
Abstract
The contemporary health subject, often described as a new, empowered patient, is not simply a character in a story of progress toward knowledge and power, away from credulity and passivity. Before the 20th century, and the assertion of a medical system that became frankly paternalistic, laypeople adjudicated on many matters of illness and its treatments. That is, 18th- and 19th-century health subjects were empowered too, and studying them, especially as consumers of health products, helps us develop a more nuanced account of our current medico-commercial selves. Comparing historical advertisements for “patent medicines” and contemporary direct-to-consumer ads for prescription pharmaceuticals, this essay contributes to such an account. It identifies strategies that drug marketers have deployed over centuries to persuade consumers to buy their products, and it tracks a rhetoric of interpellation in advertisements that not only address but also constitute health subjects. The goal of the analysis is to increase alertness to our own susceptibilities to pharmaceutical ads and adjacent rhetorics of health and illness.
Much has been written since the late 20th century about a new sort of health subject: a well-informed and media-savvy agent with choices to make about their own and their family’s care (see, for example, Eysenbach et al., 1999; Eysenbach and Jadad, 2001; Hardey, 2001; Henderson, 2002). Indeed, after decades of growth of social movements for women’s health and disabilities rights, for example, and given the ubiquity of health information, the proliferation of health-communication platforms, as well as an increasingly neoliberal view of health itself, the health subject certainly has become a more powerful agent than they were through much of the 20th century, when they were more fully under the influence of a frankly paternalistic medical system. Lupton and Jutel (2015) report that, in 2014, Internet users had access to over 100,000 mobile apps “designed for the dissemination of health and health information and healthcare and public health initiatives” (p. 128). Conrad et al. (2016) reveal the social consequences of an Internet that is not only informative but also interactive and collaborative; they specify the implications of illness transformed from a private to a public experience.
A study of the relation of drug advertising, on one hand, and the empowered patient, on the other, reveals some ways that current health subjects are not entirely novel beings. An account of persuasive strategies used by drug manufacturers on their publics suggests some continuity in health subjectivity over time. It reveals that, new resources and new technologies notwithstanding, 21st-century health subjects share with their 19th-century counterparts a consumerist attitude and an inclination toward particular health narratives that render them receptive to a catalog of routine appeals made by drug marketers. My research provides rhetorical evidence for an observation made more generally by Tomes (2016): [T]he birth of the patient as consumer lies not in the late twentieth century but rather a full century earlier. While they are completely unaware of it, twenty-first-century Googlers and their kin are indebted to several generations of Americans who sought to become more “educated” or “intelligent” patients, as they described themselves. (p. 3)
The contemporary health subject, 1 in other words, is not best understood as a character in a story of progress toward knowledge and power, away from credulity and passivity. Before the 20th century, laypeople adjudicated on many matters of illness and its treatments. 2 In the 18th and 19th centuries, health almanacs circulated widely in a world where, as Rosenberg (1992) notes, medical “knowledge and competence were not segregated in credentialed heads and hands” (p. 57). 3 The guidance of almanacs was supplemented by the pitches of drug marketers.
My reading of pharmaceutical history and the history of medicine led me to expect that there would be rhetorical correspondences between health subjects of the 19th century and health subjects emerging toward the end of the 20th century. Part of what these publics had in common was an enormous amount of drug advertising aimed directly at them; Conrad and Leiter (2008) describe current direct-to-consumer drug advertising (DTCA) as “harkening back to the patent medicine era” (p. 826). Curiosity about the rhetoric of that advertising brought me to historical materials held at the New York Academy of Medicine Library, the College of Physicians Library in Philadelphia, and the Osler Library for the History of Medicine at McGill University. 4 I studied 18th-century and, especially (as ads became both more compelling and more ubiquitous), 19th-century advertisements for patent medicines. In this essay, I compare these ads with ads for prescription pharmaceuticals covering North America in various media over the past 15 years (when I have been documenting drug ads appearing in wide-circulation magazines and on television—and, then, online). As a rhetorical critic, I turned to Aristotle for the idea itself of a catalog of appeals that can adapt and repeat. My work is in the mode of rhetorical history (or kairology: a temporal account of rhetorical opportunity), performed by rhetoricians of health and medicine, including, for example, Segal (2005), Johnson (2014), Jensen (2016), and Koerber (2018).
