
Abstract
The Outline for a Cultural Formulation (OCF) has remained underutilized in clinical practice since its publication in the DSM-IV in 1994. In the Netherlands, a Cultural Interview (CI) was developed in 2002 as a tool to facilitate use of the OCF in clinical practice. The time needed to conduct the interview, however, prevented its systematic implementation within mental health institutions. This article presents the development of a shortened and adapted version, the Brief Cultural Interview (BCI), and a pilot study on the feasibility, acceptability, and utility of its implementation with refugee and asylum seeking patients in a Dutch centre for transcultural psychiatry. Results show that the brief version scores better on feasibility and acceptability, while utility for clinical practice remains similar to that of the original CI. These results support the systematic use of the OCF in psychiatric care for a culturally diverse patient population through the application of a relatively brief cultural interview. A secondary finding of the study is that patients’ cultural identity was considered by clinicians to be more relevant in the treatment planning sessions than their illness explanations.
Introduction
The cultural formulation is a systematic method for eliciting and evaluating cultural information during a clinical encounter (Lewis-Fernández & Díaz, 2002). It aims to help clinicians who provide care to patients from diverse ethno-cultural backgrounds to assess the impact of cultural factors on all items of psychiatric illness, render a culturally sensitive diagnosis, and formulate treatment plans that are acceptable to the patient and (as is often relevant) to the family. There is a great need for culturally sensitive diagnostic procedures (Zandi et al., 2008) or additional cultural consultation services (Kirmayer, Thombs, Jurcik, Jarvis, & Guzder, 2008). However, 15 years after the introduction of the Outline for Cultural Formulation (OCF) in the Diagnostic and Statistical Manual for Mental Disorders IV (DSM-IV; American Psychiatric Association, 1994, pp. 843–844), Lewis-Fernández (2009), one of its proponents, concluded that since its publication the OCF remained underutilized in actual clinical practice. This underutilization is, according to him, “likely due to limited dissemination efforts towards practicing clinicians and because of the time required for its implementation” (2009, p. 379). Where the OCF has been used, we know little about its effects on diagnosis and treatment within mental health care due to limited research on the issue (Bäärnhielm & Scarpinati Rosso, 2009; Caballero Martínez, 2009). In addition to the time factor, this too jeopardizes the continuation and expansion of use of the OCF in clinical practice.
Contributors to the special issue of Transcultural Psychiatry on the DSM-IV OCF (Lewis-Fernández, 2009) all commented on the key topics of relevance for an evaluation of its general applicability in clinical practice. Mezzich, Caracci, Fabrega, and Kirmayer (2009) criticized the OCF for not containing any guidelines and for lacking in uniformity for implementation. Alarcón et al. (2004) had already voiced similar views. Since then, several instruments have been developed to redress this through the formulation of a number of questions that relate to each of the first four OCF components (see below; Caraballo et al., 2006; Groleau, Young, & Kirmayer, 2006; Saint Arnault & Shimabukuro, 2012). However, as far as we know, these instruments have not yet been comprehensively tested or reviewed in a field trial to study their contribution towards achieving a culturally sensitive diagnosis and the formulation of a relevant treatment plan.
Fortuna, Porche, and Alegría (2009) refer to the positive outcomes of the use of the OCF derived from the Patient–Provider Encounter Study (Alegría et al., 2008). In this study, almost two thirds of clinicians found it important and meaningful to include a patient’s social and cultural context within diagnostic formulation for posttraumatic stress disorders (PTSDs) using components of the OCF. In order for this to be effective, however, training and supervision opportunities are necessary, and the OCF needs to become an integral part of DSM-IV criteria-based diagnosis (Fortuna et al., 2009, pp. 445–446).
As a response to the lack of guidelines on how to use the DSM-IV OCF in clinical practice, a Cultural Interview was developed in the Netherlands in 2002, followed in 2006 by a Brief Cultural Interview, and a Cultural Formulation Interview (CFI) in 2013 in the fifth edition of the DSM (DSM-5; American Psychiatric Association, 2013). This CFI contains a core questionnaire with 16 questions (Aggarwal et al., 2014) with the possible use of 12 supplementary modules. In the Discussion section below, the CFI will be compared to the Brief Cultural Interview (Groen, 2006).
The Cultural Interview
The original Cultural Interview (CI) developed in the Netherlands in 2002 was intended for use as a tool in the construction of a cultural formulation in psychiatric practice (Borra, van Dijk, & Rohlof, 2002). The CI has 48 questions addressing the first four components of the OCF: (a) the cultural identity of the individual (12 questions); (b) cultural explanations of the individual’s illness (11 questions); (c) cultural factors related to the psychosocial environment and levels of functioning (19 questions); and (d) cultural elements of the relationship between the individual and the clinician (six questions). Just over half of the questions are open-ended (25 out of 48). Open-ended questions offer the opportunity to provide detailed information and to build adherence to treatment. An example of such a question in the CI is: “What do you consider the most important element of your culture?” Less than half of the questions are closed questions (23 out of 48), most of which are followed by subquestions whereby a more detailed explanation is requested (16 out of 23). An example of such a series of questions is: “Do you miss people who have the same cultural background as you? Can you explain this?”
