
Abstract
The translation of well established psychometric tools from English into Xhosa may assist in improving access to psychological services for Xhosa speakers. The aim of this study was to translate the Clinical Outcomes in Routine Evaluation – Outcome Measure (CORE-OM), a measure of general distress and dysfunction developed in the UK, into Xhosa for use at South African university student counselling centres. The CORE-OM and embedded CORE-10 were translated into Xhosa using a five-stage translation design. This design included (a) forward-translation, (b) back-translation, (c) committee approach, (d) qualitative piloting, and (e) quantitative piloting on South African university students. Clinical and general samples were drawn from English-medium South African universities. Clinical samples were generated from university student counselling centres. General student samples were generated through random stratified cluster sampling of full-time university students. Qualitative feedback from the translation process and results from quantitative piloting of the 34-item CORE-OM English and Xhosa versions supported the reduction of the scale to 10 items. This reduced scale is referred to as the South African CORE-10 (SA CORE-10). A measurement and structural model of the SA CORE-10 English version was developed and cross-validated using an English-speaking university student sample. Equivalence of this model with the SA CORE-10 Xhosa version was investigated using a first-language Xhosa-speaking university sample. Partial measurement equivalence was achieved at the metric level. The resultant SA CORE-10 Xhosa and English versions provide core measures of distress and dysfunction. Additional, culture- and language-specific domains could be added to increase sensitivity and specificity.
Almost 20 years after the abolition of apartheid, South Africa remains a country in transformation. In the years following the end of apartheid historically White South African universities have become more representative of the general population; however, Black students continue to contend with the consequences of apartheid policies (Young, 2009). These include increased education and language challenges (Sommer & Dumont, 2011), the isolation and alienation of attending a historically White university (Boughey, 2003), and often being first-generation tertiary education seekers, and second-language English speakers (Young, 2009). In this context, it is not surprising that Black students have demonstrated increased levels of psychological distress in comparison to White students (Young & Campbell, 2013). However, Black students report ambivalence about seeking psychological support at university counselling centres (Young, 2009). The restricted access to psychological services in African languages is a contributing factor. Current initiatives are aimed at broadening access to professional mental healthcare services for African language speakers by increasing the selection and training of African-language-speaking mental healthcare professionals (Swartz & Drennan, 2000). The development of psychological resource material and the translation of well studied and established psychometric tools into African languages may further assist in improving access (Health Professions Council of South Africa, 2006). A number of self-report inventories have already been translated from English into Xhosa (Drennan, Levett, & Swartz, 1991; Smit, van den Berg, Bekker, Seedat, & Stein, 2006; Steele & Edwards, 2008). However, studies report difficulties in finding Xhosa equivalents for psychological terms commonly used in English. One factor contributing to this problem is that these instruments draw from Western psychiatric modes of conceptualising and describing distress (Swartz & Drennan, 2000). Because culture shapes the way language is used to conceptualise feelings, thoughts, and behaviours, the terms and experiences used to describe psychological distress vary considerably across languages, making it difficult to find linguistically and conceptually equivalent terminology in many instances (Westermeyer & Janca, 1997). Moreover, not all psychological terminology used in the English language is as relevant and meaningful within the Xhosa language when conceptualising and describing distress. This challenge contributes to the difficulties Xhosa-speaking psychologists, trained in Western psychiatric models, confront when attempting to conduct psychotherapy with clients in the Xhosa language. The translation of psychometric tools that evaluate broad descriptions of psychological distress into Xhosa may identify equivalently meaningful domains of conceptualising and describing distress. These common domains may assist Xhosa-speaking psychologists and clients in negotiating a shared discourse congruent with both a Western psychiatric model of distress and Xhosa ways of expressing this distress.
The aim of this study was to translate the Clinical Outcomes in Routine Evaluation – Outcome Measure (CORE-OM), a measure of general distress and dysfunction developed in the UK, into Xhosa for use at South African university student counselling centres. In so doing, the study aimed to identify meaningful domains of distress that were transportable across English and Xhosa languages. The CORE-OM is a measure of general distress and dysfunction comprising four domains: subjective well-being (four items); problems or symptoms (12 items); life functioning (12 items); and risk (six items; Evans et al., 2002). The measure has demonstrated high internal reliability in UK general (n = 1,106) and clinical (n = 890) samples (α = .94 for the overall scale and α > .75 across all domains) and test–retest stability (rs = .90 for the overall scale and rs ≥ .86 across all domains except the risk domain where rs = .64; Evans et al., 2002). Convergent validity has been demonstrated with the Symptom Checklist-90-R (rs = .88) and the Beck Depression Inventories I (rs = .85) and II (rs = .81; Barkham et al., 2001). The measure has shown strong positive correlations with mental healthcare practitioners’ evaluations of levels of risk in a clinical sample of students attending university counselling centres (Lyne, Barrett, Evans, & Barkham, 2006). The CORE-OM has also shown good transportability within English-speaking South African university student samples (Campbell & Young, 2011). However, a definitive psychometric structure has been difficult to demonstrate (Lyne et al., 2006), complicating cross-cultural and language comparisons of the measure. In addition, the tool has been criticised for high item similarity, particularly within the subjective well-being and problems or symptoms domains (Bedford et al., 2010; Lyne et al., 2006).
