
Abstract
This study explores the difficulties that older lesbian, gay and bisexual residents may encounter when attempting to express their sexuality while living in long-term care facilities (LTCF), as perceived by staff. The sample was made up of 1714 staff members working in 152 Spanish long-term care institutions for older people. Answers to an open-ended question regarding barriers that older lesbian, gay and bisexual people living in residential institutions may face when attempting to express their sexuality were content-analysed. The results suggest that the barriers are almost exclusively caused by other people’s views on non-heterosexual issues, including both heterosexist assumptions (e.g. the lack of awareness of sexual diversity in LTC settings, something that is particularly frequent among care assistants) and homophobic attitudes and behaviours generally attributed by technical staff and managers to heterosexual residents. Practical and policy implications, which should take into account job role as a key factor, are discussed.
The sexuality of older people living in long-term care facilities (LTCF) is an issue that is frequently neglected by staff and relatives, who sometimes assume that sexual needs and expression disappear following admission to a LTCF or communal residence (e.g. Doll, 2012). Such beliefs are in tune with traditional widespread images depicting older people as asexual (Gewirtz-Meydan et al., 2018).
However, although sexuality may no longer be a priority (or maybe was never a priority) for some older residents (Simpson et al., 2018b), studies on these issues suggest that sexual expression and sexual needs are not uncommon among older people living in LTCF. For instance, Bauer et al. (2013) showed that most residents see themselves as sexual beings who still experience sexual needs. In addition, managers of LTCFs acknowledge that issues regarding sexual activities frequently arise in this setting (Lester et al., 2016). In a similar study, more than half of staff members working in Spanish LTCFs have witnessed residents’ explicit sexual expression (Villar et al., 2019b).
However, living in an LTCF poses serious challenges regarding expressing sexual needs, and previous studies have identified some of the barriers that prevent older people from expressing themselves as sexual beings. Such barriers include lack of privacy (Bauer et al., 2013), negative attitudes of staff (e.g. Gilmer et al., 2010), and other residents’ views on sexuality in older age (e.g. Villar et al., 2015a). Such barriers are also present for lesbian, gay and bisexual (LGB) and trans-sexual residents, who face additional challenges that do not affect their heterosexual peers and seriously compromise the preservation of their sexual rights. This study focuses only on LGB residents, since issues regarding non-normative gender are quite specific and justify separate studies.
Previous studies on LGB people living in LTCFs have highlighted at least two types of specific hindrance. The first is related to homophobic prejudices and practices within residential settings. Studies on LGB access to health care and social services, including LTCF, show that prejudices and discrimination against non-heterosexual individuals are not uncommon (Grant et al., 2010; National Senior Citizens Law Center, 2010). Although some studies have found that staff usually express respect and tolerance toward LGB residents (Ahrendt et al., 2017; Villar et al., 2015b), other studies have detected signs of prejudiced attitudes (Dorsen, 2012; Schwinn and Dinkel, 2015) among staff, particularly when non-heterosexual relationships are compared to heterosexual ones (Hinrichs and Vacha-Haase, 2010). In any case, a lack of supporting practices specifically addressed at LGB residents is widespread among LTCF professionals, as shown by studies from Spain (Villar et al., 2019b) and the UK (Simpson et al., 2018a). This situation could be partially attributed to the minimal (if any) formal training on LGB issues (Bell et al., 2010), which fuels staff’s feeling of not being prepared to provide adequate care of sexual diversity (Neville et al., 2015).
Other residents could also be a source of homophobia and hostility (Knochel et al., 2011). For instance, when faced with a hypothetical situation in which a fellow resident discloses his or her non-heterosexual sexual identity, most residents interviewed by Villar et al. (2015b) expressed negative attitudes, ranging from simply keeping one’s distance to active rejection, sometimes expressed in a bluntly open way. This situation feeds fears of being mistreated, rejected or ostracized, fears that are probably also based on long-lasting previous life experiences, and that may lead the individual to ‘go back into the closet’ or at least to selectively conceal their sexual identity (Westwood, 2016), which in turn increases isolation and hampers peer and institutional support.
