
Abstract
In 1779, Mr Thomas Brand surgically reassigned the gender of a seven-year-old child from female to male, thus enabling him to urinate standing up, wear trousers, and enjoy the privileges of being a male. This case study, published in London in 1787, illuminates 18th-century debates over gender, sexual ambiguity, and medical theories and practices. Mr Brand, Surgeon, uses his case study to claim that the body is two-sexed, and that hermaphrodism is a fiction. He proposes that the anatomical knowledge and practices of surgeons such as himself are superior to those of higher-status physicians. Mr Brand does not have a lot to say about his patient or her/his parents, except to conclude that if the patient had been of the upper classes, the case would have been a lot more interesting.
Medical procedures are products of their time, both technologically and culturally. The procedure I examine in this article is the gender reassignment of a seven-year-old child, by surgical means, from female to male, in the year 1779. It is eight pages long, plus a copyright page and three illustrations of the child’s genitalia and lower abdomen. It was written by Thomas Brand, a surgeon and anatomist, illustrated by a ‘Mr. Bell,’ and published in London in 1787 (Brand, 1787a). It is one of many 18th-century ‘meticulous anatomical descriptions of specific case histories associated with sexual ambiguity, often accompanied by visual representations.’ (Fontes da Costa, 2007: 79).
Gender reassignment in the 21st century evokes a purposive change of hormonal and/or genital gender, proposed by a ‘transgender’ person, and constructed collaboratively amongst patients, surgeons, and mental health professionals. Within the transgender framework, gender is conceptualized as a duality, and an aspect of identity rather than solely of anatomy. In the 18th century, the premodern model of gender fluidity and a one-sex body competed with the notion of an anatomical gender duality (Foucault, 2010: 2). 1 In France and Britain there was no ‘single, unified medical opinion about which traits should count as essentially signifying feminine or masculine’ (Dreger, 1998: 16). But it is clear from Mr Brand’s case study that—whatever the theory—the surgeon and physician were in charge of gender assignment, not the patient or his parents.
Mr Brand’s case study was published at 1 Soho Square, and sold in various parts of London by G Nicol, J. Murray, and J. Bew (see Figure 1). G Nicol was ‘Bookseller to his Majesty.’ The author describes himself as ‘Thomas Brand, Surgeon,’ a less elaborate description than the one he chose for another treatise published in the same year: ‘T. Brand, Member of the Corporation of London Surgeons, and Surgeon Extraordinary to his Majesty’s Royal Hospital at Greenwich’ (1787b). The lengthy title of the case study—a sort of outline of all the topics covered in it—was typical of 18th-century practice. Books were often sold without bindings, so the title page of the book functioned to attract the potential purchaser (Barchas, 2003: 14). Extra copies of the title page were printed off and posted on walls—like movie posters today—to attract the notice of buyers. If ‘a Boy… Mistaken for a Girl’ did not arouse interest, then ‘Three Anatomical Views of the Parts’ might.
Title page of Thomas Brand’s book 1787.
Mr Brand’s case study is written in English, in a readable but partially unfamiliar print style. Before the 18th century many medical treatises were written in Latin in order to communicate with medical readers who might speak English, German or French but always knew Latin. Several Latin words and phrases are used in the text, for example ‘lusus naturae,’ which translates roughly as ‘freak of nature,’ and is used to describe a simplistic and hermaphroditic (not Mr Brand’s) interpretation of bodies exhibiting irregular genitalia.
The language of genitalia is hedged. In the title, the term ‘The Parts’ is not specific about which bodily parts are at issue, although the context of ‘Girl’ and ‘Boy’ make it rather clear. It was typical of 18th-century medical texts to use Latin terms for genitalia in order to conceal matters from the prurient gaze of non-medical readers; Mr Brand uses the terms ‘labia pudendi’ and ‘corpus penis’ to describe the parts he is interested in for his case study.
The three illustrations of these genitalia are drypoint engravings 2 done on copperplate (see Hoolihan, 1998). They consist of frontal views of her/his genitalia, and the abdomen from the waist to the upper thighs. Medical illustrators of the 18th century aspired to both anatomical faithfulness and cultural commentary, the first through careful observation, the second through the addition of decorative elements that might include anything from trees to farmhouses to horses to desks and chairs (Kemp, 2010; Ollerenshaw, 2000). Mr Bell’s engravings seem detailed and realistic, but are less elaborate than some 18th-century medical illustrations. The decorative elements consist of crosshatching and what appears to be the child’s clothing pulled up and down from the waist.
