
Abstract
This article considers conceptual frameworks and models applied in research about the multiple relations between human contact with natural environments (specifically green public spaces), diverse kinds of human activities and uses of those spaces, and effects on physical and mental health. Conceptual frameworks are tools for thinking about such complex subjects. Conceptual models represent the multiple relations between key factors and variables. These models can be used to represent the mutual interactions between the core components of environmental conditions of specific green public spaces, the main kinds of human activities in those settings, and various impacts on health. A literature search showed that the authors of various conceptual models used a metaphor of pathways to represent relations between explanatory variables by linear cause–effect relations. Mutual interaction between key variables and feedback loops between different components of the model are rarely included. Hence, it is argued that these models do not represent the complexity of real world situations. The authors propose a systemic conceptual framework founded on core principles of human ecology. The proposed conceptual framework and model have been formulated during and after an EU 7th Framework project about the ‘‘Positive Health Effects of the Natural Outdoor Environment in Typical Populations in Different Regions of Europe.”
Keywords
Introduction
The potential benefits of green public spaces on health are multiple given the numerous direct and indirect relationships between environmental factors and human health (World Health Organization Regional Office for Europe, 2016). During the last three decades, numerous scientific reviews have documented the accumulated evidence from empirical research about the relationships between green spaces, human activities in those spaces and effects on health and well-being (Bedimo-Rung et al., 2005; Bowler et al., 2010; Croucher et al., 2007; Greenspace Scotland 2008; Hartig et al., 2014; Health Council of Netherlands and Dutch Advisory Council for Research on Spatial Planning, Nature and the Environment, 2004; Konijnendijk et al., 2013; Lachowycz and Jones, 2013; Laille et al., 2013; Lee and Maheswaran, 2010; Manusset, 2012; Morris, 2003; Nilsson et al., 2011; Northbridge et al., 2003; Tzoulas et al., 2007; World Health Organization Regional Office for Europe, 2016). Many contributions share an assumption that positive health outcomes can be derived from contact with ‘natural’ environments including public parks, urban forests, and botanical gardens.
Analyses of 12 scientific reviews identified a common causal mechanism logic shared by researchers in order to identify the direct pathways (and sometimes the mediating factors) linking contact with green public spaces, human activities in those spaces, and quantitative or qualitative health effects (Zufferey, 2015). The analysis also found that researchers rely heavily on proxy measures, especially those concerning access to green public spaces, which are often calculated by the distance between place of residence and the nearest green public space. Too few empirical studies record the actual size, land cover and biological components of these spaces, or the amount of time spent in these spaces, or the range of human uses that occur in them. In addition, the lack of systematic research about which components of green spaces impact positively or negatively on health (e.g. diversity of flora and exposure to allergens) has hindered the formulation and application of a broader approach. The shared reasoning of much recent research is rarely complemented by considerations of how the health of individuals and population groups influences their motives to access and use green public spaces (e.g. shift workers, handicapped persons). Consequently, much ongoing empirical research on this complex subject is ignoring the health and livelihood of many people. There is a need for a fundamental rethinking of the conceptual frameworks and models proposed and applied on this complex subject.
This article summarizes the aims of conceptual frameworks and models for thinking about complex subjects, such as the interrelations between human activities, green public spaces and human health and well-being. The added value of conceptual models and frameworks is their capacity to represent the components of real world situations according to patterns and interrelationships that are not visible (Dyball and Newell, 2015). A crucial challenge is to ensure that the core components and the multiple interactions between them are taken into account. Today, key research questions go beyond the current academic discussion about whether contact with ‘natural’ environments influences health, to analyse how the conditions of specific components of natural environments (e.g. biodiversity of flora and fauna in public gardens; size and ground cover of public parks) influence health (Pleasant et al., 2013). Furthermore, the health and well-being of individuals and groups can be considered as a resource that enables or hinders physical activity or social contact, rather than only being considered as an outcome of human behaviour in public green space (World Health Organization, 2016).
This article briefly presents our analysis of five conceptual models (as defined by their authors) that have been selected from a limited number of contributions in recent decades. These examples are considered to be representative of the concepts and thinking used by a large number of researchers in several disciplines, including biology, epidemiology, medicine, psychology, sociology and public health. Despite the different disciplinary education and training of these researchers, the synthesis section of this article shows that their contributions share a common aim of identifying and representing the pathways linking contact with natural environments, human behaviour and health effects.
The final section of this article presents a broader, systemic framework and model based on the principles of human ecology applied to people–environment relations (Lawrence, 2001). This proposal is currently being reviewed as the empirical results of an EU 7th Framework project (from 2012 to 2015) about the ‘Positive Health Effects of the Natural Outdoor Environment in Typical Populations in Different Regions of Europe’ (PHENOTYPE) are published in peer review journals (e.g. Dadvand et al., 2016; Gidlow et al., 2016; Nieuwenhuijsen et al., 2014; Ruijsbroek et al., 2017; Triguero-Mas et al., 2015). These results confirm the need for a systemic approach that accounts for the biological, cultural, ecological and geographical characteristics of green public spaces, the diverse kinds of human uses of these spaces, and both the positive and negative health effects. The empirical results of this large interdisciplinary project in four European cities show that any conceptual model should account for moderating factors, such as seasonal variability in weather conditions, seasonal change to the biological components of specific green public spaces, and change to human activities in those settings. In addition, cultural customs and predispositions concerning people–environment relations are significantly different across the European region and they have strong historical precedents which should be acknowledged. These kinds of real world differences have rarely been the subject of empirical research.
Methodology
This article examines how researchers from diverse disciplines conceive and represent the interrelations between human contact with green public spaces, individual and collective activities therein and physical and mental health. There are multiple relations between these subjects and plausible influences too. Causation interprets how and why mutual interaction can lead to change, thus explaining how and why personal contact with green public spaces influences physical and mental health. In her contribution, Kreiger (1994) argued for a rethinking of the epistemology of multiple causation. She noted that the metaphor and model of a ‘web of causation’ was originally used in the 1960s to consider how host, agent and environment interact. Kreiger criticized contemporary research that only identified causal influence between a few selected factors while ignoring the broader societal context that could influence health and disease. This kind of epidemiological research is an example of methodological individualism that she called ‘biomedical individualism’ (Hodgson, 2007) which she challenged. She proposed an ‘ecosocial’ metaphor accounting for ecological and social factors, thus predicting some principles of ecological public health (see later).
The authors of this article note that Kreiger’s criticism is valid for much recent research that applies methodological individualism because they do not define or measure environmental context, or account for human agency and social structures (Giddens, 1986). This kind of research is represented on the left side of Figure 1, while an alternative kind of research founded on systems thinking and principles of human ecology is shown on the right side given that it enables interpretations of multiple causation.
