
Abstract
The health of sex workers is considerably influenced by their position in society and by the marginalisation and stigmatisation they face worldwide. They are frequently criminalised and labelled as deviant, disordered or ‘vulnerable’: stereotypes that simplify and misrepresent their realities. Sex work policies create social and structural barriers, creating dangerous work environments and exacerbating significant health inequalities. Health organisations and their policies play an important role in highlighting inequalities and guiding health systems in reducing them. In this article, we use a document analysis design to analyse how and when sex workers are depicted in policies and publications by English national health organisations: National Health Service (NHS) England, Public Health England and the National Institute for Health and Care Excellence, along with the UK Department of Health. We find that sex workers are largely absent in these documents and, when present, are depicted not using evidence, but simplistically with moralistic undertones. The dichotomous constructions found in these texts: vulnerable yet also criminal ‘prostitute’ reflect wider political and social constructions of sex working women. This not only obscures their realities but also homogenises, blames and stigmatises, ultimately doing the opposite of what these organisations purport to do: it damages their health and well-being.
Introduction
Health policy plays an important role in providing services to meet the needs of populations and groups, including sex workers. The health and well-being of sex workers are of global concern, yet are frequently overlooked by sex work policy, exacerbating health risks (Reeves et al., 2017). In the United Kingdom, sex work public policy is criticised for homogenising and obscuring sex workers’ health needs (Carline and Scoular, 2015). An analysis of how health organisations represent and discuss sex workers in their policies and publications is missing from academic literature. Therefore, in this article we review and analyse these documents published by health organisations in England. We provide a critical overview of how sex workers are represented in these official texts and the implications for their health and well-being.
Sex work is a term used to describe ‘a range of activities relating to the exchange of money (or its equivalent) for the provision of sexual services’ (Balfour and Allen, 2014: 3). We use this term to avoid the negative connotations of the term ‘prostitute’ and to highlight the diverse nature of this ‘range of activities’ and of the individuals involved. We discuss the complexities of terminology later in this article.
Approaches on the ‘management’ of sex work differ worldwide, with various attempts to abolish and criminalise sex workers and/or clients or conversely to decriminalise or legalise the practice. These policies mirror academic and feminist debate. For the sake of brevity, this can be simplified to a polarised ‘sex wars’ between those that regard sex work as patriarchal violence against women and those that argue this approach runs contrary to sex workers’ rights, voice and homogenises experiences (Ferguson, 1984; Sanders, 2016). Despite multiple perspectives on the legitimacy of sex work, this continuum of views often features violence towards sex workers and their perceived well-being as central to their arguments.
In the United Kingdom, while sex work is not illegal, many associated acts are, for example, ‘soliciting’, ‘kerb-crawling’ or maintaining a ‘brothel’, and sex work is therefore in practice effectively criminalised. Commentators globally argue that criminalisation is damaging to sex worker’s health and safety (Amnesty International, 2016; Grenfell et al., 2016; Lancet, 2015). The stigma towards sex workers and their enforced hidden nature is thought to create a ‘discourse of disposal’ increasing the risk of serious violence or murder (Lowman, 2000: 1003). Sanders (2016) argues that the factors perpetuating this violence are not inherently their work, but in their environment, the justice system and their social status – factors negatively affected by criminalisation. These factors alienate sex workers from mainstream society. Scambler and Paoli (2008) discuss the ‘near-universal…attributions of shame and blame’ functioning as barriers to healthcare globally (p. 1859).
Sex work policy in the United Kingdom is criticised for marginalising sex workers, creating structural and social factors that endanger their health, well-being and lives. Sex workers are subject to ‘zero tolerance’ approaches, conceptualising them as ‘fallen women’ requiring stately assistance or ‘enforced welfarism’ (Carline and Scoular, 2015; Sanders, 2009). This victimhood trope focusses on ‘vulnerability’ and strays towards a narrative where sex work is a ‘problem’ and sex workers are in need of control (Brown and Sanders, 2017). Labels of deviance, risk, and vulnerability and ‘othering’ marginalise this group and converge into dichotomous constructions of ‘the sex worker’ as disordered yet vulnerable, ‘public nuisance’ yet innocent victim (Kantola and Squires, 2004; Sanders, 2009). Weitzer (2010) denounces prohibitionist policies as ‘pre-scientific’, advocating for policy that is evidence-based. UK sex work policy is similarly criticised as not being based on evidence and instead on moralistic or ideological views of the rights or wrongs of sex work and workers.
Sex workers are a heterogeneous group of individuals. Yet, alongside occupational causes, their position in society generally results in unmet needs and health inequalities, persistent in varying degrees throughout the world. Sex workers are at a significantly increased risk of serious violence and murder (Deering et al., 2014; Potterat et al., 2004). Complex circumstances intersect with social exclusion and stigma, causing harm to mental and emotional health, exacerbated by the risk and reality of violence (Sanders, 2004). Occupational hazards play a role in sexual health, compounded by issues of power and status potentially affecting their ability to protect themselves against infections or from accessing appropriate care (Ahmed et al., 2011; Overs and Loff, 2013; Scambler and Paoli, 2008). Substance misuse is more common and significantly heightens health risks and stigma (Benoit et al., 2015; Jeal and Salisbury, 2013). Sex working mothers are poorly recognised in healthcare, despite this being common (Jeal and Salisbury, 2007).