At the end of the interview a report is generated. This report contains a summary of the personal background and medical history of the patient as presented in the medical records, the answers given to the CI questions, observations made by the interviewer, and a translation of the answers into an assessment of the cultural elements that should be taken into account in psychiatric diagnosis and care.
Research setting: A Dutch centre for transcultural psychiatry
De Evenaar, a Dutch centre for transcultural psychiatry offers mental health care services to people from a range of cultural backgrounds, including asylum seekers, refugees, and migrant workers, most of whom are diagnosed as suffering from anxiety disorders, depression, and/or PTSD. Patients are referred to the centre by general practitioners, psychiatrists from other mental health institutes, psychologists in private practice, psychiatric nurses at asylum seekers centres, and a variety of other health care workers. The centre offers inpatient as well as outpatient care. Inpatient care consists of several biweekly day-treatment programmes offered to one orientation and observation group, two treatment groups, and two rehabilitation groups. Outpatient care consists of individual consultations with a psychiatric nurse or a psychologist, and in addition a number of consultations with a psychiatrist. Outpatients can also be referred to a range of therapies.
Background of the research
“Help us understand them better” was the core of the task set in 2002 for the new specialized centre for transcultural psychiatry in the Netherlands. At the time, disappointment among health workers in the northern part of the Netherlands about the results of treatment offered to asylum seekers and refugees was strong. New initiatives were fostered to improve the effectiveness of psychiatric care for this category of patients. One of the recommendations was to integrate anthropological knowledge and skills into the team at the specialized centre, which resulted in 2004 in the employment of an anthropologist, who would conduct CIs 1 day a week.
One year of conducting such interviews demonstrated that patients had difficulties with the length of the interviews, particularly when they suffered from concentration problems. In addition, it was hard to justify that the interview could take up to two hours, while psychiatric consultations generally lasted only half an hour. This problem had already been identified in a publication with a collection of cultural formulation case studies written by Dutch professionals (Borra et al., 2002, p. 235). Another problem was patients’ only partial comprehension of all CI questions (for examples, see below). Some of these questions contained a Western bias in dealing with mental health problems, such as the “mentalization” of such problems. The CI also gave rise to a formal clinical encounter in which the standard meaning of certain concepts and approaches to mental health problems were taken for granted. Adaptations in the phrasing of certain questions seemed necessary in order to obtain the cultural information that a CI aims to elicit from patients, in a way that could be easily understood.
In order to overcome the limitations of the CI, a new version was developed, aimed at facilitating an anthropological encounter (Csordas, Dole, Tran, Strickland, & Storck, 2010) and reducing the time needed to administer a CI. To distinguish between both versions, we use the original CI version (2002) in addition to the more recent BCI (2006). This article aims to contribute to the challenge of implementing the BCI by:
Presenting information on the systematic implementation of the OCF by developing a less time-consuming culturally sensitive instrument in a centre for transcultural psychiatry, the Brief Cultural Interview (BCI). Presenting evidence of the feasibility, acceptability, and utility of the BCI. Discussing the value of instrumentalizing the OCF in response to arguments related to its underutilization.
Methods
Development of a brief version of the Cultural Interview (BCI)
Use of the original version of the CI in clinical practice created the impression that refugee patients did not understand all of the questions. In the BCI, questions were reformulated so that interviewees could understand them more easily and would feel encouraged to offer an account grounded in their own cultural perspectives of the life events that may have influenced their psychopathology. In particular, questions that were considered to be too formal, direct, abstract, or prone to misunderstanding were reformulated. An example of such a question in the original CI is: “To which ethnic group do you officially belong? Do you feel that you do belong to this ethnic group, or to another one? Does this ever change?” In response, patients asked what an ethnic group was, and what it meant to “officially” belong to such a group. In the BCI, the ethnicity questions were reformulated to: “Do you belong to a group in your country that is different from other (ethnic) groups? Are your parents from the same group?” The latter subquestion was added because it came to light that many patients had encountered troubles in their home country as a result of their parents coming from different ethnic or ethno-religious descent; for example, having mixed parentage such as Azeri-Armenian or Sunni-Shia Muslim. Furthermore, based on the experience of conducting the CIs, some questions were excluded from the BCI since no relevant information for treatment plans was acquired from them. Other questions were combined with the aim of improving the progression of the interview. The final BCI was composed of 11 main questions concerning cultural identity, six main questions concerning cultural explanations of illness, seven main questions concerning cultural factors in the psychosocial environment and functioning, and one main question concerning cultural elements affecting the relationship between patient and clinician.