More recently, the CORE-OM has been reduced to a 10-item scale referred to as the CORE-10 that includes six items from the problems or symptoms domain, three from the life functioning domain, and one from the risk domain (Barkham et al., 2013). As an embedded measure of the CORE-OM, the CORE-10 has demonstrated high convergent validity with the CORE-OM across both general (n = 1,835; rs = .92) and clinical (n = 553; rs = .94) population samples drawn from the CORE UK national database, and high convergent validity with the Brief Symptoms Inventory (rs = .75), Symptoms CheckList-90-R (rs = .81), the Clinical Interview Schedule-R (rs = .74), the Beck Depression Inventory I (rs = .77) and II (rs = .76), and the Beck Anxiety Inventory (rs = .65; Barkham et al., 2013).
Method
The CORE-OM (and embedded CORE-10) was translated into Xhosa in accordance with the CORE System Trust’s translating and normalising guidelines (Evans, 2008). These guidelines consist of a five-step translation design: (a) forward-translation into Xhosa, (b) back-translation into English, (c) committee approach, (d) qualitative piloting, and (e) quantitative piloting. All translators were first-language Xhosa-speaking South African men and women aged between 19 and 50 years, having completed tertiary studies in English. The translation team included university students, psychologists working in university student counselling centres, psychiatric nurses, and Xhosa linguists. Translators were instructed to make translation choices that would allow transportability of the tool across different geographical, as well as urban and more rural contexts, so that the tool could later be applied in state mental health care contexts.
Translation procedure
Forward-translation into Xhosa
The CORE-OM was forward-translated into Xhosa by one male professional Xhosa translator, one male psychiatric nurse who routinely assisted with psychiatric interviews at a local psychiatric hospital, and one male student majoring in Xhosa language studies. The translators were provided with a set of translation guidelines to assist them in the process. These included Brislin’s (1986) suggestions of the use of short, simple sentences, utilising specific terms as opposed to vague descriptions while applying the active as opposed to the passive voice and avoiding pronouns, metaphors, and colloquialisms. These guidelines were further supplemented by previous Xhosa translation studies that suggested a focus on linguistic equivalence during forward-translation (Steele & Edwards, 2008); the selection of vocabulary that is widely applicable across Xhosa dialects (Drennan et al., 1991); and the use of written as opposed to more colloquial, spoken versions of the language (Steele & Edwards, 2008).
Back-translation into English
The Xhosa forward-translations were then back-translated into English by an independent team of bilingual translators including one male professional Xhosa translator, one male psychiatric nurse, and one female student majoring in psychology. The original CORE-OM questionnaire items along with each Xhosa forward-translation and accompanying English back-translation were tabulated for comparison.
Committee approach
All translators then met together to discuss the resultant forward- and back-translations in order to develop a finalised Xhosa version. Each CORE-OM questionnaire item was evaluated and the most appropriate Xhosa translation selected or reworded for inclusion. The tabulated forward- and back-translations assisted translators in identifying linguistically equivalent vocabulary across the languages as well as problematic descriptions of distress that required more conceptually equivalent translations.
Qualitative piloting
The initial CORE-OM Xhosa translation generated during the committee approach step was then qualitatively piloted across three groups. The first group included a third-year Xhosa language class in the Department of African Languages at a local university. The class comprised seven third-year male and female students and two academic lecturers, all of whom had developed theoretical and applied skills in Xhosa translation. The class reviewed the CORE-OM Xhosa translation for spelling and grammatical errors, then compared the Xhosa and English versions for linguistic and conceptual equivalence. Recommended changes were incorporated into the CORE-OM Xhosa version which was then reviewed by three psychologists who conducted psychotherapy in Xhosa daily within a university student counselling centre context. Again the tool was reviewed for spelling and grammatical errors, and then compared with the English version for linguistic and conceptual equivalence. Recommended changes were incorporated into the CORE-OM Xhosa version. This final review was conducted by an independent group of professionals including a first-language Xhosa-speaking psychologist and a first-language Xhosa-speaking linguist in South Africa who collaborated with a first-language Xhosa-speaking psychiatric nurse and a member of the CORE-OM UK development team in the UK, via Skype. The group reviewed the final CORE-OM Xhosa translation for linguistic, semantic, and conceptual equivalence with the original English version. The member of the CORE-OM UK development team, while not a Xhosa speaker, facilitated the group discussion from the perspective of the tool developer in order to ensure that the resultant CORE-OM Xhosa translation aligned well conceptually with the original CORE-OM English version.
Quantitative pilot
The finalised CORE-OM Xhosa translation was then quantitatively piloted with university students drawn from English-medium universities in the Eastern Cape, including both historically disadvantaged and advantaged universities. Both clinical and general student population samples were used to pilot the CORE-OM Xhosa translation.
The clinical sample was generated from student counselling centres across three South African Eastern Cape universities where Xhosa-speaking students were asked to complete the CORE-OM Xhosa version before their initial intake interview. No additional diagnostic information was recorded. A comparative clinical sample of English-speaking students completed the CORE-OM English version at a South African Eastern Cape, English-medium university student counselling centre. English-speaking students were asked to complete the CORE-OM English version before their initial intake interview. No additional diagnostic information was recorded.
