
Abstract
In this article, we illustrate how cognitive behavioral therapy (CBT) can be adapted for the treatment of PTSD among traumatized refugees and ethnic minority populations, providing examples from our treatment, culturally adapted CBT, or CA-CBT. CA-CBT has a unique approach to exposure (typical exposure is poorly tolerated in these groups), emphasizes the treatment of somatic sensations (a particularly salient part of the presentation of PTSD in these groups), and addresses comorbid anxiety disorders and anger. To accomplish these treatment goals, CA-CBT emphasizes emotion exposure and emotion regulation techniques such as meditation and aims to promote emotional and psychological flexibility. We describe 12 key aspects of adapting CA-CBT that make it a culturally sensitive treatment of traumatized refugee and ethnic minority populations. We discuss three models that guide our treatment and that can be used to design culturally sensitive treatments: (a) the panic attack–PTSD model to illustrate the many processes that generate PTSD in these populations, highlighting the role of arousal and somatic symptoms; (b) the arousal triad to demonstrate how somatic symptoms are produced and the importance of targeting comorbid anxiety conditions and psychopathological processes; and (c) the multisystem network (MSN) model of emotional state to reveal how some of our therapeutic techniques (e.g., body-focused techniques: bodily stretching paired with self-statements) bring about psychological flexibility and improvement.
Introduction
The treatment of traumatized refugees and ethnic minorities presents many challenges. They often have poor English fluency and minimal education, and many have a history of extensive traumas and are dealing with several types of stress, such as acculturation stress and that of living in poor urban areas with high levels of crime (Hinton & Lewis-Fernández, 2011). High levels of trauma and stress frequently combine with culturally generated catastrophic cognitions—for example, catastrophic cognitions generated by cultural syndromes—to bring about elevated rates of somatic complaints, comorbid anxiety disorders, and anxiety-type psychopathological processes such as worry, rumination, and panic attacks (Hinton & Lewis-Fernández, 2011; Hinton, Pich, Marques, Nickerson, & Pollack, 2010). Anger, another disorder of arousal, is also a major treatment issue in these groups (Hinton, Rasmussen, Nou, Pollack, & Good, 2009). As an additional treatment challenge, traditional exposure is usually poorly tolerated in these groups (Lester, Resick, Young-Xu, & Artz, 2010; Markowitz, 2010).
Sessions in CA-CBT and key components of the sessions
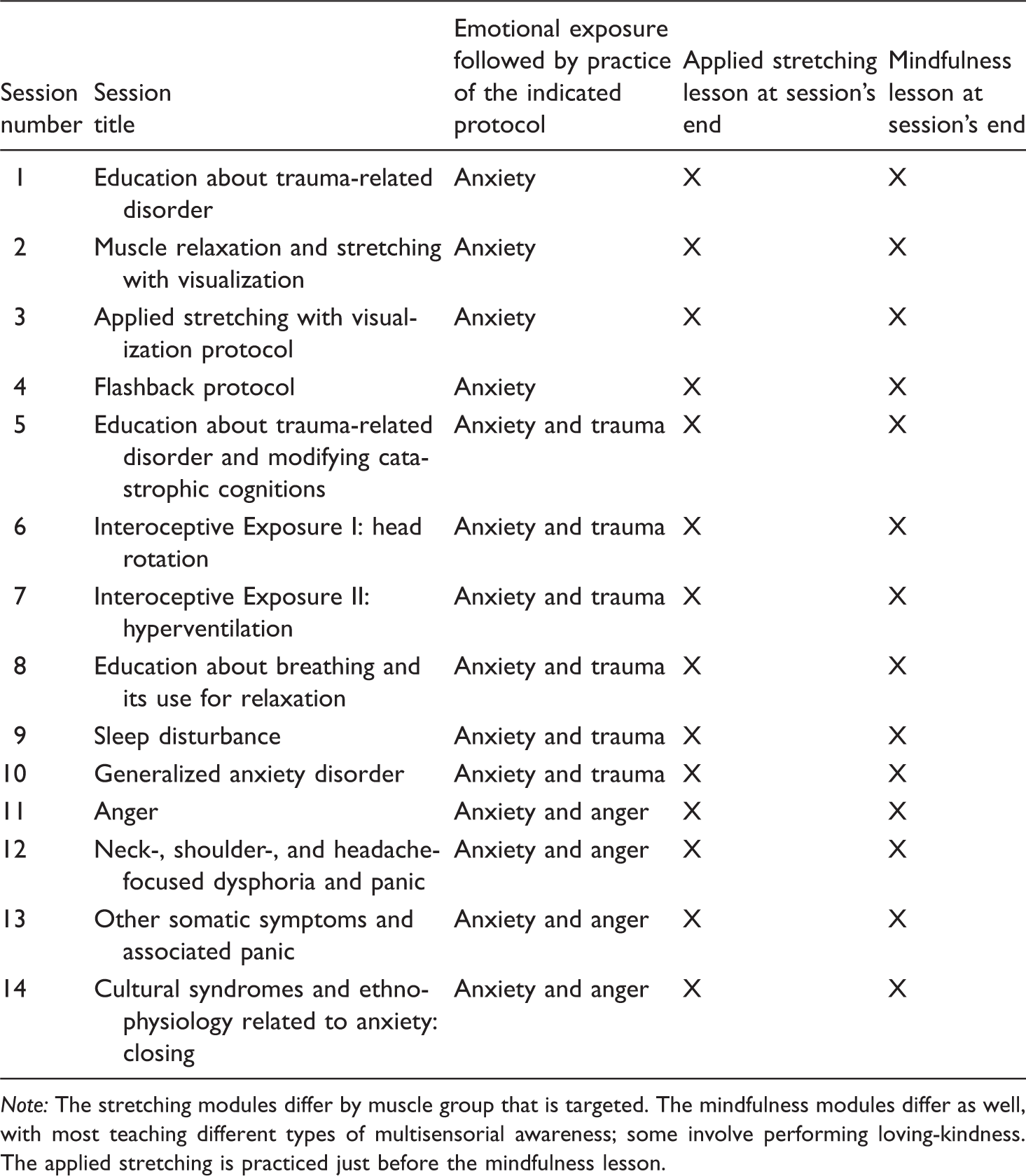
Note: The stretching modules differ by muscle group that is targeted. The mindfulness modules differ as well, with most teaching different types of multisensorial awareness; some involve performing loving-kindness. The applied stretching is practiced just before the mindfulness lesson.
CA-CBT differs from other standard treatment packages (Foa & Rothbaum, 1998; Resick & Schnicke, 1996) in several ways. It addresses the treatment challenges mentioned above: it is presented in a way easily understood by populations with minimal English ability and education, uses a unique approach to exposure, emphasizes the treatment of somatic sensations, targets comorbid anxiety conditions and anxiety-type psychopathological processes such as worry and panic attacks, and aims to reduce anger. To accomplish these treatment goals, unlike other available trauma treatments, CA-CBT emphasizes emotion exposure and emotion regulation techniques such as meditation and yoga-like stretching, 3 and aims to promote emotional and psychological flexibility (on an emotion-centered approach, see also Barlow’s unified protocol; Ellard, Fairholme, Boisseau, Farchione, & Barlow, 2010). 4 CA-CBT aims to provide the patient with a range of new adaptive processing modes—such as mindfulness that involves attending to the present-moment sensorial experiencing of environmental events—that differ from the usual mode of attending to threat.