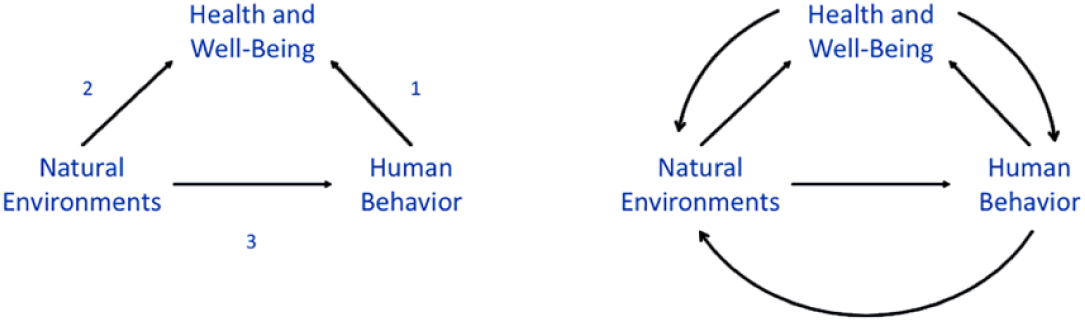
The relations between the positive health impacts of certain human behaviours (physical activity, social interaction, leisure) on health (shown in 1) have been established by a large number of empirical studies. The positive impact of nature on human health (shown as 2) has been assumed and studied by numerous uncoordinated studies in the social and psychological sciences but the accumulated evidence remains unclear. There is some coordinated empirical research (shown as 3) that has explicitly shown that natural environments are the catalysts of health promoting human behaviours that have positive health outcomes. An integrated conceptual framework (shown on the right) should replace the piecemeal approach (shown on the left) that has dominated contributions to date because it enables interpretations of multiple causation.
We interpret conceptual frameworks as sets of assumptions, beliefs and concepts that are used implicitly or explicitly to represent real world phenomena. One application of two different conceptual frameworks is shown in Figure 1. This figure includes two diagrams: on the left hand side, the relations between the concepts of human activity, green public space and health are positioned such that the relations between any two concepts are paired. Hence, this diagram represents a conceptual framework of linear causality between any two but not all three concepts. The majority of research on the subject of this article implicitly or explicitly adopts this conceptual framework (see later). In contrast, the right hand side represents the mutual interaction between the three concepts as a tripartite system. This conceptual framework founded on systems thinking applies key principles of human ecology (Lawrence, 2001). In essence, although the two diagrams have exactly the same components, the interrelations between the components are fundamentally different. This article shows that it is rare for the diagram on the right hand side to be applied in contemporary research in this field.
Bibliometric search
A search of electronic databases was undertaken in 2015 to identify published articles, books or reports that address the relations between contact with green public spaces, individual and collective activities, and impacts on health and well-being (Zufferey, 2015). These databases used were MEDLINE, Google Scholar and Web of Sciences. The subjects and keywords used for the literature search were green space, health, human behaviour, physical activity, social contact, relaxation and/or well-being. The selected publications were chosen according to criteria including the date of publication between 1980 and 2014; the language of publication in both English and French; and the inclusion of a conceptual framework and/or model. The period from 1980 to 2014 was chosen owing to the increase in research about the influence of natural environments on health from the 1970s, particularly in the field of environmental psychology, including the contribution of Kaplan and Kaplan (1982) who developed the concept of restorative environments. The literature search identified only a dozen articles in English that explicitly proposed conceptual frameworks and models. A few additional publications in North American sources were identified by interpersonal communication.
The five selected contributions illustrate different interpretations of green public spaces that are currently used in theoretical and empirical research involving conceptual frameworks and models. In particular, their geographical size and scope includes shared green spaces in housing estates, public parks in urban neighbourhoods and towns, urban forests and green infrastructure (e.g. urban and outer-urban green networks that function as biological corridors). In the majority of selected articles, these different kinds of green public spaces are interpreted as ‘natural environments’. In contrast, Northbridge et al. (2003) interpret green public spaces in urban areas as components of the built environment. Finally, the five contributions do not include private gardens, or plant containers adjacent to residential buildings (e.g. on balconies), or contributions related to the design and construction of green buildings with vegetation on roofs or walls.
Conceptual models: interpretations, types and examples
The value of conceptual frameworks and models as aids to thinking about complex subjects gained importance with the development of systems theory from the 1960s (Jabareen, 2009). Uses of conceptual frameworks have been challenged by some researchers who argue that they impose a bias that restricts naturalistic inquiry in social research, especially ethnographic research (Strauss and Corbin, 1990). In contrast, other researchers have argued that conceptual frameworks can be used to counteract the influence of cultural, social, or perceptual biases of researchers (Sbaraini et al., 2011). The authors of this article argue and show how conceptual frameworks are used implicitly or explicitly by researchers to interpret the causal relations between components of people–environment systems in green public spaces.
A conceptual model refers to a description or representation of a phenomenon. They can be derived from literature reviews, observational studies, or other kinds of empirical research. Hence, alternative conceptual models of specific subjects can coexist as shown in Figure 1. According to Knol et al. (2010), conceptual models differ in their level of complexity according to their purpose, whether ‘structural’, ‘relational’ or ‘operational’. The formulation of each kind of model requires the conceptualisation and representation of a systemic framework including several factors and variables and the interrelations between them. The key factors and variables can be identified from scientific knowledge with the intention of replicating previous empirical results, or validating new theories.
Conceptual frameworks and models can interpret people as either active or reactive subjects. Human agency is a concept applied in disciplines, including economics, psychology, sociology and philosophy (Giddens, 1986). It is used in our research to interpret whether people are considered as active agents capable of making their own choices about contact with others, uses of green public spaces and health promoting behaviours. Our interpretation recognizes that factors such as age, gender, socio-economic status and religion limit personal choices. Hence, conceptual frameworks and models should account for individual agency and social structures in precise situations.
A conceptual model is a theoretical conception that can be tested empirically (Morris et al., 2006). Thus, a model can be tested and modified. In the domain of public health, operational conceptual models commonly consider the health system, specifically the various structures, institutions and resources, and those policies and programmes that could influence health at the national, community or household level. An operational conceptual model can be useful to assess the impact of specific interventions on one or more variables at different levels (e.g. the individual, community or national levels; or the provision and the maintenance of green public spaces at the neighbourhood or regional level). The Driving Force, Pressure, State, Exposure, Effect, Action (DPSEEA) model, for example, which is endorsed by the World Health Organization, is being used to propose indicators for measuring objectives defined in the WHO-EURO Global Plan of Action for Children’s Health and the Environment (Morris et al., 2006). The DPSEEA model has subsequently been amended to include contextual factors in which people–environment relations are embedded (Reis et al., 2013).
Conceptual mapping
Concept diagrams or maps are visual representations of a subject. Concept mapping is a tool for developing and presenting conceptual frameworks by illustrating key components: the concepts and their interrelationships (Dyball and Newell, 2015). Concept maps enable researchers to clarify the content of their conceptual frameworks, and they help to develop thinking about the relationships between state variables and the interactions between them including feedback loops.
The components of people–environment systems interact mutually to influence each other as Oström (2009) explained in her pioneering research. Systems thinking recognizes that if contact with natural environments leads to positive health effects, then the change in an individual’s health can influence subsequent contact with natural environments. This circular influence is known as feedback, and it is represented graphically in conceptual models by causal loops between the components of the system. When feedback loops amplify change it is called reinforcing or positive feedback (leading to accelerated growth). When the feedback loops oppose change, it is called a balancing or negative feedback (establishing dynamic equilibrium). Feedback causation, rather than linear causation, is the dominant driver of people–environment systems.
Newell and Siri (2016) illustrate how and why low order system dynamics (LOSD) models are useful tools that enable understanding of the complex and dynamic nature of urban health subjects. They define LOSD models as those having a few state variables (e.g. not more than 5), able to illustrate non-linear effects caused by reinforcing (positive) and balancing (negative) feedback, while focusing on the endogenous dynamics within clearly defined boundaries. This type of model can be created in order to provide a shared understanding of people–environment systems. This reflexive process can replace instrumental reasoning because the latter produces linear cause–effect relations between a few selected variables while ignoring others.
The next section of this article reviews whether conceptual models have been applied in research on the interrelations between human contact with green public spaces, human activities in those spaces, and effects on health and well-being.
