
Abstract
This paper brings forth the voices of adult Aboriginal First Nations community members who gathered in focus groups to discuss the problem of youth suicide on their reserves. Our approach emphasizes multilevel (e.g., individual, family, and broader ecological systems) factors viewed by participants as relevant to youth suicide. Wheaton’s conceptualization of stressors and Evans-Campbell’s multilevel classification of the impacts of historical trauma are used as theoretical and analytic guides. Thematic analysis of qualitative data transcripts revealed a highly complex intersection of stressors, traumas, and social problems seen by community members as underlying mechanisms influencing heightened levels of Aboriginal youth suicidality. Our multilevel coding approach revealed that suicidal behaviors were described by community members largely as a problem with deep historical and contemporary structural roots, as opposed to being viewed as individualized pathology.
Introduction
Suicidal behaviors are among the most significant mental health-related problems among youth (Reynolds & Mazza, 1994), and are even more pronounced among North American Indigenous youth, including the youngest generations of First Nations communities across Canada. As part of a report by the Advisory Group on Suicide Prevention (2002), summary statistics on suicide within Canada revealed rates 5 to 6 times higher among First Nations youth compared to the non-Aboriginal population, with evidence of growing rates in some communities. While these alarming trends suggest that suicide is a problem for many First Nations, it is important to note the differences in suicide rates and risk factors across cultural groups. There are over 1 million self-identified Aboriginals (including First Nations, Métis, and Inuit) in Canada, and over 600 First Nations bands alone (Statistics Canada, 2008), with variability in histories, contemporary community characteristics, levels of enculturation, and traditional practices both within and across groups, thus underscoring the need for careful conceptualizations of “culture” (Waldram, 2009) and due attention to Aboriginal diversity.
The purpose of this paper is to share the voices of adult community members from a single cultural group across three separate central Canadian First Nations reserves who participated in focus group discussions about the devastating loss of their young people to suicide. Our research team views qualitative methods as essential to a culturally relevant understanding of community needs and strengths. Unfortunately, as Cutcliffe (2005) asserts, “the ‘voices’ of First-Nation people are noticeably ‘silent’ from the suicide related literature; without these voices—the narrative and phenomenological accounts, we are unable to account for the particular developmental-existential suicide perspectives of these people” (p. 144). This paper is one step in the efforts to break that silence within the academic literature.
Multilevel conceptualization of stressors
Much of the existing research on correlates of suicide is framed within a “risk-protective factor” approach in which those constructs thought to increase suicidal behaviors are labeled “risks,” while measures negatively associated with suicidality are viewed as “protective.” In this study, our approach is to conceptualize risks as exposure to stressors such as traumas and negative life events. The stress exposure framework affords an opportunity to investigate etiological factors found within the social environment that may be modifiable and/or preventable (Aneshensel, 2009), and therefore useful to efforts aimed at reducing suicidal behaviors. A multilevel examination of stressors related to Aboriginal suicidality broadens our focus to include not only the individual and interpersonal characteristics often identified as pathological (e.g., substance use: Kirmayer, 1994; Olson & Wahab, 2006; distress and mental disorder: LeMaster, Beals, Novins, & Manson, 2004; and prior victimization: Bohn, 2003; Shaughnessy, Doshi, & Jones, 2004), but also community- and societal-level determinants of health and health behaviors. Prior research has indicated that even broad contextual variables like community socioeconomic disadvantage are related to poorer mental health and problem behaviors (Aneshensel & Sucoff, 1996; Beautrais, 2003; Brooks-Gunn, Duncan, Kato Klebanov, & Sealand, 1993; Wight, Botticello, & Aneshensel, 2006). Macro- and meso-level explanations for differential suicide rates date at least as far back as Durkheim’s classic piece, Le Suicide (1897; Suicide: A Study in Sociology, 1951). Likewise, Bronfenbrenner’s (1979) well-known ecological systems theory delineates multiple levels of contextual and multidirectional influence on child development in particular. Thus, casting a wider etiological net that captures a range of ecological risks is imperative.