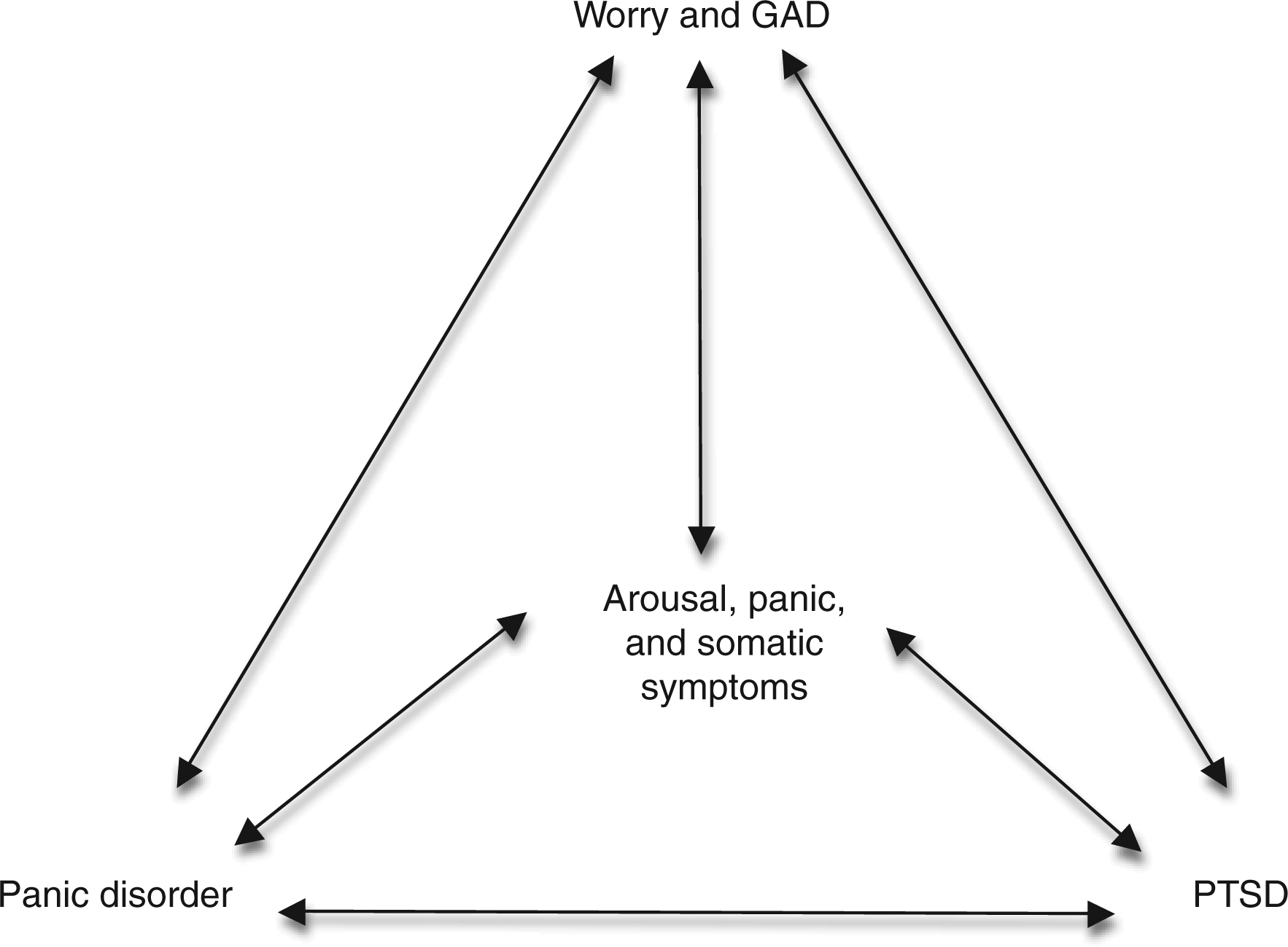
Below we present 12 key aspects of the culturally sensitive treatment of traumatized populations using examples from CA-CBT. To explain how CA-CBT brings about improvement, we present three models that guide our treatment: the panic attack–PTSD model (Figure 1) to depict the many processes that produce PTSD in these populations, highlighting the role of arousal and somatic symptoms; the arousal triad (Figure 2) to demonstrate how somatic symptoms are produced and the importance of targeting comorbid anxiety conditions; and the multisystem network (MSN) model of emotional state (Figure 3) to illustrate how several of our therapeutic techniques, such as body-focused techniques (e.g., the pairing of stretching to positive self-statements), bring about psychological flexibility and improvement.
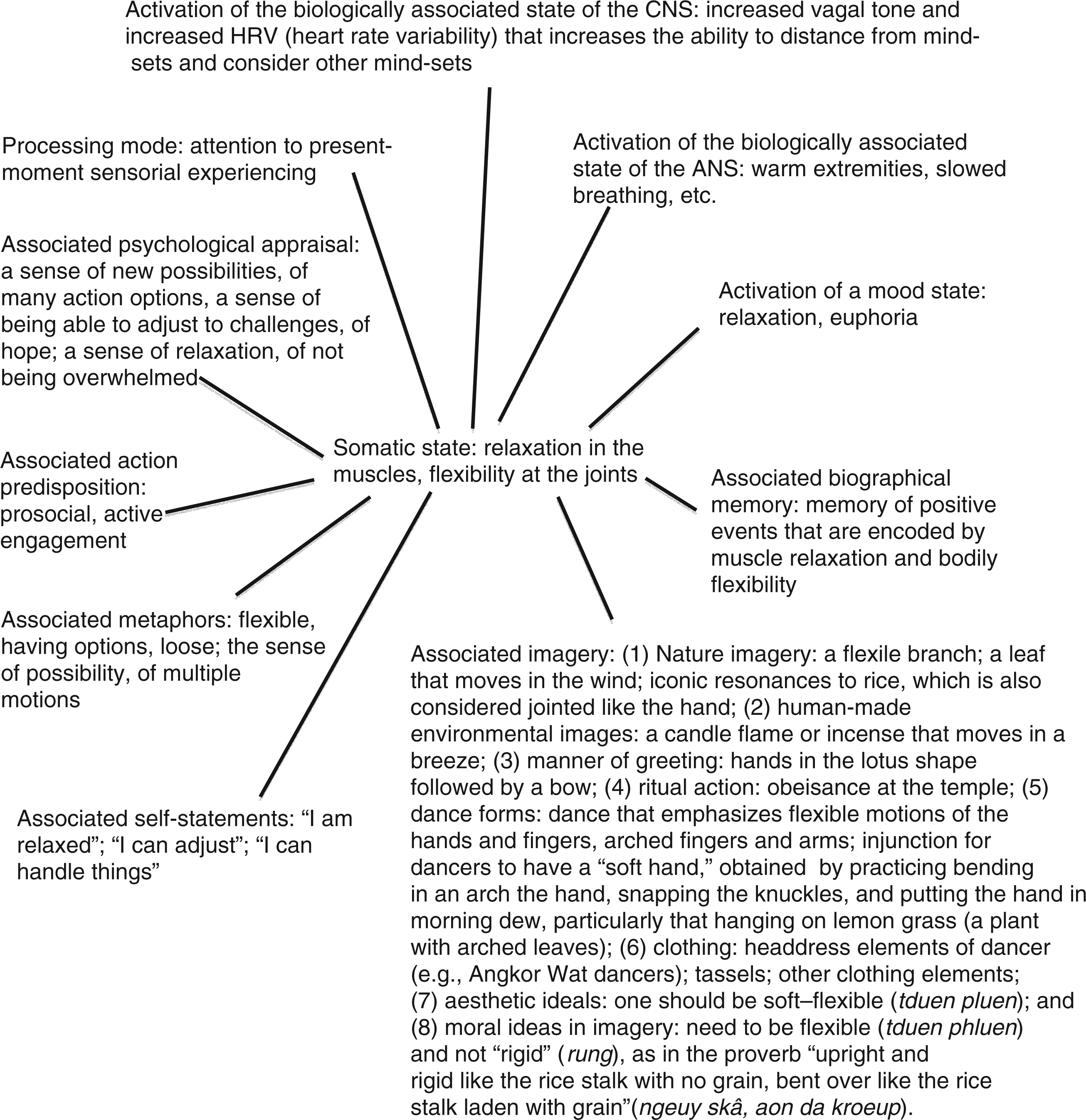
The panic attack–PTSD model. This model illustrates how various triggers (from emotional states to stress to hypervigilant surveying of the body for syndrome-related symptoms) induce somatic symptoms, arousal, and panic, and how various vicious circles are then initiated that perpetuate and worsen PTSD. The triggers (e.g., a nightmare) may induce somatic symptoms that then give rise to trauma recall and catastrophic cognitions, or the trigger (e.g., a nightmare) may directly activate trauma recall (e.g., trauma associations to dream images) and catastrophic cognitions (e.g., fears that the dream may indicate a dangerous spiritual depletion) that then cause arousal and somatic symptoms. We give emotion regulation a prominent place in the model because it will impact on almost all the processes: if the patient has good emotion regulation ability, the patient will be able to self-calm and quickly reduce arousal. The arousal triad. The figure shows three key disorders in traumatized populations, all of which produce arousal and panic. The arousal triad also plays a key role in generating somatic symptoms, in particular through the production of arousal and panic. In part because of catastrophic cognitions about the negative bodily and mental effects of worry and the dangers posed by somatic and mental symptoms of anxiety, the arousal triad seems to be particularly prominent in ethnic minority and refugee populations. Often