Research design
For practical reasons, only inpatients from the day-treatment programmes were included in the study. Inclusion criteria required that patients be 18 years or older, have no drug dependency, and display no current psychosis. To ensure that the group was representative, both asylum seekers and refugees, from a variety of countries, and of both genders and different age groups, were selected. At first, 13 CIs were conducted between April and September 2006 using purposive sampling to represent the patient population in day-treatment. BCIs were conducted with 11 other selected patients between June and October 2006. All questions of both the CI and the BCI were asked by the same interviewer word-for-word and in the same sequence. For both interviews, the time required for reporting included taking a brief clinical history, and making observations, a cultural assessment for diagnosis and care, and recommendations for the clinician. In the CI group, six interviews were conducted in Dutch and seven with the assistance of an interpreter. In the BCI group, five interviews were conducted with an interpreter, four in Dutch, and two in English. The possible effect of the use of an interpreter (Arabic, Azeri, Dari, Farsi, Papiamentu, Russian, Serbo-Croatian) during the interviews was not controlled for.
Following this, the implementation of the BCI in the Dutch centre was tested in terms of feasibility, acceptability, and utility. Feasibility was measured in terms of the time required to ask all interview questions and comprehensibility of the questions. During all interviews, patients’ reactions were noted. Further notes were made on whether or not questions were understood or had to be repeated or clarified, and whether they were answered, answered clearly, or skipped.
Acceptability was measured in terms of the patients’ evaluation of the BCI, compared to patients’ evaluation of the CI. After each BCI and CI, patients were asked to fill in a form responding to five statements about their evaluation of the interview on a 3-point scale: agree, neutral, or do not agree. These statements were: (a) “I experienced the interview as positive”; (b) “I understood all questions”; (c) “The interview gave me more tension than I expected”; (d) “The interview taught me more about myself”; (e) “Now that I know about the interview, I would do it again.”