Who was Mr Bell? No details—such as the illustrator’s first name—are given by Mr Brand beyond the surname. There were two ‘Bells’ in 18th-century Britain who were famous as physicians and medical illustrators—John, and Sir Charles—but they would have been 16 and 5, respectively, at the time of the case study. John Bell’s later medical illustrations are much more elaborate than those in Mr Brand’s case study (see Kemp, 2010)—although I suppose he could have been practicing for the future as a 16 year old. Mr Bell—or an assistant—surely, must have made on-site images of the seven-year-old patient—who I don’t think would have sat still for the engraving process—possibly by using a camera obscura (see Ollerenshaw, 2000).
This case study illuminates several aspects of 18th-century anatomical study: the nature of the gendered body, the structure of medicine within the social structure, and the place of the patient in these arguments and structures. Debates over the one-or two-sex body and the existence of hermaphrodism were competitive not only in journals but also in the quest for patients, fees and fame by physician and surgeon anatomists (Stolberg, 2003: 291). Mr Brand, a surgeon, frames his case study in a disputation over the existence of hermaphrodites. He also makes the claim that surgeons—himself in particular—have more accurate practical knowledge of anatomy than physicians, although surgeons were at that time of lower status. He also makes clear, albeit implicitly, that he has authority over the child’s body and the child’s parents, not just because they were of a ‘lower rank’ but because medical outranked individual, parental, legal or other forms of authority over the body in the 18th century.
The case study
Mr Brand’s case began with a referral from his mentor, Dr Armstrong, a well-known 18th-century physician, who had founded the Soho Square Dispensary for the Relief of the Infant Poor in 1769 during the ‘dispensary movement’ of the mid-1700s (Picard, 2000: 96). A couple brought their seven-year-old ‘daughter’ to this clinic in 1779. Dr Armstrong suspected a rupture (hernia), and ‘sent the patient for my opinion.’ Mr Brand concluded that ‘There was no rupture,’ rather, ‘an irregularity in the external parts.’ (1787a: 6).
At first the child seemed, to Mr Brand, to have female genitalia with an imperforated hymen, which, as is well known, is not a very uncommon mal-formation; and, what at first gave some reason for this opinion, in the present case, was that the skin over that part where the hymen is naturally situated, was extremely thin and vascular, and it discharged a thin mucus. (1787a: 6)
Mr Brand examined the child, ‘found that the part, which had the appearance of the labia pudendi, was in fact the scrotum… the corpus penis was bound down so tight, by its froenum, that it put in very much the appearance of a clitoris’ (1787a: 6). Mr Brand then ‘invited’ Dr Hunter, Mr Hunter, Dr Osborn and Dr Denman to examine his patient, and proposed an ‘operation to free the penis from its confinement.’ (1787a: 6). Mr Hunter ‘approved’ of the suggested operation, and Mr Brand ‘performed it before him.’ (1787a: 7).
