
Abstract
Sleep disturbances are often referred to as the hallmark of Post-Traumatic Stress Disorder (PTSD). Although PTSD is prevalent in refugees, studies on sleep disturbances in trauma-affected refugees are scarce. This article presents the results of two studies: a systematic review of the literature on treatment of sleep disturbances in adult trauma-affected refugees and a study of the role of sleep disturbances in the PTSD symptom structure. Study 1, the literature review, identified five studies on treatment of sleep disturbances: four studies were on pharmacological treatment and one study on music therapy. The identified studies had small sample sizes and few carried out statistical analysis. It was not possible from the available literature to recommend any specific treatment of sleep disturbances. In Study 2, a clinical sample of 752 refugees, fulfilling criteria for PTSD and enrolled in treatment at the Competence Centre for Transcultural Psychiatry, Denmark, completed the Harvard Trauma Questionnaire (HTQ) before and after treatment. To determine item discrimination, the data was tested with a Rasch model. 99.1% reported trouble sleeping and 98.7% reported recurrent nightmares. The Rasch analysis displayed fit residuals of 0.05 for trouble sleeping and –1.16 for nightmares, indicating sufficient discrimination. Trouble sleeping and nightmares proved important parts of the HTQ response structure. This study indicates that sleep disturbances are a prominent part of the PTSD symptom structure in refugees but that research on treatment of sleep disturbances is limited. Further research on sleep disturbances in trauma-affected refugees is therefore needed.
Introduction
By the end of 2016, the United Nations High Commissioner for Refugees (UNHCR) estimated that a total of 65.6 million people were forcibly displaced worldwide as a result of persecution, conflict, generalized violence and/or human rights violations. Approximately 22.5 million people were refugees (UNHCR, 2016). Although refugees are a heterogeneous group, for example, in terms of country of origin and cultural background, they share the experience of being forcibly displaced from their homes. Trauma-affected refugees are typically characterized by an extensive trauma history; many have faced prolonged and repeated trauma, including torture, rape and combat atrocities, and often conflict-related death of family members. Often the traumatic experiences continue during migration and after migration. Post-migration stressors, such as uncertainty concerning the safety of relatives, continued unsafe situations in home country, uncertainty concerning asylum, residence permit, language difficulties and perceived racism, may add to the previous traumatic experiences and contribute to the development and maintenance of symptoms of trauma-related disorders like Post-Traumatic Stress Disorder (PTSD) (Boynton, Bentley, Strachan, Barbato, & Raskind, 2009; Buhmann, 2014; Silove & Ekblad, 2002). It is estimated that roughly 30% of the world’s refugees suffer from PTSD, and often this is in a more chronic form compared to other populations suffering from PTSD (Boynton et al., 2009; Steel et al., 2009). It has been argued that clinical guidelines for PTSD treatment cannot be assumed to apply to trauma-affected refugees in general because these guidelines derive from research on North American and European trauma-affected populations with single or few traumatic experiences and without the specific experiences of refugees (Crumlish & O’Rourke, 2010; Palic & Elklit, 2011). Hence, clinical trials concerning PTSD in this specific population of trauma-affected refugees are needed.
Sleep disturbances
Sleep disturbances are often referred to as the hallmark of PTSD (Germain, 2013; Maher, Rego, & Asnis, 2006; Nappi, Drummond, & Hall, 2012; Schoenfeld, Deviva, & Manber, 2012; Spoormaker & Montgomery, 2008). Sleep disturbances encompass problems initiating and maintaining sleep (insomnia), nightmares, interrupted sleep, early awakening and, as a consequence, reduced length and quality of sleep.
Sleep disturbances constitute a core symptom of PTSD and a focus for treatment. As many as 70–87% of persons suffering from PTSD describe sleep disturbances (Germain, 2013; Maher et al., 2006; Miller, 2008; Schoenfeld et al., 2012; Taylor, Freeman, & Cates, 2008). However, the prevalence of sleep disturbances in trauma-affected refugees is undocumented. In particular, it is not known whether refugees have a different rate of sleep disturbances than other trauma-affected populations.
