
Abstract
The increasing prevalence of mental disorders together with the uncertain validity of psychopathological diagnostics challenges psychiatry as the primary home of studying, diagnosing and treating mental health problems and developing mental healthcare. This marks an emerging paradigmatical shift towards ‘alternative’ mental health perspectives. With the ambition of attending authoritatively in definitory practices, contemporary scholars of psychology, sociology, anthropology and philosophy call for an interdisciplinary approach to mental health, with a predominant focus on the subject. We argue that a paradigmatical shift of mental health requires structural–historical considerations of the foundations upon which subjectivity has been and still is manifested through psychiatry. On this basis, we critically investigate fluctuating psychiatric discourses on subjectivity, normality and pathology. We conducted a genealogical analysis of 13 psychiatric sources (1938–2017) focusing on ‘Psychopathy’ as a fluctuating diagnosis. We elucidate how subject concepts in psychiatry develop in parallel to subject concepts in society and culture, exemplified through convincing similarities between psychopathic symptoms and neoliberal ideals. Considerations like these, offer scholars valuable bases for mental health research and debate, and also valuable insights to healthcare professionals.
Keywords
Introduction
Early in the year 2018, the British Psychological Society (BPS, 2018) introduced the clinical psychiatric framework ‘The Power Threat Meaning Framework’ (PTMF), offering a new perspective on why people experience mental distress. The framework consists of psychological and sociological accounts for mental illness, and is, thus, a conceptual alternative to traditional models of mental health and distress, based on psychiatric diagnosis and classification. PTMF was published on the bases of yearlong critiques of the predominant medical psychiatry: for decades, perhaps even centuries, there have been battles concerning the understanding and treatment of mental illness, with various alternatives being presented. Nicholas Rose, for example, has taken an interdisciplinary standpoint exploring the growing number of psychiatric diagnoses and the growing number of people given a psychiatric diagnosis through sociological, philosophical, psychological, social medical and economic considerations. A critical opposition to descriptions, definitions and treatments of mental illness, predominantly embedded in a reductionist ‘brain-focused’ paradigm with biological medicine in the frontline, seems to be what is at stake.
This article will critically examine established psychiatric publications in order to understand and describe structural–historical developments of applied psychiatric frameworks in a Danish context. This enables a look at the current psychiatric debate that would not be possible in an investigation limited to the present. We wish, in this way, not to find a new ‘truth’ about the history of mental health, nor to outline a new framework of how to understand, define and treat mental illness. Contrarily, we wish for thought that is more critical on the commonly accepted discourses on normality and we hope that this article can supplement and inspire discussions on the development of future psychiatric policy, practice and research.
Psychiatry is a relatively new scientific discipline that, since its birth in the early 19th century, has been thought of as a medical speciality, requiring natural scientific modes of investigation. Nonetheless, understandings of the mental elements of the human psyche have undergone substantial paradigmatic shifts, before psychiatry gained the authority to define mental distress (Hergenhahn, 2005; Kendler, 2008). Epilepsy was mentioned in the Bible to be connected with the phases of the moon, and people with this condition were labelled lunatics, a term originating from the Latin word for moon, luna (Køppe, 2014b). Through other historical periods, ‘madness’ or ‘lunacy’ was ascribed many different explanations, such as unbalanced body fluids, deficits in the intellect and rationality, or that the body was possessed by evil spirits (Beyerholm, 1937; Mellemgaard, 1998). In History of Madness by M. Foucault – probably one of the most famous histories of psychiatry – one of the fundamental points is that the historical change in understanding madness is related to understandings of the ideal subject.
Before the ‘humanization’ (coined by French physician, Phillipe Pinel) of psychiatric treatment in the early nineteenth century, or before there were any treatments, madness was categorized as a demoniacal possession and, consequently, the insane could be treated as animals, as non-humans. The violence against the insane was violence against animals and not against humans. According to Foucault, the so-called humanization was motivated by the wish for defining the ‘new’ bourgeois subject (reason, reflexivity, and toning down passions and emotions). The bourgeois values and characteristics should, in this way, be intensified in the general public by showing and describing examples of the opposite: insanity was the ultimate picture of the ‘non-human human’. Also, according to Foucault, the humanization of treatment was parallel to an internalization of discipline and power. One just substituted an outer discipline with an inner one.
There are, however, other psychiatry historians who see institutionalized psychiatry as part of the state control and government of the subject. There is a tradition which describes symptoms as only determined by the society. Szasz was somewhat of a social constructivist (before it became modern). He explicitly claimed that insanity does not exist and that descriptions of insanity are at best metaphorical. Diagnostics are only stigmatizations and are used to sanction behaviour that societies do not accept and that treatment is just correction of behaviour. Psychiatry as an institution is a crime against mankind (Szasz, 1961). A more restrained analysis and discussion has been presented by David Rothman (2002), a historian who has analysed the emergence and development of different institutions and institutionalizations in the United States. Rothman argues that psychiatry emerged as a political and bureaucratic organization securing public order and a steady historical development. Psychiatric institutions are tools for the regulation of social norms and sanctions against potentially revolutionary elements. Both Szasz and Rothman are classic ideological liberalists and deny psychological understandings. The state should intervene as little as possible and needs to secure definitions of normality for the community.
It is interesting to consider the relationship between this classic liberalism and the present neoliberalism, which is suggested by several scholars (including Bourdieu, 1998; Harvey, 2007; Rose, 1998) to be the hegemonic subject concept characteristic of postmodernity. Neoliberalism is less rabid than classic liberalism, which opens up for a psychological approach with less fixation on the regulation of behaviour by the state. However, neoliberalism is, of course, still liberalism: the neoliberal subject governs by its own disciplinary mechanisms, making the inner discipline almost absolute. This demands a constant self-centred attention to one’s own needs and development (Rose, 1998; Türken et al., 2016). The neoliberal subject is morally obliged to overcome hereditary ‘challenges’ and uses its autonomy to choose its individual route to success. It is one’s right, to act in a self-centred manner, despite potential social and moral solidarity costs (Whitehead and Crawshaw, 2013).
