
Abstract
While involvement of family caregivers can play an important role in the recovery process of persons with serious mental illness (SMI), family caregivers often endure poor health and mental health issues due to caregiving-related distress. These challenges may be exacerbated for Vietnamese American families due to cultural values (e.g., familism and stigma). This qualitative exploratory study examined how Vietnamese American family caregivers of persons with SMI describe their caregiving experience. Using convenience and snowball sampling, the study recruited 21 participants who took part in two Vietnamese-language focus groups. Key findings of the study addressed three themes: (1) the influence of cultural and religious values on caregiving and mental health; (2) the negative impact of caregiving on caregivers’ wellbeing; and (3) the stigma attached to mental illness. The study offers useful insights to assist mental health practitioners in tailoring culturally appropriate and effective services for Vietnamese caregivers.
Keywords
Although serious mental illness affects many areas of a person’s life including daily functioning, employment, relationships, and overall health, individuals with mental illness can improve with proper treatment and family involvement (Cumming & MacNeil, 2008; Kaye, 2011). In the USA, one in 17 individuals lives with a serious mental illness such as schizophrenia, major depression, or bipolar disorder, which interrupts their cognitive and/or behavioral functioning (National Alliance on Mental Illness [NAMI], 2012). As a result of this disrupted functioning, mental illness has been recognized as a major cause of disability (Bond & Kukla, 2011), which often causes affected individuals to rely temporarily or permanently on their family for care. When caregivers co-reside with persons with serious mental illness (SMI) they may experience a higher level of daily caregiving burden due to the barrage of emotions and stresses related to finances, shelter, and the overall wellbeing of the person with SMI. Caregiving-related burdens can manifest as caregiving-related distress which increases the likelihood of developing mental health problems among family caregivers (FCs) (Crowe & Brinkley, 2015; Griffith, 2012; Kaye, 2011; McCann, Bamberg, & McCann, 2015).
While family involvement can have a positive impact on the recovery process of persons with SMI, existing studies show that family members who care for persons with SMI may experience chronic and persistent psychological and emotional pain, agony, and distress that often go unrecognized and untreated (Caqueo-Urízar, Gutiérrez-Maldonado, Ferrer-García, & Miranda-Castillo, 2012; Shah, Wadoo, & Latoo, 2010; Zauszniewski & Bekhet, 2014). Previous studies on non-Hispanic White FCs in the USA indicate that caregiving for a family member with mental illness is associated with poorer health and a decrease in overall quality of life for the caregiver (Caqueo-Urízar et al., 2012). Caregiving distress among ethnic minority FCs of persons with SMI has been attracting more interest among mental health professionals, researchers, and policy makers, as seen in the increased number of studies focusing on FCs of persons with SMI in the African-American and Hispanic populations. While these studies show that many family caregivers suffer from psychological, physical, financial, and familial stresses (Baldassano, 2004; Caqueo-Urízar et al., 2012; Hsiao, 2010; Kingston, Onwumere, Keen, Reffell, & Kuipers, 2016; Lively et al., 2004), they also emphasize that cultural factors can structure a caregiver’s attitudes, values, and behaviors and influence their wellbeing. This is because people’s learned responses to stress are shaped by their social and cultural context (Casstevens, 2012; Griffith, 2012; Hasson-Ohayon, Levy, Kravetz, Vollanski-Narkis, & Roe, 2011; Tan et al., 2012).