The contemporary ads selected for attention here are those with major saturation: for example, ads for Zoloft and other antidepressants and for Ambien and other sleep drugs; ads for somewhat benign top-selling drugs like Lipitor for high cholesterol and less benign top-selling drugs like Humira, a biologic, for, among other things, rheumatoid arthritis. The argument that emerges from the archive, historical and contemporary, is that current health subjects have a rhetorical history with practical implications. Because we are evidently persuaded by the same sorts of arguments used to market medicines in centuries past, it makes sense to isolate those arguments in order to consider our own rhetorical susceptibilities: we can learn to be more cautious about the health we are being sold and the ways we are being sold it.
The project of reckoning with the health subject over time requires an account of pharmaceutical-marketing regulation and its efforts to discipline not only drug manufacturers but also consumers. So I will begin there. I will then describe some rhetorical strategies that captured health subjects a 150 years ago, and that, without much variation, capture us now. 5 The description speaks to a tenet of rhetorical theorists, and Aristotle in particular, that topoi—lines of argument—can be specified and adapted and marshaled toward action in a variety of situations.
The last substantive section of my essay offers as case studies extended ads for two historical products. What is significant about the ads is that the first takes, as an underlying principle, that the expression of a problem—in that case, insomnia—is the entity to be treated, irrespective of its cause; the second argues that many problems, each clinically elusive, are caused by a single agent—in that case, impure blood—and the causal agent is the entity to be treated. The case studies not only provide insight into the macro-items of a rhetorical catalog, they also reveal importantly divergent ways of thinking about illness itself, with counterparts in contemporary health/medicine. The case studies reveal processes of pharmaceutical imagination that may be hard otherwise to see: disease-process accounts may be opportunistic, and logics of classification may be (mis)informed by cultural values.
Pharmaceutical-marketing regulation
The history of regulation of pharmaceutical marketing is well documented (see, for example, Conrad and Leiter, 2008; Critser, 2005; Greene, 2007; Greene and Watkins, 2012; Tomes, 2005, 2016; Young, 1961), and I will rehearse it here only briefly, to make the point that drug marketing has been so aggressive and so influential for so long that it has needed, repeatedly, to be regulated. The point is important, because drug advertising is one way that members of the public learn what their discomforts and miseries might add up to and how to classify their sensations and themselves: what dis-eases might actually be diseases. Healy (2004) argues that the experience of “everyday nerves” is read in the terms of direct-to-consumer advertising for psychopharmaceuticals. Conrad and Leiter (2004, 2008) name DTCA as a key factor in perpetuating the idea that there are medical solutions to life’s problems. Dumit and Greenslit (2006) implicate advertising in the “pharmaceuticalization of culture.” Tomes (2005) writes that the paradox of pharmaceutical advertising—that it is “simultaneously celebrated as a boon to modern medicine and reviled as a social curse—requires an understanding not just of contemporary issues but of historical issues as well” (p. 629).
By the end of the 19th century, many physicians, social critics, and policy makers had become intolerant of the practices of patent-medicine 6 marketers who not only kept the formulas for their tonics secret (“nostrum” is Latin for “ours”) but also made extravagant, and frequently false, claims about their products’ safety and efficacy. The products often derived their effects from alcohol, cocaine, and barbiturates; furthermore, as salves, however temporary, they often kept people from seeking more appropriate medical attention for their ills.
In 1890, the Ladies Home Journal vowed to put an end to patent-medicine advertising in its pages, and the magazine followed with an editorial condemning the “‘Patent-Medicine’ Curse.” In 1905, a harsh blow, though not a death blow, was dealt to the manufacturers and marketers of proprietary medicines with the publication in Collier’s weekly magazine of the first in a series of essays by Samuel Hopkins Adams, exposing the misbehaviors of patent-medicine marketers in a trade that exceeded annual sales of 75 million dollars. The essays would soon be collected under the title, The Great American Fraud (Adams, 1906).