There are interesting resemblances between the ideal neoliberal subject and the pathological condition labelled ‘psychopathy’. Before substantiating that claim, we will discuss the phenomenon of psychopathy, which is central in the article analysis.
Psychopathy – a case of uncertain diagnostics
Psychopathy has in a psychiatric context been described in many different ways: as an untreatable mental state, as an actual illness, as a hereditary case, as insanity, as anti-social behaviour of a sane individual and so on (Horley, 2014). Today, the concept is globally used about the specific anti-social/dissocial type of personality disorder (Arrigo and Shipley, 2001). We will in the following attempt to account for the blurriness of the history of psychopathy.
The term psychopath is meant to have been used for the first time in Germany in the 1840’s to describe general deviations or deficits of character. This was a very broad description, containing all mental disturbances related to the intellect and reason. Prognosis was poor, since the condition was a case of innate abnormal personality with ‘deficits’ in the moral (Herpertz and Sass, 2000; Horley, 2014; Rimke and Hunt, 2002; Werlinder, 1978). Emil Kraepelin later classified mental retardation as ‘moral insanity’, supporting the hypothesis of the innateness of moral ‘deficits’ in the personality. Hysteria, neurosis, paranoia and the preliminary stages of manic-depressive illnesses were, however, considered being specific types of psychopathy. Not as engaged with innateness and aetiology as his predecessors, Kreapelin focused on symptomatology to subcategorize deviating personalities in the clinic (Horley, 2014; Werlinder, 1978). The grounds for classifying disorders specifically concerned with personality began here. Kurt Schneider (a student of Kraepelin) described psychopathy as being associated with somatic illness, and he did not consider psychopathy as an actual mental illness. It was, and perhaps still is, not unlikely that the psychopath does not experience suffering.
The term ‘psychopathy’ has received considerable global distribution, which, for the most part, can be accounted for by the work of the American psychiatrists, Cleckley and Partridge (Arrigo and Shipley, 2001). According to Cleckley, the psychopath lacks normal socialization experiences, and can therefore not follow societal norms and legislation. This led to Partridge’s sociological variation of the term, the sociopath. The sociopathic personality is assessed in relation to social conditions and anti-social behaviour (Larsen, 1975). This is consistent with Schneider’s well-known definition of psychopathy: Psychopathic personalities are those abnormal personalities that suffer from their abnormality or whose abnormality cause society to suffer. (Schneider, 1923, in Werlinder, 1978: 106)
A psychopath can be diagnosed if his or her personality is deviating to a degree that is arguably pathological, despite the potential absence of experienced suffering. On the other hand, it is the society that suffers, because the psychopathic personality does not ‘fit in’. Consequently, the individual is left with minimal diagnostic authority, since it is mental healthcare institutions, today primarily psychiatry, that have the power to pathologize the non-normal elements of one’s personality.
A common feature across historical psychiatric descriptions is stressing that morality and personality are linked when describing and understanding psychopathy. In addition, links to subject concepts are common, as are the assessments of a right or wrong, normal or pathological ‘character’ which can be coined for the moral aspects of a personality. Morality is, however, out of perceptual experience because it sets its own limits for arriving at a cognition of the concept. Rather than being a universal fact without borders for immediate cognition, character and morality are defined through societal values of normality, which determine the border of scientific cognition. Character is a borderline concept because its epistemic ambiguity embeds it on the border to other, similar, concepts. The normal character is formalized through psychiatric definitions of the pathological character, despite its societal conditions for recognition. Does the discussion of the normal and pathological personality belong in psychiatry?
For the above reasons, and due to its elucidating of changing normality concepts, psychopathy can illustrate a fundamental problem in psychiatric theory and praxis, namely where to draw the line between normality and pathology.
Normality, pathology and modern diagnostics
Psychiatry is occupied with the pathological psyche and the pathological personality. On the opposite side of pathological conditions are the normal psyche and the normal personality. Normality stems, etymologically, from the Greek word nomos meaning ‘what determines norms’. But this meaning is not only very broad, it is also ambiguous. Norms are at once a fact and “a value attributed to this fact by the person speaking, by virtue of an evaluate judgement for which he takes responsibility” (Canguilhem, 1991: 125). One can be too far from a mean value, indicating deviations from the normal, but one can also deviate from a chosen value of what is correct and ideal, and can vary depending on the ‘value attributed by the person speaking’ (Canguilhem, 1991; Kragh-Sørensen et al., 2010). The logic behind previous and current psychiatric classification 1 has both concepts of normality embedded; there is an ideal mental state that one can deviate from to a pathological degree.
Taking a philosophical look at the diagnostic systems and with help from Rose (2013), it becomes clear that psychiatry places all heterogeneous subjects within the same general framework. This implies that all subjects have a common denominator from which they deviate, meaning that they all suffer from the same kind of deviation, namely one that medically trained psychiatrists can diagnose, treat and manage (Rose, 2013).
The direction from pathology to normality has an immediate logic: the non-pathological state is one of normality. However, the direction from normality to pathology is not as simple. One could definitely imagine that there are non-normal states that are not pathological. A condition that is far from a statistical mean of normality might not be varying to a pathological degree. Another condition, which is deviating to a pathological degree, might be considered ideologically normal. So, the question remains, when is the non-normal state pathological?
