
Abstract
Information about patterns of expression of neurological soft signs (NSS) in schizophrenia among individuals belonging to the same genetic ancestry may provide new insight for the understanding of the disease’s genetic functions. This study aimed to investigate whether patterns of NSS expression in first episode schizophrenia are comparable in populations with dissimilar genetic ancestry. A sample of 207 patients with first episode schizophrenia were examined using the Neurological Evaluation Scale before they were exposed to anti-psychotics. They were allocated to two African ancestry groups: Black (81 Yoruba Nigerians, and 18 Xhosa South Africans), and non-Black (98 Coloured, and 10 White South Africans). Assessments were carried out using validated measures of clinical characteristics of schizophrenia. We determined the frequency, severity, factor structure, and association of NSS with clinical characteristics. Factor derived categories were compared using the Pearson’s (r) and Tucker’s congruence methods. The associations between factor derived categories and clinical characteristics of schizophrenia were determined using Pearson’s correlations and multiple regression analyses. Neurological soft signs were more frequent and more severe in the Black African ancestry group. Also, the factor structure and presentation of NSS in the two ancestry groups were significantly different. Neurological soft signs, especially motor sequencing and cognitive-perceptual abnormalities, were independently associated with disorganization psychopathologies in all the participant groups. Differences in the profile of NSS in Black compared with non-Black African ancestry patients with first episode schizophrenia may suggest differing patterns of expression of NSS in schizophrenia according to genetic ancestry.
Introduction
Evidence from twin studies suggests that 80% of the variability in whether a person will develop schizophrenia or not is due to inherited genetic interactions (Owen, Cardno, & O’Donovan, 2000; Visscher, Hill, & Wray, 2008). Yet, specific genes for the disease onset remain to be identified (Sanders et al., 2008; Schizophrenia Psychiatric Genome-Wide Association Study (GWAS) Consortium, 2011; Williams, Owen, & O’Donovan, 2007).
An important reason for inconsistent results in genetic studies of diseases such as schizophrenia may be the scarcity of well-characterized samples due to high genetic admixture in diverse populations (Bryc et al., 2010; Sanders et al., 2008). Recent advances in high-resolution genome-wide techniques have allowed for better empirical characterization of the bio-geographical ancestry (BGA) of individuals and samples for bio-medical research (Mersha & Abebe, 2015; Rotimi & Jorde, 2010). Emerging evidence from such studies appears to suggest clusters of genetic homogeneity in many sub-Saharan African populations (Bryc et al., 2010; Lambert & Tishkoff, 2009; Tishkoff et al., 2009). This would suggest that samples for genetic studies derived from such populations are likely to be better characterized. While these single nucleotide polymorphisms and microsatellites based techniques provide the best chance of characterizing individuals and populations, this technology is not yet widely available in most of sub-Saharan Africa and many other resource-poor settings.
As the search for schizophrenia genes continues, currently explored alternatives include the possibility that intermediate phenotypes may provide relatively proximate information about gene functions in the disease (Braff, Freedman, Schork, & Gottesman, 2007; Gottesman & Gould, 2003). It is yet unclear whether intermediate phenotype expression in schizophrenia shows demonstrable patterns of similarities among individuals with similar genetic ancestry. Such information may determine their suitability as easy to measure proxies of the more expensive genomic parameters for empirical ancestry information used in the quantification of genetic homogeneity for bio-medical research. This will be especially relevant for schizophrenia research in resource-limited settings.
Neurological soft signs (NSS) are subtle but clinically measurable abnormalities that are now recognized as part of the manifestation of schizophrenia (Chan & Gottesman, 2008; Gureje, 1988). Studies demonstrating their expression independent of the clinical state of schizophrenia (Emsley, Turner, Oosthuizen, & Carr, 2005; Ojagbemi, Esan, Emsley, & Gureje, 2015; Prikryl et al., 2012), heritability (Sanders et al., 2006), and co-segregation with the disease (Mechri et al., 2009; Neelam, Garg, & Marshall, 2011) have established their profile as viable intermediate phenotypes of schizophrenia. They may therefore be relevant to establish that an individual has progressed along the neurodevelopmental pathway to schizophrenia. Neurological soft signs are of particular interest to contemporary genetic science because they can be elicited quickly, reliably, and cheaply.
In the present study, we have relied on anthropological evidence of the “Bantu expansions” to define populations shaped by over 3,000 years of West to South migration of populations within the African continent (Ehret, 2001). First, we characterized two distinct populations of Africans: Black Africans comprising Yoruba in Nigeria, and Xhosa in South Africa, and non-Black Africans comprising of Mixed ancestry and White South Africans. These ancestry categories were determined based on participants’ self-report and interviewers’ judgment of phenotypes. The White South African population is mostly of European descent. However, the Mixed ancestry population, or so-called “South African Coloured population”, is largely made up of people with Khoisan genes admixed with African, European and a smaller Asian contribution (Stull, Kenyhercz, & L’Abbe, 2014). For reasons of sample size, we included patients who self-described as White South Africans (n = 10) in the Mixed ancestry group.
