
Abstract
We conducted a review of research literature related to anxiety, depression, and mood problems in Indigenous women in Canada, the United States (including Hawaii), Australia, and New Zealand. Quantitative and qualitative research studies published between 1980 and March 2010 were reviewed. The initial search revealed 396 potential documents, and after being checked for relevance by two researchers, data were extracted from 16 quantitative studies, one qualitative research article, and one dissertation. Depression is a common problem in Indigenous pregnant and postpartum women; however, the prevalence and correlates of anxiety and mood disorders are understudied. The review identified four key areas where further research is needed: (a) longitudinal, population-based studies; (b) further validation and modification of appropriate screening tools; (c) exploration of cultural diversity and meaning of the lived experiences of antenatal and postpartum depression, anxiety, and mood disorders; and (d) development of evidence-informed practices for researchers and practitioners through collaborations with Aboriginal communities to better understand and improve mental health of women of childbearing age.
This paper critically reviews the literature on anxiety, depression, and mood disorders in pregnant and postpartum Indigenous women in North America, New Zealand, and Australia. Although the World Health Organization (WHO) does not define the term “Indigenous people” because of the vast differences between Indigenous peoples throughout the world, the term includes those who “identify themselves and are recognized and accepted by their community as Indigenous… demonstrate historical continuity with pre-colonial and/or pre-settler societies,” and “maintain distinct languages, cultures, and beliefs” (World Health Organization, 2007).
Globally, Indigenous women tend to give birth to more children per capita than their non-Indigenous counterparts. In Canada, Aboriginal women have 1.5 times more pregnancies than women in the general population (Statistics Canada, 2005). In the United States, Native American women also have 1.5 times the number of pregnancies of Caucasian women (Dye, 2008). In Australia, Aborigine women have 2.57 children per woman compared to 1.9 in the general population (Australian Bureau of Statistics, 2009). Finally, in New Zealand, the average number of children born to Maori women is 2.79 compared to 2.1 in women overall (Statistics New Zealand, 2004). Additionally, Indigenous women are more likely to experience adverse social factors (e.g., poverty, lack of support, substance use) that may put them at risk for depression (Bowen, Stewart, Baetz, & Muhajarine, 2009).
The WHO predicts that by the year 2020, unipolar major depression will be the second greatest cause of disability; however, it is already the number one cause of disability in women of childbearing age worldwide (World Health Organization, 2006). Depression may refer to a complaint or symptom such as “feeling depressed” or more commonly to a loosely defined syndrome that includes a negative emotional state during which a person feels sad, lonely, or miserable, with a lack of interest in usual pleasurable activities (Blazer, 1999). Depression may also refer to a diagnostic category with specified criteria of severity, duration, and exclusions such as “unipolar major depression” (American Psychiatric Association, 2000; World Health Organization, 2006). In Canada, 30.1% of First Nations people living on reserves had symptoms of depression for more than 2 weeks in a 12-month period; 18% had major depression; and 31% had experienced suicidal ideation (Assembly of First Nations, 2002–2003). It is estimated that 20% of perinatal women in primary care settings experience depression as measured by the Center for Epidemiological Studies-Depression Scale (CES-D; Marcus, Flynn, Blow, & Barry, 2003).
Anxiety often co-occurs with depression. Anxiety symptoms or disorders affect approximately 16% of women in Canada, with some studies indicating lifetime prevalence as high as 30% (Health Canada, 2002; Levine, Oandasan, Primeau, & Berenson, 2003). Anxiety often peaks in a person’s mid-twenties, a time coincident with childbearing (Pigott, 2003). Women who experience prenatal anxiety are 3 times more likely to report severe postpartum depression symptoms compared to those without anxiety (Austin, Tully, & Parker, 2006; Heron et al., 2004; Stuart, Couser, Schilder, O’Hara, & Gorman, 1998; Sutter-Dallay, Giaconne-Marcesche, Glatigny-Dallay, & Vedoux, 2004). There is evidence that, early identification and treatment of anxiety may prevent future depression (Flannery-Schroeder, 2006).
It has been suggested that postpartum psychosis may be closely related to the spectrum of bipolar disorders (Sharma & Khan, 2008). Fluctuating mood may put perinatal women at increased risk for postpartum depression, anxiety, and substance abuse (Kendell, Chalmers, & Platz, 1987). However, a pregnant woman without pervasive depression who discloses that she has mood problems may be told that her feelings are a normal part of pregnancy, even if they are troublesome to her (Bowen, Bowen, Butt, Rahman, & Muhajarine, 2012).
