
Abstract
Informal carers are increasingly involved in supporting people with severe and enduring mental health problems, and carers’ perceptions impact the wellbeing of both parties. However, there is little research on how carers actually make sense of what their loved one is experiencing. Ten carers were interviewed about how they understood a loved one’s psychosis. Data were analysed using a hermeneutic-phenomenological approach. Three themes described the carers’ effortful quest to understand their loved one’s experiences while maintaining their relational bonds. Carers described psychosis as incomprehensible, seeing their loved one as incompatible with the shared world. To overcome this, carers developed hermeneutic ‘mooring points’, making sense of their loved one’s unusual experiences through novel accounts that drew on material or spiritual explanations. The findings suggest that informal carers resist biomedical narratives and develop idiosyncratic understandings of psychosis, in an attempt to maintain relational closeness. We suggest that this process is effortful – it is hermeneutic labour – done in the service of maintaining the caring relationship. Findings imply that services should better acknowledge the bond between carers and care-receivers, and that more relationally oriented approaches should be used to support carers of people experiencing severe mental health problems.
Keywords
Evidence suggests that connectedness is essential for a flourishing life: good relationships reduce the risk of physical and mental health problems and suicide (Baumeister and Leary, 1995), as well supporting recovery (Topor et al., 2011). Within a mental healthcare context, many relationships are characterised by a care-giving/care-receiving dynamic. Informal carers have become an essential part of the United Kingdom’s mental health provision in the continuing move away from institutionalisation (Kuipers and Bebbington, 2005) and recent funding crises. One and a half million people are registered as caring for someone with a mental health problem in the United Kingdom and up to 7 million people care for someone unofficially (Riley et al., 2011). Recent UK policy recommendations and legislation, such as the Triangle of Care (Worthington and Rooney, 2010) and the Care Act (2014), have helped to focus clinical attention on the carer role. However, predominant biomedical models that position mental health as the result of biological processes in discrete organisms have led to a chronic neglect of the relational context of distress (Pilgrim et al., 2009).
Research on caring is often reduced to either the burden of practical tasks or the emotional strain associated with the role (Riley et al., 2011; Shah et al., 2010). There has been less focus on how carers understand their experiences, and in particular how they make sense of their relationship with the person for whom they care. This relationship is perhaps particularly complex when the person being cared for is experiencing a severe mental health problem, such as ‘psychosis’, where there is little explanatory consensus among the psychological community, and public portrayals are often stigmatising (Clement and Foster, 2008). This article focuses specifically on caring for someone in this context, but the implications are likely to be relevant to anyone caring for someone with severe and enduring mental health problems.
The caring ‘burden’: perceptions of psychosis
Informal carers typically provide a familiar and loving environment for those they care for, as well as saving the UK government up to £87 million annually (Riley et al., 2011; Worthington and Rooney, 2010). However, carers are often the untrained family and friends of service-users (Worthington and Rooney, 2010), and research has repeatedly shown that carers looking after people experiencing psychosis themselves experience a high degree of emotional distress, fatigue and depression (Riley et al., 2011; Shah et al., 2010). This distress seems to correlate with how the carer perceives their experience, whether they consider they have high levels of subjective burden (distinct from objective measures of financial, time and relational stressors), and how they think about issues such as symptom control, changeability and responsibility (Fortune et al., 2005; Kuipers et al., 2007; Onwumere et al., 2008; Patel et al., 2014).
Certain carer perceptions appear to be linked to specific coping strategies with varying outcomes in terms of carer distress. The perception that psychosis is unchangeable leads to avoidant or escapist coping mechanisms, which are related to higher distress and decreased social engagement (Patel et al., 2014; Raune et al., 2004). Carers who felt a larger sense of burden were less likely to connect with their social networks, but increased feelings of burden may also be a result of having a smaller social network (Magliano et al., 2003). Carer perceptions also affect the emotional climate of the caring relationship (Barrowclough et al., 1994; Grice et al., 2009; Hooley, 1998; Riley et al., 2011). During a first episode of psychosis, carers who believe that they have ‘lost’ their loved one (through perceived identity change) or that the person experiencing psychosis is ‘to blame’ (such as through drug use) experience a higher degree of distress, and are more hostile or critical of the care-receiver (Barrowclough et al., 1994; Grice et al., 2009; Onwumere et al., 2014; Raune et al., 2004).
The emotional climate of care-giving in psychosis
It has been robustly demonstrated that the emotional climate of the caring environment is related to mental health outcomes for the care-receiver (Bachmann et al., 2006; Butzlaff and Hooley, 1998). Caring environments characterised by high levels of criticism, hostility and intrusiveness (high Expressed Emotion; EE) are related to higher relapse rates in psychosis (Barrowclough and Hooley, 2003). EE research has been seen as family-blaming (e.g. Hatfield et al., 1987), only accounts for the maintenance of psychosis not its onset, and is associated with mood and eating disorders as well as psychosis (Butzlaff and Hooley, 1998). Nevertheless this finding is stable cross-culturally and unrelated to medication use, indicating that the relational environment is vital to recovery (Bebbington and Kuipers, 1994). Perceptions that the person with psychosis has no control, or conversely all the control are associated with higher EE (Barrowclough et al., 1994; Grice et al., 2009; Hooley, 1998), whereas perceptions of psychosis as part of a spectrum of behaviour, a personalised view of recovery and beliefs of shared control between care-receiver, care-giver and illness are associated with lower EE (Barrowclough et al., 1994; Grice et al., 2009; Onwumere et al., 2008). Carers using a broad range of coping mechanisms is also associated with lower EE (Treanor et al., 2013).
