
Abstract
People in different cultures have different concepts of the person that underlie self-understanding and self-representation. These concepts influence many aspects of individuals’ life experience, including illness and expectations toward recovery. Psychotherapies aim to promote adaptive change in experience and behavior. This goal is embedded in a social and cultural context that promotes or sanctions a particular notion of personhood. If every system of psychotherapy depends on implicit models of personhood, which varies cross-culturally, then the goals and methods of therapeutic change must consider the cultural concept of the person. This paper reviews cultural concepts of the person in relation to communal values, practices, and systems of thought observed across many African cultural contexts. It presents a practical framework that can inform therapists working with African clients. Many African cultures promote a relational-oriented personhood, in which an individual manifests his or her personhood through connections to three distinct forms of agency: (a) spiritual agency, including God, ancestors, and spirits that influence the person; (b) social agency, including the family, the clan, and the community, with extension to humanity; and (c) self-agency, which is responsible for the person’s inner experience. This distinctive form of personhood underlies concepts of the “normal” person, understandings of mental illness, help-seeking behavior, and clients’ needs and expectations. Implications of this cultural concept of the person for psychotherapy with African clients are discussed.
Introduction
Since the seminal work of Marcel Mauss (1935/1985), a major theme in psychological anthropology has been the concept of the person, understood as a social and cultural construct that underlies self-understanding and self-representation (Christopher, 2007; Knappett, 2005; Smith, 2003). Implicit cultural concepts of the person shape current psychological theories of development and social behavior, psychological assessment, psychopathology, as well as forms of psychotherapy (Hammack, 2008; Kirmayer, 2007). Different cultural contexts lead to different concepts of the person, which in turn, provide ways of interpreting individual experience. Despite much evidence for cultural variation, most approaches to mental health, counselling, and psychotherapy for African peoples are based on Eurocentric concepts of the person.
This article describes a distinctive form of personhood present in many African cultures, and explores how this concept of the person underlies major aspects of mental health in African societies, including understanding of mental illness, help-seeking behavior, and expectations for recovery. Finally, it presents some of the implications of this concept of the person for clinical practice. Attention to the ways that African cultures conceptualize personhood may have important research, clinical, and ethical implications for theory and practice in psychology and psychotherapy.
Concepts of the person and culture
The concept of the person does not refer directly to the self, defined as the locus of self-awareness, introspection, and imagination, but to the cultural construction of the person as a social entity, along with moral and juridical notions of agency and accountability (Appiah, 2005; Kirmayer, 2007; Mauss, 1935/1985). Persons do not exist in isolation; each of us lives and grows up in some specific social and cultural setting. That setting is the context in which we develop our ideas about our own and others’ personhood. Cultural systems influence individual behavior through their effects on one’s way of being-in-the-world. Through this process of enculturation, the individual as a biological entity becomes a culturally meaningful being who is recognized as a person, and hence, as an actor in a social world (Hammack, 2015; Sedikides & Brewer, 2002). One cannot be a person by oneself but only in relation to a social world (Andersen & Chen, 2002; Martin & Bickhard, 2013). Personhood is always grounded in the complexities of consensual understandings and customary behavioral routines relevant to being a person in a given sociocultural context. Such understandings and practices will influence the form and function of the psychological processes that comprise the person as a subject and social actor. As D’Andrade and Strauss (1992) note, the individual’s psyche can be seen as an internalization of culture, while culture can be viewed as an externalization of psyche. Personhood, then, can be understood as a dynamic recursive process in which participation in a given cultural system of meanings, practices, and institutions affords and fosters characteristic psychological tendencies that serve, in turn, to integrate the person into the meanings and practices of a cultural community (Markus & Hamedani, 2007; Markus & Kitayama, 1991).
Cultural and social groups are associated with characteristic ways of being a person in the world. These culturally constructed patterns arise from living one’s life in a particular cultural context. Personhood includes key cultural ideas and values characterizing the person, that is, an understanding of what a person is, as well as a moral sense of how to be a “true” or a “good” person (Narvaez & Lapsley, 2009; Pronin, 2008). Differences in the concept of person are tied to both explicit and implicit norms and tasks that each culture holds for every person, with dimensions or emphases that vary according to gender, developmental stage, and social status or position (Appiah, 2004; Hitlin, 2011).
Concepts of the person in African cultural contexts
This paper does not aim to offer a theory of “African personality” or “African identity,” nor does it pretend to theorize “the person” of all peoples in Africa. Such an ambition would present a misleading view of African peoples and their cultures, for at least four reasons. First, there is no single “African culture”; the African continent has myriad cultures, traditions, and over 2,000 different spoken languages (Heine & Nurse, 2000), each with its own systems of thought, values, and cosmology. Second, African cultures are neither fixed nor static; rather, they are constantly changing. For example, compared to previous generations, young African people today generally endorse traditional cultural beliefs to a lesser extent. Third, each African person has his or her unique ways of engaging with the normative values, systems of thought, and social practices promoted by his or her culture. Sources of individual variation in engaging with one’s own culture include religious beliefs, education level, age, gender, sexuality, and place of living (Kpanake, Sorum, & Mullet, 2016). Fourth, there is a considerable degree of fluidity, intermixing and assimilation of identities and knowledges within and between so-called “Western” and “African” traditions, resulting in a complex and changing melange of influences and cross-currents, both local and global (Mbembe, 2002).