Research into the health of sex workers in the United Kingdom highlights similar findings. Violence against sex workers in the United Kingdom is sadly well-documented (Kinnell, 2008; Phipps, 2013; Sanders, 2016). Evidence indicates an increased risk of mental health problems, sexual health conditions, substance misuse and poor health in general (Balfour and Allen, 2014; Jeal and Salisbury, 2004, 2007; Jeal et al., 2017; Mc Grath-Lone et al., 2014). Both stigma and marginalisation lie at the root and exacerbate these issues, with access to healthcare generally poor (Jeal and Salisbury, 2013; Mastrocola et al., 2015).
Importantly, however, not all forms of sex work carry the same risks. Sex work is diverse, with different environments, circumstances and associated issues (Harcourt and Donovan, 2005). For example, in some (high-income countries) the more common ‘indoor’ work is associated with less violence, substance use and risk overall than ‘street’ work (Hubbard and Prior, 2013; Jeal and Salisbury, 2007; Sanders and Campbell, 2007). Migrant sex workers and men, transgender or non-heterosexual individuals work in different circumstances and have different needs (Baral et al., 2015; Platt et al., 2013; Smith and Laing, 2012). This diversity is frequently omitted in sex work policy. Finally, there lies an important distinction between designating all sex workers as victims, instead of understanding the varying risks of becoming victims of violence, abuse or ill health. This is important, as one recognises unmet need and the other potentially obscures that need by not recognising diversity and the social and structural mechanisms behind any potential vulnerabilities.
Health organisations have an opportunity and responsibility to recognise, highlight and reduce these health inequalities. Health policy plays an important role in identifying the direction and priorities of health organisations and therefore whether or how sex workers have access to the right care for their needs.
Definitions of ‘policy’ are varied and nebulous. ‘Policies’ consist of decisions, actions, non-decisions and inaction and manifest in many ways, not necessarily comprising a document (Ham, 2009; Ritsatakis et al., 2000). They reflect the politics, values and power structures of the policy elite (Buse et al., 2012). Health policy therefore sits in an interesting position, on one hand having the responsibility to improve the health of the population and on the other hand reflecting the ideological perspectives of a political stratum. We do not intend to comment on the complex debate on the existence (or not) of evidence-based public policy, but aim to contribute the important question of how health policy in England represents sex workers and how this could affect their health and well-being.
In England, national health policies are produced by the Department of Health (DH) and its ‘Arm’s Length’s Bodies’ (ALBs). ALBs discussed in this article: NHS England (NHSE), Public Health England (PHE) and the National Institute for Health and Care Excellence (NICE) all play key roles in health service provision and access, commissioning, population health and standards for care throughout England. They play key roles in reducing health inequalities and, alongside the DH, repeatedly state this as a priority. This ‘need to reduce [health] inequalities’ is enshrined in law (Health Social Care Act, 2012). These organisations also state their dedication to evidence. PHE states, for example, ‘all our work is informed by…evidence’ (Public Health England (PHE), 2015: 5). While the debate on the existence or feasibility of evidence-based policy is complex (see, for example, Smith, 2013), these organisations make a clear mandate to use evidence to reduce inequality.
In this article, we undertake a document analysis of publications released by the UK government DH and ALBs: NHSE, PHE and NICE. The absence of an overarching sex workers’ health policy means that these documents are not necessarily designated as policy. We argue, however, that these documents contain reflections of policy-makers and of those decisions and non-decisions, actions and inactions, perspectives and values that ultimately constitute policy.
Methods
We are interested in how English national health publications discuss and portray sex workers. By selecting a systematic search methodology, we aimed to analyse a cross-section of documents containing every reference to sex work or workers in a 6-year period, from 2010 to May 2016. This period has salience due to the UK’s 5-year political cycles, with the previous Government taking up post in 2010.
Sex work/workers and synonyms were searched in gov.uk (which hosts both DH and PHE online platforms); england.nhs.uk and nice.org.uk. Synonyms included sex trade/industry/market; prostitute/ion. Where possible, terms were combined using Boolean functions and/or truncation. All resultant publications were screened for relevance.
Systematic searches for grey literature have no ‘gold standard’ with a less standardised methodology than academic searches (Godin et al., 2015). To increase trustworthiness, further systematic searches using the same criteria were undertaken. Databases were chosen because of their relevance to grey literature. They included the following:
NICE evidence search (www.evidence.nhs.uk) advanced search. Filters: ‘commissioning guide’; ‘evidence summaries’; ‘guidance’, ’policy’; ‘service development’; ‘patient information’.