Our literature review indicated that very little is known about the caregiving experience among many recent immigrant populations in the USA, including Vietnamese Americans. The majority of the Vietnamese population in the USA came as refugees after 1975 and their numbers have grown since, almost doubling every decade from 1980 to 2000 and then increasing 26% in the 2000s. As of 2014, Vietnamese Americans comprised the sixth largest immigrant group in the USA (Miller, 2015). This rapid growth of the Vietnamese population deserves attention in the literature on mental health and caregiving because Vietnamese immigrants to the USA are known to have a relatively high prevalence of mental health problems (Hays, Manione, Metzger, & Sorkin, 2008; Hsu, Davies, & Hansen, 2004; Leung, Cheung, & Cheung, 2010). Vietnamese Americans have a higher tendency for family co-residency (Pishori, 2015), and strong cultural value of familism (Han, Cao, & Anton, 2015; Hsiao, 2010), which may heighten the burden on Vietnamese caregivers and the family unit, placing such caregivers at a higher risk of developing health and mental health issues (Leung et al., 2010). Despite these potential issues, few studies have examined how cultural values related to caregiving and mental illness impact on Vietnamese FCs of persons with SMI in the USA. To address this gap in the research, we utilized an exploratory design to answer the following research question: What are the self-described experiences of immigrant Vietnamese family care givers of persons with SMI living in the USA? Specifically, we explored participants’ views on how their cultural background influenced their caregiving experience, including their emotional experience as caregivers. A family caregiver was defined as any family member who provides physical and/or emotional care for a loved one with serious mental illness residing in the same home.
Literature review
To contextualize findings on how Vietnamese immigrants experience caregiving for relatives with serious mental illness, we first examine key cultural values in this population, such as familism and the role of religion. Based on Confucianism, familism dictates that the needs of the family take priority over the needs of individual family members. Familism, or family obligation, is a critical component of Vietnamese culture, and it refers to an implicit societal expectation of mutual support among family members (Luu, Leung, & Nash, 2009; Mak & Cheung, 2012). Vietnamese culture also places a great emphasis on religious notions of morality. Indeed, many Vietnamese immigrants conceptualize mental illness as resulting from bad thoughts, a lack of willpower/personality weakness, possession by spirits, fate, and/or karmic repayment for the misdeeds of their ancestors or for their own previous lives (Han et al., 2015; Hsu et al., 2004; Luu et al., 2009).
While no empirical studies of immigrant Vietnamese FCs of persons with SMI exist, several similar studies on persons with dementia reveal the significant influence of cultural values on caregiving. Traditional Confucian and Vietnamese values tend to discourage the use of institutional services, resulting in increased burdens for FCs (Han et al., 2015; Hinton, Tran, Tran, & Hinton, 2008; Leung et al., 2010). Vietnamese culture generally echoes the Confucian values of strong family ties, mutual obligation, loyalty and collective responsibility. This sense of familism can drive immigrant Vietnamese caregivers to persevere despite the difficulties they endure (Hinton et al., 2008).
Additionally, Hinton et al. (2008) found that immigrant caregivers often coped with their own suffering by seeking solace in religion. Vietnamese religious values can be an important resource for immigrant caregivers of persons with SMI in sustaining their motivation, understanding the nature of their loved ones’ mental illness, and managing their personal suffering. Buddhism is strongly embedded in Vietnamese culture, with Buddhists comprising 43.5% of the overall religious population in the country of Vietnam (Central Population and Housing Census Steering Committee, 2009). Buddhism is also the predominant religion among the Vietnamese American community in the USA, with an estimated 45% affiliated with this religion (Statista, 2017). The Buddhism practiced by Vietnamese today is mainly of the Mahayana school, and its philosophy places primary importance on compassionate acts motivated by a desire to alleviate the suffering of others. The Vietnamese perception of mental illness is integrally linked to Buddhist concepts of suffering and karma. The term karma in Sanksrit language literally means “action”, but Buddhism refers to this concept as the law of causation. Karma can help us to rationalize our present situation: good and bad outcomes in this life are seen as the reciprocal consequences of good or bad deeds in this or previous lives (Thakkar, 2015). The life challenges one faces are a matter of unavoidable natural consequence (Hinton et al., 2008; Nguyen, 2003). Accordingly, most Vietnamese people view their suffering as a result of poor karma (Han et al., 2015; Hsu et al., 2004; Luu et al., 2009). These religious values assist caregivers in ascribing meaning to their caregiving experiences.
While its introduction to Vietnam dates back to the 16th century, Catholicism grew in the 18th century to become the country’s second largest religion. Bangston (2000) estimated that Catholics comprised about one-third to one-quarter of post-war Vietnamese immigrant refugees although they are less than one-tenth of the total Vietnamese population (World Factbook, 1999). Catholicism, like Buddhism, may provide an important resource for coping among Vietnamese immigrant caregivers of persons with SMI. A previous study of predominantly Catholic Vietnamese caregivers showed that they found emotional support and maintained their motivation through religious observance (Hinton et al., 2008).
