
Abstract
This project explored how Māori understand experiences commonly labelled “schizophrenic” or “psychotic”. Semi-structured interviews were conducted with 57 Māori participants who had either personal experiences labelled as “psychosis” or “schizophrenia”, or who work with people with such experiences; including tangata whaiora (users of mental health services), tohunga (traditional healers), kaumatua/kuia (elders), Māori clinicians, cultural support workers and students. Kaupapa Māori Theory and Personal Construct Theory guided the research within a qualitative methodology. The research found that participants held multiple explanatory models for experiences commonly labelled “psychotic” or “schizophrenic”. The predominant explanations were spiritual and cultural. It seems that cultural beliefs and practices related to mental health within Māori communities remain resilient, despite over a century of contact with mainstream education and health services. Other explanations included psychosocial constructions (interpersonal trauma and drug abuse), historical trauma (colonisation) and biomedical constructions (chemical brain imbalance). Participants (both tangata whaiora and health professionals) reported they were apprehensive about sharing their spiritual/cultural constructions within mainstream mental health settings due to fear of being ignored or pathologised. This study highlights the importance of asking users of mental health services about the meaning they place on their experiences and recognising that individuals can hold multiple explanatory models. Māori may hold both Māori and Pākehā (European) ways of understanding their experiences and meaningful recognition should be afforded to both throughout assessment and treatment planning in mental health services. Clinicians need to be aware that important personal and cultural meanings of experiences labelled psychotic may be withheld due to fear of judgement or stigmatisation.
Introduction
This paper is an attempt to weave Māori psychological concepts (mātauranga Māori) with Western concepts within a largely Western forum (a scientific journal). In this vein a traditional Māori introduction is included in the article. It is customary as Māori to introduce ourselves by providing our unique connection to our land and ancestors (pepeha). The purpose of the pepeha within this context is to provide the reader with a deeper sense of connection to the research and researchers. The first author (Melissa Taitimu) has provided her pepeha below: Ko Whakakoro tōku maunga (My mountain is Whakakoro) Ko Rotokakahi tōku awa (My river is Rotokakahi) Ko Morehu tōku marae (My meeting house is Morehu) Ko Te Uri o Tai tōku hapū (My subtribe is Te Uri o Tai) Ko Te Rarawa tōku iwi (My tribe is Te Rarawa) No Pawarenga ahau (I am from Pawarenga) Ko Melissa Taitimu tōku ingoa (My name is Melissa Taitimu)
Western historical context
Madness has been and remains an elusive thing … it is equally possible to think in terms of the manufacture of madness, that is, the idea that labelling insanity is primarily a social act, a cultural construct. (Porter, 1987, p. 8)
Most recently, psychotic experiences are considered a problem of the “body”. Since the advent of Western psychiatry, literature (Bleuler, 1913/1950; Kraepelin, 1919) regarding assessment and treatment protocols for schizophrenia have focused predominantly upon biochemical, neurological and genetic factors as explanations for these experiences (Thara, Sucharitakul, & Mendis, 2001; Carpenter & Buchanan, 1995; Dean, 2000) despite critiques regarding the reliability and validity of this body of research (Bentall, 2004; Joseph, 2017; Read & Dillon, 2013). Furthermore, research has indicated that biomedical constructions can lead to increased levels of social distance, increased rates of discrimination and negative attitudes towards those thought to have a “mental illness” (Haslam & Kvalle, 2015; Read, Haslam, Sayce & Davies, 2006).
Research indicates that listening to the subjective explanations and experiences of people experiencing psychosis can lead to a deeper understanding of the phenomena. Furthermore, the very process of being afforded an opportunity to make sense of one's own experience and offer personal understandings can have a major impact upon the recovery process (Barnett & Lapsley, 2006; Lambrecht & Taitimu, 2012; Randal, Geekie, Lambrecht & Taitimu, 2008). Despite this evidence, first person accounts of psychosis and schizophrenia have emerged within a context that has largely ignored or pathologised personal understandings of the experience (Geekie & Read, 2009; Taitimu & Read, 2006) and not taken into consideration the impact of wider historical, social and cultural factors (Porter, 1987).
Indigenous psychology: Historical context
Māori experiences are aligned with indigenous peoples the world over, whereby colonisation has subjected whole cultures to psychiatric theories and practices at both the individual and collective level. A common theme is apparent. Research and clinical practice has predominantly been done upon Indigenous peoples by non-Indigenous researchers working with “universal” diagnostic systems within Western psychological or psychiatric settings (Bhurga & Littlewood, 2001; Fernando, 1988; McIntosh, 2004). One modern example is the World Health Organization (WHO) studies that have investigated the manifestation, consequences and course of what Western mental health experts call “schizophrenia” across regions and cultures (World Health Organization, 1979). A major limitation of the WHO studies is the validity of using a Western construct on diverse cultures. It has been argued that within this colonising context, cultural meanings and experiences may have been overdiagnosed and/or misdiagnosed (Fernando, 1988). The WHO studies revealed, nevertheless, that developing countries (non-Western) experience far higher rates of recovery from “schizophrenia” than Western countries. Further research has indicated that this may be a result of the culturally embedded subjective meanings placed upon the experience, and the positive expectations around recovery (Castillo, 2003; Lin & Kleinman, 1988).