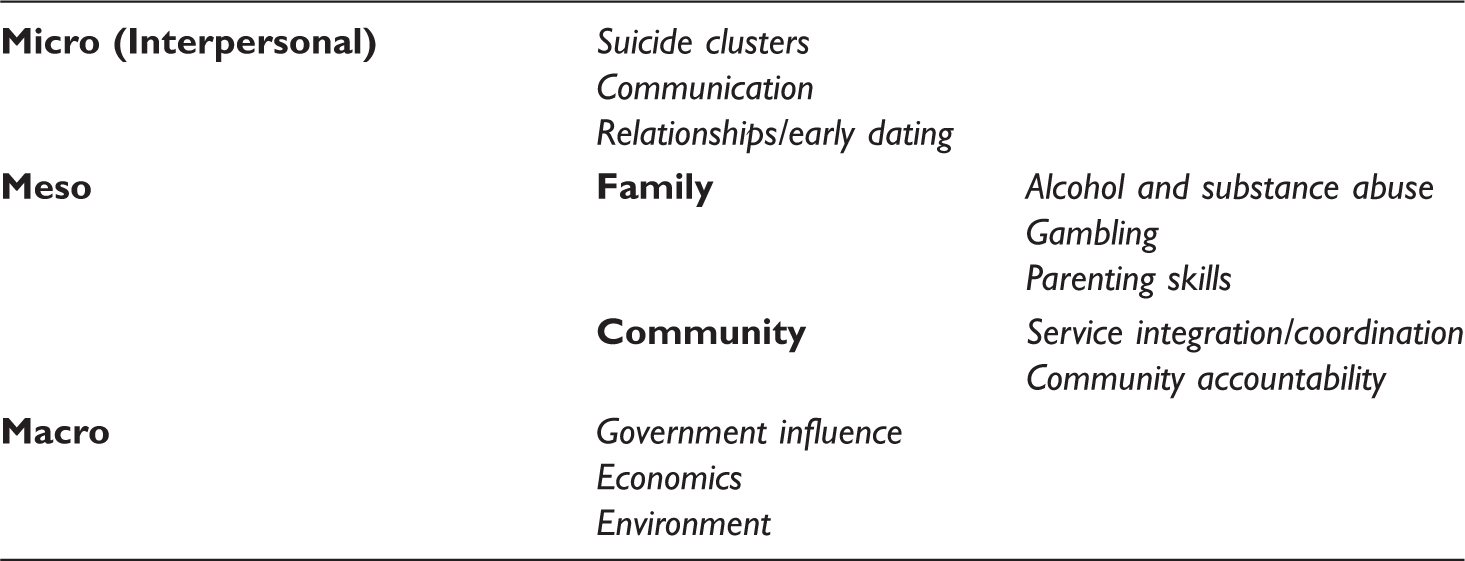
We employ Wheaton’s (1994, 1999) conceptualization of stressors and Evans-Campbell’s (2008) multilevel approach to historical trauma as theoretical and analytic guides to organizing and understanding the complex set of factors influencing suicidality among young Aboriginal community members. Wheaton provides a categorization of stress across three distinct levels: (a) macro or ecological stressors are those systemic in nature and found above the individual level, including macroeconomic problems like unemployment; (b) micro stressors, which occur on an individual or interpersonal level; and (c) meso stressors that represent an intermediary classification of stress between macro and micro levels to include neighborhood, community, and work/school conditions, for example. Of course, these categories are not necessarily clear-cut in all cases and do not fully illustrate the possible conjunction of stressors across levels. For example, exposure to individual or interpersonal stressors may well be contingent upon contextual stressors occurring at a much more macro-level (Wheaton, 1999).
A multilevel approach to historical trauma
European colonization of North America began with initial contact between Indigenous groups and immigrants and has continued over the years in many forms, including attempted assimilation of communities, the creation of reservations/reserves, relocation policies, and underfunded, inadequate health and educational services (Kirmayer, Tait, & Simpson, 2009; Roubideaux, 2005). Walters and Simoni’s (2002) Indigenist stress-coping model “acknowledges the colonized or fourth world position of Natives … and advocates for their empowerment and sovereignty” (p. 520). Their framework is consistent with an important contribution of the stress process literature to highlight the differential exposure and cumulative impact of stressors on underprivileged groups (Pearlin, 1989; Pearlin, Aneshensel, & LeBlanc, 1997; Turner & Lloyd, 1995). For the Aboriginal peoples of North America, a unique and traumatic history of colonization contributes to intergenerational exposures to stressors and contemporary chronic strains.
The pervasive effects of history on Indigenous life have been conceptualized as historical trauma, or the persistent, intergenerational exposure and response to multiple traumatic events within communities (Brave Heart, 1999; Brave Heart & DeBruyn, 1998). Traumas of this sort are considered “historical” insofar as they began in the past; however, the oppressive, restrictive policies and practices of colonization continue in many ways to the present day. Evans-Campbell (2008) has referenced the broad array of contemporary outcomes of historical trauma as multilevel in nature, affecting individuals, families, and communities.
At the individual level, research with Indigenous communities has found that perceptions of historical cultural losses are associated with sadness, anxiety, mistrust of White people, anger, distress, and other negative outcomes (Whitbeck, Adams, Hoyt, & Chen, 2004; Whitbeck, Walls, Johnson, Morrisseau, & McDougall, 2009). The work of Brave Heart (1999; Brave Heart & Debruyn, 1998) identifies historical trauma as a source of grief, ruminating thoughts, anger, distress, and guilt among Indigenous adults and parents. Evans-Campbell (2008) further notes the potential for historical traumas to increase stress vulnerability, a phenomenon documented among Jewish Holocaust survivors (see Solomon, Kother, & Mikulincer, 1988; Yehuda, 1999).