We next compared illness severity, factor structure, and the association of NSS with clinical characteristics of schizophrenia in unmedicated or minimally treated patients with first episode of the disease. Our main hypothesis was that the profile of NSS would be different in Black African ancestry patients compared with those of non-Black African ancestry.
Methods
The present study is part of an investigation of the socio-demographic, clinical, biological, and treatment aspects of schizophrenia (and related disorders) in 207 patients presenting for bio-medical treatment for the first time as out- or in-patients in psychiatric hospitals and community clinics in Cape Town, South Africa and Ibadan, Nigeria. It was conducted by multidisciplinary teams comprising psychiatrists, mental health nurses, and social workers at the two locations, and funded by the New Partnership for Africa's Development through the Department of Science and Technology of South Africa. Ethical approval was obtained from the University of Ibadan ethics committee and the Stellenbosch University Faculty of Medicine and Health Sciences Human Research Ethics Committees. Participants provided written, informed consent before interviews were conducted.
Participants
The participants comprised anti-psychotic medication naïve or minimally treated patients with first episode schizophrenia, or schizophreniform disorder (5 patients had a lifetime exposure to oral anti-psychotics of less than 4 weeks). The diagnosis of the relevant disorder was made according to criteria in the Diagnostic and Statistical Manual for Mental Disorders–Fourth edition (DSM-IV) (American Psychiatric Association, 1994) by the attending psychiatrist at the study locations. Patients were eligible if they were aged between 16 and 45 years and have had less than 4 weeks of oral anti-psychotic exposure during their lifetime. All eligible patients were informed about the study, and the procedure was explained to them in their native language. We excluded patients with previous treatment of long-acting depot antipsychotics, and those meeting DSM-IV criteria for current substance abuse. Also excluded were patients with significant physical illnesses (e.g., chronic kidney disease) determined from the result of a full physical examination and appropriate laboratory investigations. Patients with intellectual disability were excluded based on clinical history. Additional formal testing of cognitive capacity was not conducted. Participants comprised 81 Yoruba Nigerians, 18 Xhosa, 98 Mixed ancestry, and 10 White South-Africans. The Black African ancestry sample for the present study comprised the Yoruba and Xhosa participants, while the White and Mixed ancestry South Africans comprised the non-Black ancestry participants. Participants did not receive monetary compensation for their participation. They were evaluated as far as possible before antipsychotic medications were prescribed. In the few cases where severity of psychopathology prevented immediate assessment, the evaluations were conducted as soon as patients were deemed well enough to co-operate for the examinations. The following information was obtained from all patients: demographic data, personal history, psychiatric history, medical history, family history.
Measures
The Structured Clinical Interview for DSM-IV-Patients edition (SCID-P) (First, Spitzer, Gibbon, & Williams, 1996) was used in the recruitment of patients. The SCID-P provides for a standardized assessment that generates DSM-IV diagnoses using a semi-structured interview.
Neurological soft signs were evaluated using the Neurological Evaluation Scale (NES) (Buchanan & Heinrichs, 1989). The NES is a well-validated tool for neurological assessments in first episode schizophrenia. The scale includes “functionally meaningful” sub-scales which reflect signs of Motor co-ordination (tandem walk, rapid alternation, finger-to-thumb opposition, and finger-to-nose test), Sensory integration (audiovisual integration, stereognosis, graphesthesia, extinction, and right-to-left confusion tests), and Motor sequencing (first-ring, the first-edge-palm, Ozeretski, and rhythmic tapping tests). The other signs assessed by the NES include cerebral dominance, short-term memory, frontal release signs and eye movements. The NES items are scored with reference to the descriptive anchors provided on a 3-point scale (no abnormality = 0; mild, but definite impairment = 1; marked impairment = 2) with the exception of “suck” and “snout” reflexes which are scored 0 or 2. In this study, a neurological abnormality was defined as the rating of 2 on any item (except cerebral dominance) on the NES. Each item was assessed according to a fixed order.
The tests were administered by independent raters (all psychiatrists) of African (AO, BC, and OE), and Asian (LA) descent after a 3 weeks training in the use of the NES at the Tygerberg Hospital, Cape Town, South Africa. Assessments were conducted in English and/or the home language of participants. The inter-rater reliability (IRR) conducted after training ranged from kappa = 0.62 to 0.82, while the intra-class correlation (ICC) across the measurements of NSS in the participants groups after the study was 0.98 (95% CI = 0.97, 0.98).