Despite this, the “one size fits all” approach remains. Biological psychiatry is currently seeking to impose, primarily via the “Global Mental Health” movement (Mills, 2014; Read, Haslam, & Magliano, 2013), Western “medical model” concepts and treatments on numerous countries and places including India, Pakistan, Bali, Nigeria and Malawi, and, within the United States, on African Americans and Latinos. Within this movement, whole cultures are being labelled as having poor “mental health literacy” (the degree to which one agrees with psychiatry's belief that one's distress is a manifestation of a biologically-based illness) and the ongoing use of culturally embedded explanations and recovery pathways is pathologised (Mills, 2014; Read et al., 2013; Tribe, 2014). Essentially, local spiritual or social causal beliefs are characterised as misinformation or ignorance, and a typical conclusion of psychiatry's studies in this field (see Read et al., 2013) is the call for “interventions aimed at increasing the mental health literacy of traditional healers” (Sorsdahl, Fisher, Wilson, & Stein, 2010 ).
The emergence of Indigenous psychologies and research signposts a step towards “undiagnosing” Indigenous peoples and recognising what in fact may be social, political and spiritual ills (Nikora, Levy, Masters, & Waitoki, 2004; Taitimu, 2007). Indigenous research is conducted by Indigenous scholars, within Indigenous communities, and recognises the critical need to take into consideration cultural constructions of wellbeing (understandings of wellbeing that integrate traditional knowledge systems into current practice) as well as the socio-political and historical response to colonisation as meaningful in understanding Indigenous health status (Duran & Duran, 1995; Durie, 2001). A common finding within this landscape is that Indigenous peoples can hold multiple explanatory models for experiences commonly labelled psychotic that includes but is not limited to that which is on offer from biological psychiatry (Allen, 2002). Explanatory models often include cultural constructions and the socio-political landscape specific to an area (Geekie & Read, 2009; Taitimu, 2007). For example, Sadowsky (2004) found that the content of delusions in African patients in Southwest Nigeria was related to their experiences of war and colonisation. The current research was interested in the unique historical, social and political context in which Māori have been diagnosed with psychotic disorders and how Māori themselves make meaning of these experiences.
Māori psychology: Historical context
A comprehensive outline of mātauranga Māori (traditional knowledge systems) is impossible to capture within the constraints of an article. Some argue it can only be understood experientially through participation within the Māori community. The extension of this view is that any attempt to intellectualise Māori psychological concepts via research inevitably sacrifices the depth and complexity of the knowledge (Waitoki & Levy, 2016). The difficulty in defining Māori psychology is evident in a comment made by Māori Marsden's son, Taki Marsden, when asked how his father (a well-respected elder within the Māori community) would define mātauranga Māori. He replied, “to ask my father what mātauranga Māori is would be like asking a fish what water is. It remains invisible to them” (Royal, 1998) . As such, this section presents a necessarily condensed, superficial summary of a complex philosophy that is only full understood from within (Waitoki & Levy, 2016).
The nucleus of Māori society is the whānau (family). This constitutes not only one's immediate family but also extended networks such as cousins, aunties and uncles. A number of whānau belong to hapū (subtribes), while a number of hapū belong to an iwi (tribe). Each whānau, hapū and iwi is intimately connected to their whenua (land). The concept of whenua is central to Māori identity as it links them to their ancestral mountains, rivers, seas, tūrangawaewae (a place to stand) and economic base (Walker, 1990). Imbalance, disconnection and illness within one's whānau, hapū, iwi, whenua or tūrangawaewae can affect the wellbeing of individuals, families and communities.
Tapu plays an integral role in understanding wellbeing from a Māori perspective. Tapu begins with a being's birth and refers to the potential for what it can become (Barlow, 1991) . Mana is the fulfilment of that potential. In this vein, Shirres (1979) refer to tapu as “being with potentiality for power”. The “being” element of this definition refers to the essence that is tapu, “potentiality for power” indicates each being has the potential to relate to another being in a powerful way and the laws of tapu govern this. In terms of these laws of interaction, tapu has been referred to as a Māori legal system consisting of rules around prohibition and protection to ensure society flourished. Tapu could be applied to people, places, animals, food, plants, events and relationships. Sometimes tapu is a permanent state; at other times it is temporarily applied to guide encounters and restore or maintain equilibrium (Durie, 1999) . Breaches can occur when the proper respect and discipline is not afforded to tapu (Mihinui, 2002) . Mate Māori is a form of Māori illness that can be caused by transgressions of tapu (Lyndon, 1983).
An example of the epistemological differences between Māori and Pākehā (Western) ways of understanding wellbeing is evident in the term pōrangi, a form of mate Māori. This understanding was shared by a kaumatua or elder within this project. Before time, light and space entered our world, Māori creation stories hold that Ranginui (sky father) and Papatūānuku (earth mother) held each other in a tight embrace. This period of creation was called Te Pō (the darkness). The many children of Rangi and Papa, felt cramped and uncomfortable with the darkness cast by their tight embrace. They pushed their father, Rangi, up and their mother, Papa, down. Once this was achieved, time, space and light came into the world. This represented the progression from Te Pō (the darkness) to Te Aō (the light). Pōrangi (literally translated to dark night) has been described as a regression to the state of Te Pō. This is a state of disconnection and darkness. Within the state of Te Pō one loses a sense of self, time and space, becomes very withdrawn, disconnected and can hear and see things that are not physically present. Within this research, participants cautioned that some clients experiencing this form of mate Māori may be misdiagnosed with “schizophrenia”. The term Pōrangi is used today as a stigmatising term within Māori communities much like the term “schizo” or “psycho” is utilised in Western contexts. Another kaumatua within this research suggested this is likely a result of the disconnection Māori have from traditional health knowledge systems as a result of colonisation.