On the basis of this evidence, Kuipers et al. (2010) developed a cognitive model of care-giving in psychosis, in which they argue that carer appraisals relate to the pre-existing relationship, carers’ reaction to the consequences of caring (i.e. ‘burden’) and their coping mechanisms. They argue that, alongside other factors such as social support, carer appraisals feed into the emotional climate of the care relationship. While considering multiple factors involved in the caring relationship and taking account of the quality of the relationship, this model does not fully account for idiographic, relational and emotional aspects involved in loving, caring for and living with someone with psychosis. How carers themselves describe how they make sense of their loved one’s experiences remains under-explored.
Information, explanation and understanding: making sense of psychosis
Despite evidence that carer perceptions are related to carer wellbeing and care-receiver outcomes, UK carers report having difficulty learning about their loved one’s mental health experiences, needs and progress from professionals (Gerson et al., 2009; Hickman et al., 2016; McCann et al., 2012; Worthington and Rooney, 2010). In addition, the psychiatric explanations favoured by professionals, which atomise and depersonalise the individual, will not necessarily be sufficient for carers, who prioritise different types of knowing and understanding (Hoerl, 2013). Medical model explanation is unlikely to take account of the felt and relational aspects of lived experience that enable people to make sense of each other, live alongside and love each other. Understanding, however, is intersubjective: it requires a ‘meeting’ between persons at a felt, one-to-one level (Hoerl, 2013). In understanding, the other is seen as a whole person, not ‘a loose bundle of named qualities’ (Buber, 1970 [1923]: 59) as is inherent in the process of diagnosis. Understanding is relational and happens dialogically (Stawman, 2011).
Understanding their loved one’s experience of psychosis is therefore likely to be very important for carers, yet this endeavour is not well supported by services. The medical model positions experiences of psychosis, such as voice-hearing or holding unusual beliefs, as the meaningless product of the disease process, which undermines carer attempts at understanding. Although contemporary service-user-led groups (e.g. the Hearing Voices movement) have argued that psychotic experiences are meaningful if seen as symbolic representations of the person’s lived experiences and distress, most service-led psychoeducation projects prioritise the imparting of scientific explanations, with the aim of influencing carer perceptions. Individual programmes, ranging from clinician-led lectures to participant-based support groups, have improved carer self-efficacy and lowered stress (Lobban et al., 2005; Petrakis et al., 2013; Riley et al., 2011; So et al., 2006), improved caring relationships (Riley et al., 2011) and improved relapse outcomes (Harvey and O’Hanlon, 2013). However, research has not demonstrated that there is one single helpful way of appraising psychosis, or that it is possible to substantially affect carer perceptions (Barrowclough and Hooley, 2003).
This study does not seek to see if carers hold ‘right’ or ‘wrong’ perceptions or appraisals, but to explore how carers make meaning from their situation, how they come to understand and make sense of their loved one’s experience of psychosis. A qualitative approach provides a way to understand carers’ experiences (Geekie et al., 2013; Treanor et al., 2013) from a lived, relational and embodied perspective, and without recourse to pre-existing models.
