaction (Lord et al., 2020). Individuals living in wealthier countries tend to report higher life satisfaction compared with individuals in poorer ones (Helliwell et al., 2022), maybe because wealthier countries typically have more beneficial characteristics that contribute to their citizen’s life satisfaction, such as political freedom, civil rights, good governance, and low social inequality (Stavrova, 2019). Cultural and contextual dimensions may also play a role, with Eastern Asian countries emphasizing interdependence (Kamio et al., 2013; Krys et al., 2019) and others’ evaluation and opinions and Western and European countries, valuing individual freedom, achievement, and the personal pursuit of happiness (Ye et al., 2015). However, strong family ties and family support could also positively contribute to life satisfaction in Asian countries (Nainee et al., 2021; Napa et al., 2020). In this study, we compared the community integration and life satisfaction of autistic adults between China and the Netherlands to gain insights into the influence of cultural and contextual factors on the outcomes of autistic adults.
In addition to living in different countries, childhood factors have been found to correlate with or predict adult community integration and/or life satisfaction. Positive outcomes (living independently, having a job and having friends) for autistic adults are consistently associated with higher intellectual abilities (Howlin et al., 2013; Mason et al., 2021) and the absence of co-occurring psychiatric conditions (Kraper et al., 2017; Lin & Huang, 2019). Mixed findings regarding the effects of sex and age on community integration and general well-being have been found in both Asian and European countries (Howlin et al., 2013; Kamio et al., 2013; Lawson et al., 2020; Lin, 2014; Mason et al., 2018; Scheeren et al., 2022). Variations in sample characteristics, such as age of autism diagnosis and intellectual ability, may explain these differences. The association between different socioeconomic status and community integration and life satisfaction in autistic adults remains relatively unexplored. It is important to note that the majority of studies discussed here have focused on self-reporting adults with average to high intellectual abilities, leaving a knowledge gap regarding community integration and life satisfaction of adults with lower intellectual abilities and high support needs (Russell et al., 2019; Scheeren et al., 2023). Given that around 30% of the autism population has an intellectual disability and high support needs (Baio et al., 2018; Zeidan et al., 2022), it is crucial to prioritize understanding the specific challenges faced by this group. A better understanding of the differences in the community integration of autistic adults with high supports needs in China and the Netherlands fits the World Health Organization goals to enhance global social participation for autistic adults (Wickstrom et al., 2021).
We will (a) examine proxy-reported community integration (employment, independent living, friendship) and life satisfaction among young autistic adults in China, and compare them with a sample from the Netherlands, and (b) examine other factors (age, sex, intellectual ability, age of diagnosis, co-occurring psychiatric conditions, use of medicine/intervention, educational level and income level) associated with community integration and life satisfaction of young autistic adults from China and the Netherlands. This study focuses on the early adult life stage of 18 to 30 years, because life satisfaction may differ depending on life stage (Henkens et al., 2022), and early adulthood is a period of transition from school life and dependency to social life and independency (living independently, having a job and making friends) (Winpenny et al., 2020).
Methods
Participants and procedure
This study was part of a bigger study on autistic adults with varying intellectual abilities and daily life skills in China and the Netherlands (https://osf.io/bvxpu/). Participants were asked to fill in the questionnaire based on their respective roles, either as autistic adults themselves or as a caregiver of an autistic adult. Given the high number of adults who were unable to self-report in China, the study reported here focuses exclusively on caregiver reported data. This study focused on the early adult life stage of 18 to 30 years. We therefore excluded autistic adults aged below 18 years and above 31 years (see Figure 1 in Supplementary Materials for sample selection process). Participants with missing data on predictors (IQ level and use of intervention and medicine) were excluded from the final analysis. The final sample included 99 Chinese and 109 Dutch adults. There were no significant differences in age, sex, and IQ between the included and excluded participants.
The Chinese participants were recruited via the Autism Research Centre of Nankai University (NKARC), Tianjin, China in the autumn of 2022. NKARC has built a network of over 100 service centres of adults with autism covering all major regions of China. To increase the recruitment of autistic adults, we employed the snowball method through help from leading Chinese psychiatrists, as well as autism researchers and service providers in the autism field. These professionals have connections with autistic adults, groups of autistic adults, or families including autistic adults. The participants were from the eastern side of the Heihe–Tengchong Line, with 94% of China’s population resided east of the line (see Figure 2 in Supplementary Materials for the city distribution of Chinese participants), ranging from first-tier cities (typically with a population of more than millions of people) to fourth-tier cities (typically with a population of hundreds of thousands). Caregivers of autistic adults were invited to participate in our study through an online survey and reported on behalf of the autistic adult. All of the included Chinese adults were diagnosed with autism by clinicians (psychiatrists, psychologists and paediatricians).