The second barrier highlighted by the literature is perhaps more insidious and subtle than open prejudiced attitudes and discrimination, and refers to the widely shared assumption of heteronormativity, that is, the belief that the heterosexual experience is the ‘normal’ human experience (Yep, 2002). From that perspective, non-heterosexual sexual identities and orientations are thought to be irrelevant to providing care, which is conceived as sexually neutral. Consequently, the taken-for-granted heterosexual assumptions remain unquestioned, which help to reinforce the invisibility of LGB residents in LTCF and neglect their specific social and care needs (Willis et al., 2016). In fact, the failure to recognize the existence of LGB residents or, even if they are recognized, a well-meaning emphasis on the ‘sameness’ of treatment, in other words, applying a heterosexist standard of care to all the residents regardless of their sexual orientation, sexual background or sexual biography, might lead to the entrenchment and exacerbation, rather than elimination, of inequalities (Simpson et al., 2018a; Willis et al., 2016). Consistent with this, some studies emphasize that, according to LGB people, the extent to which formal caregivers are aware of and feel comfortable with sexual diversity is an important ingredient for experiencing quality in care (e.g. Grigorovich, 2016).
Based on the foregoing findings, it seems clear that in relation to barriers experienced by LGB residents, the role of staff is key, since they are in charge of providing direct care for residents (including how to handle sexual needs and sexual expression) and enacting institutional care policies to guarantee rights and equality. They are also supposed to be responsible for detecting and eradicating any discriminatory practice, including those related to sexual orientation, and for supporting sexual diversity (Donaldson and Vacha-Haase, 2016; Porter and Krinsky, 2014).
Existing studies on staff perceptions of barriers to and difficulties for residents’ sexual expression often involved small samples and tended to consider staff in an undifferentiated way, ignoring the diversity of professional roles (e.g. Aguilar, 2017; Mahieu et al., 2016). However, the position within the organization of different professionals may influence their views on barriers that residents, and specifically LGB residents, have to face and, consequently, also how they deal with these issues. Thus, while managerial staff are mainly responsible for designing inclusive policies, the everyday enactment of these policies is the responsibility of the care assistants, who also both provide direct care and support to LGB residents and handle their sexual needs and rights. Located in the middle ground, technical staff, coming from both health and social fields, are better suited to supervising and supporting the application of policies, and providing specialized care or counselling if it is needed. Different job roles also involve different amounts and types of training. In that respect and ironically, care assistants, who are ultimately responsible for recognizing and supporting LGB residents’ needs, are at the same time those with the least formal training on sexual issues, including sexual diversity (Villar et al., 2017).
Despite the potential importance of job role on sexual issues in LTCFs, only a few studies have specifically explored its influence (e.g. Bouman et al., 2007; Mahieu et al., 2016). These studies have found that, compared to care assistants, staff in higher positions (e.g. managers or technical staff) tend to have more knowledge about and be more permissive and sensitive to residents’ sexual needs. To the best of our knowledge, only one study has explored working position in relation to LGB issues in nursing homes. In that study, Simpson, Almack and Walthery (2018a) found that care assistants considered themselves to be less knowledgeable about LGB issues, and reported being both less trained and less keen on additional training on these issues than managers. However, that study did not examine the perception of barriers for LGB residents. Exploring this issue could give us some important clues about to what extent staff carrying out different tasks within an organization are aware of the presence of some homophobic and heteronormative beliefs and, consequently, to what extent they are prepared to break down these barriers and give adequate support to the needs of LGB residents.
The present study aimed to fill this gap in knowledge by exploring the type and frequency of difficulties that staff in different job roles (managers, technical staff and care assistants) perceive that LGB residents may encounter when attempting to express their sexuality while living in LTC facilities.
Methods
Participants
We found 1714 staff members who were working in LTCF to volunteer to participate in our study and supply the requested information. They belonged to 152 institutions, and all 17 Spanish regions had at least two LTCF in the study.
Women made up 86.5% of the respondents, which reflects the degree of feminization of residential care staff in Spain (Tobaruela, 2003). The mean age was 39.75 years (SD = 10.74), ranging from 18 to 70 years. The study included managers and directors (8.9%), technical staff (31.9%) such as doctors, nurses, psychologists, occupational therapists and social educators, and care assistants (59.3%).
To be selected for participation in the study, LTCFs had to be included in the authorized register of residential centres of their corresponding regions. Additionally, LTCFs had to provide long-stay care for older residents, as we are interested in the barriers experienced by older people actually living in institutions. Accordingly, we excluded palliative care units, acute or short-stay care units, and day-care centres.