Many have argued that in order to answer, or at least attempt to answer, these questions, one must look at psychiatry from an interdisciplinary standpoint. The object field of psychiatry is, besides biology and neurology and, depending on the time in history, about the mental, and abnormalities and anomalies in the conscious mental life. The epistemology of psychiatry is, rather than stringently reductive, interdisciplinary, making psychiatry one of the scientific disciplines with the largest ‘grasp’ (Kendler, 2008; Simonsen and Møhl, 2010).
Subject concepts
Concerned with the concepts of ‘the human subject’ and remembering Foucault’s argument that historical changes in the understanding of madness are related to understandings of the ideal subject, compel us to elaborate on subjectivity as a psychiatrically relevant point of analysis. We will pay attention to three theoretical and methodological challenges that emerge when concerned with subject concepts in a historical perspective, namely the historicity of the human subject, a moral sense of conscience in the psyche and the creating role of subjectivity theories of subjectivity.
First, one must consider the historical relevance of the specifically operationalized parts of human subjectivity. One can be inclined to think of the development and nature of human personality and the human psyche as something universal and ahistorical. In the most part, many think of the medieval farmer as, besides his or her more primitive way of life, more or less like us today (Køppe, 2014b). However, the subject and its personality(-ies) are very diverse across time and place. Basic psychological functions, such as memory and perception, are fundamental for developing a personality. These are conditions that might not have changed much throughout history, since we are, genetically, identical to the primitive humans living 30,000–40,000 years ago (Køppe, 2014a). Thus, there must be another explanation to historical variance than genetic evolution. Social practices and societal circumstances must have a creating role in the historicity of the human subject. It would be too vague simply to claim that ‘society defines’ the human subject and personality, but an illustrative example is the development from feudal society to the civil market-oriented structure of society, which changed the personal circumstances of the individual crucially (Køppe, 2014b; Sonne-Ragans, 2013). The wish for defining a ‘new’ bourgeois subject consisting of reason and reflexivity, and toning down passions and emotions (as mentioned in the ‘Introduction’) created an inner discipline, which enabled the emergence of a scientific concept of subjectivity. 2 Liberal values, such as reason, rational thoughts, free market and political freedom characterize this liberalistic view of the subject. Emotions and passion were objectivized as irrational and processes were meant to be contained. The bourgeois emergence caused a separation between home and work, which was earlier in the same sphere, creating a sphere solely for production and a sphere solely for personal privacy. A humanistic 3 view of the subject developed on the basis of this. The ideal subject was characterized by emotional elements, making naturalness, spontaneity and feelings forming the actual nucleus of the human subject. Founded in the sphere of production, a mechanistic subject emerged in industrialization, where complex technology revolutionized society. The human subject was, loosely expressed, reduced to physical–chemical regularities accounted for by physiology and neurology. This resulted in a view of the subject as a more or less well-oiled machine that could be fixed. This is a view that is prevailing today in both the somatic and psychiatric departments of the health system: see The Medical Model of Disease (Rose, 2013).
Naturally, ideas about the world, society and humans have existed prior to this, but it is interesting to consider that features such as instincts and emotions are not universal. All features of the human can be attributed to stages in a historical developmental process (Heede, 2002), and Foucault even disputes that the purely biological body is subject to historical processes. Discussions on historically different views of the subject can contribute to an investigation of subjectivity, since societal and historical spheres contribute to the creation of views on the subject. Furthermore, views on the subject can illustrate what Foucault has called ‘dividing praxes’: the subject is divided from other subjects through societal changes, and this objectivizes and labels him or her. Examples are the sane and the mad: in other words, the ideal/normal and the pathological subject (Foucault, 1982). From this claim, one can elaborate on the character of societal circumstances that affect and create a certain (pathological) subjectivity, since the individual subject is governed dynamically by changing logics with normative demands.
The second discussion is concerned with moral aspects of the human subject. Psychological mechanisms and functions, such as memory, language and perception, are not directly linked to specific personalities. Other psychological aspects, such as morality, are linked to the idea that the human subject inevitably has moral aspects. What is interesting in this article is the investigation of when something is right or wrong, good or bad, since this can shed light on different moral stances in mental health. How an individual proceeds and behaves facing moral dilemmas can label him or her as, for instance, being introvert, neurotic, narcissistic or conscientious.
Morality has played a big role in mental health history, and has been used in at least three alternative meanings, founded in various theoreticians and psychiatrists’ use of the term (Werlinder, 1978). Pinel thought of ‘moral treatment’ as a way of affecting the emotional life of the patients, and morality was for him ascribed with affective aspects of the psyche. Prichard included character-constructing elements such as free will and passion to the ‘moral department’ of the psyche (Rimke and Hunt, 2002; Werlinder, 1978). The third use of the term moral in a psychiatric context is even broader, as it has been used merely as another way to describe the psyche. Hence, moral phenomena were equivalent to the psychological object field today, namely mental phenomena. Morality has thus been formalized very differently, and capturing the moral aspects of the human subject, specifically in regard to psychopathy, arguably requires historical awareness. What is further interesting is the, already discussed, strong link between morality and psychopathy. Psychopathy is throughout its varying definitions concerned with a pathological personality or character, and is thus an exemplification of when and how a certain behaviour is objectivized and diagnosed as being wrong. Some have argued that psychopaths lack a basic moral sense of conscience, making moral aspects of the human subject interesting for historical discussions on psychiatric pathology (Werlinder, 1978). The diagnosis changes across history, and can provide an example for a general discussion on the societal shifts of morality.