Legislators acted. The Pure Food and Drug Act of 1906 created the Food and Drug Administration (FDA) and established policies and guidelines that were aimed at consumer protection. In 1912, the Sherley Amendment prohibited labeling medicines with false claims intended to deceive the public. The Harrison Narcotic Act of 1914 identified certain drugs as so potentially dangerous that their dispensing required the written prescription of a licensed physician. The year 1938 saw the passage of the Federal Food, Drug, and Cosmetic Act which extended the power of the FDA and created a larger class of prescription-only drugs, further separating “ethical” medicines (for which formulas were on record) from “patent” ones. Subsequent amendments and legislation—the Durham-Humphrey Amendment of 1951, the Kefauver-initiated Drug Amendments of 1962, the Drugs Abuse Control Amendment of 1965, and the Comprehensive Drug Abuse Prevention and Control Act of 1970—placed further limits on drug access and drug advertising.
In the United States, direct-to-consumer advertising for pharmaceuticals, including prescription pharmaceuticals, was permitted, albeit under constraints, into the 1980s, until it fell under an FDA-requested voluntary moratorium in 1982. The moratorium on DTCA was lifted in 1985—over the objections, surprisingly perhaps, of key members of the pharmaceutical industry, concerned that DTCA was “unprofessional” and that patients exposed to prescription-drug ads might run amok with information and cause harm to themselves, putting pharmaceutical companies in legal jeopardy (see Critser, 2005 and Conrad and Leiter, 2008). However, claims to freedom of speech won out, and, after 1985, DTCA increased. Currently, following a 1997 loosening of regulations on DTCA, the United States (along with New Zealand) has the most relaxed provisions for drug advertising in the world. 7
Over a hundred years ago, physician Robert Hessler (1905) complained in the pages of The Journal of the American Medical Association that drug ads directed to doctors in medical journals were no more virtuous than ads directed to the public in popular publications. 8 The need was clearly felt then not only to protect patients directly but also to protect doctors from forces that would keep them from protecting patients. 9 As consumers, we are indeed persuaded, directly and indirectly, by drug marketers at our own risk. People considering Nuedexta (Avanir, 2017) for uncontrollable crying or laughing are advised by the advertiser to call their doctor if they “lose consciousness”—a warning with which it might be difficult to comply. People considering Opdivo (Bristol-Myers Squibb, 2017) for advanced-stage lung cancer are advised that the drug may cause “serious side effects” including death, but the main claim of the ad—that the drug offers “a chance to live longer”—is, on its face, seductive. As Hessler warned, advertising aimed at physicians does not do the job of protecting patients. For example, as is now widely known, between 1996 and 2002, physician-only ads for Purdue Pharmas timed-release opioid Oxycontin made demonstrably false claims about the drug’s safety (e.g. promising low risk of addiction/abuse), claims now blamed, in part, for the “opioid crisis” in North America. 10