Untreated perinatal depression and anxiety may have potentially adverse consequences for the mother and child. Women who are depressed engage in more high-risk behaviours and are less likely to receive adequate prenatal care (Bonari et al., 2004). Their pregnancies are more likely to end prematurely, result in operative deliveries, and have more obstetrical complications (Chung et al., 2001). Women with depression are also more likely to suffer from future severe depressive episodes, including postpartum depression, psychosis, and thoughts of harming self or others (Blazer, 1999). Infants whose mothers were anxious or depressed during pregnancy are at increased risk for the consequences of preterm delivery, lower Apgar scores, lower birth weight, less frequent and shorter duration of breastfeeding, poorer weight gain, and increased admission to neonatal intensive care units (Chung et al., 2001; Hellin & Waller, 1992; Murray, Cooper, & Hipwell, 2003; Zuckerman, Bauchner, Parker, & Cabral, 1990). Children of mothers who are depressed experience ongoing physical, psychological, behavioural, and developmental problems (Maki et al., 2003; Murray et al., 2003; O’Connor, Heron, Golding, Beveridge, & Glover, 2002; Wilkerson, Volpe, Dean, & Titus, 2002).
In summary, perinatal mood problems are important public, mental, and population health concerns. Since Indigenous women overall experience a higher prevalence of depression as well as a higher birth rate, there is a need for better understanding of depression and other maternal mental health problems in this vulnerable population.
Methods
We reviewed the literature published between January 1980 and May 2010 related to women who were: (a) Aboriginal, First Nations, Indigenous, Inuit, Maori, or Métis; (b) resided in Australia, New Zealand, Canada, or the USA (including Hawaii); and (c) were pregnant or up to 1-year postpartum; and (d) experienced depression, anxiety, or mood disorders. The countries of origin were determined by Health Canada who commissioned the study, based on the premise that the Indigenous peoples in these selected countries were most comparable to Aboriginal people in Canada.
The search, designed with the collaboration of a medical librarian, included the published and unpublished literature using both subject headings and keyword searches representing the three main concepts in the search: (a) mood problems; (b) obstetrical terms; and (c) Aboriginal terms. (The keywords searched in each database are presented in an online supplement.) The two exclusion criteria were (a) papers that presented commentary or opinion not based on quantitative or qualitative research; and (b) studies that included Indigenous women as part of a larger study group where the results could not be linked to the Indigenous participants. Databases searched included the OVID versions of Medline, as well as Embase and PsycINFO, CINAHL, Cochrane, AMED, Web of Science, Scopus, Native Health Databases, Natural Standard, BMJ Clinical Evidence, and the University of Saskatchewan’s iPortal. OCLC WorldCat and Amicus were searched for book titles. Reference lists of the relevant studies were checked for further sources. Authors of relevant studies were contacted and asked whether they were aware of any other studies; some were requested to provide missing information pertinent to the review of their study.
The grey literature search included the Proquest Dissertations and Theses database; Conference Papers Index; Knowledge Utilization Database; and GreySource. We also searched websites and reports from government and other agencies including the World Health Organization; the Pan American Health Organization; the Australian Government Departments of Health and Aging, and Families, Housing, Community Services and Indigenous Affairs; the U.S. National Library of Health and the National Institutes of Health; the U.S. Department of Health and Human Services; state websites; the New Zealand Families Commission; the New Zealand Office for Women in the Department of Local Government, Planning, Sport and Recreation; Health Canada; Aboriginal Nurses Association of Canada; Indian and Northern Affairs Canada; the Canadian Institute for Health Information; Statistics Canada; and Canadian provincial and territorial government sites.
Two trained research assistants reviewed studies to ensure they met the inclusion criteria. Two team members independently reviewed each quantitative study that met the relevance criteria using a tool developed by Loney, Chambers, Bennett, Roberts, and Stratford (2000). This tool gives studies a score based on eight critical items: randomized or whole population; sampling frame; measures; unbiased assessors; adequate response rate; refusers described; statistics used; subjects described. In order to include potentially useful but lower quality studies, a score of 3 or more was required to retain a study in the review. Qualitative studies were evaluated for relevance by a trained research assistant. Team members worked independently to assess the quality of each study by applying the 10 questions of the Critical Appraisal Skills Programme Assessment Tool (CASP; Public Health Resource Unit [PHRU], 2006). A scoring process adapted by Duggleby et al. (2010) was used to evaluate the studies. A 3-point rating system determined the scores for each study against each of the CASP’s eight research questions. A weak score (1 point) was assigned to studies that offered little to no justification or explanation for a particular issue (e.g., where, when, or how the data were collected was not mentioned). A moderate score (2 points) was given to studies that addressed the issue but did not fully elaborate on it (e.g., the justification for using constant comparisons of emerging data by coding after each interview, and comparing to previous interviews was presented, but the procedure itself was not explained). A strong score (3 points) was assigned to studies that extensively justified and explained the issue at hand (e.g., the authors explained that semistructured interviews were used, transcribed verbatim, and modified partway through the study, and then offered some sample interview questions). The scores from the eight questions were totalled for a maximum score of 24 (Duggleby et al., 2010).
Some of the authors have authored papers included in the review (Bowen & Muhajarine, 2006; Bowen et al., 2009; Bowen, 2007); to reduce potential bias the research team was increased to include members who could independently assess those studies. Summary tables were created to organize the data (Pinch, 1995). Team members extracted data for each study independently in order to minimize bias. As these were not intervention studies, further statistical analyses beyond reported descriptives and prevalence were not undertaken.