Finally, utility was measured by noting which and how often items of the BCI reports, compared to the CI reports, were discussed by clinicians during treatment plan evaluations. Clinicians were unaware of whether the reports had been composed following a BCI or a CI. The composition of the multidisciplinary team of clinicians did not vary during these sessions. The researcher registered which cultural items clinicians discussed. This resulted in a list of 14 cultural items. For each item, the researcher evaluated whether, during treatment planning meetings, the information provided by a particular patient was perceived by care providers as relevant to take into account in his/her treatment. The aim of this final step was to find out whether the BCI resulted in at least as much useful information for treatment as the CI, despite the reduction in the number of questions. Ethical approval was obtained for the study at the University Medical Center Groningen of the University of Groningen (2012.404).
Results
Respondents
Demographic characteristics of respondents to BCI or CI
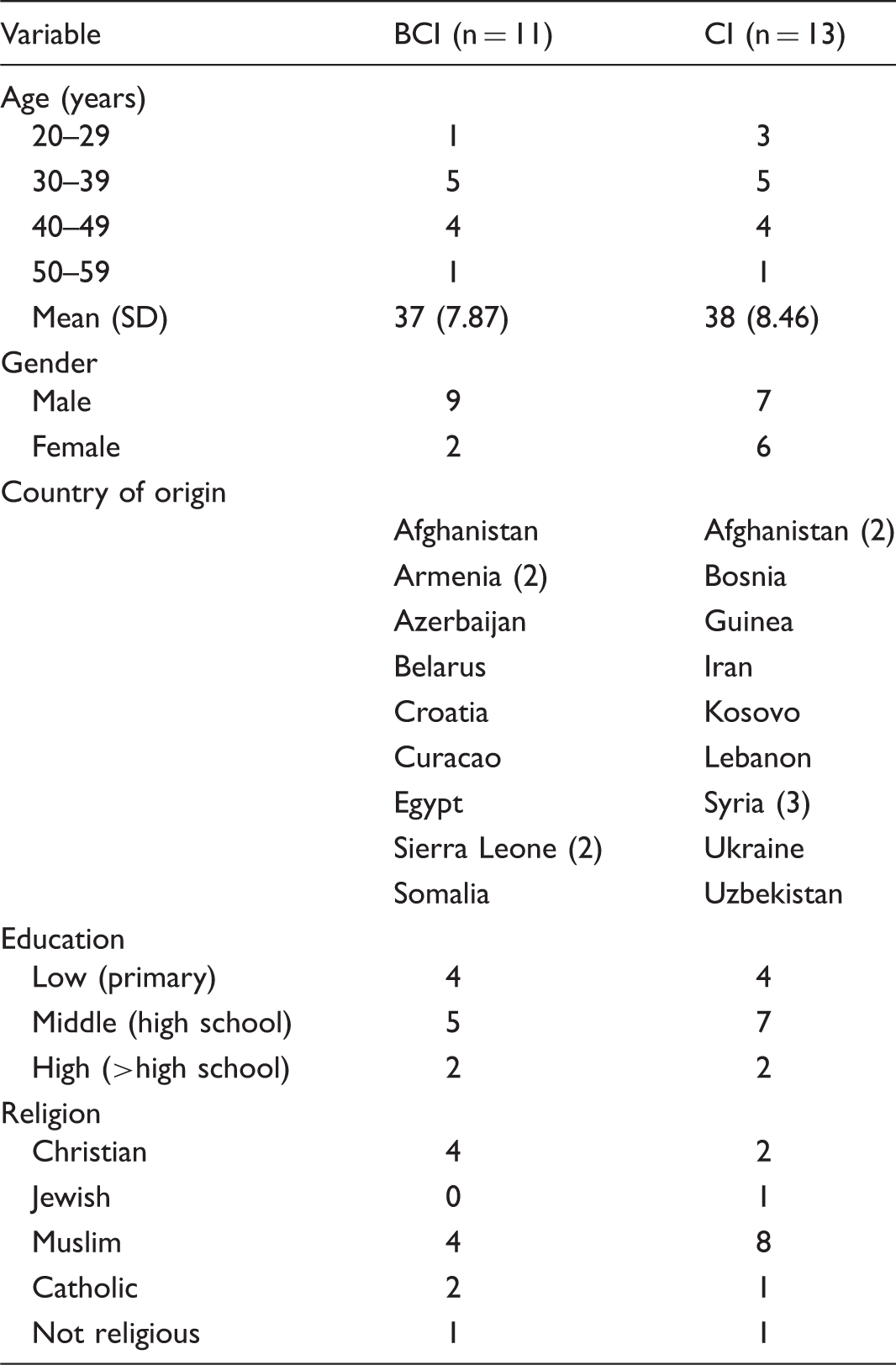
The mean age and level of education of the respondents in the first and second group were comparable. The BCI group contained relatively more men than did the CI group. There was a large variety in terms of country of origin between both groups, and also within the groups. The BCI group consisted of more Christians, the CI group of relatively more Muslims.
Feasibility: Time needed and comprehensibility
The feasibility of the BCI was measured in terms of the time needed to conduct the interview and make the report. It took the interviewer on average 80 minutes (SD 15.6) to complete the entire BCI compared to more than 2 hours for the entire CI (M 126 min, SD 27.9). For the CI, second appointments had to be made for 11 respondents because the time available for the interview per contact was only 90 minutes. When using the BCI, one second appointment had to be made. Reporting on the interviews for the BCI took 71 minutes on average (SD 22.3; range 45–120 min), while for the CI it was 143 minutes (SD 42.2; range 75–210 min).
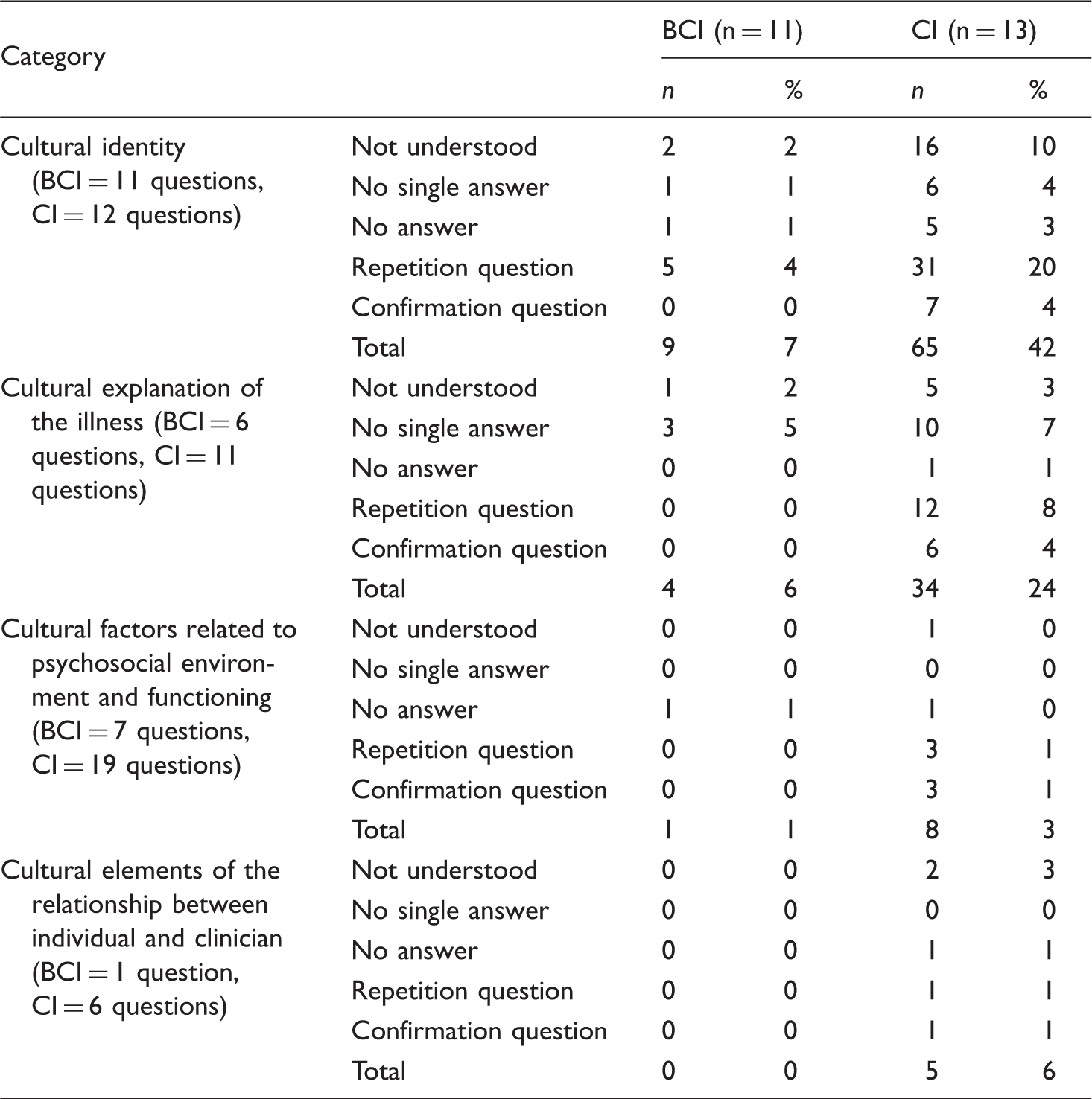