Conceptual models of contact with green spaces and health effects
Researchers adopt concepts and conceptual frameworks in order to achieve their theoretical and empirical studies. Instrumental rationality is commonly used, as Sen (2002) noted, to efficiently study a subject, such as the effects of contact with green public spaces on physical and mental health. It posits that those factors that can explain this relationship can be considered as variables that are controlled in precise situations. Our analysis of the conceptual frameworks and models shows that researchers commonly apply a metaphor of pathways that represent causal relations between contact with green public spaces, and health outcomes. In all the cases studied, the path begins with contact with green public spaces and it ends with health outcomes. Some authors include modifiers and mediators along the pathway.
The five examples of conceptual models discussed in this section are founded on reviews of published reviews of theoretical and empirical research presented by Northbridge et al. (2003), Bedimo-Rung et al. (2005), Tzoulas et al. (2007), Lachowycz and Jones (2013), and Hartig et al. (2014). We do not summarize the findings of each review, but concentrate on the diagrams that illustrate conceptual models. Each of these models is meant to represent those key factors and state variables, their interrelations, and their influence on human contact with green public spaces, human activities in those spaces, and effects on individual, group or population health. Therefore, it is interesting to compare these conceptual models, consider differences between the state variables they identified, as well as the proposed interactions and processes between them.
Environmental conditions and social determinants
The conceptual model proposed by Northbridge et al. (2003: 559) includes macro-level environmental and social factors; meso-level or community level factors about the societal context including specific characteristics of the built environment, micro-level or interpersonal proximate factors including behaviour, stressors and societal conditions; all leading to effects on health and well-being at both individual and population levels. This model is a sequential one that begins on the left hand side and represents plausible pathways across each of the four levels. Although some interactions between adjacent levels are proposed this is a mechanistic interpretation not a systemic one.
The model, shown in Figure 2, represents three key domains which ‘contain the fundamental factors that underlie and influence health and well-being via multiple pathways through fundamental access to power, information and resources’ (Northbridge et al., 2003: 560): These three domains are the natural environment which includes ‘topography, climate and water supply’; macro-social factors ‘including historical conditions, political and economic orders, and human rights doctrines’; and inequalities including ‘those related to the distribution of wealth, employment and educational opportunities, and political influences’. Although historical conditions prescribe cultural predispositions, this model does not include a temporal perspective that accounts for seasonal variability in the characteristics of public green spaces, or weather conditions, or changes in human behaviour. Therefore, significant differences in the state of green public spaces (e.g. flora and fauna) and hours of daylight, sunlight, precipitation and ambient air temperature are not explicitly taken into account even though they can explain changes to environmental conditions and human behaviour.
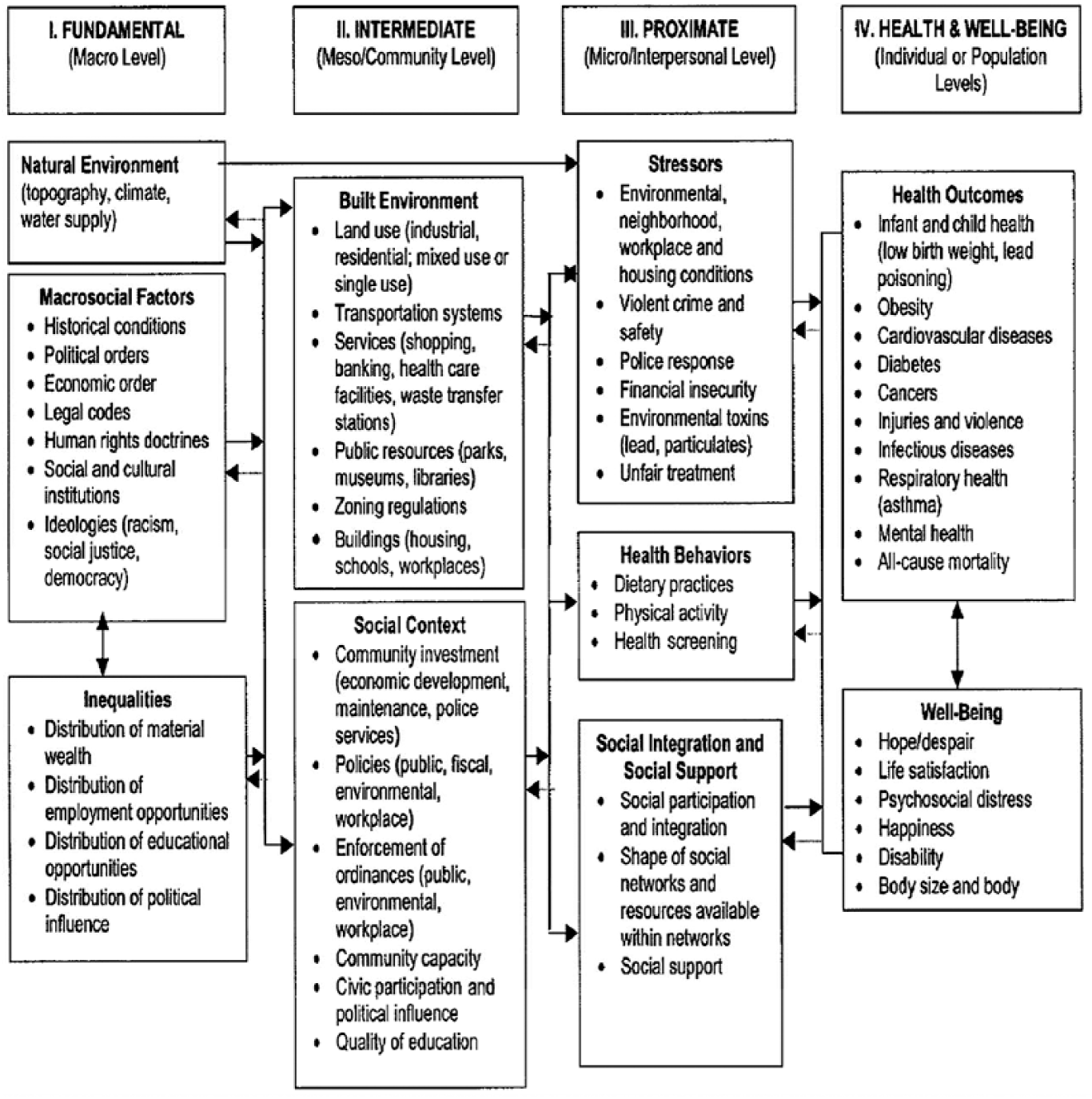
The title of this model is ‘Social determinants of health and environmental health promotion’. The model was presented in an article by Schulz and Northridge (2003).
This model has a broad interpretation of state variables that can influence health. The authors give limited attention to the constituents of green spaces which are considered within the built environment, not the natural environment. In addition, zoning regulations are classed with other factors in the built environment at the meso-community level, but they could have been grouped with legal codes at the macro-level.
The multiple levels of this model represent relationships between and across various domains, as well as different levels of human experience. However, health and well-being are only interpreted as outcomes rather than a resource that can influence human behaviour in public green spaces. The model could have been systemic if interaction and feedback loops between all four levels and their state variables had been included. Despite this limitation, this contribution is broader in scope and content than others published since 2003. This suggests that there is a lack of accumulated knowledge during the last 12 years.
Public parks and physical activity for health promotion
Bedimo-Rung et al. (2005) discuss how public parks can influence population health by ‘mechanisms’ that relate their environmental characteristics to physical activity. The authors are researchers in public health, medical and health sciences. They are among many who have studied the health benefits of regular physical activity in North America and other countries.