Methodology
Participants
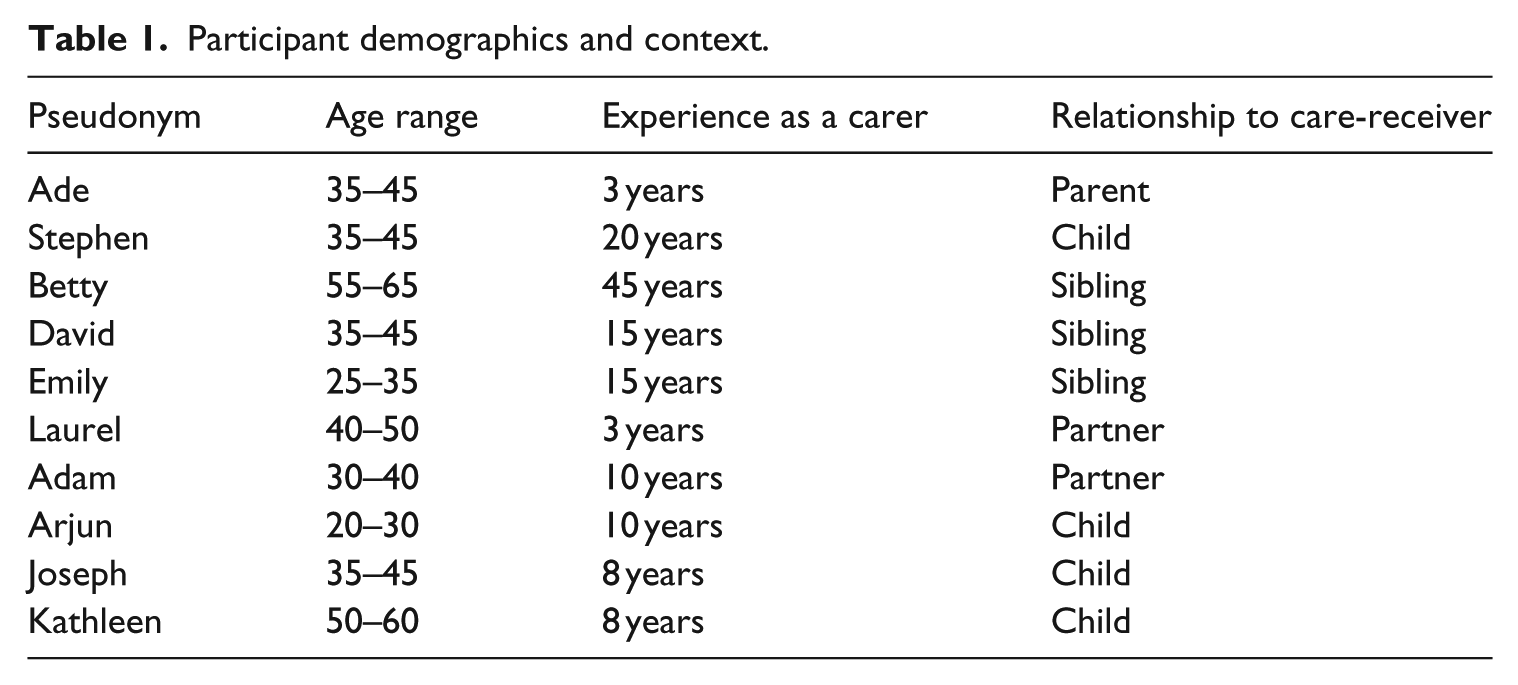
Ten participants were purposively recruited via UK carers’ and mental health charities, social media and word of mouth (see Table 1). Participants were adults, of mixed ethnic and cultural backgrounds, who, for at least 6 months, had been an informal carer for someone experiencing psychosis. They were recruited to participate in an interview study about how they understood psychosis and their experiences of caring. Psychosis was defined as experiencing perceptions or holding beliefs that others do not share (Cooke, 2014). A carer was defined as someone who lived with, or looked after the primary needs of, the person with psychosis. Participants who were experiencing mental health problems themselves or who worked professionally in the mental health sector were excluded. All participants are referred to by pseudonyms. Participants self-selected and were thus likely to be people for whom the question had particular salience.
Participant demographics and context.
Data collection
Data were collected in 2016 in the United Kingdom. The study followed British Psychological Society ethical guidelines and received University approval. Participants gave informed consent and data were anonymised and confidential. The interviewer (Luderowski) was sensitive to potential distress and signposted participants towards carer support services as required. One-to-one semi-structured, phenomenologically oriented interviews were undertaken, guided by an interview schedule. Open-ended questions, with prompts and probes, enquired about carers’ sense-making processes throughout their experience as a carer. Topics included carers’ meaning-making around the experiences of the service-user, diagnosis, causal and maintaining factors, treatment and recovery. Interviews lasted 90 minutes on average and were transcribed verbatim, noting additional non-verbal information.
Data analysis
The study took a hermeneutic-phenomenological approach, based on the Interpretative Phenomenological Analysis (IPA) methodology (Smith et al., 2009). IPA typically holds methodological commitments to both phenomenological and hermeneutical principles, exploring the ‘what-is’ and the ‘how-is-it-understood’ both in terms of the participants’ experience and in the researchers’ approach to analysis (Boden, Larkin & Iyer, 2018). In this study, we most strongly focused on the hermeneutic commitment, that is, the participants’ sense-making and how we could understand this process. Thus, the analysis involved describing what participants shared about their meaning-making and the researcher’s interpretation of their account (Smith et al., 2009). This ‘double hermeneutic’ involves an analytic dialogue between the participants’ and the researchers’ sense-making processes (Smith et al., 2009). Data analysis was undertaken by both authors, with discussion at each stage of the process. Working participant-by-participant, initial notes were made for each transcript, paying attention to the content of what participants said, their relationships with what mattered to them and the context. Data were coded into ‘emergent themes’, paying particular attention to the participants’ sense-making processes and capturing descriptive, conceptual and linguistic aspects of the data (Smith et al., 2009). Codes were then clustered into higher order themes, according to conceptual similarities. Thematisation is necessarily an interpretative process; however, to ensure analytic rigour, consensus was sought between authors, and careful attention was paid to negative cases. Once the thematic structure captured the complexity of the participant’s lived experience, analysis began on the next case. Once separate thematic structures were developed for each person, these were collapsed into a master table of themes that drew similarities and differences between participants’ accounts. Luderowski kept a reflexive research journal throughout the data collection and analytic processes to aid validity, and maintained a thorough audit trail.
