
Abstract
This study examined the association between exposure to domestic violence and dissociative symptoms. A sample of 68 Israeli opiate use disorder patients in recovery, 80 battered Arab Israeli women, and 103 respondents from a community sample participated in structured interviews that included the Dissociative Disorders Interview Schedule (DDIS), the Dissociative Trance Disorder Interview Schedule (DTDIS), and the Dissociative Experiences Scale (DES). As predicted, community participants reported significantly less exposure to traumatizing events and lower levels of dissociative psychopathology than individuals sampled from specialized treatment centers. In all, 91% of battered female participants were taxon-positive for dissociative disorder with 1 of every 2 respondents reporting symptoms corresponding to dissociative amnesia and depersonalization disorder, suggesting that this group may be particularly vulnerable to dissociative psychopathology. Extrasensory and paranormal experiences (ESP) and dissociative trance disorder experiences were strongly related to dissociative experiences and features of dissociative identity disorder (DID). These statistical associations suggest that dissociative disorders and ESP/trance experiences may share an underlying construct. Further research is needed on trauma and dissociation among female victims of domestic abuse in patriarchal, collectivist societies, particularly in the Arab world.
Dissociative phenomena have been documented in many non-Western societies where psychiatric models of dissociation are less dominant and the ethos and metaphors for illness and healing differ from those employed in the industrialized West (Boddy, 1988; Cardeña, van Duijl, Weiner, & Terhune, 2009; Ginzburg, Somer, Tamarkin, & Kramer, 2010; Somer, 1993, 1997; van Duijl, Cardeña, & de Jong, 2005; Xiao et al., 2006a, 2006b; Yu et al., 2010). In approaching research on Western psychiatric constructs in such contexts, strong arguments have been made in favor of a more interpersonal study of behavior in local worlds (e.g., Lewis-Fernández & Kleinman, 1994) and against reductionistic, decontextualized views of mental illness and the reification of mental processes (e.g., Kirmayer, 2011). The literature on mental health and multiculturalism has critiqued essentialist notions of psychopathology (Littlewood, 1991). Contemporary comparative psychiatry posits that non-Western illnesses should not be construed merely as primitive forms of universal taxonomic classes (Radwin, 1991). As a result of this less ethnocentric stance, the DSM-IV grouped illnesses unclassifiable in terms of Western psychiatry under the non-pathologizing heading of “culture-bound syndromes” (Yap, 1967, 1974), a term intended to represent a compromise between essentialist Western psychiatry and more social constructionist approaches to psychopathology (e.g., Kirmayer, 2001; Kirmayer & Sartorius, 2007). In the DSM-5, the term “culture-bound syndromes” has been discarded in favor of more nuanced approaches to recognizing the influence of culture on the experience and expression of mental illness, for example, the identification of cultural idioms of distress (American Psychiatric Association, 2013).
Many of the cultural syndromes and idioms of distress addressed in recent versions of the DSM involve dissociative phenomena, broadly defined as possession or nonpossession experiences involving sudden, time-limited alterations in identity, behavior, and mental state (Bourguignon, 1976; Cardeña et al., 2009; Huskinson, 2010; Krippner, 1997; Lewis-Fernandez, 1994; Somer, 2006; Suryani & Jensen, 1993). Examples include amok, a dissociative episode characterized by a period of brooding followed by an outburst of aggressive behavior (American Psychiatric Association, 1994; Prince, 1991); latah in Java, Indonesia (Simons, 1983), a condition characterized by an exaggerated motor startle response, often followed by hyper-suggestibility and mimicry sometimes accompanied by obscene expressions (Ward, 1989); or pibloktoq among the native people of the Arctic, an alteration of consciousness accompanied by erratic behaviors (Foulks, 1985). These and other nonpossession trance syndromes were grouped under the broader diagnosis of dissociative trance disorder in the DSM-IV (American Psychiatric Association, 1994).
To date, very little research exists on the prevalence of possession/trance phenomena (PTP), or dissociative trance disorder (DTD) and related paranormal experiences in various cultures and on their relationship to dissociative disorders. It is noteworthy, however, that the definition of possession trance offered by Cardeña et al. (2009), which includes identity alteration, made movements (a Schneiderian first rank symptom common in DID), and amnesia is similar to dissociative identity disorder (DID) symptoms. Moreover, Ross (2011) showed that trance, sleepwalking, paranormal, and possession experiences were more common among DID patients than in two comparison samples. It has been recently suggested by one research group that PTP be differentiated from similar phenomena that are culturally sanctioned and nondistressing and included under the revised umbrella category of DID in DSM-5 (Spiegel et al., 2011).