The experience of colonisation for Māori resulted in a number of negative experiences and illnesses (Walker, 1990; Durie, 1997). One example is the Tohunga Suppression Act 1909 (Durie, 2001), which effectively prohibited the use of traditional healing methods to address mate Māori (illness attributed to transgressions of tapu) and signalled that health care was to be based on Western constructions and treatments. This strategy, along with others such as rapid urbanisation during the 1960s, contributed to increased rates of utilisation of Western mental health services throughout the second half of the 20th century (Durie, 2001). Māori make up more than 25% of all admissions to inpatient units despite representing only 15.4% of the total population. Further investigation has found that 47.9% of Māori admitted to inpatient units have a diagnosis of “schizophrenia” and Māori are significantly more likely than non-Māori to be diagnosed with “schizophrenia” or other psychotic disorders (Wheeler, Robinson, & Robinson, 2005).
Despite overutilization of mainstream mental health services, Māori spiritual beliefs regarding mental illness remain resilient (Cherrington, 1994; Lapsley, Nikora, & Black, 2002; Lyndon, 1983; Wharewera-Mika, 2012). This is largely a result of the Māori renaissance where Māori have reclaimed their voice in the areas of education, health and media (Walker, 1990). Cherrington (1994) interviewed Māori with a diagnosis of schizophrenia using mental health services and found that 93% of her participants knew about cultural concepts such as tapu and mate Māori and 78% believed that mental illness could be related to these concepts. At the same time, Māori have been found to be apprehensive to discuss their subjective beliefs within mainstream mental health settings because of a fear that these beliefs will be ignored, marginalised or pathologised (Lapsley et al., 2002; Lyndon, 1983).
In a survey of 247 New Zealand psychiatrists, in 2000, the majority recognised the need to consult with Māori staff when working with Māori clients; but 28 (11%), all male, New Zealand born, and with 10 or more years' clinical experience, expressed the view that Māori were particularly biologically or genetically predisposed to mental illness; and several psychiatrists offered other racist comments (Johnstone & Read, 2000, p. 141): Genetically Māori as a culture seem predisposed to mental illness. Stop sending me crap studies like this, about pointless, meaningless, cultural rubbish. Māori only represent about 10 per cent of the population, for God's sake. Medication is the answer – but they just don't take their pills – if cannabis was prescribed, I'd bet they'd bloody take that.
Background: Nga Whakāwhtinga
The current research was established after consultation with the community (elders, mental health services, non-government organizations [NGOs], mental health service users and policy level advisors) raised great concern about inpatient utilisation rates and statistics for psychosis and schizophrenia. The overwhelming feedback was that Māori needed access to their own ways of understanding wellbeing when they are labelled “schizophrenic”. In fact, a common theme raised during consultation was that “schizophrenia” was a negative term that negatively impacted upon the health of those it was ascribed to. Consultation is a significant first step for many Kaupapa Māori research projects. Within this project many meetings both formal and informal were held to establish the aims and methodology of the research. Nga Whakāwhitinga is the name bestowed upon the research by one of the elders advising the research journey. The term translates to “standing at the crossroads” and represents the space in which this research was conducted, at the juncture between two worlds, te ao Māori (the Māori world) and te ao Pākehā (the Western world). In this vein, one of the major aims of the research was to gather Māori constructions of experiences commonly labelled psychotic in order to better understand the manifestation, content, course and outcome of these experiences; and compare these findings to current Western psychiatric constructions found within mainstream mental health services.
Theoretical and political frameworks
Kaupapa Māori Theory (G. Smith, 1997; Pihama, Smith, Taki, & Lee, 2004) and Personal Construct Theory (Kelly, 1991) were utilised to guide the research within a qualitative methodology. Kaupapa Māori Research is conducted from within rather than upon Māori communities. This process centralises Māori ways of understanding and practising health and is invested in the survival and revival of these practices (Pihama, 1993; L. Smith, 2003) . Kaupapa Māori research also aims to critique social structures that prioritise the ideas and practices of the dominant group over others. Kaupapa Māori research is invested in creating the conditions for transformative change, calling for local solutions to local issues (Nikora et al., 2004). The core principles of Kaupapa Māori research proposed by G. Smith (1997) were used as the foundation for the current research: Tino rangatiratanga (the “self-determination” principle) affords Māori the right and responsibility to determine their own definitions of illness and wellbeing and how this is protected, treated and maintained. Taonga tuku iho (the “cultural aspirations principle”) actively aims to validate and legitimise Māori ways of understanding wellbeing. Ako Māori (the “culturally preferred pedagogy” principle) Māori are able to choose their own ways of understanding their experience that may incorporate a combination of mātauranga Māori and Western knowledge. This integration does not make the knowledge less Māori. Whānau (the “extended family structure” principle) the process of whānaungatanga allows all key stakeholders to define present and future commitments in reference to each other and the kaupapa (direction/aims) of the research. Kaupapa (the “collective philosophy” principle) this research holds at the core of any decision the goal of Māori development (politically, socially, economically and culturally).