Instruments
Description of the sample.
The second section included a series of both open-ended and multiple alternative questions aimed at gathering staff’s perceptions on barriers to and management of different kinds of sexual expression in residents. The data analysed in this article were obtained in response to one of the open-ended questions, as follows: ‘The main difficulties that lesbians, gay men and bisexual people living in residential institutions may have when attempting to express their sexuality are …’.
Procedure
After obtaining agreement from the 152 selected LTCFs to collaborate in the study, 3627 questionnaires were sent by mail, of which 2295 were returned, giving a response rate of 63.3%. However, 581 questionnaires did not include a response to the question that was the focus of this study, and consequently were discarded from the final sample. The rate of no-response to the question about barriers for LGTB was far higher for care assistants than for managers or technical staff (χ2 (2) = 73.46, p < 0.001).
In each LTCF a member of staff was designated to coordinate the administration of the questionnaire. The number of questionnaires that the designated person thought could be collected in his/her centre was sent to him/her by mail. To standardize the application of questionnaires, the envelope also included a written protocol with indications about which professionals should be invited to participate, how to assure confidentiality and how to collect, store and return the questionnaires. The designated person delivered the questionnaires to the participants, who answered them individually and gave them back to him/her once completed.
The questionnaire included an informed consent section on its first page, explaining the objectives of the study and assuring the anonymity and confidentiality of the data that would be provided. Participants had to sign their consent. No compensation of any kind was offered or received for their participation. The process was approved by the Ethics Committee of the Faculty of Psychology of the University of Barcelona.
Analytic strategy
Authors 3 and 4 transcribed the participants’ responses and entered them into a database. After that, a content analysis was conducted..
Firstly, researchers read all the responses to become acquainted with the data. Secondly, they isolated units of meaning (ideas) within each response. That is, as responses could contain one or several ideas, researchers identified the number of separate, different ideas contained in each response. These different ideas, or units of meaning (rather than the complete responses), were the ones that were subsequently categorized. Thirdly, they independently created categories, or groups of units of meaning, inductively created according to similarity or repetition of keywords (Krippendorff, 2013). Fourthly, categories obtained by each researcher were compared and differences were discussed until a consensus on the category system was reached. Once the researchers had reached an agreement, categories regarding the different types of difficulties LGTB residents have to face were subsequently grouped into those describing a specific barrier or difficulty and those that did not describe any specific barrier or difficulty. This latter group included answers expressing ignorance, absence of LGB residents in their centre, nonspecific barriers or simply denial of the existence of any barrier.
Categories (including definitions and examples) regarding difficulties LGB residents have in expressing their sexual needs and identity in LTC facilities. Each example includes the respondent’s work position, gender and age.

Once the category system had been created, an independent judge (researcher 5) who had not participated in the previous process received a randomly selected 20% of the units of meaning, and the category system with category definitions. Her task was to assign units of meaning into categories. By means of the kappa reliability index, her independent categorization was compared to the one upon which researchers had agreed. The kappa index was .88, which indicates very good reliability (Landis and Koch, 1977).
The frequencies of types of difficulties and the different actors responsible for these difficulties were calculated. In the case of difficulties, a χ2 test was applied to check differences in category frequencies among work positions.
Results
The participants’ experience with non-heterosexual residents was infrequent. Thus, only 3.8% of participants mentioned having witnessed a situation involving non-heterosexual sexual relationships in the LTCF. A higher, but still relatively low percentage, 9.3%, mentioned having known residents who openly disclosed their non-heterosexual sexual identity. These percentages did not vary significantly among work positions.
Frequency and percentage (in brackets) of barriers/difficulties mentioned by our participants, according to their work position.

*p < 0.05; ** p < 0.01; *** p < 0.001.
Most of the participants who did not mention any specific barrier (23.6%) simply stated that they did not have any non-heterosexual residents in the LTCF in which they worked, while 5.9% said that there was no barrier or difficulty. Both lack of heterosexual residents (χ2 (2) = 14.98, p < 0.01) and absence of any barrier (χ2 (2) = 9.22, p < 0.05) were more frequently mentioned by care assistants than by managers or technical staff. However, comparisons according to gender, age or intensity of religious beliefs were not statistically significant.