A proposed common denominator potentially linking experiences of trance, dissociation, and possession is absorption (Luhrmann, 2004). Tellegen and Atkinson (1974, p. 275) defined absorption as an “openness to absorbing and self-altering experiences.” However, absorption might not be sufficient to explain involuntary, distressful forms of (pathological) possession and is considered only one component of dissociation as measured by the Dissociative Experiences Scale (Dalenberg et al., 2012).
Several case studies have reported a relationship between exposure to precipitant stress and the development of DTD (e.g., Ferracuti & DeMarco, 2004; Somer, 1993), yet controlled studies of DTD are very sparse. Ng, Yap, Su, Lim, and Ong (2002) described a consecutive sample of 58 Chinese, Malay, and Indian patients in Singapore diagnosed as suffering from DTD following diagnostic criteria adapted from DSM-IV. Most respondents reported being possessed by Buddhist, Taoist, and Hindu deities or the Holy Spirit, with a minority reporting possession by departed relatives and ancestral spirits or animal spirits. In a later report Ng and Chan (2004) suggested that military stressors, conflicts over religious and cultural issues, and domestic conflicts had influenced the precipitation of DTD in this group. While no standardized structured instruments for the diagnosis of DTD were employed in this study, it does provide some evidence that DTD in an Asian sample was both stress-related and associated with such dissociative experiences as loss of control, altered identities, and amnesia. In another study, the newly developed Dissociative Trance Disorder Interview Schedule (DTDIS; Ross, Schroeder, & Ness, 2013) was instrumental in demonstrating that a wide range of possession experiences and classic “culture-bound syndromes” were present among predominantly Caucasian, American, English-speaking trauma program inpatients and that both possession and the syndromes were predominantly dissociative in nature.
The purpose of the present article is to report data on the frequency of possession, DTD, and dissociative disorders and the relationships between these phenomena in three Israeli samples including one nonclinical group and two clinical groups: opiate use disorder (OUD) patients and Arab female victims of domestic violence. OUD patients were recruited because opiate users are known to have a high incidence of reported childhood abuse (Somer, 2003) and a documented yearning to experience (chemical) dissociation (Somer, 2009; Somer & Avni, 2003). Arab women subjected to domestic violence were invited to take part in this study not only because of the gender discrimination and chronic traumatization this group has been exposed to, but also because we were interested in the prevalence of our target phenomena in an ethnic group known to use possession and trance as idioms of illness and healing (e.g., Lewis, 1971; Somer, 1997; Somer & Saadon, 2000).
Hypotheses
Our clinical samples will report higher levels of traumatization than our nonclinical sample. Our clinical samples will report higher levels of dissociative psychopathology than our nonclinical sample. Our clinical samples will report higher levels of possession experiences than our nonclinical sample. Dissociative Trance Disorder Interview Schedule total scores will be positively correlated with scores on standardized measures of dissociative symptoms.
Method
Participants
Sociodemographic variables of the research groups: Opiate use disorder patients, battered Arab women, and a nonclinical group in Israel.
