
Abstract
This article focuses on contemporary responses to public health messages in Denmark, a country whose system of social welfare is, like that of the United Kingdom and the rest of Europe, undergoing increasing levels of marketization and privatization. Drawing primarily upon Robert Crawford’s analysis of healthism as a neoliberal project, the aim of this article is to develop critical understandings of how individuals respond both bodily and emotionally to ideologies of health and the body in the context of a changing marketplace for the consumption of health and its messages. This article will analyze perceptions and practices of health in Denmark. The findings will then be discussed in relation to dimensions inspired by the work of Crawford, who regards “health” as a “super-value,” an outcome of individual security strategies, and mode of citizenship in the marketplace. The article argues that Crawford’s discussion does not fully capture the ways in which people use their bodies to valorize themselves. First, the perception of the state is perceived as being aligned with commercial interests. As a consequence, neither state- nor market-based (i.e. commercial health product and service providers) health advice is fully trusted. Instead, the opinions of non-market actors such as peers and friends as well as of alternative practitioners that are considered outside the market since they do not represent corporate interests become more attractive among citizen-consumers who are concerned about their health. The article concludes with a discussion of the implications of our findings for theorization of public health and health policy.
Introduction
Notions of “health” have become more ideologically complex than ever. As the public medical systems in many countries become increasingly intertwined with market-based mechanisms, individuals have also made a significant ontological and epistemological shift away from being “patients” under the care of a medical expert to independent agents who make decisions for themselves. Thus, the notion of the individual as a consumer of healthcare has become widely accepted in many parts of the world as the forces of neoliberalism and marketization sweep across healthcare systems (Ayo, 2012; Crawford, 1980, 2004; Henderson and Peterson, 2002). The withdrawal of the state from providing universal health coverage for its citizens has meant that the individual is situated more and more as the locus of responsibility and control for his or her own health and well-being while the public sector provides a large amount of information in order to guide the “health consumer” in making what is perceived as rational choices (Henderson and Peterson, 2002; Lupton, 1995, 1997a; Rose, 2010, 1999; Williams, 1998). At the same time, the consumer is bombarded with messages and warnings about health and well-being from media and private health actors. The question then becomes how much of health—including the foods and messages about the food consumed—is ideologically saturated with prevailing moral, political, and economic values and fashions of the day? (Lien and Nerlich, 2004; Ulver-Sneistrup et al., 2011). Relatedly, to what extent does the individual “buy into” health messages and how do they chose between the often baffling plethora of different voices in the marketplace? Furthermore, what are the social, political, and moral implications of this phenomenon for consumers?
This article discusses, and builds upon, the political economist Robert Crawford’s concept of healthism in the context of a changing healthcare system in Europe, Denmark, in order to show how consumers negotiate public health messages and their own, often conflicted, health and life choices. Crawford argues that public health awareness from the 1970s onwards was a consequence of a political ideology which regarded health in terms of individual acts and omissions (Crawford, 1977, 1980, 1994, 2004, 2006). As a result, what he calls “healthism” is ideological in nature and scope. Healthism is a crafted lifestyle that prioritizes health and fitness over anything else and relies on individuals’ drive and motivation to achieve these aims. Crawford (1980) argues that “for the healthist the solution (to health problems) rests within the individual’s [author’s italics) determination to resist culture, advertising, institutional and environmental constraints, disease agents, or simply, lazy or poor personal habits” (p. 368).
The purpose of the article is consequently to analyze how people respond to health messages, using Denmark as a case study. In so doing, we challenge Crawford’s analysis and point to some of the possible implications of public health ideologies as understood by the layperson (e.g., Popay et al., 1998; Popay and Williams, 1996). Additionally, we draw on the notion of the imaginary (Castoriadis, 1987 [1975]; Durand, 1993) as a way of understanding contemporary healthism. For Castoriadis (1987 [1975]), the social imaginary designates a particular socio-historical and institutionalized form of the imaginary. Castoriadis’ theorization of social change is bound up in his metaphor of collective social significations: these systems of signaling approval or disapproval of self and others shape society and social behavior, allowing social forms to emerge through processes of creation. This creative process is as important as the systems that bind us all. In this context, Durand (1993) adds a psychological dimension to Castoriadis’ notion of the imaginary and schematizes the ways in which the imaginary challenges existing, institutionalized conceptualizations and re-rationalizes them in new ideological forms. He qualifies this process as a combination of “progressive rationalizations of the mythic” and “progressive disqualification of conceptualizations” (Durand, 1993: 22).
In this light, we argue that whereas bodily health belongs among the most consistent significations in the social imaginary, contemporary ideological expressions of healthism have significant consequences for the ways in which this fundamental part of our social imaginary forms and informs our lives, choices, and evaluations. Healthism also links to how consumers negotiate with the social and moral values perceived in being “healthy” while this process is itself intimately tied to the microphysics and practices of everyday life and the ways people negotiate and position themselves in the health landscape among their social peers. As Crawford (1980) argued, healthism is associated with a set of tensions and dilemmas inscribed not only in the bio-medical domain, but which also interpenetrates moral, political, and social spheres of life.
The drive toward “healthism” and the political-industrial complex that surrounds it—as well as the ideological pressures it engenders—has been pointed out by a number of scholars, such as Petr Skrabanek (1994), who declared in The Death of Humane Medicine that “healthism” led men and women to a state of fear and repression. He argued that the pursuit of perfect health was a weapon of the totalitarian state, and made specific references to the Nazi regime in Germany and the Soviet Union. Even less radical approaches are indicative of the increasing evidence with which healthism—qua state policy—is increasingly internalized by citizen-consumers in overt and subtle ways, and through strategies and practices which are not as yet fully understood (Cohn, 2014; Cole and Gaeth, 1990; Crawford, 1980; Oliver and Berger, 1979).