The frequency of nightmares has been found to have a strong correlation with a diagnosis of PTSD (Hinton, Hinton, Pich, Loeum, & Pollack, 2009; Maher et al., 2006; Schoenfeld et al., 2012). In trauma-affected populations, sleep disturbances are hypothesized to contribute to the etiology of PTSD rather than being only a secondary symptom (Pace-Schott, Germain, & Milad, 2015; Spoormaker & Montgomery, 2008). Untreated sleep disturbances can maintain and exacerbate PTSD symptoms. Sleep disturbances may also affect the efficacy of first-line PTSD treatment and constitute a risk factor for poor outcome of psychiatric treatment (Germain, 2013; Maher et al., 2006; Schoenfeld et al., 2012). Furthermore, effective treatment to enhance sleep consolidation may accelerate recovery in PTSD (Germain, 2013; Maher et al., 2006; Nappi et al., 2012; Pace-Schott et al., 2015; Schoenfeld et al., 2012; Spoormaker & Montgomery, 2008). The high frequency of sleep disturbances and the influence on treatment response highlight the importance of improving sleep for patients suffering from PTSD (Pace-Schott et al., 2015).
Several studies have been published on the subject of treating sleep disturbances in war veterans and civilians suffering from PTSD (Byers, Allison, Wendel, & Lee, 2010; Germain et al., 2012; Raskind et al., 2003, 2007; Taylor et al., 2006; Taylor, Martin et al., 2008; Thompson, Taylor, McFall, Barnes, & Raskind, 2008). However, studies on sleep disturbances in refugees suffering from PTSD are scarce, and there is no formal overview of the literature concerning treatment of sleep disturbances in trauma-affected refugees (Boynton et al., 2009). As mentioned above, clinical guidelines for PTSD treatment, derived from research on other trauma-affected populations, fail to account for the prolonged and repeated stress experienced by refugees and thus cannot be assumed to equally benefit the refugee population. In our clinical work with trauma-affected refugees at the Competence Centre for Transcultural Psychiatry (CTP), nightmares and interrupted sleep are some of the most frequently reported complaints.
The article aims to address the relationship of sleep disturbances to PTSD among refugees through two complementary studies. First, we review the existing literature on treatment of sleep disturbances in adult refugees with PTSD. Second, based on PTSD questionnaire responses from a clinical sample of adult refugees, we investigate the role of sleep disturbances in the symptom structure of PTSD. Finally, we examine baseline data on sleep disturbances and evaluate the changes in the symptom structure during psychopharmacological and psychotherapeutic treatment of PTSD.
This article is the first to review the literature on treatment of sleep disturbances in adult trauma-affected refugees and the first to explore sleep disturbances in trauma-affected refugees in a large sample. Results from the two analyses can indicate whether sleep disturbances are a prominent part of PTSD in trauma-affected refugees and whether evidence for treatment exists.
Method
Between May 2014 and December 2014 the PubMed, Cochrane database, PsychINFO and Embase were systematically searched using the terms PTSD, refugee, sleep, sleep disturbance, sleep disorder, nightmare and insomnia. The terms were searched in different combinations, both with and without truncation, as MeSH terms and as free text.
A total of 70 articles were identified. The first author read all abstracts, and the articles were included in the final assessment if they included an intervention for sleep disturbances in trauma-affected refugees diagnosed with PTSD (≥18 years). Articles were excluded if sleep and/or nightmares were not evaluated and explicitly mentioned as an outcome measure.
No studies were excluded on grounds of language.