The general student sample was generated through random stratified cluster sampling of full-time students registered at a historically disadvantaged university where the majority of students were Xhosa speakers. Level of study (undergraduate or postgraduate) and choice of faculty were used as strata. Academic lectures conducted across three or four subjects within each faculty were sampled in order to reduce design effect (Raudenbush, 1997). A comparative general sample of English-speaking students completing the CORE-OM English version was collected through random stratified cluster sampling at a South African Eastern Cape, English-medium university. Level of study and choice of faculty were again used as strata. Academic tutorial groups conducted across three or four subjects within each faculty were sampled in order to reduce design effect (Raudenbush, 1997). English-speaking students were asked to complete the CORE-OM English version.
The results of the qualitative and quantitative piloting were used to consider (a) whether the full CORE-OM Xhosa version was appropriate for use or should be reduced to a shorter scale, and (b) if reduced, whether that scale was equivalent across its English and Xhosa language versions.
Data analysis
Analyses were conducted in SPSS for Windows, Version 16.0 and AMOS Version 19. CORE-OM questionnaires containing more than three item omissions or more than one item omitted per domain were unusable and removed from the sample. Missing data on the remaining CORE-OM questionnaires (containing three or less omissions) was replaced using the HOTDECK macro from SPSS (Myers, 2011). Data analysis comprised three stages.
Stage 1: Evidence for reducing the CORE-OM scale
The lack of agreement in the literature on the psychometric structure for the CORE-OM (Bedford et al., 2010; Lyne et al., 2006), coupled with criticism of item similarity and redundancy across CORE-OM items (Bedford et al., 2010; Lyne et al., 2006), led the authors to consider evidence for reducing the measure to a shorter 10-item scale. Mean scores and standard deviations were calculated for each item and domain as well as CORE-OM and CORE-10 scales across the English and Xhosa versions. Cronbach’s alpha was used to calculate item-total correlations and internal stability within each domain and across the CORE-OM and CORE-10 scales. CORE-OM items that had poor psychometric properties and proved challenging to translate into Xhosa according to qualitative feedback during the qualitative review process, were marked as problematic and considered for removal from the scale. A South African CORE-10 measure was proposed as a result of this analysis.
Stage 2: A measurement and structural model of the SA CORE-10 English version
A measurement model of the South African CORE-10 (SA CORE-10) English version was investigated through principal component analysis with oblimin rotation, using a subgroup of English-speaking students who completed the CORE-OM English version (n = 104, Group A) randomly selected from the total sample (n = 733). Oblimin rotation was used based on evidence of the item similarity and high correlation across the subjective well-being, problems or symptoms, and life functioning domains in the original UK CORE-OM English version (Evans et al., 2002; Lyne et al., 2006). Considering that nine of the 10 SA CORE-10 items were from these domains, any resultant factors should correlate.
A structural model of the SA CORE-10 was then developed in AMOS Version 19 based on this principal component analysis. This model was compared with the data generated by Group A using confirmatory factor analysis with maximum likelihood estimations to establish model fit. The model was then cross-validated on the remaining sample of English-speaking students (n = 629, Group B). Model fit was evaluated using the chi-squared goodness-of-fit test (χ2), χ2/degrees of freedom ratio (CMIN/DF), the comparative fit index (CFI), and the root-mean-square error of approximation (RMSEA) with increasing levels of constraints. Differences across constrained models were compared using likelihood ratio test (Δχ2) and changes in CFI values (ΔCFI), in order to establish the level of equivalence obtained.
Stage 3: Equivalence and psychometric properties of the South African CORE-10 English and Xhosa versions
The structural model developed for the SA CORE-10 English version was then compared with data from the SA CORE-10 Xhosa version using a sample of first-language Xhosa-speaking students who completed the CORE-OM Xhosa version (n = 243). Model fit was again evaluated using χ2, CMIN/DF, CFI, and RMSEA with increasing levels of constraints. Differences across constrained models were compared using Δχ2 and ΔCFI in order to establish the level of equivalence obtained.
Internal consistency of the SA CORE-10 Xhosa and English versions was established using Cronbach’s alpha. Convergent validity with the CORE-OM and CORE-10 was investigated using Spearman’s rho. Discriminant validity was demonstrated through the measure’s ability to differentiate between a clinical and general sample, comparing sample means with t tests using a probability of .05. Effect sizes were used to indicate the size of difference between the samples.