The family-level outcomes of historical trauma include contemporary attention to ancestral traumas and associated guilt. Moreover, the widespread enrollment of Indigenous children in government- and church-based boarding/residential schools represents a critical interruption of healthy, culturally rooted caretaker socialization. Numerous sources chronicle the abuses endured by many of the children residing in boarding schools (e.g., Adams, 1995; Ahern, 1994; Milloy, 1999). As a result, some Indigenous adults have struggled and felt overwhelmed in their role as parents (Brave Heart, 1999), thus affecting subsequent generations’ development.
The last unit of classification in Evans-Campbell’s (2008) approach emphasizes community-level responses to historical trauma; she asserts that this level of impact has received little attention in the academic literature. Beyond attacks on Tribal sovereignty and, for some communities, a lack of basic, well-functioning agencies and institutions (e.g., education and health care systems; Roubideaux, 2005), historical traumatic events and policies have the potential for community-wide perceptions of loss and grief. Especially germane to this study are historical community losses of Aboriginal children to boarding schools, adoptions outside the reserve, and foster care. Disproportionate youth suicide rates represent one additional community trauma response (Duran & Duran, 1995).
Methods
The focus group methodology employed for this study was built upon on an already established longitudinal survey research project created in partnership with a United States university and several U.S. reservations and Canadian First Nations. This smaller, qualitative component of the study was facilitated by the community networks, advisory boards, and Tribal research workers already implemented and maintained through the survey project.
Focus groups were led by the first author at three separate First Nations reserve locations across central Canada in the summer of 2005. Throughout the planning and recruitment process for these focus groups, an on-site project coordinator facilitated communication and planning between university-based staff and the reserve community members. All project methodologies and questions were developed in partnership with and approved by an advisory board comprised of Tribal members from each participating reserve.
Advisory members from each reserve agreed to recruit participants for two separate focus group sessions at each community: the first groups included Elders, and the second was comprised of service providers who worked within the community as mental health workers/counselors, crisis response team members, youth and family welfare/child safety employees, youth educators, substance use or chemical dependency counselors, and so forth. Elders were invited to these discussions because of their cultural status as wisdom-keepers, storytellers, and respected caregivers. Service providers were included because of their proximity to and experience dealing with crisis situations like suicide within the communities. In this case, all of the service providers were in fact Aboriginal community members themselves and thus maintained kinship roles (including the role of Elder in some cases) in addition to their professional duties. A total of six focus groups were planned and completed. Upon recruitment, participants were provided with a brochure containing project information, the goals of the focus groups, and the basic content of our planned discussions. Our recruitment goals included 10 Elders and 12 service providers per site, with an even split by gender; this goal was generally met at each site, with the exception of one or two recruited members being replaced, not being able to attend, or, in some cases, including additional interested community members. This flexibility was an important part of our focus group process and helped in our goal of creating a welcoming and trusting atmosphere for community members (see also Krueger & Casey, 2000). For all focus groups, the first author (a member of the cultural group included in this study) was accompanied by project coordinator Allan Morrisseau for guidance, advice, and practical considerations (e.g., driving directions in remote reserve areas). In addition, a project consultant and Aboriginal Elder and translator, Calvin Bombay, accompanied us to half of the focus groups.
Location and materials
Advisory board members at each site were responsible for locating a convenient and available space where focus group conversations could take place. The selected sites were a community building/shelter, a church, and a school classroom. Community cooks were hired to provide participants with a warm meal. In addition, refreshments, a traditional offering of tobacco, and a monetary gift were given as incentives for participation.
Prior to each discussion, participants were provided with University of Nebraska Institutional Review Board (IRB) approved consent forms. As part of the consent process, participants were informed that the audio-tapes resulting from the group discussions would be returned to their advisory boards upon completion of transcription and data analysis. Signed consent forms were obtained from all participants prior to each discussion. Focus group discussions ranged in length from approximately 1.5 to 3 hours (with meal). No distinct differences in active participation (i.e., speaking) rates were observed across groups or by participant gender; however, the Elder groups did tend to last longer on average than did the service provider gatherings. A copy of the questioning route used for these discussions can be found in the Appendix.
Analytic procedure
All audio-taped focus group conversations were transcribed verbatim and open-coded by the first author with hand jottings and notations that identified general themes in the data (Creswell, 1994; Lofland, Snow, Anderson, & Lofland, 2005). This process of open-coding resulted in over 30 themes related to suicide risk and prevention strategies. A focused coding strategy (Charmaz, 2006) was used to more directly identify excerpts and combine open-coding categories where appropriate. Using the team’s list of focused thematic areas, the second and third authors independently classified each theme into “levels” of risk using the multilevel frameworks described earlier. That is, each author examined transcript excerpts by theme to assign a label of “macro,” “micro,” etc. A simple calculation of interrater reliability for their multilevel classification of 88% (κ .81; p < .001) was calculated, indicating a high level of agreement between the two raters (Landis & Koch, 1977). Disagreements in the multilevel classification were discussed among all authors until consensus was reached. Participants are identified below by gender, group type, and group number corresponding with reserve location to protect confidentiality. Beyond the findings discussed in this paper, the themes that emerged from these data are being/have been used to develop community reports and inform the development of suicide prevention programming.