The severity of the baseline psychopathology was evaluated by administering the Positive and Negative Syndrome Scale (PANSS) (Kay, Fiszbein, & Opler, 1987). The model of the PANSS adopted in this study (van der Gaag et al., 2006) included 5-factor analysis derived domain for “positive symptoms” (delusions, hallucinations, unusual thought content, suspiciousness, and grandiosity), “negative symptoms” (lack of spontaneity, blunted affect, emotional withdrawals, apathetic social withdrawals, motor retardation, poor rapport, and active social avoidance), “disorganization” (stereotyped thinking, poor attention, disorientation, conceptual disorganization, and difficulty in abstraction), “excitement/hostility” (poor impulse control, excitement, hostility, and uncooperativeness), and “emotional distress” (anxiety, depression, guilt, and tension).
The overall clinical status was assessed using the Clinical Global Impression (CGI-Severity) (Guy, 1976), while pre-morbid adjustment and depression symptoms were explored using the Pre-morbid Adjustment Scale (PAS) (Cannon-Spoor, Potkin, & Wyatt, 1982), and the Calgary Depression Scale for Schizophrenia (CDSS) (Addington, Addington, & Maticka-Tyndale, 1993), respectively. These measures have been used for the assessments of African patients with schizophrenia in previous studies (Gureje, Aderibigbe, Olley, & Bamidele, 1994).
In this study, duration of untreated psychosis (DUP) was defined as the period in months from the onset of psychotic phenomena to first presentation to the psychiatric units. In line with previous studies, onset of psychosis was defined as the presence for one week or more of one of the following psychotic symptoms; delusions, hallucinations, marked thought disorder, marked psychomotor disorder, and bizarre, grossly inappropriate and/or disorganized behavior, with a marked deterioration of functioning (Morgan et al., 2006; Singh, 2007).
Statistical analyses
Descriptive statistics such as mean, median, and standard deviations were used to summarize quantitative variables, while frequencies and proportions were used for discrete variables. The frequency and severity scores of NES subscales for the two Ancestry groups (Black and Non-Black) were compared using the X2 test for categorical variables and t-test for continuous variables respectively. The same methods were used for the comparison of the total NES score for the two groups.
Exploratory factor analyses (EFA) were conducted on NES items that were abnormal in more than 10% of each participant group. Items testing for cerebral dominance were excluded. Factors obtained following initial maximum likelihood exploration were rotated using the varimax procedure. Factors are reported when they have eigenvalues greater than unity and when they contribute at least 10% to the cumulative variance (Sewell et al., 2010). For the factor extraction, loadings of ≥0.5 were considered meaningful.
We next compared the factor loadings in the participant groups for similarity with the corresponding group. For this objective, we used both the Pearson product moment correlation (r) (Pearson, 1895), and Tucker’s congruence co-efficient (φ) methods (Tucker, 1951). These comparisons were conducted using the full factor loadings in each group before extraction of the representative items by size. For the Pearson (r) method, the factors were paired up one from each group and the correlation coefficients were determined. The Pearson (r) computes the similarity between factors based on their respective deviation from the mean. The method is able to detect both the differences in the pattern and magnitude of the compared factor loadings. For the Tucker’s method, we multiplied each loading in one group with the corresponding loading in the comparative group. The products of these multiplications were then summed. The sum of the products was next divided by the square root of the sum of squared loadings in one group multiplied by the sum of squared loadings in the comparative group. In this study, factors are considered similar if the congruence between them is 0.82 or higher (Tucker, 1951). The Tucker’s congruence computes co-efficients based on the deviations of the factor loadings from zero (cosine = 1.0) for perfect similarity. Co-efficients of Pearson (r) and Tucker’s congruence for the group comparisons are presented.
For the relationship between the factor categories in each participants group with the clinical characteristics of schizophrenia, we first conducted a Pearson correlation between each factor with the clinical characteristics of interest. Characteristics that were significantly correlated with factor categories were then entered as independent variables into separate multiple regression analyses for each participants group using the method of forward selection of variables. The same method was followed for the association between total NES and the clinical characteristics of schizophrenia.
Analyses were conducted using Stata version 13.0 (StataCorp, 2013). Values of p < .05 were considered significant.
Results
Characteristics of the two ancestral groups (N = 207).