these symptoms result from cultural syndromes (e.g., khyâl attacks in Cambodian populations; neurasthenia in Chinese populations; nervios and ataque de nervios in Latino populations.) This may explain in part the prominence of somatic symptoms in refugees and ethnic minorities. A positive mood focused on a somatic sensation: The example of muscle relaxation and joint flexibility among Cambodian refugees. This multisystem network model (MNM) shows how a somatic sensation induces a positive mood. This is a node-network model of emotions, demonstrating how a nodal network that maintains a mood may be centered on a somatic sensation. As one node shifts to being characteristic of another mood state, all the other nodes tend to shift. The network can be activated by any of the nodes. We detail the cultural imagery associated with flexibility in the Cambodian culture; those images—and associated acts—also activate the network. (The main overall type of shift is from negative to positive affect, or vice versa.)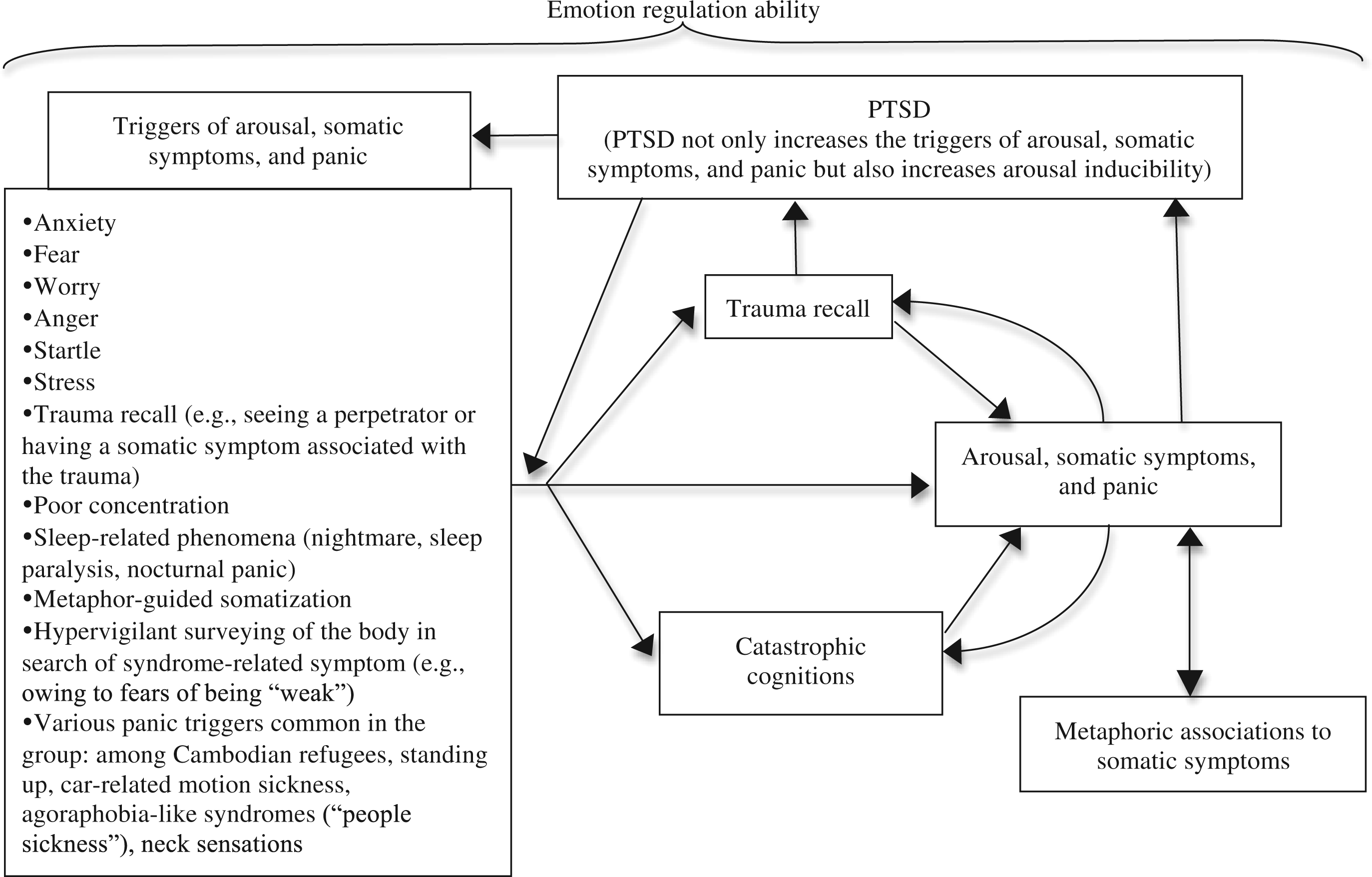
In the first sections we discuss why typical trauma exposure is not ideal for these populations and how our treatment deals with exposure. Among patients with PTSD, fear networks related to the trauma are constantly activated. Activation may result from a range of reminders of the trauma—from persons or places resembling the trauma context to somatic symptoms present in the trauma—and that activation leads to recall of a trauma event that brings about arousal, panic, and state of hypervigilance (see Figures 1 and 2). This is a core aspect of rigid and dysfunctional responding among trauma victims that creates a default processing mode of constant hypervigilance to threat (on this, see Hinton, Pich, et al., in press). 5 After the sections discussing trauma exposure and emotion exposure more generally, we describe CA-CBT’s approach to improving emotion regulation ability and psychological and emotional flexibility. Next we detail how trauma networks are activated by such processes as worry, panic attacks, catastrophic cognitions, and sleep-associated disorders (see Figures 1 and 2) and how those processes are treated, ending with a description of how a treatment’s final session can incorporate a particular culture’s transitional rituals.