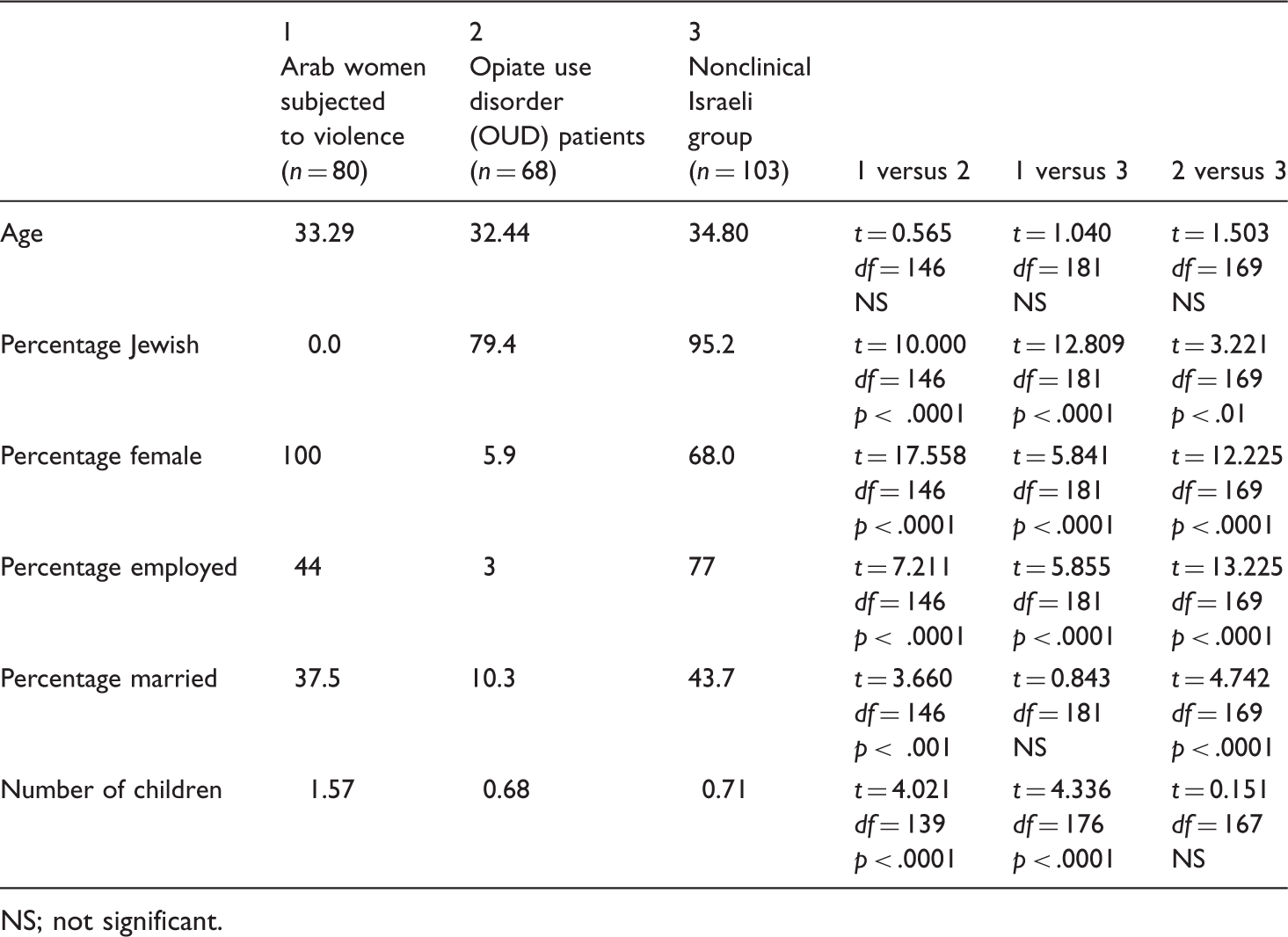
NS; not significant.
Instruments
The Dissociative Experiences Scale (DES) was developed in the United States (Bernstein & Putnam, 1986; Carlson & Putnam, 1993) and is used to measure the frequency of 28 dissociative experiences that are considered important aspects of the dissociation construct (Putnam, 1991). The instrument was shown to be a valid and reliable screening instrument (Frischholtz et al., 1990; Waller, 1995). The Hebrew translation of the DES (H-DES) demonstrated high reliability and validity (Somer, Dolgin, & Saadon, 2001).
The Dissociative Disorders Interview Schedule (DDIS) has been used in a series of research projects in North America, Turkey, and China (e.g., Ross, Duffy, & Ellason, 2002; Ross & Ellason, 2005; Ross & Halpern, 2009; Sar & Ross, 2009; Xiao et al., 2006a). It is a 131-item structured interview that inquires about a range of symptoms and DSM-IV diagnoses, as well as childhood abuse. The DDIS had good concurrent validity with the Dissociative Experiences Scale (DES; kappa = 0.81; Bernstein & Putnam, 1986), the Structured Clinical Interview for DSM-IV Dissociative Disorders (SCID-D; kappa = 0.74; Steinberg, 1995), and a clinical interview (kappa = 0.71) in an inpatient psychiatric hospital in the United States (Ross et al., 2002).