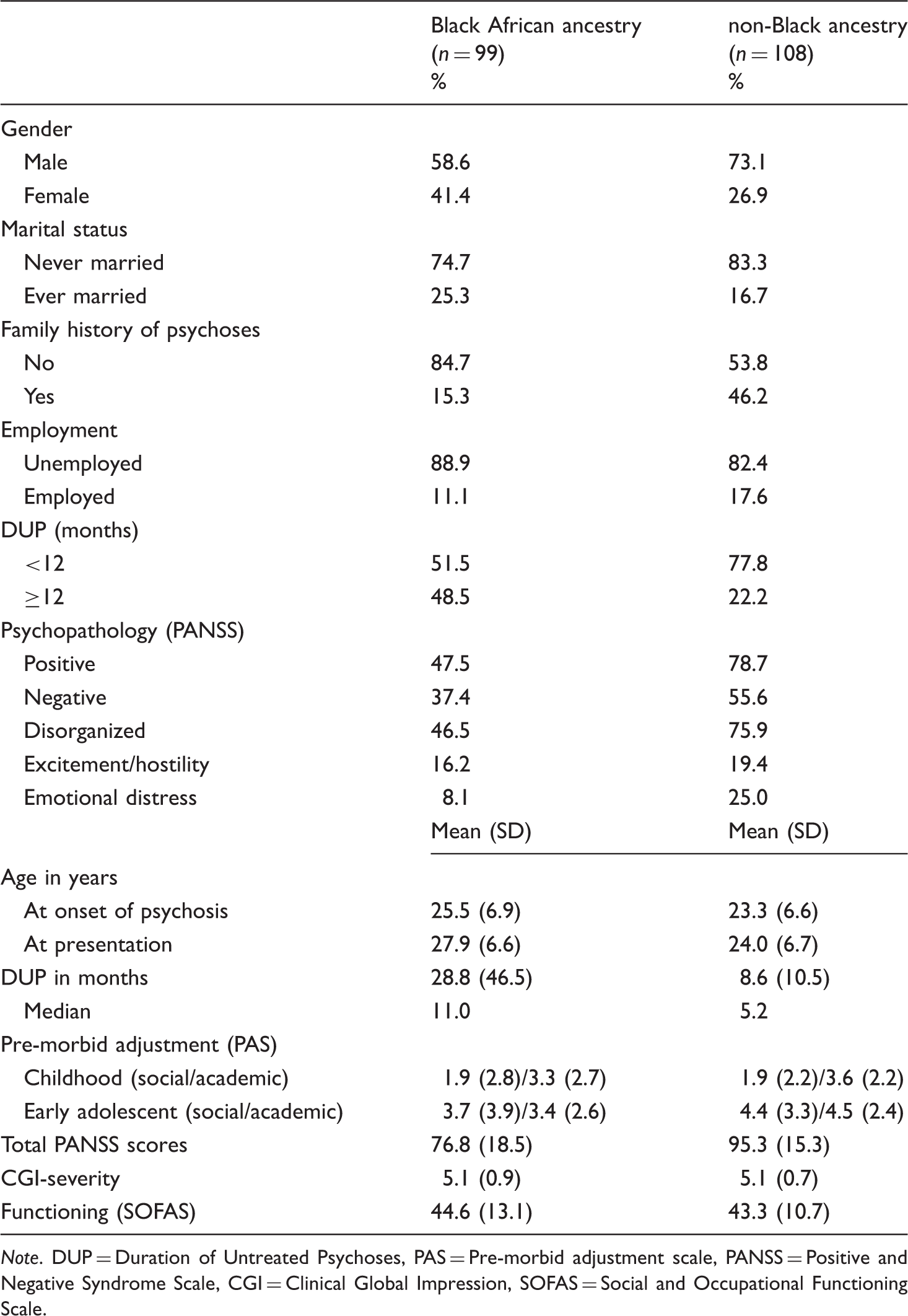
Note. DUP = Duration of Untreated Psychoses, PAS = Pre-morbid adjustment scale, PANSS = Positive and Negative Syndrome Scale, CGI = Clinical Global Impression, SOFAS = Social and Occupational Functioning Scale.
Frequency and severity of neurological abnormalities in the Black and non-Black African ancestry samples.