Results
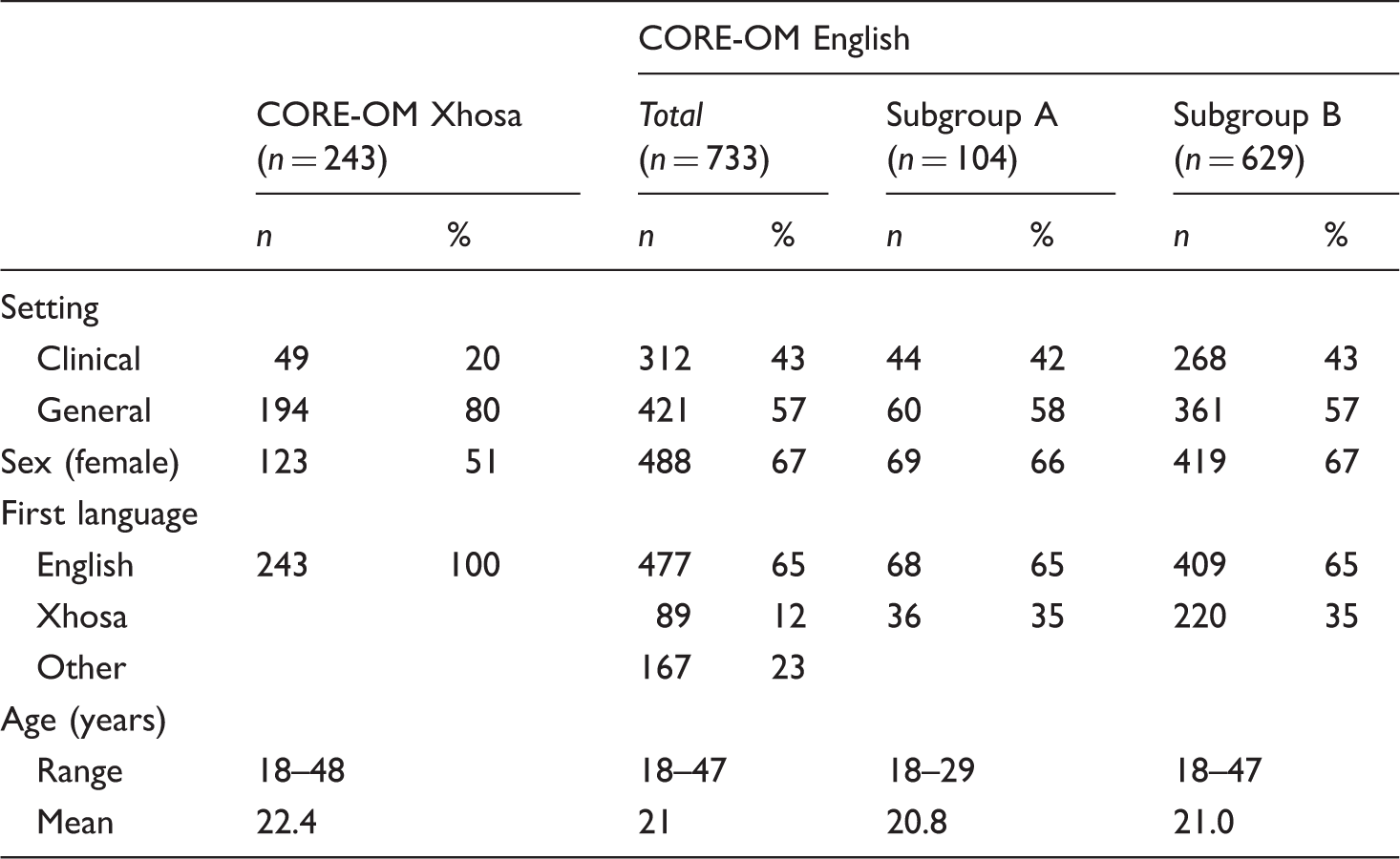
Demographic characteristics of participants in pilot test of CORE-OM Xhosa and English language versions.
Stage 1: Evidence for reducing the CORE-OM scale
CORE-OM Xhosa and English language versions.

Indicates embedded CORE-10.
Within the subjective well-being domain, the overall mean score was lower within the Xhosa-speaking clinical sample than the English sample, but similar across the Xhosa and English general samples. Similarly, item mean scores tended to be lower within the Xhosa clinical sample in comparison with the English clinical sample, but similar across the Xhosa and English general samples. Comparisons of the original CORE-OM English version subjective well-being domain items with their Xhosa translations and English back-translations suggested that while a degree of conceptual similarity had been achieved across the language versions of the domain, the translations were not necessarily equivalent. For example: Item 4 (“I have felt OK about myself”) was translated into the Xhosa “Ndizive kakuhle ngesiqu sam” which was back-translated as “I felt good about myself”; Item 31 (“I have felt optimistic about my future”) was translated into the Xhosa “Ndizive ndithemba ngengomso lam,” and back-translated as “I had hope for or trusted in the future.”
Within the problems or symptoms domain, the total mean score was lower in the Xhosa clinical and general samples in comparison with the English clinical and general samples. Similarly, item mean scores tended to be lower within the Xhosa-speaking clinical and general samples in comparison with the English clinical and general samples. Feedback from the qualitative piloting indicated that within the problems or symptoms domain, simple, concrete statements such as Item 13, “I have been disturbed by unwanted thoughts and feelings” (“Bendiphazanyiswe ziingcinga neemvakalelo ezingafunekiyo”), and 27, “I have felt unhappy” (“Ndizive ndingonwabanga”), generated less debate amongst reviewers and were generally easier to translate. Similarly, items describing physical or somatic symptoms were easier to translate, such as Item 5, “I have felt totally lacking in energy and enthusiasm” (“Ndizive ndithyafile ndingenamandla akwenza nto”), and Item 18, “I have had difficulty getting to sleep or staying asleep” (“Andilali kakuhle okanye ndiyaphuthelwa”).
However, reviewers reported difficulty finding consensus about the most appropriate Xhosa vocabulary to accurately denote the intensity of the English terminology relating to psychological symptoms of distress. For example, during review of Item 15, “I have felt panic or terror,” reviewers debated the most appropriate Xhosa vocabulary to denote the intensity of panic (“Bendinophaphazela,” or “Bendinongxungupholo”), while sufficiently differentiating this term from terror (“noloyiko”). Similarly, during review of Item 23, “I have felt despairing or hopeless,” reviewers reported difficulty finding consensus on the most appropriate Xhosa vocabulary (“ndingento,” “ndinikezele,” or “ndiphelelwe lithemba”) to depict the intensity of these feeling states. For Item 28, “Unwanted images or memories have been distressing me,” reviewers reported no available Xhosa terminology for these concepts and again found it difficult to reach consensus on the most appropriate Xhosa phrases to convey conceptual equivalence. These difficulties may account for differences in the total and item mean scores across the Xhosa and English clinical samples for this domain.