Social Care online search (www.scie-socialcareonline.org.uk) – advanced search. Filters: ‘government publication’; ‘legislation’; ‘consultation document’; statutory guidance’; ‘practice guidance’; ‘practice examples’; ‘standards’.
Opengrey.eu.
Google Advanced Search.
Inclusion and exclusion criteria were set. Any document containing any search term, published between 2010 and May 2016 by NHSE, PHE, NICE or DH was included. This incorporated instances where these terms arose in quotes from individuals, but only when not used for research or illustrative purposes. Exclusion criteria were publications from countries outside the United Kingdom and commissioned documents. This latter criterion is critical, as the DH commissions documents written by academics or other health organisations. These documents have been excluded from this study as their status in relation to both policy and academia is unclear.
We analysed the documents using a combination of content and thematic analyses, concurrently assessing the context of the search terms, that is, desired readership and publication topic. While content analysis and thematic analysis are sometimes regarded as interchangeable, we conceived content analysis as achieving an additional descriptive layer of reliability by quantitatively assessing terms, document types, repetition and terminologies. We analysed the documents using a descriptive search for the frequency of all accounts of sex workers (Bauer, 2000). The physical units of analysis were the documents themselves, and the semantic units we counted were those features of text that involved any mention of sex workers. This involved a practical process of reading all documents identified in the search and highlighting all references to sex workers which were then cut and pasted into a framework and coded under a theme (see section ‘Results’). N.P. developed the codes and J.B. checked for consistency and interpretation. This process is, of course, a matter of our judgement, and while we acknowledge this as a limitation, there was consistency in our interpretation of these themes between the two of us. The themes were informed by our interpretation of the text and the judgements we think are apparent in the text (Bauer, 2000). This was an inductive process, augmented by a recursive activity where ‘hunch, clue, metaphor, explanation or pattern is imagined or recalled from existing theory to make sense of the data’ (Carter et al., 2009: 106).
Results
This search strategy found 34 documents none of which relate directly to sex workers. This highlights the absence of sex workers in health policies and is noteworthy, especially when put into context of the thousands of documents published by these organisations over the same period. Furthermore, in 21/34 documents, sex workers arise only in a list alongside other groups, with no further discussion or explanation. This lack of visibility, recognised throughout sex work research, risks exacerbating negative stereotypes and myths (Cusick et al., 2009). Their lack of presence here, we argue, in itself constitutes a ‘policy’, but by non-decision and inaction.
The themes emergent from these documents are displayed in Figure 1. Underlying tropes are the absence of sex workers, gender assumptions and the terminology used. The case studies presented of part of their content function as useful examples of how these themes intersect to conceptualise sex workers in these documents.
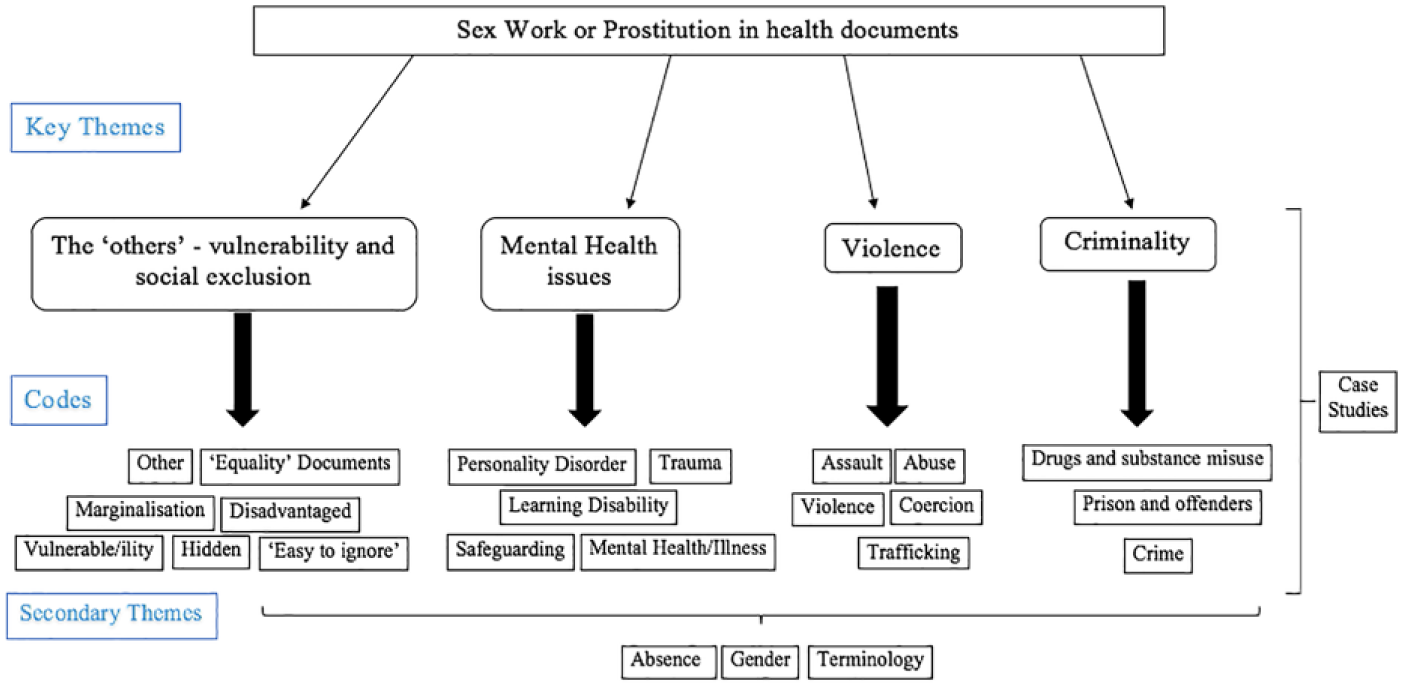
Outline of themes.