A third discussion deals with the questions of whether theories of subjectivity, personality and morality contribute to creating the very same concepts. It can appear as an academically arrogant statement, but it has been shown how, for instance, human ideals of social behaviour are discursively determined and how many have an immediate ‘unconsciousness’ repertoire as a result of the popularity of psychoanalysis (Brinkmann, 2005; Køppe, 2014b). We do not see the world as it truly is just by attending to the facts. Instead, our perceptions of the world are influenced by our (theoretical) conceptions of it (Kendler, 2008). According to Kendler (2008), the interdependency of theory and the world as it is, is especially evident in psychiatry, since psychiatric theory and literature are inevitably affecting psychiatry: the interdisciplinary nature of psychiatry’s objective field makes psychiatric phenomena as they are impressionable to theorizations, ideologies and ideas from many different directions. We will not attempt to uncover new ‘truths’ or the true origin (Ursprung) of psychiatric normality concepts, but instead research into the emergence (Entstehung) and birth (Herkunft) of psychiatric normality concepts, which makes theories’ contributions inevitable and manageable (Foucault, 1984).
Methodology
The aim of this article is to unravel the complexity of contemporary psychiatric discussions related to mental health, mental normality and mental pathology, and thus present a critique of norms. Genealogy is one of the means for this kind of investigation, as it sheds light on discoursively structured patterns of concepts of truths.
Based on an excavation of historical texts, genealogy, primarily coined by Foucault (1984), identifies “. . . the accidents, the minute deviations – or conversely, the complete reversals –the errors, the false appraisals, and the faulty calculations that gave birth to those things that continue to exist and have value for us . . .” (p. 79). Genealogy requires a critical approach, in which common definitions and applied practices are not just accepted, but are repudiated in order to understand the basis of their existence. The critique is related to the historicity of phenomena. However, as useful and intuitive a historical awareness seems, so is it difficult to gain accurate and reliable information about historic phenomena. Two types of methodological challenges emerge: the discontinuity of history and the stratified nature of populations (Køppe, 2014b).
History does not evolve continuously, in the sense of a linear progression. Historical transitions have involved a qualitative change in the way phenomena as subjectivity, personality and psychopathology are conceptualized. Thus, a study of subjectivity carries the risk of becoming discontinuous (Baumeister and Hawkins, 2005) because of what Kuhn referred to as ‘incommensurability’: namely that concepts from one historical period cannot be directly translated into another. Not totally overcoming historical discontinuity, we steer out of major discontinuity problems by conducting a historical qualitative content analysis by selectively choosing passages about the theoretical foundation of three types of psychiatric literature at selectively chosen points in time; thereby discovering underlying assumptions about definitions of normality (Foucault, 1984) and views of the subject in the psychiatric institution and about the concept of the diagnosis ‘Psychopathy’.
The second methodological challenge is the stratified nature of populations. Historical sources are often centred on the privileged sections of a population and, thus, may not apply to an entire population at a given moment. The three groups of materials included in this study are conducted by very different groups and, presumably, contain stratifications or at least some between-group variation. Legislation is formulated by national politicians and jurists, textbooks by local academic and clinical psychiatrists and diagnostic manuals by a global board of academic and clinical psychiatrists. However, the literature is not constructed to be applicable just to a specific layer in society, but is intended to be applicable for all individuals that meet the different psychopathological criteria employed. Furthermore, we delimit the analysis from the actual psychiatric practice, since we are interested in the underlying discourses found ‘at a distance from the patient’. Patients might come to psychiatric issues with their own beliefs and opinions that, not only say little about the scientific psychiatric institution, but may also vary across populations (Kendler, 2008). Combining these three types of sources, allows us to expose ruptures and struggles over power, in what might seem a homogeneous psychiatric discourse.
Empirical sources
A genealogy comprises, according to Foucault (1984), a large amount of texts, which are frequently quoted, and recopied many times (p. 76). The empirical material for this analysis consists of three groups of primary sources, from 1938 to 2017, that have relations to and consequences for the scientific psychiatric institution and the treatment of mental illness. Our focus is the Danish psychiatric context in regard to Psychopathy, and the international element is the ICD (International Classification of Diseases) manuals. Table 1 is an overview of the included material, which is elaborated in the following.
Included empirical material.