The starting point for the authors is that health promotion interventions that were proposed to change individual human behaviour (e.g. promote regular physical activity in a sedentary population) have not been wholly successful. The authors accept the proposition that interventions intended to promote access to public green spaces are not only feasible but can lead to positive health effects. They note that, since the 1980s, a large volume of research on leisure has studied the environmental, economic, social and individual benefits of recreation in parks, whereas physiological health outcomes stemming from physical activity have not been systematically measured. However, a number of publications before and since 2005 have analysed these relations (Biddle and Asare, 2011; Fox, 2007; Paluska and Schwenk, 2000).
The authors propose a conceptual model that considers ‘park environments in terms of their benefits, and more specifically, proposes the linkage between physical activity and specific park features’ (Bedimo-Rung et al., 2005: 160). Bedimo-Rung et al. (2005) present a conceptual model, shown in Figure 3, which is derived from a behavioural and epidemiological framework that represents linear pathways and sequences between variables. The lowest level comprises sets of antecedents including individual characteristics and the structural characteristics of parks, positioned at the bottom of the model. Then the linear pathway shifts upwards to an intermediate level which comprises state variables for human behaviour (e.g. access to the park irrespective of a specific use and activities in the park). Finally, the pathway reaches the highest level of positive effects at the top of the model including physical health benefits as well as psychological, social, economic and environmental benefits.
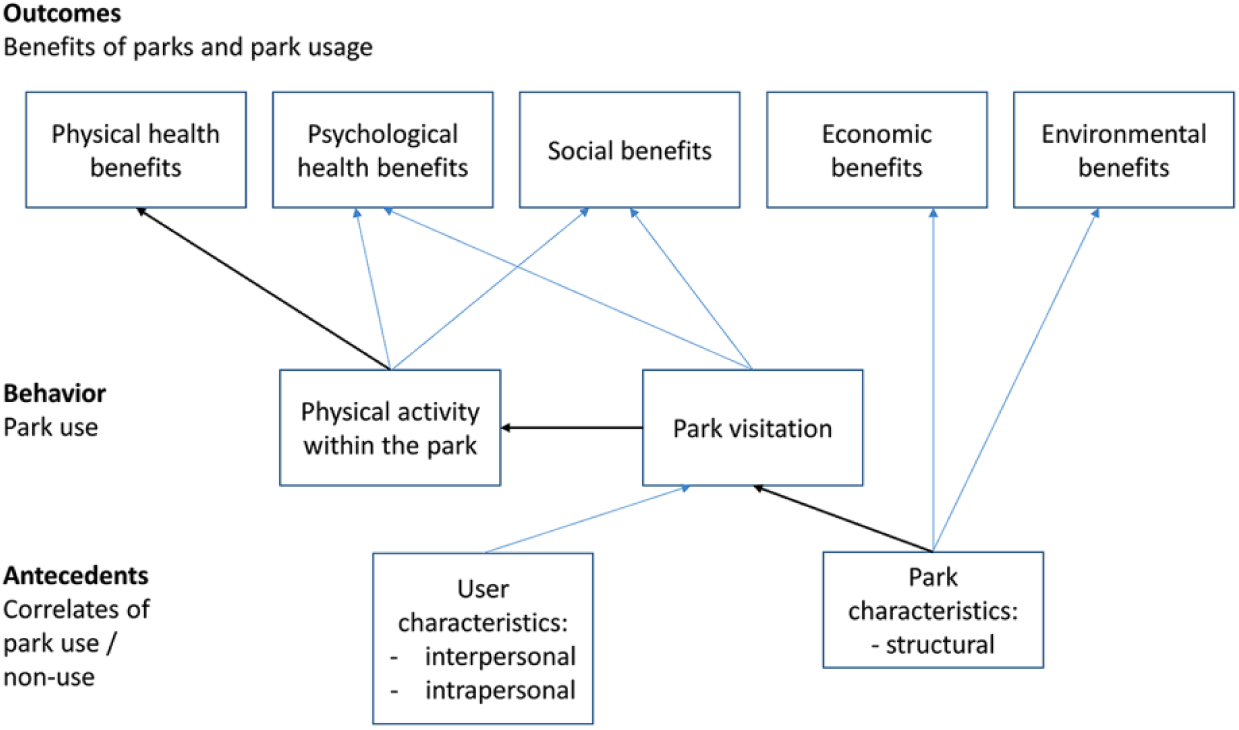
The hierarchical model proposed by Bedimo-Rung et al. (2005) redrawn by the authors.
This model presents major and minor pathways that represent linear cause–effect relations between the environmental characteristics of parks, the personal characteristics of park users, visits to parks, physical activity in parks, and a number of benefits including physical health. It is an example of instrumental reasoning not systems thinking. In contrast to the previous model, this representation of the health of park users does not incorporate the contextual conditions (e.g. the geographical, political and social environment) in which public parks and individual users coexist. It does not account for historical precedent, and it does not include a temporal perspective. Health is considered only as an outcome rather than a state variable that can influence human behaviour; there are no inter-linkages or feedback loops between health benefits and user characteristics; indeed, there are no feedback loops at all.
This model is a hierarchical one. It is mechanistic and only represents the linear causal relations between characteristics of parks, physical activity and health benefits. Hence, adaptive or reinforcing behaviours of park visitors who may use green spaces for a number of reasons are excluded. Thus, this model cannot account for real-world situations in which people–environment relations are dynamic and change owing to the role of human agency and contextual variables. This type of narrowly defined conceptual model ignores mutual interaction, feedback loops and cumulative effects.
Green infrastructure, ecosystem health and human health
Tzoulas et al. (2007) propose a conceptual framework of the associations between green infrastructure in urban areas, ecosystem health and human health. This framework is derived from a literature review of definitions, interpretations and applications of the concepts of urban and peri-urban green spaces (e.g. green infrastructure), ecosystem health and human health. The authors discuss the human ecosystem model applied to analyse socio-ecological systems in urban areas. They claim that many contributions do not identify relationships between natural ecosystems and public health. Although the Millennium Ecosystem Assessment (2003) addressed this shortcoming by explicitly linking ecosystem services, human well-being and socio-economic factors, the interpretation of well-being does not account for the physiological and psychological dimensions of human health.
The proposal by Tzoulas et al. (2007: 73) shown in Figure 4, comprises two main interrelated parts, each having several components and subcomponents. The top part represents three main components of ecosystems with two-way arrows representing mutual interactions between state variables of green infrastructure, ecosystem functions and services, and ecosystem health. Collectively, all these variables constitute the context for public health shown in the bottom half of the figure. This lower half includes four main components with two-way arrows between their state variables: socio-economic health, community health, physical health and psychological health.
