
Abstract
Few studies have examined the association between childhood maltreatment (CM) and personality disorders (PDs) in adulthood in two different cultural contexts, including sub-Saharan Africa. The aims of this study were to compare the frequency of CM between patients in treatment in France and Togo for a major depressive disorder (MDD), to explore the link between CM and PDs, and to examine the mediating effect of personality dimensions in the pathway from CM to PDs in 150 participants (75 in each country). The 28-item Childhood Trauma Questionnaire, the International Personality Item Pool, and the Personality Diagnostic Questionnaire (PDQ-4+) were used to assess CM, personality dimensions, and PDs respectively. Togolese participants reported sexual and physical abuse (PA) and emotional and physical neglect significantly more frequently than French participants. In Togo, severe PA was associated with schizoid, antisocial, narcissistic, obsessive-compulsive, depressive, and negativist PDs whereas in France, PA was only linked to paranoid PD. In Togo, emotional instability partly mediated the relationship between CM and PDs while in France, no personality dimension appeared to mediate this link. Our results support the hypothesis that CM is more common in low-income countries and suggest that the links between CM and PDs are influenced by social environment.
Introduction
Childhood maltreatment (CM) is associated with personality disorders (PDs) in adulthood (Grover et al., 2007; Sansone, Lam, & Wiederman, 2010; Tyrka, Wyche, Kelly, Price, & Carpenter, 2009). Childhood abuse and neglect are significantly linked to clusters A, B, and C of PDs in the general population as well as in samples of psychiatric patients (Afifi et al., 2011; Zhang, Chow, Wang, Dai, & Xiao, 2012). Childhood adversities are also linked to personality dimensions. More specifically, CM is linked to high scores of neuroticism (Allen & Lauterbach, 2007; McFarlane et al., 2005; Rogosch & Cicchetti, 2004) and to low scores of agreeableness, conscientiousness and extraversion dimensions (Tani, Greenman, Schneider, & Fregoso, 2003).
Most studies examining the relationships between childhood adversities and personality dimensions or between CM and PDs in adulthood have been performed in the West or in developed countries. Little research exploring the link between CM and PDs has been done in Africa. Research on this subject in sub-Saharan Africa has been carried out in English-speaking countries and has mainly explored the associations between CM and mood, anxiety, or addictive disorders (Benjet, 2010; Jewkes, Dunkle, Nduna, Jama, & Puren, 2010; Oladeji, Makanjuola, & Gureje, 2010). To the best of our knowledge, there has been no study examining the links between CM and PD in sub-Saharan Africa countries, including Togo.
Very little research has examined how specific environmental factors shape the influence of CM on the development of psychopathology in adulthood. The frequency of childhood adversities and their consequences in adulthood may differ according to environmental contexts. A few studies have been carried out between countries in Europe and sub-Saharan Africa and have shown higher levels of childhood trauma among African patients (Lochner et al., 2010). The Lochner et al. study, for example, concerned South African and Swedish patients with social anxiety and panic disorders. South African patients reported childhood trauma, in particular sexual abuse and emotional and physical neglect, significantly more often than their Swedish counterparts.
More recently, Beiser et al. (2012) compared levels and predictors of emotional problems among preadolescent Ethiopians in Addis Ababa and Toronto and found differences depending on the country of residence. Parental perceptions of prejudice were predictors of emotional problems in Ethiopia, but not Canada, and parent–child discordance regarding ethnic adherence predicted self-rated emotional problems in Addis Ababa, but not in Toronto. Another comparative study by Rossier, Rigozzi, and the Personality Across Culture Research Group (2008) described the link between PDs and a dimensional model of normal personality traits (Five-Factor Model) in two different cultural settings. The participants of the study comprised a large nonclinical sample from Switzerland and nine French-speaking African countries: Algeria, Tunisia, Benin, Burkina-Faso, Mali, Senegal, Democratic Republic of Congo, Republic of Congo, and Mauritius. Rossier et al. found that correlations between PDs and the domains of the Five-Factor Model were similar in both samples (Switzerland and French-speaking African countries). They concluded that the association between PDs and the Five-Factor Model was stable in two samples separated by a great cultural distance. However, this research concerned a nonclinical sample and did not account for CM in the examination of the link between PDs and the domains of the Five-Factor Model. Further research on the relationship between PDs and personality traits in a clinical sample could be warranted.
Previous studies have reported that cultural differences exist in the perception and interpretation of traumatic experiences and the expression of responses to traumatic events (Hinton & Kirmayer, 2013; Seedat, Nyamai, Njenga, Vythilingum, & Stein, 2004). Thus, we decided to conduct the present study in order to verify if the consequences of childhood maltreatment for adult personality would be the same in French and Togolese samples.