Results
Interpersonal factors
Both Wheaton (1994, 1999) and Evans-Campbell (2008) cite individual-level factors in their models to include anxiety, sadness, depression, and other affective states and emotions. Focus-group participants did not emphasize individual-level pathologies (e.g., mental illness, depression, etc.) or risk factors in our discussions. In the rare event that individualized risks were identified, they were explicitly linked to their ecological causes as opposed to individual dysfunction. For example, feelings of hopelessness were caused by environmental risks; alcohol and drug use was viewed as learned intergenerational behavior. There were, however, several examples of interpersonal risk factors within the data that correspond to Wheaton’s micro-level description:
Suicide clusters/normalized suicidality
On all three reserves, participants noted that youth suicides often occurred in “clusters.” Clusters, or “copy cats,” refer to a series of suicides and/or suicide attempts that occur within a short period of time and among a group of friends or family members. I went to [another community] about 3 years ago … had a boy there, he was about 12 years old. He was playing around that evening with his friends. In the morning they found all those boys hanging [emphasis added], they had committed suicide. (Male Elder, Group 3) And I think that it has a lot to do with modeling too. They pick up from each other and form, if one person does it, it’s okay; get rid of my problems and so forth. And, I’ll do this and it works to solve my problems. (Male service provider, Group 1) That young man, I guess he told them he was going to commit suicide, but they [the friend] didn’t tell anybody because that’s the pact that they make: That once somebody’s going to commit suicide that they follow or they do it that same time he’s going to do it. But some of them feel bad about it then that’s where the chain reactions sets in. (Male service provider, Group 3) You could see it [suicide] at a young age here and then you think that’s the way out. Well, it seems they [suicides] can just become the normal part of life. They accept it like that. (Shared dialogue, male and female service providers, Group 2)
Communication barriers
A lack of communication between youth and adults was discussed across all six focus groups in the three reserve communities. Alcohol and substance use and abuse, a feeling that there is nobody to talk to, and an inability to trust were viewed as key barriers to effective communication. In the family, substance abuse interferes with effective communication about important life issues (i.e., breaking up with a significant other, alcohol/substance issues, family problems, etc.). They [youth] need ways to talk about it or they talk about it and say it when they’re drunk or they have stress and they don’t know how to deal with to get through it, talk about this dilemma. (Male service provider, Group 1) I always think it’s a lack of communication from the parents. They can’t ask them, they don’t discuss things, you know? Even if they [parents] are out drinking, go and look for them [youth]. Even if they can’t find them at least they will always know that you care; it might not stop them from drinking but at least that child knows how much you care about them. (Female Elder, Group 1) The school didn’t allow the Elders to come in and talk to the kids; discipline is different between school and home—not enough Elders talk to the kids, there is a big communication gap between Elders and kids. (Female Elder, Group 2) Like the Elders, they opened it [healing circles] up to the Elders to come in and sit with them [youth], to help them. It was good. Those guys talk about how good it was for them to come here and be in that circle. But then it just kind of broke or something. (Female service provider, Group 1) Now when we talk about suicide, I see the same thing. What is it the youth couldn’t talk about? They couldn’t find anyone to share this with. (Female Elder, Group 3) I think an issue that I’m seeing on the reserve is the trust. A person you don’t trust, you don’t talk to … just who [is there] to trust? … [They are] probably spreading around rumors so who can you trust? (Female service provider, Group 1)
Relationships/early dating
Problems associated with early dating and romantic relationships were identified as influencing youth suicidal behaviors. A key component to this theme was coping with the rejection feeling of a break-up. As the kids are breaking up with their boyfriends and girlfriends, they commit suicide. (Male Elder, Group 1) And one of the things about young people why they take their lives because they go through relationships and the minute there’s separation in their relationships they can’t handle rejection and they just take their life because it’s so painful. Rejection is so painful that they can’t take it. (Male Elder, Group 3) They start early … and by the time they are 14 or 15 they are a mother of two. They’ve been in a relationship for 4 or 5 years. Then one day one of them wants to break up and they don’t know how to deal with it. (Male service provider, Group 2) I would probably say [we need] more sex education because there seems to be a lot more teens into sexual activity, teen pregnancy, and abortions here and there. You know they’re starting young nowadays. I think there needs to be more sexual education. (Female service provider, Group 1)
Meso-level factors
Wheaton’s (1994, 1999) model includes meso-level stressors that represent an intermediary classification of stress between micro and macro levels to include community and family. Evans-Campbell’s (2008) multilevel conceptualization of historical trauma model includes a distinct family and community level. Participants focused heavily on risk factors in the family, which made it useful to analyze the family level separately from community risks, although such divisions are somewhat arbitrary given the extended kinship patterns traditionally observed.