Results
The search returned 396 studies. All studies retrieved were written in English. Forty-two met the initial relevance criteria (see Figure 1).
Flow diagram of literature search results.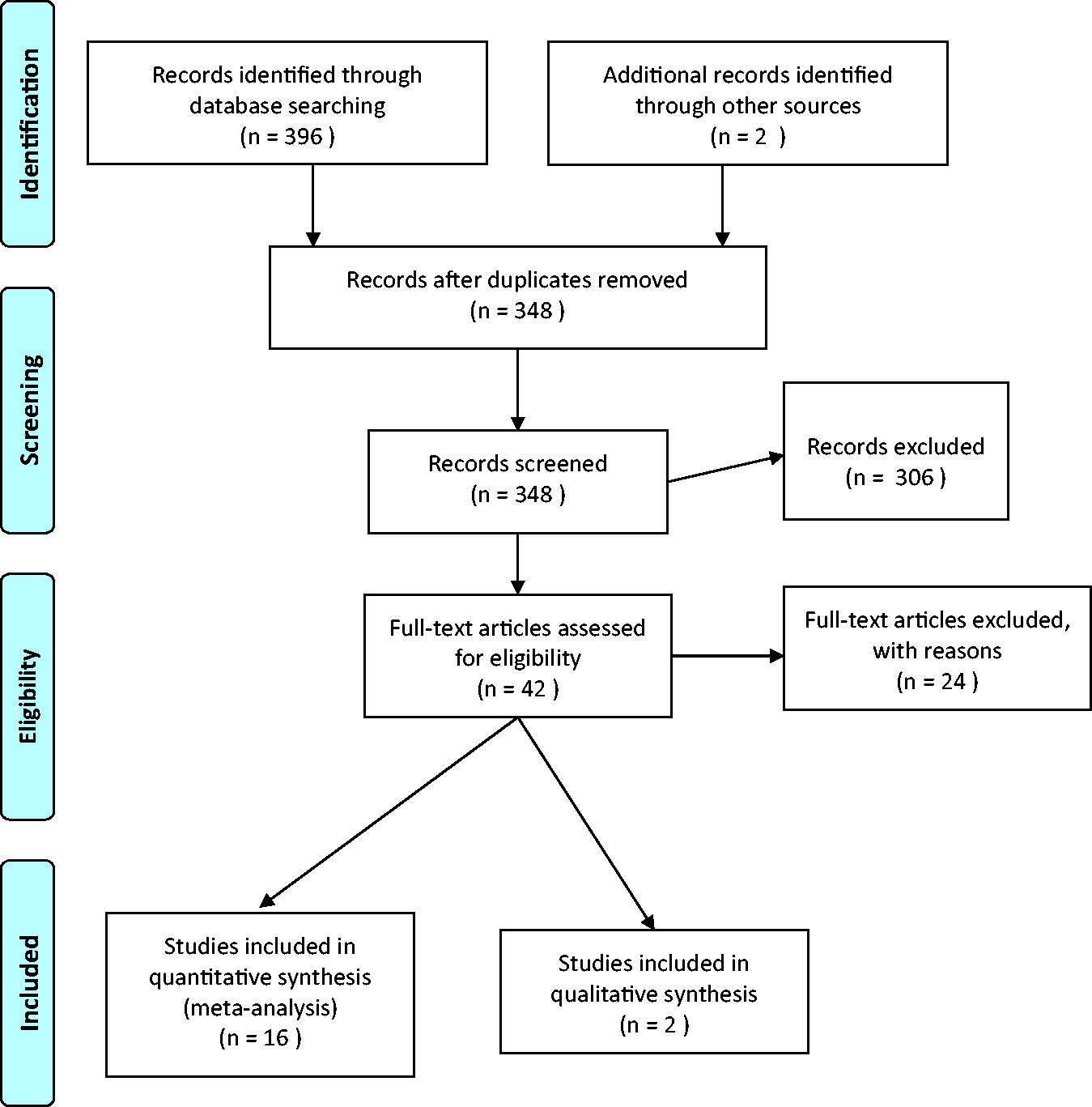
Quantitative studies
Sixteen studies remained in the review after screening for relevance (see Supplementary Table 1, which will be available with this article online). The studies focused almost exclusively on depression. Two studies discussed anxiety (Bowen, Bowen, Maslany, & Muhajarine, 2008; Goebert, Morland, Frattarelli, Onoye, & Matsu, 2007) and one study described neonatal complications of schizophrenia and affective disorders in the mother (Jablensky, Morgan, Zubrick, Bower, & Yellachich, 2005).