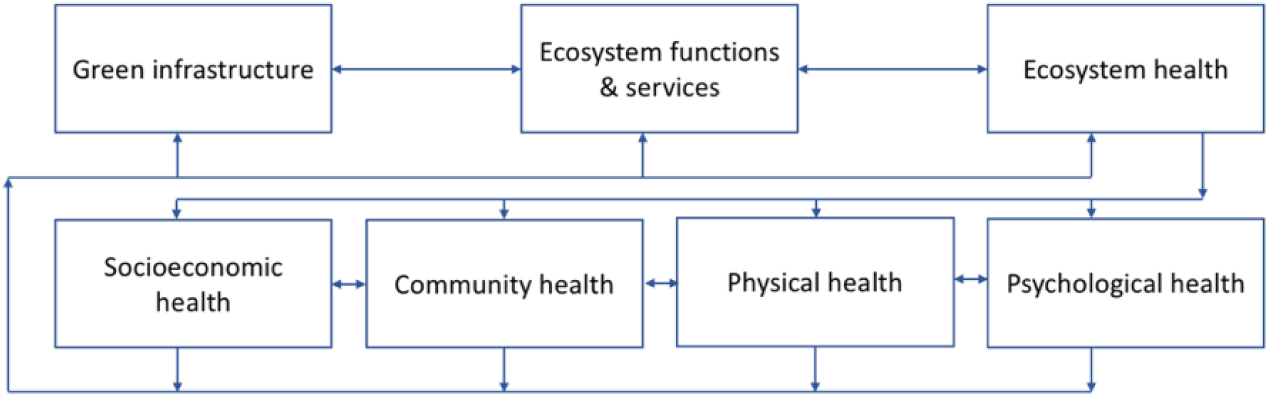
Conceptual framework integrating Green Infrastructure, ecosystem and human health redrawn by the authors. The framework has two main components separated by two-way arrows. The top half (natural and human-made ecosystems) has three interrelated boxes and the bottom half (human health) has four interrelated boxes each with numerous parts not shown here but included as a list in the original. Two-way arrows indicate mutual interactions between the components and their parts.
The model proposed by Tzoulas et al. (2007) illustrates the complexity of multiple relationships between ecosystems and human health. However, the kinds of relationships between the components, including feedback loops, are not mentioned. In essence, the contribution by Tzoulas et al. (2007) is a compilation and aggregation of seven sets of components and subcomponents that represent natural ecosystems and human health. It is crucial to note that the authors do not interpret health only as an outcome but as a state or condition that can influence the way people interpret and use natural environments. However, their interpretation does not integrate macro-level factors and state variables that were explicitly addressed by Northbridge et al. (2003). In particular, cultural, historical and political dimensions associated with policy definition and implementation are absent. This is another example of instrumental reasoning that excludes pertinent variables necessary for an understanding of multiple causation.
Influences of mediators and moderating factors
Lachowycz and Jones (2013) challenged the majority of empirical studies about the tangible effects of the provision of public green spaces on the health of those who use these spaces. The authors argued that the divergent results of empirical studies can be largely attributed to the absence of a shared conceptual framework. They addressed the need to improve current knowledge about ‘the potential mediators’ as well as the ‘plausible moderating factors’ that can influence those ‘pathways and mechanisms’ linking green spaces to health and well-being.
The conceptual model proposed by Lachowycz and Jones (2013: 64) shown in Figure 5 is derived from the authors’ interpretation of socio-ecological theory (in contrast to psychological theory, or epidemiological conceptual frameworks). Socio-ecological interpretations of health maintain that the bio-physical and social environments in which people live provide both opportunities and constraints for individuals, households and population groups to undertake activities that may promote or be harmful to their health (Sallis et al., 2006).
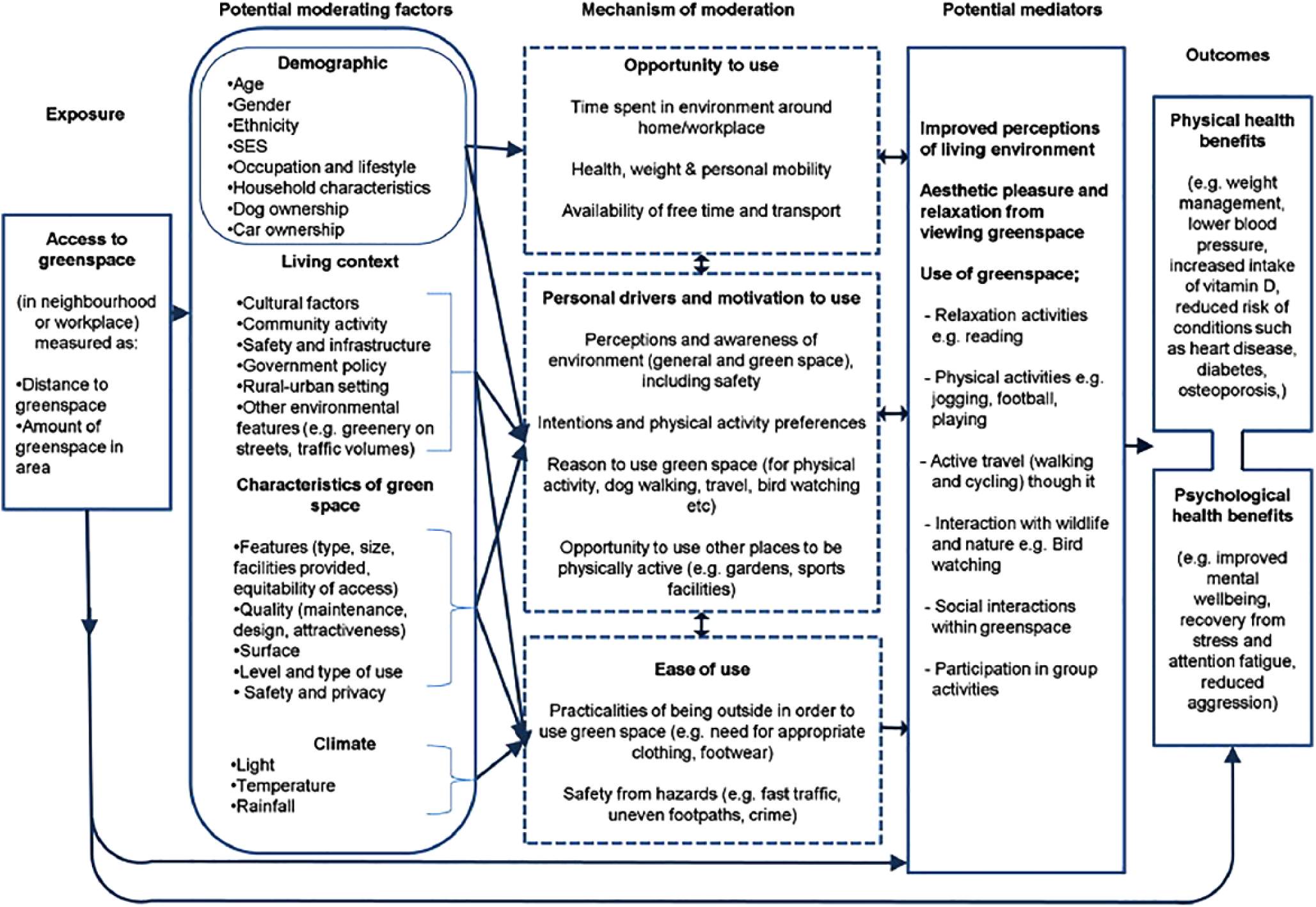
The conceptual model proposed by Lachowycz and Jones (2013).
Despite their references to socio-ecological theory, the authors proposed a behavioural model that represents how human activities can be influenced by moderators and mediators that influence uses of green public spaces. The model includes a linear pathway of the linkages between access to green space, on the left hand side, and physical and psychological health benefits, on the right hand side. This pathway begins on the left with access to green space using objective measures of distance and or surface area. It then shifts right to address how exposure to green space can be potentially influenced by ‘moderating factors’ that account for some contextual societal conditions, including demographic and socio-economic variables, cultural and societal factors, environmental features, local climate, and five characteristics of green spaces. This bundle of moderating factors does not explicitly account for historical precedent. Moving further right, the authors argue that contact with green spaces is influenced by ‘mechanisms of moderation’ including the opportunity to use green spaces, personal motives and reasons, as well as ease of use. A temporal dimension is included as time spent in specific settings, whereas seasonal variability and change to human behaviour are not included. The next step in the pathway comprises ‘potential mediators’ which include improved perceptions of living environments, the aesthetic benefits of green spaces and six uses of these spaces (e.g. relaxation, physical activities, travel, social interaction, interaction with wildlife, and participation in group activities). Finally, on the right hand side, health outcomes are presented only as physical and psychological health benefits.