To develop our understanding of how citizens negotiate with their own bodies and identities in the realm of healthism, we conducted fieldwork in two Danish cities, Copenhagen and Odense. Denmark, while being widely admired in the West for its robust social welfare system and high standards of living, is undergoing important and far-reaching changes to its health and welfare systems, much like the rest of Europe. At the present time, health and social services in several Western countries are increasingly characterized by marketization and privatization (Petersen, 1997; Petersen and Lupton, 1996), a trend which is, in fact, still under-researched by health and political economists, health marketers as well as social researchers. The neoliberal ethos, with its emphasis on autonomy and self-management, is already having a clear impact on Danish consumers. Studying the Danish case, therefore, is theoretically and politically important because Danish consumers are coming to accept many of the ideological features of a marketized healthcare system that are already firmly entrenched and accepted by Americans, for instance, but which are still in transition in Europe as a whole.
Healthism and the neoliberal doctrine
Researchers have recently pointed to the pivotal role of the neoliberal state in shaping citizens’ health practices. As noted by Ayo (2012), governmentality is a useful tool for understanding how health promotion works “by inciting the desire within autonomous individuals to choose to follow the imperatives set out by health promoting agencies, and thus, take on the responsibility of changing their own behaviours accordingly” (p. 100). Indeed, as pointed out by Rose (1999), many of us no longer require state bureaucracy to monitor and direct consumer behavior with regards to, for instance, the habits of eating, personal hygiene, dental care, and so on. Rose (1999) notes that In the name of themselves as consumers with rights, they take up a different relation with experts and set up their own counter-expertise, not only in relation to food and drink and other “consumables,” but also in relation to the domains that were pre-eminently “social”-health, education, housing, insurance and the like. (p. 87)
The public have internalized “healthism.” The recent wave of cutbacks, crises, and austerity throughout Europe has engendered a growing sense that the individual cannot depend forever on the state’s largesse. The state, in effect, has now in many ways withdrawn from the individual’s life-frame as a defining (or authoritative) source of control.
Fundamental problems emerge, however, as the state withdraws from health and social services provision for its citizens with the public increasingly exhorted to take individual responsibility for their bodies by engaging in strict self-care regiments. These regimes require individuals to accept the body as a project whose interior and exterior can be monitored, nurtured, and maintained at optimally functional levels (Schillings, 2003: 199). The body has, therefore, become a site of “personal strategies of health” (Turner, 2008 [1996]) that reflects the image of the body as a closed self-contained autonomous entity in a global system characterized by multiple and inescapable risks (Beck, 1992). As pointed out by Beck (1992) and Thompson (2005), it is difficult for citizen-consumers to evaluate health risks in connection to consumption as health threats unfold through complex mechanisms and indirect causal chains, which operate through time and space. Although health choices made by consumers increasingly stand in opposition to traditional knowledge hierarchies and consumer activism thrives in a culture of “DIY” beauty and health regimes and enhanced individualization of the body, it is unclear how far individuals can actually control their symptoms and underlying illnesses without resorting, to some extent, to professional medical and clinical expertise. Yet, the neoliberal regime promotes the ideology that the individual alone is the agent of change. Furthermore, the neoliberal state, as noted by Bauman (1999), exacerbates bodily anxieties because the individual is now thrown into a situation where her or his health becomes a matter of personal responsibility.
Crawford’s political economy of healthism
Crawford notes that the pursuit of health in modern societies occurred within the context of a movement that emerged in the 1920s and 1930s, culminating in its formation as an individual matter, a problem “within the boundaries of personal control” (Crawford, 2006: 408). Healthism, as understood by Crawford (1980, 1994, 2006), represents a kind of supreme value for many citizens in developed economies, and encompasses a plethora of social practices and arrangements appear to empower the individual to improve or even perfect her/his health and to encourage others to do the same. Paradoxically, however, healthism engenders both control and helplessness: as individuals use healthism to guard against anxiety, their health becomes a cause for anxiety. Although publicly and openly marketed as a highly social and energetically celebratory set of practices (through DVDs, videos, classes, gyms, etc.), the onus is still on the individual to do with them what is necessary to achieve visible change. Health is to be achieved through self-effort, something to be discussed only with one’s general practitioner (GP), personal trainer, or specialist (Crawford, 2004). To this extent, healthism is a state ideology that has been so pervasive since the 1970s (especially in the United States and parts of South America) that it is, today, virtually taken for granted as part of the social imaginary.
Crawford’s analysis resonates strongly with Michel Foucault’s notion of biopower, which refers to the body as a machine, and its disciplining and optimization of capabilities. Biopower is therefore seen as a source behind the rise of capitalism, and in this context healthism can be associated with capitalism’s demands for high productivity (Foucault, 1976; Rabinow, 1984). Likewise, a Foucauldian approach can help provide nuance to the critique of clinical medical institutions, in particular by questioning assumptions of freedom from the exercise of power—a narrative which tends to dominate the portrayal of the individualized and empowered consumer-citizen who is critical of the medical system (Lupton, 1997b).
Building on Crawford’s work, a number of empirical studies have been undertaken, such as Julianne Cheek’s (2008) study of healthism in advertisements, articles, and government initiatives in Australia; Mary Rysst’s (2010) study of body ideals and bodily practices in Norway; and the study by Trisha Greenhalgh and Simon Wessely (2004) on healthism in clinical situations among the middle classes in London. As noted by Greenhalgh and Wessely, despite the wealth of publications on the impact of healthism, there is surprisingly little on citizens’ perceptions of the phenomenon. Even scarcer in the literature is the link between the lived empirical reality of healthism and its links to broader economic, social, and cultural frameworks.