In keeping with this framework, consultation and the establishment of a Māori advisory group (rangahau whānau) supported the development of the research project. The advisory group was developed from personal networks and included: Māori clinicians, Māori researchers, tangata whaiora (service users), cultural support workers and two elders (kaumatua), Pio and Chrissy Jacobs. Extensive Māori ethical protocols (see Kaupapa Māori theory principles above) were followed during recruitment and throughout the research process, guided by the rangahau whānau. One example of Māori ethical approval is evident in a dream that one of the elders had after the first author (Melissa Taitimu) had been for a visit. Uncle Pio advised our rangahau whānau that he knew we were “on the right path” as Melissa's grandfather had visited him in his dream.
Personal construct theory (PCT) was included in the research to emulate the title of the project, standing at the crossroads. The aim was to weave a Western psychological theory with traditional Māori research methodologies. The central principle of PCT that was utilised within this project was that words are not independent of reality (Kelly, 1991). More specifically, the constructs we use, such as schizophrenia, can influence the course, content and outcome of experience.
Method
Ethical approval was received from the University of Auckland Human Subjects Committee. Signed informed consent was obtained from all participants.
Recruitment
The project was designed to use qualitative methodology in such a way as to give voice to people who have the experiences in question and to those who work to support them. A convenience sampling approach was employed in order to access people in both groups. Recruitment utilised Māori networks (whakawhanaungatanga), general media and public hui (meetings). The inclusion criteria asked for participation from people who had worked with or experienced psychosis or schizophrenia, who also identified as Māori. Non-governmental mental health services (NGOs) in the Auckland and Northland regions of New Zealand were also approached. A total of 57 Māori participants attended the semi-structured interviews.
Interview schedule
Within each semi-structured interview, participants were asked about their understanding of seven experiences that could be considered to be psychotic or labelled schizophrenic, including what they thought caused a person to have such experiences. The experiences presented to the participants were drawn from clinical literature such as the Diagnostic and Statistical Manual, psychotic symptom checklists and other clinical accounts. For example, “A person hears a voice putting them down or telling them to hurt themselves”. Participants were then asked what questions they would ask (context, history, etc.) to understand more about the experience if someone came to them for help, and what help-seeking pathways they would recommend to someone with these experiences. Finally, within each interview, participants were asked their understanding of the terms schizophrenia and psychosis.
Data analysis
All interviews were audio-taped and transcribed by the first author. Transcripts were sent to participants for comment. Fifteen provided feedback, which was mostly minimal, such as a small elaboration on a concept mentioned in the interview. Thematic analysis (Braun & Clarke, 2006) was then conducted on the transcripts. This is a method, commonly used in psychology research, involving an inductive approach to developing themes directly from the data on the basis of shared meaning. NVivo, a data analysis package, was used to facilitate the thematic analysis, leading to the themes described in the Results section.
Results
Sample characteristics
Demographic frequencies and percentages of interview participants.
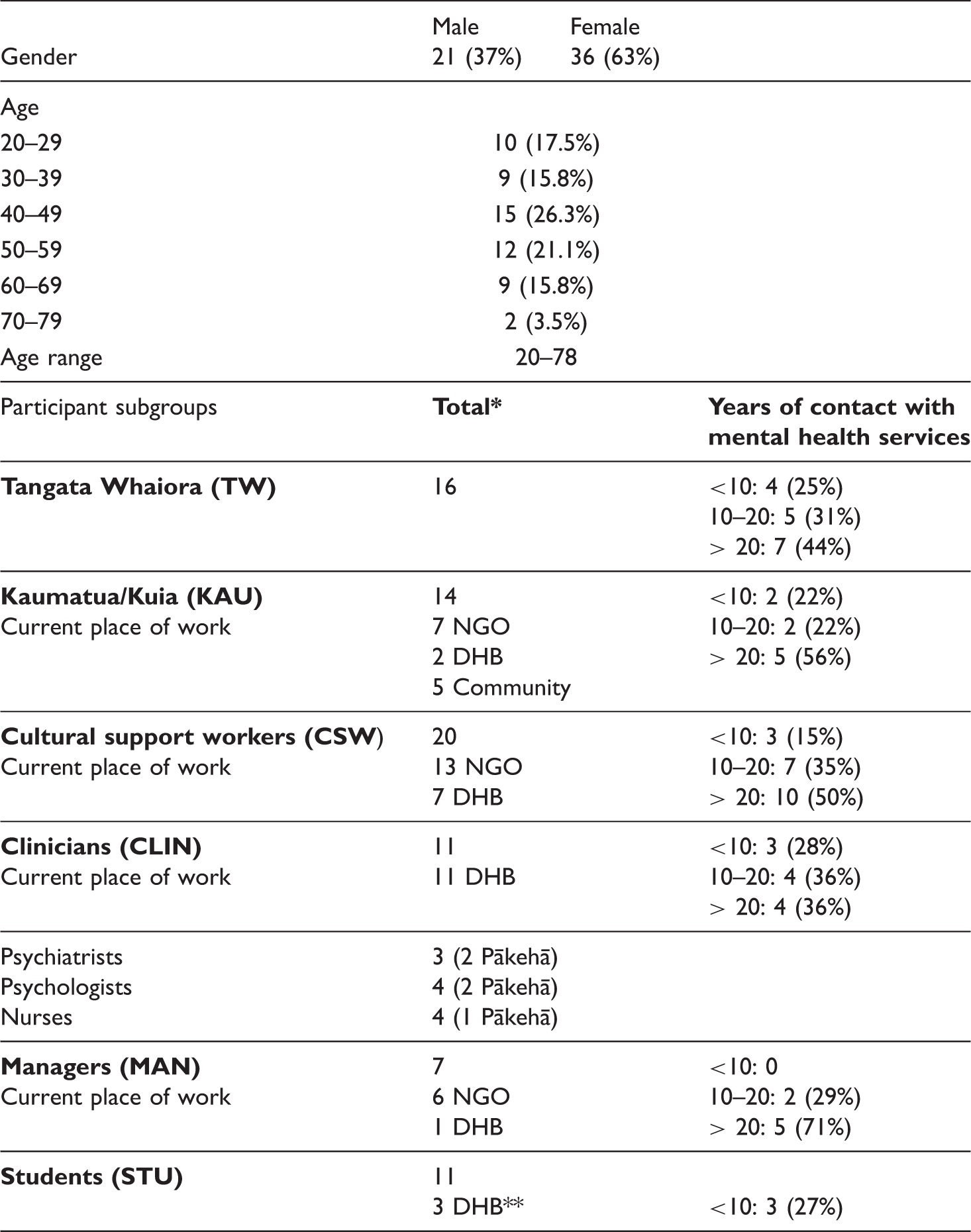
aSome participants belonged to more than one subgroup.