The Dissociative Trance Disorder Interview Schedule (DTDIS), a new instrument, has been used only once previously (Ross et al., 2013) and no data on its psychometric properties are available. The DTDIS gathers standardized data on possession states and related experiences including symptoms of classic culture-bound syndromes (amok, latah, bebainan, pibloktoq, and ataque de nervios). These syndromes overlap with each other and involve discrete episodes of behavioral, vocal, and emotional dyscontrol, confusion, exaggerated startle and, in the case of amok, aggressive and sometimes murderous behavior. The DTDIS has eight sections: Traditional Treatment (25 items); Identity Changes (15); Environmental Precipitants (16); Memory (7); Dissociative Trance (10); Cognition (5); Physical and Somatic Symptoms (16); and DSM-IV Dissociative Trance Disorder (6). Seven of the section scores are added together to yield a DTDIS overall score that ranges from 0 to 84. The symptom score is calculated as follows: Total score = (Traditional Treatment + Environmental Precipitants). The diagnostic criteria for the culture-bound syndromes are embedded in the seven symptom sections. The DTDIS makes DSM-IV diagnoses of dissociative trance disorder, trance subtype, dissociative trance disorder, and possession trance subtype; questions are close to verbatim transcriptions of the DSM-IV criteria.
The DDIS and the DTIS were translated into Hebrew and Arabic. The Arabic version of the DES was translated from the H-DES. Translations were done by the first author (a native Hebrew speaker) and the third and fourth authors (native Arabic speakers) and were then back-translated into English and Hebrew by native English speakers who were blind to the original English and Hebrew versions. The back-translations were compared to the original versions and differences were reconciled.
Data analyses
For the 261 participants, average DES total scores and the numbers of participants in the DES-taxon (DES-T; Waller, Putnam, & Carlson, 1996) were calculated. For the DDIS, average section scores were calculated including Schneiderian symptoms, somatic symptoms, DSM-IV borderline personality disorder criteria, secondary features of DID, and ESP/paranormal experiences; in addition, the numbers of participants positive for the five dissociative disorders were tabulated, as was the average number of dissociative disorders positive. For the DTDIS, the average section scores and overall scores were calculated. In addition, the number of participants responding “Yes” to individual items was tabulated, as was the number of participants meeting criteria for dissociative trance disorder.
For the demographic variables shown in Table 1, groups were compared to each other using t tests for continuous variables and chi squares for dichotomous variables. An analysis of covariance was conducted on the DES, DDIS, and DTDIS results with gender, age, being married, and being separated entered as covariates. Each of the individual groups was compared to the other two using two-tailed t tests; for these comparisons, each group was compared separately to the other two. We applied the Bonferroni correction for multiple comparisons was applied (Dunn, 1961), resulting in a corrected significance level of p < .001. This was done in order to avoid Type 1 errors, due to the large number of comparisons. Additionally, these variables were entered into a Pearson correlation matrix. After a Bonferroni correction, significance for these correlations was p < .001.
Results
Trauma histories among opiate use disorder patients, battered Arab women, and a nonclinical group in Israel.