Nederlof, van der Ham, Dingermans, and Oei (2010) found that CM types are differently associated with personality dimensions and with personality pathology and they concluded that these differences are probably due to specific gene–environment interactions. Although findings of several other studies have suggested that environmental factors, CM, and personality dimensions are related to PDs in adulthood, very few studies have simultaneously examined the associations between CM, personality dimensions, and PDs in two different cultural contexts or in French-speaking sub-Saharan African countries, where no research exploring the link between CM and PDs has been carried out to date, as far as we are aware. This research was undertaken to fill the gap in the existing literature.
The aim of our study was to compare rates of CM in patients treated for major depressive disorder (MDD) in France and in Togo, in order to explore the relationships between CM, personality dimensions, and PDs, and to examine the mediating effect of personality dimensions in the pathway from CM to PDs in each country. Our hypotheses were the following: (a) Togolese patients will report CM more frequently than their French counterparts; (b) Physical abuse will be associated with PDs in both countries; and (c) The pathway from CM to PDs will differ between French and Togolese samples.
Method
Participants
This paper describes a cross-sectional study carried out in France and in Togo with patients being treated for MDD. The choice of a depressed clinical sample is explained by the fact that depression is a major public health problem in France and one of the main reasons for seeking psychiatric care in Togo. In France, data were collected from December 2010 to October 2011 in the following psychiatric services: the Psychiatric and Medical Psychology Service and Brief Therapy Center of Toulouse University Hospital Center (CHU), and the Aufréry Clinic located in Balma. In Togo, the study took place from March to October 2010. Data were collected in the Psychiatric and Medical Psychology Clinic of the two CHUs of Lomé, at the Mental Health Center of Agoe (a northern suburb of Lomé), and at the National Mental Health Center, which is the only psychiatric hospital in Togo. Inclusion criteria were: French-speaking, and between 18 and 65 years old. Prior history of psychotic disorders, bipolar affective disorder, or mental retardation was exclusionary. All participants gave informed consent for the study.
In France, of the 92 eligible patients using these services, 75 (81.5%) participated in the study. Seventeen patients (18.5%) refused to participate in the research for various reasons including, most commonly: they (the patients) were not interested (n = 10), they no longer wanted to recall their painful childhood experiences (n = 3), they believed that they would receive no personal benefit from participating in the study or they had no time (n = 4).
In Togo, 75 (93.7%) of the 80 eligible patients were included. Three patients refused to participate in the study as they were not interested whereas the other two explained their refusal by the fact that they had lived a painful childhood and did not want to talk about it.
Procedure
In all the care centers where participants were recruited, staff psychiatrists provided us with a list of eligible patients who were being treated for MDD according to the DSM-IV criteria. First, the eligible patients were visited to introduce the study to them. Then they were given an information notice, which contained all study details. Within a reasonable time frame (between a few hours to a few days, depending on the patient), the patients were revisited to obtain their consent. After collecting the patient’s signed informed consent forms, we agreed on an appointment for assessments of approximately 40 to 90 minutes.
This research procedure was approved by the Ethics Committee of CHU Campus of Lomé and written informed consent was obtained from all the participants.
Instruments
The 28-item Childhood Trauma Questionnaire (CTQ; Bernstein & Fink, 1998; Bernstein et al., 2003) was used to evaluate five types of CM: emotional abuse (EA), physical abuse (PA), sexual abuse (SA), emotional neglect (EN), and physical neglect (PN). The items of the CTQ are rated on a 5-point Likert scale with responses ranging from 1 (“never true”) to 5 (“very often true”). The score for each type of CM (composed of five items) varies from 5 to 25, providing a quantitative index of the severity of CM. A high score for any CTQ type reflects severe childhood maltreatment. According to the score of each subscale and the cut-off point specified in the CTQ manual, results for every CM type can be dichotomized as either having or not having experienced severe abuse/neglect. We used the French validated short form of the CTQ (Paquette, Laporte, Bigras, & Zoccolillo, 2004) for the assessment of all participants. French is the official language in Togo and all Togolese participants spoke French.
The CTQ was adapted to the local context of Togo before use. To adapt the CTQ, in collaboration with the “Psychology Laboratory” of the National Institute of Educational Sciences – University of Lomé (Togo), we changed some items slightly. For instance, in Item 26, we added expressions to reflect Togolese contextual realities; the original item “There was someone to take me to the doctor if I needed it” became “There was someone to take me to the doctor, the clergyman, the traditional healer, or the marabout if I needed it.” We decided to add these expressions to the item, which assesses physical neglect, in order to better represent the reality of medical pluralism in sub-Saharan African. For this study, in France, alpha coefficients were .81 (EA), .76 (PA), .85 (SA), .82 (EN), and .67 (PN). In the Togolese group, alpha coefficients were .68 (EA), .73 (PA), .70 (SA), .76 (EN), and .64 (PN).