Family factors
In addition to and distinct from other interpersonal risk factors, problems in the family were frequently cited risk factors for youth suicidality. In particular, three family-level risk factors were identified: (a) alcohol and substance abuse, (b) gambling, and (c) lack of parenting skills. Although alcohol abuse and gambling might be conceptualized as individual- or community-level problems, the data suggest that these two themes have the strongest effect within the family.
Alcohol and substance abuse
Alcohol and substance use and abuse among youth, family, and community members were issues discussed in all of the focus groups. Parents who abuse alcohol and other substances were viewed as unable to effectively raise a child. Substance abuse problems within the family interacted with the theme of communication (see Interpersonal Factors section) and parenting skills (see below). In combination, these factors increase the likelihood of suicide ideation among youth. Some of it is unemployment, not enough food in the house due to alcoholism or drugs in the family. And they get, they get really depressed when they see their parents actually drinking and doing drugs instead of providing for them. (Male service provider, Group 3) I don’t think that hanging, taking pills, shooting yourself, as the only form of suicide. Drinking yourself to death is also a form of suicide. Rotting your brain with lacquer [liquor] is a form of suicide because you’ve rotted it so much you don’t have the cognitive ability to raise a child. (Dialogue between two female service providers, Group 2)
Gambling
Parental gambling was viewed as a serious problem across the three communities. Participants noted that unlike alcohol and substance abuse, gambling is not perceived as a social problem among most community members. That’s what I noticed; it’s not considered a problem at all, gambling. (Male service provider, Group 1) They’re [older siblings] home babysitting so their parents can go to bingo. Yeah, they’re babysitting their little siblings. And most of them run around hungry. (Dialogue between two male service providers, Group 3) They’re [the children] running around with, while the parents go play … their keno games or whatever just to go to bingo. That adds to their depression. That adds to their outlook. (Male service provider, Group 3)
Parenting skills
Ineffective parenting and a lack of positive parenting skills were frequently discussed across all three of the reserves. This theme interacted with several other findings, including communication problems and alcohol and substance abuse. Substance abuse issues were associated with negative parenting and ineffective, inadequate family communication. Many of the participants noted that parent alcohol and substance use harms the children because the addiction takes priority over care for the children. As their own mother and father they should be providing for the children before they even start doing the drugs or alcohol. That’s what I find in the community, there’s a lot of alcohol and drugs being pushed around and the children are the ones that are being left without the services that they need from their parents … I say we have to make the parent’s aware that they’re doing this. They’re the ones that are harming our children. (Male service provider, Group 3) This is a problem. There is a place where they [youth] are always drinking at night. Sometimes I’ll see them and say, oh, boy, he’s up early, but he hasn’t even gone to sleep yet … and it’s 8 o’clock in the morning! These are like 12, 13 year olds. Many, many years ago, when we were that age, we went to bed with the sun and got up with the sun! Parents were strict, then. Now, they just let them run. (Female Elder, Group 1) Parents let their kids stay at home too long—don’t make them take responsibility for themselves. Parents aren’t home and the children are left at home all the time. (Female Elder, Group 2) We got to work with the parents and … because everything comes from the parents … if we would [work] with the youth only, then they go back to the same situation at home. (Male service provider, Group 1) Getting the kids healthier will involve getting their parents healthy first, and that’s who I always see as the target is the parents. Parents need to be educated for their children. And the way we’re going to have to do that is give them a workshop on this stuff. Start giving workshops on anger management, on family violence, on alcohol and drugs and what that stuff does to the mind and the body and the spirit. I really believe that we have to educate these parents first. (Male service provider, Group 3)
Community-level factors
Community-wide social problems and norms were also found to influence suicide among First Nations youth. Two salient themes emerged from the data: (a) insufficient services and coordination, and (b) lack of community accountability. One of the first issues identified was how the community copes with and responds to suicide. I don’t think it [the community] really copes, it copes by lying back sort of like, you know, burying it or put a blanket on it. You know, it’s something that’s done and there is no way of reversing it, what happened. (Female service provider, Group 2)
Insufficient service coordination
Respondents discussed inadequate mental health services and ineffective service coordination in their reserve communities, highlighting the associated problems preventing and responding to suicide. The thing that gets me is … when they [youth] attempt … they come to the hospitals, they are sent to the hospitals, the next day they are out of there. It’s like a revolving [door], you come in and you go out. I think we need to work on that. (Male Elder, Group 2) I found that the communication was rather slow for the [counseling] center to be contacted. I think that really needs to be improved there, the communications within our counseling group … and I would like to see child and family involved … by arranging resource meetings, I think that’s the way we all come up with a good action plan. (Male service provider, Group 3)
Community accountability
To effectively combat First Nations youth suicide, focus group participants cited the need for the community to take accountability for suicide on the reserves and to take proactive measures to prevent it. In particular, most participants felt that not enough prevention work was happening. The need for more services and the ability to sustain these services after a suicide were also identified. People are going to have to start doing more … can’t just wait for the next person [to commit suicide]. (Male Elder, Group 2) So, this commission comes together after a suicide and tried to create suicide prevention. This seems to be the pattern, so there’s a rise in organized concern after a suicide, but then it fizzles out. (Male service provider, Group 2)
Macro-level factors
The community members who participated in these focus groups frequently reflected upon a variety of macro-level influences in their attempts to explain youth suicidality. We identified three major thematic patterns in the data at this level: federal government influence, economics, and reserve environment/norms. The interdependence of these processes is illustrated within the transcript excerpts that follow.