In closing, we note that while some scholars regard the phenomena of healthism as having the potential for empowerment and political democratization (Ekpe, 2001; Greenfield et al., 1988), notably through the latest wave of technologies for self-tracking and self-monitoring validated by a growing number of celebrities on social media (cf. Askegaard and Eckhardt, 2012), others point out that healthism exacerbates social differences and inequalities and creates a tendency to attribute moral flaws to individuals who have the wrong body shape, especially to the very overweight (Barsky, 1988; Blaxter, 1997; Crawford, 1977; Fitzpatrick, 2001; Yoder, 2002). Furthermore, healthism can distort public health priorities, increase health anxieties through media hype, and increase economic healthcare costs due to escalating demands for unnecessary tests and referrals (Greenhalgh and Wessely, 2004; Moorman and Matulich, 1993: 208).
By integrating the notion of state and control in relation to consumer culture, we are faced with two apparently contradictory yet mutually constitutive tendencies. On one hand, individuals in modern consumer societies are increasingly perceived as enterprising selves capable of controlling and governing their own health (Rose, 1999). Thus, in line with neoliberal discourses, healthy citizens will be ensured their rights through a combination of the market, expertise, and regulated autonomy (Rose, 1998: 162). On the other hand, we find new forms of governmentality emerging from state control that enters the intimate microphysics of human lived experience, which is played out in a context of consumerism that leads to a set of tensions and dilemmas that cannot be captured fully by the theories provided by of Crawford and Rose and which therefore require further analysis.
Context: the Danish healthcare system
The Danish healthcare system consists primarily of a public sector financed by local and state taxes. For all citizens with residence permits, access to healthcare is free of charge, while visits to dentists, pharmacists, and other services require co-payment. The system, however, is undergoing radical change. The focus of reforms has been on patient choice, waiting times, quality assurance, and coordination of care (Strandberg-Larsen et al., 2007: xiii). These changes involve the privatization of the health sector in the form of the rapid expansion of private hospitals and health services and the introduction of private health insurance which took place between 2007 and 2011, when a change of government brought about a momentary expansion of the private healthcare sector. This expansion was later reinforced by the Danish state through the provision of tax benefits for citizens with private health insurance. Furthermore, a reform introduced in 2007 changed the ways in which the state organized healthcare with the number of regional and local units reduced and healthcare responsibilities transferred from the regional to local level. The balance of responsibility—and blame—between the citizen and the state is now in a process of transition in Denmark.
These developments have reconfigured the role of citizens both in relation to their own health and to the healthcare system in general. Rather than being passive patients and recipients of healthcare prevention, citizens are increasingly perceived as active health-seeking individuals. Instead of patients being entitled to free healthcare, they are increasingly expected to prefer to have the choice to pay for individually oriented alternatives and have individual preferences in the management of their own health and well-being. As a consequence of these changes, the notion of health as a desirable product and service to be pursued has taken root, together with an emphasis on citizens’ autonomy, self-management, and responsibility. In the Danish case, we witness a strong welfare state and public sector that goes hand in hand with an increasing emphasis on the notion of the patient as a citizen. The primary role of public authorities is to inform the population about risky and unhealthy behaviors (Vallgårda, 2001: 390). Key focus areas in the current health promotions include reducing tobacco and alcohol use, and improving diet and levels of exercise, which are all choices that are independently exercised by individuals. The health improvement strategy is to help citizens make informed choices and to motivate the population to live healthily. The focus on individual responsibility is accompanied by a fast-growing industry for health enhancing services in the marketplace, which is reflected in the commercial branding of omnipresent “healthy products,” as well as a plethora of self-powered and self-engineered processes of control over the body, for example, dietary regimes, slimming programs, electronic devices for self-tracking.
On 14 November 2011, the Director of the Danish Health Authority, Else Smith (Smith, 2011), announced the rise of healthism among the Danes: I am very pleased about the fact than during the last 5-10 years, managing one’s health has become one of the most conspicuous trends. You find blogs, advertisements and discussion on health that makes a Director of the Health Authority want to shout with joy. To live a healthy life has simply become part of the zeitgeist. (Jyllandsposten)
Her statement is backed up by studies that show that the Danish diet has, to all appearances, become healthier over the last years. According to research, the Danes eat more fish and vegetables than they did 15 years ago (Pedersen et al., 2010: 170). Likewise, in 1964, 15 percent of the adult population in Denmark above the age of 16 years declared that they played sports; in 1987, this number rose to 42 percent, and in 2004 to 59 percent (Fridberg, 2010). Another report stated that the percentage of people exercising increased from 29 percent in 1975 to 64 percent in 2011, running being the most preferred form of sport, with 31 percent running on a regular basis (Laub, 2013). It is clear that health and healthy living in recent years have come to play an important role in the lives of many Danish citizens.
Method
This study focuses on “health” as a construct; furthermore, how citizen-consumers describe the ways in which health emerges throughout their everyday lives is also under investigation. We employed a qualitative approach to the study, framed both by our concerns as described above and also by current discourses on health and food consumption. The participant observation method was applied following the format of the Go-Along interview style as carried out by the first author (D.K.) and field assistant (Kusenbach, 2003). The respondents comprised 25 citizens between the ages of 20 and 60 years. Using purposive sampling, we identified consumption settings with different attributes that covered a relatively broad spectrum from discounted goods food shops to specialist, high-end supermarkets, and recruited five informants in each setting (Gobo, 2008). The aim was to get maximal variation in the group of informants (Gobo, 2008). The informants all identified themselves as Danish, but one had Bosnian roots. Informants were asked to share their reflections on food and healthy living, with informants’ consent given in all cases. Ethical clearance was not required in the Danish setting.