Twelve key components of the culturally sensitive treatment of traumatized refugees and ethnic minorities
I. Conducting “exposure” in a culturally acceptable way
Probably the best-known CBT treatment of PTSD, prolonged exposure (Foa & Rothbaum, 1998), takes exposure to trauma memories to be the central part of treatment for PTSD. Therapy mainly consists of repetitive exposure to a trauma memory that is evoked in all its sensorial aspects until the person is quite distressed. Vivid reliving and high distress is thought to be necessary for efficacy, with cure resulting from extinction of anxiety and fear associated with memories. In another prominent protocol, Cognitive Processing Therapy (Resick & Schnicke, 1996), exposure is also a central component: the person writes down the trauma event in detail and repeatedly reads it. The only published manual for treatment of refugees that has been empirically tested is Narrative Exposure Therapy (Schauer, Neuner, & Elbert, 2005). 6 It is based on the prolonged exposure approach but is much briefer (usually 3–6 sessions; prolonged exposure therapy is 12 sessions; cognitive processing therapy, 12 sessions). It focuses almost exclusively on exposure, with multisensorial reliving in the context of constructing the person’s trauma narrative, and aims to achieve extinction. For several reasons, none of these three treatments conducts exposure in a manner that is optimal for traumatized refugees and ethnic minorities.
For one, even English-speaking Western populations who are highly educated often find traditional exposure hard to tolerate and experience worsening at certain points of the treatment (for a review, see Cahill, Foa, Hembree, Marshall, & Nacash, 2006; Markowitz, 2010). Given that ethnic minorities and refugees are often highly distressed, these techniques would seem more likely to have negative results, such as worsening of symptoms and drop out. In one study, traditional exposure was poorly tolerated by ethnic minorities and refugees, with African Americans dropping out twice as often as Caucasian patients (55% vs. 27%; Lester et al., 2010).
Second, the theory of how exposure works has changed. Before it was believed that exposure was effective because exposure to the memory reduced its automaticity, activatibility, and “hotness,” and that a key part of “extinction” was having the person experience the memory with high levels of multisensorial vividness and distress (Foa & Rothbaum, 1998). Now it has been found instead that the trauma memory is never erased through treatment (Craske et al., 2008; Hofmann, 2008). Exposure works by creating new nonthreatening associations to the trauma memory network and by creating new verbal links to and representations of the trauma memory that decrease the memory’s uncontrollability and “hotness” (Brewin, Dalgleish, & Joseph, 1996; Craske et al., 2008). The person does not need to experience high levels of distress to get this result; rather, the goal is creating the expectancy that the trauma memory can be tolerated (Craske et al., 2008; Hofmann, 2008). This suggests that new and less distressful treatments are possible.
Third, researchers have increasingly realized that emotion regulation techniques should be taught prior to conducting exposure so that the patient’s level of arousal is reduced. Otherwise the person will be unable to tolerate exposure. This is often called a phase approach and is used in one new 16-session treatment (Cloitre, Cohen, & Koenen, 2006; Cloitre, Koenen, Cohen, & Han, 2002). 7 Phase treatment is especially important in highly traumatized populations and with patients under great stress (Markowitz, 2010), which is commonly the case among refugees and ethnic minorities.
Finally, it has been increasingly realized that exposure should be conducted not only for certain event memories but also for somatic sensations (Hinton, Hofmann, Pitman, Pollack, & Barlow, 2008; Otto & Hinton, 2006; Wald & Taylor, 2007, 2008). Interoceptive exposure is especially indicated for those patients with prominent somatic complaints, extensive catastrophic cognitions about somatic symptoms, extensive trauma associations to somatic sensations (e.g., each trauma results in the encoding of the trauma by somatic sensations), and many comorbid anxiety disorders, all of which are commonly found in ethnic minority and refugee populations. Interoceptive exposure to sensations decreases catastrophic cognitions about them, diminishes the tendency of sensations to recall trauma events, and reduces panic attacks and panic disorder, as well as somatization more generally (Barlow, 2002; Craske et al., 2009; Wald & Taylor, 2007, 2008).
Taking into account these recent theories about exposure, we make our exposure in CA-CBT acceptable and efficacious in the followings ways:
Phase approach. We use a phase approach, teaching emotion regulation skills, such as applied muscle relaxation, applied stretching, and meditation, before starting exposure. See Table 1 for a description of the first three sessions that precede exposure and the emotion regulation techniques that are introduced. Trauma protocol. To promote acceptability of exposure during verbal recounting and to make it more effective, in CA-CBT we have the patient discuss trauma memories at the beginning of several sessions (Sessions 5–10), and then when the patient becomes upset, we have the patient perform a trauma protocol. This protocol consists of a series of emotion regulation techniques, including mindfulness and applied stretching with a visualization (see Section II for further discussion of why the trauma protocol is efficacious and Section III for further discussion of culturally adapted techniques used in the trauma protocol). Interoceptive exposure with reassociation. We conduct interoceptive exposure to sensations such as dizziness while creating positive reassociations to them to compete with sensation-type trauma associations and catastrophic cognitions. Creating positive reassociations to sensations increases acceptability and efficacy.
II. Emotion exposure paired with practice of emotion regulation
Emotion regulation deficits are a key deficit among persons with emotional disorders (Fairholme, Boisseau, Ellard, Ehrenreich, & Barlow, 2010; King & Sloan, 2010) and form a key part of our model of how PTSD is perpetuated. Other than fear and other emotions caused by trauma recall, such as shame, trauma survivors who are refugees or ethnic minorities often have problems with anger, general anxiety, and worry (Hinton, Nickerson, & Bryant, 2011; Hinton, Rasmussen, et al., 2009). As shown in the panic attack–PTSD model in Figure 1, these emotions often give rise to arousal, trauma recall, and catastrophic cognitions, which start vicious cycles of worsening.
Recent research suggests that an important treatment approach for emotional disorders consists of exposure to intense emotions in such a way that the patient learns to tolerate the affect and to utilize more adaptive ways of reacting to it, an approach that is a central part of Barlow’s Unified Protocol in which he expands his work on interoceptive exposure to include emotional exposure (Ellard et al., 2010; Fairholme et al., 2010; Otto, Powers, & Fischmann, 2005; Wilamowska et al., 2010). Emotion exposure is easily accomplished with other cultural groups if it is framed as being a way to practice the emotion regulation techniques, and this then also gives an opportunity to practice emotion regulation. (We consider emotion exposure to involve both the exposure to negative affects and the induction of and exposure to positive affects, such as compassion and loving-kindness. Exposure creates a broader behavioral-emotional repertoire because those states become action options under greater volitional control.)