Social stigma and its impact on the Vietnamese community
Regardless of ethnic background, stigma remains one of the greatest barriers to families seeking professional mental health services (Pescosolido, 2013). Vietnamese attach a high level of stigma to mental illness, which significantly affects their help-seeking attitudes and behaviors leading them to underutilize mental health services (Wong, Kim, & Tran, 2010). Mental illness is associated with shame, ostracization, and loss of face in the community (Kramer, Ton, & Lu, 2008). In Vietnamese households, defined familial roles often prioritize one’s family obligations over individual desires (Nguyen, 2003). A mentally ill person’s behaviors may be considered as negative acts that bring shame to his/her family, relatives, and ancestors (Nguyen & Anderson, 2005). Therefore, in order to maintain their reputation, many Vietnamese families hide family members’ mental illness until the situation becomes unbearable (Nguyen & Anderson, 2005).
According to Nguyen (2003), the history of psychiatry in Vietnam helps to explain why Vietnamese people still consider psychiatric institutions a last resort. Formal psychiatry was first introduced in Vietnam during the French colonial period in the early 20th century. Psychiatric clinics during this period served primarily as custodial wards to imprison patients rather than rehabilitate them. In 1919, the French built the first psychiatric hospital in Biên Hoà Province, which the locals called the “crazy house of Biên Hoà”.
Even after renovation in 1939, Bach Mai general hospital in Hanoi still contained a special area called the “Et Prisonniers Service des Aliénés” (And Prisoners Services of the Insane), which was used to imprison people with dysfunctional behaviors, sick prisoners, and political dissidents (Le & Nguyen, 2014; Nguyen, 2003). During the 1950s, clinical psychiatry in Vietnam slowly transformed. Hospitals that initially functioned mainly as custodial wards began to act as treatment centers. Since then, mental health care in Vietnam has improved substantially, and there have been advances in policies and practices in the last 50 years to enhance the efficacy and availability of mental health treatment. However, public attitudes and the pervasive societal stigma against those with mental health problems persist (Nguyen, 2003).
In summary, the studies described above support the premise that among ethnic minorities cultural values greatly impact FCs’ perceptions of mental health problems and caregiving. Given the lack of studies focusing specifically on Vietnamese Americans in this literature, we sought to explore the relationship between caregivers’ cultural frameworks and the negative as well as positive aspects of caring for persons with SMIs in this population.