Findings
Findings are presented as three interlinking themes that indicate the carers’ quest to understand: ‘The struggle to understand: Inaccessibility and incomprehensibility’, ‘Understanding what cannot be understood: The care-receiver as incompatible with the carer’s world’ and ‘Maintaining the relational bond: Mooring points of understanding’.
The struggle to understand: inaccessibility and incomprehensibility
All participants, except Arjun, described a struggle to make sense of their loved one’s experiences of psychosis. For some (Stephen, Betty, Laurel, Joseph), their loved one’s mind was seen as a ‘black box’ that was neither accessible from the outside nor the inside. Stephen describes his challenge to understand the nature of his mother’s psychosis: If someone’s asking how she’s coping in the mind, I’d struggle, […] ‘cause how I can understand mental health difficulties if the poor person doesn’t understand it herself?
For Stephen, intersubjective understanding is impossible in the perceived absence of self-understanding.
Betty also describes the mystery of her sister’s intrapsychic experience: ‘I don’t know what really goes on in her head’. Instead, Betty focuses on how she and the staff at her long-term residential service can be with her sister, maintaining a relationship in the absence of understanding and dialogue. Betty’s language illustrates the tension between the impersonal and perfunctory (‘deal with her’) and her hope that her sister maintains some personal (‘meaningful’) relationships: We all know how to, to sort of deal with her [… the staff] are so skilled at being with her, […] enough of the staff there have a good relationship with her, in a way that works for them both to be meaningful.
Stephen similarly describes the act of caring as simply being with the person in distress: Just being there, that’s what carers are, just being there even if you can’t help, aid in recovery; witnessing their decline so they’re not walking that path alone.
Stephen’s desire to walk alongside his mother in her distress implies empathy and connection, but by describing himself ‘witnessing’ this he perhaps feels fundamentally outside this experience. A witness has no agency in the situation; they experience the situation ‘secondhand’. Without the opportunity for dialogue, Stephen professes to having only a superficial understanding, where anything deeper appears impossible.
Other participants found their loved one’s experiences inaccessible because of their apparent irrationality. They felt psychosis defied the logical approach that participants typically relied on to make sense of their experiences. When trying to reason with her son about his unusual beliefs, Ade says, ‘I’m in cuckoo-banana land, la-la land, where I can’t say ‘but I’m not’, because that brings a worse response’. Interacting with her son transports Ade to an alien place where she is unable to engage with him normatively, and where her rational sense-making fails her, and her son. Laurel also spoke about confronting what she sees as the confounding lack of logic in psychosis: It’s so, I’ve found it so disturbing. I, you know, the mean- of trying to, trying to understand psychosis when you can’t understand. It’s the one thing you can’t understand, because it’s madness. […] That’s the definition of madness. […] You can’t understand it. It’s not rational. It’s not ‘true’. […] Which isn’t true.
Laurel is deeply troubled by the apparent irrationality of her partner’s psychosis, and her belief that ‘madness’ is incomprehensible. Laurel has tried hard to make sense of something that she feels is beyond her understanding, and there is a sense of absurdity in this project. However, she seems uncertain about her claim that there is no ‘truth’ in psychosis and contradicts herself – it is not true that psychosis is untrue. However, the truth of psychosis seems to come from somewhere beyond her own rational sense-making.
Understanding psychosis as incomprehensible was seen by some participants as liberating, allowing them to stop trying to make sense, analyse and interpret everything that was happening. Stephen, Betty, Laurel and Joseph suggested that no one knew what was going on with their loved one: not them, not the clinicians and not even the person with psychosis. They understood this not as ignorance, or a deficiency in understanding to be overcome, but as a definitive ‘truth’, the absolute incomprehensibility of psychosis. As Stephen said about one clinician’s explanations, ‘I don’t know, they don’t know’.
Understanding what cannot be understood: the care-receiver as incompatible with the carer’s world
All participants in this study made sense of the inaccessibility and incomprehensibility of psychosis by conceptualising their loved one as incompatible with their world. Some participants saw this as a result of the person being too ‘underdeveloped’ to handle the ‘real’ (carer’s) world, therefore locating the problem with the person. Others felt their loved ones had been rejected by the world because of societal, familial and religious prejudice, locating the problem with the world. Either way, the loved one was positioned as somehow ‘other’ to the shared world of the carer and the rest of society.
Ade, Betty, David, Emily, Laurel, Arjun and Kathleen suggested the world was ‘too much’ for their loved ones, due to their innate sensitivities, weaknesses or immaturity. These carers felt that the person experiencing psychosis hadn’t developed what was necessary to take on the world as an adult. For several participants, this was seen as a deficiency in their loved one’s own sense-making capacities. They suggested that those they cared for were childlike, and unable to understand how the ‘adult’ world works. Ade described how her son’s distress stems from entering into the adult world lacking the necessary understanding and mental maturity: ‘He’s got the tendencies of the-the physical teenager, tendencies, but mentally not’. Ade stresses that her son was not mentally developed enough to understand the developmental changes in his body, and that this lack of understanding of the new world he was being thrust into led to his distress.