Within the life functioning domain, the total mean score was higher in the Xhosa clinical and general samples in comparison with the English clinical and general samples. Similarly, item mean scores tended to be higher within the Xhosa-speaking clinical and general samples in comparison with the English clinical and general samples. Feedback from the qualitative piloting suggested that items within the life functioning domain focused on concrete experiences generated less debate amongst reviewers and were generally easier to translate. Such items included Item 3, “I have felt I have someone to turn to for support when needed” (“Ndizive ndinaye umntu onokundixhasa xa ndidinga inkxaso”), and Item 32, “I have achieved the things I wanted to” (“Imizamo yam iphumelele”). However, items that drew on colloquial expressions such as Item 7, “I have felt able to cope when things go wrong,” and items that described more complex emotional experiences generated more difficulties. For example, reviewers reported difficulties finding the appropriate Xhosa phrases to express grammatically the experience of irritation when in the company of others described in the English phrasing of Item 29, “I have been irritable when with other people.” Similarly, Item 33, “I have felt humiliated or shamed by other people,” proved difficult to translate into a Xhosa version that indicated clearly that the humiliation or shame was inflicted by others.
Within the risk domain, the total mean score was similar across the Xhosa and English clinical samples, as well as the Xhosa and English general samples. Item mean scores also tended to be similar across the Xhosa- and English-speaking clinical samples and Xhosa- and English-speaking general samples. Feedback from the qualitative piloting of the risk domain items indicated that reviewers found consensus easily with simpler, concrete statements such as Item 9, “I have thought of hurting myself” (“Bendinengcinga yokuzenzakalisa”), and Item 16, “I have made plans to end my life” (“Ndiye ndenza amalungiselelo okuzibulala”). However, it was more difficult to find grammatical consensus on more complex statements with more than one idea or concept, such as Item 34, “I have hurt myself physically or taken dangerous risks with my health” (“Ndizenzakalisile okanye ndenze izinto ukubeka impilo yam emngciphekweni”).
These results indicate important differences in the performance of items and domains across the CORE-OM Xhosa and English versions. Considering that the reduced CORE-10 version maintained adequate internal consistency across Xhosa (α = .79) and English (α = .88) versions and good convergent validity with the CORE-OM across the Xhosa version clinical (rs = .89) and general (rs = .91) samples, and the English version clinical (rs = .94) and general (rs = .95) samples, we decided to reduce the measure. The CORE-10 included Items 2, 3, 7, 10, 15, 16, 18, 23, 27, and 28 from the original CORE-OM (marked with an asterisk in Table 2). While many of these items had translated fairly well into Xhosa, three items (Items 23, “I have felt despairing or hopeless” and 28, “Unwanted images or memories have been distressing me” from the problems and symptoms domain, and Item 7, “I have felt able to cope when things go wrong” from the life functioning domain) had been identified as difficult items to translate into linguistically and conceptually equivalent Xhosa versions during the translation process.
During the original reduction of the CORE-OM into the CORE-10, items were paired for similarity of content, phrasing, and intensity, and the item that best predicted the original cluster was selected for inclusion in the scale (Barkham et al., 2013). Item 23 was paired with Item 5; Item 28 with 13; and Item 7 with 32 (Barkham et al., 2013). In preparing the CORE-10 for use within South African English- and Xhosa-speaking populations, Item 7 “I have felt able to cope when things go wrong” was replaced with Item 32 “I have achieved the things I wanted to” which had proven to be easier to translate into Xhosa, while Item 23 “I have felt despairing or hopeless” was replaced with Item 5 “I have felt totally lacking in energy and enthusiasm”; and Item 28 “Unwanted images or memories have been distressing me,” with item 13 “I have been disturbed by unwanted thoughts and feelings.” The resultant 10-item CORE measure referred to as the South African (SA) CORE-10 included Items 2, 3, 5, 10, 13, 15, 16, 18, 28, and 32 from the original CORE-OM version.