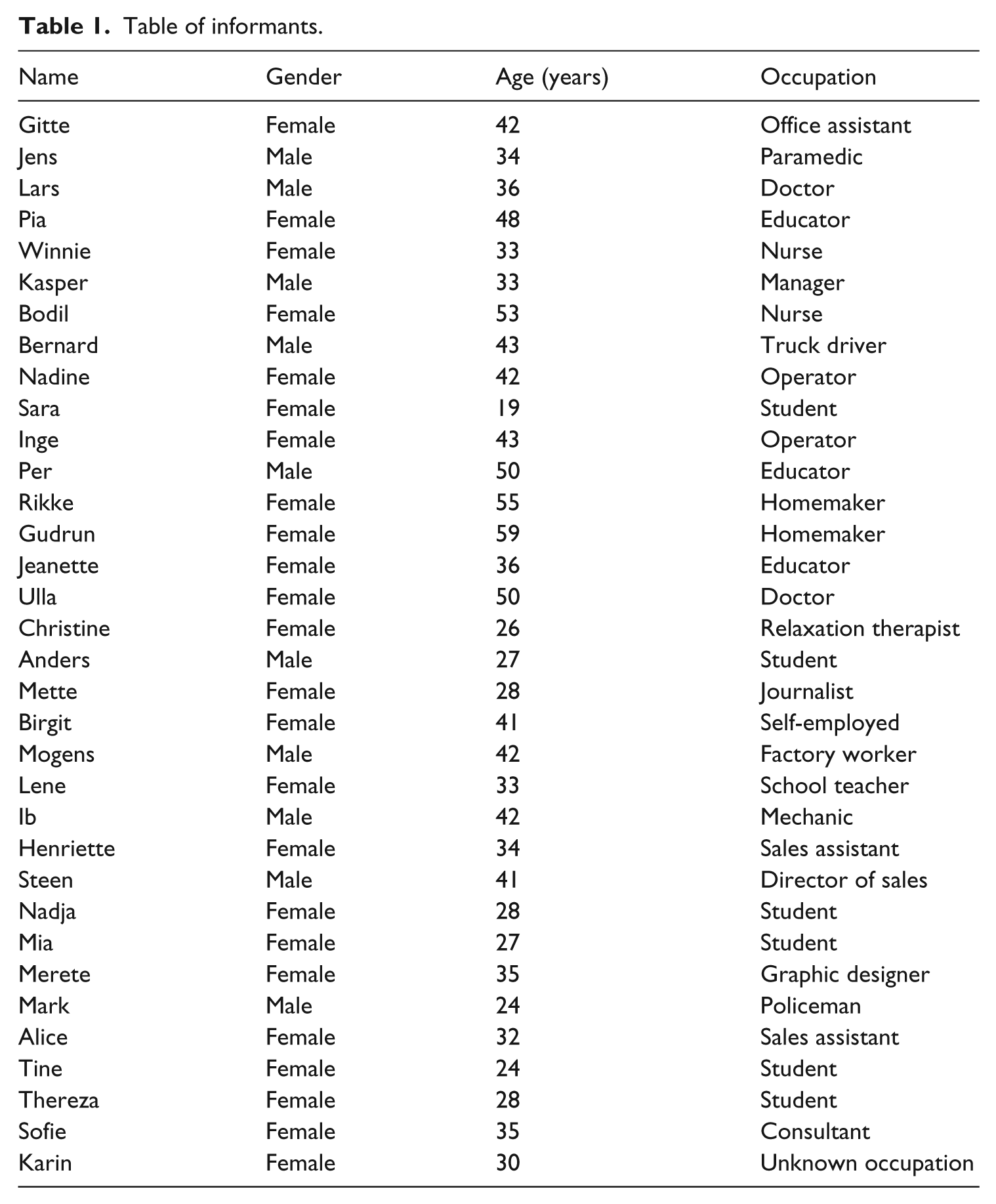
We faced some challenges in the recruitment process, as some informants refused to participate in interviews due to the fact that they did not feel comfortable in doing so, as they felt that they lived unhealthy lifestyles. Therefore, the sample cannot be considered representative of the Danish population, as most informants interviewed consented to be interviewed because they already felt that they were already living a healthy lifestyle and were, thus and thereby, more or less quite willing to share their notions of what health meant to them (Table 1).
Table of informants.
The informants were asked to share their reflections and thoughts on consumption choices they made when shopping. After the shopping session, interviews were carried out in informants’ homes focusing on narratives of food culture, eating behavior, lifestyles, and notions of health (Jackson, 1996; Thompson et al., 1989). The interviews were transcribed and coded according to the procedure suggested by Miles and Huberman (1994). Based on thematic inductive coding, we analyzed how consumer narratives about health practices reflected their perceptions of their health status vis-à-vis that of the general population. We coded clusters of themes that were brought up by the informants or that appeared in field notes based on observations. We also found the engagement in blogs to be salient, especially among young informants. For this reason, a follow-up study was conducted with 9 additional informants recruited from blogs on healthy living. In total 34 informants participated in the study.
Findings: healthism in Denmark
The following analysis of our findings is structured around themes drawn from Crawford’s (1980, 2004, 2006) conceptual apparatus. Crawford’s analytical categories serve as the analytical units that structure the empirical analysis. Specifically, we examine how Danish consumers’ responses to ideologies of healthy eating and behavior highlight Crawford’s thematic contributions to health as a battlefield: health as a super-value and individual security strategies in the market for health products and services.