Methods
Study Design and sample
This exploratory study utilized semi-structured focus group interviews with Vietnamese FCs of persons with SMI to illuminate the caregiving experience and the influence of cultural values. Because the study aimed to gather information about beliefs, values, and practices shared within a cultural group, we used the focus group method, which allows for discussion and interaction among participants.
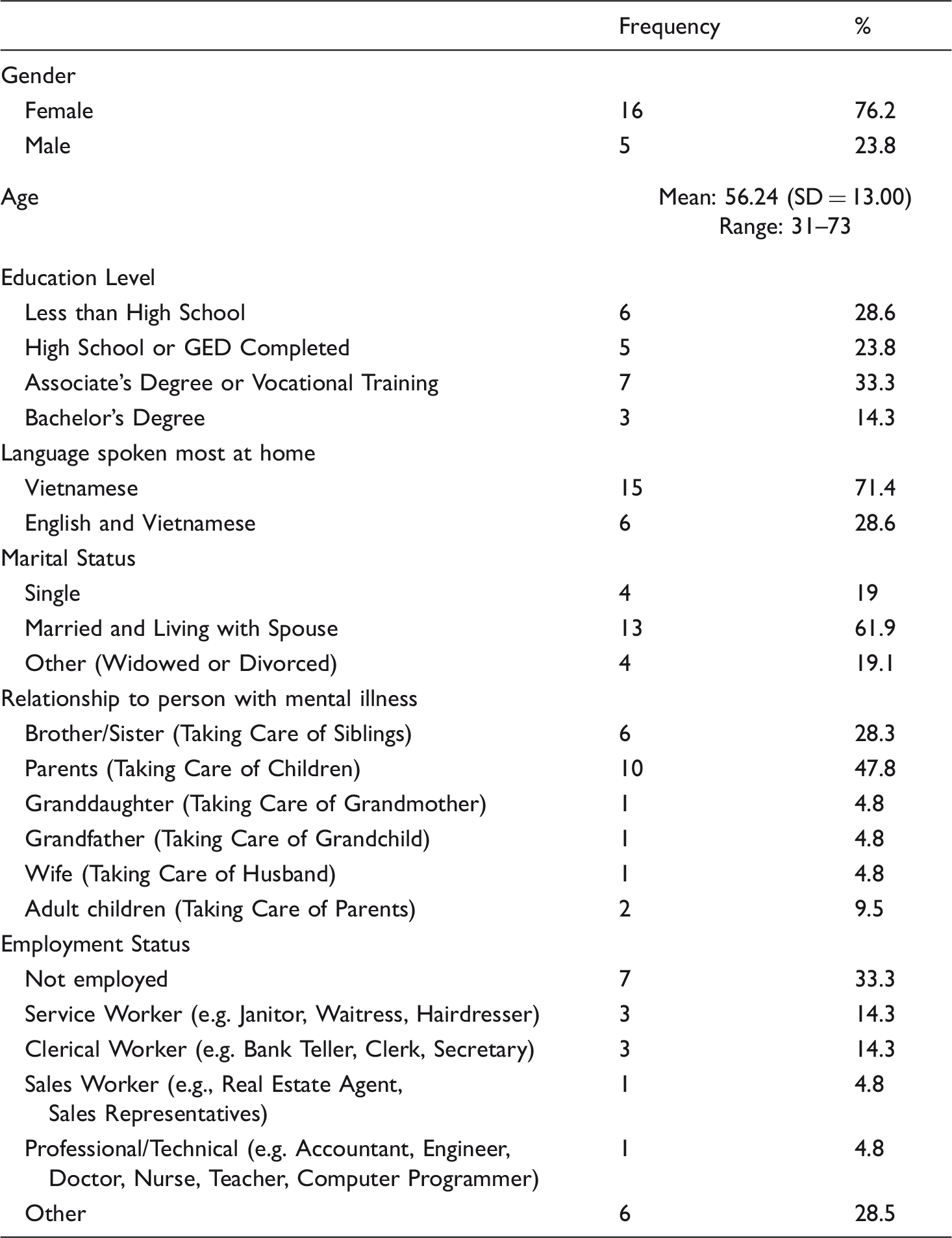
Participants’ Characteristics (N = 21).
Sampling and recruitment
Study recruitment, using a combination of convenience and snowball sampling, took place in Santa Clara County (SCC), California, in collaboration with several organizations including the National Alliance on Mental Illness Santa Clara County (NAMI SCC) and two community-based organizations in SCC that provide out-patient behavioral health services to primarily Vietnamese immigrants/Vietnamese-American clients. The predominant recruitment method involved posting flyers (in Vietnamese) and circulating a newsletter description (through NAMI SCC) that invited family members of clients of the community-based mental health clinics and Vietnamese members of NAMI SCC, along with any friends and family who were also FCs of persons with SMI, to participate in the study. Both the flyer and the newsletter description included information about the purpose of the study, the confidential nature of the group, and how to register if interested.
Prospective participants who contacted the study’s bilingual research assistants were screened using the following criteria: 1) Vietnamese FCs of persons with a serious mental illness, such as schizophrenia, bipolar disorder, or major depression; and 2) currently living with the person with SMI. Focus groups were held at a location familiar to the immigrant Vietnamese community, which had held multiple events there previously. The study proposal was approved by the San José State University Institutional Review Board (IRB) and all members of this research team, including the research assistants, completed training on the protection of human subjects.
Data collection
Two bilingual Vietnamese-English graduate student research assistants from a Masters in Social Work program translated the study materials, including the consent forms, conducted the focus groups, which were audio-recorded, and then transcribed the recordings. Both graduate students’ Vietnamese language proficiency was considered to be high based on their training and experience working with Vietnamese immigrants in the health/mental health field.