If viewed in a vacuum, sex workers’ presence in documents pertaining to (in)equality, substance misuse, mental health, violence and women’s health are not surprising and even welcomed. These are issues that are described by this group of individuals. The key point is that these documents constitute the sole representation of sex workers and therefore lead the readership into assumptions about this population through the language and stereotypical depictions presented.
Terminology is important, as there are implications to these terms. Twenty-two documents use the term sex work/er, eight use prostitute/ion and four use both. The term ‘prostitution’ is associated with ‘shame, unworthiness and wrongdoing’ (Bernstein, 1999: 111). ‘Sex work’ implies a perspective where sex work is work, thus portraying a viewpoint that is also not universally accepted, although avoids the negative connotations of ‘prostitute’. In these documents, a pattern emerges. ‘Prostitute/ion’ tends to be in relation to more negative subtexts, for example, substance misuse, crime, coercion or assault. ‘Sex work’ tends to be in more neutral circumstances, frequently when referring generically to ‘other groups’. The singular use of ‘rent boy’ will be discussed further below. This different usage of terms suggests an underlying implicit understanding of the value-judgements assigned to them. Conversely or perhaps additionally, especially where both are used in one text, it implies a lack of understanding of the use and meaning of such terms, suggesting an overall ignorance of this topic.
The sex worker as ‘other’
There is a recognition that sex workers face inequalities in these documents. The UK Equality Act (2010) and legislation requiring ‘regard to’ health inequalities (Health Social Care Act, 2012) have spurned a plethora of so-called ‘Equality Impact Assessments’ (EIA). The worth of these documents has been called into question (former British Prime Minister, David Cameron, called them ‘bureaucratic nonsense’ (Cabinet Office, 2012). Yet, it is in these documents or similar that sex workers arise in a third of cases (11/34). In these documents plus in a further 10 and therefore in the majority of the texts (21/34) sex workers arise solely in lists of groups variously described as ‘disadvantaged’, ‘marginalised’, ‘socially excluded’, ‘hard-to-reach’, ‘vulnerable’, ‘hidden’ and, once even, ‘easy to ignore’. These lists include fellow marginalised groups, typically ‘refugees’, ‘homeless’ or ‘traveller communities’. While a discussion of sex workers’ vulnerabilities or exclusion is welcomed, these lists risk compounding the issue of their absence, as they recognise inequality, yet lack this meaningful discussion. These are lists of ‘others’, even designated as such (‘other disadvantaged/vulnerable groups’) almost encouraging the process of ‘othering’, identifying them as ‘different’ and potentially perpetuating marginalisation. These discourses of vulnerability and exclusion also carry undertones of social control.
Brown’s (2014a, 2014b) work on ‘vulnerability’ voices concern about these ‘subtle mechanisms of social control’ (p. 371). While it is of potential advantage in, for example, receipt of benefits, this concept can be related to ideas of power, stripping the voice and power from those already marginalised, exacerbating stigma and labelling and creating a social hierarchy with the powerful and the vulnerable at two ends of the spectrum. Brown and Sanders (2017) relate this directly to sex workers, where this narrative risks exacerbating moralistic agendas in which sex workers are deemed a risk to themselves and others. This is reflected in our documents where the following is reported: Understanding the vulnerabilities associated with prostitution and sex workers
In only one document, the DH’s Framework for Sexual Health Improvement in England (2013), is there a recognition and discussion of structural causes of vulnerability and poor health. Sex work is otherwise described as a ‘behaviour’. First, in relation to symptoms of personality disorder: … impulsivity and self … impulsive acts of recklessness … (e.g. substance misuse, prostitution, suicide attempts). (p. 139)
Second, in relation to poor access to services: … behavioural characteristics, for example illicit drug use or commercial sex work … (National Institute for Health and Care Excellence (NICE), 2014a: 2)
These highlight individualistic concepts of blame and ‘behaviour’. They also introduce the concepts of the sex worker as mentally unwell, and the sex worker as a criminal.