The operation consisted of a longitudinal incision on each side of the penis, as close to the os pubis as I could safely go. It was also necessary to divide the froenum, which bound the glans down … After I had divided the skin as best I could, I made a stitch on each side in the angle of each incision, for the purpose of producing as much length to the part as I was able. (1787a: 7)
This case study offers a remarkable window into 18th-century sexual medicine: its gender debates, surgical practices, and professional and social contexts, all of which were played out in sites of competition such as medical journals and the Royal Society, and within tussles between surgeons and physicians. The treatise also offers insights into the place of the patient in medicine—both the working-class child and—as we will see later—a wished-for upper-class patient. These themes, and the writing up of the case study itself, are framed within linked post-medieval debates: whether there are one or two sexes, and whether human bodies can be hermaphroditic, or must (be made to) conform to a duality of gender. Although the two-sex model of gender that he espouses generally admits the possibility of hermaphrodism (Stolberg, 2003: 288), Mr Brand is having none of it. Indeed, he issues a salvo on the first page of his case study: By the term hermaphrodite is properly understood as an animal that has both the male and female organs equally and perfectly formed. But …there is no reason to believe that such a case ever had existence in the human subject. (1787a: 2)
Hermaphrodism in the one- and two-sex body
The western concept of hermaphrodism originated in Greek mythology. Hermaphrodite, a fusion of his parents Hermes and Aphrodite, was further fused with a nymph, Salmacis, resulting in a body with aspects of both genders (breasts, penis, testicles, ovaries, uterus, vagina). The concept of hermaphrodism continued into Roman philosophy and medicine, reappearing in the Renaissance and Enlightenment as a philosophical medical and scientific category. Not all scholars from Greece to Freud agreed on the scope and nature of human hermaphrodism. Some scholars in the 16th and 17th centuries regarded the notion as ‘medieval superstition’ (Stolberg, 2003: 276). Paulo Zacchia in the Renaissance, and Robert Todd in the 19th century believed that physicians made false diagnoses of hermaphrodism in cases of large clitorisis (Laqueur, 1990: 161).
In the 18th century, anatomists developed their skills in the search for the meaning of ambiguous genitalia, seeking to assign male or female bodies and legal rights to persons. There was skepticism about the category, although some anatomical evidence argued for its existence: one 18th-century dissection was of a body ‘female on the right side… male on the left’ (Fontes da Costa, 2007: 83). Other scholars denied the existence of hermaphrodites, regarding all such cases as women with ‘deformed genitals’ (Fontes da Costa, 2007: 80). Mr Brand continued in this skeptical tradition, but with a novel claim: a child with erroneous female genitalia—a secret, hidden male.
The debate over the legal and medical status—or even existence—of hermaphrodites took place in the context of the Aristotelian ‘one-sex’ vs. the Hippocratic ‘two-sex’ body (Stolberg, 2003: 285). Prior to about 1600 in northern Europe, somewhat later in Iberia (Cleminson and Garcia, 2013; Stolberg, 2003), there was a shift from a one- to a two-sex model of gender; by the 18th century ‘individuals were increasingly saturated with gender.’ (Harvey, 2004: 6). As Dreger points out, even by the 19th century, French and British anatomists had very different ideas about ‘hermaphrodite theory and medical practice’ (Dreger, 1998: 16); the 18th century was a site of competition between the theories of ‘true’ vs. ‘pseudo’ hermaphrodites (Foucault, 2010: 2).
Mr Brand set out to perform an anatomical ‘deciphering of the true sex that was hidden between ambiguous appearances’ (Foucault, 2010: 2). In Mr Brand’s case study, the possession of a buried penis did not turn the woman into a man, but—once revealed—reassigned her/him to the ‘proper’ pre-existing gender. Although Mr Brand says that he won’t ‘enter… into a disquisition on the subject of supposed hermaphrodites,’ (1787a: 5) he in fact does so. He admits that there may be people who have no gender, and describes a case presented by Dr Hunter: The fore parts of the unhappy object were entirely wanting. It had the appearance as if the external parts of generation … had been cut off …there were no external parts that had the least resemblance to either the male or female organs, yet this unhappy object was vulgarly called an hermaphrodite. (1787a: 5)
Mr Brand casts doubt on (at most) the existence of human hermaphrodism or (at least) that some cases of hermaphrodism are actually something else—something that he will discover and disclose. He says that when genital ‘malformation’ is observed, the person so afflicted is referred to as a ‘hermaphrodite… an animal who has both the male and female organs perfectly formed’ (1787a: 2). Mr Brand recognizes the existence of hermaphrodites among animals, but adds that ‘there is no reason to believe that such a case ever had existence in the human subject’ (1787a: 2). He thus sets the stage—as a surgeon rather than a physician—for making his own contribution to the discourse on hermaphrodism. At the same time, he argues not only for the superiority of ‘modern’ over earlier anatomical knowledge, but for the superiority of surgeons over physicians in this area—in particular, Mr Brand himself.