Still, there is little that critics can say about pharmaceutical marketers that they have not already said about themselves, with pride. A glance at current periodicals like the Journal of Health Marketing or Medical Marketing and Media makes it clear that advertisers are proud of their ability not only to attract but also to create markets for their products. Angelmar et al. (2007), for example, are keen to advise other marketers of the advantages of “condition-branding”: A strong condition brand enjoys high awareness and strong favourable associations among patients, physicians, payers and other stakeholders. Associations tend to be favourable when a condition is perceived as having serious consequences, for which individuals are not blamed or stigmatised, and which is caused by factors for which individuals are not responsible and over which they have no control … (p. 343)
Notably, experts were dispensing almost exactly the same advice to marketers in 1913: When you write an ad for your own blood medicine you can … convince first and create desire second. That is, convince your reader that his blood really is in bad condition, that he has that “tired feeling,” … then create desire on his part to buy your blood medicine. (O’Connor, 1913: 258)
Physicians and legislators were quite successful at wresting medication control from patients for much of the 20th century. Patent-medicine ads had called to us long ago as sleepless, bloated, anxious, despondent, and sexually disappointed. We answered by consuming medicines. Now we answer, in large part, by consuming different medicines, some carefully keyed to advertised checklists (see, for example, Emmons, 2010, on depression checklists). We might wonder what would have happened if patients had not become disempowered for the 80 years or so between the late 1800s and the 1970s—and if we had become collectively better-educated about the strategies of drug marketers and the risks and benefits of pharmaceutical consumption. 11 It will be interesting to see what effect recent cautions against overscreening, overdiagnosing, and overmedicating 12 will have on health subjectivity and health-product uptake—as campaigns against rampant medicalization and possibly unnecessary medical intervention gain ground. It is a campaign on many fronts, but it co-exists vertiginously with still-aggressive drug advertising and with some experts’ continuing advice that, if knowledge is power (a premise assumed), then acquiring more information enabling more intervention is the powerful thing to do. 13 Consuming drugs for risk conditions and possibly incipient illness then seems apposite too. 14
Drugs ads and their audiences, then and now
The first proprietary-medicine advertisement (“DAFFY’S Elixer Salutis, very good, at four shillings and six-pence per half pint Bottle”) appeared in British America in 1706, according to Young (1974: 1), but ads came prominently to view in North America in the early 19th century, and both products and ads then proliferated exponentially. Ads often took the form of testimonials from satisfied customers; some ads were layered with testimony to the legitimacy of their testimonials. By 1847, 11 million medicine ads ran in 2000 newspapers in the United States (cited in Conrad and Leiter, 2008: 827). Ads appeared not only in newspapers but also on a variety of surfaces we don’t now take to be advertising surfaces at all—like the front and back pages of the substantive books of reputable publishers. 15 There were, as well, dedicated advertising genres: chemists dispensed collectible pharmaceutical trade cards, printed with art on one side and product claims on the other (see Figure 1); 16 ad posters were a form of popular art; and there were medicine shows, often linked to other entertainment, at which manufacturers sold their self-dosage medicines directly to consumers, without the mediation of retailers. 17
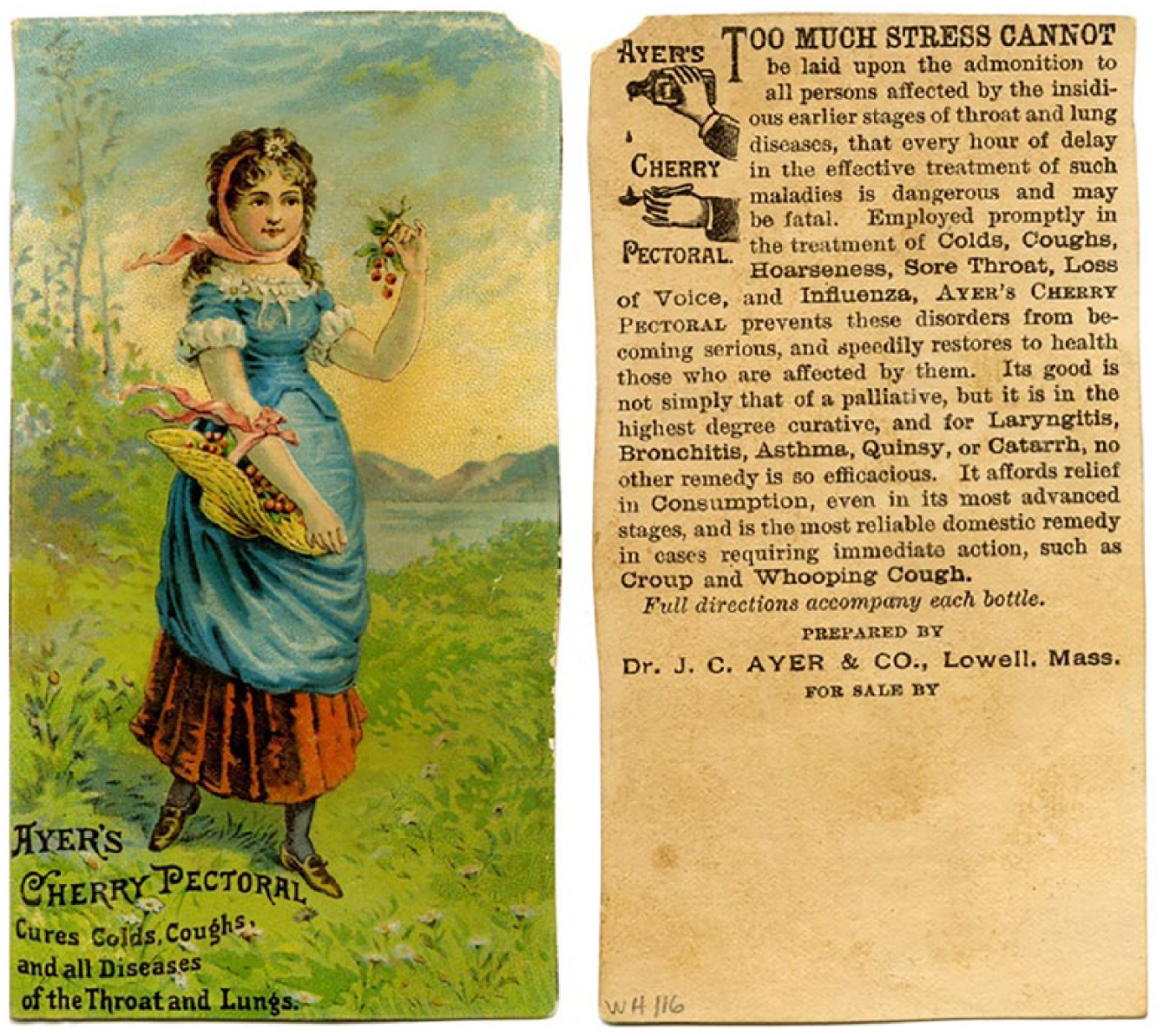
Images courtesy of the New York Academy of Medicine Library.