The Personality Diagnostic Questionnaire (PDQ-4+; Hyler, 1994) was used to assess PDs. The PDQ-4+ is a self-report questionnaire, composed of 107 true/false items, that screens for 12 Axis II DSM-IV PDs. The overall score of PDQ-4+ is calculated by adding pathological answers and gives a general index of personality disturbance. The higher the score of PDQ-4+, the greater the probability of the existence of a personality disorder. In the current study, the PDQ-4+ alpha coefficients were .81 in both the French and the Togolese samples. In the French group, alpha coefficients were .73 (Cluster A PDs), .78 (Cluster B PDs), and .58 (Cluster C PDs) whereas in Togo, they were .63 (Cluster A PDs), .71 (Cluster B PDs), and .72 (Cluster C PDs). More specifically, alpha coefficients for the 12 PDs in France ranged from .61 (borderline) to .79 (dependent). In Togo, alpha coefficients ranged from .58 (negativist) to .76 (avoidant).
The International Personality Item Pool (IPIP-50; Goldberg, 1999) was used to assess personality dimensions. The IPIP-50 is concordant with the Five-Factor Model and assesses five dimensions: agreeableness, conscientiousness, extraversion, intellect (openness to experiences), and emotional stability (neuroticism). The IPIP-50 comprises 50 items. It is a Likert-type scale with five possible responses ranging from “strongly disagree” (1) to “strongly agree” (5). Each personality