Surgeons and physicians
Surgeons in England were, for centuries, in competition for status with physicians. In the 14th century there was a Guild of Surgeons in London; the Guilds were similar to trade unions in later centuries. By the 16th century, surgeons had joined with barbers into the Company of Barber-Surgeons, an arrangement changed in 1749 when the surgeons broke away from the barbers. Surgeons’ surge to the top—a Royal Charter—began in 1800 with the Royal College of Surgeons; a medical degree was required for members of the Royal College of Surgeons of England by 1843. English surgeons are still known as ‘Mr’ rather than ‘Dr’ in recognition of this history.
Surgeons and physicians were in competition, but they were also part of a complex system of medical referral, and communication. In this case study, Mr Brand consulted with, or was consulted by, a number of medical men, including Mr John and Dr William Hunter. Dr William Hunter was a well-known physician who established a teaching theatre and museum in London in 1768 (Buchanan, 2003: 1261); Mr John Hunter has been called ‘the Father of Surgery’ (Moore, 2005). Dr Osborn (Lord, 1999) and Dr Denman (1807) were ‘midwives’ and gynecologists; they were mentioned in a House of Commons Report on medical education (Royal College of Surgeons, 1834: 277).
Mr Brand surrounded himself with top-drawer expertise in anatomy, surgery and midwifery throughout this case. He both collaborated with and was deeply competitive with, these colleagues, comparing himself favorably with earlier surgeons (see also Brand, 1782) and with contemporary surgeons and physicians: Before the art of surgery was cultivated by men of science … when few surgeons were capable of performing operations but under the direction of physicians—when, in defect of medical knowledge …the forming of new theories and establishing of systems seem to have engrossed attention rather than the art of curing diseases. (1787a: 4)
Although some 18th-century anatomists allowed for the possibility of human hermaphrodites, others sought to distance themselves from ancient mythologies and ‘erase the concept and the figure of the hermaphrodite’ from the Enlightenment (Fontes da Costa, 2007: 81). Both surgeons and physicians could profit from successful anatomical demonstrations of ambiguous gender, and ‘these opportunities could have significant implications for their professional status and credibility’ (Fontes da Costa, 2007: 79). The theme of practice vs. theory informs Mr Brand’s views of hermaphrodism, which, for him, is based on empirical observation rather than Galenic or other models of gender. As a ‘pupil’ of the ‘late Dr. Hunter, Professor of Anatomy’ (1787a: 5), Mr Brand takes on Dr Hunter’s take on hermaphrodism.
Mr Brand described Dr Hunter’s demonstration of a case of such ‘defect of the parts’ that the person had no genitals at all, and was yet ‘vulgarly called a hermaphrodite.’ The other surgeons and physicians mentioned by Mr Brand would also have classified the child he treated as a ‘hermaphrodite’—a classification for which he had ‘contempt.’ He describes non-scientific surgeons as quacks, who ‘in defect of real knowledge… fought to bring themselves into notice, by rendering every thing [sic] as mysterious and marvelous as possible… we find attempts made to establish doctrines which had no foundation in truth, and only existed in the wild and extravagant imaginations of those who suggested them’ (1787a: 4). Mr Brand’s former teacher, Dr Hunter, was wrong in presenting the genitalia-less ‘object’ as a hermaphrodite. Dr Armstrong, the Soho Dispensary physician, was wrong in the initial diagnosis of his seven-year-old patient with a rupture (1787a: 6).