Meanwhile, pamphlets and even whole books itemized the virtues of single products. These were often imitations of domestic health guides: The cover of The Ladies Handbook and Family Almanac (1885 and 1886) promises “matters of interest” to women and “facts about health,” but the handbook, so-called, is essentially an advertisement for Brown’s Iron Bitters, offered as treatment for headache, indigestion, biliousness, dyspepsia, nervousness, malaria, chills and fever, general debility, pains in back and sides, impure blood, rheumatism, neuralgia, diseased kidneys, liver troubles, and female infirmities (Brown Chemical Company, 1886: 3), the last covering an additional 32 complaints. Drug promotion like this reveals efforts by marketers to establish relationships directly with consumers, and these efforts persist. The strategy is to disintermediate the physician—to remove the physician as the primary locus of health information and services. 18 Notwithstanding the now conventional “Talk to your doctor about [X]” that is part of DTCA, the fact that consumers elect to talk to their doctors about some X is a sign that the doctor has already been, to some extent, disintermediated: the doctor is already not the first person who is generating options for addressing the patient’s complaint. 19
In comparing patent-medicine ads to contemporary DTCA, we observe two interacting persuasive processes. The first concerns the strategies themselves that marketers deploy to convince consumers to buy their products—a catalog of specific topoi (all explored below): identification, flattery, authority, statistics, friendship, anticipation, degree, and social obligation. The second is the process of interpellation: the constitution of consumers, through special hailings that audiences for pharmaceutical ads answered and still answer. 20 Drug ads address us as peers (of the marketers themselves) and as at least a little bit sick. Imagine, then, the 19th-century subject now, at the end of the second decade of the 21st century. She (in this case) is sitting (or, if she has read the latest health studies, standing) at her computer—different hair, different outfit, different research skills, better resources, more of them, but with many of the same complaints, and, more than one might expect, much of the same vulnerability and desire. She participates in the same sort of illness narrative. In the 19th century, Lydia Pinkham’s vegetable oil 21 for women’s complaints helped to constitute a female health subject that might now consider Serafem for her Premenstrual Dysphoric Disorder (Greenslit, 2015), Addyi for her sexual “dysfunction” (Segal, 2018), and Gardasil … for her daughter (Malkowski, 2014).
We—the advertiser, the testifier, and the public—are all companion humans, in this view; drug ads depend, in the first instance, on a rhetoric of identification, as that rhetoric is articulated by Burke (1969): “You persuade a man only insofar as you can talk his language by speech, gesture, tonality, order, image, attitude, idea, identifying your way with his” (p. 55; emphasis in original). “Persuasion by flattery,” Burke continues, “is a special case of persuasion in general” (p. 55). Drug advertising has long flattered consumers that they, like the advertisers, are empirical sorts of people. An ad for Hood’s Sarsaparilla (n.d.) says, “The people are quick to recognize true merit, and this is why the sale of Hood’s Sarsaparilla far exceeds all similar preparations.” The 21st-century candidate patient for Lyrica to treat “the widespread pain of fibromyalgia” is addressed as someone accustomed to being “on top of things” (Pfizer, 2017). Moreover, the consumer, then and now, is addressed as someone who recognizes an expert when they see one. One of the trade cards for Brown’s Iron Bitters (n.d.) features a quotation from “a leading Medical Professor,” speaking about the importance of Iron. The quotation finished, the card’s narrator resumes: “With such medical authority the use of Iron cannot be too strongly urged.”