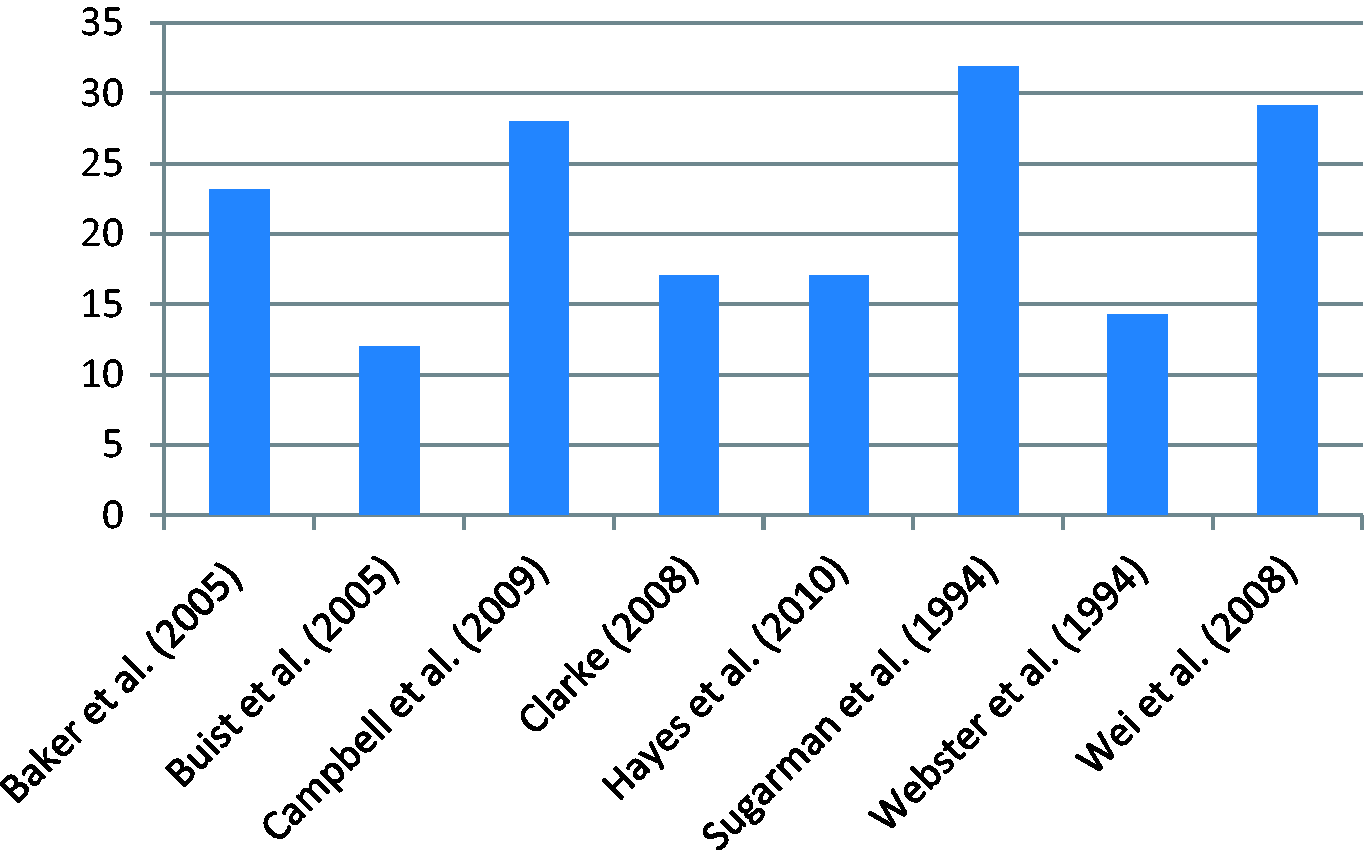
Figure 2 shows the prevalence rates of depression or depressive symptoms in pregnant Indigenous women across studies. Figure 3 illustrates the prevalence of depression in postpartum Indigenous women. There is no single “gold standard” measure for depression; therefore, the prevalence of depression identified by any diagnostic interview or scale may be an estimate rather than an actual rate. Self-report tools are more likely to find higher prevalence rates than those based on diagnostic interviews (Gavin et al., 2005). The Edinburgh Postnatal Depression Scale (EPDS; Cox, Holden, & Sagovsky, 1987) is the most thoroughly validated and widely utilized perinatal depression screening tool worldwide and was the tool most frequently used in the studies included in this review. Seven of the 16 studies assessed used the EPDS (Bowen et al., 2008; Bowen & Muhajarine, 2006; Bowen et al., 2009; Campbell, Hayes, & Buckby, 2008; Clarke, 2008; Hayes, Campbell, Buckby, Geia, & Egan, 2010; Webster, Thompson, Mitchell, & Werry, 1994). Some authors have identified an anxiety subscale within the EPDS (Items 3, 4, 5; Bowen et al., 2008; Ross, Gilbert Evans, Sellers, & Romach, 2003). Only two studies described validation of the scale for use with Indigenous women. Clarke (2008) validated the EPDS, the Beck Depression Inventory (BDI II), and the Postpartum Depression Screening Scale (PPDS). Hayes et al. (2010) modified the EPDS for use with Indigenous women in Australia through iterative consultations within various communities.