The main goal of this paper is to explore a form of personhood as promoted by many African cultures, and to draw a practical framework that could inform the clinical practices of therapists working with African clients who are engaged in this form of personhood. Being aware of such a cultural form of self-understanding and self-representation allows for a deeper understanding of the system of meanings conferred on mental illness, symptom experience and distress, help-seeking behavior, and expectations of recovery (Kirmayer, 2004, 2007; Moodley & West, 2005; Tseng, 2004).
When exploring cultural concepts of the person in many parts of Africa, one is confronted with a central dynamic of connectedness, defining the person in relation to three types of agency located or elaborated in relation to the social world, the cosmic world, and the self.
Social agency
One fundamental value system promoted by many African cultures is what has been called the Ubuntu system. Ubuntu is a pan-African concept which translates as “personhood” or “humanness” (Ramose, 1999, 2003). Even though Ubuntu is a Zulu (spoken in South Africa, Lesotho, Zimbabwe, Malawi, Swaziland, Botswana, and Mozambique) word, the concept is found in numerous African languages, though not necessarily under the same name: umundu in Kikuyu – spoken in Kenya), bumuntu in Sukuma (spoken in Tanzania), vumuntu in shiTsonga (spoken in South Africa, Zimbabwe, and Mozambique), nunhu in Shona (spoken in Zimbabwe and Mozambique), bomoto in Bobangi (spoken in the Republic of Congo and the Democratic Republic of Congo), and gimuntu in kiKongo – spoken in Angola, Gabon, Republic of Congo, and the Democratic Republic of Congo – (Kamwangamalu, 1999). Cognate terms are also found among the Yoruba – of Nigeria, Bénin, Ghana, and Togo – (Gbadegesin, 1991), and the Akan – of Ghana and Côte d’Ivoire – (Gyekye, 1995). The concept of Ubuntu refers to African values of collective relatedness, interdependence, communality, group solidarity, and conformity; as one Akan (of Ghana and Côte d’Ivoire) saying puts it, “Wiase yi mu yedi no nnoboa [Life is an enterprise of mutual aid] (Wiredu, 2009, p. 16). In the concept of Ubuntu, the self is perceived in relation to the group; that is, individuals are perceived not as entities that are independent from one another, but as part of an interdependent communal system (Kamwangamalu, 1999; Ramose, 1999, 2003).
Ubuntu values are transmitted from one generation to the next by means of core cultural media including fables, proverbs, riddles, and storytelling. This is illustrated in the Ciluba (spoken in the Democratic Republic of Congo) proverb “Bubedi bwa disu mbubedi bwa diulu”, literally translated as “the sickness of the eye is the sickness of the nose,” which means your neighbor’s problem is your problem (Kamwangamalu, 1999). This collective consciousness is strengthened developmentally through rites of passage, which aim to create new social connectedness. For example, among the Maasaï (of Kenya and Tanzania), “young people who have been initiated together become mystically and ritually bound to each other for the rest of their life: they are in fact one body, one group, one community, one people” (Mbiti, 1990, p. 123). This social personhood may not be a once-and-for-all achievement but may deepen or evolve across the lifespan. In describing the Tallensi (of Ghana), for example, La Fontaine (1985, p. 137) notes: “as more social relations are added through life, personhood approaches completion.” The fundamental belief in the concept of Ubuntu is that “umuntu ngumuntu ngabantu”, a Zulu (of South Africa, Lesotho, Zimbabwe, Malawi, Swaziland, Botswana, and Mozambique) saying which, literally translated means “a person can only be a person through other persons” (Shutte, 1993, p. 46). Thus, for many African cultures, being human is not a sufficient condition for being a person. Personhood in these contexts is considered as a reward for contributing to the community. For instance, among the Akan (of Ghana and Côte d’Ivoire), communal involvement such as taking responsibility for the upbringing of relatives or nonrelatives enabled the individual to achieve the status of person, as indicated by references to him or her as oye onipa paa – literally, he or she is “a real person” – (Wiredu, 2009). Conversely, when an individual appears to be selfish, the Akan would say of that individual that he or she is onnye ‘nipa – “not a person” (Gyekye, 2000). This account has an obvious similarity with the Igbo (of Nigeria), for whom chieftaincy title-taking is a way for wealthy people to share their wealth with their community (Ukpokolo, 2009).