Six out of 10 participants did mention a specific barrier or difficulty regarding LGB residents. These barriers were of various kinds, the most frequent being homophobia, both in terms of prejudiced beliefs (e.g. ‘homosexuality is frowned upon by people of older generations’, technical staff, female, 32) or discriminatory practices (e.g. ‘Gays and homosexuals are rejected by their peers’, manager, female, 54). The category ‘homophobia’ was more frequently mentioned by managers and technical staff than by care assistants (χ2 (2) = 14.54, p < 0.01). In contrast, there were no differences according to gender, age and intensity of religious beliefs.
The presence of fears or lack of freedom to disclose their sexual identity was mentioned as a difficulty by 12.3% of participants (e.g. ‘I suppose that gay men, and maybe also lesbians, are afraid of being mocked if they come out of the closet’, care assistant, female, 28), being more frequently mentioned by managers and technical staff than by care assistants (χ2 (2) = 8.15, p < 0.05). However, comparisons by gender, age or intensity of religious beliefs did not yield any statistical difference in this category.
A total of 9.2% of participants stated that LGB residents are misunderstood (e.g. ‘Some residents cannot simply conceive that a man could be sexually attracted by another man: for many, this is simply out of the question’; technical assistant, male, 40), while a lack of privacy and lack of peer support were mentioned by even lower percentages, 2.8% and 1.5% respectively, with no differences according to job role, gender, age or intensity of religious beliefs.
Frequency and percentage (among brackets) of actors perceived as being responsible for the barrier/difficulty.
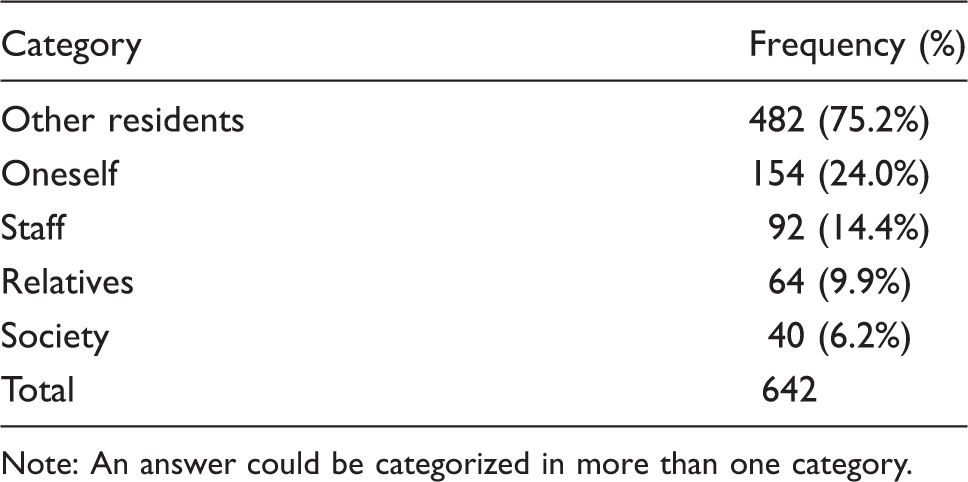
Note: An answer could be categorized in more than one category.
Discussion
The objective of the study was to identify the kind of difficulties that staff working in different positions (managers, technical staff and care assistants) perceive that LGB residents may encounter when expressing their sexuality in LTC facilities.
In this respect, most staff members have had little experience with LGB residents, and only 10% of them have ever known a resident who openly expressed their non-heterosexual sexual identity. This finding, which is similar to the kind of response ‘we don’t have any at the moment’, which frequently appears in qualitative responses in studies such as the one by Simpson, Almack and Walthery (2018a), suggests that many LGB residents opt to remain invisible and sacrifice the open expression of their identities and needs: staff do not have any experience with LGB residents probably because many of them have chosen to hide their identity, which may reinforce existing heteronormative beliefs, closing a vicious circle. At the same time, not having (apparently) any LGB resident functions as a reason to downplay LGB issues and the extent to which sexual diversity could challenge established assumptions on care, the quality of care one is able to provide and the training one should have on these issues. So, many participants deny the existence of any specific difficulty posed by LGB residents as they do not knowingly have any of them, and thus they cannot mention any difficulty, a stance similar to the ‘out of sight out of mind’ attitude found by Neville et al. (2015) among LGB staff when asked about LGB residents. Others said that there were no difficulties for LGB people in their nursing home, or that difficulties were the same as for heterosexual residents.