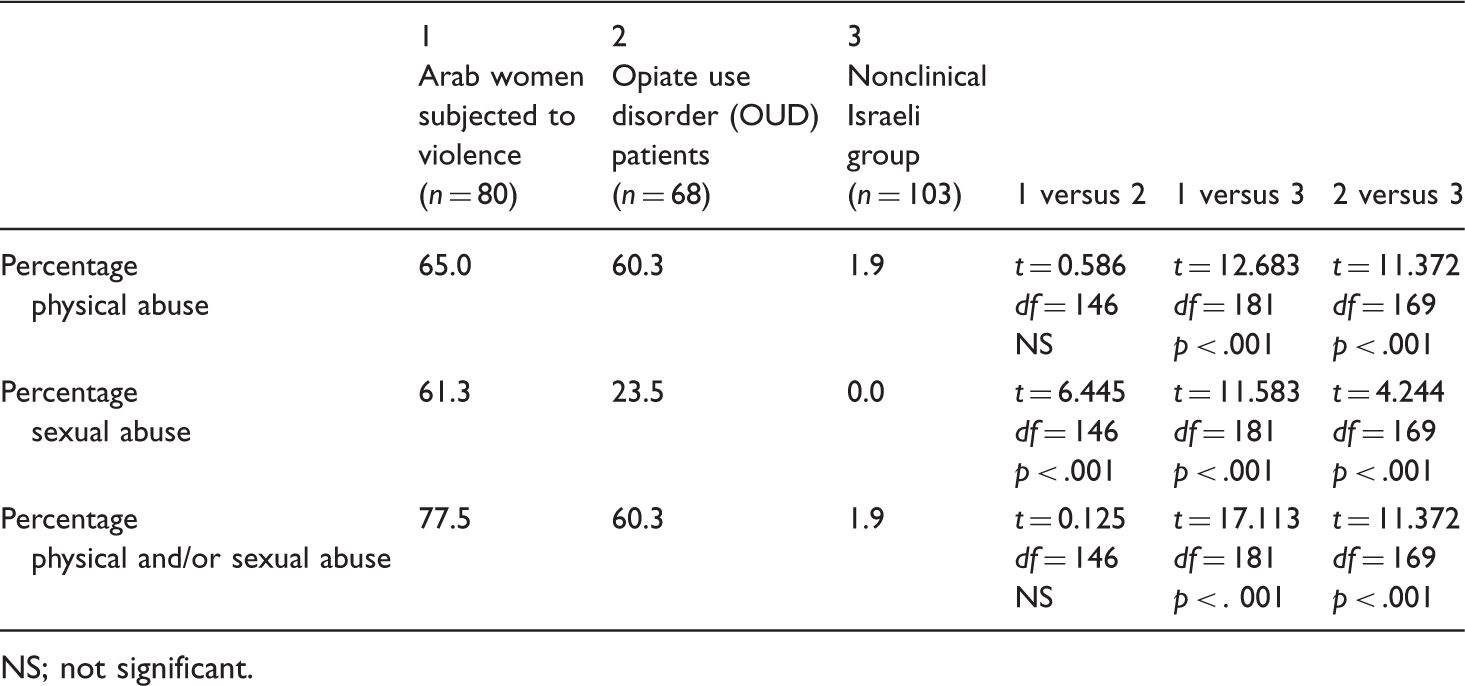
NS; not significant.
While our two clinical samples reported similar levels of exposure to physical abuse, Arab women subjected to domestic violence were 2.6 times more likely to report a history of sexual abuse than recovering OUD patients, a group that has repeatedly shown extensive levels of trauma exposure (e.g., Somer & Avni, 2003; Somer, Altus, & Ginzburg, 2010).
Dissociative symptoms and disorders in opiate use disorder patients, battered Arab women, and a nonclinical group in Israel (life-time).
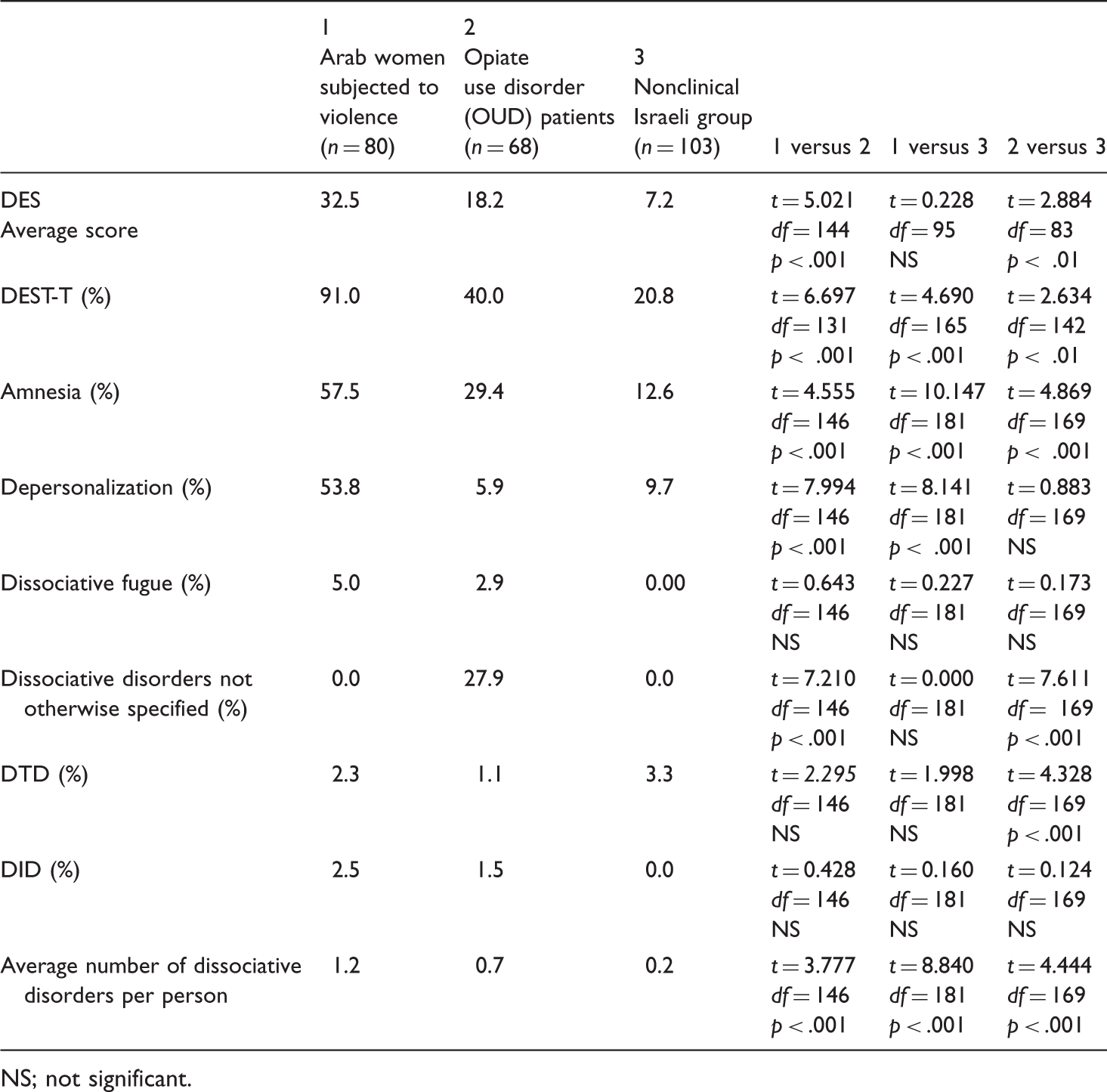
NS; not significant.
Reported possession experiences in opiate use disorder patients, battered Arab women, and a nonclinical group in Israel (percent positive, life-time).
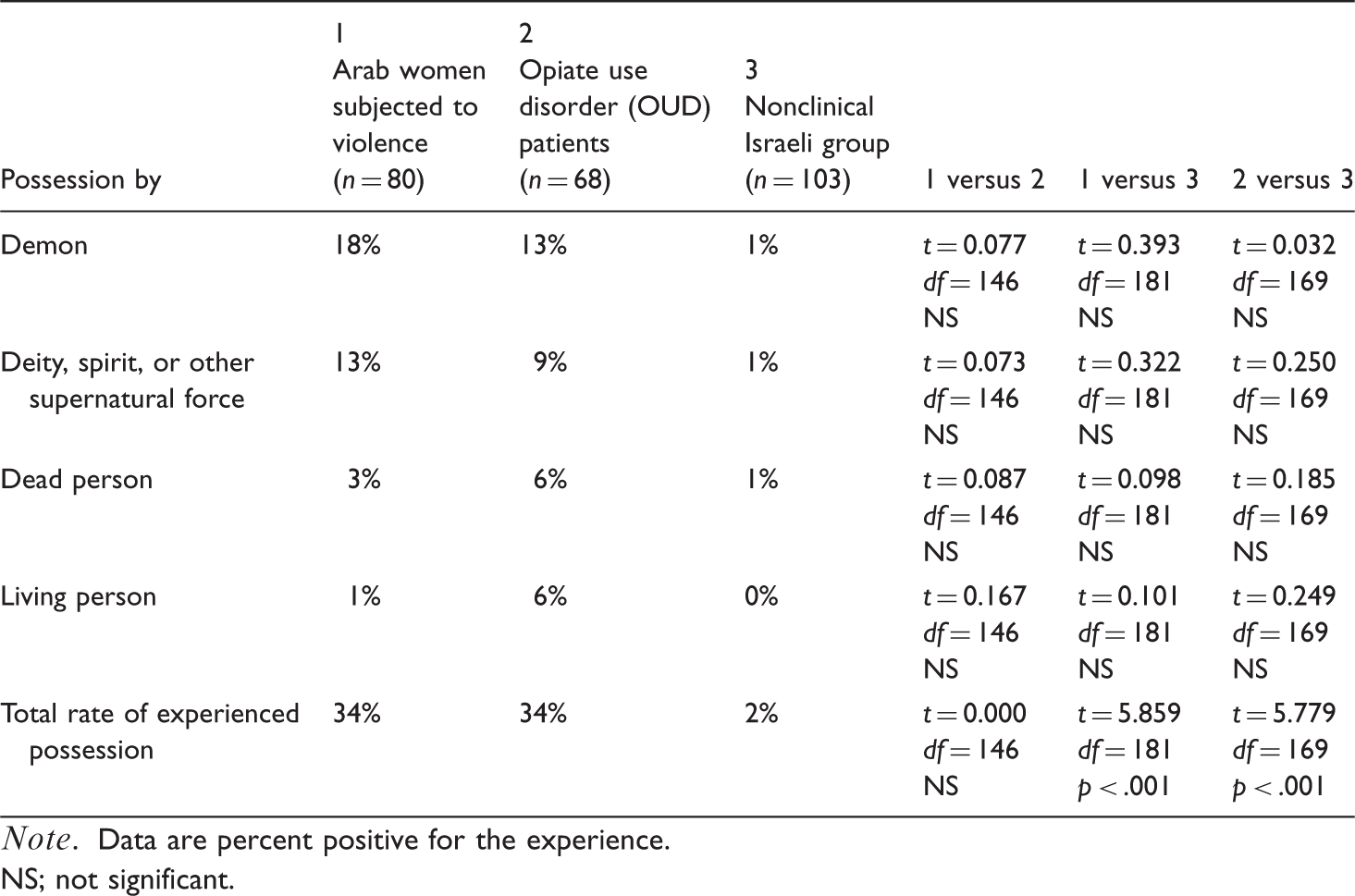
Note. Data are percent positive for the experience.
NS; not significant.
Pearson correlation matrix for key DDIS and DTDIS variables among all research respondents.