Influence from outside of the reserve was found to undermine traditional forms of social control and led to an inability of the community to regulate its own future. More specifically, participants noted two subthemes related to government influence: (a) the inability to discipline children, and (b) the effects of the welfare system. We can’t say nothing to the kids. We can’t say nothing … You’re not allowed to touch your own kids. (Dialogue between two Elder females, Group 2) Right now I would say that the White man has the predominant control of the way the community is going. It’s not like we think the way we think. So you know again when you’re talking about suicide, you know to me it is a symptom of rebuilding our people. (Male Elder, Group 3) The residential school system … there is too much influence from the outside. The welfare system is messing up the family system. (Female Elder, Group 2) Where are we today? We sit in a position of begging. Begging cap and hand to the government you know for a little measly amount of those crumbs we see off a very rich table that we call welfare which robs the dignity of the human being. (Male service provider, Group 3) We never had suicides before they created the reservations. Now we are stuck in one place and can’t roam wherever we want to. (Traditional language translation; male Elder, Group 1) I think all of our youth should go out and work outside of the reserve to know what is out there in terms of … what’s available to everybody. It’s just not happening. (Male service provider, Group 3) We’ve been looking at the poverty, the environment that we’re living in today. We did not create the poverty in our community. We did not choose to be born in this community. And the lack of economic opportunity, this community has created the anxiety, the depression, the hope and the addiction of drugs in this community. We did not choose you know for our families to be dysfunctional here in this community and other communities because what was taught to us was nothing less than dysfunction. (Male Elder, Group 3) Well … there’s a host of things that we need … economics, unemployment situations in reserves. It’s horrible. But, you know we want to live in our reserves, this is our home … these reserves are the only lands we have left and we want to keep them. We want to keep our communities but we desperately need jobs and stuff like that. (Male service provider, Group 3)
Historical trauma as an overarching, unifying theme
Although the risks for suicidal behaviors are presented here largely as independent factors, it is important to note that they represent a group of complex, interdependent variables. Focus group respondents likewise conceptualized “risk” in terms of a constellation of problem behaviors that share a historical root: These problems we have are just symptoms of our main problems, I think … like we try to solve alcohol problems, sniffing, and the fighting families, you know … those are just symptoms to me … Like residential schools, for example, that’s where we lost pretty well everything. (Male service provider, Group 2)
Effects of European contact and residential school system
I think there was no such a reason for committing suicide back then. Because with contact came in all kind of poisons … It was infected and then also the alcohol is what they turned to. So it [suicide] became a way to solve a problem. (Male service provider, Group 1)
The residential schools were viewed as a place where culture was, in large part, attacked and destroyed. The loss of the traditional way of life was seen to have impacted the dynamics of the family, with ramifications across generations. We’re all affected by the residential schools, everybody, all the people. Our grandparents that went there, it’s affected us. That is what I see. (Female service provider, Group 1) And our parents, they’re feeling that, feeling the effects of the residential school system. And I’d say the lack of parenting is a big issue. And we need them to realize that they’ve lost that love growing up. We need to instill that. We need them to because of the need for love is there. It’s the most important aspect of their children’s growing up and their behaviors. (Male service provider, Group 3)
Loss of identity
Another component of historical trauma/cultural losses discussed by participants was a departure from traditional cultural identity. Specifically, First Nations youth were seen as struggling to find their identities as Indigenous people in a contemporary context: Now if you go back in the history, where our … we had this building here. A concentration camp, I call it. Here you were stripped with your identity and it still lingers. (Male Elder, Group 3) We say we are like [cultural group]. We sound like a White man. So there is a massive confusion with our youth … Because we, because we fail to, to teach the traditions of our youth. The line is very, very important for them to find their identity as [cultural group]. (Male Elder, Group 3) You look at the institutions; they are not [cultural group]. To me, this, these are the things that are telling us why. Just let us be what we are, [cultural group]. When you speak the language, you feel it, you understand. Like when you ask questions, there’s all silence because we don’t follow. But, you talk to us in [our traditional language] we’ll respond right away; that’s how [cultural group] is. So, if you’re going to design a program, what kind of program can you design it to be? We have to go back to our way of life. So I am really glad that we are [cultural group]. (Male Elder, Group 3)
Returning to a traditional way of life
In order to reduce Aboriginal youth suicide, cultural reclamation was a critical step in the rebuilding of a wounded culture. Instilling a sense of pride about one’s language and spiritual ceremonies can lead to a better sense of self. Most of us don’t realize we carry a lot of pain, a lot of anger. And you know when we go to court, everybody’s treated equal but, we’re not equal to them because all those things were taken away from us. And the judges and the lawyers, they pretend they don’t understand why so many of us are in jail or in trouble, you know. But we’re not equal to them unless we recover those things we’ve lost, then we would be equal [emphasis added] … I didn’t realize I carry a lot of pain, a lot of anger. That was the only way I handled that pain was to drink. And I’m sure I’m not the only one that feels that way. (Male service provider, Group 2) I try to put that in perspective and then try understanding what it was like prior to the precontact of the European when he landed here in our homeland, and what I genetically remember from our ancestors is that our people were living a very beautiful life. There was an abundance of riches of the land and spirit. Our people were a spiritual people and we are a spiritual people and will always be a spiritual people. (Male Elder, Group 3)