Results
Overview of the literature on treatment of sleep disturbances in refugees suffering from PTSD
Studies on pharmacological treatment
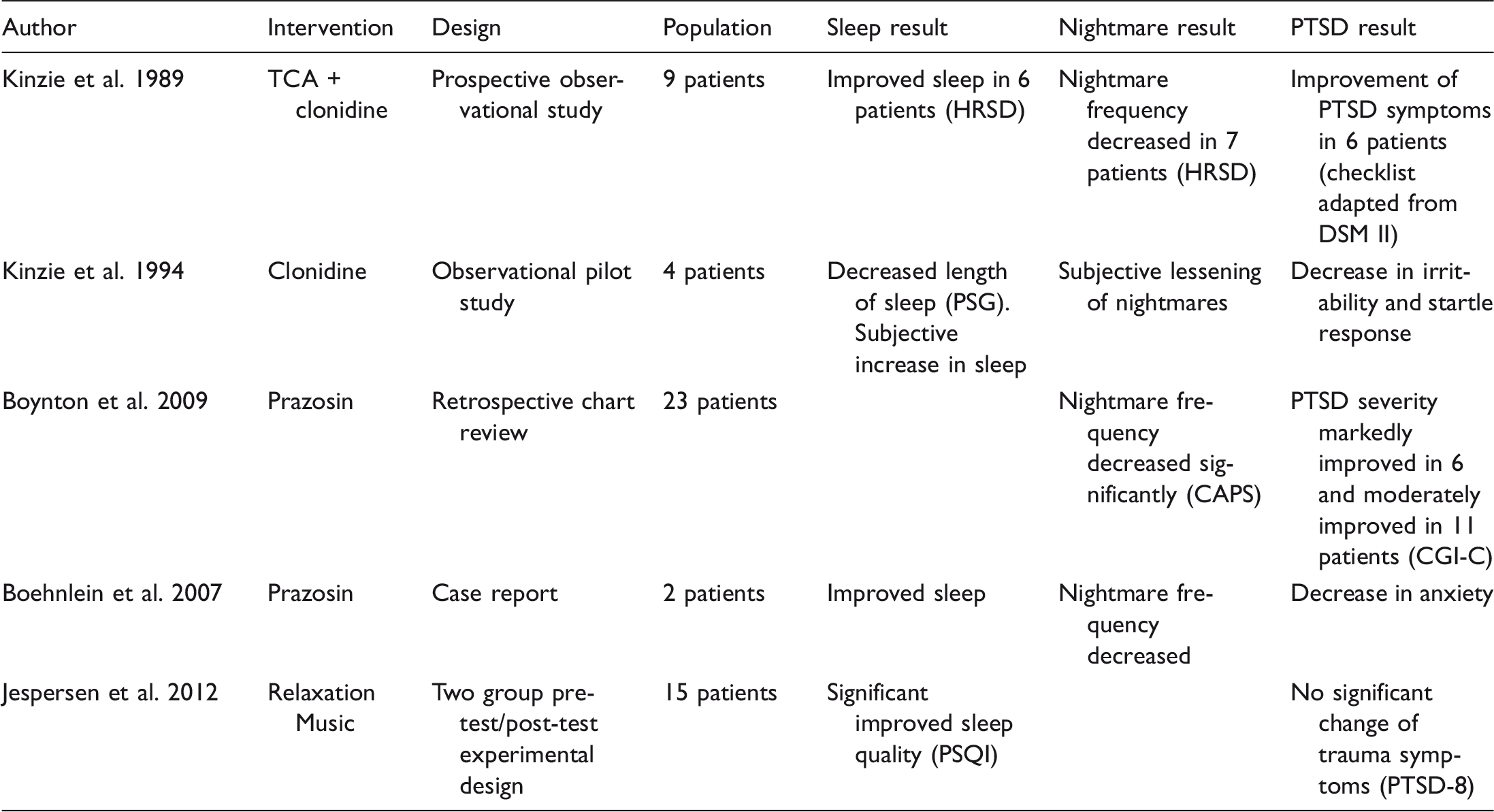
In this section, the four studies on pharmacological treatment will be presented according to level of evidence, with prospective studies first, then retrospective studies, and lastly case studies. Prazosin was used as intervention in one study, clonidine in two studies, and prazosin and clonidine were combined in one study. Prazosin is an alpha1-adrenergic receptor antagonist and is used to treat hypertension and benign prostatic hypertrophy in the USA. Alpha1- adrenergic activity is associated with fear, startle and sleep responses. Patients with PTSD have an increase in adrenergic activity, thus suggesting that an alpha adrenergic antagonist can be effective in treating some symptoms of PTSD, particularly arousal symptoms, such as nightmares and startle reactions (Boehnlein & Kinzie, 2007; Green, 2014; Taylor & Raskind, 2002). Clonidine is an alpha2-adrenergic receptor agonist that is used as an anti-hypertensive drug in the USA. Activation of the alpha2 receptor may be beneficial for PTSD symptoms by down-regulation of noradrenergic outflow and as such to treat hyperarousal symptoms of PTSD and to block an elevated startle reaction (Aurora et al., 2010; Boehnlein & Kinzie, 2007; Taylor & Raskind, 2002).