Comprehensibility of the questions of the cultural formulation during BCI and CI
Acceptability
Regarding acceptability, 5 out of 11 BCI patients and 10 out of 13 CI patients responded to the written statements after the interviews. Over half of the respondents in the BCI group agreed that it had been a positive experience, while this was the case for exactly half of the CI group (3/5 compared to 5/10). In terms of understanding the questions, respondents were considerably more positive after the BCI (4/5, compared to 5/10 after the CI). Four out of five respondents reported that the BCI had made them feel more tense (CI: 6/10). After the BCI, two out of five respondents had learned more about themselves (CI: 2/10). There were no differences in terms of willingness to participate: no respondent would refrain from being interviewed again.
Utility
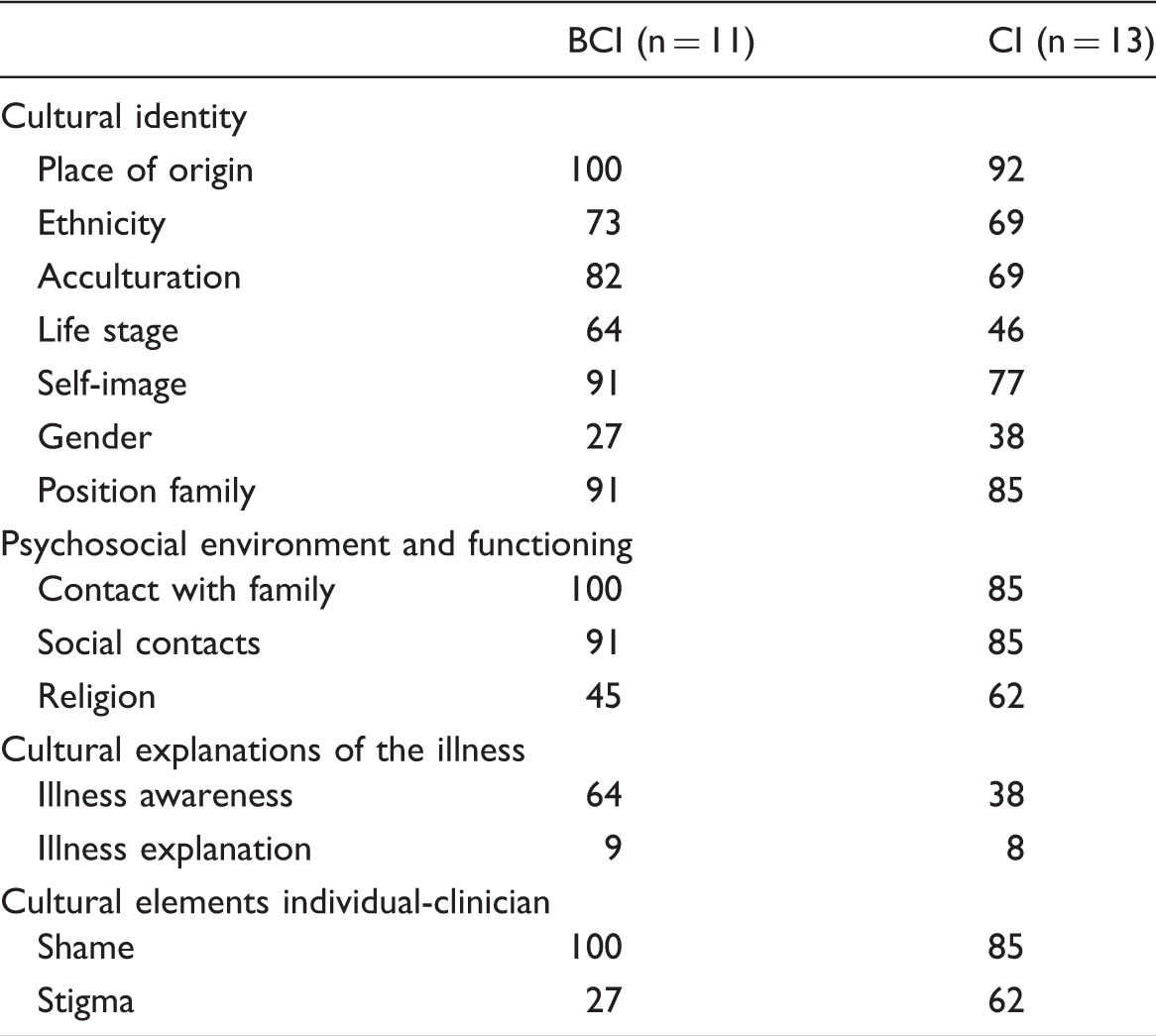
Prevalence of cultural domains in treatment sessions for each component of the cultural formulation after BCI and after CI (in %)
Discussion
The implementation of a culturally sensitive questionnaire in the Dutch centre for transcultural psychiatry has been shown to be useful. The brief version of the questionnaire (BCI) was found to be more feasible and acceptable than the original longer version (CI), while its utility remained equal. The BCI took about two thirds of the time to complete as the CI, while reporting on the results of the BCI took less than half the time of the CI. We found a better comprehensibility of the BCI compared to the CI among patients, which is relevant given the goal of the OCF, namely to bridge the cultural gap between health professionals and patients with different ethno-cultural backgrounds. Ten percent of the CI questions on cultural identity were not understood, while this was only 2% for the BCI. In addition, patients required considerably less clarification for BCI questions, which may have contributed to the shorter duration of the interviews. The reasons for not understanding some CI questions may have been caused by their formal character, by a lack of social contact with members of their same ethnic group or cultural background, by a lack of contact with their family, or by a lack of knowledge of mental health problems within the family.