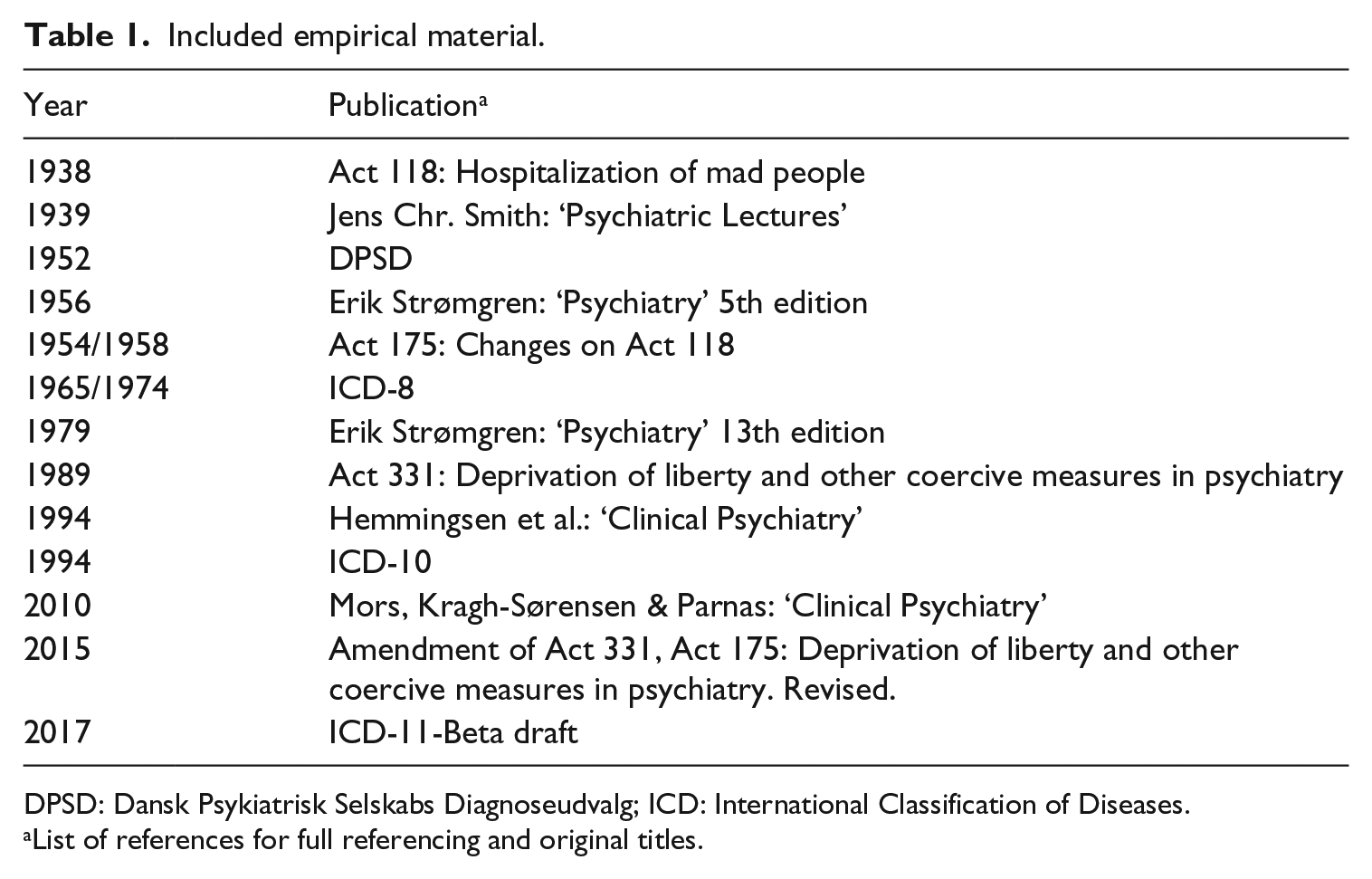
DPSD: Dansk Psykiatrisk Selskabs Diagnoseudvalg; ICD: International Classification of Diseases.
List of references for full referencing and original titles.
The first group consists of four diagnostic manuals. ‘Dansk Psykiatrisk Selskabs Diagnoseudvalg’ ((DPSD); Danish Psychiatric Association’s Diagnose Committee) from 1952 is the earliest included manual, since it was the first official nomenclature in Denmark. It was inspired by the structure of the ICD, but the ICD system was generally not accepted by Danish psychiatrists (Strømgren, 1956) until ICD-8 appeared in 1956. ICD-8 is therefore also included (World Health Organization (WHO), 1974). ICD-10 (WHO, 1994) is included since it is applied in the current Danish psychiatric context and then finally the beta version of the forthcoming ICD-11 is included (WHO, 2017).
The second group of material comprises five psychiatric textbooks used for teaching medical students in Denmark, and they can reveal something about the medical discourse among scientific psychiatrists. Until 1951, psychiatry was not an independent examination subject in Denmark, and by 1956 the Danish psychiatrist Strømgren (1956) published a textbook that “involves everything relevant to know about psychiatry” (foreword). Strømgren (1956) is the fifth edition of a less extensive book by Smith from 1939, which is also included (Smith, 1939). Strømgren was an early key figure in Danish psychiatry (Bjerrum, 2008), and the 13th and last edition of his textbook from 1979 is therefore also included (Strømgren, 1979). Two finally included textbooks are the current psychiatric textbook used in medical schools in Denmark (Mors et al., 2010), which is a third edition of the original from 1994 (Hemmingsen et al., 1994).
The third source of empirical material is four psychiatric acts of parliament. The first legislation in Denmark that specifically deals with the psychiatric area, is Act No. 118 from 1938 (The Danish Ministry of Justice, 1938), and it remained unchanged until 1989 where the first act (No. 331), that is not only concerned with hospitalized psychiatric patients, was published (The Danish Ministry of Health, 1989). There was, however, also a constitutional change in 1958, which has consequences for psychiatric appeal rights, for which reason the act following this change is included (The Danish Ministry of Justice, 1954). The last included legislation is the current psychiatric legislation (The Danish Ministry of Health, 2015).
Procedure
Reading and rereading of the primary sources together with several secondary sources, contributed alongside the analysis with valuable knowledge about the historical, structural and scientific foundations of the psychiatric institution. The included sources were internally selected in order to omit irrelevant information. The entire legislations are included, but the commission reports were omitted since they have no direct influence on psychiatry. Descriptions of specific diagnoses, apart from Psychopathy and Antisocial/Dissocial Personality Disorder, were also omitted in the textbooks and diagnostic manuals.
Several themes were condensed on the basis of empirical data from the sources, through a historical critique of sources and through utilization of sources. The historical critique of sources is a method of investigating sources, and on that basis interpreting and extracting hypotheses and deductions (Egaa Kristensen, 2007). This includes an identification of the sources, which places the source in connection to the situation and the circumstances under which it was published. The identification is concerned with the text type, time of publication, place of publication and grounds behind its publication. Furthermore, genealogical themes were identified: power, knowledge and norms. Knowledge is concerned with the relationship between true and false, power with definitory authorities and the norms distinguish between ‘good’ and ‘bad’ (Christensen, 2016).