bThree students were also cultural support workers or trainee clinicians within a District Health Board.
Preference for cultural and psychosocial understandings but no one Māori way
Themes for making sense of the experience including number of participants.
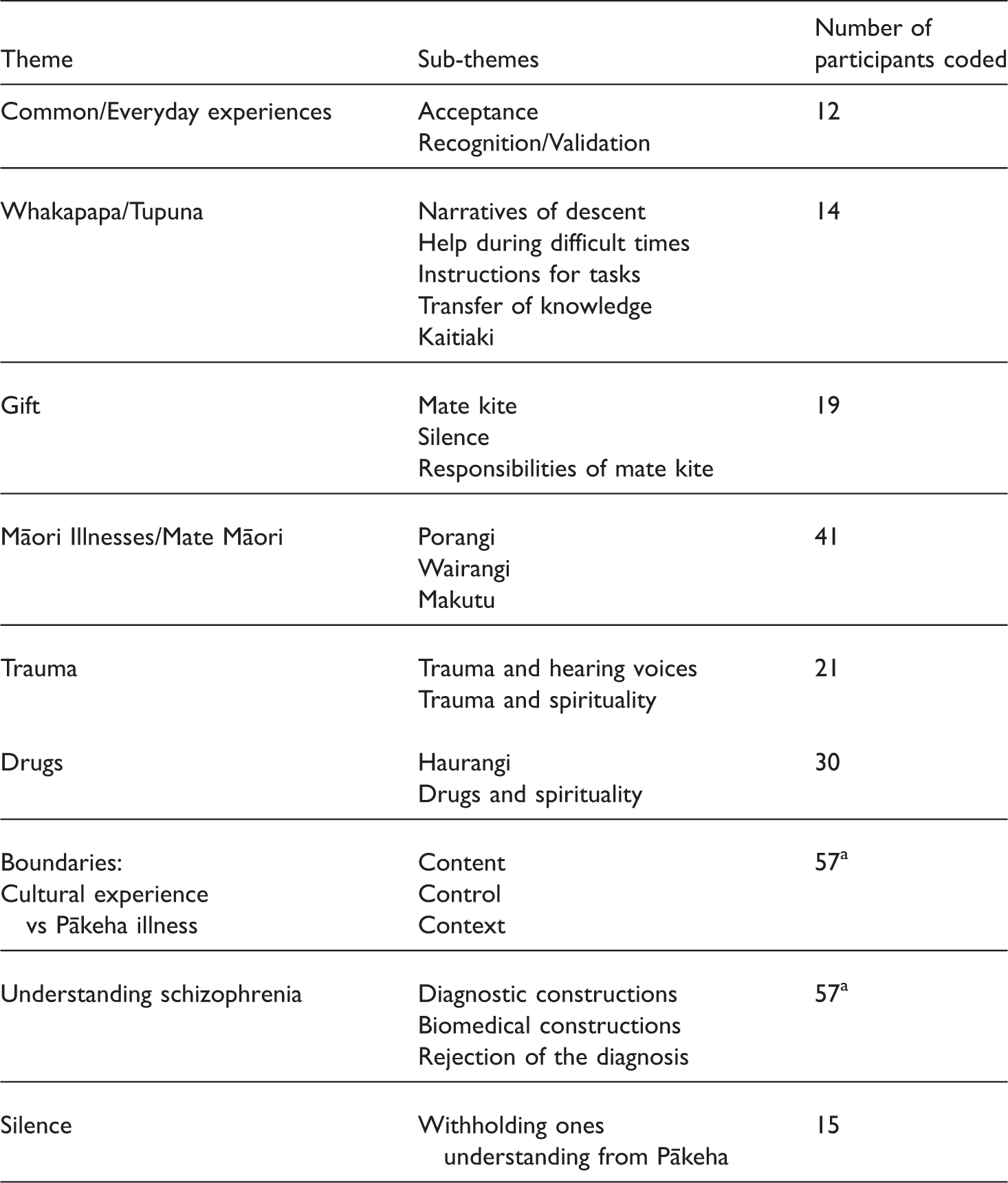
aAll 57 participants were asked about this theme; therefore 57 participants were coded.