Dutch participants were included via the Netherlands Autism Register (NAR, https://www.nederlandsautismeregister.nl/english/), a nationwide autism register that collects information on an annual basis from autistic individuals and their caregiver. All Dutch participants had a formal autism diagnosis according to DSM-IV or DSM 5. The NAR has a diverse distribution of men and women, across all ages, intelligence levels and the entirety of the Netherlands (https://cijfers.nederlandsautismeregister.nl/index.html).
Participants were invited to complete the study through an online survey. Participants did not receive payment for their participation. Caregivers consented to participate by reading the informed consent statement and checking a box indicating their agreement. The data collection has been reviewed and approved by the ethics committee of the Vrije Universiteit Amsterdam (VCWE 2020-041R1) and Nankai University (NKUIRB2022127).
Measurements
Outcome measures
Community integration
Following research by Howlin et al. (2004) and Scheeren and Geurts (2015) community integration was measured by employment, independent living, and friendship with hierarchical ratings reflecting different levels of attainment in these areas. The overall community integration rating of an individual was summed up by points on employment scale, independent living, friendship, and leading to a composite score ranging from 0 to 8, making it possible to classify individuals as having very poor (0 points), poor (1–3 points), fair (4–6 points), good (7 points) and very good (8 points) overall community integration; See also Table 1 in Supplementary Materials with detailed codes column and scale points.
Life satisfaction
Life satisfaction was measured by the 0 to 10 Cantril Ladder scale: ‘Where would you rate the life of the person with autism generally on a scale from 0 to 10?’, with ‘10’ indicating the best possible life and ‘0’ the worst possible life. Higher scores indicate higher life satisfaction (Cantril, 1965). This measure has also been used with autistic adults before (Grove et al., 2018; Scheeren et al., 2021). The World Happiness Report data also include Cantril Ladder data from China and show cross-cultural validity (Helliwell et al., 2022). The Cantril ladder has been found to be a culturally sensitive measure that can be used internationally (Bartels & Boomsma, 2009).
Demographic variables
Age and age of diagnosis were coded into in years. Sex (1 = male, 0 = female) and Country (1 = China, 0 = Netherlands) were coded into dichotomous variables.
Intellectual ability was reported by the caregiver at a numerical scale, ranging from 1 (IQ below 40 (severe intellectual impairment)) to 7 (IQ above 130 (gifted)), with each number corresponding to a specific IQ range and description. Informants were asked about their IQ test history and asked to select the appropriate IQ level that best described the adults’ intellectual ability. If autistic adults had never taken a IQ test or their IQ score was unknown, informants were asked to estimate their intellectual ability and select the corresponding level. In the current study, 81.7% of Chinese IQ reports and 82.6% of Dutch IQ reports were based on a prior IQ test. A high correlation (r = −0.71) between proxy-reported IQ and adaptive functioning has been found in previous study (Werkman et al., 2020) providing initial support for the validity of proxy-reported IQ.
Co-occurring psychiatric conditions was assessed by asking if autistic adults currently had any other psychiatric diagnosis besides autism. The options for response were ‘Yes’, ‘No’, or ‘Don’t know’. If the response was ‘Yes’, a follow-up question was asked to specify the specific diagnosis. Co-occurring psychiatric conditions was coded on a dichotomous scale (0 = Yes, 1 = No).
Use of interventions and medicine was measured by asking if autistic adults have taken any interventions related to autism. The options for response were ‘Yes’, ‘No’ or ‘Don’t know’. ‘Yes’ responses were followed up with a question about the specific intervention and specific medication, including and an indication of the duration and intensity of the intervention followed. Use of interventions and medicine was coded on a nominal scale (0 = no use of intervention and medicine, 1 = receives intervention or medicine, 2 = receives intervention and medicine).
Household income level was categorized into income bands per country, based on country-specific percentiles (low: below 30th percentile; middle: 30th–70th percentile; high: above 70th percentile) of the National Bureau of Statistics of China (2021) and Statistics Netherlands (CBS; 2021) separately. The exact bands were as follows: low (China: ¥0–¥4110 a month, €0–€6740 a year; Netherlands: €0–€30,000 a year), middle (China: ¥4110–¥10,292 a month, €6740–€16,878 a year; Netherlands: €30,000–€70,000 a year) and high income (China: above ¥10,292, above €16,878 a year; Netherlands: >€70,000 a year). We considered income levels based on household population for each country separately rather than absolute income over both countries, because some adults may live independently or living in a care facility.
Educational level was categorized into the low, middle and high level of education in each country, based on the Chinese and Dutch educational systems. Primary school and special school were categorized into low level of education, secondary school were categorized into middle level of education, and university (Bachelor, Master, Doctoral) were categorized into high level of education in both countries.
Topics in the online survey were assessed in the following order: sex, age, IQ test, diagnosis of autism, age of diagnosis, co-occurring psychiatric diagnosis, use of medicine/intervention, educational level and household income level. Questions about demographics were followed by questions about employment status, living situation, friendship and life satisfaction.