The sequential pathways in this conceptual model are predominantly mono-directional even though the authors state ‘these mechanisms are intertwined and hence linked by two-way arrows on the framework’ (Lachowycz and Jones, 2013: 65, col.1). However, there are no feedback loops. The differences between ‘moderating factors’ and ‘mechanisms of moderation’ are not clearly explained; they appear to be limited to their influence on uses of green public spaces. However, moderating factors have the potential to change a relationship between green space, human activities and health effects, as well as different sequences along the pathway.
The main issue about this conceptual model is that the authors stated that they ‘consulted key examples of existing socio-ecological models looking at environmental influences on health and health-related behaviours, including health and physical activity’ (Lachowycz and Jones, 2013: 63, col.2). It is important to qualify this statement by emphasizing that the examples they reviewed are research by authors trained in ecological psychology, social ecology, and social psychology. Collectively, the contributions from these fields have acknowledged the importance of the built and natural environments in which behaviour occurs (e.g. the concept of behaviour setting is often used to explain human behaviour in specific situations). However, these contributions have rarely developed a typology of the characteristics of these settings in order to study how they mutually interact with human activities. In addition, human agency is not valued to the extent that the personal motives of individuals, or the shared goals and values of groups, are ignored. Human motivation can explain why different population groups access green public spaces for diverse sometimes conflicting uses (e.g. children’s play, drug trafficking) that are difficult to predict and change over time.
Pathways linking nature and health
The final and most recent conceptual model was proposed by Hartig et al. (2014) in their review of research on ‘pathways between nature and health involving air quality, physical activity, social cohesion and stress reduction’ (p. 207). The authors are educated in environmental psychology, geography and public health. They noted that the majority of empirical research they reviewed ‘focused primarily on benefits of contact with nature’ (Hartig et al., 2014: 208). Hence, negative impacts from exposure to allergens, sun or extreme heat, are rarely included. A large amount of empirical research since the 1990s has been driven by a concern about restorative processes stemming from contact with nature and reducing environmental stressors (such as exposure to air pollution or high ambient noise levels especially in urban areas). Hartig et al. (2014) have identified shortcomings in the reviews of contributions on these topics. First, they noted that the characteristics of natural environments were not always addressed but considered indifferently as a neutral or static context. Second, they noted the lack of interdisciplinary collaboration, especially between epidemiology and psychology. It is noteworthy that there is no reference to the pertinence of other behavioural or social sciences, or political sciences, that concern public health policy agendas, although these were explicitly addressed by Northbridge et al. (2003). Third, the authors stated that the diversity of health outcomes resulting from contact with nature are rarely considered: ‘Most of the evidence covered by the reviews related to intermediate health-related outcomes such as amount of physical activity […] changes in emotional states […] and changes in cognitive capability[…] rather than to disease states or measures of mortality’ (Hartig et al., 2014: 211).
The authors also noted that there is a large amount of research about mediators and modifiers in relationships between air quality, physical activity, social cohesion, and stress reduction. They proposed a conceptual model of these mechanisms, as well as those contextual and individual variables that can modify them (see Figure 6).
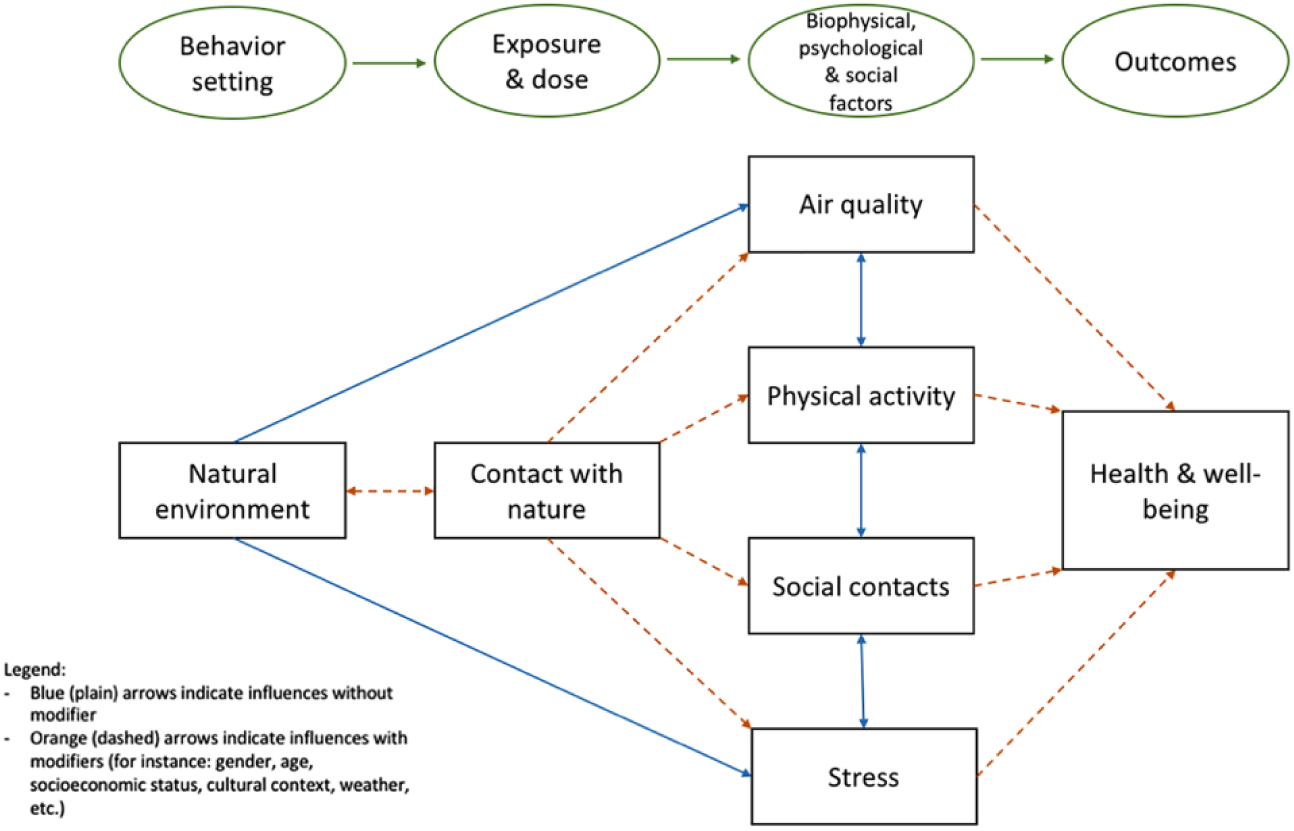
The conceptual model proposed by Hartig et al. (2014) has been redrawn by the authors.
This conceptual model shares the logic of the two preceding ones especially given its linear pathway from left to right. However, the plausible pathways from contact with green spaces include a distinct intermediate sequence involving different types of modifiers. Although the model addresses ‘modifiers’, mutual interaction only exists between some variables, such as the characteristics of natural environments and contact with nature; also the reciprocal relations between air quality, physical activity, social contact and stress. However, the societal context is interpreted as a modifier. There are no feedback loops in the model that could account for internal or external factors that influence and change human behaviour or physical and psychological health. Hence, it is assumed that health status is an outcome following contact with nature rather than a state that can influence human contact with nature. This begs the question about the role of human agency, and the multiple consequences of human activities in green public spaces, and health and well-being. Finally, a comprehensive temporal perspective, including historical precedent, cultural predispositions and seasonal variability, is lacking beyond accounting for the time spent in green spaces and the frequency of that contact.