Data condensation of the sources’ contents is of course crucial for the thematic analysis. Here, we utilize the fact that the included sources are actual publications, since they are manifestations of actions that have actually taken place. We interpret and conclude on the basis of text extracts and thereafter conclude on reality, because we presume that the source is similar to a past reality (Egaa Kristensen, 2007:125).
Results
An obvious conclusion to be drawn based on the analysis, is the confusion over the phenomenon, term and diagnosis of psychopathy: the manuals and textbooks have, across time, placed psychopathy on different levels and given different names. 4 The earliest textbooks and diagnostic manuals have psychopathy as a very broad category, contrary to the later, narrower use, in which psychopathy is coined to a specific type, the dissocial type of personality disorder (DPD). The DPSD placed ‘Permanent personality deviations of non-psychotic nature’ as one out of nine main categories of all mental disorders, not having a dissocial type as a subcategory. ICD-11-beta places ‘Personality Disorders and related traits’ as 1 out of 19 main categories, making it possible to ascribe ‘prominent dissocial features’ to the diagnosis. Smith argued in 1939 for ‘Psychopathies’ as one of three main categories, with no subcategories related to dis- or anti-social features, which is very different from Mors et al. (2010) who arrange the chapter ‘Personality disorders and sexual deviations’ as 1 of 17 main chapters. The term ‘psychopathy’ was used up until Hemmingsen et al. (1994), where ‘personality disorders’ override the terminology. The included psychiatric legislation does not specifically deal with the term ‘psychopathy’, but the law dictates which patients can be characterized as insane (and therefore not punishable) and which cannot (i.e. punishable). Despite this, the legislative measure of ‘insanity’ does not change much across the involved legislation, suggesting that it is hesitant in clarifying the concept into meaningful legislative measures.
The concept of psychopathy has, in the historical period covered by the present analysis, been connected to moral aspects of human subjectivity – despite evidently inconsistent usage of the term ‘moral’. This might be explained by looking at psychiatric epistemology. It seems that the psychiatric sources included in this study attempt to describe, define and treat mental illness without definitions of normality that are critically discussed in a historical and cultural perspective. A phenomenon such as morality is viewed in a biomedical vacuum, with no critical reflections on the usage of the current understandings of morality. Another perspective could be the labelling of psychopaths as insane or not insane. Psychopathies and severe personality disorders are difficult to place in this regard, because they are generally not ‘insane in the legal sense’. Psychopaths are ‘simply’ deviating in the moral aspects of their personality, and are not, per se, delusory or experiencing of suffering. They are described as lacking morals or as not having a normal personality (meaning the opposite of a pathological one). A ‘wrong’ personality is difficult to treat. Imagine telling one’s patients that they have a ‘wrong’ personality and that they must think of what is good, and not what is bad.
The analysis further showed how psychopathology was first organized according to ideal mental states that, if adequately searched for, could be found in its neurobiological basis. Later, psychopathology was organized symptomatologically, in recognition of lacking neurobiological findings suitable for aetiologically based classification. The subject is reduced to his or her symptoms, and normality concepts are kept in an ahistorical vacuum. Psychopathy in 1952 was a personality deviation and later, with ICD-8, it was a personality disorder, which signals a move towards symptomatology. Similarly, the textbooks develop from a delimited focus on aetiology towards aetiological considerations being in the background. The newest textbooks have descriptive symptomatology as their highest priority, although heredity is kept as ‘an interesting field of research’. Smith thought that hereditary aspects dominated the psyche more than environmental aspects, and he sought neurobiological components as explanatory for all mental illnesses. Similarly, Strømgren thought of heredity as a dominating factor and believed that all mental disorders had a neurobiological basis, but concurrently acknowledged neurobiological shortcomings in research. The newer the publication, the more focus is on symptomatology. However, the psychiatric subject is persistently kept in an essentialistic understanding where time-consistency is desired, adhering to the subject in biomedicine.
In 1952 the DPSD directed that a patient could only be diagnosed with one main diagnosis. ICD-8 and ICD-10 accommodated this, introducing a hierarchy of diagnoses where the main diagnosis should be ‘higher’ in the hierarchy if more than one diagnosis was appropriate for the patient. It is only ICD-11-beta that seems to be outlining a more dimensional approach, where stringent categorical demands are omitted. The analysis shows that the biomedical scientific standpoint of the manuals, where the diagnostic criteria meet reductive ideals, demands the assignment of a diagnosis to a deviating and pathological state. This focus on placing the patient and his or her symptoms within the diagnostic framework is in danger of leaving out historical, philosophical and psychological considerations concerning the phenomena behind the symptoms, in spite of an increased focus on involving other disciplines than medicine. This is, interestingly, also evident in the legislation. There is an indication of an acknowledgement of the psychiatric field’s complexity, since the source of psychiatric legislation has shifted from the Ministry of Justice to the Ministry of Health.
An implication of the focus on symptomatology could be that a comprehensive assessment of the psychiatric patient, where aetiological factors such as heredity, social relations and other elements in and around the individual, are in danger of disappearing.
Finally, our analysis showed that the psychiatric patient is ascribed an increasing amount of personal responsibility: paternalism gives (partly) way to the autonomy of the patient.
As outlined above, the newest textbooks have descriptive symptomatology as their highest priority, which indicates an increased acknowledgement of the shortcomings of understanding the psychiatric patient solely from a biomedical standpoint. This gives room for a view describing the psychiatric patient as a more responsible subject who can act on his or her mental state, and not a ‘victim’ of inheritance.