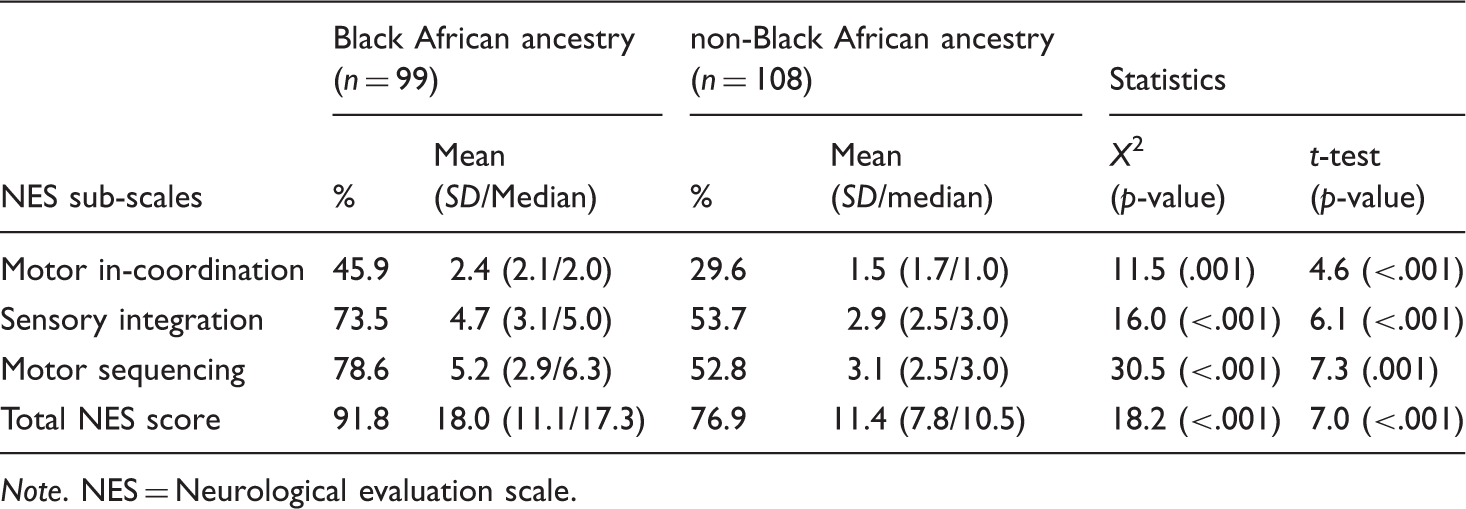
Note. NES = Neurological evaluation scale.
Factor structure and similarities in Black and non-Black African ancestry participants.
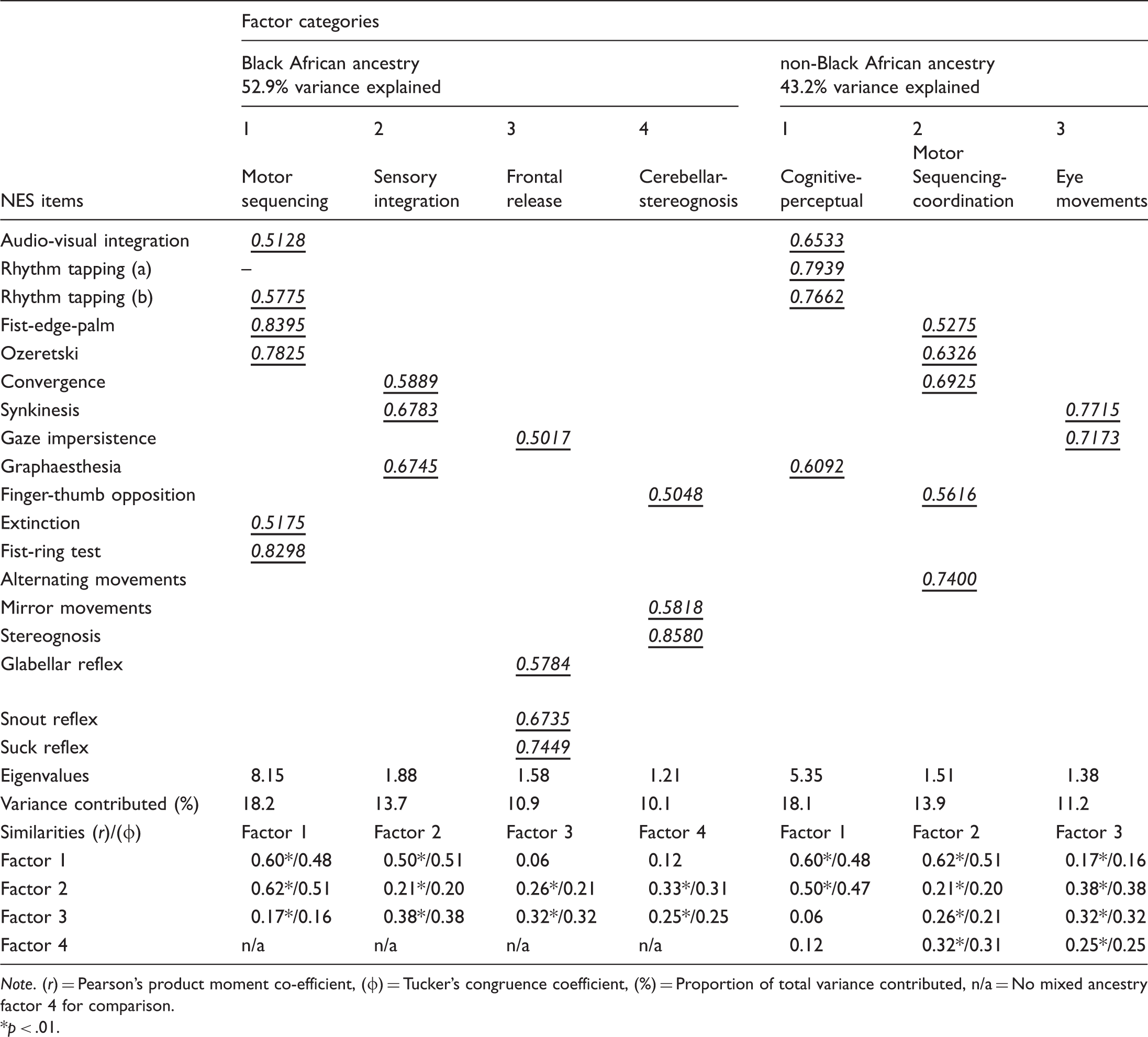
Note. (r) = Pearson’s product moment co-efficient, (φ) = Tucker’s congruence coefficient, (%) = Proportion of total variance contributed, n/a = No mixed ancestry factor 4 for comparison.