Prevalence of antenatal depression in selected studies (%). Prevalence of postpartum depression in selected studies (%).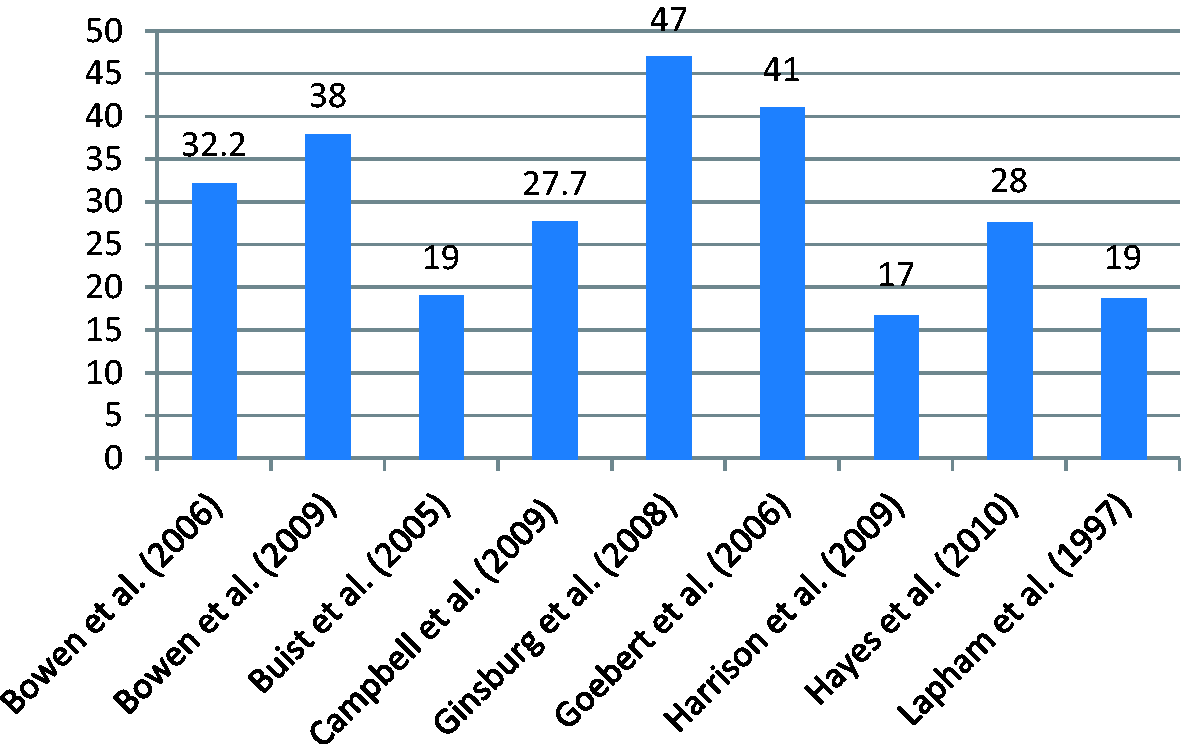
There are many different Indigenous populations throughout the world; however, very few studies gave detailed descriptions of the Indigenous samples; an exception was a study that described women (n = 53) from the Navajo and White Mountain Apache reservations in the United States (Ginsburg et al., 2008). Most studies described Indigenous women as subsamples of larger epidemiological samples of women in a specific geographical area, often collapsed into one general category. For example, in one study, the Aboriginal population was 65% of the sample (Bowen et al., 2008; Bowen & Muhajarine, 2006; Bowen et al., 2009).
The studies retrieved were equally divided between studies of antenatal women (n = 8) and postpartum women (n = 7). Two reports were longitudinal studies of antenatal and postpartum women (Campbell et al., 2008; Hayes et al., 2010). All Canadian studies reviewed were based on women from one province: Saskatchewan (Bowen et al., 2008; Bowen & Muhajarine, 2006; Clarke, 2008). We did not find any studies that included Inuit women, but did find one study that describes Aleut and Eskimo women from Alaska who were living outside their home community (Sugarman, Brenneman, LaRoque, Warren, & Goldbering, 1994).
Of note, Beyondblue: The National Depression Initiative (2008) in Australia included a large study of depression in over 40,000 antenatal and 15,000 postpartum women; of these, 3.3% of the women were Aboriginal/Torres Strait Islander, representative of the national prevalence of 3.6% of Aboriginal/Torres Strait Islanders in the wider population. The strongest risk factor for depression was Indigenous ethnicity. Among the Indigenous women, 19% had antenatal depression versus 8.9% among non-Indigenous women, 12% had postnatal depression versus 7.6% in non-Indigenous women, and 6.3% had both antenatal and postpartum compared to 2.7% in non-Indigenous women (Buist & Bilszta, 2005).