Discussion
Multilevel classification of community identified risks for Aboriginal youth suicidality
Our attempt to organize risk factors by various levels of impact illuminates the wide range of social, historical, and cultural influences on suicidality within these Aboriginal communities. We found it difficult to categorize several of the often overlapping themes into distinctly unique levels of influence. For example, widespread substance use and gambling problems (both individual behaviors) were discussed as community-level issues, but seemed to impact youths from within extended family networks. Thus, we urge readers to interpret these findings with due consideration of the interdependence of themes.
A careful review of results reveals a complex web of intersecting stressors, traumas, and social problems seen by community members as underlying mechanisms influencing heightened levels of Aboriginal youth suicidality. Corroborating the “Indigenist” stress-coping paradigm presented by Walters and colleagues (Walters & Simoni, 2002; Walters, Simoni, & Evans-Campbell, 2002), our multilevel coding approach revealed that suicidal behavior—a phenomenon often conceptualized as individual pathology—was in fact described by community members largely as a problem with deep historical and contemporary structural roots. Our findings likewise echo Inupiat views of youth suicide as presented by Wexler (2006), in which historical perspectives of community strengths contrasted with ongoing cultural losses and contemporary manifestations of colonial assaults in terms of abuse, neglect, and substance abuse.
We were somewhat surprised to find that almost none of the focus group participants highlighted individual mental health problems as critical foundations for suicidal behaviors, in spite of direct questioning regarding why youth commit suicide (see Appendix) and a great deal of literature devoted to this issue both in majority population (e.g., World Health Organization, 2002) and Aboriginal/Indigenous-specific studies (Freedenthal & Stiffman, 2004; LeMaster et al., 2004). Despite widespread public awareness and popularity surrounding medical models of mental disorder in which individual pathology and associated behavior is understood as a “disease” caused mainly by physiological or inherited dysfunctions, the participants of these groups understood suicide from a broader, sociohistorical point of view. Structural and systemic (meso- and macro-level) problems were afforded the bulk of the blame, perhaps reflecting the keen sense of endured oppression felt and expressed by Aboriginal participants. It is also likely that a de-emphasis of individual “risk” is the result of the traditionally collectivist nature of the particular Indigenous culture included in this study. This is not to say that individualized risk factors should be altogether ignored; rather, it illustrates how adult participants in these Aboriginal communities viewed an individual behavioral construct as something inseparable from its structural and historical roots. For example, individual adolescent behaviors like alcohol abuse and emotions/cognitive states such as hopelessness were discussed, though always in the context of interpersonal relationships and/or elaboration of them as outcomes of colonization. This conceptualization was summed up nicely by one service provider (quoted earlier) and is worth restating here: These problems we have are just symptoms of our main problems, [emphasis added] I think … like we try to solve alcohol problems, sniffing, and the fighting families, you know … those are just symptoms to me. (Emphasis added)
Each set of quotations organized here by thematic focus for the sake of analysis and presentation reflects incredibly complicated layers of perspective and interpretation. For instance, throughout the focus group transcripts participants shared deeply emotional lived experiences and perceived intergenerational outcomes of residential school survival. As with Brave Heart’s (1999) findings in the United States, the lack of parental role modeling and missed traditional socialization experiences were seen as causal agents for confusion, guilt, and ineffectiveness as parents. At the same time, we heard numerous instances of adults criticizing themselves for missed opportunities to pass on traditional teachings, and similar criticism of parents as “the ones that are harming our children.” Participants eloquently expressed ways in which colonial trauma impacts individuals, families, and communities, while simultaneously bearing the burden of more proximal causes for youth suicidality. The nuanced and seemingly paradoxical depth of such perceptions may reflect the realities of how cultural loss is manifested in a contemporary state. The adults’ desire to shoulder some blame for local social problems could be viewed as a cultural strength in the form of personal and collective responsibility tied to a sense of efficacy insofar as respondents felt knowledgeable of the actions necessary for change (i.e., returning to a traditional way of life) From another vantage point, however, such self-blame could be viewed as a community’s oppression turned inward (Duran & Duran, 1995), another predicament of postcolonial life that remains in many ways veiled. As Wexler (2009) explains: “By understanding how modern colonialism cloaks Western assumptions and expectations in matter-of-fact language, young people can be helped to see how this process renders people—their people—failures” (p. 17). Without doubt, the suicide problem and its associated “risk” factors must be considered as part of “tensions created and fostered by colonization” (Wexler, 2009, p. 16).