p < .01.
Conceptual meanings of the factor categories were derived based on previously identified categories. For the Black African ancestry sample: Factor 1 (audio-visual integration, fist-ring, fist-edge palm, Ozeretski, rhythm tapping (b), and extinction tests) was mostly “Motor sequencing” (Heinrichs & Buchanan, 1988); Factor 2 (Graphaesthesia, rhythm tapping (a), synkinesis, and convergence) was mostly “Sensory integrator” (Heinrichs & Buchanan, 1988; Malla, Norman, Aguilar, & Cortese, 1997); Factor 3 (gaze impersistence, glabellar tap, snout, and suck reflexes) was mostly “Frontal release” (Egan et al., 2001; Peralta et al., 2011); while Factor 4 (stereognosis, finger-thumb opposition, and mirror movements) was mostly “Cerebellar-stereognosis” (Egan et al., 2001). For the Non-Black ancestry sample: Factor 1 (audio-visual integration, graphaesthesia, rhythm tapping (a and b), and extinction) was mostly “Cognitive-perceptual” (Sanders et al., 2000); Factor 2 (fist-edge palm, and Ozeretski tests, rapid alternating movements, finger-thumb opposition, and convergence) was mostly “Motor-sequencing-coordination” (Malla et al., 1997); while Factor 3 (synkinesis and gaze impersistence) comprised of “Eye movement” abnormalities (Ojagbemi, Akpa, Esan, Emsley, & Gureje, 2015). Functionally, the eye signs may have sensory integrator characteristics (Heinrichs & Buchanan, 1988; Malla et al., 1997).
Also in Table 3, the indices of statistical similarities in factor structure of NSS in the two ancestry groups are presented. Notably, correlation between the NSS factors in the two ancestry groups were mostly low to moderate. Also, there were no statistical similarities between factors in the two groups (Table 3).
Neurological soft signs and clinical characteristics of schizophrenia in the Black and non-Black African samples.