Instruments translation
All of the questions and questionnaires were originally developed and collated in Dutch based on the NAR annual survey. The translation of the questions and questionnaires into Mandarin Chinese was conducted following the forward and backward procedure (Hall et al., 2018). First, all of the items were translated from Dutch into Mandarin Chinese by two Chinese PhD candidates in the Department of psychology at Utrecht University and the University of Amsterdam, who are fluent in Dutch and obtained at least a B1 Dutch language certificate. To maintain the meaning of words and sentences between Dutch and Mandarin Chinese, a back-translation was conducted by a Dutch translation agency, translating it back into Dutch. The original Dutch and back-translated versions were compared by two native Dutch speakers, co-authors of this paper (A.S. and S.B.). Discrepancies were revised to more accurately express the intent of the wording in the original version. The translated Chinese items were checked and adapted by the authors. Therefore, the Mandarin Chinese questions could be considered linguistically equivalent to the original Dutch version.
Data analysis
We performed hierarchical multiple regression analyses to investigate the predictive value of country (China/Netherlands) on community integration and life satisfaction of autistic adults, by controlling for the impacts of age, sex, intellectual ability, comorbidities and use of medicine/interventions. In each regression model, we first entered age, sex, intellectual ability, co-occurring psychiatric conditions and use of interventions, followed by country in a second step. Three ordinal logistic regression analyses were also conducted to investigate whether demographic factors and country predicted each component of community integration (employment, independent living, friendship).
Based on a power of 0.95 and an alpha level of 0.05, the required total sample size to detect a medium effect (f = 0.15) in a multiple regression analysis including 6 predictors is 146 participants in total (Cohen et al., 2014).
Due to the missing values in the educational level (42 Dutch missing data) and income level (16 Chinese missing data and 38 Dutch missing data), the participants included in the final analysis did not meet the power to detect a medium effect. Therefore, we conducted supplementary analyses by adding either the educational level or income level as an extra predictor in the multiple regression model to explore their impacts on community integration and life satisfaction.
Community involvement
In this study, autistic individuals were not actively involved in the design, but formulation of the NAR (Dutch) survey was developed in collaboration with a panel of autistic individuals and their parents. Every year, the NAR brings together a panel of stakeholders (autistic individuals and parents of children of varied abilities) to discuss and exchange opinions on current research issues, methodology and dissemination of findings. The NAR also has several autistic team members.
Results
Descriptive statistics
The complete data consisted of proxy-reported data on 99 Chinese and 109 Dutch autistic adults, aged 18 to 30 years, with no missing data on predictors (IQ level and use of intervention and medicine, see Table 2 for participant details and statistical details).
The demographic variables between China and the Netherlands.
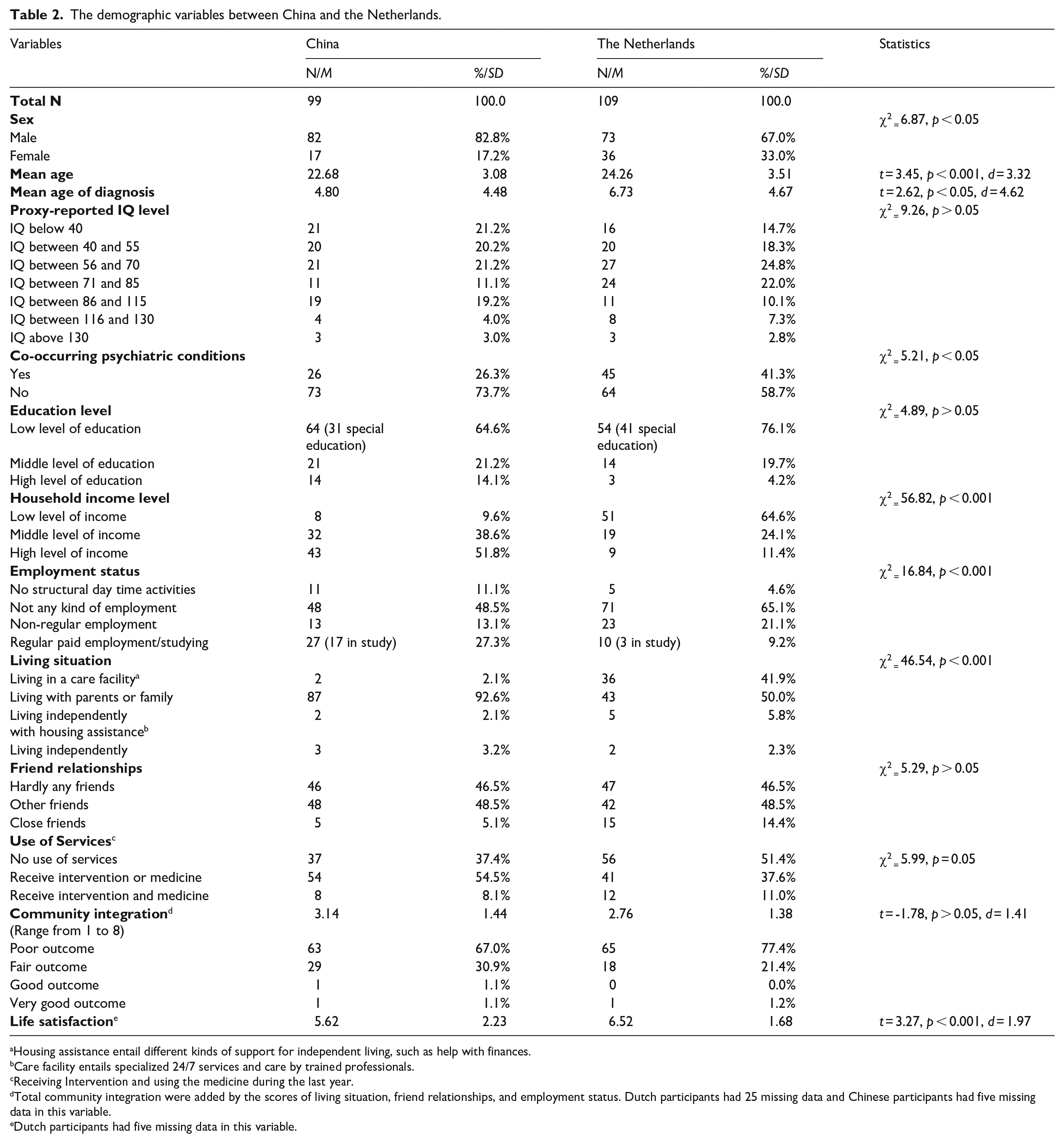
Housing assistance entail different kinds of support for independent living, such as help with finances.
Care facility entails specialized 24/7 services and care by trained professionals.
Receiving Intervention and using the medicine during the last year.
Total community integration were added by the scores of living situation, friend relationships, and employment status. Dutch participants had 25 missing data and Chinese participants had five missing data in this variable.
Dutch participants had five missing data in this variable.