Healthism as zeitgeist and super-value
The notion of personal responsibility was one of the clearest themes that emerged from the data. A number of respondents were cognitively oriented toward the various state institutions’ preoccupation with, and celebration of, health as reflected in governmental programs and discourses. This theme was reflected in citizens’ narratives of health; for example, in the way they emphasized an increased sense of personal responsibility and bodily self-control and self-management in relation to health and diet. When asked about their perceptions of the importance of healthy living, respondents were quite clear about the “responsibility” they had for their own well-being: as Jeanette, a mother of three children, remarked in a way that resonated with several other informants’ formulations: You simply have to take responsibility and think to yourself that I have to eat something healthy to have more energy. You need to be conscious and take responsibility in order to make the body work.
Jeanette works as an educator, and with a relatively low salary and three children she has to be financially prudent. For instance, she bakes her own bread as it combines her ideals of thrift and healthiness. To Jeanette, being a mother is strongly associated with the role of caretaker, especially in relation to the health and well-being of her family. According to her, health is still all about taking personal responsibility, having awareness, and making healthy decisions which lead to an overall increased level of well-being; therefore, the rational, decision-making self is the pivot of all health choices for her.
Generally, informants were eager to share their reflections in that such choices were very much an individual and private matter, and that they themselves were capable of self-management and self-responsibility. The neoliberal stance that comes through in respondents’ views echoes Crawford’s analysis of healthism as a privatization of the struggle for well-being as well as Nikolas Rose’s (1998) point that health is increasingly withdrawn from state bureaucracies and considered a personal enterprise.
Health was presented as a private and personal responsibility, as well as having a meta-value. An example of how healthy living becomes paradigmatic for experiencing a good life is Robert, a 42-year-old mechanic, who related how a change of lifestyle—in his case by quitting smoking, eating more fruits and vegetables, and exercising regularly—changed his life: I have more energy. I can really feel that I live a healthier life. I have more energy at work; even if I work overtime I still have energy when I come home to exercise, wash the dishes, cook …
Robert recently participated in a test offered by the Danish health authorities to test blood, strength, bone density, fitness, which made Robert realize that in terms of fitness, he was not doing as well as he had thought. Despite the fact that his health indicators were generally fine, he felt motivated to do something about his lifestyle because of what he perceived to be clear signs of being in bad shape. Robert and his girlfriend subsequently became inspired by a self-proclaimed Danish expert in health (a public health promoter and lifestyle expert, Chris McDonald) who claimed that, “it is possible for us to reach our goal on our own.” Robert likes to sum up the benefits of his recent lifestyle changes in terms of having more energy, higher productivity, and a slimmer and more attractive body shape. Hence having a healthy and good-looking body is seen as a realization of the healthy self. It is also interesting to note how Robert explicitly makes the link between individual health practices, bodily discipline, and productivity as a worker. This resonates with Crawford’s link between a focus on health and political economy. Similarly, other respondents linked healthy lifestyles with feelings of happiness, self-confidence as well as the liberation of bad consciences due to the knowledge that one “is doing the right thing.”
Health as a socially dividing practice
We have described some of the implications that arise when citizens seize the zeitgeist of healthism. As citizens increasingly develop an awareness of “healthist” bodily control, monitoring and surveillance become key competences which unfold within individual health security strategies. As also pointed out by Crawford, health becomes a socially dividing practice that informs people’s self-understanding and positioning in the health landscape. The demand for personal responsibility in the marketplace first fuels an acceptance of control over health consumption as the key to good living. Robert remarks, I do think that many people are in a state of denial of what they actually consume. Many of my colleges buy chocolate, not every day, but several times a week, then they go down to the vending machines and get some bags of candy. I personally do not go there myself … And here you clearly see a difference in what people do.
The success or failure of the healthiest ideology becomes a pivotal point for the evaluation of the self and other, and the control or lack thereof in relation to the consumption of unhealthy food as observed in everyday life among peers. As already described, informants judge themselves according to whether their health meets standards which are regarded as having a meta-value for all that is good. Healthism is seen as being potentially empowering for those who prove themselves to be capable of managing their own health in a satisfactory way as in the case of Robert, but it also poses a perennial threat to internal volition and control. As a result, distinctions are drawn between those “morally” responsible citizens who fulfill their moral obligations to steer away from the temptation of the market, that is, commercial providers of health products and services and those who do not.
This morally dividing practice unfolds in everyday life. Food choice and consumption becomes a window through which we glean information not only about moral issues and citizens’ choices, but also of the moral character of citizens. The shopping basket becomes a window into the moral character of a person. For this reason, unhealthy food is often bought and consumed discreetly. Several—especially women—talk about their lack of will power and of not being capable of controlling their food consumption, which makes them feel ashamed and often like “complete failures.” According to this understanding, the body is at the mercy of the will of its owner and, therefore, needs careful training and discipline. Thus, the notion of self-responsibility, control, and self-mastery is seen as a reflection and mirror of the inner self. Therefore, as the perceived capability—or otherwise—to control food consumption and body shape becomes a crucial socially dividing practice and a sign of moral character, which leads to constant anxiety and fear of public judgment. This anxiety leads to the search for a “moral anchor point,” something we will now explore.