From this perspective, there exists a common bond between the individual and the community, and it is through this bond that the person discovers his or her own essence (Hallen, 2009). Hence, for many African cultures, the person cannot be regarded as a separate entity to be understood and dealt with individually, but must always be seen as embedded in a social context. For example, when introducing individuals, the Iraqw (of Tanzania) used to refer to the community they belong to, rather than to their personal identity or accomplishments (Snyder, 2002). This does not mean that there is no sense at all of the person as a separate individual, but self-disclosure or talking about the self is regarded as dangerous and foolhardy (Snyder, 2002). Thus, it is not simply rude, but actually transgressive to ask people in many Western African cultures to elaborate on their personal selves (Fiske, Kitayama, Markus, & Nisbett, 1998). This fundamental basis of personhood in many African cultures has been well presented by Paris (1995), who maintained that separation between the individual and his or her social agency is not possible in numerous African systems of thought. The preeminence of social identity is illustrated by Evans-Pritchard’s (1956) account of a situation in which funeral ceremonies were held for a Nuer (of South Sudan and Ethiopia) man who was thought to be dead, but who lived and later returned to his community. Rather than receiving a warm welcome when he returned, he was considered to be an embodied ghost—not a human person—because, according to his community, his soul had left when they performed the ceremonies for his funeral. Since in this cultural context personhood is explicitly constructed, conferred, and taken away by the community, the individual’s physical presence in the community did not automatically restore his personhood. Within such a framework, depriving some people in Africa of their social identity would be therefore equivalent to outright erasure or annihilation.
Spiritual agency
The notion of spiritual agency refers to the ways that people incorporate invisible entities into their daily life. Cosmology in many African cultures represents life as such a tragedy that the self alone, as a vulnerable and mortal entity, could never achieve its aspirations. Personhood therefore requires the intervention of spiritual entities to secure the person’s protection against malevolent spiritual forces. These spiritual entities—including God, ancestors, divinities, and spirits—constitute forces that constantly influence the course of the person’s life through beneficial or harmful events (Bojuwoye, 2005; Kpanake & Ndoye, 2013; Magesa, 1997).
Apart from God, many systems of thought in Africa locate ancestors on the first level, not because the ancestors are equal to God but because they are intermediaries whose work is highly valued. Ancestors are the closest links that the person has with the spiritual world. They are called by different names depending on one’s ethnic group, such as badimo among the baPedi (of South Africa, Zimbabwe, and Botswana), amadlozi among the amaZulu (of South Africa, Lesotho, Zimbabwe, Malawi, Swaziland, Botswana, and Mozambique), nfosia among the Bamiléké (of Cameroon), and sosso among the Kabyè (of Togo). The ancestors are the “living dead,” members of the kin who have died, but continue to live as “shades” (Berg, 2003; Bojuwoye, 2005). The place of ancestors in the person’s life reflects the belief that the dead person does not wholly disappear (Kalu, 2000). As such, they have profound influence on the individual’s daily life. The role of the ancestor as an active participant in the individual’s life begins before birth. For example, among the Fon (of Bénin and Togo), each foetus is considered to be the result of the ancestor’s “mixing the ball of earth” that is used to form the foetus before it is placed in the mother’s womb (Blier, 1996). The founding ancestor is called djoto among the Fon, which is literally translated as “agent of birth,” and amedjoto among the Ewe (of Ghana, Togo, and Bénin), which similarly means “agent of the person’s birth” (Blier, 1996). Maupoil (1981) explained further that every person possesses a djoto, and as soon as a child is born, one must ask Fa (a divination) which ancestor sent him or her into the world. Accordingly, djoto is believed to fashion the physical and psychological person. Central to this view is the belief that the formation of the person is performed by the ancestor. After birth, the founding ancestor assumes critical roles along the development of the child, including protecting him or her, and overseeing his or her physical, psychological, and moral development.
In many African cultures, ancestors are considered the guardians of family affairs, traditions, ethics, and activities. For instance, among the Tallensi (of Ghana), the Kallabari (of Nigeria), the Lugbara (of Uganda and South Sudan), the Taita (of Kenya and Tanzania), and the Fon (of Bénin and Togo), ancestors are believed to play an active part in individual life, acting as moral guardians and enforcers of the social order (Blier, 1996; Bojuwoye, 2005; Morris, 1994; Paris, 1995). They are omnipresent and their influence is benign and all embracing (Hammond-Tooke, 1989). They act as the guide, the watchperson over the individual, offering protection from seen and unseen malevolent beings, illness, social misfortune, and destroyers of the kinship (Bojuwoye, 2005; Vontress, 2005). The recent widely reported marriage between a young boy and an older woman in Tshwane, South Africa, illustrates the role of the ancestor in the person’s life (Webb, 2013). The case involved Sanele Masilela, an 8-year-old boy and Helen Shabangu, a 61-year-old woman who was already married. The wedding was celebrated 2 months after the boy said his “dead ancestor told him to tie the knot.” The boy’s mother explained: Sanele is named after his grandfather, who never had a white wedding before he died so asked Sanele to get married. He [the ancestor] chose Helen because he loves her... By doing this we made the ancestors happy. If we hadn’t done what my son had asked then something bad would have happened in the family. I didn’t have a problem with it because I know it’s what the ancestors wanted and it would make them happy.