In a prospective study, Kinzie et al. (1989) analysed data from nine patients diagnosed with PTSD who were treated with tricyclic antidepressant (TCA) and clonidine as add-on. Patients were scored on a checklist for PTSD (adapted from DSM III) and the Hamilton Rating Scale for Depression (HRSD) by the attending psychiatrist at the entrance to the study and subsequently every 6 to 8 weeks. In Hamilton scores, Kinzie et al. found that nightmares lessened in seven patients, sleep improved in six patients and complete recovery from insomnia occurred in five patients. PTSD symptoms improved in six patients (Kinzie & Leung, 1989).
In a second prospective observational study, Kinzie, Sack, and Riley (1994) analysed data from four patients diagnosed with PTSD and depression treated with clonidine. The patients had two sleep assessments conducted before and after treatment. The assessments consisted of polysomnograph (PSG) recordings and subjective sleep and nightmare reports. All patients reported a subjective increase in sleep and a lessening of nightmares post-treatment and a general decrease in irritability and startle response. The PSG data, however, showed that total sleep time was slightly reduced in all individuals post-treatment.
In a retrospective chart review, Boynton et al. (2009) analysed data from 23 refugees diagnosed with chronic PTSD who were treated with prazosin as add-on to their usual psychoactive medications (for example, selective serotonin reuptake inhibitors, tri-cyclic antidepressants, benzodiazepines, antipsychotics, valproic acid, trazodone), 95.7% suffered from comorbidity of depression. Nightmare severity (intensity and frequency), as measured using the Clinician Administered PTSD Scale (CAPS), and overall improvement of PTSD symptoms on the Clinical Global Impressions-Change (CGI-C) were assessed retrospectively based on data recorded in the patients’ chart by an independent psychiatrist. The scores on recurrent distressing dreams in CAPS decreased significantly during the course of 8 weeks of prazosin treatment. On the CGI-C, 6 patients were rated as markedly improved and 11 were rated as moderately improved (Boynton et al., 2009). The study concluded that, among severely trauma-affected refugees, nightmares may play a central role in the presentation of PTSD symptoms (Boynton et al., 2009). Boehnlein et al. (2007), in an article on noradrenergic activity in PTSD, described two cases where refugees were treated with prazosin causing a reduction in frequency of nightmares. In both cases they found improved sleep accompanied by decrease in anxiety and general state (Boehnlein & Kinzie, 2007).
Studies on non-pharmacological treatments
One non-pharmacological study was identified. In a two-group pre-test/post-test experimental design, Jespersen et al. (2012) analysed data from 15 refugees who suffered from sleep problems and trauma symptoms. The participants were assigned to either a control group or a three-week intervention with relaxation music. The music was played through a music player designed for use in bed, with a bar above the pillow and two small loudspeakers at each side of the head. The Pittsburgh Sleep Quality Index (PSQI) was used to measure quality of sleep pre-treatment, weekly and three weeks post-intervention. The PTSD-8 questionnaire (PTSD-8) was used to assess PTSD symptoms pre- and post intervention. The ‘How do you feel’ questionnaire (HDYF) was used to measure well-being pre- and post-intervention. Using a paired sample t-test, Jespersen et al. (2012) showed a significant improvement in global sleep quality (PSQI) in the intervention group; significant improvement on the component of subjective sleep quality and sleep latency. They found no significant change of PTSD symptoms on PTSD-8. Wilcoxon Signed-Rank test showed significant change in well-being on HDYF. Furthermore, they found a correlation between improved sleep quality and improvement in well-being (Jespersen & Vuust, 2012).