Synthesis
Each of the five conceptual models presented has shared the common aim of identifying key factors and variables (sometimes called mediators and moderators), their components and subcomponents, and the plausible relationships between them. In each case, a linear pathway has been represented, sometimes with qualifications about mutual interaction between the main component parts, their variables and the influence of moderating or modifying factors. The majority of the contributions have not provided a comprehensive account of environmental correlates of human behaviour in specific green spaces, or identified the relative importance of personal and group variables, or broader cultural and environmental variables on the provision of green public spaces, their management and human behaviour in these settings. None of the conceptual models reviewed in this article have adopted the broader framework requested by Kreiger (1994), or the core principles of ecological public health proposed by Rayner and Lang (2012).
The formulation of an ecological model of public health requires systems thinking of the kind applied by Newell and Siri (2016). Ecological models recognize that any internally or externally generated changes to one of the components or state variables of the system will impact on the other components or variables including the initial component that was changed. Therefore, it is too restrictive to assume that improved access to green public space will change human behaviour and then improve health and well-being. In addition, it is necessary to consider how improved health and well-being could influence uses of public green space and what consequences would result. This has rarely been discussed by researchers in this field but it was addressed during the EU-FP7 PHENOTYPE project (www.phenotype.eu).
Proposed ecological public health model
During the period 2012–2015 of the EU 7th Framework project ‘‘Positive Health Effects of the Natural Outdoor Environment in Typical Populations in Different Regions of Europe” (PHENOTYPE), a systemic conceptual model was formulated using core principles of human ecology (Lawrence, 2001). This model was elaborated during a transdisciplinary research process involving researchers from different disciplines (including biology, human ecology, medicine, land use planning, public health and sociology) and professional practitioners (in landscape architecture, health promotion and urban planning) working in the public or private sectors.
The conceptual model proposed is shown in Figure 7. It is inscribed in a broad multi-level context including environmental conditions at different levels with biological, climatic, ecological, geological, human and physical dimensions at each level. In addition societal conditions have historical precedents that are contextually defined and include cultural, economic, political and social variables at different levels of human experience.
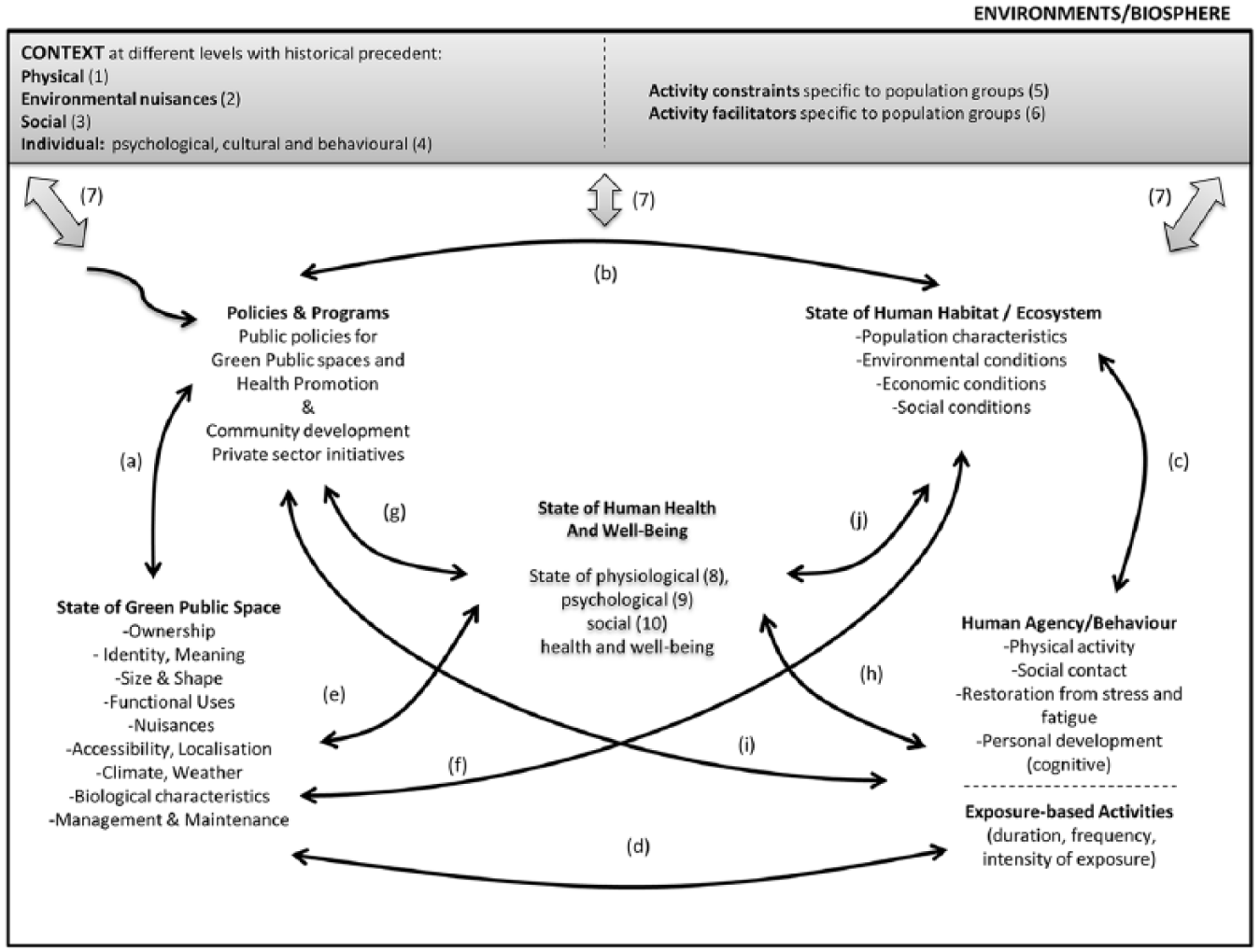
The Conceptual Model formulated during and after the EU-FP7 PHENOTYPE project shows the context in which 5 key domains are interrelated systemically. Policies and programs influence the provision of green public spaces for several purposes including health promotion. The state of human habitat refers to living conditions for human populations. Human agency denotes individual and collective behaviours. The state of green public space includes 9 core variables. Human health is a state or condition that influences human livelihoods including uses of green public spaces The legend with examples: CONTEXT: (1) Geography, climate, weather (2) Air quality, noise, natural risks (3) Community, demography, urban development (4) Personal factors: age, sex, gender, socio-economic position, behaviour, education, perception, motivation, culture, health status, active living (5) Parental restrictions, lack of time (6) Positive attitude (7) All contextual variables (in the grey box) influence the 5 domains and all variables (in the white box) by mutual interaction and feedback. STATES VARIABLES: (8) Body mass index and blood pressure, better metabolism (9) Level of relaxation and restoration (10) Extent of social interaction. STATE-CHANGE PROCESSES: (a), (b), (c), (d), (e), (f), (g), (h), (i), (j).