In any case, these results suggest that many staff members are not informed or simply are not aware of the challenges and specific needs posed by sexual diversity in LTC facilities. A lack of LGB issues in their training, assumptions of heteronormativity and the effort of some LGB residents to remain invisible may at least partly account for these results. The apparent ignorance shown by many professionals, and particularly by many care assistants, might contribute to the neglect of the specific social and care needs of LGB residents. According to Willis et al. (2016), providing person-centred care to older LGB adults living in LTCFs involves being attentive to non-normative sexual lives and instilling LGB residents with sufficient trust and confidence so that they can share aspects of their sexual biography and needs. Obviously, the detached attitude detected in some of the responses, based on heteronormative assumptions, do not facilitate achieving this goal. According to our results, this attitude is particularly frequent among care assistants, that is, the people who are in charge of daily care tasks and who supposedly are, consequently, the ones with the easiest access to the intimate information needed to build stronger bonds of confidence with residents. The fact that they are more likely to mention that ‘we do not have any’ suggests that, at least in some cases, they fail to establish these confidence bonds and are less aware of the specific needs of LGB residents.
When specific difficulties were mentioned, categories regarding explicit recognition of heteronormativity (such as ‘incomprehension’ or ‘invisibility’) were not the most frequently mentioned categories, which suggests that heteronormativity acts in a subtle, often subconscious, way. In contrast, most of the difficulties identified by our participants concerned homophobia, in terms both of prejudices and direct discrimination. The fact that more than 40% of the whole sample (and 70% when just participants citing specific barriers were taken into account) indicated that homophobia is present in LTCFs prompted us to think about the importance of dealing with these open forms of mistreatment directed at LGB residents. Homophobic attitudes and behaviours clearly imply a violation of rights and might impel LGB residents to remain hidden, or to ‘go back into the closet’. Combined with heteronormative attitudes, homophobia is not just a source of suffering and distress, but may also result in becoming socially and emotionally isolated (Hughes, 2009; Jewell et al., 2011).
In comparison to care assistants, managers and technical staff were more aware of the stigma that LGB residents may suffer and their fears of being marginalized and harassed. This finding could be interpreted in optimistic terms, since recognizing the presence of a barrier is the first step towards overcoming it, and particularly since managers and technical staff are in the best position to design and enact specific policies targeted at deactivating homophobic attitudes and practices. However, these kinds of policies are not particularly widespread in Spanish LTCFs (Villar et al., 2019b), which suggests that even more effort and commitment are needed.
When the response mentioned the person that was to blame for LGB difficulties, most participants mentioned the residents themselves as the main source of barriers, and few of them recognized their own weaknesses and the potential contribution of staff to LGB difficulties. This finding may reflect staff’s assumptions about older people’s beliefs and values and about their limited capacity to change. When blaming residents, many participants did so on the grounds of the specific cultural and generational coordinates that attribute older people a higher level of conservatism in sexual issues and, particularly, more homophobic attitudes, as a result of the increasing visibility of LGB issues and recognition of LGB rights in recent decades. In the case of Spain, such a generational gap could be particularly intense, because although Spain seems to be a particularly tolerant country with respect to LGB issues (Smith, 2011), and is a pioneer in the enactment of laws recognizing same-sex couple rights, it is also true that older Spanish generations spent their youth in Franco’s regime, a dictatorship that severely curtailed liberties and rights, including sexual ones. Under Franco’s rule, non-heterosexual practices were considered dirty and sinful, and lesbians, gay men and bisexuals could be incriminated and imprisoned (Pérez, 1994). In addition, although younger people are mostly secular, Spain has traditionally being a Catholic country, and Catholicism is particularly conservative with respect to sexual issues (Curran, 1992). Taken together, these cultural and historical contexts could explain why, according to staff perception, heterosexual residents in LTC facilities may hold particularly homophobic attitudes, whose consequences could even be amplified in the closed social network of an institution.