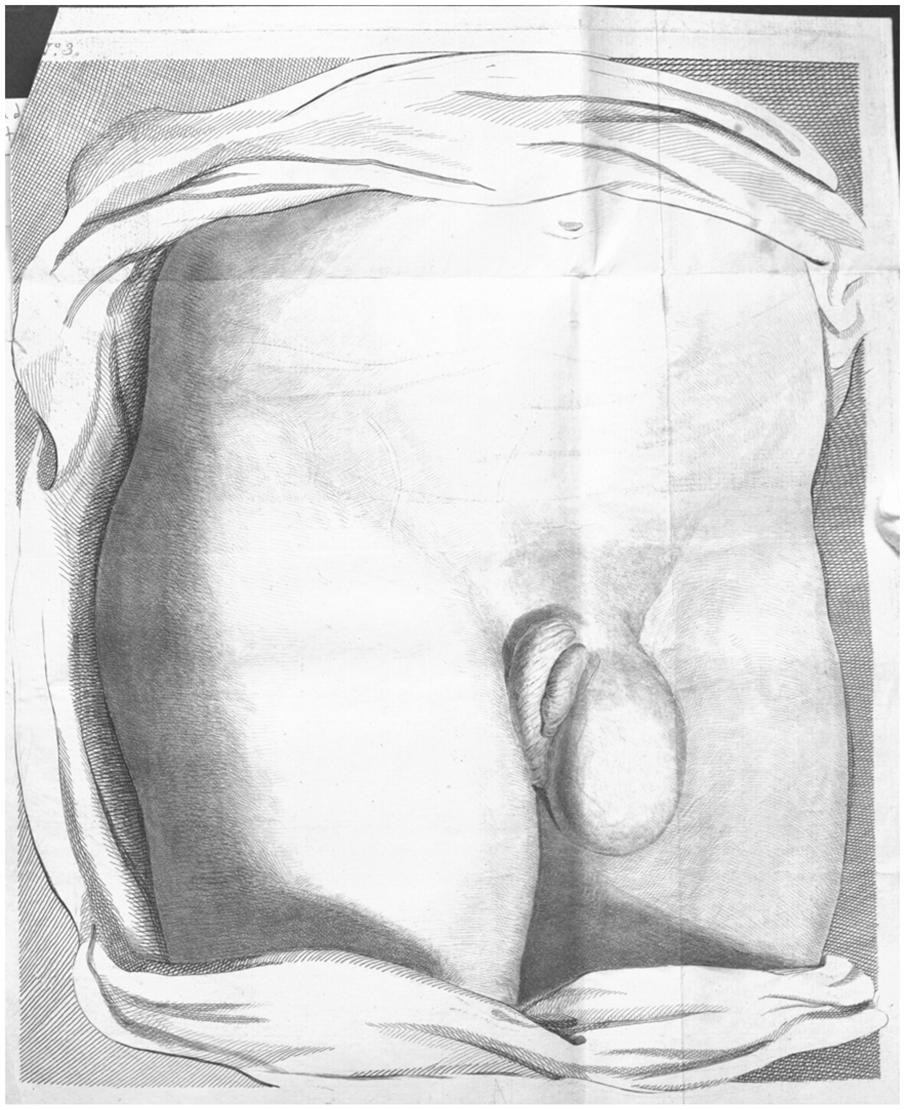
Mr Brand even seemed to have a superior anatomical artist in Mr Bell: the third illustration he provides gives a view of the patient’s ‘hydrocele’ as ‘perhaps more correctly drawn than some that have been published’ (1787a: 8). This illustration provides, for Mr Brand, the final evidence that the patient was not a hermaphrodite—nor a woman who ejected her penis to become a male—but a born male. A hydrocele, otherwise known as a ‘watry Rupture’ is ‘a collection of water… in the… testis’ (Brand, 1782: 53) and occurs only in males. Therefore, it proved, to Mr Brand, that the patient was really a male, and not a hermaphrodite.
But it was not enough to cure patients better than other surgeons or doctors did; publication of success stories was necessary. Mr Brand seems to have made somewhat of a name for himself in 18th-century medicine beyond this case study. In the same year, he published a lengthy treatise about misrepresentations made by Mr Foot about the medical writings of Mr Hunter (1787b). A few years later he published a treatise on the diagnosis and treatment of ruptures. He must have been somewhat of a businessman, too; trusses were made, at the time, using ‘Mr Brand’s principles’ (Brand, 1782: 75).
The publishing and dissemination of new medical knowledge and procedures was enormously significant in the 18th century, crossing boundaries of nationality and language, from England to America and back to Europe. There were many medical journals (more than 20 devoted to electricity in medicine alone), and there was the Royal Society for the presentation and scrutiny of scientific and medical findings. Competition—ultimately, for fame and fortune—threaded throughout the system of medical cooperation and communication, as it does today. As Stolberg (2003: 291) puts it, from the 16th century onward in northern Europe ‘a scientific reputation and a lucrative practice’ was based on ‘personal discovery and innovation over lengthy commentaries on ancient works.’ This personal discovery involved the body of the patient.