The Dutch sample was older and diagnosed later than the Chinese sample, the differences in age (d = 3.32) and age of diagnosis (d = 4.62) between countries were large in effect size (Cohen, 1988). Most autistic adults in both countries had low educational levels (64.6% in China and 76.1% in the Netherlands) and over half (62.6% of Chinese and 57.8% of Dutch adults) of the samples in both countries were reported to have an IQ below 70. More Dutch adults (41.3%) were reported to have a co-occurring psychiatric diagnosis than Chinese adults (26.3%). Intervention and medicine use were similar across countries, with 62.6% of Chinese and 48.6% of Dutch adults using at least one service (intervention or medicine).
More Chinese adults (51.8%) were reported to have a relatively high household income level compared with Dutch adults counterparts (11.4%). It should be noted that we only asked about the household income. Since a larger proportion of Chinese adults (92.6%) lived with their parents than Dutch adults (50%), their household income included their parents’ income. However, a larger proportion of Dutch adults (41.9%) lived in care facilities compared with Chinese adults (2.1%). Therefore, when an adult was reported to reside in a care facility, their household income was primarily based on their personal income. Consequently, more than half of the Dutch autistic adults included in the study exhibited low household incomes.
Outcome measures
Most participants did not have any kind of paid or unpaid employment (59.6% in Chinese and 69.7% in Dutch sample), and few of them were reported to have close friends according to their caregiver. Very few Chinese adults (5.3%) and Dutch adults (8.1%) lived independently with or without housing assistance.
Chinese and Dutch adults showed limited, but similar community integration (d = 1.41; see Figure 3 in the Supplementary Material for the score distribution of the overall community integration in each country). Most autistic adults in both countries had a poor community integration according to their caregiver (67% in Chinese sample and 77.4% in Dutch sample) and 30.9% of Chinese adults and 21.4% of Dutch adults had a fair community integration. For the life satisfaction, Dutch adults had higher proxy-reported life satisfaction than Chinese adults, with a large effect size (d = 1.97). In both countries, adults’ community integration and life satisfaction were modestly, but positively correlated (Netherlands: r = 0.280, p < 0.05; China: r = 0.272, p < 0.05). When examining the correlations between life satisfaction and the different facets of community integration in each country, life satisfaction was only significantly correlated with employment status (r = 0.249, p < 0.05) and friend relationship (r = 0.307, p < 0.05) in the Chinese sample.
Predictors of community integration and life satisfaction
Based on the hierarchical multiple regression analyses, demographic factors (age, sex, intellectual ability, co-occurring psychiatric conditions and use of medicine/intervention) explained 28% of the variance in overall community integration at Step 1, F (5, 172) = 13.55, p < 0.001 (see Table 3). Autistic adults with a higher proxy-reported IQ level (β = 0.47, p < 0.001) and younger age (β = −0.06, p < 0.05) were reported to have better community integration. None of the other demographic factors were associated with community integration. Chinese and Dutch adults showed similar impacts on community integration (R2 = 0.01, β = 0.33, p > 0.05). After adding country into the model at Step 2, age lost its association with community integration (β = −0.05, p > 0.05), suggesting that there might be a country-specific effect. A post hoc regression analysis on community integration in each country separately revealed that younger adults were reported to be more integrated in the community in the Dutch sample (β = −0.08, p < 0.05, see Supplementary Table 3), but not in the Chinese sample (β = −0.01, p > 0.05).