Note. Significance level: * = correlation significant at p < .001; DTDIS = Dissociative Trance Disorder Interview Schedule total score; DES = Dissociative Experiences Scale; 20 DID = secondary features of dissociative identity disorder; Somatic = somatic symptoms; Schneiderian = Schneiderian first rank symptoms; BPD = borderline personality disorder; ESP = extrasensory and paranormal experiences; Trauma = total trauma score on DDIS.
The DDIS total trauma score was only mildly related to the likelihood of reporting extrasensory and paranormal experiences and was not associated with our Dissociative Trance Disorder Interview Schedule total score, as shown in Table 5. Statistical information for the significant findings is included in the tables.
Discussion
The results were consistent with our hypotheses. First, Israeli community participants reported significantly less exposure to traumatizing events than responding individuals sampled from specialized treatment centers. The reported trauma levels of the Israeli community sample were lower than those measured in comparable samples in North America (Briere & Elliot, 2003; MacMillan et al., 1997) and in line with a previous comparison of Israeli and American respondents (Lauterbach, Somer, Dell, & Vondeylen, 2008). Second, our clinical samples reported higher levels of dissociative psychopathology than our community sample. In fact, the average DES score among Arab women subjected to domestic violence exceeded the commonly accepted cut-off score of 30, a suggested boundary between normal and abnormal dissociation (Carlson & Putnam, 1993). Fully, 91% of the Arab participants were taxon-positive for dissociative disorder (Waller et al., 1996), with 1 of every 2 respondents reporting symptoms corresponding to dissociative amnesia and depersonalization disorder, suggesting that this group may be particularly vulnerable to dissociative psychopathology. To the best of our knowledge, no systematic studies on dissociative psychopathology in Arab samples have been published. In line with interpretations offered by Boddy (1988) concerning phenomena of spirit possession among Muslim Sudanese women, we propose that some abused women in conservative, male-dominated cultures, such as the one we sampled from, use dissociation as a coping strategy to manage painful memories, threatening environments, and aching bodies.