Limitations and future research
Our goal of bringing forth Aboriginal perspectives on suicide deserves consideration of those voices not represented here. First, although important segments of the adult population (parents, aunties, uncles, etc.) were not explicit parameters for focus group membership, many of the service providers served multiple roles both as community professionals and parents, relatives, and in some cases, Elders within the reserves. Second, we did not speak directly with the Aboriginal youth on these reserves due to some community-based apprehension regarding the potential for such discussions to trigger additional suicidal thoughts. It is, of course, imperative that the voices of youth become a key source of knowledge and information when suicide prevention strategies develop within communities. Drawing from the youth-involved works of Wexler (2006, 2009) and Kral Idlout, Minore, Dyck, and Kirmayer (2011), research with younger generations may reveal an even greater degree of postcolonial problems in terms of identity confusion, perceived (limited) choices, and the struggle to “live in two worlds, yet feel … deeply rooted in neither” (Kral et al., 2011, p. 10). After several years of work and a recently funded intervention project, we are happy to report that parent and youth-based discussions are in progress and will become a vital source of information for our collaborative mental health promotion efforts on four reserves, including the three represented by these data.
Conclusion
Across the globe, Indigenous peoples suffer suicide rates of epidemic proportions. Although individual, community, and culture-specific determinants exist, a frequent explanation for these devastating losses centers around the lingering effects of shared colonized histories and genocide (Duran & Duran, 1995; King, Smith, & Gracey, 2009; Wexler, 2006). The Elders and services providers who participated in this study agreed: historical trauma represented the common thread entwined across a range of more proximal stressors and was the overwhelmingly salient and most frequently discussed theme in the data. Furthermore, and coinciding with Evans-Campbell (2008), participants identified outcomes of historically endured traumas across multiple ecological levels.
The results of this study suggest that the most effective suicide prevention and mental health promotion programs would be those that address multiple levels of risk and work to reduce exposure to stressors (Rosich & Hankin, 2010; Wight et al., 2006). Likewise, comprehensive reports on suicide prevention have recommended targeting multiple ecological contexts, including the family, community, and individual (e.g., Kirmayer et al., 2007). Similar sentiment was reflected upon by a participant who felt that the many difficult issues her community faces must be brought to the forefront before suicide can be addressed. So it’s like cleaning and mopping the floor first before you can have a clean house. You know, you have to clean up all the underlying dirty stuff before you can have a healthy community. (Female service provider)
The potential and widely recognized acute “warning signs” for suicide, such as mood changes, reckless behavior, and hopelessness (Rudd et al., 2006), although important, may in fact serve only as temporary bandages to much deeper wounds brought on in many cases by widespread and cumulative stressors. Culturally safe, competent individualized mental health services serve important functions for secondary prevention (early intervention and treatment) and tertiary or postvention suicide prevention (Kirmayer et al., 2007, p. 93) Unfortunately, an overreliance on individualized mental health care has led to what Gone (2008) has called a “cottage industry devoted to the surveillance and management of the ‘mental health’ problems of North America’s Indigenous peoples” (p. 311). This most frequently Westernized model of behavioral health dominates the industry as another form of Euro-cultural proselytization (Gone, 2008) and pathologizes individuals while ignoring any effects of cultural genocide (Duran & Duran, 1995). And, although countless culturally derived mental health interventions have been developed within Indigenous communities, few have been systematically evaluated for effectiveness and/or sustainability (Gone, 2011; Gone & Calf Looking, 2011; Whitbeck, Walls, & Welch, 2012). Recognizing these bounds, the results of this and other studies (e.g., Commission on Social Determinants of Health [CSDH], 2008; Hankin & Wright, 2010) suggest that contemporary mental health disparities like suicidality would be reduced with due consideration of the multiple levels of social determinants of health/mental health and validation of the ways in which colonial traumas intersect contemporary Indigenous ways of life.
Footnotes
Funding
This study was supported in part by a grant from the National Institute of Mental Health (MH076705), Melissa Walls, Principal Investigator.
Acknowledgements
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Mental Health or the National Institutes of Health. We graciously thank the community-based Advisory Board members for their guidance, advice, and support of this project. Special thanks to Allan Morrisseau and Calvin Bombay for their mentorship and assistance to the first author throughout data collection.
Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.