While the time needed to conduct the interviews was reduced considerably through use of the BCI compared to the CI, the average time investment required to conduct a BCI is still relatively large for most mental health institutes. While in this study all questions of the BCI had to be asked for reasons of comparison, which may have contributed to the relatively high mean interview duration of 80 minutes, in clinical practice a maximum of 45 minutes is scheduled for the BCI at the Dutch centre for transcultural psychiatry. Greater experience in completing the BCI report after the interview has also led to a reduced average duration of 60 minutes. The question remains whether this time investment at the beginning of treatment will indeed pay off in later stages of the treatment in terms of reduced drop-out rates, improved medication adherence, and better understanding between patients and clinicians. Additional empirical research is needed to prove this, with specific consideration given to the time needed and the overall feasibility of such an instrument. The BCI is also still evolving as used in the centre, for instance towards the inclusion of a guide to the interviewer containing introductory questions for further probing.
The acceptability of the BCI among the respondents was higher than that of the CI, especially in terms of comprehensibility of the questions. A higher number of the BCI respondents than CI respondents answered on the evaluation form completed afterwards that they were positive about the interview, and said that they had understood all questions. This finding is supported by a better comprehensibility of the questions observed during the BCI. These results have to be interpreted with some caution, however, since the number of responses to the evaluation form was relatively low. Patients were allowed to take the form with them to fill in after the interview and three out of 13 CI respondents, and five out of 10 BCI respondents never returned it. Further bias might have arisen due to the fact that the interviewer (who had developed the BCI), was also evaluating his own method. Finally, in considering the dynamics of having to repeat or confirm questions, patients’ problems with the Dutch language, and their mental status during the interview may also have influenced the results.