Other studies in traditional societies have shown how sanctioned paranormal and possession experiences may allow the “ventilation” of distress via “non-me” agents and permit communal healing rituals that do not involve any explicit verbal expression of psychological distress (Somer, 1993, 1997, 2006; Somer & Saadon, 2000).
Recently, a wide range of possession experiences and exorcism rituals, as well as culture-bound syndromes listed in the DSM-IV, were identified in an American clinical sample (Ross et al., 2013). Consequently, we predicted that our clinical samples would report higher levels of possession experiences than our nonclinical sample. While only 2% of our community sample reported having had a possession experience, 34% of our clinical respondents endorsed items describing possession experiences, thus substantiating our third hypothesis. This trend appeared to transcend ethnicity, as rates of reported possession experience were identical both in the mostly Jewish and the purely Arab Israeli samples. These data indicate that possession may not be “culture-bound,” as Ross et al. (2013) have already suggested.
To explore the assumption that paranormal and possession phenomena (as measured by the DTDIS) are dissociative in nature, we tested the hypothesis that DTDIS total scores would be positively correlated with scores on standardized measures of dissociative symptoms. The data we collected supported this fourth prediction. However, our data also showed that extrasensory and paranormal (ESP) experiences and dissociative trance disorder experiences were strongly related to dissociative experiences, secondary features of DID, and symptoms of borderline personality disorder, as well as to Schneiderian first rank and somatic symptoms. These statistical associations suggest that dissociative disorders and ESP/trance experiences may share a common underlying construct that is not associated with trauma, as trauma appeared to correlate with dissociation but not ESP. Our data are in line with findings by Ross (2011) who recently reported that patients with DID in North America disclose paranormal, trance, and possession experiences much more frequently than those in control samples. Our results diverge, however, from arguments presented by Targ, Schlitz, and Irwin (2000) who reviewed evidence showing that psi-related phenomena (PRE) had been reported by up to 67% of community respondents. Different definitions and measures of ESP/PRE may account for some of these discrepancies.
Contrary to our expectations, total trauma score was only mildly related to the likelihood of reporting paranormal experiences and was not associated with the Dissociative Trance Disorder Interview Schedule total score in our data set. One possible explanation for this outcome is that trauma, as measured by our instruments, is not the only pathway to the phenomena gauged in this study. For example, ESP and possession trance could represent broader idioms of distress or alternative forms of spiritual experience.
There are several important limitations of this study. First, although our research groups were similar in age, sampling and sociodemographic differences complicate the interpretation of some of our comparative findings. Beyond the obvious ethnic differences between the Arab women and the other groups, additional differences were, arguably, not accounted for among Jewish participants. For example, while both Arabs and Jews were represented in the OUD sample, among Jewish members of this group there were more participants from a Mizrahi (Sephardi) background. Future research should attempt to identify the contribution of Arab ethnicity to the explained variance by sampling a nonclinical female Arab sample. Second, our clinical groups were fairly small and not representative of the majority of the treated populations. Our conversations with individuals belonging to the 48% of Arab women who declined our invitation to participate in the study revealed lingering concerns about confidentiality and fear of reprisal for tarnishing “family honor” by talking to members of the research team. It is conceivable that the troubling psychological outcomes documented among Arab women subjected to domestic violence would have actually been much worse had we had a higher response rate. Third, although literacy level was not measured in this study, many members of our clinical samples, particularly the Arab respondents, were unaccustomed to responding to psychological questionnaires and found some of the wording difficult to understand. While the research instruments were written in literary Arabic, the interviewers had to translate many of the items into spoken Arabic (which is not a written language). This seemed to enhance the respondents' understanding of our questions, but it also represented a deviation from our strict translation protocol. Lastly, the psychometric properties of the DTDIS, a new instrument, are yet to be established. Further research with the DTDIS should be conducted in a wide range of cultures, languages, and population samples including both clinical and nonclinical groups. Future research on trauma and dissociation among female victims of domestic abuse in patriarchal, collectivist societies is also warranted.
Footnotes
Acknowledgements
We wish to thank Goor Somer and Merav Lapid for their assistance with data collection.