All empirically-based textual and visual representations of the human body from autopsies, examinations and surgeries have as their basis the human body of the patient, whether real or imagined. In Mr Brand’s case study, the patient’s body is the fulcrum around which pivot debates over hermaphrodism, and competition between anatomists—but the patient him/herself is seen only indirectly, as a shadow.
The patient
In Mr Brand’s text, the seven-year-old child patient is presented in anatomical words and illustrations. His/her name is not given, although it was commonplace in the 18th century to provide the names of patients—as well as doctors—in case studies, so that readers could track down the patients and verify the treatment. Neither the child’s nor the parents’ names were given in this case study, although Mr Brand did provide patients’ names in his treatise on ruptures (Brand, 1782). There is no mention of parental consent, informed or otherwise. Only the consent of the doctors and surgeons was, apparently, relevant.
The child is most present in the three illustrations of her/his body made by Mr Bell; there is no face, and no identity. These illustrations separate the child’s body at the waist, showing only abdomen, genitalia, and a few inches of thigh, clothing pulled away from the body. Given the relationship of gravity and genitalia, the torso seems to be standing or propped up rather than lying down. His first drawing (see Figure 2) is of the parts in their original state. They are turned up a little, and the skin which covered the glans penis (supposed to be the clitoris) is drawn back in order to bring that part into view. Without this, the external parts, left to themselves, would have had almost the precise appearance of the labia pudendi. (1787a: 7)
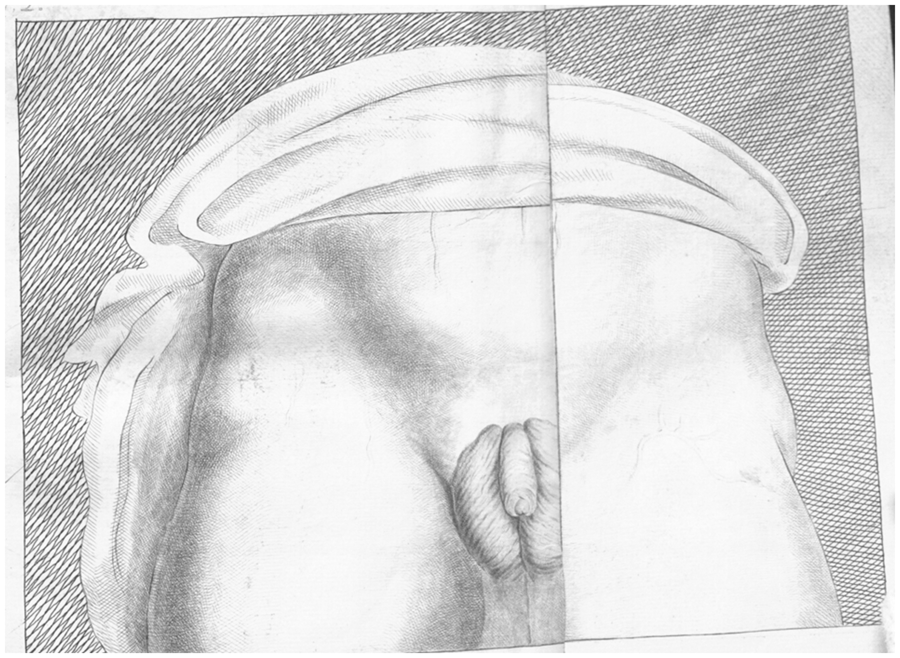
The first drawing in Brand’s book showing the child’s body before the operation. The third drawing showing the effect of hydrocele on the child’s scrotum. The second drawing, which shows the child’s body after the operation.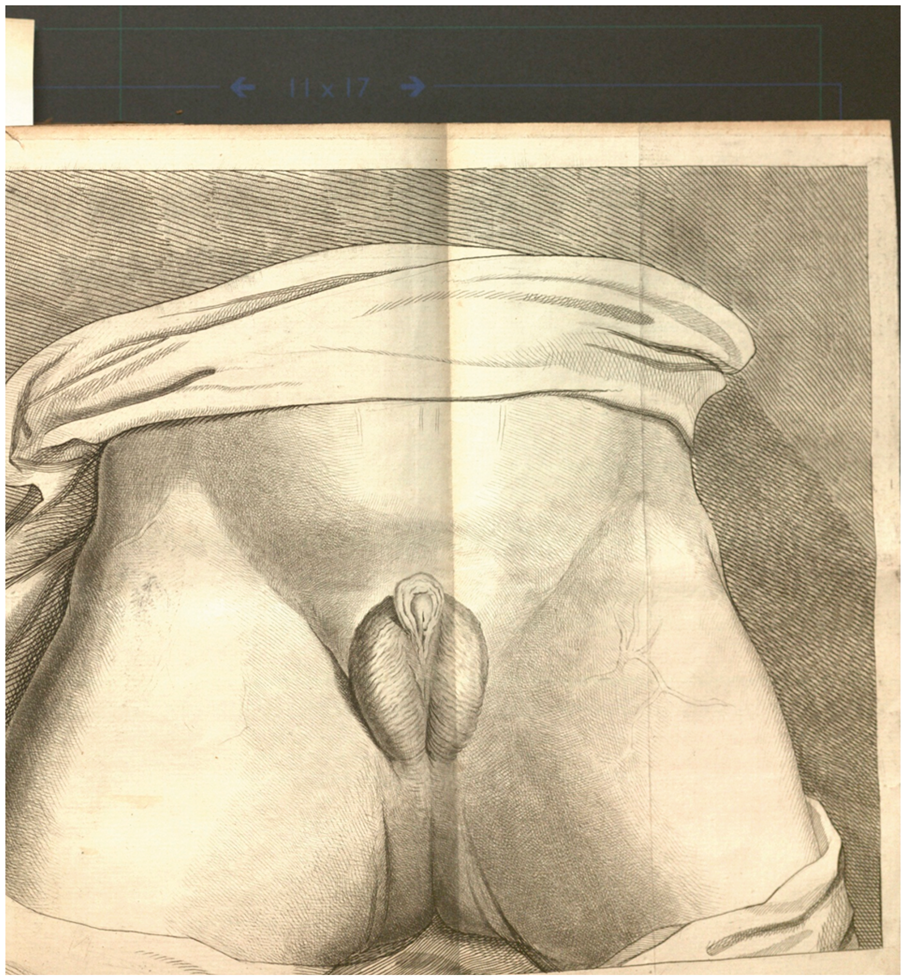