Data collection consisted of two semi-structured focus group interviews of 1.5 hours each with Vietnamese FCs of persons with SMI. When participants arrived for the focus group, they received a written consent form that described the purpose of the study, the nature of their voluntary participation, the potential benefits and risks of their participation, confidentiality and audio-recording, which they reviewed and signed prior to participating in the focus groups. During the focus group, participants’ caregiving experiences were explored through the following two main questions: 1) Please tell us how you think your cultural background influences your thoughts about and experiences with mental illness and caregiving; and 2) Caregivers often report having a variety of emotions or feelings at different times – both positive and negative. Please tell us about the feelings or emotions that you experience at different times when caring for your family member. Within these two broad questions, we explored various aspects of the caregiving experience such as caregivers’ views on mental illness, their roles as caregivers, and the ways caregiving influenced their lives and overall wellbeing. Further, instead of approaching the question of Vietnamese cultural influences on caregiving with a preconceived framework, we asked participants in an open-ended manner to reflect on how culture and immigrant status might influence the totality of their caregiving experience.
During the focus groups, one bilingual student researcher who had training and clinical experience in group work assumed the primary moderator’s role of facilitating the discussion in Vietnamese. This moderator encouraged everyone to participate in the group discussion and probed for further information by observing nonverbal clues and following up on ambiguous statements. The second bilingual student researcher monitored the group process and time management. The study investigators were also present at both groups to observe the process and answer any questions that participants had about the study.
Verification of qualitative data and analysis
To increase the credibility of the qualitative data, we performed word-for-word translations of the focus groups from Vietnamese to English and then back-translated from English to Vietnamese. In order to ensure the accuracy of the transcription of the study material, we also gave the recording to a third Vietnamese bilingual student research assistant who was not involved in the focus groups. She completed a separate, independent translation and back-translation of the data. The final versions of the translated transcripts were then reviewed again by the first author, who is bilingual and whose first language is Vietnamese. We then compared these translations to the original version and identified and eliminated any inconsistencies. After transcribing the material, qualitative analysis involved an iterative process of reading and rereading interview transcripts to identify themes. Using Luborsky’s (1994) thematic analysis approach, five research team members, including the authors, read the transcripts to identify overarching themes and subthemes regarding caregiving experiences and challenges and the role of cultural factors. Subsequently, each author independently read all of the transcripts and coded the data using the themes and subthemes developed.
Results
Three main themes emerged from our analysis of the data: 1) the influence of cultural values, such as beliefs and religious factors, on FCs’ experiences related to caregiving and mental illness; 2) the negative impact of caregiving on caregivers’ psychological wellbeing; and 3) stigma as a key challenge to seeking external help.
Theme 1: The influence of cultural values
When participants were asked about how one’s cultural background may influence the caregiving experience, they discussed several cultural values, including Confucian ideals of family obligation/familism as well as core principles of Buddhism and Catholicism/Christianity.
Family obligation
Participants described the importance of fulfilling their family obligation by practicing “self-sacrifice” when taking care of a person with mental illness. Based on cultural values associated with Confucianism, participants agreed on the importance of bearing difficulties and enduring self-sacrifice in order to demonstrate love for the person with mental illness. Caregiving responsibilities disturbed many aspects of caregivers’ lives, but caregivers still seemed ready to overcome any obstacles and endure any hardship necessary to take care of their mentally ill family members. One participant shared the following: Even though I know money is necessary, my son is more important to me than money. That is why I sacrificed everything to stay home to take care of him. He got sick by nature, so it is our responsibility to take care of him.
Karma and Buddhism
According to some participants, Buddhism helped to explain their understanding of mental illness and the impact it had on them. They emphasized how Buddhist teachings focused on the philosophy of karma could explain why a person has a mental illness. The participants shared that their suffering stems from their karma. For instance, one participant stated, Based on Buddhism, it’s karma. A person did some bad things in one incarnation/past life, thus he has to suffer in his current incarnation. …Why is my brother the only one with this illness? That’s why I think karma is the reason.