In a CA-CBT, we elicit certain emotions in a vivid way. Some emotions are induced during trauma recall at the beginning of sessions. Other emotions—namely, anxiety, anger, and worry—are induced by asking about recent experiencing of the emotion, the events that caused the emotion, and the somatic sensations associated with the emotion. After the emotion is induced during the CA-CBT session, we have the patient practice shifting state by using an emotion regulation technique (see Table 1). Almost every session of CA-CBT begins with an enquiry about anxiety states in the previous week, followed by practice of the anxiety protocol (see Table 1). As discussed above, several sessions of CA-CBT (Sessions 5–10; see Table 1) begin with trauma exposure during which the patient experiences fear and other trauma-recall-related emotions, followed by practice of the trauma protocol. Several sessions involve the review of causes of anger, which will invoke that emotion, followed by practice of the anger protocol (Sessions 11–14; see Table 1).
In particular we think that trauma exposure, which elicits a number of negative emotions, followed by practicing emotion regulation through the trauma protocol, has several positive effects. The patient is able to verbalize the trauma and thereby creates frontal representations that should decrease automaticity of recall (Brewin et al., 1996; Clark & Ehlers, 2004). The patient is able to practice the emotion regulation and acceptance techniques, techniques that can be used whenever trauma recall occurs and whenever any dysphoric state is experienced. Through the exposure protocol, the patient pairs a positive memory state to the trauma memory, with the positive memory being characterized by a sense of agency and self-esteem and by adaptive emotional states such as curious, detached observance, loving-kindness, compassion, and aesthetic engagement with the sensorial surround. 8 Furthermore, the patient changes his or her self-image to one of mastery and ability to cope with the trauma memory.
III. Culturally adapted emotion regulation techniques
Poor emotion regulation is a key aspect of PTSD and anxiety disorders more generally (Fairholme et al., 2010). In this section we describe several emotion regulation techniques we teach in CA-CBT and how they are culturally adapted.
The anxiety protocol is practiced at the beginning of most sessions after asking about recent events that produced anxiety (see Table 1), and it can be used whenever the patient becomes anxious or distressed in any way. This anxiety protocol not only serves as a means to regulate emotion; it also serves as exposure to dizziness sensations, creates positive reassociations to dizziness (e.g., dizziness becomes associated to the image of the lotus that competes with catastrophic images), and acts as a visual analog of flexibility, a self-image of flexible adjustment. In the first part of the anxiety protocol, the patient uses applied stretching to relax any tense areas, and then uses applied stretching and muscle relaxation to relax the shoulders. The imagery in the next section depends on the cultural group. We have the patient straighten the spine through tightening the stomach muscles and then do head-rolling. While doing the head-rolling with the straight spine, we have Southeast Asian patients imagine a lotus flower circling in the wind on its stem and compare the spine to the stem and the flower to the head. At the same time we have the patient make self-statements of flexibility: “May I flexibly adjust to each situation just as the lotus flower is able to adjust to each new breeze.” For Latino patients, we use the image of a palm tree at the beach, with its long trunk and its fronds moving and circling in the wind. The self-statement is the following: “May I flexibly adjust to each situation just as the fronds of the palm tree adjust to each new breeze.”
We teach a loving-kindness meditation to help decrease anger (for a review of the efficacy of loving-kindness meditation, see Hofmann, Grossman, & Hinton, 2011). We change the imagery depending on the cultural group. We have Southeast Asian patients imagine love spreading outward in all directions like water. This is because in Buddhism water and coolness are associated with values of love, kindness, nurturing, and “merit-making,” that is, doing good deeds like making donations to the poor or to the temple. 9 In many Buddhist rituals, water is poured into a bowl to symbolize the merit being made by participating in the rite and the “cooling” influence of the merit-making for the dead and the living. We have Latino patients imagine love as a warmth and light that spreads from the heart and body in all directions. We refer to the image of the “Sacred Heart of Jesus,” or Sagrado Corazón de Jesús, one of the best-known images in Christian iconography. In the image, Christ points a finger to his flame-surrounded heart that emanates light; often the heart is surrounded by a wreath of thorns that further symbolizes the overcoming of difficulties. In the Western European ethnopsychology and iconography, warmth connotes love and affection and has extensive positive symbolic meanings (for one review, see Hinton, 2000).
The trauma protocol also varies by cultural group. The trauma protocol begins with acceptance of having endured the trauma, followed by self- and other-directed compassion, then loving-kindness, and next multisensorial mindfulness meditation. After that, we use a technique that aims to bring about the multichannel embodying of flexibility. The technique pairs together bodily representations of flexibility (actual stretching and rotational movements), self-statements of flexibility, and musical analogs of flexibility, that is, acoustic images of flexibility. The five-step multichannel flexibility protocol is as follows:
Applied stretching. The patient stretches any area of sensed tension. Arm stretching that emphasized flexibility icons. The patient stretches the arms and its joints by extending the arms out and rotating them with the wrists bent back, by rotating the wrists, and by extending and fluttering the fingers (for further discussion of the efficacy of such body-based flexibility techniques, see Hinton, 2008). Evocation of an acoustic icon of flexibility. These arm-stretching motions have a dance-like quality, particularly the wrist rotations and finger fluttering, and next we have the patient think of music appropriate for the patient’s cultural group. For Cambodian patients, we suggest imagining the arms dancing to the songs of a famous singer, Seng Sii Samut; that dancing can occur at the level of the whole arm, forearm, wrist, or fingers (this highlights the highly flexible aspect of the human body). For Caribbean Latino patients, we use the example of salsa and bachata, for Mexican Americans, ranchero music. In the salsa example, we instruct the patient to imagine the rhythm of the singer’s voice and that of the conga drum, bongos, timbales, horns, cowbells, piano, and maracas; and in the ranchero example, the rhythm of the singer’s voice and that of polka-like oompah sound of the accordion, the sound of the guitar, and so on. We mention several musical genres of the group in question in order to bring about further cognitive shifts, from salsa to bachata to bolero. Embodying the acoustic icon of flexibility. We describe each of the music’s sound layers, stating that the patient can choose to dance to any of these music layers and that making these movements is practice in flexible adjustment (it is a form of set-switching). Self-image of flexibility paired to music listening. We conclude by commenting that the music is a reminder to stay flexible, to know how to adjust.
This five-step multichannel flexibility protocol has several effects other than shifting from the dysphoric states induced by trauma recall. It pairs bodily flexibility to a musical metaphor that emphasizes psychological flexibility; it teaches the powerful effect of attention on experiencing because the patient attends to one layer and then another layer of music, for example, from one instrument to another; it teaches set-switching, as the patient switches between musical layers; it creates cultural pride because a certain cultural music is presented; and it creates a prompt—viz., hearing music—to remind the person to be flexible, a prompt that will often be experienced in the everyday world. 10
IV. Utilizing emotion regulation techniques from the patient’s religious or cultural healing traditions
To make the treatment culturally acceptable and to improve efficacy, we try to utilize emotion regulation techniques from the culture in question and to frame our techniques in terms of those locally prominent emotion regulation techniques. In CA-CBT, we determine the emotion regulation techniques in that cultural group that can be used in treatment: some Islamic groups repetitively recite Allah’s name, a ritual called dhikr, to bring about a peaceful state of mind.