dimension is calculated as the sum of 10 items. A high score indicates a significant presence of this dimension. In the French sample of our study, alpha coefficients were .72 (extraversion), .78 (agreeableness), .69 (conscientiousness), .90 (neuroticism), and .72 (openness). For the Togolese group, alpha coefficients were .66 (extraversion), .70 (agreeableness), .68 (conscientiousness), .95 (neuroticism), and .67 (openness).
Statistical analyses
The χ2 test and the Fisher’s exact test enabled the comparison of categorical variables (gender, professional status, severity of CM, etc.) between the two groups and the examination of associations between the severity of different types of CM and PDs. Pearson’s correlation analyses were performed to examine the association between the independent variables (types of CM) and the dependent variables (symptoms of PDs, score of personality dimensions).
Mediation analyses were performed in order to evaluate the potential mediating effect of personality dimensions between CM and PDs (score of PDQ-4+). These were conducted using the bootstrapping resampling procedure (Preacher & Hayes, 2008), entering the CM (total score of the CTQ) as an independent variable, the PDs (score of PDQ-4+) as a dependent variable, and the personality dimensions as mediation variables. Gender, age, and prior history of severe somatic pathology were controlled for in these analyses. We also adjusted for severe somatic pathology because previous research reported interaction between medical illness and personality disorders (Douzenis, Tsopelas, & Tzeferakos, 2012). For all the mediation analyses, 1,000 samples were generated and the indirect effects were calculated to get a 95% confidence interval corrected for the estimation bias.
Statistical analyses were performed with the software SPSS 18.0. For all statistical analyses, the significance threshold was .05.
Results
Sociodemographic characteristics
Sociodemographic characteristics and childhood maltreatment (CM) frequency in all participants (N = 150): Patients in France versus Togo.
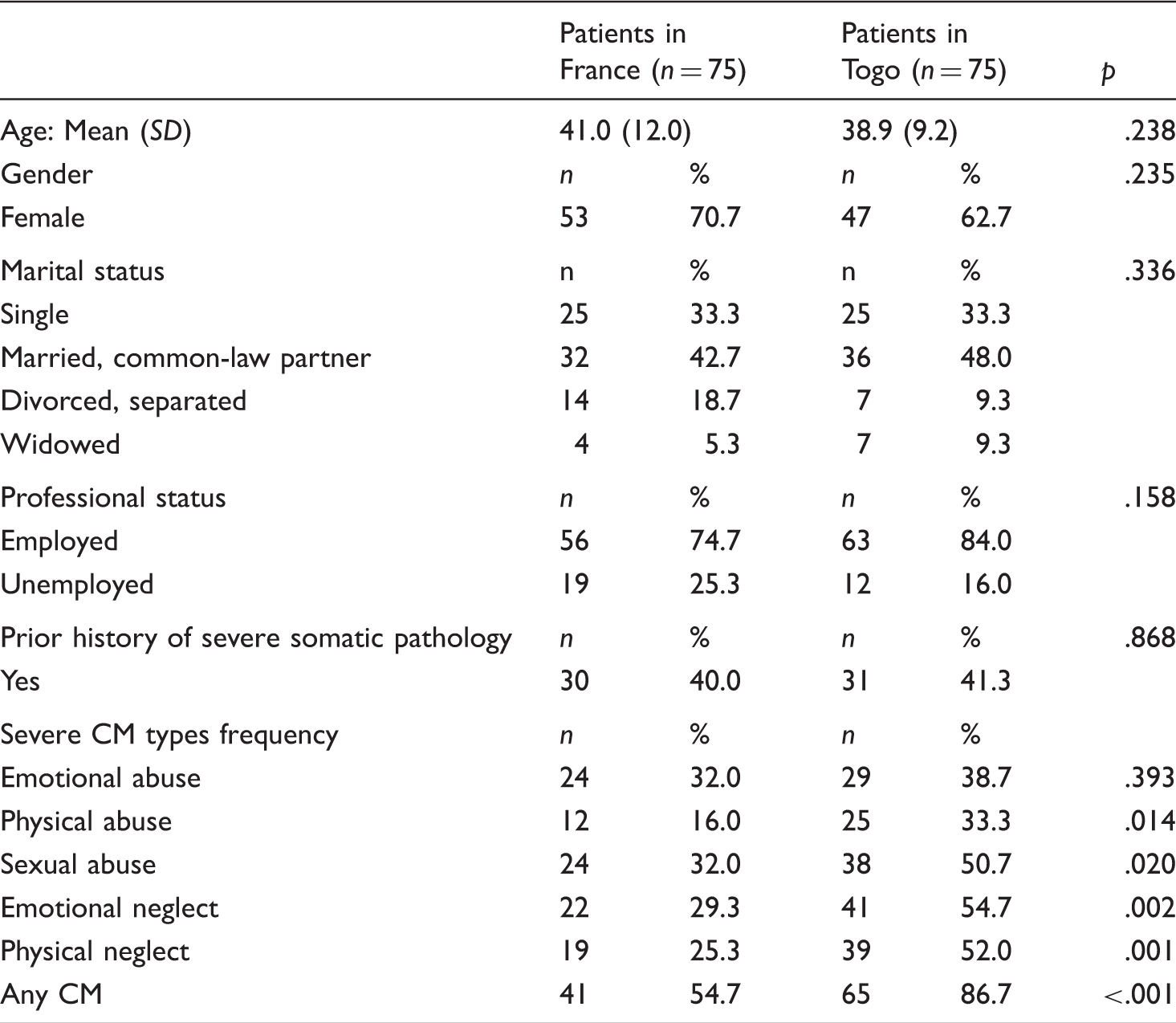
Togolese patients endorsed all types of severe CM significantly more frequently than their French counterparts except for emotional abuse, for which p > .05.
Association between childhood maltreatment and personality disorders
Association between severe CM and PDs in each country (χ2 and Fisher exact test).
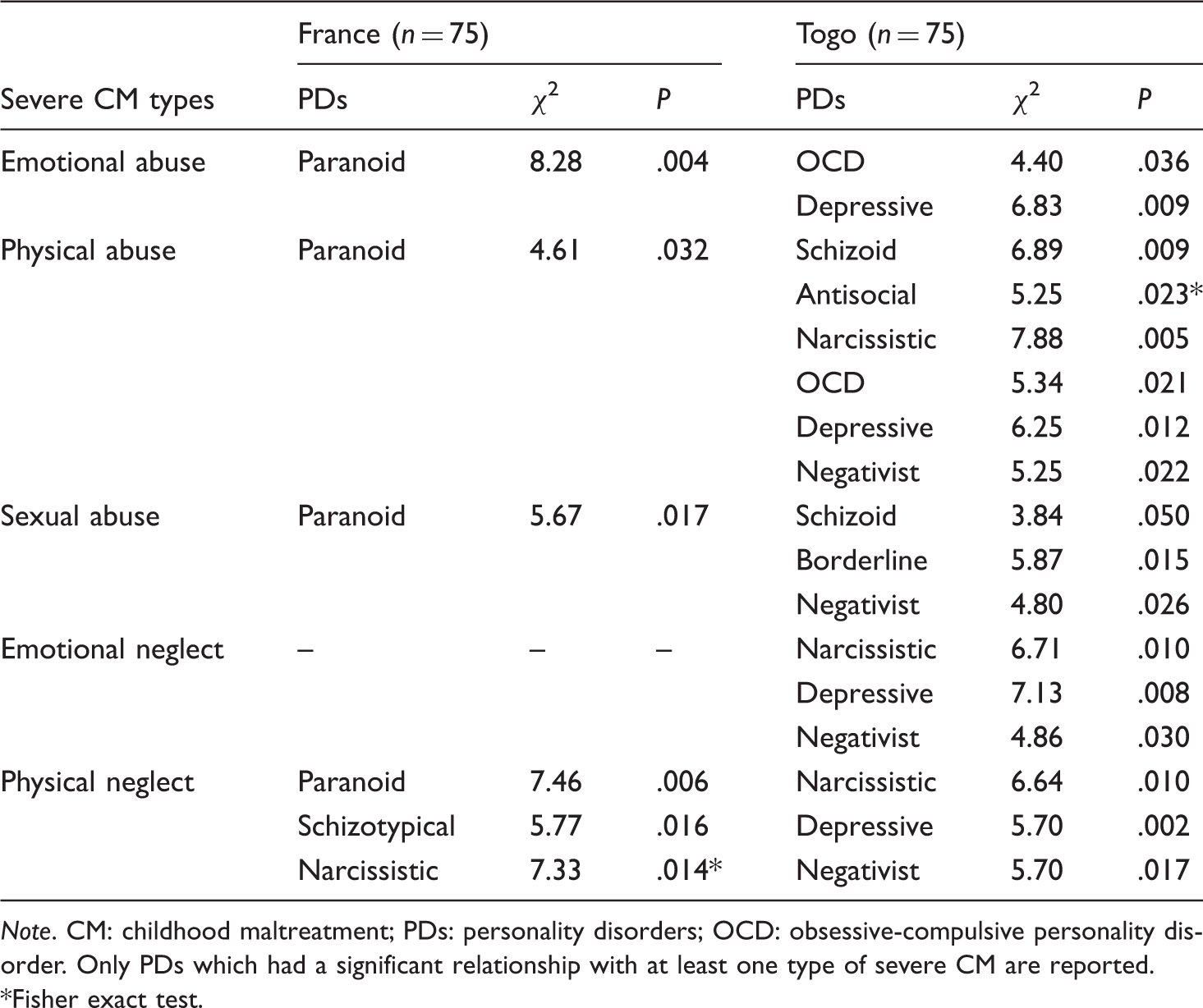
Note. CM: childhood maltreatment; PDs: personality disorders; OCD: obsessive-compulsive personality disorder. Only PDs which had a significant relationship with at least one type of severe CM are reported.
Fisher exact test.
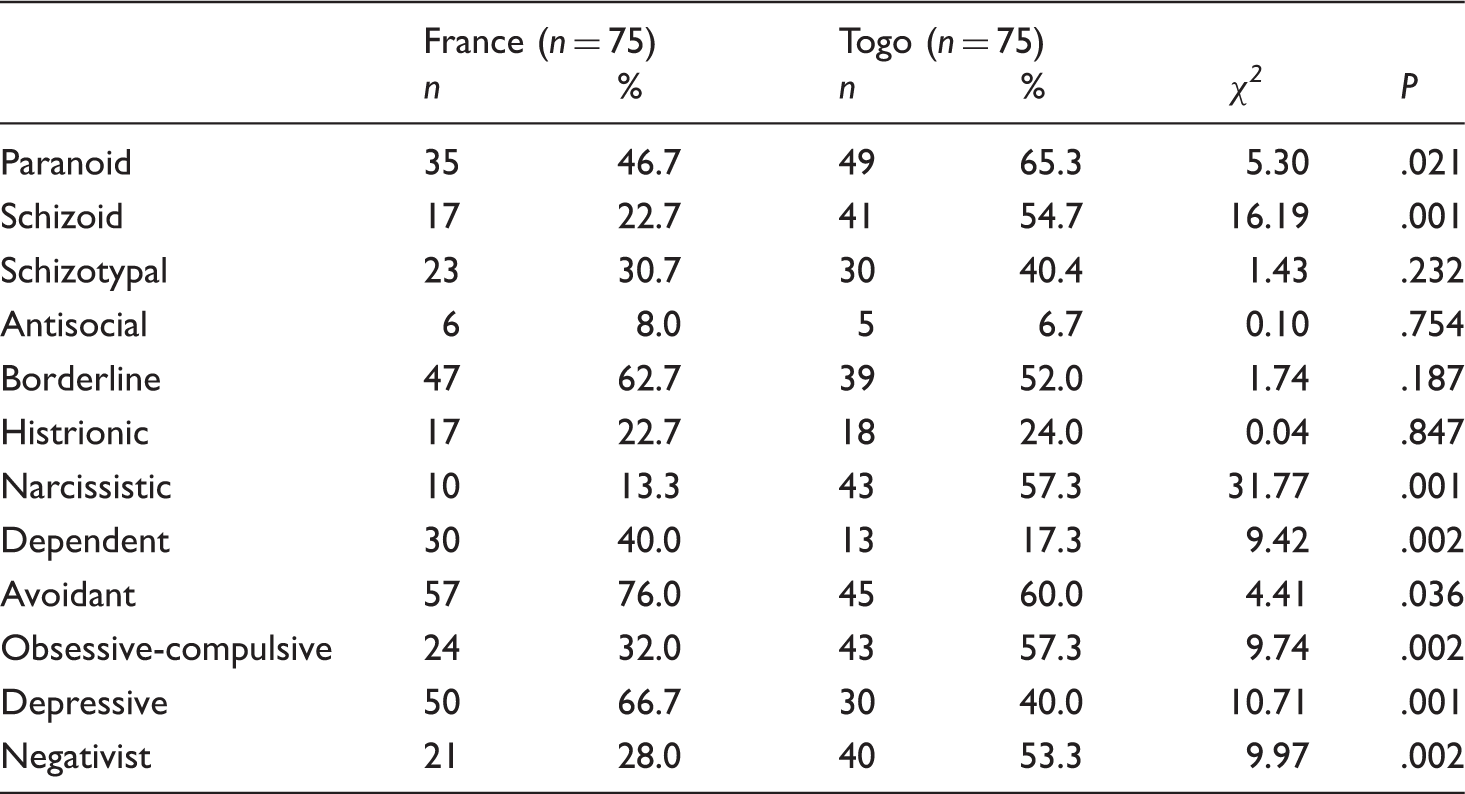
Comparison of personality disorders (probable presence) between French and Togolese patients.