David echoed this when he discussed a key difference between why his brother experienced mental distress in his 20s, while he did not: He just had something more sensitive in him or whatever. I’ve read a lot on it and one of the things they say is it’s like an inability to form a sort of shell around yourself to take you into adulthood.
David has sought out ways to make sense of his brother’s distress. His word ‘shell’ evokes an absent shield, a protective toughness that failed to develop, leading to vulnerability in the face of the grown-up world. Several other participants shared this view that one must develop armour growing up, in order to protect oneself from the inevitable ‘slings and arrows’ of adult life. Although never explicitly blaming their loved ones, this sense-making strategy situates responsibility for the psychosis with the person. It is because something about them or their development was atypical that they were unable to survive the adult world as others do. Without the shell, participants believed the world was simply too much for their loved one who then retreated into another, alternative world.
Adam articulated how this retreat into ‘otherness’ became deeper with each crisis, resulting in his partner seeming to be more and more incompatible with his world: It’s a bit like uh, an elastic band in that, once, be-when she had one crisis she kind of got back, but, the second and third crises it just went a bit too far, for her to properly get back.
For Adam, his partner cannot return to their shared world because she had travelled too far away and ‘stretched’ too much; the change had become permanent. This image of being lost to some ‘other’ world captures Adam’s sense of alienation from his partner, and his belief in the inaccessibility of her experiences.
In contrast, Stephen, Emily, Laurel, Adam, Arjun, Joseph and Kathleen saw their loved ones as people who had been rejected from the world because of their perceived difference, for reasons including race, religion, culture, disability, single-parent status and even having red hair. This understanding is encapsulated by Emily, who draws on the literary idea of ‘Russian Superfluous Man’, a character in 19th-century Russian literature who had no place in society and therefore lacked both home and purpose. Emily suggests that for people with psychosis: ‘there’s no proper place for them in society because society isn’t built for people like them’. She situates the problem in the restrictive society rather than the person. Kathleen illustrates this by describing the multiple ways her mother was marginalised as an Irish Catholic single-mother of a mixed-race child in the 1960s: Her internal philosophy, plus the political, social environment in the outside world, where she’s kind of you know, against the Irish, against the Blacks, against single parents, she has to have that, and then, on top of that then her family, cast her off […] so every single, possible avenue externally, in the external wide world, the smaller family world, and then the um, internal world.
Kathleen focuses heavily on her mother’s rejection – being ‘cast off’ to fend for herself – by her family, her culture, then eventually, as all avenues closed, becoming cut off from herself due to the values she internalised. For Kathleen’s mother there was no home or no accepting place to take refuge because her mother was made to feel ‘wrong for being alive’.
Joseph’s account of his mother echoes this: She got loads of shit from her family for getting pregnant. She worked in the church so the-the shame that she must have felt must have been enormous.
Like Kathleen, Joseph stresses that his mother had no sanctuary from the world. Once her loved ones rejected her she had to hold ‘secrets’ and ‘shame’ within herself.
Arjun also describes multiple rejections when he relates his mother’s distress to a calamitous combination of cultural and familial loss: When she came to the country, uh, like I said, she didn’t really integrate so well […] the only thing she had was me, and my brothers after my dad left. […] she just found it quite difficult to cope, and she felt that kind of her world was being taken away from her. Because she was, even though she’s lived here for, uh, 29 maybe 30 years she still feels, quite alien in society.
Arjun understands that refuge can be taken in various worlds: familial, societal, religious, political and internally, but that when there are multiple sources of rejection, this can be overwhelming. Arjun sees his mother develop psychosis when she loses the stability of her family, having already having lost her social stability through migration.
Maintaining the relational bond: mooring points of understanding
Despite, or perhaps because of, their sense of their loved ones’ otherness and incomprehensibility, carers sought ways to maintain their relational bonds. Wherever their worlds overlapped or collided, participants sought out or created a ‘mooring point’ of understanding. These were attempts to ‘latch on to’ something in order to stop their loved one ‘drifting away’ from them relationally. This was an effortful process that resulted in connections that were typically tentative, partial and unidirectional. These mooring points were discrete attempts to understand specific facets of the care-receivers’ experiences, and were not attempts to create holistic explanatory models.
Adam articulated this idea when he spoke about spotting Dr. Who references in his partner’s delusional beliefs: ‘It just got me somewhere […] because I realised [the belief] comes from somewhere, it’s not completely mad’.
The phrase ‘completely mad’ refers to Adam’s experience of his partner as inaccessible. Finding one aspect of her experience of psychosis that he could understand – the TV programme Dr. Who – provided a ‘mooring point’ for Adam to connect himself and his partner together through shared understanding.