Most of the quantitative studies used convenience samples and were cross-sectional, with a single measure of depression or anxiety at one assessment point. There was one longitudinal study in pregnant and postpartum women (n = 210; Campbell et al., 2008), which found that 27.7% of pregnant women were depressed, and 28% experienced postpartum depression. Few of the studies (n = 5) achieved the recommended sample size of 300 (Loney et al., 2000).
Qualitative studies
Only two qualitative research studies met our relevance criteria. The first by Chamberlain and Barclay (2000), examined a birthing project in two Arctic communities. The study used a broad, qualitative approach to describe the psychosocial effects of transferring Inuit women from their home communities to give birth in urban settings. Three major themes emerged from in-depth analysis of the transcripts: (a) stressors; (b) choices; and (c) support. Unique stressors experienced by women who suffered enforced separation to deliver outside their home community related to emotional, physical, or financial issues. Returning to their home community after a lengthy separation was also very stressful. Physical stressors included the lack of choice in birthplace, the type of delivery, the amount of labour and delivery support during a particularly painful birth, and the lack of help initiating and sustaining breastfeeding. Costs incurred from having to be sent out of the community (e.g., telephone calls home or paying for babysitters) contributed to financial stress. Having little say in health care decisions or having the health care team make these decisions on their behalf were also major sources of stress. The subtheme of support was evidenced by the trauma of going through labour without support from partners, family, or cultural practices, and with little support from the nursing staff. In contrast, the mothers who delivered in their community said that they appreciated the care and follow-up provided to them.
Chamberlain and Barclay (2000) emphasized that the psychosocial disruption to women who were relocated for delivery was related to the lack of support from their families, community, and culture. However, the views expressed should be interpreted with caution given the challenges of conducting the research (e.g., lack of skilled interviewers, inaccessibility to families, or limited funding). While this was not a robust qualitative study (i.e., it lacked rigorous methodology), it yielded useful insights into the stress and worry experienced by these women.
The second included study was a doctoral research project using grounded theory methodology with a sample of First Nations and Métis women in an urban community in Saskatchewan, Canada (Clarke, 2008). The goal of the project was to examine the participants’ perceptions and beliefs regarding the nature and perceived cause of their postpartum depression. A majority of the nine participants were single, with low levels of income and education, and ranged in age from 20 to 31 years old. An interview was also conducted with an Aboriginal Elder to shed light on traditional childbearing practices and the sociocultural implications of postpartum depression (Clarke, 2008). Central to Clarke’s (2008) theoretical model was the ambivalence and conflict surrounding motherhood, which she believed were the core of postpartum depression. Within this core, four interdependent themes were abstracted: (a) becoming a mother; (b) being a mother; (c) partnership: being and feeling alone; and (d) lack of support. Becoming a mother included denial, disbelief, and sometimes a lack of acceptance of their unplanned pregnancies; the postpartum period was portrayed as a time of turmoil, pervasive loss, and lack of bonding. Manifestations of ambivalence and conflict included the mothers’ anger, frustration, and resentment towards themselves, their babies, and their social networks. Participants described feeling alone, betrayed, abandoned, and unsupported by their partners. Lack of emotional and practical support from partner, family, and community was discussed by many of the participants. Overall, the women felt overwhelmed with emotional and interpersonal conflict in many aspects of their lives. Clarke (2008) also identified three sociocultural factors related to motherhood and postpartum depression: (a) cultural disconnectedness; (b) sociodemographic barriers; and (c) history of abuse. Cultural disconnectedness emphasized that traditional practices failed to consider the issue of postpartum depression. Clarke suggested that health care providers consider the psychological adjustment required for Aboriginal women giving birth. In particular, it is important for care providers to assess anxiety, depression, maternal attachment, and social support (Clarke, 2008). Interestingly, Clarke chose a grounded theory methodology, although her research questions were not change-oriented, nor did they indicate a process that would be amenable to producing theory. Of note, there was a lack of acknowledgement of diverse or conflicting views throughout the discussion; rather, there tended to be reliance on other studies that supported her findings.
This was the only relevant study to comment on the impact of spirituality on Aboriginal women’s experience of perinatal depression. The Aboriginal Elder explained how traditional spiritual and religious practices such as prayers and smudging could help to reduce or prevent depressive symptoms and teach pregnant women how to take care of and to raise a child. The thesis also discusses how colonization and giving birth within hospitals of the predominantly Euro-Canadian society have altered childbearing experiences (Clarke, 2008).
Although the two included qualitative studies drew participants from very different backgrounds, northern rural versus urban, the women shared some common experiences. All felt disconnected from the comfort and support of their culture, their partners, family, and friends, whether or not they were geographically separated from them. They shared their experiences of feeling alone, and noted that having access to an Aboriginal midwife would be welcome.
Excluded qualitative studies
Despite not meeting the CASP critical review criteria, six studies are worth commenting on, given that they provide information about the experience and health of pregnant and postpartum Indigenous women. The main reason for exclusion of these studies was lack of a focus on depression during pregnancy or postpartum among Aboriginal women (Carruthers, 1987; Pollard, 2005; Smith, Edwards, Varcoe, Martens, & Davies, 2006; Solowski, 1995; Wilson, 2000; Woodman, 2006). We summarize the key points from each study.