Our treatment involves the use of many Buddhist-type techniques, so in the case of a Buddhist patient, the treatment already includes a key aspect of his or her religious tradition. The treatment includes “loving-kindness” (metta) and many meditation techniques, with a new mindfulness exercise being provided at the end of every session (Table 1). A key Buddhist principle, “equanimity” (upekkha)—that is, practice in distancing from emotions and mental content, treating them as if clouds in the sky—is also a part of the treatment. For a Buddhist patient, these acts can be referred to by the term used in that tradition, and it be can stated that performing these actions is “merit making” and that this “merit” can be shared with oneself and others. This “merit making” promotes a sense of agency and greatly decreases suicidality and depression. If a patient has survivor guilt, he or she can be reminded of the culturally indicated duty to make merit at least yearly for the person about whom the patient feels guilty in order to ensure the deceased will have a good rebirth and spiritual health.
To promote flexibility among Christian Latino patients, we instruct them to note how the flexile flame of votive candles moves in each breeze and assert that this motion is a reminder to stay flexible—the image in question serves as a flexibility primer (Hinton, 2008). As indicated above, we use Christian imagery in the loving-kindness meditation. In addition, we suggest that the Christian Latino patient use other religious-type techniques of emotion regulation, such as random opening of the Bible to select a passage to be read or reciting the rosary (e.g., if the patient is Catholic). If the patient is a Pentacostalist, we suggest that speaking in tongues, with its layers of voices, is a reminder that there are many paths to God, many ways of acting and feeling.
We consider emotion regulation techniques in the broad sense, ranging from proverbs in a culture that are used to deal with negative affects to healing rituals. In the anger module of our treatment, we use a Cambodian proverb to help teach anger restraint: “If you control your anger once, you gain a hundred days of happiness.” We specifically ask about how patients cope with anxiety, anger, and trauma recall in order to elicit the patient’s typical ways of dealing with distress, including culturally specific healing traditions and emotion regulation techniques. In CA-CBT we also suggest that the patient be encouraged to participate in healing rites from his or her culture that may improve emotion regulation: among Buddhists, relevant healing ceremonies, such as anointing with lustral waters or listening to Buddhist tapes; among Latinos, going to church services, lighting a votive candle, or reciting the rosary; among Native American groups, participation in traditional ceremonies such as the sweat lodge. Ideally, therapeutic metaphors, ideas of causation (e.g., “historical trauma”), ideas of cure, and ideas about ontology (i.e., the nature of personhood) from that tradition should be integrated into treatment. (For further discussion of the incorporation of traditional healing into treatments, see Gone [2009, 2010].)
V. Cultural adaptation of key CBT techniques
CBT techniques should be adapted for the group in question. We have described how relaxation imagery and exposure are adapted for a particular group. Here we will examine in more detail the cultural adaptation of a particular aspect of exposure, namely, interoceptive exposure. In interoceptive exposure in CA-CBT, we do positive reassociations of somatic sensations to culturally appropriate images. Among Cambodian refugees, when doing head-rolling, we have the patient imagine various traditional games: a game in which a person is made to run around in circles while holding a scarf (lea geunsaeng), or another game in which the person runs to get a stick that has been hit into the distance, all the while humming, making it impossible to inhale. Among Latinos, we have the patient imagine playing traditional games that induce considerable dizziness: playing the piñata game, which involves being blindfolded and spun around, or playing gallinita ciega. In these games, the person is spun until very dizzy.
VI. Increase emotional and cognitive flexibility
Psychological flexibility—defined as the ability to distance from current mindsets and consider other possible mindsets (Kashdan, 2010)—is a meta-level processing mode that CA-CBT tries to create as a default mode of processing. Psychological inflexibility is a key cause of psychopathology (Ehrenreich, Fairholme, Buzzella, Ellard, & Barlow, 2007; Hinton, Hofmann, Pollack, & Otto, 2009). Psychological flexibility creates a new adaptive processing mode that competes with the threat mode (Hinton, Pich, et al., in press; Kashdan, 2010; Kok & Fredrickson, 2010). It is a key aspect of emotion regulation.
Psychological flexibility is a crucial skill for refugees and ethnic minorities who are dealing with multiple adaptations that require great flexibility: they must reconcile their own culture and their new one, learn a new social and geographic location, learn to switch language registers, and deal with different ideas about proper behavior and social interaction, such as how children should behave. One theory of adapting cultural treatments among Native American groups emphasizes as a key goal the achieving of “postcolonial hybridity,” given the complex bricolage necessary to construct identity in such localities (for a discussion of Duran’s use of this term, see Gone, 2010).
CA-CBT aims to increase psychological flexibility in many ways. It does so through teaching emotional distancing, a key aspect of emotional flexibility, by practicing the labeling and distancing from affect (Ayduk & Kross, 2010; Hinton, 2008). It does so through the emotion and trauma protocols by practicing distancing from one affect and taking on another one: emotion switching. It does so through the visualization part of the anxiety protocol. It does so through the applied muscle relaxation with self-statements of flexibility. It does so in a multichannel way through the “dancing” part of the trauma protocol. It does so through decreasing anxiety (e.g., through the anxiety and trauma-recall protocols), which is an emotional state characterized by narrowed attention and a rigid responding style.
We have used the multisystem network (MSN) model of emotional state to depict the psychological-flexibility processing mode induced by applied stretching and by the visualization part of the anxiety protocol. 11 The model is based on recent research on emotion (Fairholme et al., 2010; Teasdale, 1996). 12 Figure 3 shows the processing mode induced by the anxiety protocol or applied stretching more generally. This nodal network is constantly activated during CA-CBT. Applied muscle stretching is practiced at the end of each session, each night before sleep, and whenever the person is anxious. The anxiety protocol is practiced in every session (see Table 1) and outside of the sessions whenever the patient feels dysphoric. More generally, whenever a state of psychological flexibility is experienced (e.g., when the patient distances from an affect mindset during the practice of equanimity), this type of network will tend to be activated but focused on that psychological flexibility in question.
VII. Worry and GAD as important treatment targets
Uncontrollable worry itself is a key treatment target among refugee and minority populations (see Figures 1 and 2). Refugees and ethnic minorities often engage in worry because of life circumstances; they live in dangerous localities and frequently confront financial problems and other stresses. Furthermore, trauma victims tend to have difficulty disengaging from worry and tend to experience arousal—and not uncommonly panic attacks—upon engaging in worry, what might be called “arousal inducibility” (Hinton, Nickerson, et al., 2011). The arousal induced by worry may give rise to catastrophic cognitions and trauma recall. Worry also brings about a state of ruminative hypervigilance to threat. In CA-CBT we elicit worry themes, address catastrophic cognitions about the negative effects of worry, and determine whether the worry episodes induce trauma recall or panic attack. Learning the patient’s worry themes builds the patient–clinician empathic bond (the patient feels his or her problems are understood by the clinician) and improves the therapeutic alliance. In CA-CBT, we specifically teach emotion regulation techniques to decrease worry that have been proven to be effective for generalized anxiety disorder (GAD) such as meditation (Roemer, Orsillo, & Salters-Pedneault, 2008) and PTSD (Follette, Palm, & Pearson, 2006).