Ancestors are consulted in response to many life events, including rites of passage, marriage, when waiting for a new baby, preparing for hunting, before starting farming activities, searching for a job, as well as in contexts of illness. Depending on the reasons for consultation, the ancestor may be requested to provide blessings, guidance, or protection (Berg, 2003; Kpanake, 2015). Ancestors are not approached only for current challenges, but also to thank them for past good events, such as a prosperous harvest, a birth in the family, a healthy year, and academic or professional success. Rituals are the most common channels of communication used to convey a message to ancestors (Thorpe, 1991). In turn, unexplained somatic symptoms, mental illness, social misfortunes, nightmares, and dreams are among the most common channels that ancestors use to send a message to the person. For example, among the Zulu (of South Africa, Lesotho, Zimbabwe, Malawi, Swaziland, Botswana, and Mozambique), an encounter with a python or a dream about one indicates approval from the ancestors, whereas seeing a mamba is associated with a warning (Cumes, 2004). Verification and validation of the meaning of ancestors’ messages to the person is a key task of traditional healers (Semenya & Potgieter, 2014; Vontress, 2005). This issue will be dealt with in greater detail in what follows.
Self-agency
The importance of social and spiritual agency in the way personhood is characterized in many African cultures should not be understood as implying that such agency overshadows the self. As in other parts of the world, most African cultures recognize a self that differentiates the individual from others with deictic terms that correspond to “I” or “me” (Bloch, 2012; Zahavi, 2009). This self is a locus of agency that is responsible for introspection, feeling, and questioning, and an entity that one is proud of and seeks to improve. The self is responsible for the individual’s social presence, and accommodates the life essence. Moreover, the notion of self in many African cultures transcends its bodily, anatomical, and physiological substrate (Cumes, 2004; Gumede, 1990; Niehaus, 2002). The self in these cultures’ systems of thought may take the form of a physical self, an invisible self, or an environmental self. For instance, one’s clothes, contaminated with one’s smell or sweat, or even a material one has touched, are believed to become an extension of the self and even its substitute (Kpanake, 2015; Niehaus, 2002; Nwoye, 2006). This metonymic process explains why the environment, with which the body is in constant contact and transaction, is viewed as an extension of the body, and hence as an extension of the self (Aina, 2006; Niehaus, 2002; Nwoye, 2006). Following the same logic, in the Zulu culture, it is taboo to leave one’s hair lying around after haircut. One should collect the cut hair and always burn it until nothing is left. It is believed that if one’s hair gets blown away by the wind it might get into the hands of witches who will use it for evil purposes such as making one “mad” (Cumes, 2004; Gumede, 1990). This representation of the self is manifested in many Zulu individuals’ refusal to use urine bottles in hospitals because they are afraid that the contents may fall into the hands of sorcerers (Hammond-Tooke, 1989). Similarly, people in the lower Congo meticulously avoid stepping on someone else’s shadow or having their own shadow stepped on, especially by others with a superior social status. Having one’s shadow stepped on is thought to empower the other person with one’s own self-agency (Jacobson-Widding, 1990). Another powerful cultural belief in the lower Congo is that possessing photographs of other people diminishes the power and life essence of those in the photographs. Indeed, a popular practice among people in the lower Congo is to display pictures of smiling and enthusiastic faces from magazines in order to extract the power and life force from them (Jacobson-Widding, 1990). Such an understanding of the self explains why among the Zulu, malevolent people are believed to be able to use their spiritual powers to bewitch their victims without coming into physical contact with them (Ashforth, 2000). Among the Sotho (of South Africa, Lesotho, Botwana, and Swaziland), for example, should a person die in a road accident, there is concern that further deaths may occur at the same location until a diviner cleanses the location to capture the moya (invisible self) and release it in the family garden (Niehaus, 2002). The same logic of self-understanding is found among the Poroporo (of Tanzania), where annihilation of a witch’s personal identity consists of shaving his or her body hair (Green, 1994). Similar understandings were noted in many cultural groups along the Guinean Gulf where, for instance, placing one’s hand on the head of someone is considered a potential act of sorcery action, especially when it is a stranger who touches the head of a child (Blier, 1996). Among the Ewe (of Ghana, Togo, and Bénin), a ritual called zindo-bo is believed to allow the transformation of the person’s visible body to an invisible one (Blier, 1996). Reflecting the same logic, a Fon (of Bénin and Togo) mortuary tradition has people at the cemetery carve a piece of wood and dress it to represent the deceased and place it in the tomb, otherwise the deceased will “claim” (kill) someone from the community (Blier, 1996). The reasoning behind this tradition closely resembles the well-known case of nueer among Nuer (of South Sudan and Ethiopia), where the view was that the murderer had a spiritual bond with the victim and was so polluted that only a leopard skin priest could cure him (Evans-Pritchard, 1956). Again, one popular belief in many African cultures is that individuals considered to be witches can travel during the night in order to bewitch their victims by transforming themselves into animals and birds like owls, bats, snakes, and cats (Child & Child, 1993; Hammond-Tooke, 1989). What is clear from these examples is that the visible form of the self is mutable and may not have the appearance of a human being, but be embodied in an animal, a tree, or any other being in nature. Thus, claiming that a person died because a spell was cast upon him or her, when that person was killed by a venomous snake’s bite, may appear nonsensical, until this underlying ontological framework is understood.