Carruthers (1987) undertook “culturalogical” (unstructured) interviews with eight Native/Indian women living on a reserve referred to as “Eagle” Canada. Carruthers suggests that postpartum depression is rare among Eagle women: “It is a white illness and only white women suffer it” (p. 80). Only one firsthand account of “sad or overwhelming feelings in the immediate postpartum period” was heard (p. 81), which conflicts with the evidence from our review of the quantitative literature. Carruthers mentions that Eagle women feel “trapped” in stressful situations, and, in a crisis, “it is the women who must go from the reserve” (p. 68).
A review article by Pollard (2005) discussed issues related to childbearing among Indigenous women in Australia with a focus on “understanding of the biological systems impinging on our lives,” and the impact of existing inequities. Pollard’s findings suggest that when women feel a sense of control over their lives, wellbeing is promoted and this is more effective than providing unsolicited advice about behaviours such as smoking, diet, and exercise. Pollard states, “Reproductive risk, particularly among teenage mothers, reflects low socioeconomic status, inappropriate lifestyles and high levels of distress” (p. 399).
Smith et al. (2006) explored issues related to Aboriginal women’s access to prenatal care in two Canadian communities. The authors used a case study design within participatory action research, guided by a critical, postcolonial stance. Exploratory interviews and small group discussions with community-based stakeholders were used to explore experiences related to improvements in care for pregnant and parenting Aboriginal people. The authors conclude that colonizing policies, which might involve demeaning and disrespectful interactions between care providers and Aboriginal people, are one of the root causes of inequities in health and access to services. Participants saw pregnancy as an important opportunity for change, but health care organizations and relationships must be safe and responsive.
To investigate the spiritual, social, and psychological factors that motivate women to bear children, Solowski (1995) interviewed seven urban First Nations women who had experienced a pregnancy. She reported that “Pregnancy is traditionally believed to be a blessing from the creator”; it is a natural process and not considered an illness (p. 93). Pregnant women are encouraged to have positive, pleasant thoughts and to communicate with their babies. Even though prenatal care is generally believed to be beneficial, “many [women] perceive no benefits” (p. 96). This may be based on previous, uncomplicated pregnancies or on the difficulty in attending prenatal care (e.g., lack of babysitting services). Often, communication with health care providers is less than ideal. First Nations women can be shy and reluctant to ask or answer extensive questions; these women generally desire interactions that are nonauthoritarian and friendly.
Wilson’s (2000) thesis studied the perceptions of five socially high-risk pregnant Aboriginal women from Western Canada. Aboriginal women Elders were contacted to discuss the themes that emerged from participant interviews. Wilson concluded that “High-risk pregnant women often experience poverty and inadequate prenatal care, and experience feelings of ambivalence, depression, low self esteem, unhappiness, and little control over one’s life” (p. 9). She discusses barriers that women encountered seeking prenatal care, such as structural barriers (e.g., inadequate finances, lack of transportation, and child care needs), barriers related to sociodemographic conditions (e.g., young age, marital status, financial status, education level, and parity), and individual barriers (e.g., personal perceptions, personal issues). Wilson also asserts that many Aboriginal women want traditional midwives and healers included in their pre- and postnatal care.
Woodman (2006) used semistructured interviews to gather the perspective of 10 pregnant Aboriginal women from Eastern Canada about the barriers to a positive birth experience. Pregnancy is viewed as a natural process among Aboriginal communities, and consequently the participants did not feel the need for medical interventions or changes to their lifestyles. The author recommends that government provide extra funding for mental health services to pregnant women who require them. These services should deliver culturally sensitive mental health to help women deal with emotional changes and stress management during pregnancy and postpartum depression, if needed.
In summary, the above studies echo the two included qualitative studies by Chamberlain and Barclay (2000) and Clarke (2008) about the need to engage Indigenous women in prenatal health care services and to use Indigenous traditions in the care of and interaction with pregnant or postpartum Indigenous women. Further, there is no denying the impact that poor socioeconomic conditions and colonization have had on Indigenous peoples. Because of the effect on pregnancy and offspring, these factors will continue to affect future generations.
Literature for mental health promotion
We also explored grey literature, videos, and books to identify work that could inform research, policy, and practice. We note here three reports that discuss factors related to depression in Indigenous women.
“Celebrating the Circle of Life” (British Columbia Perinatal Health Program, 2009) is a culturally responsive document for Indigenous pregnant and postpartum women. While this is a woman-friendly, easy-to-read document, there are no references or sources listed for the content. The Beyondblue (2008), report which addresses perinatal mental health in Australia, notes that perinatal depression is more common in Aboriginal and Torres Strait Islander women than in other Australian women. It recommends further research, particularly to determine appropriate measurement tools for Indigenous women. The report emphasizes that a national strategy is essential to help alleviate perinatal depression in Aboriginal and Torres Strait Islander women. The MCH Screening Tool Project recommends the use of two tools for depression during and after pregnancy by the Maternal and Child Health Family Visitors (Stout & Jodoin, 2006): (a) the Edinburgh Postnatal Depression Scale (EPDS; Cox et al., 1987) as valid for use in First Nations and Métis women, and (b) the Postpartum Depression Screening Scale (PDSS; Beck & Gable, 2000) as useful for Native American women.