Multiple regression analyses of demographic variables of autistic adults and country as predictors of total community integration in ASD.

p < 0.05; **p < 0.005.
At Step 1, demographic factors did not contribute to the variance of the proxy-reported life satisfaction of our participants, R2 = 0.03, F(5, 197) = 1.34, p > 0.05. At Step 2, country had a significant impact on life satisfaction, with lower proxy-reported life satisfaction in Chinese adults, R2 = 0.06, F(6, 196) = 3.41, p < 0.005 (see Table 4). After adding country into the model, autistic adults without a co-occurring psychiatric diagnosis showed better life satisfaction than those with a co-occurring condition (β = 0.65, p < 0.05). A post hoc regression analysis on life satisfaction in each country separately showed that adults without co-occurring psychiatric conditions reportedly had a higher life satisfaction in the Dutch sample only (β = 0.78, p < 0.05, see Supplementary Table 4).
Multiple regression analyses of demographic variables of autistic adults and country as predictors of life satisfaction in autistic adults.
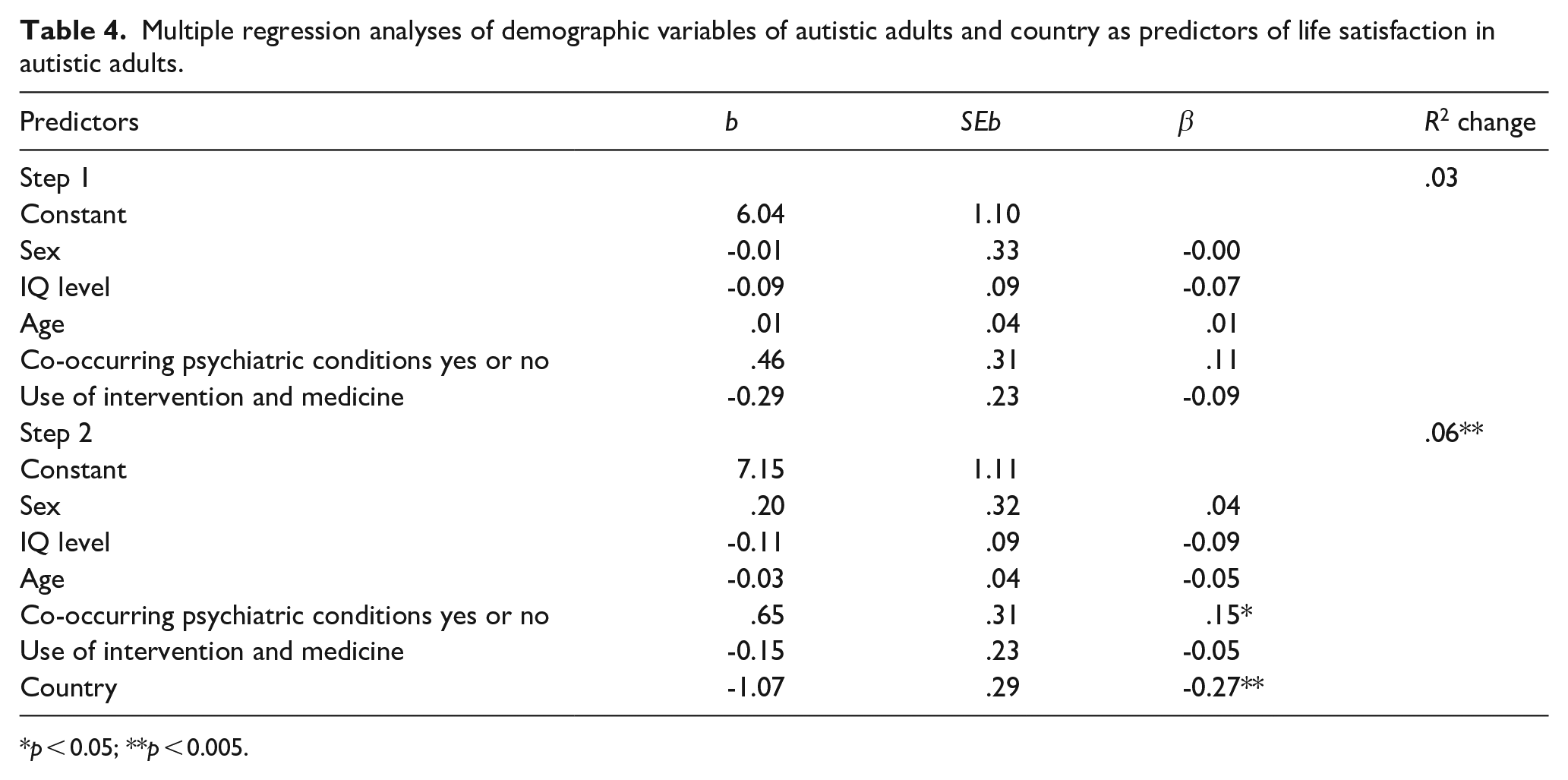
p < 0.05; **p < 0.005.