Methods
Setting and Sample
The Competence Centre for Transcultural Psychiatry, Denmark (CTP) is a tertiary outpatient clinic. The majority of the trauma-affected refugees referred to CTP are from Afghanistan, Iraq, Iran, former Republic of Yugoslavia and Lebanon. Approximately one-half require an interpretor. Approximately one-half have experienced torture (Buhmann, 2014). The population’s immigration status is diverse; all patients have obtained a residence permit but some of the patients have temporary residence, some have permanent residence and some have Danish citizenship. All respondents were adult refugees undergoing psychiatric treatment at CTP from 2008 to 2012 and fulfilling the criteria for PTSD (F 43.1), according to International Classification of Diseases, 10th edition (ICD-10), based on a clinician’s diagnosis. Patients with known alcohol or substance abuse (defined by ICD-10 F.1 × .24–F1 × .26) or patients suffering from serious psychotic disorder (defined by ICD-10 diagnosis F2x and F30.1–F31.9), based on structured clinical interviews, were not offered treatment at CTP.
The baseline data included patients fulfilling the above criteria and who participated in three trials during the period 2008–2012. The resulting sample consisted of a total of 752 patients.
The analysis of pre- and post-treatment prevalence included a subset of patients where three ratings were available. The Danish Ethics committee approved all three trials. The resulting sample consisted of a total of 386 patients. These patients received a standard combination of psychopharmacological and psychotherapeutic intervention, but with variation depending on the objective of the ongoing study at the time of referral (Buhmann, 2014; Vindbjerg, Klimpke, & Carlsson, 2014).
In the above-mentioned trials, the treatment consisted of both psychopharmacological treatment and psychotherapy. The patients initially all received weekly doctors’ appointments over a 2 month period with a focus on psychopharmacological intervention and psychoeducation. For the following 4 months, the patients attended weekly psychotherapy sessions and monthly doctors’ appointments. A separate rating was completed at the transition between first and second treatment stage.
Measures
As a standardized assessment routine at CTP, patients are administered a number of psychometric questionnaires, including the Harvard Trauma Questionnaire (HTQ; Mollica et al., 1992); the Hopkin’s Symptom Checklist-25 (HSCL-25); Hamilton Depression and Anxiety Scales; the SCL-90 somatization section; visual analogue scales (VAS) for back pain, pain in the upper and lower extremities and headache; Sheehan Disability Scale; Global Assessment of Functioning, Function and Symptom section; and the WHO QOL-5 on Quality of Life.
The HTQ-part IV, which is used in this analysis, features 16 items based on the 17 symptoms of the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV; American Psychiatric Association, 1994). Each item assesses to which degree respondents were bothered by a particular symptom during the last week. Responses are rated on a four-point scale, with the response categories not at all (1), a little (2), quite a bit (3) and extremely (4). It should be noted that HTQ has been applied and validated internationally (de Fouchier et al., 2012; Hollifield et al., 2002; Lhewa, Banu, Rosenfeld, & Keller, 2007; Mollica et al., 1992, 2014).
Data analysis
Means were calculated for each of the items, as well as for the full HTQ scale, in order to describe, first, the extent of sleep disturbances and recurrent nightmares in the sample and, second, how sleep disturbances and recurrent nightmares corresponded to the total scale score. As sleep-related symptoms had been found, in clinical experience and previous analyses, to be among the most prevalent symptoms at CTP, they were expected to display a somewhat limited range, which in turn would limit the item-rest score correlation (Macdonald & Paunonen, 2002). To circumvent this problem, we tested the data with a Rasch model, using the software program RUMM2030 (Andrich & Sheridan, 2010). We did not expect the unmodified HTQ scale to conform to all requirements of a Rasch model, however, fit residuals can still give an indication of the individual items’ contribution to the fit. A negative fit residual means the item displays higher discrimination than predicted by the model, and vice versa for a positive fit residual. As a guiding principle, a positive fit residual above 2.5 indicates poor discrimination (RUMM Laboratory, 2009).
Item characteristic curves were generated for each symptom, to illustrate the distribution and discrimination of the data, as well as the theorized response function across a wider range of PTSD than represented by the current sample.