Compared to the utility of the CI, the BCI was considered equally useful for treatment. The utility of the BCI was tested in terms of the number of cultural items from the reports that were considered to be relevant in the respondents’ treatment plans. We found it crucial that the reduction in the number of questions did not lead to a reduction in the amount of information found to be useful for the treatment plan. In general, the same cultural items from both interviews were considered relevant during treatment sessions. Some items of the BCI were more often discussed (acculturation, self-image, illness awareness, contact with family, shame) than others, as were some items of the CI (gender, religion, stigma). Although it was not proven that these items remained useful to pay attention to during the course of treatment, we can conclude that the BCI did not result in reduced utility for treatment. The feasibility and acceptability results affirm that, compared to the CI, the BCI is easier to understand and more positively evaluated by patients.
One of the unexpected results in terms of the utility of both interview forms was that in treatment plan sessions, the items of cultural explanations of illness appeared to be less useful than items of cultural identity, such as place of origin, ethnicity, acculturation, and self-image. This implies that cultural information on a person’s identity could be more useful to clinicians than how that person explains her or his illness (Groen, 2009; Groen & Laban, 2011). This implication is supported by Bäärnhielm and Scarpinati Rosso (2009), who, based on research conducted in Sweden, recommend focusing less on cultural explanations of illness and more on migration and acculturation issues, since they have such a strong impact on the mental well-being of refugee patients. Furthermore, the authors stress that the meaning of the concept of cultural identity needs to be clarified and guidelines should include how to approach refugee patients and how to document their history without stereotyping and discriminating.
The results from our study support this latter recommendation, since cultural explanations of illness were considered of limited usefulness in treatment plan meetings, while acculturation and its impact on cultural identity were considered by clinicians to be highly useful. The likelihood of change in cultural identity through acculturation has been explored by Schwartz, Montgomery, and Briones (2006), as well as its relationship to mental health (Bhugra, 2004). These issues may be hard to address using the concept of cultural identity in the DSM-IV OCF, which includes a limited number of subcomponents with unclear interdependence: cultural reference group, language, cultural factors in development, involvement with culture of origin, and involvement with the host culture (Lewis-Fernández, 1996). In the BCI, the meaning of cultural identity for the person is explored in more depth. However, because of the limited number of participants in this study, more research on differences between the usefulness of cultural identity compared to cultural explanations of illness is required in order to make more firm statements, or confirm our results.
The BCI proved to be a practical tool, partly because of its relatively limited length and good comprehensibility. In the Dutch centre for transcultural psychiatry, the outcomes of the BCI have been incorporated into the standard clinical assessment and are included in patients’ medical files. Since the completion of the research project in 2006, the role of the BCI in the centre has increased. In 2010, 99% of patient files included a BCI (incomplete assessments and reentries excluded). As a consequence, every update of a patient’s treatment evaluation is made with consideration of the cultural assessment of the OCF.
Based on psychiatric evaluations of the OCF in Spain, Caballero Martínez (2009) suggests that even within a limited timeframe, a minimal procedure is still necessary in order to obtain cultural information during standard clinical assessment and to incorporate the information acquired into clinical reports. Caballero Martínez states that clinicians need to have a baseline level of cultural knowledge about the patient, asking empathically when cultural doubts are detected, and planning an extra interview when cultural doubts remain (2009, p. 511). The author also criticizes the lack of “clear connection between the OCF and other formulations of psychiatric cases” (2009, p. 510), on the basis that this leads to it being more of an academic exercise than a practical tool. In the Dutch centre where this research took place, the BCI is administered following a psychiatric assessment. A summarized assessment of the BCI is then made and supplemented with recommendations for diagnosis and treatment, which is then incorporated in the medical files. Both assessments (psychiatric and the BCI) are discussed in formal multidisciplinary team meetings, leading to the initial treatment plan. The BCI therefore, has a practical application in this clinical context. Furthermore, apart from its use in transcultural psychiatry centres, the BCI is also being applied in more general health care practice in the Netherlands; how this is done, and to what effect, is something that must be investigated further.
The BCI is not merely a set of questions; we consider it a tool to be used for clinical ethnographic exploration, in accordance with how others regard the OCF (Bäärnhielm & Scarpinati Rosso, 2009; Lewis-Fernández & Díaz, 2002). This implies that the interviewee is the potential cultural expert and that the interviewer must ask questions to encourage the interviewee to speak about his or her cultural background. The BCI is meant to be the starting point of a conversation, leaving space for patients to enhance their answers, especially when the interviewer notices a strong emotional response to the questions. When used in an ethnographic way, the interview starts from the microcosm of the interviewee in order to gather a holistic view on mental health problems and the context in which they have been generated and maintained. In this study, the interviewer was restricted to administer all questions literally; in ethnographic research, however, the interviewer uses his or her own words to enter into a dialogue. In future development, a guide to the BCI questions, including the main topics of the OCF and the purpose of the questions, could be included in the general BCI tool.