One video was also reviewed: Boodjarri Business: Working With Aboriginal Mums, Babies and Families (Women and Newborn Health Service Health Professionals, 2007), from Western Australia. The video provides a general overview of the blues, anxiety, depression, and psychosis as well as the risks and supports unique to Aboriginal childbearing women. Interestingly, the video views the postpartum period as up to 36 weeks after birth, compared to the usual 1-year time period common in other parts of the world. The video’s strengths are the inclusion of Aboriginal women telling their stories of depression and the portrayal of the impact of mothers’ mental health on children and fathers. It also talks about the “stolen generation” of women—those women who are forced to travel to deliver away from home—and the importance of traditional healing.
Discussion
There is a paucity of literature devoted to the study of depression, anxiety, and mood problems in perinatal Indigenous women. This could be improved, if researchers address the following:
More studies are needed to identify the extent of the problem
Better understanding of the true prevalence, associated factors, and effects of perinatal depression can be achieved through large, population-based, longitudinal studies and through oversampling. Studies need to focus on depression, anxiety, and mood problems as the primary outcome rather than the secondary finding of the research. Research needs to be conducted in ways that will not raise concern about child apprehension if women disclose their actual feelings of anxiety, depression, mood problems, or of inflicting harm on herself or the child.
Furthermore, it would be of interest to identify factors within the Indigenous woman’s postpartum structure that may put her more at risk for postpartum depression. Several studies report lack of partner support as a significant predictor of depression (Bowen & Muhajarine, 2006; Ginsburg et al., 2008; Lapham, Henley, & Skipper, 1997; Webster et al., 1994). Other structures that were found to influence depression were a lack of public services (Ginsburg et al., 2008) or health insurance (i.e., in the United States; Sugarman et al., 1994).
Adapt or develop culturally appropriate screening tools
Translation, modification, and validation of anxiety and depression screening tools can increase recognition of mental health needs and accessibility for First Nations, Inuit, and Indigenous women in both research and practice.
Increase our understanding of culture and meaning in illness experience
A variety of strategies can improve the integration of cultural knowledge in mental health research. These include promoting researchers who are “insider” members of the community rather than “outsiders” (Tuhiwai Smith, 1999). However, it is important to bear in mind that research can also be difficult for an insider, as they can feel torn between obligations to their institution, as well as their cultural group (Lincoln & Gonzalez, 2008). Narrative approaches and participatory action research (PAR) have been identified as the most ethically appropriate methodologies for studying Indigenous populations (Assembly of First Nations, 2007). The challenge for researchers is accessing Indigenous women willing to share their stories and ensuring that the researcher’s interpretations are accurate. This can be improved by including Elders and women with lived experience with perinatal mood problems to ensure the rigour of methodology and interpretation of findings. Indigenous women must be able to voice what is most helpful to them in order to better understand their responses to commonly available treatment modalities in non-Indigenous populations.
Outcomes of mental health problems
There is a dearth of reported research that evaluates the outcomes of untreated perinatal depression on the family, including Indigenous women, their partners, and their children.
Understand more about positive mental health in Indigenous women
Despite increased exposure to social circumstances that put them at greater risk, a majority of Indigenous women appear to be resilient and do not develop mood problems. Therefore, it is essential for women to share their stories of resilience and positive mothering following recovery from mental health problems in order to inform caregivers and to support other women who may be experiencing similar situations.
Ensure scientific rigour
Researchers who wish to explore mental health within Indigenous perinatal women need to ensure or demonstrate scientific rigour, as well as sensitivity to Indigenous values. The CIHR Guidelines for Health Research Involving Aboriginal People (Canadian Institutes of Health Research, 2007) address the ethical necessity and pragmatics of research collaboration with Indigenous communities. The guidelines recommend co-ownership of data between communities and the researchers, ensuring that individuals retain the right to access data about themselves; and that Indigenous group members be included in the research process. Research questions need to be generated in collaboration with the community with a goal of understanding and improving the lives of perinatal Indigenous women and their families.
Conclusions
Indigenous women are a growing segment of the population of women giving birth. Overall, they experience more risk factors for mental health problems than non-Indigenous women. This critical review confirms that compared to women in the general population, a larger proportion of Indigenous women experience mental health problems during pregnancy and postpartum. However, the dearth of detailed information about the mental health problems of Indigenous demands rigorous, longitudinal studies that primarily explore depression, anxiety, or mood problems and positive mental health.
Footnotes
Funding
This research received funding from Health Canada.
Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.