As a last step in the analysis, change in sleep symptoms during treatment was assessed. Means were calculated for each of the two sleep-related items, as well as for the means HTQ-score, at baseline (rating 1), 2 months (rating 2) and 6 months (rating 3). Mean changes from rating 1 to rating 2, as well as rating 1 to rating 3, were calculated, allowing a comparison of the extent and rate of change of the two sleep-related symptoms and the mean HTQ-score.
Results
Baseline prevalence of sleep-related symptoms on the HTQ

Note: N = 752.
Rasch-model based item-fit indices
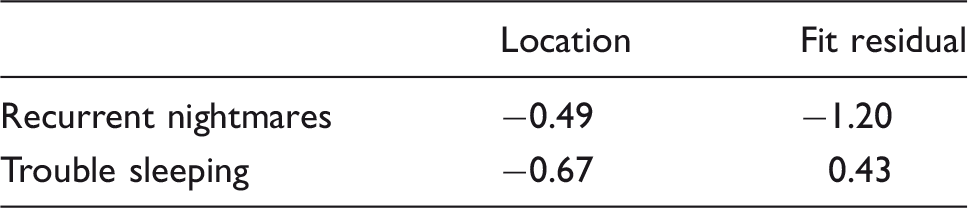
Note: High negative fit residual indicates high discrimination. N = 752.
Item characteristic curves for the sleep-related items are presented in Figure 1. While responses (marked by dots) are primarily distributed on the right side of the figure (corresponding to a high trait level in the sample and a low threshold for endorsing the particular item), the middle and left part of the curve illustrates the model’s prediction of higher item discrimination for persons with a lower trait level. The steeper slope at the middle of the graph indicates that item-rest correlations for both of the sleep-related items would be higher in a sample with this trait level, that is, in a sample of somewhat less traumatized patients (patients with single or few traumatic experiences) than the current sample.
Item characteristic curves for item 3, Recurrent nightmares, and 8, Trouble sleeping.
Symptom change during treatment

Note: Based on ratings from 386 patients who completed both the 1st, 2nd and 3rd rating. All differences are significant at the 0.001 level.
Discussion
The overview of the literature revealed only five studies on treatment of sleep disturbances in trauma-affected refugees. Four studies investigated pharmacological treatment: two studies on clonidine; and two on prazosin. All four studies showed reduction in nightmares, improved sleep and improvement of PTSD symptoms. One study on treatment with relaxation music was identified. This study showed improved sleep, but no significant reduction of PTSD symptoms. Generally all the studies have limitations due to small sample sizes and limited statistical power. In the case reports, only qualitative descriptions were provided; no rating scales were used to describe outcome and no statistical analysis were done (Boehnlein & Kinzie, 2007; Kinzie et al., 1994). In the retrospective study and the prospective study, changes were reported on rating-scales (Boynton et al., 2009; Kinzie & Leung, 1989). Statistical analyses were performed in only one study on pharmacological treatment, which showed significant reduction of nightmare frequency although statistical analysis was not carried out to determine reduction of PTSD severity (Boynton et al., 2009). All studies lacked a placebo control group. No studies allow for causal conclusions and the therapeutic effect, observed from baseline to evaluation, can neither with certainty be attributed to prazosin nor clonidine.
Jespersen et al. (2012) used rating scales and performed statistical analysis that found significant improved sleep quality (PSQI), improved well-being, but no significant change of PTSD symptoms (Jespersen & Vuust, 2012). The study found a correlation between sleep and well-being, yet this does not allow for causal conclusions. There is a need for further studies on music therapy to determine the effect on sleep disturbances and PTSD symptoms in general.