Many participants latched onto a mooring point by bypassing ‘rational’ routes to understanding, and instead discovering idiosyncratic ways to make sense of their loved ones’ behaviour and experiences. These were either material accounts (creatively drawing on ideas from genetics, nutrition, physical health or pseudoscience), or supernatural and spiritual accounts. Participants occasionally shuttled between these in an attempt to find a functional sense-making strategy that was ‘good enough’.
Perhaps because of the British cultural and historical context of this study, 7 out of 10 participants utilised (secular) material accounts in order to maintain connections with their loved one. Material ‘mooring points’ acted as inroads for understanding, where one, discrete part of the service-user’s experience was isolated, and understood. All three sibling carers (Emily, David and Betty) were drawn to genetics as means of partial understanding and connection, citing their shared upbringing, as David explains: It’s got to be a part genetic, cause we’re all brought up at the same, you know together, in the same room and everything we didn’t have, that much different circumstances.
When no other differences could be identified, the idea that the siblings were genetically different (something invisible, but profound) offered a physical separation between the siblings, as well as a way of understanding their loved one’s anomalous experience. For some, the perceived inevitability of the genetic explanation helped normalise their loved one’s experience, making them less ‘other’. Betty describes her sister’s experience ‘as something intrinsic within her, you know some people has asthma, some people have diabetes’. By comparing it with other health conditions, Betty normalises the psychosis as part of her sister’s ‘natural’ existence, which may feel less disturbing.
Ade and Kathleen looked to nutrition as a physical root cause. Ade described in detail how a poor digestive system made sense of her son’s psychosis: He had the problem with his gut, he had serious toxicity in his system, it damaged his internal, his lining of his wall, and, toxins leak into his system. And when they do that from the gut, it gets into the brain … So, from all what I’ve read, what I’m meant to do is to bring down the toxicity in his system.
For Ade, nutrition becomes the way that her son’s psychosis can become tangible. Food is something we grasp, offer and control as part of caring for ourselves and others. Focusing on nutrition allowed Ade, and Kathleen, to construct healing diets for their loved ones, allowing them to experience a sense of contributing to their loved one’s recovery on a daily basis.
Kathleen understood one facet of her mother’s distress, hearing voices, through a physiological/medical explanation: Because she can’t hear in one ear, when you can’t hear, sometimes your, ear drum, creates sounds […] like, noises. Like tinnitus. […] Um, so, in a logical way, I’ve sometimes tried to kind of think like, that might be a logical reason to understand, what, these kinda noises in her head.
Kathleen seems to acknowledge her creativity and tentativeness in this sense-making process, which takes the ‘mysterious’ phenomenon of voice-hearing and makes it ‘logical’. Neither the doctors nor her mother said she had tinnitus; however, Kathleen’s understanding provided a normative way of making sense of what was happening. Seeing her mother’s voices as stemming from a ‘real’ sound allowed Kathleen to position them as part of the shared world, rather than understanding them as emanating from an inaccessible, ‘other’ place.
Three participants also made sense of their loved one’s experiences through recourse to supernatural or spiritual understandings, which released them from the confines of rationality. Psychosis did not have to make logical sense if it was deemed to involve aspects of experience beyond material boundaries, and this allowed carers stay ‘moored’ to their loved one despite not having rationalised their experience. Ade speaks about how doctors could not help her son because of this: ‘The doctors only know what they’re taught, they’re afraid to go out of the boundaries’. The homoeopathic remedies she added to her son’s diet were understood to ‘act on another level in the human s[ystem …] another level entirely’, suggesting she felt her son’s psychosis originated from a deeper level or higher plane.
Kathleen believed her mother’s psychosis has a spiritual nature: [From] the upbringing that she’s had and the environment, that it would sort of channel itself in that sort of um, that world of the kind of um, that other-worldness, which is sort of not in the real world, but it’s in the spiritual, realm.
For Kathleen, her mother’s marginalisation and distress have been expressed at a spiritual level, unbounded by ‘real world’ rationality. The incomprehensibility of this other ‘realm’ is understandable and unavoidable. While Kathleen is not able to understand that ‘other world’ her mother is in, she is able to make sense of why it is part of her mother’s experience, and therefore live alongside it. Laurel similarly discusses how seeing psychosis as supernatural helped her make sense of it: I got really interested in that whole idea about, possession and, […] before they, mental illnesses were diagnosed and psych – psychiatry thing came in, […] back in the 16th century and things like that. Possessions – well that makes loads of sense.
For Laurel, psychosis makes more ‘sense’ in a spiritual realm than a medical one; ‘psychiatry’ is juxtaposed against historical ideas of ‘possession’, thus Laurel is juggling between the ‘rational’, hegemonic understanding (Western psychiatry) and what makes intuitive sense to her (possession).
Two participants, Ade and Kathleen, shuttled between material and spiritual understandings. Ade believed her son’s digestive problems were causing him to hear voices, but that this was also irritating him spiritually and that his soul was agitated. Kathleen attributed her mother’s voice-hearing to tinnitus, and also linked this to her spiritual unease due to her religious persecution. For these participants, the spiritual and material explanations for their loved one’s distress were not contradictory, but offered a more comprehensive understanding where ‘logical’ accounts failed.