VIII. Addressing catastrophic cognitions about anxiety and PTSD symptoms
See Figure 1 for an illustration of the role of these catastrophic cognitions in producing arousal, somatic symptoms, and PTSD. In CA-CBT we ask patients about their understanding of what produces their anxiety symptoms, including their conceptualization of the physiology that produces those symptoms, and we ask about their fears about the danger posed by those symptoms. Cambodian patients often fear that dizziness indicates the start of a khyâl attack (Hinton, Pich, et al., 2010); in Latino patients, that shakiness of the limbs or racing thoughts indicate a problem with nervios or an imminent ataque de nervios (Hinton & Lewis-Fernández, 2010b; Hinton, Lewis-Fernández, & Pollack, 2009).
Every PTSD symptom—from nightmares to startle—may give rise to such catastrophic cognitions. Many cultural groups fear that trauma recall indicates imminent insanity (e.g., Cambodian refugees; Hinton, Rasmussen, et al., 2009), and many groups fear that trauma recall results from persecution by dangerous spirits of the dead (e.g., Cambodian refugees and Rwandan trauma survivors; Hagengimana & Hinton, 2009; Hinton, Hinton, et al., 2009). Some groups consider startle to have the power to dislodge the soul and to cause death or serious illness (e.g., Latino and Southeast Asian populations; for a review, see Hinton & Lewis-Fernández, 2010a, 2010b), and some groups consider startle to indicate a dangerous “weakness” of the heart that brings about a general cardiac hyperreactivity that may lead to death (e.g., Cambodian and Vietnamese refugees; for a review, see Hinton & Lewis-Fernández, 2010a, 2010b). (In the CA-CBT manual, catastrophic cognitions about anxiety and PTSD symptoms for certain groups are specified, viz., for several Asian groups [Cambodian, Chinese, and Vietnamese] and for Latino populations.)
IX. Addressing cultural syndromes
We devote one session in our treatment to evaluating and treating anxiety- and PTSD-related cultural syndromes. Patients often attribute PTSD and anxiety symptoms to a cultural syndrome, and this attribution produces catastrophic cognitions that the symptoms indicate a serious bodily dysfunction or imminent insanity. These catastrophic cognitions start an escalating spiral of arousal, panic, somatic symptoms, and PTSD (see Figure 1).
Assessing cultural syndromes gives the clinician a better sense of the patient’s experiencing of anxiety and PTSD and the effects of anxiety and PTSD on his or her lifeworld and relationships. This also allows the clinician to assess and modify key catastrophic cognitions. It also increases treatment adherence because some of the patient’s key concerns are being addressed. (On the clinical utility of assessing and treating cultural syndromes, see Hinton & Lewis-Fernández [2010a, 2010b].)
As some examples, in our treatment of Cambodian speakers we specifically ask whether the patient fears having “weak heart” or “khyâl attacks,” how they treat episodes of those cultural syndromes, and what fears they have about them (for a review of these syndromes, see Hinton & Lewis-Fernández, 2010a, 2010b). In our treatment of Latino speakers, we specially address concerns about nervios and ataque de nervios through these same questions.
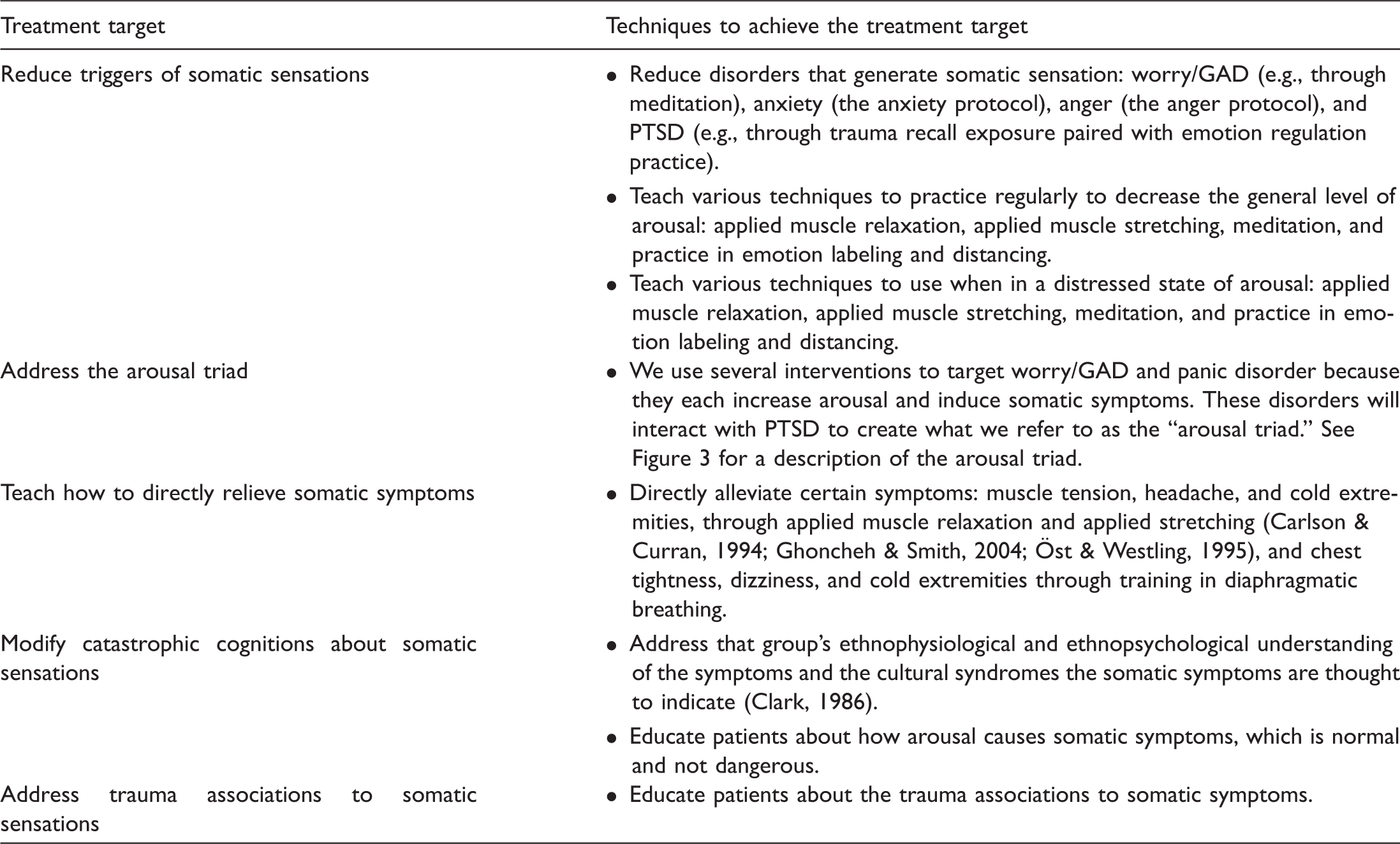
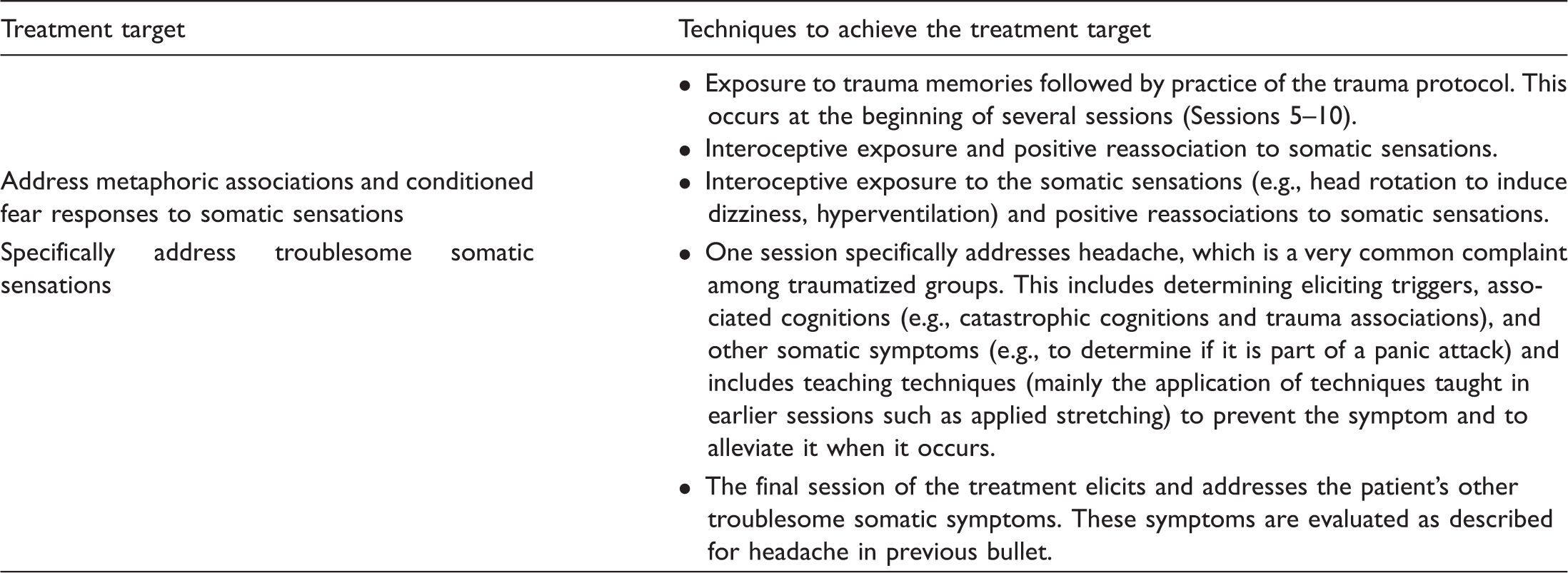
X. Target somatic symptoms
How CA-CBT reduces somatic symptoms
XI. Addressing sleep-related phenomena
In CA-CBT one session specifically addresses several sleep-related phenomena, namely, nightmares, sleep paralysis, and nocturnal panic (see Figure 1 for an illustration of the importance of these phenomena in generating PTSD). Sleep paralysis occurs upon falling asleep or awakening. The person suddenly can neither move nor speak even though awake, and often sees a black shadow approaching the body. In nocturnal panic, the person awakens in a panic but is able to move (ruling out sleep paralysis) and the person cannot recall a nightmare.
We evaluate the meaning of nightmares according to the patient. In many cultural contexts, the nightmares are considered the visitation of a deceased person or an indication that the dreamer is in a physically and spiritually vulnerable state (Hinton, Hinton, et al., 2009). We specifically ask about sleep paralysis and its meaning. Sleep paralysis worsens anxiety and PTSD and is caused by them, and in certain cultural groups, sleep paralysis is given extensive cultural elaboration and is quite common (Hinton, Pich, Chhean, & Pollack, 2005). Distressed Cambodian refugees often have sleep paralysis, and it is usually attributed to the visitation of a malevolent spirit or to dangerous physiological problems; African American groups likewise often have sleep paralysis and frequently give it a catastrophic interpretation (Hinton, Pich, et al., 2005). We assess for nocturnal panic and its interpretation. In order to improve sleep, we also have patients do yoga-like stretching before sleeping to prevent cramping and decrease arousal, (Patra & Telles, 2009). Those yoga-like stretching methods are taught at the end of every session (see Table 1).