Common everyday experience
A number of participants reported that these experiences could be normal and do not need to be pathologised: For me hearing voices is like saying hello to your whānau in the morning it is nothing unusual. (CSW) My understanding of that is that I absolutely accept that if someone tells me that they see someone standing in the room that I can't see that there actually is. They actually can see it. I understand that. (KAU/MAN).
Whakapapa/tupuna (ancestors)
Participants referred to psychotic experiences as possibly being indicative of one's ancestors trying to contact them for particular reasons: They come to me when things are about to get bad… they sometimes tell me what to do and if I do it then I get through. I used to think them coming meant I was going crazy again but now I realise that when times were tough, they were there to help me through. (TW) Yep a lot of them have something that needs to be done. You will know when you're supposed to do it, they're not subtle, they will show you what you need to do and they won't stop until you do it. (TW) In my family we had to go back a fair way to get an understanding why all of this was happening now [diagnosis of schizophrenia in family]. We had to visit the place where it started and get some of our kaumatua [elders] to talk to them to find out what really went on and then how we could go about finding some sort of resolution or utu [balance]. (KAU).
Matakite (gifted)
Psychotic experiences were also understood at times as a sign of giftedness (Matakite, Tohunga). This is a spiritual gift and includes the role of seer (of future events) and awareness of activities and actions in other places. Having this gift was discussed as being passed on through generations: And there was families who were like that. That's when that korero [saying] used to come “he momo tangata he wena” [they are a different type of person], and they were known for that sort of thing and the rest of the whānau accepted they're like that. They come down from a line of tohunga and it's being able to understand those people and still accepting them for what they are and supporting them. (KAU) I never wanted to accept it, I said no it isn't, it isn't [matakite] but it wouldn't stop and in truth I knew what I had to do, help my people, I didn't want the responsibility but here I am. They helped me understand it and told me what to do with it. (KAU).
Mate Māori (Māori illness)
Psychotic experiences were not always considered within a normative or positive cultural lens. Mate Māori was described as a term loosely translated as Māori illness. A number of participants referred to various illness states that could be understood as mate Māori: You know when hearing a voice in Māoritanga there is only two things with mental health, there was only pōrangi [literal translation: dark night] and wairangi [literal translation: water/sky] but now they've got another one, haurangi [under the influence of alcohol or drugs] … There wasn't any such thing as bipolar, schizophrenia, we didn't lock ours up and throw away the key, that's it. (KAU) Pōrangi [a form of Mate Māori] is that the poor person is in darkness, his mind is in darkness. If we go back to rangi and papa [sky father and earth mother] and his mind is in darkness, he doesn't see any light at all, his world is in darkness. (KAU/CSW) When the wairua goes wandering that is wairangi [a form of Mate Māori]. People are not their whole selves. They do not have the ability to communicate or fully function. (KAU) The main person that was behind me was my father. He passed away in 1998, so he was pushing and I was being dragged through, there were familiar faces and not so familiar faces, and some faces that had been long gone, and getting through that, it actually terrified me, I had all these body sensations. I knew where I was but I felt as though I was somewhere else and that somewhere else was actually in [home town]. I actually found myself standing in [my home town] and I was standing in the cemetery and as fast as I tried to get back, if you can call it get back from there, I was held there, my wairua couldn't get back to my body. (TW/CSW).
Tapu
Others referred to the important role of tapu and noa in Māori society and the illness that will result if this balance is not restored: Tapu [sacred] does not mean don't touch, it is a mark of respect, you respect it … you're gonna get hurt or sick or something if you don't respect it. (KAU)
Trauma
A number of participants referred to the effects of trauma on experiences of psychosis, especially hearing voices and delusions: Is that mum in the background? Is that the abusive parent? Is that mum always putting them down or is it in relation to some sort of trauma when they were growing up? I think quite often things can be explained by people's nurture and how they got to that point prior to seeing you. That is why the context is so important in relation to how they got there. (CLIN) It is really scary when you start to hear people who aren't physically present, you freak out at first. Especially when everyone around you doesn't want anything to do with you, you feel so alone, it is one of the scariest things I have ever had to go through. (TW) I think with trauma it's almost like you've opened up to something, you've opened up a side to you. Our belief is that our people are spiritual and it's very very spiritual and that's who we are and something comes in and there's a breach that shocks you personally, the breach of tapu is there and so you are open to all negative spiritual things. (KAU/CSW) A lot of them just don't know who they are because they have been brought up away from their whānau, hapū, iwi… In my books the major ill is loss of identity not schizophrenia. (CLIN) They are most likely second or third generation living in state housing in towns, benefit families. I am not surprised that it is higher [Māori admission rates] because Māori have got all of these social issues going on. (STU)
Substance use and abuse
A number of participants referred to the increasing levels of drug and alcohol abuse within Māori communities as explanation for psychotic experiences: The issue for me is I think too many of our whānau are getting sick due to the use of drugs. … Because what you are doing, when our young people become mentally unwell because of drugs it is a European drug that has caused it. I think that is where we get a lot of our paranoia from. (KAU/CSW)
Rejection of the diagnosis schizophrenia
All participants were asked in the latter part of the interview what the term “schizophrenia” meant to them. Most tangata whaiora appeared confused about the term: Like you are not all there or something. Like so stressed out… I suppose a part of that person has been taken away. They are not their full selves or something. I have never had the term explained to me… Psychotic, schizophrenic. (TW) Learning a lot I suppose. Being a schizophrenic. Learning new things that you've never really believed in. That is something new. Oh, I don't know… (TW) It's about another perspective making a judgment on another based on their own cultural norms of what hearing, seeing and believing is and labelling that as schizophrenia when in fact that may not be. (CSW/MAN) I really believe that schizophrenia does not exist as a diagnosis. And we need to identify the symptoms from the field of psychosis. So when people say to me oh he is schizophrenic, that means nothing to me. But when we talk of it in terms of he is hearing voices or whatever, then I have something to work with. (KAU/MAN)
Silence: Withholding personal meaning
A number of participants discussed their experience of adhering to psychiatric ways of understanding their experiences and strategically withholding their subjective understandings due to fear of being judged or pathologised: When they asked me, they didn't ask me what I saw. I was like, okay, I want to get out of here so I had better start talking their talk. You don't tell the shrink because you want to get out so you just try and make up stuff that they want to hear so you can get better or so that you can get out of there. (TW) If you fight against being a psychiatric you're going to go down, you're going to get locked up you're going to get hurt. I've done Lake Alice, that's a highly psychiatric prison, I've been to Lake Alice and you've just got to face it, the truth is psychiatrics, you're getting punished by god. (TW)
Boundaries between Māori illness and psychosis/schizophrenia
In general participants understood psychotic experiences to be indicative of either a Māori illness (Mate Māori), a gift (Matakite) or a Pākehā illness (Western psychiatric condition). The boundaries placed between these experiences generally referred to the content, control and context of the experience, however, boundaries placed by one person were not necessarily placed by the other. Some comments are outlined below.