Consumers have not tired of the appeal from medical authority: we typically value the imprimatur of an apparent expert. In a popular, and persuasive, advertising campaign, Dr Robert Jarvik, inventor of the artificial heart, was the face and voice of cholesterol-lowering Lipitor (Pfizer, 2008)—until the manufacturer withdrew the ad in response to FDA censure: while Jarvik was an expert on artificial hearts, he was not a cardiologist, an expert on real ones.
Advertisements for Iron Bitters and for Lipitor, over a hundred years apart, are evidence of more than our enduring embrace of authority: we have a propensity also to admire the isolation and measurement of metabolic materials. We like to see numbers raised (as in the case of iron) or lowered (as in the case of cholesterol). We take numerical rising and falling to be signs of something pertinent to our health, which they may or may not be (see Greene, 2007).
Statistical appeal itself is common today as it was in the 19th century—as a means of normalizing the pathological while pathologizing the normal. An ad for Burdock’s Blood Bitters (n.d.) notes, “There are thousands of females in America who suffer untold miseries from chronic diseases common to their sex.” Compare that appeal to the contemporary condition branding that recently prepared the market for Addyi to treat “Female Hypoactive Sexual Desire Disorder.” Frequently cited in promotions for Addyi has been the impressive, albeit recanted, claim, from a JAMA article by Laumann et al. (1999) that 43 percent of women suffer some form of sexual dysfunction. Advertisers deploy statistics also for a bandwagon effect: Chloralamid (Lehn & Fink, 1890) boasts that sales soared from 200 g to 20,000 in a month; Humira (Abbvie, 2018) boasts that dermatologists have prescribed the drug for 10 years, “with more than 250,000 patients treated.”
While scientists and physicians are foci for appeals of authority, drug ads sometimes make a point of undermining professional authority, suggesting that the companies themselves are actually the superior support, the true friends of the patient. Burdock’s Blood Bitters sets up a story of suffering in which only the pharmaceutical company itself (and not the physician) can be counted upon to listen to and understand patients. The text of one of Burdock’s ads has an intimate tone and a leisurely pace; it defines an audience and addresses it directly, under the banner, “
The historical health subject was addressed not only as a savvy sort of person but also as a vigilant one, who does not wait to get very sick before seeking treatment. Being a good health consumer meant, and still means, anticipating illness—medicating before you are properly, and perhaps irretrievably, ill. Early diagnosis and treatment begin with self-surveillance. This is an attitude we readily associate with 21st-century medicine, and it has been particularly well documented by Greene (2007, 2012) and by Adams et al. (2009). Regimes of anticipation, however, have important precedents in patent-medicine advertising of the 19th century. An ad for Hartshorn’s Sarsaparilla (n.d.) warns, “The first deviation from perfect health should receive attention. Even feeble people attain long life by the use of simple remedies in season.”
Hartshorn was one of many 19th-century marketers to encourage early intervention—hailing a health subject who is ready to medicate prophylactically. A trade card advertising Ayer’s Cherry Pectoral (n.d.) (Figure 1) says, “
Aristotle identified degree (“greater and less”) as a common line of argument. Currently, prescription-drug advertisers appeal to patients through magnification: you thought you just had indigestion, but maybe you have gastroesophogeal reflux disease (GERD); you thought you were just bloated, but maybe you have irritable bowel syndrome (IBS); you thought you were just shy, but maybe you have social anxiety disorder (SAD). 24 Ads for non-prescription medicines typically reverse the appeal. For example, GERD is not mentioned in ads for non-prescription medications for indigestion. An iconic example of a minifying approach for a non-prescription drug is this 1933 ad for Phillips Milk of Magnesia: “He Spent His Days Worrying About a ‘Disease’ He Didn’t Have. Thousands of People Who Think They Have ‘A Serious Disorder’ Have only ‘Acid Stomach’ Now Easily Relieved” (Chas H. Phillips Chemical Company, 1933). For their part, 19th-century ads danced the topos of degree in both directions: your discomforts are symptoms of a disease you can treat yourself, with our product, BUT, if you neglect these symptoms, and don’t purchase the drug, you could become quite sick indeed.