Both Smith and Strømgren do not believe psychopathy to be a condition that can be treated, since it is a predisposed defect-state. This leaves the patient with absolutely minimal autonomy, creating a subject concept captured in its (perhaps imputed) pathology. Hemmingsen et al. are not as definitive about prognosis, but they state that the severe personality disorders are seldom treatable, and their view of the patient is someone in need of psychiatric help. The pathological symptoms of the patient must be removed. Mors et al. are vague in this regard. Psychopathy is not conceived as insane (and requiring treatment), but also not as sane. Mors et al. further argue that the mentally ill person must be viewed and treated as a normal individual, but the urge to establish that fact throws suspicion on its sincerity. Although it is not as clear, there is a small development towards more autonomy for the patient, in the diagnostic manuals. DPSD did not leave an impression of the patient as a human person with autonomy, but more as an ‘interesting object of investigation’. On the contrary, ICD-11 seems to become more flexible in handling a patient’s complex, and sometimes contradictory, symptoms. The logic in ICD-11-beta is that the severity is diagnosed prior to assigning a specific type to the patient, and, thus, a diagnosis might become more adjusted to the individuality of the patient, rather than the patient adjusting to a diagnosis. This implies an individualistic view of the psychiatric subject.
Across the included sources there is, furthermore, an established paternalism. Smith wished to give the patient as much freedom as possible, but the moment the doctor prescribes a treatment, the patient is not in a position to reject it. Strømgren went as far as not trusting the patient in providing reliable and fulfilling information, for which reason the doctor must always have the last word. Hemmingsen et al. and Mors et al. did not leave much room for the discussion of paternalism versus patient autonomy, which can be interpreted in different ways. Either the discussion is not important enough, suggesting that diagnostic principles and psychopathological explanations are of more importance, or the discussion is of such a delicate matter that is it ‘best not to go into it’. The latter interpretation is inspired by the included legislation that is very clear on matters of paternalism manifested as coercion.
The autonomy of the psychiatric patient, in regard to coercion, goes from being at an absolute minimum to having the character of an ultimatum in the newest legislation from 2015. Act 118 of 1938 is not very specific about consent to coercion, but the patient’s own wishes ‘can be taken into consideration’. Constitutional changes in 1958 made it possible for the patient to complain and to appear before an impartial court, which was a major tilt of power towards the patient. By 1989, the doctor was required to enter the use of coercive measures in their protocol and could face judicial investigation on it, and the patient must always be informed of the act and consequences, before any form of coercion. Most interesting is precisely the informed consent. A passive response from the patient to coercion was, prior to the newest Act of 2015, considered to imply consent. Since 2015, hospitalization and treatment in psychiatry cannot begin or continue without a clearly informed consent from the patient. The fact that the psychiatrist cannot perform coercion without the patient’s informed consent, but at the same time has the right to perform coercion is a self-contradiction in the law, and supports the idea of a hesitant legislation. With Act 1160, an almost unlimited self-evaluation is placed on the patient, who must decide what he or she wishes to accept and what not. Consequently, the psychiatric subject is given almost unlimited autonomy and responsibility for his or her own illness, own actions and own life.
This observation draws immediate and interesting connections to descriptions of the neoliberal subject, which is, as described above, highly self-oriented and solely responsible for its own success in life. These features are, in the neoliberal logic, positively connoted features, but they are also closely related to negative features, such as egoism and selfishness. The egotistic subject will be willing to satisfy his or her own needs at the expense of others’ satisfaction of their needs. This characteristic is comparable to the ICD-10 description of anti-social personality disorder. Here, anti-social personality disorder is characterized (among other clinical descriptions) by a ‘disregard for social obligations, and with a callous unconcern for the feelings of others’ (WHO, 1994). Furthermore, ICD-10 emphasizes that there must be a ‘gross disparity between behaviour and the prevailing social norms’ (WHO, 1994).
Through our analytical findings, we assert the evidence of a clear connection between psychiatric discourses in relation to normality and those in society, questioning biomedical hegemony in psychiatry. Our analyses showed that the concept of Psychopathy has undergone classificatory and definitial changes from the first mention of the term in the 1840s until today, an indication of insufficient psychiatric conceptualizations of mental illness. Furthermore, the analysis showed an epistemic understanding of mental illness rooted in essentialism, implemented through searches for a neurobiological basis of mental illness. Finally, our analysis showed that the psychiatric patient is increasingly assigned a larger degree of autonomy and personal responsibility, which seems to be a development towards a subject of neoliberal ideals being the definition of normality.
Discussion
The aim of this article was to investigate how mental illness has been understood in psychiatric institutions, historically and up to the present day. Our objective has been to elucidate and indicate how subject concepts have changed over time in a psychiatric context. This is in order to unravel the complexity of contemporary mental health discussions related to normality. To validate the utilization of our findings, we begin with a clarification of our standpoint. We do not subscribe to a constructivist theory. We think a critical realism is more appropriate both in relation to accepting the reality of the patients’ symptoms and in relation to the theoretical developments in a historical context. The historical contexts are important because the developments show the defining properties which science uses to conceptualize the human subject and define pathology as every deviation from this. Although the PTMF offers promising perspectives to a struggling definitory psychiatry, we notice a risk of creating ‘just’ a new psychiatric subject concept with no traces to historical discourses that have laid the ground for contemporary understandings. An example could be the moral evaluative sense of subject concepts.