The sex worker, mental health and consent
Sex workers are directly associated with mental health or disability in four texts, most notably learning difficulties or personality disorder. In a further four, they are listed alongside ‘mental health issues’ (and other causes of ‘vulnerability’). The conflation of sex work and mental health or disability issues raises serious concerns as we will illustrate through the UK Government’s Care Act Statutory Guidance case study of Miss P. Miss P is introduced as a person who does not have capacity to consent and: Miss P was being coerced into prostitution and physically assaulted. (Department of Health (DH), n.d.)
The issue of consent, disability and ‘prostitution’ as conceptualised in this case study is very problematic. We have earlier introduced the ‘sex wars’ debate: put simply, the ‘sex-work-as-work’ versus ‘prostitute-as-victim/prostitution-as-violence-against-women’ debate. The sex workers’ rights movements ‘resist accounts that cast them as mere victims’ (Scoular, 2004: 346), arguing it constructs sex workers as ‘devoid of choice, responsibility or accountability’ (Maher, 2000: 1). Sex work is legitimate work, only achievable with consent. The latter view conceptualises sex work (or prostitution) as inherently a violation against women’s rights, and argues that they are always coerced regardless of context (see, for example, Jeffreys, 2010). The implication in this case study is that consent is irrelevant to ‘prostitution’ status, which links to this latter view. Irrespective of these dichotomised views on consent, the description of Miss P and her status as a ‘prostitute’ obscures her inability to consent and fails to acknowledge that, regardless of her status as a prostitute (or not), sex without consent is rape. This conflation between consenting sex work and non-consensual sex (or rape) has similarities to the debate on what was previously called ‘child prostitution’, which is now recognised to be a damaging misnomer due to the inability of children to consent and correctly renamed ‘child sexual exploitation’ (CSE) (Crellin, 2015).
Despite these issues, this case study does at least imply a recognition of a distinction between coerced versus non-coerced ‘prostitution’. This is not always the case in these documents, as we will now discuss.
Sex work as violence
The conflation of sex work with violence, abuse or trafficking is a common theme in sex work literature (Kempadoo et al., 2015; Lancet, 2015; Weitzer, 2007). Trafficking or CSE are widely recognised as human rights’ violations requiring global policy and action, however conflation with sex work ignores the different experiences of those involved. It again misrepresents the difference between consensual sex work and non-consensual abuse, with potentially damaging effects around sex workers’ ability to report rape or violence (Sanders, 2016). These conflations and misconceptions are replicated in these documents.
Eight documents associate sex work and violence, recognising that sex workers not only have an increased risk of violence, but also depicting sex work as violence. Two documents, both from ‘Health & Justice’ (H&J), list the following: … advice for sex workers and those who have been subjected to domestic violence and abuse. (Guite et al. for PHE, 2014a: 6) … support for those who may have been victims of domestic abuse or sex workers. (PHE, 2014b: 17)
A ‘Liaison & Diversion’ (L&D – a service for offenders with issues around mental health, learning disability or drugs) document quotes: … experiences of domestic violence, sexual violence, prostitution and human trafficking. (NHSE, 2014: 8–9)
Despite not defining sex work as abuse, there is an implicit association between sex work and violence in these statements. Going a step further, the EIA accompanying the DH’s (2010c) Improving Services for women and child victims of violence explicitly states, [Violence against women] includes domestic violence, forced marriage, ‘honour’ crimes,
This clearly defines all ‘prostitution’ as violence, putting it in apparent parity with human rights’ violations and violent crime.
The final two documents discussing sex work in relation to violence (both regarding sexual violence) do so in passing, under ‘other services’, in a list of ‘key informants’ and under ‘data sharing’ (DH, 2011: 13,17; NHSE, 2015 1 :19). This further underlines the lack of presence in documents where special attention to sex work is perhaps warranted. In no document is there a discussion of the heightened risks of violence for sex workers, the potential health impacts or management.
The sex worker, mental health and crime
The further three documents where sex workers are discussed directly in relation to mental health, do so in relation to the criminal justice system and, predominately, personality disorder. Two documents are from L&D, who provide services for offenders. The third is guidance for ‘working with offenders with personality disorder’ (Motz et al., 2015). These documents imply mental health conditions are the cause of sex work:
… prostitution and sex workers … recognising depression, anxiety and personality disorders which may have gone undiagnosed. (NHSE, 2014: 9) … with a history of borderline personality disorder and depression … involved in street prostitution. (NHSE, n.d., no page numbers)
The following two in relation to symptoms of personality disorder: impulsive acts of recklessness as a means of emotion regulation (e.g. substance misuse, prostitution, suicide attempts). (Motz et al., 2015 for PHE and National Offender Management Service, p. 139) impulsivity and self-damaging behaviour (substance abuse, prostitution, self-harm and suicide attempts). (p. 10)
The relationship to borderline personality disorder is interesting. Feminists and sociological commentators contest this psychiatric diagnosis on the grounds that it is the modern ‘hysteria’, disproportionately associated with ‘femininity’ and ‘emotionally unstable’ women (Rogers and Pilgrim, 2014; Ussher, 2011, 2013). Women deemed ‘mad’ have long been associated with ‘promiscuity’ (Chesler, 2005). These accounts of deviance and sexuality seem to coalesce both in accounts of sex workers and in accounts of women and ‘madness’, both pathologised due to a perceived deviation from ‘socially acceptable’ behaviour for women. Their co-presence in these documents seems to imply that these conceptions are not as outdated as perhaps could be thought.