Individual security strategies and the “welfare-consumer”
Becoming a “healthy” citizen obviously has many positive side-effects according to societal norms, such as having more energy for work and a better figure. The individual responsibility for health, however, creates certain tensions and dilemmas in citizens’ interactions with their environment and society in general. The focus on individual responsibility, for instance, is often accompanied by skepticism of a conventional (bio-medical) authority. Robert and his wife Henriette, for example, have both recently become interested in health matters, and actively attend talks and read magazines and blogs on the Internet about health-related subjects. This interest, however, creates a dilemma, as Henriette points out: I become really curious when I listen to the news when it says that they have found out something that goes in the complete opposite direction of what we had heard before. Then I think to myself “how interesting.” But at the same time, I also find these contradictory messages really annoying. Then I really don’t know where to check what is really healthy and what is unhealthy. It often becomes just a matter of belief.
As Robert and Henriette want to also rely on guidelines from health authorities, they are caught in a “babble of voices” (Tulloch and Lupton, 2002: 365–367). Health, thus, becomes, as Henriette mentions, a matter of “personal belief.” The informants’ alignment with the ideology of healthism and their focus on health as a private enterprise lead many citizen-consumers to point to their physical well-being and “gut feeling” as their main point for navigation. At the same time, the respondents demarcate clearly between what official rules may recommend and what they believe to be a more reliable barometer of health.
Relying on one’s own instincts is, however, a rather a complicated task as citizens need some knowledge of health in order to organize their health practices and to steer clear of the most obvious and serious health risks. This kind of knowledge becomes even more important as citizens increasingly start to “invent” their own health regime. As Henriette remarked, “Sometimes it makes you so confused. There isn’t any clear proof and it is one against the other unless you go online and Google.” Citizens actively seek to live the ideology of healthism through gaining knowledge, but does this, which is often gleaned anecdotally informally and randomly, count for as much as some consumers seem to think in a complex area such as health? Notwithstanding these concerns, it is clear that respondents were increasingly inventing their own health regimens through searching for answers to their questions online. Some of this behavior was driven by an increasing mistrust in traditional authorities, a theme we explored in greater detail in a follow-up study.
An example of this is Helene, a psychology student and a 28-year-old mother of one child. She presented herself as an extremely health-conscious person, and we found her through an online blog on healthy eating. Due to health problems, she recently initiated a healthier lifestyle, with inspiration from self-help books. Helene’s interest in health started due to panic attacks. After medical tests showed nothing, she then started to search for information online and to read self-help books. Helene remarks that … if you have a health problem, you are the one who knows what is best for you. They [the doctor] might know how to treat you, but do not tell me that you yourself do not know what the problem is. If you get stomach pains every time you eat bread, you might want to have a look at it.
Crawford (2004) underlines that health practices in the healthist ideology are constructed as “individual security strategies” in which control plays a central role in structuring consumption choices (p. 456). In the Danish case, many citizens use the Internet as well as books and the advice of alternative medical dietary practitioners to acquire knowledge of healthy practices. This kind of behavior is characterized as the democratization of healthcare, where numerous attempts to “empower” patients (often using the vocabulary of healthism) result in a situation where patients increasingly act as health consumers or so-called “expert patients” as they actively seek health knowledge, and thus and thereby demonstrate a capacity and appetite for independent decision-making (Cederström, 2009; Henderson and Peterson, 2002; Thanem, 2009). The availability of medical information through a vast number of channels and media, both physical and digital, can potentially turn anyone into their own doctor. This does not mean, however, that medical science loses its power; rather it becomes part of a personalized repertoire for the pursuit of meaning.
Health citizens in the marketplace
The search for an authoritative voice was a general characteristic among this article’s respondents. Hence, sources of authority and normative control appear to be decentered. For Jeanette, who expressed concern about making healthy choices in the marketplace for her and her family, control placed on food by health authorities made it possible for her to make responsible decisions: “as long as there is control it cannot go that wrong. But I might be wrong.” In this way, Jeanette embodies the kind of ambivalence and multiple contradictions already noted previously. On one hand, an individual can trust in the safety net provided by the welfare state and, to a lesser extent, on “expert knowledge,” while the individual may also feel obliged to seek out sources of knowledge for themselves. At the same time, individuals recognize that self-generated knowledge carries risks because there is not the expertise available to evaluate health messages and information, relying instead on “gut instinct” to manage medical conditions. Further complicating this picture is the fact that individuals are themselves suspicious of experts’ opinions. As a last resort, individuals such as Jeanette fall back on the state as a kind of arbiter and appear to want the state to take a more active role in regulating the food industry.
Robert and Henriette also showed some degree of trust toward official health messages when they tried to navigate the complexities of dealing with health authorities and commercial health gurus; however, they generally felt insecure. Asked whether she could imagine consulting an online webpage of health authorities, Henriette replied, “Of course I could do that. Certainly. However, I am more inclined to believe what my acupuncture indicates, to believe more in the alternative than the official.”
What is interesting here, however, is the fact that the state is generally perceived as absent, as an entity that does not control, but merely protects, consumers’ right. Helene complains, When I was pregnant, I was very frustrated when I talked to the health visitor, who told me not to use perfume, and if I smoked or drank I should wait until after breast feeding. Then I thought that I really ought not to drink nor smoke AT ALL when pregnant. You [the health professionals i.e., representatives of the state health care system] should not act as this health visitor and saying, it might best if you abstain. They should say: YOU CANNOT! I thought it showed such a lack of regard for the consequences.