Stage 2: A measurement and structural model of the SA CORE-10 English version
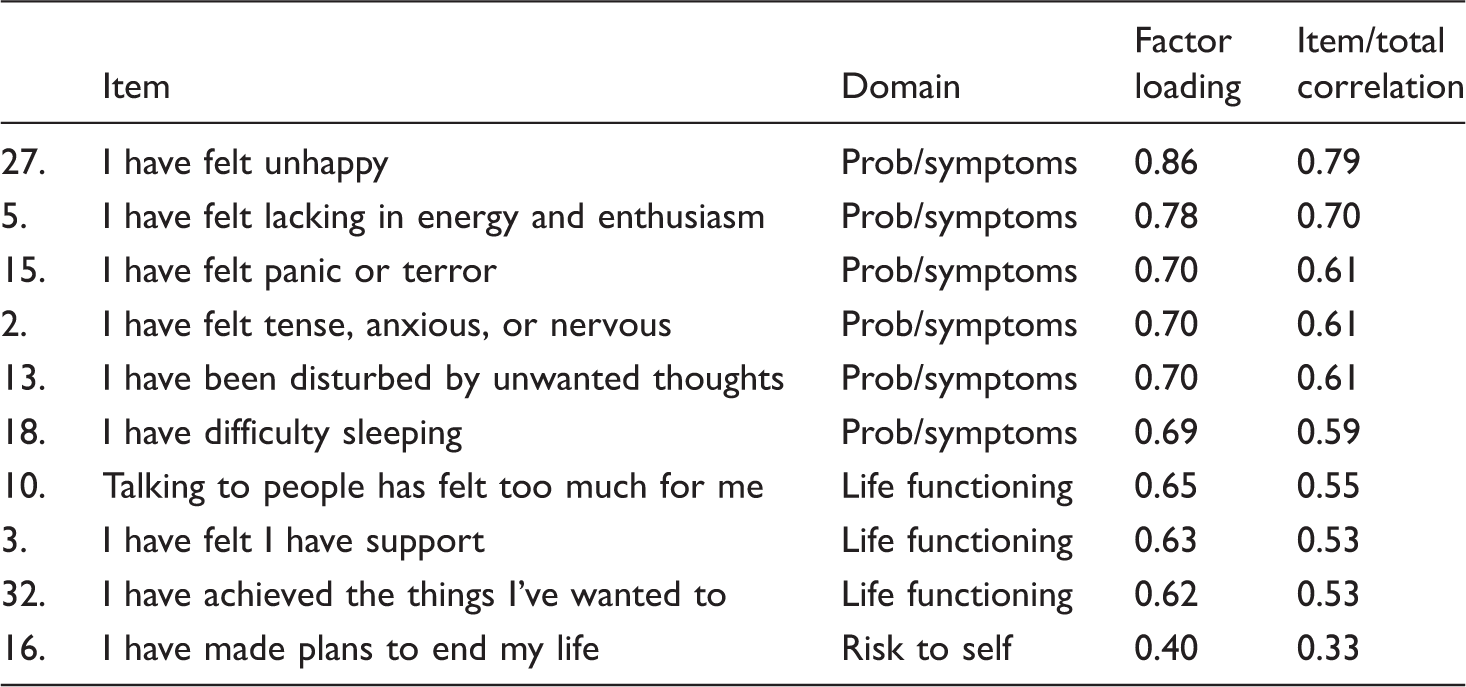
Factor loadings, internal consistency SA CORE-10 English version.
A one-factor structural model was developed in AMOS Version 19 and compared with the data from Group A, demonstrating a good fit, χ2(35) = 35.536, ρ = 0.443; CMIN/DF = 1.015; CFI = 0.998; RMSEA = 0.012; 90% CI [0.00, 0.072]. This model is presented in Figure 1. The model was then cross-validated on the remaining sample of English-speaking students (n = 629, Group B). While χ2 were significant across increasing levels of constraints, likely as a result of the large sample size of Group B, these results must be interpreted in context of the other goodness-of-fit indices (CMIN/DF, CFI, RMSEA) which revealed a consistently good model fit. Comparisons across increasing constraints models indicated no significant differences, demonstrating both measurement and structural equivalence (see Table 1S in online supplemental material).
Structural model of the SA CORE-10.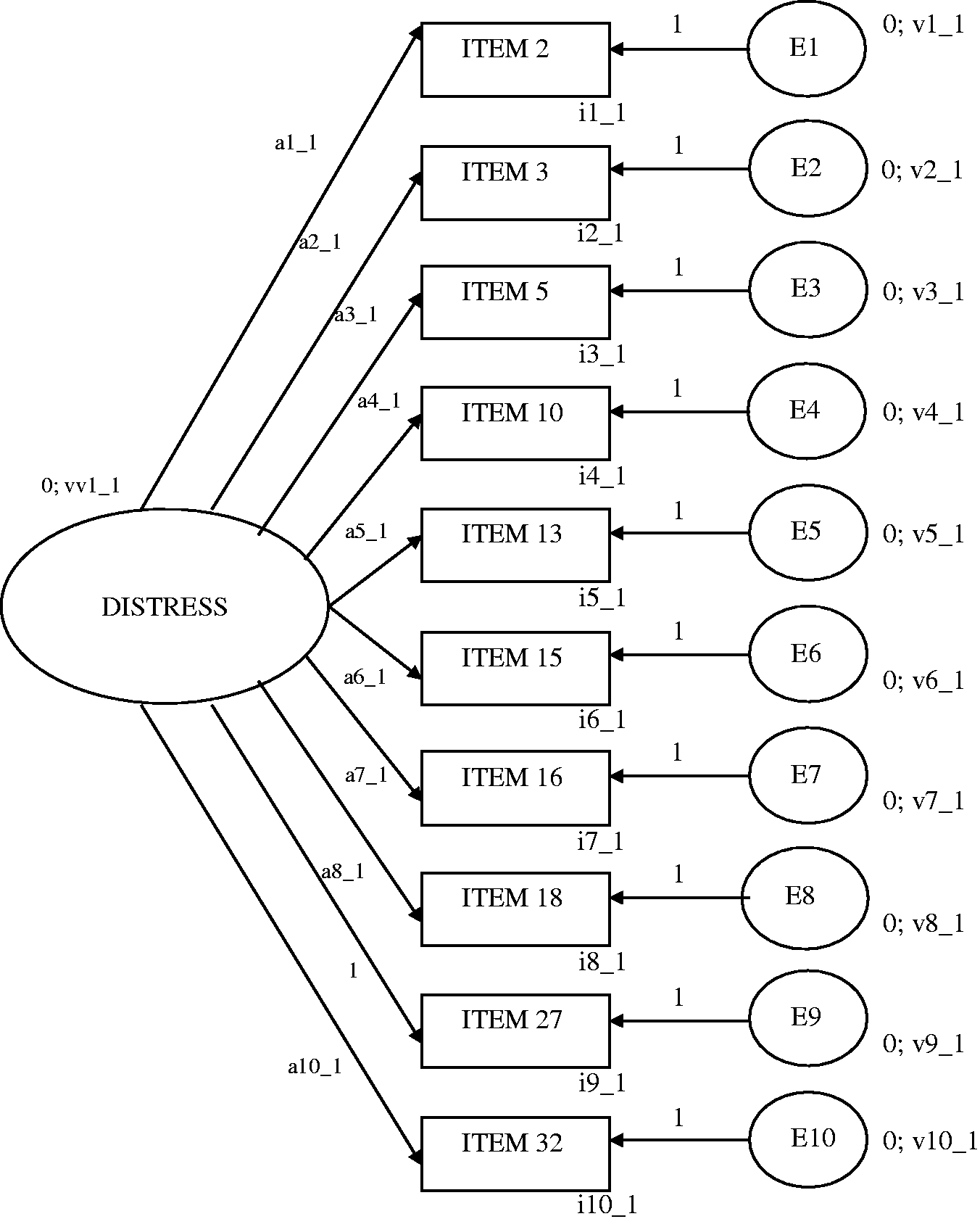
Stage 3: Equivalence and psychometric properties of the South African CORE-10 English and Xhosa versions