Our analysis indicated interesting similarities between descriptions of the neoliberal subject and the characteristics of the DPD. What then can we do with this knowledge? The diagnoses DPD and Antisocial Personality Disorder (ASPD) have not been described thoroughly with prevalence, type of diagnostic manual and sample sizes ranging highly from study to study (Tyrer et al., 2015). However, a meta-analysis on the prevalence of personality disorders in Western countries shows that ASPD is second in prevalence among 10 distinct types of specified personality disorders at 3 per cent (Volkert et al., 2018). The same study reported that the prevalence of any personality disorder is 12 per cent. With this in mind, we see two different directions for the future of the DPD/ASDP diagnosis. One hypothesis is that prevalence will decrease. If the characteristics of the neoliberal subject will become increasingly common and accepted, behaviour such as egoism and low regard for other people might become a ‘new normal’. This would normalize many of the symptoms of DPD and ASPD. Egoistic behaviour, for example, might be pathologized to a lesser degree, watering-down the diagnoses resulting in smaller prevalence. It is, however and on the contrary, also likely that the increasing hegemony of a neoliberal subject will result in an increase in DPD/ASPD prevalence. Increases in ‘neoliberal behaviour’ may develop in parallel to an opposition that will to a lesser degree tolerate, for example, egoistic behaviour. A decrease in tolerance for certain behaviours will lower the threshold for when something is, for example, ‘with no regards to others’, making minor violations of the rights of others considered as symptoms of DPD/ASPD, possibly placing DPD/ASPD as the personality disorder highest in prevalence. However, will then the symptoms, and, hence, the diagnoses change in order to make the diagnosis ‘fit’ clinical symptomatology? This, again, raises questions about the validity of psychiatric diagnostics. Some researchers (e.g. Brinkmann, 2015; Rose, 2006, 2013) have suggested an emergence of a ‘psychiatrization’ of the social world, meaning that general conceptions of normality have been tightened and the pathological threshold has been lowered substantially. The critical point in discussions like these, from our point of view, is to question normality as an essentialism since the normal psyche, personality and subject evidently are historical phenomena. If one is to believe the significance of interdisciplinary contributions to the mental health debates, we will strongly argue for a strengthened focus on historicity.
Another critical point when discussing normality and psychiatry is the application of definitions of normality in the psychiatric practice. While focused on discourse, we accept the conduct of everyday life in the psychiatric practice and the reality of the patients’ suffering, hence our critical realism. We have looked at psychiatry from a distance to the patient and the practice, and our findings are consequently delimited from movements and lessons from the actual practice. We point out in the analysis that the Danish legislation is increasingly favouring the patient’s autonomy and reinforcing the control for coercion, and we link this to the neoliberal movement also favouring autonomy. This is, however, a conclusion drawn by looking at discourses. Another explanation for the legislative focus on autonomy could represent an attempt to decrease coercive measures in the psychiatric practice. This can be supported by the fact that Denmark was criticized by the European Committee for the Prevention of Torture and Inhuman or Degrading Treatment or Punishment (CPT) in 2008 for the use of mechanical restraint, which CPT considered as ill-treatment (Bak and Aggernaes, 2012). Thus, there could be strong political motives for controlling coercive measures in psychiatry; motives not directly linked to neoliberal ideologies. It could be interesting and valuable to compare our findings with explorations of a neoliberal logic of subjectivity in the psychiatric practice among psychiatric patients and professionals. Balancing autonomy, ethics, security and coercive measures is a constant dilemma in psychiatric practice, and national and international intentions to limit the use of coercion to an absolute minimum will undoubtedly affect decisions on the use of coercion (Klaebo Reitan et al., 2018). However, we argue that a concept such as autonomy from a discursive perspective can still unravel concepts of normality a study limited to present and context-near perspectives could not.
Furthermore, it is interesting to consider the concept of user involvement in psychiatry. In the early textbooks, legislations and diagnostic manuals included in this article, the patient was given very little autonomy, since the doctor’s paternalism was dominating the practice, and psychiatry was more or less a monodisciplinary field of medicine. If the doctor decided you should be hospitalized, then you were hospitalized – even if you were in no danger to yourself or others. Today, user involvement in psychiatry has gained substantial attention, with an aim of seeing the patient–professional relationship as an equal give-and-take collaboration among partners (Holen, 2011; Ringer, 2013). This movement may be orchestrated by increasingly placing responsibility on the patient, because of the above-mentioned focus on decreasing the use of coercion. Furthermore, user involvement could have the possibility of opening up for a questioning of powerful discourses in psychiatry. There is, however, also bad news for supporters of user involvement. First, scholars have suggested that an intimate relationship between discourses, practices and user involvement causes the question of whether patients are involved in the treatment to be a question of how the particular psychiatric patient is defined (Holen, 2011; Ringer, 2013). There are significant differences in defining the patient as a victim of a brain disorder and defining the patient as an autonomic user who chooses freely among service providers. Naming and thinking of someone as a victim versus a user will consequently differentiate the treatment and patient–professional relation. This means that paternalism is intact, since the psychiatrist has the defining power; thus, also the discursive power of the positioning of the patient. Second, user involvement might only serve to perpetuate and reinforce existing power relations. Stickley (2006) points out that this will be the case if patients are expected to adopt prevailing understandings in the psychiatric practice.
It seems there emerge power relations, issues of complex dependencies and struggles on definitions of mental health problems in the meeting between patients and psychiatry, all of which seem also to exist in psychiatric theory and research. Further research into the similarities and differences between psychiatric research, legislation and practice in regard to autonomy, coercion and user involvement could be of high relevance and importance.
Supplemental Material
Clemmensen.Koppe.2018.Supplementary_material – Supplemental material for Normality, subjectivity and mental health: A genealogy of Danish psychiatry, 1938–2017
Supplemental material, Clemmensen.Koppe.2018.Supplementary_material for Normality, subjectivity and mental health: A genealogy of Danish psychiatry, 1938–2017 by Malene Broch Clemmensen and Simo Køppe in Health:
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online
Notes
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.