Discussion
This study describes a three-phase process of how carers make sense of a loved one’s severe mental health problems. Initially participants described difficulty understanding their loved one’s psychosis because it seemed beyond rational explanation, inaccessible and incomprehensible. Participants therefore understood the psychosis by viewing their loved one as somehow ‘other’, lacking those aspects that would allow them to cope in the adult world or marginalised because of their difference. This ‘otherness’ made their loved one incompatible with their own world. While providing a way to make sense of their loved one’s seemingly strange or unknowable experiences, this strategy conflicts with the participants’ desire to maintain their relational bonds and understand their loved one through familiarity and normativity. The final part of the process involved participants attempting to find ways to make sense of their loved one’s psychosis that would not threaten those relational bonds. These new attempts to understand bypassed the need for ostensibly ‘rational’ or ‘logical’ sense-making, and instead utilised material or supernatural/spiritual understandings to explain discreet aspects of their loved one’s experiences. This seemed to allow carers to feel at least partially connected to the person with psychosis, despite the fact that these understandings were not always experienced as fully adequate. This study suggests that for those caring for someone with psychosis, there is an effortful and idiosyncratic process to make sense of their loved one’s experience and to comprehend something that seems initially incomprehensible. It is this process of ‘hermeneutic labour’ (Leventhal, 1994) – working to find a way to understand – that helps to maintain the relationship.
Understanding and the person
In this study, carers viewed psychosis as incomprehensible, yet at the same time they went to significant lengths to try to find meaning and make sense of their loved one’s experiences. These carers predominantly ignored mainstream psychiatry’s view of psychosis as a biologically determined brain disorder (the exception was some participants’ recourse to genetics), and instead privileged idiosyncratic and personally relevant ways to make meaning from their situation. Carers and professionals are likely to need different ways to make sense of psychosis. Hoerl (2013) argues that while explanation is enough for clinicians, only understanding is sufficient for someone in a relationship with a person experiencing mental health problems. Explanation is predicated on a surface-level examination of multiple cases (Hoerl, 2013) and, like all scientific processes, artificially stands outside or above the phenomena, objectifying and reducing the lived experience (Merleau-Ponty, 1964). Scientistic explanation of this sort ‘misses’ the fundamental felt, embodied, relational aspects of lived experience that allow people to maintain relational bonds. Understanding, in contrast, privileges the ‘between’ (Buber, 1970 [1923]: 59), the dialogic, intersubjective space that emerges out of ‘meeting’ the other as a whole person. It is this type of understanding that permits the rediscovery of what might be shared (Dilthey, 2002 [1910]), despite our differences. In a contemporary clinical context, this philosophical view is most strongly endorsed by the Open Dialogue approach to psychosis (e.g. Seikkula, 2002), which works with the entire social network where someone is experiencing psychosis. This approach aims to support person-to-person meeting, encourages shared understanding through dialogue and radically respects the importance of relational bonds in recovery from mental health crises.
Seeing psychosis as incomprehensible challenges Western scientific principles of logical explanation, but (drawing on Jaspers, 1962) it also indicates a failure of ‘everyday empathy’. Everyday empathy relies on the belief that we can use our own experience of the world as a template for understanding others; little in the carers’ life experience prepares them to understand psychosis, which seems radically ‘un-understandable’ (Hoerl, 2013: 118). However, this study suggests that some understanding was possible. Carers found ways to develop understandings that ‘fit’ their loved one’s experiences, but did not necessarily stand up to logical scrutiny (even their own). Rather than static appraisal, understanding in these cases was emergent, contingent, fluid and even contradictory. Seeing their loved one as incompatible with the shared world may be an intuitive way of acknowledging that the carer’s own experience would be insufficient scaffolding for everyday empathy, and that other hermeneutic strategies would be necessary to maintain emotional connection.
Bridging the relational gulf: hermeneutic labour
Understanding, being understood and sharing a meaningful life are central to feelings of belongingness. Belongingness, in turn, is fundamental to wellbeing and protects against mental health problems (Baumeister and Leary, 1995). It is also a better predictor of recovery in psychosis than symptom severity (Norman et al., 2013). Many of these carers intuitively placed disrupted relational experience at the heart of their loved one’s distress. They described experiences of marginalisation and alienation from multiple relational spheres (relationships, family, society, culture), and while this psychosocial account of psychosis is gaining traction (e.g. Bhugra, 2000; Read et al., 2013; Selten et al., 2007), it is still notably absent from much mainstream psychiatry. Mental health stigma was also cited as a reason for the loved ones continuing to feel ‘locked out’ of the world, which is a well-established barrier to recovery (see Birchwood, 2003). It is perhaps unsurprising then that carers went to such lengths to avoid repeating this relational trauma in their own relationships with their loved ones. However, they seemed to encounter a dilemma: a conflict between the perceived incomprehensibility of their loved one’s experience and a deeply held and fundamental desire to understand them and their experiences.