This systemic model has five domains. It is human centred with one domain comprising human agency for individuals and groups (notably activities, motives, lifestyles and values) as well as a temporal dimension of contact with green public spaces that can vary between seasons and also across the lifespan. It accounts for different kinds of activities (notably active living, social contact, restoration, personal development) as well as different sometimes conflicting uses of green public spaces. A second domain includes the multiple characteristics of green public spaces that also vary between seasons. These characteristics are defined by nine sets of state variables that can be quantified or assessed qualitatively. A third domain concerns the health and well-being of individual, groups and populations, which is also variable and can be a catalyst for behavioural change. Health is influenced by both positive and negative effects of specific kinds of socio-ecological conditions of green public spaces. These effects are quantified as measures of physiological and psychological health, as well as social/community health and well-being. The fourth domain comprises the state variables of the human habitat and ambient environmental conditions for everyday life. These include ecological, socio-economic and other cultural conditions. The fifth domain refers to explicit public policies and programmes, and private initiatives that influence the provision, management and maintenance of green public spaces, health promotion campaigns, or land use planning.
Comparative analysis
Table 1 presents a synthetic overview of the analysis of the five models as well as the characteristics of the proposed model founded on the principles of ecological public health. The vertical column includes the main state variables and these include numerous components and subcomponents not presented in detail here. For example, health has been considered by researchers as physical and mental health outcomes that can be assessed by objective and subjective measures of diverse kinds. The vertical column also includes the main kinds of interactions and processes between the state variables. In addition a temporal perspective is included to account for behaviour change as well as seasonal biological and climatic change. The societal context of any research on this subject has a historical precedent which prescribes cultural predispositions and social norms that should not be ignored. This comparative analysis shows that the main differences between the five published models and the proposed ecological model occur in relation to the nature of the relations and processes between the state variables, the inclusion of feedback loops, and a multidimensional temporal perspective.
Comparison of models.
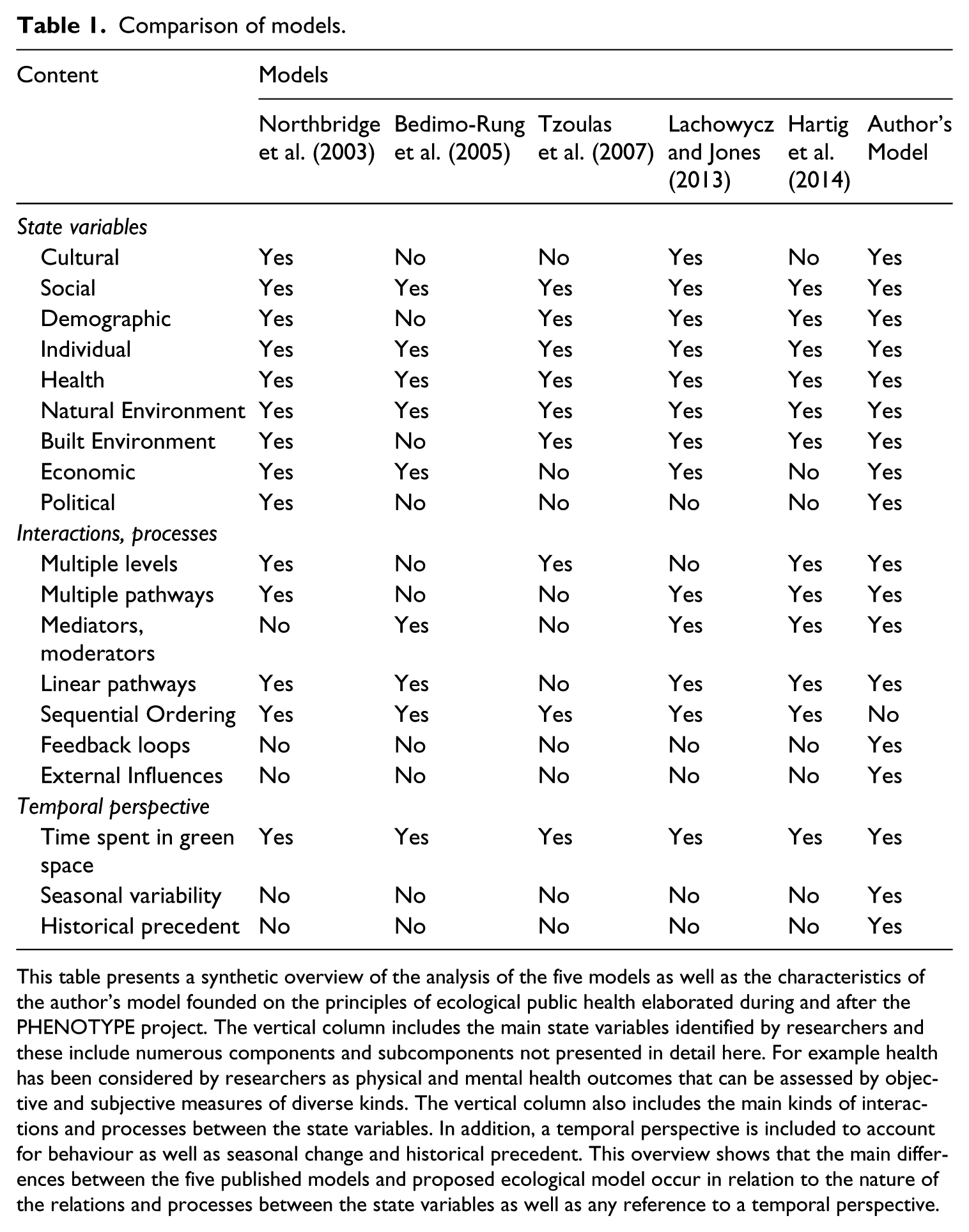
This table presents a synthetic overview of the analysis of the five models as well as the characteristics of the author’s model founded on the principles of ecological public health elaborated during and after the PHENOTYPE project. The vertical column includes the main state variables identified by researchers and these include numerous components and subcomponents not presented in detail here. For example health has been considered by researchers as physical and mental health outcomes that can be assessed by objective and subjective measures of diverse kinds. The vertical column also includes the main kinds of interactions and processes between the state variables. In addition, a temporal perspective is included to account for behaviour as well as seasonal change and historical precedent. This overview shows that the main differences between the five published models and proposed ecological model occur in relation to the nature of the relations and processes between the state variables as well as any reference to a temporal perspective.
Conclusion
The findings of the research presented here confirm that although Kreiger (1994: 896) provided sound arguments for an “ecosocial metaphor” for epidemiology including “history and agency” nearly 25 years ago, her request has not been incorporated in the conceptual frameworks and models reviewed in this article. Indeed, the metaphor of the web of causation has often been replaced by a metaphor of pathways. This has meant that thinking systemically has been replaced by linear causality. In addition, human agency and the societal conditions of daily life have not been included in some interdisciplinary research that is meant to improve understanding of the complex relationships between contact with public green spaces, individual and collective behaviours and health. This article has suggested and illustrated a different ontological perspective of people – environment relations which is contextual, dynamic and systemic, and then illustrated its application for addressing this complex subject in the future.
Footnotes
Acknowledgements
The authors would like to thank the following members of the PHENOTYPE Consortium–Christopher Gidlow, Hanneke Kruize, Magdalena van den Berg, Irene van Kamp, Mark Nieuwenhuijsen, and Wim Swart–for their comments and suggestions on the first draft of this paper in 2015. Special thanks to Professor Barry Newell, Australian National University, for his discussions and written advice during the writing of this article after the completion of the EU-FP7 project. We appreciate the comments and suggestions of three anonymous reviewers.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship,and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article has been produced by WP5 team members of the EU 7th framework project “Positive Health Effects of the Natural Outdoor Environment in Typical Populations in Different Regions of Europe” (PHENOTYPE) under grant agreement no: 282996 (ENV.2011.1.2.3-2). The article was finalized during a two year period after the completion of that project and presents the viewpoint of the authors.