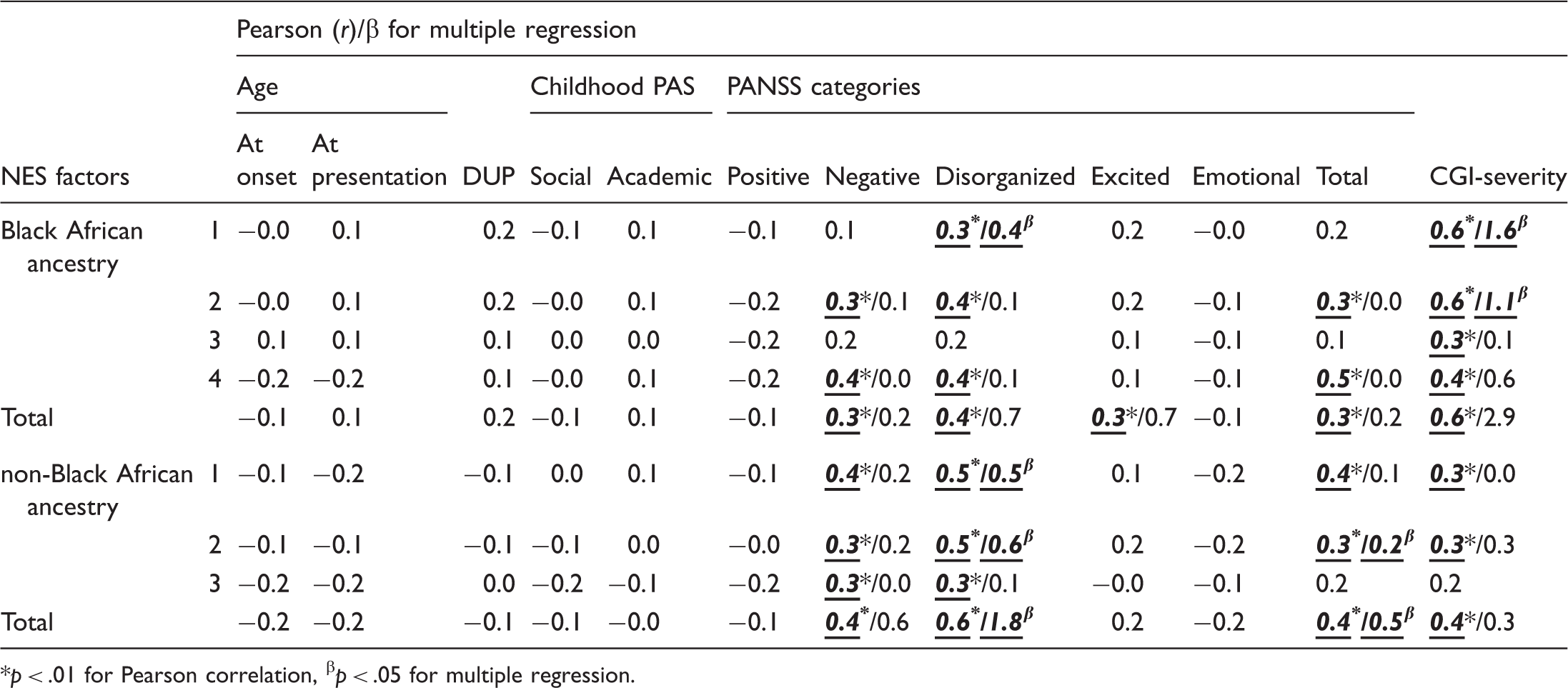
p < .01 for Pearson correlation, βp < .05 for multiple regression.
Discussion
This study is based on a sample of over 200 mostly medication naïve or minimally treated patients with first episode schizophrenia drawn from two independently replicated studies in ethnically distinct populations of Africans. We report a high prevalence of NSS in the two ancestry groups (Black and Non-Black Africans) before the institution of antipsychotic medication treatment. The NSS exhibited important differences in frequency, severity, and factor structure in the Black African compared with the non-Black ancestry sample. Neurological soft signs, especially Motor sequencing and Cognitive-perceptual abnormalities, were associated with severe negative and disorganization psychopathologies in the two ancestry groups. NSS were also associated with excitement/hostility psychopathology in Black African participants.
The finding of a high prevalence of NSS in both participant groups is in keeping with previous studies of NSS in anti-psychotic naïve patients with first episode schizophrenia (Dazzan et al., 2004; Keshavan et al., 2003; Zabala et al., 2006). This observation has often been interpreted to mean that the signs are not due to the effect of antipsychotics (Dazzan et al., 2004). The higher prevalence and severity of NSS in the Black, compared with the non-Black African ancestry participants is also in keeping with some previous studies comparing African American and Caucasian subjects with schizophrenia (Compton, Bercu, Bollini, & Walker, 2006; Keshavan et al., 2003). The possibility that longer DUP in the Black African Ancestry group might have accounted for the differences in prevalence of NSS is made less likely by the finding in subsequent analyses that NSS were not statistically associated with DUP in either ancestry groups.
The interpretation and clinical relevance of the differences in the prevalence of NSS according to self-described ethnoracial categories in studies conducted using samples in Europe and North America have often been unclear. The possibility that these differences may have genetic basis has been challenged because of high genetic admixture in diverse populations (Mersha & Abebe, 2015). As such, self-described population categories such as race and ethnicity do not often match up to empirically determined ancestry in such settings (Bresnahan et al., 2007; Rotimi & Jorde, 2010). In the present study, we have used samples derived from two ethnically distinct African populations. The Black African sample of Yoruba and Xhosa patients has proven common ancestry (Yoruba and Xhosa) based on genetic (Bryc et al., 2010; Tishkoff et al., 2009) and anthropological (Ehret, 2001) evidence. The literature on NSS in healthy individuals is notably sparse. Available studies are based on populations outside the African continent. These studies have mostly extrapolated from findings when using normal controls in comparison with schizophrenia (Compton et al., 2006; Dazzan et al., 2006). In many such studies, prevalence rates of between 0 and 50% have been reported among normal control populations.