Dynamics of connectedness
The essence of personhood in the African cultures explored above is the connectedness between the self, social, and spiritual agencies of the person. Each of these agencies is associated with particular ways of self-understanding and self-representation that are invoked in causal explanations and interpretations of actions and events. Figure 1 illustrates this theoretical framework. Connectedness in this framework involves mutually dependent links that connect the person to his or her self, social, and spiritual agencies. In this model, an individual manifests his or her personhood by relational means. Relational manifestations, as promoted by those cultures, are found in the connections between the person and his or her three agencies: (a) an intrapersonal connectedness which ties the person to his or her physical self, environmental self, and invisible self; (b) an interpersonal connectedness which ties the person to his or her family, clan, and community; and (c) a trans-personal connectedness that ties the person to his or her ancestors and divinities. These agencies correspond to ontological levels or realms that have been termed the endocosm, mesocosm, and exocosm, respectively (Ebigbo, Elekwachi, & Nweze, 2014).
A model of cultural concepts of the person in Africa.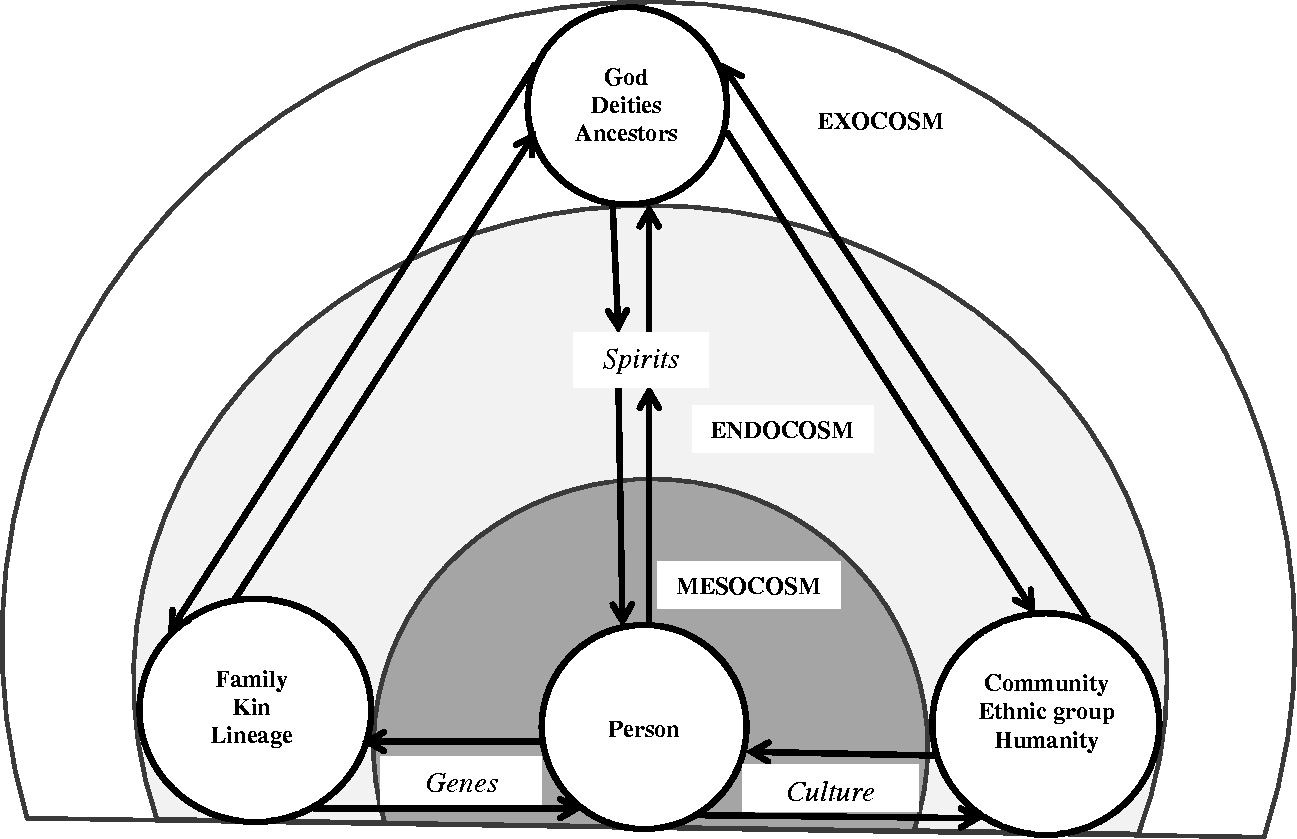
The fundamental role of interconnectedness for personhood is reflected in the ways that health and illness are understood. For instance, according to the Iraqw (of Tanzania), if one member of their matrilineal kin is ill, they will feel the sickness in their own blood (Snyder, 2002). A similar system of thought is found among the Banyarwanda (of Rwanda) where health is perceived to require the free flow of body fluids such as blood, semen, and maternal milk from one community member to another (Taylor, 1992). Conversely, illness results from blockages of the interpersonal flow of individuals’ body fluids. The same beliefs are found in numerous other ethnic groups, including the Yaka (of the Democratic Republic of Congo and Angola; Devisch, 1991), the Zulu (of Southern Africa; Berglund, 1989; Schoepf, 2001), the Akan (of Ghana and Côte d’Ivoire; Minkus, 1980), and ethnic groups from the Great Lake region in Central Africa (Vincke, 1991). The central idea to be appreciated is that a person who lives according to the cultural ideal of personhood, which is rooted on connectedness, will be healthy, while failure to maintain such harmonious connectedness leads to vulnerability to illness and social misfortune. Mentally ill persons, for example, typically dwell in a threatening world in which they feel in disharmony with entities belonging to one of the ontological realms or levels of personal agency.