The correlation analyses performed independently in each country showed that in France, EA, SA, and PN were positively correlated with Cluster A PDs symptoms, respectively (r = .252, p < .05), (r = .304, p < .01), and (r = .248, p < .05). Emotional stability was negatively correlated with the three clusters of PDs symptoms. The Pearson correlations were (r = −.378, p < .01) with Cluster A PDs symptoms, (r = −.368, p < .01) with Cluster B PDs symptoms and (r = −.514, p < .01) with Cluster C PDs symptoms.
In Togo, severe PA was associated with PDs of all the three clusters. EA was positively associated with Clusters A, B, and C PDs symptoms, respectively (r = .326, p < .01), (r = .318, p < .01), (r = .317, p < .01), and with openness (r = .230, p < .05), and negatively linked to emotional stability (r = −.312, p < .01). PA was significantly linked to Clusters A (r = .288, p < .05) and B (r = .429, p < .01) PDs symptoms. SA was positively linked to Cluster B PDs symptoms (r = .315, p < .01) and negatively linked with conscientiousness (r = −.245, p < .05). EN was positively correlated with Cluster B PDs (r = .314, p < .01) and with openness (r = .236, p < .05), and negatively associated with emotional stability (r = −.296, p < .01). Emotional stability was negatively associated with Clusters A (r = −.443, p < .01), B (r = −.324, p < .01), and C (r = −.366, p < .01) PDs symptoms.
When controlling for other types of CM, in the Togolese group, a positive relationship was found between EA and paranoid (r = .239, p < .05), borderline (r = .233, p < .05), and obsessive-compulsive (r = .342, p < .01) PDs. In the French sample, after adjusting for other types of CM, schizoid PD was positively correlated with SA (r = .313, p < .01). Controlling for other forms of CM, in the Togolese group, a positive association was found between PA and narcissistic PD (r = .244, p < .05), antisocial PD (r = .298, p < .05), and obsessive-compulsive PD (r = .275, p < .05) whereas in the French group, the relationship between PA and specific PDs was not significant.
Because CM was related to PDs in both countries, we decided to examine the pathway of CM to PDs in each group.
Pathway of childhood maltreatment to personality disorders
In Togo, the results of the mediation analyses suggest that the five personality dimensions together significantly mediate the link between CM and PDs, (c = .44, p < .0001; c = .28, p < .01; B(SE) = .16(.066), 95% CI [0.032, 0.300]). Nevertheless, the study of specific mediating effects showed that among the five dimensions, only low emotional stability (i.e., emotional instability) contributed to the mediating relationship, a = −.68, p < .05; b = −.16, p < .001; B(SE) = .11(.051) 95% CI [0.024, 0.227]; see Figure 1.
Relationship between childhood maltreatment and personality disorders (PDQ-4+ score) as mediated by personality dimensions in Togolese group (N = 75).
In France, no personality dimension was found to mediate the link between CM and PDs (Figure 2).
Relationship between childhood maltreatment and personality disorders (PDQ-4+ score) as mediated by personality dimensions in French group (N = 75).
Discussion
This study is one of the first to examine the associations between CM and PDs in two different sociocultural contexts, including a sub-Saharan African French-speaking country, simultaneously. To our knowledge, this is also one of the rare studies exploring the relationship between CM and PDs in adulthood in sub-Saharan Africa, and particularly in Togo. The main results of this study suggest that CM (specifically PA and SA) is linked to Cluster A PDs symptoms, and that emotional instability is linked to Clusters A, B, and C PDs symptoms in both France and Togo. These findings are in line with previous research carried out in the West (Nederlof et al., 2010; Tyrka et al., 2009) and partly confirm the results of our last study, in which EA and SA significantly predicted the PDQ-4+ score in Togo (Kounou et al., 2013). More specifically, in our previous study, only SA and EA contributed significantly to the prediction of the PDQ-4+ score. The difference between findings of our current study and these previous findings may be explained by the homogeneity of our present sample compared with our first study that included patients with MDD and healthy controls without psychiatric history. Overall, our study supports a cross-cultural relationship between PDs and child maltreatment. The pathway from CM to PDs may be partly explained by personality dimensions in Togo whereas in France this mediating effect does not exist.