XII. Culturally indicated transitional rituals
In CA-CBT, if the culture has “purification” or transitional rites, such as steam bath rituals among Cambodian refugees, Vietnamese refugees, and certain American Indian groups (Silver & Wilson, 1988), the patient should be encouraged to perform that rite at the end of treatment. This creates a sense of closure, and of positive transformation. These rituals also have healing properties in themselves. For example, the steaming ritual induces a somatic state that is analogous to an anxiety state: shortness of breath, a feeling of strong heat, and shortness of breath. It thus acts as exposure to those sensations and as a positive reimagining of them; the steaming ritual often involves odiferous substances and symbolic objects that become associated with—conditioned to—the somatic sensations. This type of healing semiotizes certain sensations, that is, creates new positive associations to sensations. 13
Conclusion
In this article we have tried to illustrate how CBT can be adapted to traumatized refugees and ethnic minorities, giving examples from CA-CBT. We presented 12 key principles to guide the culturally sensitive treatment of these traumatized populations and described several models that can be used to design treatment. These models are the panic attack–PTSD model, the arousal triad, and the multisystem network model of emotional state.
Our treatment emphasizes emotions and somatic symptoms and considers these to be key treatment targets. It is an emotion- and somatic-sensation-focused treatment. Somatic sensations are the focus in two respects. We target somatic sensations that cause distress by addressing arousal and other causes of the sensations, by addressing sensation-associated trauma associations and catastrophic cognitions, and by conducting interoceptive exposure. 14 We also try to bring about certain types of sensorial experiencing as part of emotion regulation techniques. We teach multisensorial mindfulness, create positive reassociations to sensations, and teach how to attain a sense of stretched relaxation that serves as an embodied metaphor priming to psychological flexibility. This emphasis on somatic experiencing is an aspect of the treatment that makes it effective for somatic sensations and makes it easily taught to persons of other cultural groups and low education. Likewise the emphasis on emotion and emotion regulation improves the ease with which such groups will find the approach appropriate.
Future research needs to explore the applicability to cultural groups other than Latino and Southeast Asian populations. It also should be noted that the three models we presented as guiding our treatment (panic attack–PTSD model, the arousal triad, and multisystem network) are heuristic tools. Future studies need to further explore their validity. Also, future dismantling studies need to be done to determine which elements of the treatment have efficacy. There is also a need to explore the efficacy of our culturally adapted approach to standard CBT treatments, such as those based on exposure (Foa & Rothbaum, 1998; Resick & Schnicke, 1996). Future studies need to determine whether such variables as gender, PTSD severity, and acculturation moderate the response to our treatment. Finally, future studies will need to determine whether CA-CBT can be successfully done when the therapist is not a member of the treated person’s cultural group. We anticipate that the treatment would be successful in that case as well but that the sessions would take longer to complete.
The treatment we propose contains modules for particular problems, such as one for somatic symptoms and one for anger. Therapists could use specific modules for patients with the problem in question. For training purposes, it would be useful for therapists to screen patients for particular problems and then use the relevant module in order to learn the treatment approach and to improve patient care. In addition, through such an approach, the particular modules can be refined for use with particular cultural groups. In a busy practice this modular approach might both improve care and increase training. Future studies could be done to examine efficacy of particular modules in such an approach.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.