As stated earlier, the above analysis is neither a characterization of African people nor a description of a concept of the person reflecting the results of a survey of what a representative sample of African peoples refer to in their daily lives. Rather, it is an attempt to offer a practical framework about cultural concepts of the person based on communal values, practices, and systems of thought as promoted by many African cultures. Thus, even though those cultural patterns influence individual Africans’ ways of self-understanding and self-representation, they do not prevent them from choosing their own ways to engage with their culture; shared cultural patterns set no limits to an individual’s personal beliefs and values.
The relevance of cultural concepts of the person for mental health in Africa
The following case study, from the author’s clinical practice in Togo, West Africa, may serve to illustrate the practical relevance of the cultural concept of person described above in mental health. The patient’s permission to report information in the case was obtained. Certain identifying details have been disguised.
M. T. is a 27-year-old Togolese man who was completing a Bachelor’s Degree in Law in Togo. When he came to the mental health department of a university teaching hospital, he was in his senior year in law school. As the final examination date approached, he had started to feel quite anxious and experienced difficulty with concentration, painful headaches, chronic fatigue, and sleep disturbance; and came to the clinic for help with these symptoms.
The patient was born in a polygamous family, and self-identified as an ethnic Kabyè. He followed all the cultural rites of passage required for each developmental stage and participated in traditional ceremonies. At 25 years of age, he received Catholic baptism and since then had attended church regularly.
At the start of his symptoms, he initially felt they were a manifestation of malaria, a disease that he had experienced numerous times. As was his habit, he bought antimalarial drugs at a local market stall and took them but without any change in symptoms. One week later he consulted a general physician who ordered blood tests. Finding nothing wrong, the physician prescribed some vitamins and referred the patient to the mental health department of the hospital. On presentation, his main concerns were tension headaches and chronic fatigue. He was seen by a team composed of one psychiatrist, two psychologists, and three residents in clinical psychology. The team provides clinical consultations that take into account social and cultural context to provide assessment and treatment services.
It soon became evident to the clinical team that the patient’s symptoms began when his father was diagnosed with metastatic cancer. Although the patient’s father did not deny that biomedical diagnosis, he and his family consulted a traditional healer who attributed his sickness to sorcery by his third wife, B. K. Following this diagnosis, the patient’s father was living at the traditional healer’s home where he was receiving treatment. The patient’s father’s most recent wife lived with him at the healer’s home and was in charge of cooking and providing personal care to her husband. After 5 months, she had a heart attack and died. That death was also attributed to B. K.’s sorcery, which aimed to make the patient’s father more vulnerable by killing those who supported him.
Exploring the family system, the clinical team discovered that the patient was very close to his maternal family members. Consequently, the clinical team wondered if consulting with some members of his maternal lineage would be beneficial. The patient agreed, and three family members were invited to a meeting.
The patient attended the third session accompanied by the eldest of his maternal lineage, one of his uncles, and one of his aunts. He said he could not take the final examination because his headaches had been so intense that he could not concentrate well enough to read a text of even one paragraph. He was angry at himself for not being able to take the examination, but even more anxious about his health and future. During this session, the accompanying family members told the clinical team that the whole clan was extremely proud of the patient’s educational achievements. He was the first of the clan to attend university, while no other member of the clan had completed elementary level of schooling. He aspired to become a magistrate. The eldest of the clan said: “He is the one who would raise our djedjewiye [clan] name.”
When asked about their understanding of the difficulties the patient was facing, the family’s elder responded: “the rest of it is in the hands of ancestors; they will not accept that their names be annihilated.” When asked for clarification, the patient’s uncle stated that “some turmoil is happening in the djedjewiye, and we must react before it is too late.” He then described the illness of the patient’s father, the death of one of the patient’s stepmothers, “and now the blockage of the promising future of our child, all that in 5 months period.” He added “all that is too much to keep sleeping, so we went to ask [a traditional healer]. It came out that there is a person that joins our clan who is responsible for those bad things.” When asked for further clarification about the patient’s stepmother’s responsibility for the sicknesses and the death within the family, the patient’s uncle explained: After a violent quarrel with her husband, B. K. whose eyes “see” [meaning she has supernatural powers enabling her to see the invisible world] told her husband she would make him suffer for the rest of his life. Our brother-in-law [the patient’s father] started feeling pain in his right leg the following day. These healers told us that several members of the family, including the patient, his father, and his stepmother who died are, in fact, victims of Kamtou: that woman [B. K.] has captured their Kalizo [invisible self] and confined them at the bottom of Kara river.
When the patient was asked how much he believed in this narrative, he replied: “Jesus said, ‘if forces of goodness exist, therefore forces of the nether world exist too.’ I am a Christian, and I know the devil exists.” However, asked by the clinical team if he wanted to be involved with his family in a traditional healing, the patient declined, expressing concern about the embarrassment that would be brought upon members of his church if his undergoing traditional healing became public knowledge within his Christian community. Fearing that he could even be excommunicated from his church, he reaffirmed that he believed in Jesus Christ, and was certain that Jesus Christ was “stronger” than the devil forces. The patient then elaborated, Actually, as a Christian I cannot engage in these traditional healing procedures. I believe they are powerful. I was witness a couple of years ago to the recovery of a neighbor who was a victim of Kamtou, but—as I told you—now I am a Christian, and I cannot continue in that way.