Childhood maltreatment is widespread in many societies and different cultural contexts across the world. We used CTQ to assess CM, as did a previous study (Lochner et al., 2010) comparing childhood maltreatment between a high-income country (Sweden) and a low-income country (South Africa). Our findings suggest that Togolese MDD patients have experienced more CM than patients treated in France. In fact, more than 80% of patients in Togo reported at least one type of severe CM, as opposed to just over half of their counterparts in France. More specifically, PA and PN frequencies were twice as high among Togolese patients than French patients. These high rates of CM in Togo may be partly explained by cultural socioeducative practices such as painful ritual practices (scarification), female genital mutilations in some communities, and disrespect of children’s rights. Overall, the high CM levels in psychiatric patients in Togo seemed to be normative and confirmed findings of other studies (Mbagaya, 2010). Table 3 shows high likely existence of PDs among all participants. We found that Togolese patients reported paranoid, schizoid, narcissistic, obsessive-compulsive, and negativist PDs symptoms more than their French counterparts. These results are in accordance with those of Rossier et al. (2008) who found that PDs scores for African populations were systematically higher than the scores observed in Switzerland. The differences between French and Togolese participants in our study may be partly explained by the use of a questionnaire for the assessment of PDs. We hypothesize that these differences may also arise from divergent conceptualizations of the structure of personality in sub-Saharan Africa and the West. Sow (1977) hypothesized that the construction of personality is approached differently in Africa than in Western countries. He proposed that African individuals are conceived of as the fruits of their family circles and ancestors, whereas the Western individual is viewed as the result of their parent’s education. In sub-Saharan Africa, the individual personality is the construct of two axes, a horizontal axis (society, community, and parents) and a vertical axis (ancestors; Sow, 1977), while in the West, it is the triad (father–mother–child) that is emphasized. Differences in results may also be explained by the fact that in the relatively collectivist culture of Togo, behaviors and responses to questionnaire items may be determined more by social context than by consistent individual traits (Rossier, Dahourou, & McCrae, 2005).
Child maltreatment was associated with more features of PDs in Togo than in France. This result could be explained in part by the harsh economic and social conditions in which children are raised in this low-income country, including exposure to child labor in difficult conditions and without legal protection, poverty, and the violent sociopolitical crises Togo has experienced in the past two decades. Benjet (2010) has found that child labor, family violence, poverty, and discrimination are risk factors leading to poor mental health in sub-Saharan African countries that have experienced armed conflicts (Sierra Leone, Uganda, Democratic Republic of Congo, and Rwanda). Thus, given these environmental factors, the mental health of participants in Togo may have been compromised, leading to more negative outcomes (Kounou, 2013; Oladeji et al., 2010).
The finding that CM was linked to Cluster A PDs symptoms and neuroticism (emotional stability) was linked to all three PDs clusters (negative correlations) in both countries suggests the universality of these associations and increases the international literature concerning the harmful consequences of CM on mental health in adulthood. However, the relationship between neuroticism and PDs was weak in our study. We hypothesize that the weak relationship between neuroticism and PDs could be explained by the measures used in our study. For instance, the PDQ-4+ used in this research was not validated in France or Togo.
There were some differences in associations between France and Togo. For example, in France, CM scores were linked only to Cluster A PDs while in Togo, there was a significant association between CM and the three PDs clusters (A, B, and C) with higher correlation coefficients for Cluster B PDs. The results obtained in Togo confirmed previous findings in non-Western cultural contexts. In fact, Zhang et al. (2012) found that in China, traumatic childhood experiences correlated positively with the three clusters of PDs and that CM had the most significant impact on Cluster B PDs.
In France and Togo, EA was positively correlated with Cluster A PDs. The correlation coefficients were not different statistically (Z = .48, p = .316), and we may hypothesize that the effect of EA on Cluster A PDs is similar in both countries. Our findings that CM is related to Cluster A PDs symptoms in both countries are in line with those of recent work on schizophrenia (Braehler et al., 2013; Carr, Martins, Stingel, Lemgruber, & Juruena, 2013; Fisher et al., 2014).
In Togo, severe PA was associated with a higher number of PDs than the other types of CM (six in total: schizoid, antisocial, narcissistic, obsessive-compulsive, depressive, and negativist). The opposite was found in France, where PA was only associated with paranoid PD. These differences may be partly explained by the fact that in Togo (as in many sub-Saharan African countries), physical punishment habits are set up as standards and are regularly put into practice. In the Ewe community (one of the major ethnic groups in Togo), for example, there is a proverb: “the stick educates the child.” Even though during these last years, efforts have been made to eradicate the corporal punishment of children, this practice persists. Thus, it appears that some forms of physical abuse are still culturally acceptable in Togo, despite growing awareness that they can be deleterious. The fact that physical abuse was not related to PD in the French sample contrasted with reports from other developed countries (Afifi et al., 2011), and may be partly explained by sampling error and/or the use of self-administered questionnaires for the assessment of participants. Future studies in French-speaking sub-Saharan Africa to evaluate the impact of PA on mental health in general and particularly PDs prove necessary. It is furthermore important to ascertain whether individuals perceive physical beatings as traumatic experiences (Zhang et al., 2012).