No intervention studies, with a pre- and post-treatment outcome measure on sleep disturbances, were identified concerning the use of the newer antidepressants serotonin reuptake inhibitors (SSRIs), which are recommended as first-line medications for treatment of PTSD (Maher et al., 2006). SSRIs and add-on treatment with mirtazapine have been reported to reduce frequency and intensity of nightmares in 300 refugees suffering from PTSD (Lewis, 2002). In a large-scale trial on treatment of trauma-affected refugees at CTP, sertraline and add-on treatment with mianserin showed significant improvement of sleep on all measuring scales. It was not possible to separate the influence of the different treatment modalities, and it is only hypothesized that the change could be caused by treatment with mianserin due to an inhibition of histamine H1 receptors by mianserin (Buhmann, 2014; Buhmann, Mortensen, Nordentoft, Ryberg, & Ekstrøm, 2015). Some antidepressants, however, do not improve sleep and may even cause a worsening depending on receptor stimulation. Attention must be paid to specific effect of antidepressants on REM sleep, since several antidepressants are associated with suppression of REM sleep and sleep fragmentation (Maher et al., 2006; Mayers & Baldwin, 2005; Pace-Schott et al., 2015).
Similar to SSRIs, psychotherapy, primarily cognitive behavioural therapy (CBT) is recommended as first-line treatment of PTSD (Maher et al., 2006). No intervention studies with a pre- and post-treatment outcome measure concerning psychotherapy, aiming to either reduce nightmares and/or improve sleep, were identified. Imagery rehearsal therapy (IRT) for treatment of disturbing nightmares has shown promising results for other groups of patients suffering from PTSD (Cook et al., 2010; Forbes, Phelps, & McHugh, 2001; Krakow et al., 2000; Krakow, Hollifield, et al., 2001; Krakow, Johnston, et al., 2001; Lu, Wagner, Van Male, Whitehead, & Boehnlein, 2009)., and there is a lack of studies on the effect of IRT in trauma-affected refugees
When first-line treatment fails to relieve sleep disturbances, antipsychotics or benzodiazepines are often used (Maher et al., 2006; Schoenfeld et al., 2012). No studies were identified concerning the use of antipsychotics in the treatment of sleep disturbances in trauma-affected refugees. In studies on other populations with PTSD, antipsychotics have shown promising results with sleep disturbances, including frequent nightmares, but antipsychotics are not recommended for the treatment of sleep disturbances and should be used with caution due to significant potential adverse effects (for example, weight gain, diabetes mellitus, tardive dyskinesia). There is a lack of long-term follow-up studies on treatment with antipsychotics in patients suffering from PTSD (Byers et al., 2010; Maher et al., 2006; Miller, 2008; Schoenfeld et al., 2012). No studies were identified concerning the use of benzodiazepines in the treatment of sleep disturbances in trauma-affected refugees. The use of benzodiazepines is not recommended and caution is advised when prescribing due to the risk of dependency, withdrawal symptoms and cognitive impairment (Maher et al., 2006; Miller, 2008; Schoenfeld et al., 2012).
When studying trauma-affected refugees and psychopharmacological treatment, one should keep in mind the acceptance of the medical treatment (Kortmann, 2010). The experience at CTP, from a previous trial focusing on PTSD and comparing psychopharmacological treatment with psychotherapy, indicated a small but significant advantage for psychopharmacological treatment. At the same time, however, 11–16% of the patients discontinued the psychopharmacological treatment because of adverse reactions. Furthermore, the mean dose of medication was quite low compared to other trauma-affected populations. This trial suggests that while psychopharmacological treatment is definitely possible, education regarding the medicine should be emphasized, and a slow titration may be necessary to minimize adverse reactions (Buhmann, Nordentoft, Ekstroem, Carlsson, & Mortensen, 2015).
Based on the literature reviewed, it is not possible to recommend any specific treatment of sleep disturbances in refugees with PTSD. There is a lack of randomized clinical trials of high quality, with sample sizes that allow for statistical power calculations to determine effects of and differences between both pharmacological and non-pharmacological treatment modalities of sleep disturbances in refugees suffering from PTSD. The lack of studies concerning psychoeducation, psychotherapy, as well as pharmacological treatment with antidepressants and antipsychotics, leaves clinicians without validated clinical guidelines for treatment of sleep disturbances.
The questions of how sleep disturbances should be treated and whether sleep disturbances and nightmares must be targeted for intervention independently of other symptoms of PTSD remain unanswered by the review of the literature concerning treatment of sleep disturbances in trauma-affected refugees.