The results are similar when country is entered first (instead of second) into the regression model. Country was not a significant predictor of community integration, R2 = 0.02, F(1, 176) = 3.16, p > 0.05, and was a significant predictor of life satisfaction, R2 = 0.05, F(1, 201) = 10.67, p < 0.005.
The ordinal logistic regression analyses showed that all predictors accounted for a significant amount of variance in employment status, likelihood ratio χ2(7) = 33.14, p < 0.001; independent living, likelihood ratio χ2(7) = 50.51, p < 0.001; and friendship, likelihood ratio χ2(7) = 19.60, p < 0.01. Autistic adults with a higher proxy-reported IQ level were reported to have greater levels of employment, independent living and friendship (see Table 5 to 7 in Supplementary Materials for statistical results). Country only was a significant predictor of the independent living scale, with Dutch participants more likely living in more strongly supported accommodations than Chinese participants (B = -2.069, SE = 0.445, Wald χ² = 21.587, df = 1, p < 0.001, OR = 0.126, 95% CI [0.053, 0.302]). This difference was explained by Dutch participants being much more likely to live in residential care facilities (42%, and 50% living with parents) while Chinese participants mostly lived with family (93%).
When only adding educational level into the model, the samples were reduced (99 Chinese and 68 Dutch adults) due to missing educational data. Lower educational levels predicted poorer community integration (β = 0.62, p < 0.005). Educational level did not significantly predict life satisfaction (β = 1.02, p > 0.05). Only adding household income level into the model also reduced the samples (83 Chinese and 77 Dutch adults). Household income level did not predict community integration (β = 0.23, p > 0.05) and life satisfaction (β = 0.35, p > 0.05) for both samples.
Discussion
In China and the Netherlands, we investigated levels and determinants of community integration (employment, independent living, friendship) and life satisfaction of autistic adults with relatively high support needs. In both countries, community integration was limited, with low rates of employment, limited independent living and few close friendships according to their caregiver. Chinese autistic adults had lower proxy-reported life satisfaction than their Dutch counterparts. Autistic adults with a higher proxy-reported IQ level were reported to have better community integration. Only in the Dutch sample, younger adults were more integrated into the community than older adults, and adults without co-occurring psychiatric conditions tended to have better life satisfaction. Sex, household income level and use of intervention/medication did not predict community integration or life satisfaction in both samples.
In our study, the majority of both Chinese (67%) and Dutch (77%) participants showed poor community integration, as indicated by low rates of employment, limited independent living, and few close friendships. The employment rates (40.4% Chinese and 30.3% Dutch adults had some form of (un)paid employment) align with previous studies involving participants with intellectual disabilities (31%–48%) (Billstedt et al., 2011; Cameron et al., 2022; Farley et al., 2018). These findings highlight that young autistic adults with relatively high support needs in high-income developed countries appear to face similar challenges to those in middle-income developing countries. Barriers such as negative attitudes (Wei et al., 2018) and limited accessibility to appropriate services (Malik-Soni et al., 2022; Sun et al., 2013) can hinder the integration of autistic individuals into mainstream settings in both high- and low-income countries. For example, in China, despite the initiation of social inclusion training programmes for autistic individuals by service organizations and special schools (Li & Qi, 2023; Xiao, 2023), the provision of effective social inclusion services for autistic adults is hindered by financial constraints (Clark et al., 2019), particularly for individuals with lower socioeconomic status, as well as limited funding for the recruitment and training of professionals and the development of well-designed training programmes (Li & Qi, 2023). This limitation in service delivery results in restricted access and diminished quality of support for autistic individuals, potentially impeding their community integration. Similarly, in high-income countries, despite a potentially higher availability of support services, challenges may arise due to long waiting lists, inadequate funding, or difficulties in navigating complex service systems (Malik-Soni et al., 2022). Community integration could be improved by promoting awareness and understanding of autism, challenging negative attitudes and stereotypes, improving accessibility to appropriate services and providing tailored support for individuals with high support needs.
Even though average community integration level was comparable in both countries, a notable difference was identified in living situation. 92.6% of Chinese adults resided with their families, while around half (50%) of the Dutch adults lived with their families. Around 42% of Dutch adults lived in a care facility. This result indicates that Chinese parents tend to take care of their adult autistic child, whereas care for autistic adults with high support needs appears more institutionalized in the Netherlands. In 2021, Mainland China witnessed a notable rise in the total number of autism rehabilitation institutions designated by the China Association of Persons with Psychiatric Disability and their Relatives (CAPPDR), reaching 2304 establishments (source: https://www.cappdr.org/). However, there is an obvious exclusion of children above the age of seven (Li & Qi, 2023). Among these institutions, 60% of these institutions primarily cater to children aged eight and below, while only 17% of the services were directed towards children aged 9 to 14. This data underscores a substantial gap in support for older autistic adults in these institutions. To address this issue, it is essential for autism rehabilitation institutions to expand their services more to older autistic adults and ensure that all age groups within the autism spectrum receive the appropriate care and support they need.