Stolorow (2007) suggests that when one feels as though the other’s experiential horizons do not cross with one’s own (incomprehensibility), a gulf opens up that feels difficult to bridge. This study demonstrates the effort undertaken by carers in an attempt to bridge this gulf, or at the least to create mooring points with the hope of stopping their loved one drifting away entirely. This is ‘hermeneutic labour’ (Leventhal, 1994), an effortful grasping towards understandings that seem to take account of the person (including their history and personality) and which enable a meaningful meeting between the carer and their loved one. Hermeneutic labour transforms what is initially felt as incomprehensible and the ‘other’ into something that is more familiar and accessible by repositioning it within their horizons of shared experience.
Hammerschlag (2014: 24) writes that ‘the language of science cannot adequately explain the mystery that is an essential part of the human experience’. In this study, medical models of understanding psychosis were experienced as insufficient, and medical practitioners were positioned as essentially ignorant. Instead, participants created idiosyncratic material understandings that they found relatively simple and tangible (e.g. nutrition), or supernatural and spiritual explanations (e.g. possession), which released them from the confines of Western secular rationality. There was noticeable diversity in the understandings among and between participants. Many went to some lengths to seek out ways to sense-make that felt sufficient; useful explanatory evidence was gathered both ad hoc and purposively from websites, support groups, academic books, news articles, local cultural knowledge and novels, and was pieced together in a patchwork of understanding. Their hermeneutic labour in creating, and emergently recreating, understandings that best accounted for their loved one’s experiences provided spaces to contact and ‘meet’ their loved ones in ways that felt shared. The goal of this purposeful process was therefore to develop and maintain emotional proximity and relevance, and support relational bonds.
Thinking differently about carers and psychosis: some implications for practice
With the care for people experiencing psychosis falling increasingly on informal carers, rather than psychiatric professionals (Kardorff et al., 2016), how carers make sense of psychosis is increasingly relevant. In this study, carer sense-making occurs within the context of carers feeling unsupported and excluded by clinician’s explanations of psychosis, or lack thereof. Arguably, objective scientific understandings fit poorly with the subjective, relational caring role (Wajcman, 1991) and the understandings that emerge from that role. Carers often feel that their contributions and expert knowledge go unrecognised (Worthington and Rooney, 2010) and many feel ignored, not listened to or blamed for the service-users’ problems (Lyons et al., 2009; Rowe, 2012).
Most carers wish for more empathetic communication with mental health professionals and greater involvement within the care team (Worthington and Rooney, 2010). One way this is done is through involving carers in psychoeducation programmes, although this study suggests that this could be problematic. Psychoeducation that is based on imparting biomedically oriented ‘truths’ about psychotic experiences and recovery may be deemed a form of intellectual colonisation, to be actively resisted or simply forgotten. These carers seemed sceptical that the medical model could offer understandings that were helpful, or which were likely to be consistent with personal, experiential and (auto)biographical truths, such as histories of marginalisation and rejection. This scepticism might be reinforced by actual or perceived differences between clinicians and carers (e.g. class, ethnicity). Disenfranchised groups may also be more mistrustful of biomedical models of mental health because similar models have been used to justify social disadvantage (Schnittker et al., 2000). Carers in this study preferred more grassroots networks for information, including friends and Internet fora. Understandings that do not take into account the real-world inequalities and social exclusion experienced by carers and service-users are unlikely to be integrated smoothly into pre-existing understandings.
A mismatch between carer (and service-user) understandings and those of the clinical staff is a missed opportunity to forge closer relationships between services and those they serve. Psychoeducation programmes are not typically tailored to meet the individual needs of specific relationship settings, and therefore the ‘unique strengths and vulnerabilities’ of each system are missed (Martindale, 2009: 59). While a recent meta-analysis suggests that psychoeducation groups offer support through providing a peer-to-peer environment that normalises carers’ experience (Sin et al., 2017), the opportunity for staff and carers to engage in meaningful dialogue about carers’ specific experiences and perspectives is also needed. Psychoeducation sessions can provide a forum for carers to share their personal understandings with services (Addington et al., 2001) – educating them about their patients – and services should value and respect these perspectives, even when these are at odds with established views. Corocoran (2017) agrees that clinicians must respectfully listen to their patients’ loved ones if psychosis care is to improve.
Carers in this study crafted their understandings in dynamic and idiosyncratic ways in order to manage the conflict between the perceived incomprehensibility of their loved one’s experiences and their desire to maintain a close relational bond with that person. Services should not assume that how carers make sense of psychosis, or any mental health problem, will remain static, nor should they prioritise the content of carers’ sense-making over the sense-making process. This study suggests that carers’ attempts to understand their loved ones, and the efforts they go to do this, are perhaps more important than the understandings themselves.
Footnotes
Acknowledgements
The authors would like to thank the generosity of the research participants.
Author’s Note
Dr. Boden is also affiliated to the University of Brighton.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.