Mr Brand says almost nothing about the child or parents, noting that ‘the child was baptized as a female, and brought up and educated under that belief till seven years of age,’ and adds that ‘I shall not trouble the reader with the surprise into which the parents were thrown when I first told them their child was not a girl, as they had supposed, but a boy’ (1787a: 7). Nothing was said about if or how the child was sedated during the surgery, or how s/he responded to bodily redirection after it. Mr Brand’s predominant gender concern, as we saw earlier, was penis length. He also worried that this mis-labeled boy had to urinate sitting down before the operation; after it, ‘he performed this function like any other boy’ (1787a: 7). Standing to urinate was one of the many 18th-century male privileges bestowed by a penis (Laqueur, 1990) along with trousers and a medical education.
Social class threads its way through the text, with Mr Brand noting that the patient and parents came from the Soho Dispensary for the Poor, indicating that they were working class. We know that they were astonished to find out that their daughter was really a son. But even after the third illustration was made, ‘some time after the cure was performed’ (1787a: 8) nothing was learned about what had happened to the child or parents, beyond the medical conclusion that ‘the case… went on very favorably’ (1787a: 7). Mr Brand concludes by meditating upon an idealized ‘better’ patient—a ‘child of rank’ who would give THAT case interest and importance: Considered as a Lusus Naturae, this case may be ranked as extraordinary. As an anatomical fact it has been thought sufficiently interesting for me to publish it, and it is easy to believe, that if the same kind of mal-formation should ever happen to a child of rank, it might prove an interesting and important case. (1787a: 8) F I N I S
Footnotes
Acknowledgements
Thanks to the following people who helped with various stages of this project: Ken Plummer, Agnes Skamballis and the anonymous reviewers of Sexualities, Kathryn Kirigin, Kelley Massoni, Judy Mandel, Myra Kallen, Carol Gray, Doris Besikof, and Susan Case (in memoriam).