The sex worker and crime
Moving on from understandings of sex workers as mentally unstable, vulnerable and/or victims, a third (13/34) of documents relate sex work directly to criminality. They affiliate sex work with substance misuse, crimes such as theft or more generally associations with offending, the justice system or prisons.
‘Healthy Lives, Healthy People’ (DH, 2010b), a key public health white paper, introduces this with their only reference to sex work: … drug users are more likely to be involved in crime (such as theft and prostitution) … (20)
While actions associated with sex work are criminalised in the United Kingdom and a relationship between substance misuse and sex work is recognised in the evidence, the affiliation between crime and ‘prostitution’ is recurrent, representing ‘prostitution’ as crime. This is an oversimplification and implies a misunderstanding of laws and definitions around sex work. Neither sex work (nor prostitution) is, in itself, a crime in the United Kingdom.
NICE guidance on drug use reports, Many acquisitive crimes … are committed by people whose drug use has become an addiction … [who] support their drug use with low-level dealing or prostitution. (NICE, 2014b: 2)
A NICE accompanying document for ‘services for pregnant women with complex social factors’
2
lists: … prostitution and criminal activity … (NICE, 2012: 15)
All five NICE publications discuss sex work only in relation to drug use. While substance misuse and sex work may co-exist and interact to confer health problems, the complexities in this discussion is missing from these documents, referring to ‘prostitution’ as merely deviant criminal activity as a means to fund a drug problem. This misrepresents the myriad potential economic motivators behind sex work, which include poverty, debt, childcare or funding education (Sanders et al., 2009: 39–40).
The report ‘crime reduction benefits of drug treatment’ (NHS National Treatment Agency for Substance Misuse, 2012)
3
repeatedly lists ‘prostitution’ between ‘drug dealing’ and ‘other stealing’, alongside ‘fraud’ and ‘violent theft’. This document also states, women involved in street prostitution typically spend over 75% of their income on drugs. (p. 22)
This references a UK Home Office document (Hunter, 2004) which references another (May et al., 1999) which bases its findings on a small sample of sex workers chosen because of their association with both sex and drug markets. This poorly researched statement reinforces a simplistic, one-dimensional (1D) view of sex work that is easily corroborated with a moralistic agenda. This misrepresentation is not an isolated case; as Cusick et al. (2009) highlight, the Home Office was criticised in 2009 for the sweeping statement ‘nearly all sex workers are addicted to drugs or alcohol’ (p. 707).
Sex workers’ needs in these crime-related documents, when they are mentioned, are poorly acknowledged. Support for sex workers in prison is both important and lacking (Ahearne, 2016) yet they arise only three times in two H&J documents – twice in relation to rehabilitation companies, who simply list sex workers among those individuals for whom they provide support. There is a passing recognition that a significant number of women in prison may have worked in the sex industry, as outlined in the second H&J document (2014a), who reference a statistic (27%) to Plugge et al. (2006). No discussion of the health or well-being impacts of this is forthcoming.
The sex worker as a women
The constructions of sex workers frequently strays into discussion of female sex workers. While this is perhaps predictable, given most sex workers are women, the lack of recognition of sex workers of other genders and sexualities is an important criticism and likely contributes to their poor health and safety (Smith and Kingston, 2015).
Five documents explicitly affiliate sex work with women’s health and none with male or transgender health. Two out of the three documents with a topic of violence discuss sex work in relation to ‘violence against women and girls/children’. Three of the four case studies provided have women as their focus, one focusses on a man with no references to other genders.
NHSE’s ‘Equality Diversity System’ lists ‘women and men involved in prostitution’ (NHS, 2013: 11) and the EIA for the Department of Health (DH)’s (2010a) National Sexual Health Policy lists sex workers under ‘gender’, displaying a welcome recognition of diversity: Sex workers – like the rest of the population – form a diverse group, and their sexual and health behaviour will vary greatly. However, sex workers may have particular sexual health needs, and these are likely to differ according to their gender and personal circumstances. (p. 19)
The case study ‘Billy’ (not a real case, but ‘representative case material’) is a welcome example, in presence although not in content, of a male sex worker, in addition to the only reference to non-heterosexuality. However, here too there is reference to female sex workers. His story is combined with that of his mother, an (oddly phrased) ‘seductive and loving’ ‘prostitute’, which resulted in his ‘very disturbed’ childhood (Motz et al., 2015: 29, 69). This briefly refers an important and otherwise lacking concept, which is sex workers with children. The opposition of ‘good mother’ as the normative female role and ‘bad’ sex worker creates a ‘dual condemnation’ of sex workers with children (Dodsworth, 2014: 100). Billy is the result of this undesirable collision of roles, resulting in a ‘self-damaging’ and offending ‘rent boy’ (p. 69). This is indicative of the negativity surrounding sex-working mothers. Furthermore, this reference to Billy as a ‘rent boy’ is perplexing both due to its colloquial nature and its association with homophobia (Caudwell, 2017). This document portrays damaging views and terminology in relation to sex workers. Further case studies similarly construct 1D characterisations.