Content
Some participants believed if the content of the experience was not Māori (specifically referring to Māori people, language or experiences) it was likely a “Pākehā illness” and not culturally embedded: Just again if they know who it is or if they can recognise any links between the voices and anyone that they know. You know if they said they were hearing Pocahontas or something I'd be a bit suspect of that you know I'd kind of thinking well why's Pocahontas trying to talk to you sort of thing. (STU) One of mine believes she's royalty. At first I thought it was funny, we thought oh this one thinks she belongs to the British royal family. But as time moved along for me, I thought it's not about British royalty, it's about Māori royalty. It took me a long time, to work it out. That opened my eyes. I thought, you know she's not as crazy as what people think she is, she's actually connecting to her Māori royalty, now it's not such a big thing to me. It's just that she's used the British royalty names. (CSW)
Control
Some participants believed that being out of control with the experience was more indicative of an illness state: One [Pākehā illness state] is very controlling, it consumes them actually and they can't function. The other one [matakite] is fully operating as a person they can tell you about what is happening and they say it in a very authoritative way because they are in control. (CSW) I used to be so scared of the voices, they were terrifying ... now I know what they are trying to say and who they are, I can also control it and tell them not now, it's choice for me now. (TW)
Context
Some participants discussed that if the individual could hear voices from a young age it would mean they had a spiritual gift or ability rather than an illness: When you ask them how long they have been hearing voices, this can give you a pretty good idea if it is matakite. They hear these things usually from a really young age unless it has been suppressed in them. (KAU) She died in XXXX hospital, when my grandfather passed away he couldn't look after her anymore. Our family knew that she wasn't schizophrenic, she didn't have a mental illness we were quite clear that she was a tohunga however her immediate family believed that she had schizophrenia and she was in hospital when she died. She wouldn't have been schizophrenic if she was allowed to just come with us. (KAU) For me, one the most significant distinctions is who is around you at the time? Do they think you are crazy, because if they do, then you probably will be. It is easy to become what others think you are. Us Māori have been doing that for ages, taking on these things that the Pākehā put on us. But if we are around our own, they may not be told it is crazy to hear things and see things, and guess what? Maybe we won't be crazy just by virtue of being understood and told this experience actually has a perfectly plausible explanation. (CLIN)
Discussion
The findings of this research support the current literature from both Indigenous and service user literature indicating that individuals can hold multiple, and what may appear to be competing, explanatory models for psychotic experiences including spiritual, psychosocial and biological explanations. This finding indicates Māori will likely benefit from both clinical and cultural interventions. Further to this, the current findings draw attention to a potential barrier to this aspiration where Māori service users and clinicians have found spiritual and cultural constructions to be marginalised and/or pathologised within mainstream settings resulting in a survival coping strategy of silence.
Incorporating both cultural and clinical understandings of psychotic experiences into assessment and treatment is necessary if one considers the additional finding that the boundaries between Māori giftedness (Matakite), everyday/normal experiences for Māori, Māori illness (Mate Māori) and Pākehā illness (schizophrenia/psychosis) are blurred and can be misinterpreted within both Māori and Pākehā contexts. Some participants stated that an individual could experience both mate Māori and psychosis and would recommend seeking help from both pathways. Others commented upon the higher levels of tolerance/acceptance of psychotic experiences within Māori whānau (family) resulting in some individuals presenting at health services at an acute stage of their illness, a trend that is often cited within Māori health literature (Mental Health Commission of New Zealand, 2001). At the same time, participants commented upon circumstances where protective voices or visions within a cultural context may be pathologised by health practitioners and treated with a view towards symptom reduction. This highlights a significant issue for Māori during their recovery where aspects of their experience that may represent a site of resilience are ignored or considered part of the illness process. It is doubtful that the boundaries will ever be clear between what experiences are considered matakite, Mate Māori or schizophrenia/psychosis. Therefore, understanding personal meanings and cultural context will continue to play a pivotal role in determining the appropriate pathways for recovery on a case by case basis.