This structural model was then applied to the SA CORE-10 Xhosa version, using a sample of first-language Xhosa-speaking students who had completed the CORE-OM Xhosa version (n = 243). While χ2 was significant in the unconstrained model, additional goodness-of-fit indices suggested a good fit, χ2(68) = 117.70, ρ < 0.00; CMIN/DF = 1.731; CFI = 0.976; RMSEA = 0.034; 90% CI [0.02, 0.04]. However, while comparisons across increasing constraints models indicated no significant differences at measurement level with regard to metric equivalence, significant differences were noted at the level of scalar equivalence indicating only partial measurement equivalence. This finding indicates that while similar meanings are assigned to the construct of distress across the SA CORE-10 Xhosa and English language versions, the levels of the underlying items represented by their means and intercepts differ across the two language versions producing different measurement scales and making direct comparison of scores difficult across the two language versions. These results are presented in Table 2S in online supplemental material.
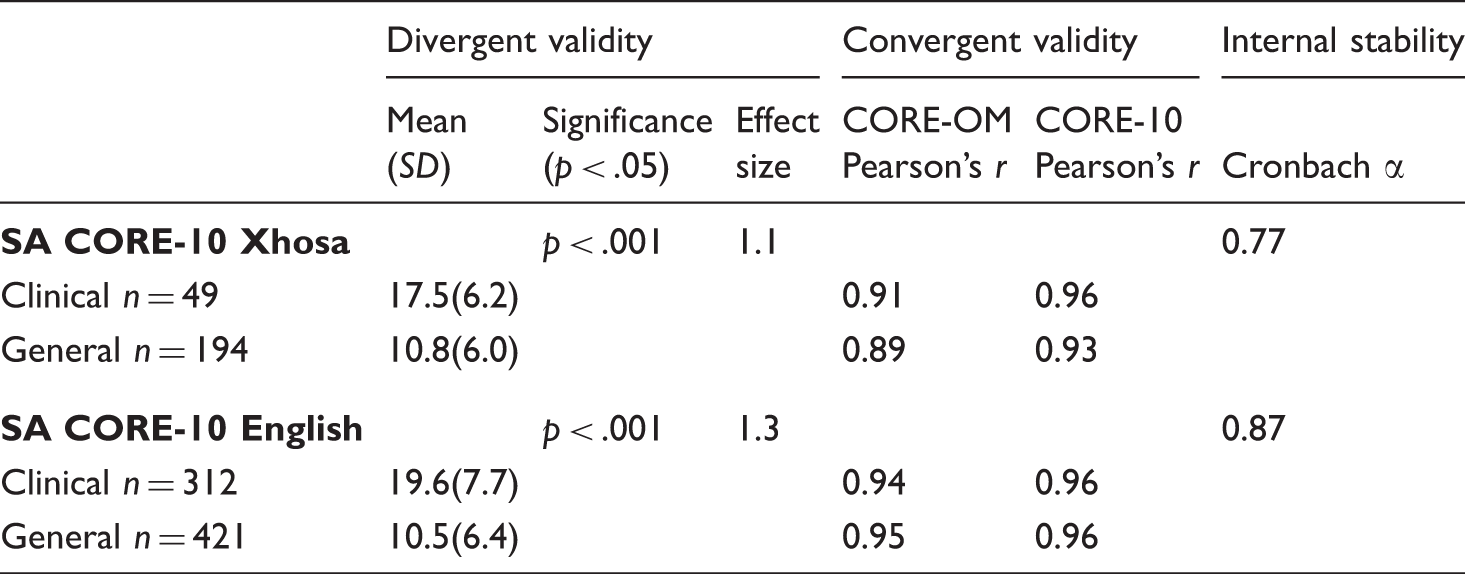
Psychometric properties of the SA CORE-10 Xhosa and English language versions.