In Helene’s case, this lack of moral commitment on the part of the state is explained by the state lacking moral values. It then becomes difficult for individuals to distinguish between the different voices in the marketplace since they all seem interested in marketing health messages in order to gain economic profit. Good health is in many cases indicated by a resistance to commercially marketed products and to marketers. As health promotion often goes hand in hand with commercial interests—for instance, the branding of healthy food products—the state and corporations are perceived as profit-seeking entities, without having a sense of morality or ideals. An example of this alignment can be seen with the health pyramid. As Helene states, We have a food pyramid in Denmark. This was not made with health in mind. Rather, it was made when thinking about what we can produce, and how we get people to eat it, and what they can afford to eat. Well, let us put a lot of cereal and dairy product at the bottom and tell people that this is what they should eat, because this it is what they can afford. And this is also what we produce. You cannot avoid becoming a bit skeptical, can you?
Another often-cited example was that of an official nutritional expert who was accused of receiving money from the sugar industry. As a consequence, consumers increasingly have to look harder for authentic, honest voices. This search for authenticity represents a movement toward one’s own inner core, toward one’s own senses and common sense (Kristensen et al., 2013). The search for “healthy,” “pure,” and “natural” foods takes place not only within a neoliberal logic based on self-management and self-control, but is also a matter of “resisting” temptations of the market. The navigation of the marketplace is fuelled by a quest for finding an authoritative voice, or a moral compass. In the case of Helene, her frustration with the health visitor led to a search for counter-expertise; thus, she was happy to find an alternative health expert who acted as a “normal human being.” In a similar way, Robert too felt motivated by an alternative health guru. Likewise, his girlfriend revealed how she dealt with issues of health “by asking her acupuncturist” for advice.
These examples underline Crawford’s (2004) point that the healthist’s quest for well-being shapes a self that is receptive to consumerism; hence, health-seekers promote an image of the self that is well-suited to the interests of corporate proprietors and managers in the prevailing culture. We take this point further, as the Danish case shows, by revealing how choices in the marketplace are inscribed in an apparent paradox, as consumers actively use market resources to enhance their well-being while also often expressing a pronounced skepticism of the marketplace. This contradictory double-mindedness—both of mind and of body—creates the paradox that the state becomes associated with a lack of transparency and morality while actors in the marketplace—and specifically markets not governed by the medical industry—are seen as being part of a reliable expert system that acts to counter the uncaring and sometimes arrogant stance of the state; private practitioners thus act as what is perceived as “human beings,” that guide consumers in taking control of their own health.
The social imaginary of health
Based on our observations, health is indeed a central constituent of contemporary social imaginary as described by Castoriadis (1987 [1975]). This is perhaps not surprising given the ubiquity of health references in public-mediated discourses. However, public discourse cannot be considered a cause in a traditional sense, as in a linear causation model, since it is in itself a product of such imaginary. The centrality of health in contemporary social imaginary must be seen in the broader sense of social changes in modernity. Here, we note two related processes, namely, a process of secularization which reorients existential focus and value toward the life on earth rather than the afterlife, and the modern reflexive self and its life-project.
The combination of secularization and the late-modern self as a project involves a reconfiguration of the Cartesian dualism of mind and body. Instead, the combination gives rise to a holism including the mental as well as the bodily self and the belief in a high correspondence between the two. This holism is visible in its positive features in terms of the critique of medicalization as an overly somatic approach to good health (Lupton, 1997b) and the concurrent rise of holistic health discourses. However, there are also negative outcomes of this in many ways. One example is the current, and much debated, tendency to stigmatize obese people in terms of their flawed personalities (e.g. Gard and Wright, 2005; Solovay, 2000). Another is the contemporary tendency to attach a medical diagnosis to all kinds of mental states, something which has been criticized in a Danish context by Brinkmann and his colleagues (Brinkmann, 2010).
The notion of risk also came up strongly for respondents, another finding that confirms Crawford’s conceptualization of risk. As he observes, risk has become central to the understanding of the modern social imaginary of health (Skolbekken, cit. in Nettleton, 1997). Risk management and risk reduction and management have become the ultimate measures of success of the mastering of one’s own health. As outlined, our informants oscillate between making references to “objective” determinants of health and “subjective” determinants of well-being in their accounts of risk management practices (Petersen, 1997), with the latter indicative of what is commonly referred to as a holistic approach to health.
Neither the state nor the public medical system functions as a reliable moral compass for our informants. This is because, first and foremost, the public system’s alignment with classical medical and somatic approaches to health is represented by what critics call the medicalization process (Lupton, 1997b). At the same time, the state’s health policies are driven by a hidden agenda that results in the health practices of the population serving the economy more than the people themselves. Consequently, the neoliberal state generates distrust by considering the population first and foremost as a workforce, an ethos underlined by repeated references to the “costs” of a non-productive population, such as retirement age (must be raised), productivity (must be improved due to global competition), educational systems (must be more efficient), and programs (must qualify for the needs of the labor market). But, as alluded to by our informants, the state also arouses suspicions that the advice it gives about what to consume in terms of food promotes market opportunities for the national food production sector rather than consumer-citizens’ health and well-being.
As a result, consumers turn to their own embodied experiences (cf also Kristensen et al., 2013), to peers willing to share their personal embodied experiences and, not least, to a plethora of alternative market agents that are seen as relatively innocent and trustworthy and act as a moral compass in comparison to both the state and the market agents. This movement corresponds to the “progressive rationalization of the mythic” (Durand, 1993) and the institutionalization of new social forms based on the social imaginary of health and risk. The contemporary social imaginary of health is thus paradoxical in its effects since it not only promotes new risk narratives that are ultimately supposed to provide consumer-citizens with better control over their own life through practices of actualization and avoidance (do’s and don’ts), but also contributes instead to uncertainty produced and promoted through a variety of risk narratives and agendas (Petersen, 1997). We argue, therefore, that the contemporary social imaginary of health therefore produces citizens who are health consumers that navigate a complex mediascape (Appadurai, 1990) while at the same time negating, or fundamentally de-securitizing, their need for morally and medically efficacious care and information. As a consequence, individuals seem to be suspicious of the standard institutionalized system of public medical institutions while at the same time still want it to deliver the kind of safety and assurances they seek. In the meantime, citizens try to manage their health by seeking out alternative health market agents.