Overall, the current findings are consistent with previous research that has identified the resilience of Māori spiritual beliefs relevant to the diagnosis and understanding of mental illness (Beaglehole & Beaglehole, 1946; Cherrington, 1994; Lyndon, 1983). Lyndon (1983) predicted, more than 35 years ago, that Māori constructions regarding tapu and mate Māori would continue to be used to understand what Pākehā call “mental illness” in the future as she observed these beliefs were already being passed on to the next generation of young Māori. Lyndon also believed that increased acceptance of Māori constructions through the period of Māori development in health would serve to strengthen these beliefs (Durie, 1997). The current research has found support for this prediction as many of the participants interviewed, who had been in contact with mental health services for long periods of time, still retained strong cultural/spiritual constructions of their experiences and work. However, it was also apparent that many participants had their constructions ignored, marginalised or pathologised within mainstream settings. This indicates that in some instances, there has not been a significant shift in the system in terms of acceptance of Māori constructions. This may be especially the case for the diagnosis of schizophrenia, as it remains the most medicalised mental disorder.
To broaden the language around Māori constructions of psychotic experiences this research makes a unique contribution towards understanding culturally embedded concepts such as pōrangi and wairangi in terms of their manifestations and underlying mechanisms that may impact upon the health of Māori. To the best of our knowledge, aside from early anthropological and medical writings these cultural experiences have not been well documented or understood. Indeed, due to limited access to this knowledge many in the Māori community do not understand these concepts or know who they could seek help from (Durie, 2001). Further research is required to understand the various manifestations and current ways of working with matakite and mate Māori within Māori communities and how this can inform mainstream mental health practices to not only reduce the likelihood of misdiagnosis but also broaden the pathways Māori are able to access during recovery.
While participants were able to develop a dialogue about experiences such as hearing voices, or delusional beliefs, the term schizophrenia held little utility or relevance for many Māori participants even those who have been labelled with, and work with, the diagnosis. This finding supports the literature that advocates for a focus on symptom clusters as opposed to broad-based syndromes such as schizophrenia (Bentall, 2004). In addition, participants commented upon the stigmatising impact the word “schizophrenia” has upon their recovery not only in terms of how they perceived themselves but also how their whānau and community responds to them. This finding is consistent with service user perspectives cited in recovery literature (Lapsley et al., 2002).
Finally, this research has implications regarding access to mental health services for Māori with psychotic experiences by advocating for research and interventions that address barriers and facilitate pathways between communities and services. This project asked Māori about their recommendations for pathways of healing (Taitimu, 2007); however, the discussion is outside the scope of this article which primarily focuses on the meaning of the experience. One recommendation from the research was for the development/enhancement of bicultural services that deliver both cultural and clinical assessment protocols that are not independent but meaningfully acknowledge and inform each other. To achieve this shift within services future research and initiatives should target the development of the Māori mental health workforce and culturally competent non-Māori clinicians. In the words of one of our most influential Māori leaders, Sir Āpirana Ngata (1874–1950; n.d.), an integrated approach would ideally weave the strengths of both pathways: E tipu e rea mō ngā rā o tō ao Ko tō ringa ki ngā rākau a te Pākehā Hei ora mō te tinana Ko tō ngākau ki ngā tāonga a ō tïpuna Māori Hei tikitiki mō tō māhuna Ko tō wairua ki tō atua, Nānā nei ngā mea katoa Grow and branch forth for the days destined to you Your hands to the tools of the Pākehā for the welfare of your body Your heart to the treasures of your ancestors as adornments for your brow Your spirit to god, who made all things.
Limitations
Despite being the largest number of qualitative interviews in this field to date, 57 is too small a sample to have confidence in any generalisations to the Māori community as a whole, or to make comparisons between participant subgroups. Larger studies would be desirable in the future.
As is the case with all qualitative forms of enquiry, in particular Kaupapa Māori research, a limitation could be the inherent subjectivity in conducting and interpreting the interviews. However, Kaupapa Māori theory posits that subjectivity is not only a strength, but an integral part of Indigenous research. The primary researcher (MT) being a Māori researcher and sharing to some extent identity, values and beliefs with participants may have allowed for personal meaning and understanding to be shared especially given the finding that many Māori are cautious of sharing their beliefs about their experiences lest they be judged or pathologised. On the other hand, being a younger Māori female may have influenced what information was shared, for example, kaumatua (elders) may have withheld some information due to their belief that the interviewer was too young, did not speak Māori fluently, and it was not her time or role to know such things within our community.
As is the case with most research conducted in Māori health, a balance must be sought between generating and sharing knowledge that is going to help whānau [family, community] who use mental health services, and risking the exploitation, misuse and/or misinterpretation of cultural intellectual property. With the guidance of the rangahau whānau, this research used the benchmark of positive Māori development to make moral, ethical and academic decisions throughout the research process (International Research Institute for Māori and Indigenous Education, 2002).
Footnotes
Acknowledgments
Ngā mihi ki ngā kaitautoko o tēnei rangahau.
We would like to acknowledge the support and trust participants and the advisory group placed in the research.
“Whaowhia te kete Mātauranga” (Fill the basket of knowledge).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported financially by the University of Auckland, Nga Pae o te Maramatanga, and the Māori Education Trust.