At the following session, 1 month later, the patient reported that elders of his kin and two traditional healers had performed the Kalizo kpèziou (the releasing of the invisible self) ceremony, as expected. He also said “the traditional healers had requested that in order to strengthen their intervention, the family had to perform a ritual slaughtering of a white ram to beg for the founding ancestor’s protection.” He was planning to give his forthcoming monthly scholarship money to his maternal grand-uncle to buy the requested ram. At the same time, the patient, one of his aunts, and two of his cousins who were Christians had organized a novena (9 days of prayers), 1 week of fasting, and requested one Sunday worship especially for protection of the whole family.
One month later, when asked what had improved since the first session, the patient responded that he noticed improvements in anxiety, concentration, and sleep, and was “feeling full of serenity because I know I am on the right path.” When invited to return in the next month for additional support, he said he felt ready to end the psychotherapy because “I feel stronger now; I am winning the battle.”
Discussion
This clinical case illustrates how people in certain areas of Africa conceptualize and understand their personhood in terms of a dynamic interplay of spiritual, social, and self-agency, as suggested by the personhood framework described above. In addition, it illustrates how the dynamics of cultural concepts of the person may influence major aspects of mental health, including the meanings conferred on mental illness, help-seeking behaviors, and expectations of recovery.
Role of spiritual agency
Following the lead of the patient’s spiritual engagement, the clinical team recognized and honored his spiritual agency, which had been particularly invested in the recovery procedures prescribed by the traditional healer and by members of his Catholic Church congregation. The ancestors had a major role in the way the patient and his family construed mental illness and recovery. The ritual slaughtering of an animal requested for the ancestors, as part of the healing process, aimed to reestablish a harmonious connectedness between the patient and his ancestors. Such healing practices emphasize the archetypal symbol of the ancestor, which may be present in invisible ways but is also tied to ritual objects, places, and practices. African mental health professionals influenced by Jung have characterized the ancestor as the expression of the African collective unconscious, since this spiritual entity is a fundamental part of Africans’ experience of mental illness (Berg, 2003; van Breda, 1999). In fact, the role of ancestors resembles Jung’s (1968) notion of parental imagos, which continue to influence a person long after the absence of the physical parent. According to Weinrich (1990), the ancestral spirit is the parent archetype, accounting for their power and complexity. Furthermore, the ancestral spirit is interpreted as a projection from the unconscious, giving such an external agency a quality of authority and sacredness (Bührmann, 1984; van Breda, 1999).
In addition, the patient’s reluctance to perform by himself the rituals for his ancestors because of his Christian identity illustrates why it is a mistake to think of every African individual’s self-understanding as a faithful embodiment of the form of personhood promoted by his or her culture. Rather, the individual’s self-understanding, insofar as it is coherent, is a complex mixing of multiple collective identities—including ethnicity, religion, gender, age, socioeconomic status, and place of living—all of which may influence the degree of match between the individual’s self-understanding and the culturally promoted person.
Role of social agency
Following lines of clinical inquiry based on their knowledge of the cultural concept of person among the Kabyè, the clinical team was able to recognize that in the patient’s view, as for others in his family, he exercised no responsibility for his sickness. Rather, he was one of several victims of B. K.’s malevolent actions; his illness was a sign that there were disturbances in his kin social order. The interdependence of the patient and his social agency gave rise to an understanding of psychopathology as a failure to maintain channels of connection with some members of his clan. Community involvement in the patient’s life events such as illness experience and paths for recovery reaffirmed his sense of belonging. The patient was not directly responsible for the affliction, because he was not an isolated entity, but rather an embodiment of the social order. Instead of blaming the patient for his illness, he was perceived as the one who alerted the community to some weakness in the whole social order, expressed through his illness. Failure to investigate what has gone wrong in the social order may have led to the spread of illness throughout the community. This may explain why, in many parts of Africa, the community and others are implicated in help-seeking for any affliction and participate in the healing process (Nqweni, 1999; Vontress, 1999). Hence, forms of psychotherapy which do not incorporate family and community members—attending to their salient life events, hopes, and concerns—may not speak to African clients embodying such a communal personhood.