Chinese autistic adults were reported to have significantly lower life satisfaction (5.62) compared with Dutch adults (6.52). The difference in life satisfaction may be attributed to three possible factors. First, China has a less comprehensive system of support services for adults on the autism spectrum compared with the Netherlands, including lower per capita healthcare expenditure, lower effective social protection coverage and a shortage of psychiatrists and child psychiatrists (Table 1). These inadequate services limit access to professional and financial support (Xiang et al., 2018), possibly leading to lower life satisfaction. Second, limited public knowledge about autism in China (Yu et al., 2020) may contribute to stigma experienced by families with autistic adults, which can negatively impact the caregivers and lower the autistic individuals’ sense of social inclusion and happiness (Ma et al., 2023; Wei et al., 2018). The Netherlands demonstrates a longer history of Dutch autism self-advocacy (Waltz et al., 2015) and organizations such as the Dutch Autism Society (NVA, founded in 1978) dedicated to the inclusion and support of autistic individuals. This may contribute to reduced stigma and improved life satisfaction in Dutch autistic individuals. Third, heightened parenting stress among Chinese compared with Dutch caregivers may also have resulted in lower perceived life satisfaction of their child. A more comprehensive understanding of the experiences and life satisfaction of autistic adults in different countries is needed for the development of targeted interventions and policies to improve their quality of life.
Our study found that Chinese autistic adults were reported to have lower life satisfaction compared with Dutch autistic adults, consistent with the World Happiness Report’s observation that European countries generally have higher average life satisfaction than China (for example, the Netherlands with an average score of 7.40, in contrast to China’s average score of 5.82) (Helliwell et al., 2022). Our findings need to be understood within the broader context of country-level differences in life satisfaction. In both countries, the life satisfaction of autistic adults with relatively high support needs was lower on average than the life satisfaction of the general population. This highlights the significance of prioritizing mental health support and interventions aimed at enhancing the life satisfaction of autistic adults with high support needs worldwide.
When examining predictors of life satisfaction, demographic factors only explained 3% variance in proxy-reported life satisfaction. It is important to recognize that life satisfaction is a complex and multi-dimensional construct that may not be fully explained by demographic characteristics alone. Our study primarily relied on yes/no responses and basic information about employment and living arrangements, which likely do not capture the full complexity of individuals’ experiences. Only within the Dutch sample, co-occurring psychiatric conditions predicted lower life satisfaction, consistent with previous findings (Kraper et al., 2017; Lin & Huang, 2019; Scheeren et al., 2022). However, in our Chinese sample, the prevalence of co-occurring psychiatric conditions (26.3%) was surprisingly low compared with both the Dutch sample (41.3%) as well as prior adult studies (75%) (Sharma et al., 2018). This limited variability within our Chinese sample likely impeded us from thoroughly investigating the association between co-occurring psychiatric conditions with life satisfaction. The lower report of co-occurring psychiatric conditions may be related to the Chinese tendency to prioritize physical health over mental health (Lin & Cheung, 1999), lack of professional services and trained diagnosticians (Pang et al., 2018), as well as a greater stigma surrounding mental health issues in China (Yin et al., 2020). Future studies should utilize multiple methods of assessment to capture a more accurate representation of mental health issues, for example, incorporating clinical diagnostic assessments and standardized measures of co-occurring psychiatric conditions.
There are a number of limitations of this study. First, because over half of autistic adults in our samples were reported to have an IQ below 70 and could not independently participate, we used proxy-reported life satisfaction as one outcome measure. This is a limitation, because life satisfaction is inherently a highly personal and subjective experience. Caregiver reports may be influenced by the caregiver’s own perspectives and feelings, such as parenting stress, and may therefore not be a valid substitute for self-reports (Knuppel et al., 2018). However, Hong et al. (2016) did find strong correlations between adult self-reports and proxy-reports. Second, given our focus on young autistic adults with relatively high support needs, a majority of whom were reported to have intellectual disabilities, participants in this study are probably not representative for older autistic individuals with low support needs and/or an adult autism diagnosis in both countries. There is likely a large number of undiagnosed individuals (with higher intelligence levels) in China (Zhou et al., 2020) and, in line with other Western countries, a presumed majority of autistic adults in the Netherlands has an average to high intelligence level. Third, despite similar proxy-reported IQ levels, cross-country differences in clinical practices and participant recruitment may have resulted in less comparable samples. For instance, in China, adults and those with relatively few symptoms are less likely to be diagnosed (Huang et al., 2013). Therefore, our Chinese sample, recruited via autism research centre, mainly consisted of individuals with a co-occurring intellectual disability who may have shown more typical autism symptoms from a young age. Conversely, in the Netherlands, recruitment through an online survey allowed for the inclusion of participants with a broad range of skills, intellectual abilities, and autism symptomatology. This may also explain why the Chinese participants in this study were diagnosed at an earlier age than the Dutch participants. Fourth, limited by the online survey context, we were unable to directly verify the IQ levels of the autistic adults and solely relied on caregiver reports. Future studies should ideally incorporate standardized IQ measurements.