Although the BCI has a similar aim as the Cultural Formulation Interview (CFI) included in the DSM-5 (American Psychiatric Association, 2013), there are important differences. First, the CFI is meant to be used prior to the psychiatric assessment, while the BCI is used afterwards. The CFI begins with questions concerning the cultural definition of the mental health problems for which a patient is seeking help, while the BCI initiates with questions concerning cultural identity, the first component of the DSM-IV OCF (Aggarwal, 2016). Mental health problems in this context have already been elicited through a psychiatric assessment. Second, the CFI offers a broad overview of the influence of culture on mental health problems through 16 questions, which can be supplemented by a selection of 12 supplementary modules on different CFI topics, while the BCI offers a broad scope on the cultural context of mental health issues through 27 questions. The core of the CFI therefore aims to achieve a broad overview of a cultural contextualization of mental health problems, which could be expanded upon using supplementary modules, while the character of the BCI is that of an in-depth analysis of the cultural context. Third, in the field trial of Aggarwal, Nicasio, DeSilva, Boiler, and Lewis-Fernández (2013), the time required to complete the CFI was 15 minutes (excluding the use of any supplementary modules), while the BCI in this study needed 80 minutes (for practical reasons, in clinical practice today it is scheduled for 45 minutes).
In sum, the CFI aims to draw an inventory of the cultural background of patients’ mental health problems in 15 minutes prior to a psychiatric assessment, while the BCI offers an in-depth cultural focus taken after the mental health problems have been elicited, and takes three times longer than the CFI to complete. It should be taken into account, however, that when a clinician conducting the CFI chooses to use the supplementary module on cultural identity, which contains 34 questions, probably more time will be needed than for the BCI. Finally, the BCI has proven its usefulness in clinical practice for more than 10 years, while clinical evaluation of the CFI still needs to be published. A comparison between a CFI group and a BCI group is recommended for further research.
The promising results in our study have to be interpreted in light of at least four limitations. Firstly, the number of patients was insufficient to test for statistically significant differences between the BCI and the CI. The small sample also calls for expansion of the number of patients used in future inquiries. Secondly, there was a bias in terms of the involvement of the developer of the BCI, who was also the coder for the comprehensibility section of the BCI and CI questions. Another limitation was that the research location is a mental health care centre exclusively for refugees, asylum seekers, and migrant workers, who are not representative of a general patient population in transcultural psychiatry. As such, the data might have been biased by the nature of the psychopathology that these particular patients showed. Many of them had been referred to the centre after years of mental health care in nonspecialized mental health care units. Disappointment over previous treatments might have influenced their judgement of the BCI. A final limitation was the difficulty in generalizability and the lack of representativeness: the limited duration of the research period for data collection resulted in the inclusion of a selection of patients who do not represent the entire actual patient population of the centre, while the ethnic origin of both samples of patients differed considerably (as the ethnic composition of the refugees in the Netherlands differed between both periods of data collection). There may also have been a bias due to the interpreters that were used. The limitations of this pilot study call for a replication and expansion of the study in future inquiries.
Conclusion
This research has shown that the objection that implementation of a questionnaire that leads to a cultural formulation takes too much time to be used in clinical practice can be addressed through use of the shorter BCI. This implies that it is possible for mental health institutes to implement the OCF. The BCI is still a lengthy assessment tool, though the time needed to administer it is much reduced compared to the CI, and the time spent is justified by the wealth of information obtained about the cultural context of patients’ mental health problems. This study has given evidence that, without losing its usefulness for the sake of valid diagnosis, the BCI offers higher feasibility than the longer CI. Despite the worldwide underutilization of the OCF, in a Dutch centre for transcultural psychiatry we have managed to incorporate the BCI into the standard clinical assessment procedure for more than 10 years. A fully employed cultural anthropologist conducts several BCIs every day, resulting in almost complete coverage of OCFs among patients who have been referred to the centre. The promising results of these pilot data could offer an encouraging impulse for the culturally sensitive treatment of mental health problems, though it requires confirmation from other studies around the globe.
Footnotes
Acknowledgements
We thank all the patients that have participated in this study and Zoe Goldstein for the editing in English. Data can be accessed by contacting the first author by email.
Ethical Approval
Ethical approval was obtained for the study at the University Medical Center Groningen of the University of Groningen.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding by Fonds NutsOhra, Stichting tot steun VCVGZ, and Commissie Onderzoek en Programma-Evaluatie GGZ Drenthe Mental Health Care.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.