Role of self agency
The patient’s presenting symptoms are related to self-agency, which is at the forefront of concerns for healthcare seeking. A common belief in the patient’s culture is that this agency is the most vulnerable dimension of the person and is the usual target of external aggressors seeking to harm an individual. Similar beliefs were found among the Fon (of Bénin and Togo), where the stomach is believed to be the body region most frequently identified with acts of sorcery (Blier, 1996). Moreover, the clinical case illustrates the concept of the invisible self: because the patient’s Kalizo (invisible self) is considered a substitute of his whole person, one could make him sick by manipulating his Kalizo from a distance. The aim of the healing ritual was to release the captured Kalizo and reconnect it to its “owner.” This cultural self-representation of the self-agency is similar to Frazer’s (2002) logic of contagious magic. In this logic, an individual who gets one’s unwashed clothes or one’s hair has got hold of the whole person, since these elements are considered substitutes of the person (Beattie, 1980). Therefore, not having control over who keeps one’s clothes can be stressful because people are concerned that their clothes might fall into the hands of an enemy who will bewitch them through these clothes (Niehaus, 2002). The same logic is behind the Ewe (of Ghana, Togo, and Bénin) use of dolls as substitutes for the person (Blier, 1996). The doll is addressed as if one were talking to the real person and manipulating him or her from a distance. This practice goes along with the observation that among the Xhosa (of South Africa and Zimbabwe), husbands “mixed wives’ footprints with potions to prevent them from leaving home” (Niehaus, 2002, p. 195). Ignoring such a cultural understanding of the self in clinical practice might lead to total misleading of clients’ understandings of their illnesses and their expectations.
Healing factors
The patient and his family construed their distress in cultural idioms that involve external agencies, and place an emphasis on relationship issues. In terms of psychodynamics, awareness of such relational dynamics may take the form of what Kirmayer (1992) has termed unself-conscious awareness, in which attention is directed externally and the personal narrative is centered on a third entity. Psychotherapy informed by this notion of the person identified the nature of the patient’s person disconnectedness and then prescribed compensatory rituals that serve to engage the patient’s tri-dimensional person in order to reestablish the oneness and harmony among his personhood agencies. This has been done through the involvement of kin-group members in the therapy process, by supporting his spiritual projects, and by promoting self-enhancement. In many African societies, such an approach is more readily understood and accepted by clients since it fits with their cultural understandings and representations of their persons, along with their phenomenological world, which is fundamentally holistic, with no clear boundary between the self (both visible and invisible), the social world, and the spiritual world.
Furthermore, analysis of African traditional healing practices, which are the services on which the majority of African people rely for treatment of mental illness (Ayorinde, Gureje, & Rahman, 2004; Mkhize, 2004; Vontress, 2005), shows that their healing principles rely on the concept of the person discussed in earlier sections (see e.g., Bojuwoye, 2005; Crawford & Lipsedge, 2004; Vontress, 2005). In fact, African traditional healing goals of wholeness and harmony within the person are achieved through family involvement in the healing ceremony, which represents a form of conflict resolution for anomic and fragmented kinship, as well as through rituals devised to manage the person’s connectedness with his or her spiritual entities. The therapeutic function of African traditional healing in restoring the person’s equilibrium and balance has been analyzed from a psychodynamic perspective. For example, writing from a post-Jungian perspective, Hillman (1995) found an analogy between animal sacrifice performed during healing rituals and the symbolic sacrifice of the individual’s ego, which saves the person from an overwhelming or inflated ego. This deflation of the ego helps to reset the balance in the disturbed person and to recover the totality of personhood which extends well beyond the individual ego.
Conclusion
Personhood is always grounded in consensual understandings and expectations of being a person in a given sociocultural context. Such a sociocultural construct of self-understanding and self-representation influences many aspects of our living experience as human beings. Concerning mental health, for instance, every form of healing or psychotherapy involves normative questions of how to live a “good” life, and hence its goals and methods are tied to specific cultural concepts of the person (Kirmayer, 2007; Tseng, 2004). Failure to consider the specificity of cultural concepts of the person may limit therapists’ ability to assess and treat patients’ diverse backgrounds (Dwairy, 2009; Tseng & Streltzer, 2004). Psychological adjustment may depend in part on the degree of match between the patient’s cultural ideal of the person and the concept of the person inherent in any given therapeutic practice (Dwairy, 2009; Kirmayer, 2007). Cultural concepts of the person among people in certain areas of Africa are grounded in the dynamics of a three-dimensional self that encompasses the self, the cosmic world, and the social world. The dynamics of this person is expressed in African narratives, proverbs, beliefs, myths, fears, and conditioned attitudes assimilated through enculturation. This distinctive form of personhood lies behind African notions of health, illness, and recovery. In psychotherapy with African clients embodying such a form of personhood, this concept of the person suggests the value of an approach that emphasizes the two fundamental psychic processes inspired by African traditional healing practices: establishing links and containment. To work in this mode, therapists should consider the following: (a) involvement of the patient’s family and community members; (b) support of the patient’s spiritual projects and respect for his or her spiritual narratives as objective realities; and (c) being aware of the way that people conceptualize their self and using this to devise relevant psychotherapeutic interventions. Such a therapeutic approach would emphasize the whole person’s change, rather than aiming to produce an internal reorganization of one of the person’s components. Consideration of cultural concepts of the person in Africa and their relevance to psychopathology in such a context responds to a basic but important challenge in transcultural psychiatry: contextual abnormality is always derived from contextual norms. To continue ignoring how peoples in Africa conceptualize the “normal” person is to continue to misunderstand many African patients’ needs and expectations. According to Kirmayer (2007, p. 234), psychotherapy that ignores the internalized concept of the person runs the risk of leaving the patient with no way to continue either the coherent construction of the private experience of self or the social interaction that sustains the self in community.
Footnotes
Acknowledgements
I thank the anonymous reviewers for helpful comments on earlier versions of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.