In keeping with the trends demonstrated by the differential frequency of NSS among Black compared with the non-Black African ancestry sample, our factor analyses and comparisons demonstrated the absence of statistical similarities between the factors in the two groups. While expressions of intermediate phenotypes such as NSS are unlikely to exactly match those of specific genes, they are able to provide proximate information for the understanding of gene functions in the relevant disease (Braff et al., 2007; Gottesman & Gould, 2003). The finding of differences between the Black African and non-Black ancestry populations in this study would suggest that, as with the expression of genes (Bryc et al., 2010), NSS are expressed differently in populations with differing genetic ancestry. Using genomic techniques (Bryc et al., 2010; Tishkoff et al., 2009), a consistent genetic clustering has often been demonstrated among Africans belonging in the “Niger-Kordofanian family” (Ehret 2001), extending from Yoruba speaking areas of West Africa, through Kongo speakers in East Africa, to the Venda/Xhosa speaking regions of South Africa. Given the evidence of NSS co-segregation with the schizophrenia phenotype (Mechri et al., 2009; Neelam et al., 2011), the finding of differences in severity, and factor structure of NSS in the Black compared with the non-Black African patients with first episode schizophrenia in this study may not be surprising.
It is important to note that there were conceptual similarities between some of the factors in the non-Black (Factors 2 and 3) and Black African (Factor 1) samples. In keeping with this pattern, we found in this study that conceptually similar factors demonstrated the same pattern of association with the clinical characteristics of schizophrenia. For instance, while NSS were generally associated with severe negative and disorganization psychopathologies, the Black African ancestry Factor 1 and the non-Black ancestry Factor 2 (both motor sequencing) were independently associated with disorganization psychopathology in multiple regression analyses. Motor sequencing NSS and disorganization psychopathology in schizophrenia reflect abnormalities of context processing (i.e., action and speech planning, respectively, in the presence of competing events) (Zalla et al., 2006). This occurs following changes in pre-frontal integrity (Gay et al., 2013; Rao et al., 2008).
The finding in this study of a relationship between NSS and excitement/hostility psychopathology of schizophrenia has not been previously reported. This relationship is present in the Black African sample. There is a possibility that this may be an artifact, as some of the acute phase symptoms of schizophrenia are known to affect the performance of patients on neurological tests requiring repetitive movements (Lawrie et al., 2001). Another possibility considered is that previous studies of the relationship between NSS and schizophrenia psychopathology have relied on the older three sub-scales of the PANSS (Kay et al., 1987). This earlier model had no separate excitement/hostility category. As such, the relationship between NSS and excitement/hostility was not reported in studies using this version of the PANSS. On the other hand, some neuro-imaging studies using the five factors model have found an association between the excitement/hostility component and activation of the right pre-frontal cortex (Nishimura et al., 2011). While it is important to note that the pre-frontal cortex sub-serves impulsivity and disinhibition, the relationship between NSS and excitement/hostility in groups of patients would require further verification in future studies.
There are several factors limiting the interpretation of our findings. First, while the measurements were conducted independently by trained raters using uniform methods with good IRR, raters were not blind to the clinical state of the patients. Therefore, we are unable to completely eliminate the possibility of observer bias. Nevertheless, the near perfect ICC would suggest a consensus of measurements between raters. Furthermore, the large sample size should allow for a wider generalization of our findings to many sub-Saharan African contexts. Second, it is not possible to ascribe the differences between the populations to genetic factors alone. There are numerous environmental factors that could account for the NSS differences that were not assessed in the present study. These include potential differences between the sites regarding factors such as obstetric complications, general medical conditions, nutritional status, educational status, and substance use. Third, we did not include a healthy control group so that inferences regarding severity of NSS in schizophrenia compared with the rest of the population cannot be made. Strengths of the study include the relatively large sample, the inclusion of first-episode, largely unmedicated patients (thereby excluding confounding effects of illness chronicity and treatment), and the use of standardized and validated instruments to measure NSS and other clinical symptoms.
Conclusion
We have found important statistical and conceptual differences in the severity, factor structure, and clinical correlates of NSS in this large sample of Black compared with non-Black African patients with first episode schizophrenia. This provides preliminary evidence that NSS may follow patterns of expression according to ancestry. Although this finding requires confirmation from similarly designed studies using a larger number of ethnically and geographically diverse populations, it raises the possibility that NSS might represent affordable and easy to measure proxies for ancestral information required for genetic homogeneity in schizophrenia research. Better characterization of patients beyond categories such as race and ethnic groups (which are usually self-ascribed) should help with the accurate assessment of variations in the risk of schizophrenia among populations, response to bio-medical treatments, and adverse drug reactions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.