Although previous studies examining the attitudes of Spanish residents support the presence of prejudiced and discriminatory attitudes (e.g. Villar et al., 2015b), there also lies a risk in exclusively blaming residents for their LGB counterparts’ difficulties: staff may think that nothing can be done (after all, the traditional prejudice says that ‘old dogs cannot learn new tricks’) and, what is more, that they cannot improve their own practices to better meet LGB needs, particularly in relation to the more subtle forms of harm related to heteronormativity.
Limitations
To interpret these results, we must take into account the limitations of the study. Firstly, although the sample was very large, it was gathered using a non-probabilistic procedure in a specific country, which limits the generalization of results. Secondly, the study asked about LGB residents as a whole, when it is likely that gay men, lesbians and bisexual people have some common difficulties, but also some specific ones not addressed in this study. In addition, difficulties that transgender people may have (which may differ from those faced by LGB residents) were not covered by the study. We would need further research to determine those particular difficulties.
Conclusions and recommendations
The main contribution of our study to the incipient but growing literature on sexual issues concerning people living in an LTCF is that it highlights the specific barriers that, according to staff, LGB people must cope with when living in an LTCF, and how this perception of barriers may depend on job role. In fact, the main finding of the study is that most staff members are able to mention at least one specific barrier that LGB residents have to face. If no specific barrier is mentioned, ignorance, lack of recognition or lack of experience with LGB residents are the main reasons given. These results tend to support a view of LGB residents as particularly marginalized and stigmatized in LTCFs – a view, at least according to staff perceptions, that leaves hardly any room for optimism. Only 4.1% of the participants said that there were no barriers, and 4.8% said the barriers are similar to the ones experienced by other residents; however, the degree to which these responses could be interpreted in optimistic terms is open to debate.
In fact, the results of this study also differ from those studies focused on heterosexual residents, which emphasize that the lack of privacy or the standardization and collectivization of live-in institutions are significant barriers to sexual expression (e.g. Bauer et al., 2013). In contrast, our results suggest that in the case of LGB residents the barriers are overwhelmingly focused on people’s attitudes and practices. That is, according to staff, the main (and almost only) perceived barrier is based on other people’s views towards non-heterosexual issues, and mainly on the other residents’ stance. This stance includes both heterosexist assumptions (not just ignoring specific difficulties of LGTB residents, but also not being aware of sexual diversity in LTC settings, an assumption that is particularly frequent among care assistants) and homophobic attitudes and behaviours, which were more frequently mentioned by technical staff and managers, generally attributing these attitudes to heterosexual residents. We have discussed how such attitudes might feed each other and, when combined, contribute to hampering the LGB experience in LTC facilities. In fact, they represent a second layer of difficulties for sexual expression in these institutional settings, added to the ones also experienced by heterosexual residents.
To resolve this situation at least two measures could be put into practice. First, training on LGB issues should be improved to deactivate heterosexist and homophobic attitudes. In fact, training was identified as a key gap by previous research (Bell et al., 2010). Our results suggest that at least two key elements should be taken into account in the design of training on sexual issues. In the case of staff, training should be tailored depending on job role, since the needs of care assistants, technical staff and managers might not be the same. For instance, training in the case of care assistants should include rather basic aspects, such as the recognition of the presence of sexual diversity in LTCFs and the specific needs that LGB residents may have. Training should not be limited to staff, but should also include other residents. Homophobic attitudes and practices might be particularly entrenched among heterosexual residents, and this is likely to play a major role in the everyday experiences of their LGB counterparts in an LTCF. This fact leads to a second kind of measure: the need for appropriate institutional policies. Such policies, which must be explicit and involve all the relevant actors (at the very least, residents, staff, and relatives), should guarantee a sexually inclusive LTC setting. They might include the inclusion of LGB issues when assessing residents and collecting their life story, guidelines for handling sexual situations involving LGB residents so that their sexual rights are respected, and the design of protocols to detect and eradicate signs of homophobia (Lester et al., 2016; Shuttleworth et al., 2010).
Both training and policies could contribute to increasing the staff’s sensitivity towards LGB residents and help guarantee a skilled and homogenous response towards the specific social and care needs of LGB people, a response that not only needs to eliminate explicit homophobic practices, but also avoids the ‘treating everyone the same’ stance, which paradoxically boosts inequalities rather than eliminates them.