Discussion
Translations of the CORE-OM into other European languages like Norwegian (Skre et al., 2013), Swedish (Elfstrom et al., 2013), and Italian (Palmieri et al., 2009) have shown small psychometric differences with the original English CORE-OM version, suggesting good transportability of the measure across these different European contexts. This is not surprising considering that the Western psychiatric model of conceptualising and describing distress may be fairly consistent across these contexts. In contrast, the translation of the CORE-OM (and embedded CORE-10) into Xhosa proved considerably more challenging. Despite a rigorous translation method, it was only possible to achieve partial measurement equivalence across the two language versions. The extensive time and resources that were expended during this translation process call into question the efficiency of such an approach. Perhaps these resources would have been better utilised in developing a Xhosa measure of general distress and dysfunction as opposed to translating an English measure. That being said, valuable findings emerged from the process.
First, items within the subjective well-being domain proved particularly difficult to translate into linguistically and conceptually equivalent Xhosa versions. One reason for this may be that the subjective well-being domain contains descriptions of distress that draw from fairly abstract, individualistic evaluations of personal well-being (e.g., “I have felt OK about myself”; “I have felt overwhelmed by my problems”; “I have felt optimistic about my future”). These evaluations draw from a culture-specific, not universal, conceptualisation of self (Markus & Kitayama, 1991) that does not seem to be well supported in the Xhosa language. A reconceptualisation of subjective well-being that is more culturally relevant may be valuable in a Xhosa measure of general distress and dysfunction.
Second, within the problems or symptoms, life functioning, and risk domains, simple, concrete statements containing a single concept or concrete experience appeared easier to translate, as did items relating to physical or somatic symptoms. Difficulties arose in finding consensus for Xhosa translations of items relating to psychological symptoms of distress that attempted to differentiate between intensities of these symptoms. This finding is congruent with the South African literature highlighting the far larger scope of vocabulary in the English language for describing emotional states, in comparison with the available Xhosa vocabulary (Drennan et al., 1991; Smit et al., 2006; Steele & Edwards, 2008).
When developing future Xhosa measures of general distress and dysfunction it may be useful to include more physical and somatic expressions of distress, and concrete lived experiences (“I have felt I have someone to turn to for support when needed”) as opposed to abstract emotional descriptions of distress (e.g., “I feel OK about myself”). With regard to psychological symptoms, the difficulty in finding appropriate Xhosa vocabulary to distinguish between intensities of emotional states suggests that it may not be meaningful to differentiate between these intensities in a Xhosa measure of general distress and dysfunction.
This study has important limitations. The sample sizes were small, and limited to a student population in only one of the nine South African provinces and hence, not representative of all English- and Xhosa-speaking students across South African university contexts. However, despite these limitations, this study provides a baseline from which future researchers can build towards the improved development of culturally sensitive, valid Xhosa measures of general distress and dysfunction.
Conclusion
The SA CORE-10 English and Xhosa versions, drawn predominantly from the problems or symptoms and life functioning domains of the CORE-OM, demonstrated good psychometric properties as brief self-report measures of general distress and dysfunction that are equivalent at measurement level. Additional, more culture- and language-specific domains of describing and conceptualising distress, unique to Xhosa and English languages, could be developed and then added to these core measures in order to increase the sensitivity and specificity of the tools. In particular, the inclusion of a combination of items that target broad descriptions of psychological and somatic symptoms may be more meaningful and congruent with how these experiences are expressed in the Xhosa language.
Footnotes
Acknowledgements
The authors would like to acknowledge and thank the translation team involved in the development of the CORE-OM Xhosa version: Z. Bomoyi (Rhodes University), S. Xeketwana (Rhodes University), D. Witboy and V. Jelu (Fort England Hospital), T. Fatyi (Rhodes University), A. Matebese (Rhodes University), V. Ngqaliso (Fort England Hospital), B. Magobiyane (Rhodes University), P. Maseko (Rhodes University), M. Sam (Rhodes University), the isiXhosa III class of 2010 from the Rhodes University African Languages Department, L. Mlisa (University of Fort Hare), P. Dabula (University of Fort Hare), L. Mpono (University of Fort Hare), and Z. Mvinjelwa (Priory Hospital, UK), as well as the student counselling centre directors and staff who assisted with the data collection process: Dr. Colleen Vassiliou (Rhodes University), Delvene Gelderbloem (Rhodes University), MaLily-Rose Mlisa (University of Fort Hare), Dr. Andre de Jager and Dr. Maud Ntanjana (Nelson Mandela Metropolitan University), and Marietjie Sparks (Nelson Mandela Metropolitan University).
We would also like to acknowledge the valuable contributions made towards this research by Prof. Chris Evans (CORE IMS), Prof. Fons van de Vijver (Tilburg University), and Prof. Joop de Jong (University of Amsterdam, Rhodes University). Finally, we would like to thank the reviewers from Transcultural Psychiatry for their valuable and insightful comments in developing this manuscript, and particularly the input from Prof. Deon de Bruin (University of Johannesburg).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Megan Campbell was funded by an Andrew Mellon Citizens Scholarship during her PhD, and received additional support from the Rhodes University Research Office for purposes of writing up this manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.