Case studies
These texts contain a further three case studies, all involving female sex workers. Including Billy, all four case studies involve individuals with mental health problems underlying their involvement in sex work; all four have experienced sexual abuse or assault; three of the four cases involve drug use. These cases paint a picture of complex individuals involved in damaging sex work. While we do not deny that such complex circumstances do exist for individuals in the sex industry, this is representative only of sex workers in those circumstances and not of sex work in its entirety and diversity.
Discussion
How are sex workers constructed in these documents? We argue, when present, they are depicted as ‘others’, as vulnerable and/or deviant individuals with mental health issues, putting themselves in the path of violence and abuse and committing crime to fund drug use. Despite representing these themes as distinct entities, in practice they overlap to formulate one contradicting construction of the sex worker. Figures 2 and 3 illustrate how these key themes intersect to create what we call the (female) ‘mad/bad/victim’.
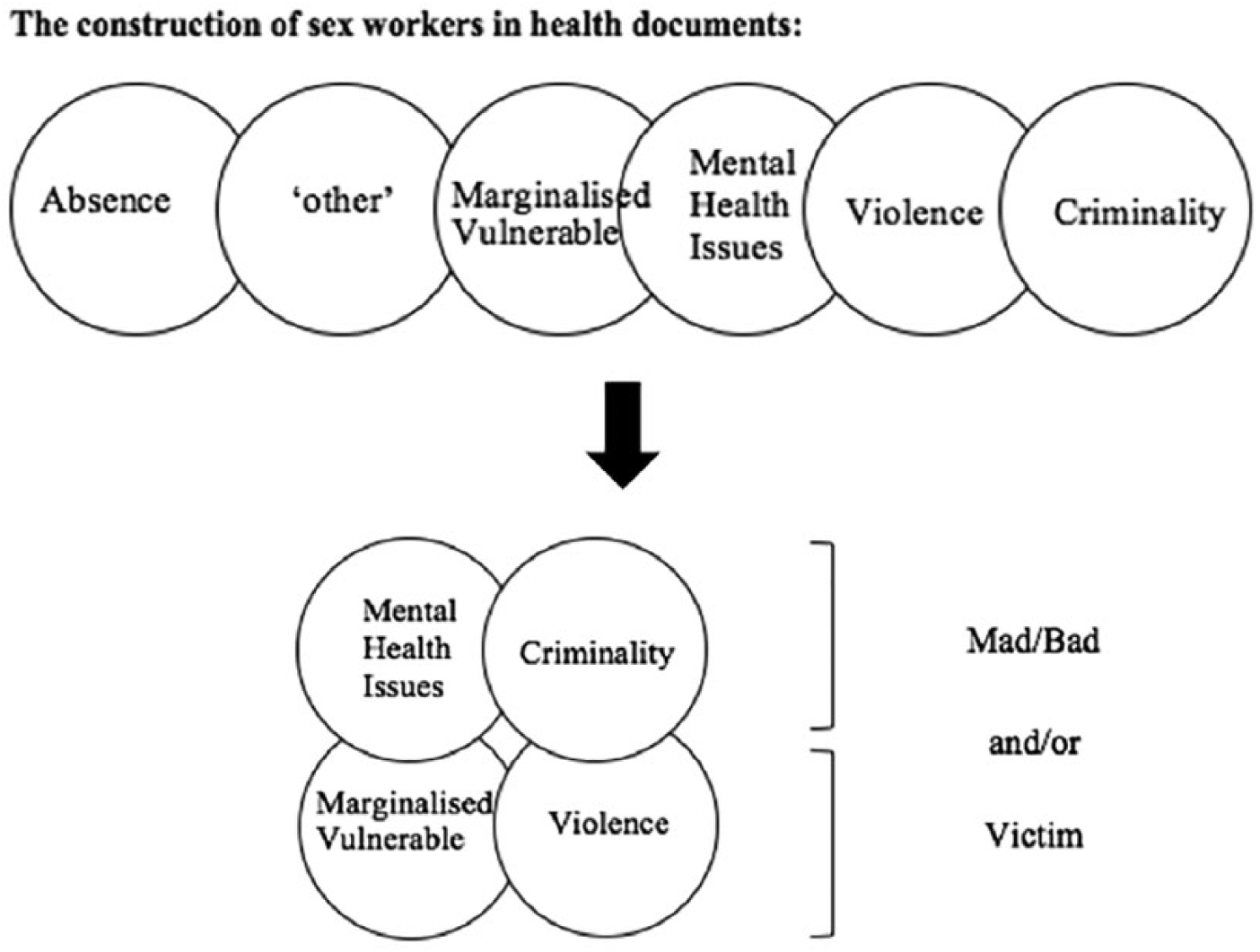
Image depicting the construction of the ‘mad/bad and/or victim’.