As this is one of the first English publications on community integration and life satisfaction of autistic adults in Mainland China, we call for more research on the outcomes and experiences of autistic adults in Eastern Asian countries, such as China, preferably via self-report. Despite extensive efforts and a nationwide network, recruiting self-reporting autistic adults in China for research purposes proved especially challenging. Many Chinese autistic adults have a co-occurring intellectual disability and receive their autism diagnosis in early childhood. Stigma surrounding autism and mental health issues in general may discourage adults seeking a diagnosis or openly identifying as autistic (Huang et al., 2013; Ma et al., 2023). This is further compounded by a general lack of awareness and expertise in diagnosing autism in adults, particularly among those who exhibit adequate social functioning (Huang et al., 2013). In addition, given the lack of subsidy and financial support for neurodiverse adults in China, it is generally not beneficial to be diagnosed autistic. Enhancing public awareness of autism and collaborating with local autism organizations and support groups are pivotal steps towards building trust and fostering increased engagement in research within the autistic community.
In our study, autistic adults in both countries showed low rates of employment, limited independent living, and few close friendships, suggesting that common, but culturally sensitive and tailored interventions could be developed. Specific skills necessary for community integration, such as self-care and daily living skills (Kamp-Becker et al., 2010), could be targeted to increase integration and participation. Moreover, we encourage more research on autistic adults with high support needs, in both low- and high-income countries. Using a brief adaptive functioning caregiver-report measure and/ or a brief measure of autistic traits could help provide a more comprehensive understanding of this group. Furthermore, community integration measures often rely on ‘normative’ standards that may not always be desirable or fitting for autistic adults, particularly for those with high support needs (Bishop-Fitzpatrick et al., 2016). Other crucial aspects such as access to meaningful and enjoyable everyday life activities, good physical and mental health, neighbourhood support, supportive family contacts are also important to consider when evaluating the community integration of autistic adults (Howlin, 2021). It is crucial for future research to include direct input from autistic individuals themselves (both with and without high support needs), integrating qualitative and quantitative research methods, to provide deeper insights into their personal experiences of what it means to belong to a community and to learn more about optimal ‘person-environment fit’ (Lai et al., 2020). Also, self-report measures, such as the PROMIS (Vaughan et al., 2020) or Single Item QoL (Williams, 2021), could provide a more direct and accurate assessment of adults’ life satisfaction. In order to gather information directly from autistic adults with co-occurring intellectual disability, the use of technology, such as self-administered electronic interfaces, could be useful (Walton et al., 2022).
In conclusion, this study sheds light on the community integration and life satisfaction of autistic adults in China and compares them with their counterparts in the Netherlands. The findings highlight the shared challenges faced by both Chinese and Dutch autistic adults with high support needs.
Supplemental Material
sj-docx-1-aut-10.1177_13623613241258182 – Supplemental material for Autistic adults in China and the Netherlands: Proxy-reported community integration and life satisfaction
Supplemental material, sj-docx-1-aut-10.1177_13623613241258182 for Autistic adults in China and the Netherlands: Proxy-reported community integration and life satisfaction by Fangyuan Liu, Sander Begeer, Rosa A Hoekstra, Chongying Wang and Anke M Scheeren in Autism
Footnotes
Acknowledgements
The authors would like to thank all caregivers for participating in this study. Great thanks to Mengtian (Maggie) Xia, Postdoc researcher in Radboud University and Kaiyang Qin, Postdoc researcher in University of Amsterdam for helping translating the Dutch questionnaire into Chinese. Many thanks to Lingyue Kong and Jing Fan (founder of Qingdao Yilin Autism Center) for all of the help with the data collection and double-checking the data.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect of the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper is an outcome of a major research project granted by Natural Science Foundation of Tianjin Municipal Science and Technology Commission (23JCZXJC00320), Beijing Natural Science Foundation (J230013) and the National Social Science Foundation of China (Grant No. 21&ZD182) titled as “Social Mechanism of Vitality of NGOs for the People with Disabilities”. FL is funded by China Scholarship Council (no. 201806990043) for the study at Vrije Universiteit Amsterdam. SB and AMS are financially supported by the NWO (grant no. Aut.17.006) and the ZonMW (grants no. 40-00812-98-16064 and 60-63600-98-834). RAH receives support from the National Institute of Health Research (NIHR200842) using UK aid from the UK Government. The views expressed in this publication are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.