Patent-medicine ads addressed consumers not only in their individual bodies but also in their social roles. Much like the 2005 Zoloft ad that targeted mothers for failing their children by not being cheerful enough (“Mommy, you’re no fun anymore,” complains a bean-shaped child, prompting its bean-shaped mother to visit her bean-shaped doctor to “ask … about Zoloft” (Pfizer, 2005)), 19th-century ads addressed patients in their lived contexts and advised them on what sort of people they should be. This is Burdock’s Blood Bitters again, on a trade card, under the heading, “
Practices of self-dosing did not end, of course, once professional authority was asserted and legislation began to restrict the advertisement of patent medicines. By the mid-20th century, however, people had become increasingly removed from decision-making about their own care. As health subjects rose again as more autonomous agents in the last decades of the 20th century, they irresistibly brought to their role a persuadability forged in the language of pharmaceutical advertisers. Moreover, as we have seen, it was a moral language as well as a biological one. We were all a little sick and we were all obligated, to ourselves and to our loved ones, to have as much health as possible. Many pharmaceuticals are now aimed at acceptable pleasures (the pleasures of productivity and sociality, for example), and the products are, notwithstanding the recent appearance of targeted “designer” drugs, ironically, again, frequently “cure-alls”: Before Bayer was forced, in 2011, to withdraw overstated claims about its birth-control product, Yaz (Bayer, 2008), the drug was said to relieve “emotional and physical premenstrual symptoms,” including irritability, moodiness, feeling anxious, bloating, increased appetite, fatigue, headaches, and muscle aches; it would also induce weight loss and clear the skin.
Two case studies of patent-medicine advertising: macro-strategies less visible
Chloralamid Schering was advertised as a Hypnotic, for the treatment of sleeplessness. Its promotional pamphlet saw three editions, the third published in 1890. The pamphlet is rhetorically elegant: scientific and at the same time genteel, like a good physician. Being genteel, the copy overstates its case mainly by understating it. It takes care to note, for example, that one of 25 people in the subject group did not respond to the hypnotic. Reportorial even-handedness becomes the backdrop then for extravagant claims. Importing the style of the clinical case report, the pamphlet tells, for example, of Regina H, age 69, who “slept so soundly that she could be washed and have her toilet arranged without waking up” (Chloralamid, 1890: 3). The main text is a series of short articles by endorsing physicians, who speak as scientists. The physicians write under titles like, “Chloralamid a Valuable Addition to Therapeutics,” reproducing the rhetoric of the medical-journal article.
Much of the evidence for Chloralamid’s value is presented proleptically: objections are anticipated and answered, not only to the product but also to the pamphlet. The advertising is both rhetorical and meta-rhetorical. It is not only about the drug; it is also about the selling of the drug: it is about itself. For example, one endorser writes, “Although it may seem superfluous at first sight—considering the proportionately large number of hypnotics—to busy ourselves with new ones … we must nevertheless come to the conclusion … that such action cannot prove useless” (p. 10).
The most significant act of the pamphlet, however, is to call forth a patient, formed in the very act of address. This patient is sick in both a specific and a nonspecific way: her sleeplessness may be the result of “nervous excitement, heart troubles … or asthma …,” but she is, most saliently, sleepless. She is not, in the first instance, compromised by weak nerves or heart or lungs. She is an insomniac; her sleeplessness, not any precipitating condition, is her complaint. The figure of the insomniac stays with us, poised for relief, and, in the 21st century, she is the target of treatments now aimed at getting her, irrespective of anything else, productively to work in the morning. A widely circulating magazine ad for the prescription sleep drug Ambien was not about sleeping so much as it was about having slept and being ready for work the next morning (Sanofi-Synthelabo, 2005). The ads featured a split image: an office setting, featuring a woman at work (“A full day …”)—and a bedroom with slept-in bed (“starts here”).
A second extended 19th-century advertisement provides a structural counterpoint to the Chloralamid example. The author/marketer is Dr William Swaim (1828), and the document is his book-length Treatise on Swaim’s Panacea, Being a Recent Discovery for the Cure of Scrofula, or King’s Evil, Mercurial Disease, Deep-Seated Syphilis, Rheumatism, and All Disorders Arising from a Contaminated or Impure State of the Blood, with Cases Illustrating Its Success. Swaim’s luxurious title itself is important: the book is advice to consumers whose suffering is otherwise disorganized. Scorfula, syphilis, rheumatism, and so on, Swaim says, are “disorders arising from a contaminated or impure state of the blood.” Within the title itself is a course of action: the blood, of course, must be purified.