Sleep-related symptoms in the PTSD symptom structure
Analysis of the HTQ confirmed that sleep disturbances and nightmares are among the most prevalent symptoms in trauma-affected refugees treated at CTP. However, an item-rest correlation of 0.33 appears to indicate that the symptom of sleep disturbances provides a poor contribution to the measurement of PTSD. The item-rest correlation for nightmares was slightly higher, at 0.42. The results of the Rasch analysis clearly differ in this regard. With a fit residual of only 0.43, trouble sleeping followed the predicted relationship to the level of PTSD, providing sufficient discrimination. For nightmares, the discrimination was above that predicted by the model. Thus, trouble sleeping and particularly recurrent nightmares constitute important parts of the HTQ response structure in this sample of refugees. This, to some extent, likely reflects the role of these symptoms in PTSD. On the other hand, it may also be partly ascribed to the intelligibility and cultural familiarity of the sleep-related questions.
It should be noted that the above results are only as valid as the construct of PTSD as assessed by the HTQ (in its various translations; Hollifield et al., 2002). The insufficient discrimination displayed by three of the items is enough to indicate compromised validity in the scale. If the scale were measuring something essentially different from PTSD, then our results would apply to that construct, rather than PTSD.
Given the relatively low discrimination of the sleep-related items in this sample, it is all the more remarkable that they display some of the largest changes during treatment. One possible explanation for this outcome is that these symptoms respond particularly well to pharmacological treatment, in this case sertraline and/or mianserin. This would also account for the particularly high rate of change during the initial 2 months of treatment, where focus is on the introduction of these drugs. Furthermore, it is possible that such early improvement of sleep acts as a catalyst in the improvement of the remaining PTSD symptoms (Germain, 2013; Spoormaker & Montgomery, 2008).
In line with the US NIMH Research Domain Criteria (RDoC) project to create a framework for research on pathophysiology, it would be of interest to examine the underlying mechanisms of dysfunction in PTSD and sleep disturbances, including the potential role of REM sleep disturbances in the aetiology of PTSD (Insel et al., 2010). There also may be value in a research approach that looks at sleep disturbances independent of diagnosis, rather than focusing on studies based on diagnostic criteria. REM sleep fragmentation has previously been found to be the main abnormality of sleep in PTSD patients. This suggests the potential relevance of further research on the specific role of treatments that reduce REM sleep disruptions (Germain, 2013; Mellman, Bustamante, Fins, Pigeon, & Nolan, 2002; Mellman, Pigeon, Nowell, & Nolan, 2007; Pace-Schott et al., 2015; Spoormaker & Montgomery, 2008). Additionally, an RDoC-like approach would consider whether the construct of PTSD is an artificial grouping of symptoms, and would point toward the potential value of studying sleep disturbances independent of diagnosis.
Limitations
Depression is often found as a comorbid factor to PTSD. This can influence the symptoms, the ratings and the treatment of sleep disturbances in trauma-affected refugees. This aspect has not been discussed in the current article. Additionally, there may be cultural variations in how self-ratings scales are answered, that influence the results. The lack of studies constitutes a major limitation for the literature review. The quantity and quality of the existing studies does not allow for the application of clinical guidelines on treatment of sleep disturbances in trauma-affected refugees.
Conclusion
This study, combining a systematic literature review and empirical findings, shows that sleep disturbances are a prominent part of PTSD in adult refugees but that there is little research on relevant treatment approaches. It is not possible from the available literature on refugees to recommend any specific treatment of sleep disturbances. There is an evident need for research on the effect of different treatment modalities on sleep disturbances in trauma-affected refugees. In particular, further research is needed on the use of mianserin, which has shown promising results in treating trauma-affected refugees at CTP, as well as on IRT, which has shown promising results treating other trauma-affected populations. Such research would ideally include randomized controlled trials with large sample sizes. The assumption that treatment and improvement of sleep disturbances can alleviate general PTSD symptom severity also requires further research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Biographies
Her published works has a focus on trauma-affected refugees, post-traumatic stress syndrome, sleep disturbances and on mental health services research and disparities in service delivery.