Some associations were found in Togo but not in France. For instance, in the French sample, EN was not linked with any PD, a result that is contrary to our findings among Togolese individuals. However, the lack of significant effect does not mean EN is not harmful in France. Future investigation to explore EN and PDs in adulthood in France may be useful.
Our findings suggest that the pathway from CM to PDs could be partly mediated by personality dimensions in Togo whereas in France, the mediating role of personality dimensions is not significant. Personality dimensions failed to predict personality disorders in the French sample. This result, which contrasts with findings of other studies (Rossier et al., 2008), could also be explained by the likely sampling error and the questionnaire used in our study. Another probable reason for the contrast between our results and those of Rossier et al. (2008) could be the characteristics of the samples in each country. In fact, in our study, the diagnosis of depression was made by physicians without using validated tools; it could be useful to compare the results of previous studies in which personality disorders diagnoses were made by clinicians, to our own. Furthermore, the possible comorbidity with other psychiatric disorders, which likely affected homogeneity of the samples, may explain the differences. We may also hypothesize that local responses to trauma could explain the differences observed between the French and the Togolese samples. In every cultural context and community, there will be particular ways to respond to the effects of trauma (Hinton & Kirmayer, 2013). Thus, the process leading from CM to PDs may not be identical in both countries. Indeed, other mechanisms such as immature defensive organization and self-esteem injury (Finzi-Dottan & Karu, 2006) and the latent dimensions (Keyes et al., 2012) may mediate the course from CM to PDs in adulthood. In summary, in Togolese patients, emotional instability could partially explain the link between CM and PDs while in France, other mechanisms (not evaluated in our research) may underlie this relationship.
The results on the mediating effect of emotional instability in Togo confirm those of Bowen, Balbuena, Leuschen, and Baetz (2012), according to which mood instability is a predictor of worse mental state. Our results in Togo suggest that taking into account emotional instability in the treatment of depressed patients with PDs may be appropriate. Sociocultural context may also determine differences in pathways from CM to PDs. Future research should include other mediation factors that could explain the link between CM and PDs, and the national differences in personality reported by previous research (Allik, 2012). Our findings are in line with a study by Bhui (2011) which discussed social and cultural influences on risks and responses to mental illness. Differences in frequency of CM and in the progression of CM to PDs among French and Togolese depressive patients support the results of other cross-national comparisons, which also have found differences in terms of the frequency of trauma exposure and service availability (Kohn, 2011; Lora et al., 2012). To better explore the differences between French and Togolese samples, we believe that diagnoses made by clinicians in each cultural context are more appropriate than those based on questionnaires which are not validated in French-speaking sub-Saharan Africa (PDQ-4+ for example). This is an explanatory hypothesis which may be verified by future studies.
Limitations
Our study has several limitations. This is a cross-sectional study relying on retrospective assessment of CM. It is not certain that the proposed temporal associations of CM–personality dimensions–PDs exist. The supposed mediation relationship is a hypothesis which could be better examined in a longitudinal study. This study was performed on patients with a primary diagnosis of MDD. The probable existence of psychiatric comorbidities or other Axis I disorders of DSM-IV among the patients may have distorted our results. The small sample size used in this study, its specificity (patients with primary diagnosis of MDD) and its nonrepresentative French and Togolese populations do not enable us to generalize these results to the whole of these countries. Another limitation of our study is the use of the PDQ-4+, which does not produce reliable clinical PDs diagnoses and has not been validated in Africa. However, previous research by Rossier et al. (2008) also used the PQD-4+ to assess PDs in sub-Saharan Africa. Future research with prior validation of PDs measures could help to limit some of the inadequacy of our current study. Another limitation of our study is that it is an exploratory one. Our study sample was not representative of French and Togolese populations and our findings therefore may not be generalizable. Furthermore, we used univariate statistics and did not correct for multiple comparisons. Future research with the use of multivariate models or with data collection by interviews would help to replicate our current findings and would provide additional insight into these relationships.
Conclusion
Despite its methodological limitations, this study is one of the very few to examine, simultaneously, the links between CM, personality dimensions, and PDs in two different cultural contexts. Findings suggest that sociocultural environment could have an influence on the evolution and consequences of adversities from childhood to adulthood. This study has attempted to fill the gap in research in French-speaking sub-Saharan Africa concerning the association between CM and PDs in adulthood. Future longitudinal research on a representative sample aimed at further exploration of these relationships seems necessary.
Footnotes
Acknowledgements
Cosy Blewussi Kounou received a PhD grant from “Agence Universitaire de la Francophonie” within the framework of this research. We thank Kathleen Evans, Dominique Marcou, and Damien Armengol for their translation assistance.