Conclusion and future research
In this article, we have explored the social imagery of health by building on Crawford’s analysis of neoliberal healthism. By so doing, we have explored and analyzed Crawford’s concept of healthism, as well as the implications of healthism from the perspective of lay health knowledge. In the Danish context, health has become a super-value for what is good in life. Health is an identity marker: “I am who I am because I am healthy/I am healthy because of who I am” (Crawford, 2004: 414). This turns health into a private and individual enterprise and a social battlefield, but only partly.
Our findings show that “healthism” is a multi-faceted construct with individual, and also statist or institutional, elements. While the state sends out public messages exhorting citizens to behave in certain ways or, at the very least, attempts to inform them of the dangers of certain kinds of health-related behaviors, these are merged with messages from commercial brands and private health gurus, all contributing to an overall omnipresence of health. In this context, citizens are highly, even painfully, reflexive about their dietary choices and habits, and self-management and control of body, health, and consumption. This corresponds to what Deborah Lupton (1997a) calls the “rational, reflexive self,” a self who acts in a calculated manner, who constantly monitors and evaluates their own health and who is skeptical of traditional sources of expert knowledge. Ideologically, healthism appears to be a socially divisive practice because it sets new—and also arbitrary—norms of citizen psychology, thereby increasing the repertoire of pathologies. In this respect, our article supports some of the existing criticisms of healthism, namely, its potential for identifying victims or blaming them, as well as generating moral judgments upon those who are perceived as unwilling to obey those norms. These processes, in turn, may lead to social inequalities and stimulate a spiral of control and anxiety.
Our findings, however, also showed the flip side of the notion of the rational, self-reflexive self, and pointed to the fact that the healthist self is a template that seems to give rise to a set of dualisms and tensions that lead to the reconfiguration of traditional authority, transferring power from the state to actors in the marketplace. The doctor–patient hierarchy is put under erasure while consumers themselves search for alternative sources of intelligence and help in order to achieve what is socially idealized as being healthy. A key consequence of our research can be seen in how concerned citizens manage to overturn the traditional hierarchical relationship between doctors-as-experts and patients as non-experts. This distinction is seriously challenged in our findings, with a form of “counter expertise” set up in response to decisions that were previously socially accepted without question in the case of healthcare information and provision. It is interesting to note that this counter-expertise is often found on the marketplace and perceived as a consumer-to-consumer relationship. Consequently, what has not been described by Crawford is how the marketplace also offers a reduction of the spiral of control and anxiety, through the embodiment of the counter-expert, who serves to reduce risks in the marketplace.
Theoretically, our initial findings showed that citizens simultaneously experienced both agency and helplessness. This highlights the fact that hitherto divergent sets of literatures which posit citizens’ autonomy, on one hand, and victimhood, on the other, as being less accurate than they first appear when viewed in isolation. Instead, both constructs exist as a continuum and, as our findings show, often mutually co-produce one another. In a number of contexts, sources of authority and normative control appear to lack centrality and a subject: food labels, dietary guidelines, and so on are not directly attributed to a particular person or agency but, nevertheless, exercise power over the individual’s psychological beliefs. Citizens appear to accept a high level of psychological distress as the price to pay for good health and well-being, a phenomenon which has yet to be studied in depth.
As a result of the proliferation of risk consciousness, another dilemma presents itself to healthist citizens, namely, that healthism presupposes its opposite: pathology. In other words, the more illnesses that are defined by society, the more the ideology of healthism thrives. As argued by Brinkmann (2010), modern societies are increasingly “diagnostisized,” which means that more and more types of behavioral, mental, and bodily symptoms are subject to some kind of (more or less authorized) medical diagnosis. We would argue that this process is a logical consequence of, and further promoter of, healthism. Furthermore, social media and the consequent democratization of medical expertise mean that this pathologizing tendency is manifested in the erosion of trust in government. This fuels a trust in actors in the marketplace who are often paradoxically seen as having been “removed” from the “evilness” of the market. What is even more interesting is the fact that state protection actually invokes a perception that “it cannot go wrong” as it safeguards its citizens against fraud.
As the welfare state retrenches some long-standing services, citizens of these countries have to negotiate a path between reliance on the state, on one hand, and more entrepreneurial behavior, on the other. It may be surmised that the increasing tensions between state provision and self-directed health-seeking behaviors will only increase in years to come and should be better understood by consumer researchers, policy makers, and health professionals.
Future research could include a much more detailed study that makes cross-national, cross-cultural comparisons among a range of demographic, economic, and ethnic groups. In this regard, it would be interesting to understand how different nationalities perceive the role of their national governments, corporations, and private health actors in monitoring, regulating, and ultimately influencing individuals’ behavior. How a deepening of the “DIY” framework of healthism affects state provisions in future and whether consumers are being persuaded by conflicting notions of healthism as they search for “what works” and “what is best” are also questions which should be addressed. Since healthism is not global yet in scope but is, nevertheless, in the process of being globalized, the emergence of healthism in new social contexts provides an excellent opportunity for insights into how this particular social imaginary alters consumer-citizens’ consumption proclivities according to their capabilities for conceptualizing and performing healthiest behaviors in the context of what they hear, see, believe, or choose not to believe in their respective societies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study presents results from the project “Health Branding” funded by the Danish Strategic Research Council.