This is not a novel portrayal and has been noted elsewhere, for example regarding women who commit murder (Weare, 2013). This also relates to how sex workers are depicted in policy generally, similarly as public nuisance, yet innocent victim, as sexually ‘disordered’ yet vulnerable ‘fallen women’ (Carline and Scoular, 2015; Kantola and Squires, 2004; Sanders, 2009). This is reminiscent of representations of female sexuality, in what Tavris and Wade (1984) called the Madonna/whore dichotomy. Indeed, feminist discussions have long recognised these binaries: on one hand ‘weak and defective’ and the other ‘dangerous and polluting’ (Ehrenreich and English, 1976: 14). These conceptions do not truly represent women or sex workers. They obscure diversity, agency, reality and are based on ideological beliefs of womanhood and female sexuality, portraying moralistic undertones. This construction misrepresents the reality of sex workers, reinforcing normative ideals of femininity and inferiority.
Our analysis of policy-relevant health documents adds a new dimension to this discussion. The position of health policy and health organisations affords the opportunity and responsibility to use evidence to recognise and reduce health inequalities, potentially allowing a different perspective than politicians, legislation or other forms of public policy. The stark inequalities faced by sex workers in England clearly demand some focus from health organisations – both in relation to human rights and equality but also to cost (and life)-saving prevention and early intervention. The absence and construction of sex workers in these documents portray not an evidence-based perspective, but a lack of interest and/or a moralistic point of view – one that is unlikely to be conducive to reducing these inequalities.
There is more however. In addition to a lack of focus, the moral slant of these constructions risks further exacerbating these inequalities. The way people are defined in public documents dictate the strategies and plans for how their needs will be met (or not). The language and perspectives used influences how sex workers are envisaged by those reading these documents. While we can find no evidence on how widely read these documents are, especially given the significant range included in this analysis, it is very likely that many of these documents are widely read by health service staff, including public health professionals, policy-makers, managers and frontline staff. In other words: those responsible for organising and delivering frontline services. Therefore, the perspectives presented risk exacerbating stigma and perpetuating a narrative where sex workers are inferior, deviant and devoid of (sensible) choice or agency. They perpetuate a ‘discourse of disposal’ (Lowman, 2000: 1003) increasing the risk of violence, abuse and poor health and well-being. These documents risk reinforcing those social and structural norms that create the damaging environment in which sex workers currently work and live.
There are limitations to our methods; separating units of text to analyse risks inaccuracies of interpretation and the relationship between segments of text and the original meaning may be lost (Bauer, 2000). In addition, the analysis is a subjective process where we have reinterpreted these units of text from our own theoretical perspectives on sex work to give them meaning beyond that which they were explictly meant. Our search strategy intended to include every mention of sex workers in DH, NHSE, PHE and NICE publications. These documents thus form a disjointed collection, not intended to be read together and thus any conclusion drawn from examining their entirety needs to be taken in context. However, any member of the public or healthcare staff searching for discussion or guidance on the care of sex workers come across a similarly disjointed array. Our findings also suggest how an analysis across documents can be as fruitful as an individual policy analysis, the latter deemed to be of utmost importance in understanding the roots and direction of health systems (Buse et al., 2012).
We have focussed on sex workers as a diverse yet defined group with clear health inequalities who are marginalised, stigmatised and subject to myriad social constructions typically defined by people other than themselves. We could however have concentrated on any of the ‘other vulnerable groups’ so often listed alongside them: homeless people; traveller or migrant communities. Our findings have salience across this spectrum, posing the question of how balanced the views of health organisations are in relation to marginalised groups generally?
Recent high profile publications such as by Amnesty International (2016) and the UK Government Home Affairs Committee (2016) recognise and advocate the health benefits of decriminalising sex work. The Home Affairs Committee Report states ‘current practice … ha[s] an adverse impact’ and ‘it is wrong that sex workers … [are] … stigmatised and penalised’ (p. 21). This welcome focus on the harms of current policy has the potential to bring sex worker’s real needs to the fore.
Evidence from New Zealand, where the 2003 Prostitution Reform Act decriminalised all forms of sex work, indicates a positive effect on sex worker’s health and safety (Abel, 2014). A comparative analysis of Australian states with differing sex work laws demonstrates similar findings (Harcourt et al., 2010). While legislation lies outside the scope of our recommendations, research from these countries highlight the importance of government and health organisation perspectives to the health of this group. They highlight the health benefits of opening the conversation about sex worker’s rights, decriminalisation and their health and safety.
We recommend that the UK health policy follow this lead and start considering the root causes of sex worker’s health inequalities. We recommend they display a balanced, non-partisan view of sex workers and start doing just as they purport to do: use evidence to improve the health of this politicised and marginalised group.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.