Whereas, in the case of Chloralamid, insomnia was the disorder to treat, irrespective of its cause, here, in the case of Swaim’s Panacea, cause is everything: this ad works in the opposite direction. The question is not, what is the symptom of your disease? Rather, what is your dis-ease a symptom of? The reversal is important. Someone who lacks sleep may, for that reason alone, be a willing candidate for treatment. However, someone with scrofula (a tubercular lymphatic cyst) or rheumatism may have abandoned hope and require a new narrative if they are to enroll for treatment. The purification of the contaminated is that narrative. Each drug casts the widest possible net. The hypnotic hails the sleepless subject as ambiguously ill; the Panacea hails the ill subject as storied, and the patient is a character in a narrative that involves the medication itself as agent. Even though Swaim’s Panacea was useless in the treatment of most of the conditions for which it was advertised, an illness narrative that centrally included a pharmaceutical agent was constitutive of the 19th-century health subject, that narrative and that patient, in some form, endure.
Significantly, the divergent approaches to illness represented by the Chloralamid hypnotic and Swaim’s panacea, respectively, have classificatory counterparts in contemporary medicine. In the logic of Chloralamid, for example, although “fat” bodies may be the result of hormones, lifestyle, microbiomes, infrastructure planning, and so on, fatness itself is generally understood as the condition that needs to be corrected. Contrastingly, in the logic of Swaim’s Panacea, for example, since cancer, dementia, and Parkinson’s (and other diseases) are most commonly diseases of old age, it is old age that needs to be cured. The rhetoric of the extended ads indicates the role that cultural values, and their exploitation in marketing, play in our understanding of health and illness and how they are organized for action.
Conclusion
Like so many illness narratives that circulate publicly now, 19th-century patient accounts have pleasing arcs of restored health—and the happy ending is part of the constitutive narrative of the health subject. The health subject is a person who, through an intervention, notably a pharmaceutical intervention, becomes, if ill, then well again, and, if not ill, then better than well. 26 The health subject is part of an historical narrative with an impressive teleology. That is, not just the advertising itself, but the particular form that much of the advertising took in the 19th century—the testimonial as an illness narrative with a happy ending—went a long way to constitute the health subject. In the second decade of the 21st century, installed at their computer, the health subject is not an ahistorical free agent empowered by the astonishing amount of information they can access with a keystroke. They are determined in part by their role in a narrative that has them seeking particular sorts of information and intervention in the first place.
The 21st-century health subject is new, of course, by virtue of being both a product of social movements and technologies that have, at the very least, increased their access to good and much health information and constituted them as a technological form of life: a life form in which the computer is both prosthetic and transformational. 27 They are not, however, always more advantaged consumers than their 19th-century counterparts. 19th-century health subjects picked up trade cards, at the chemist’s; their domestic health guide represented knowledge and assumptions that patients shared, for the most part, with doctors; they consulted family members and friends about matters of health; they stood among others at medicine shows, and perhaps complained, or vomited, to specify their conditions. Notwithstanding their well-documented susceptibility to the appeals of advertisers, and an apparent credulity from which many critics of patent-medicine advertising were determined to save them, the 19th-century consumer was, as Strasser (2008) reports, not simply an “ignorant or superstitious dupe”: they “interpreted the commercial messages [they] received, and acted upon those interpretations, not necessarily on the intentions of the advertisers” (p. 93).
We are, arguably, socially more isolated than our 19th-century counterparts, though we are virtually, as Conrad et al. (2016) have demonstrated, more public in our illness experience. It remains for us to finesse the relation between health and consumerism, and seek further to acquire practical wisdom (phronesis) about both. That project includes developing the means to evaluate the claims of advertisers, whose tactics, as we have seen, have not much changed in 150 years.
Footnotes
Acknowledgements
The author gratefully acknowledges Nan Johnson for generous gifts of carefully collected almanacs and ephemera. The author also acknowledges her research assistant, Anna MacDonald.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author acknowledges funding from the Social Sciences and Humanities Research Council of Canada (grant #410-2011-0259).