Catholicism/Christianity
A parallel exists for caregivers with other religious affiliations. Similar to those relying on the Buddhist concept of karma as a mechanism for understanding suffering related to mental illness, some participants mentioned the impact of religious prayers to God. This is well summarized by the following statement: …but we keep praying [asking my loved one to keep taking medication, then God gave us a special method [to overcome personal hardships and then things turn] like a normal one … that’s why because of our prayer, our higher being is really nice. That’s why God has made our son normal now.
Theme 2: The negative impact of caregiving on caregivers’ psychological wellbeing
Even though participants generally accepted caregiving as their responsibility, this acceptance did not seem to lessen the degree of their burden. Participants reported the negative impact of caregiving on their general wellbeing and on their social, family, and personal lives.
Impact on wellbeing
Participants in both focus groups shared about the intense emotions and feelings of frustration and worry they experienced as a direct result of constant exposure to the behaviors of the person with SMI. One FC said the following: By taking care of him, I have learned many things, such as how to control my temper. If I let go of my temper, it would be like “adding oil to the fire.” So I learned to be patient, but I do think that patience has a limit. If we put up with too much, then we might end up having the same mental problems. He (my son) made me stressed out and so nervous. Sometimes, he just took a knife and then ran into the streets, or he just really likes to argue with his younger brother. I was really worried every time I went out, like to the supermarket. It causes me to lose sleep, and then I have to consult a doctor. I think I have this mental problem [myself].
Impact on social and family life
Participants reported that behaviors of the person with SMI and dislike of social situations prevented the entire family from attending social functions. The caregivers felt compelled to perform constant and intensive monitoring of the person with SMI, which further prevented them from attending most community events. One FC discussed this issue as follows: My life has changed a lot. For example, every Friday night, my family got together to sing karaoke. Then my sister got sick, and every time we sang, she yelled “too loud, too loud.” Then she forced everyone to stop singing and turn the karaoke machine off. We began to do less and less on Friday night, and now we don’t do anything ... Like on Sunday, I went to a tournament to support my team. It’s like an all-day thing, but she couldn’t even take one day with me being gone ... When I came home, I checked the number and she was knocked out. And the next morning when I called her back, she attempted suicide by drinking a lot of Nyquil … so just basically getting out of the house, but it’s like a catch 22. The negative aspect is that I feel trapped because I put my career on hold. People keep asking me, “What are you going to do?” So I said, “Well, I am going to take care of my mom first.”… And people keep on asking me, “Are you going to take care of your mom forever?” You know, she is really affecting my life. I can’t even be gone for one day, you know, so I feel trapped. I do not want to look into the future, knowing that she might get worse.
Theme 3: Stigma as a key challenge to seeking external help
One of the most important aspects of the focus group discussions concerned how the stigma attached to mental illness, reflected in a negative and disempowering way of talking about persons with SMI, impacted Vietnamese FCs. For example, one person stated: The Vietnamese think that when there is a member in the family who has mental illness … they usually think that they are Khùng điên [crazy] or té giếng [falling into a well] or that something is seriously wrong with them. They do not view it as a normal illness, like a physical illness in the body … the Vietnamese still have a lot of stigmas about people with mental illness.
Participants reported that, due to stigma, Vietnamese caregivers avoided telling outsiders about their situation in order to avoid bringing shame and humiliation to the family. For example, one participant stated that, “… American society is greatly different from our [immigrant] Vietnamese society… Vietnamese society is all about saving face, as we are worried about humiliation since our kid got sick. We didn’t let anyone know.” Another participant also discussed this stigma, revealing that, “The Vietnamese think that when there is a member in the family that has mental illness… people usually judge them… Therefore, the outsiders discriminate against them.”
The participants also spoke at length in the focus group about the labeling of people with mental illness and their caregivers. The participants all agreed with the term người chăm sóc [caregiver] to describe themselves. Participants stated, “người chăm sóc [caregiver] is already the best. It’s clear and sounds good.” Participants agreed that the term often used to refer to mental illness in Vietnamese, tâm thần [mental], was very negative and stigmatized. The participants reported that in their opinion, tâm thần [mental] literally means “crazy” in Vietnamese. Overall, participants agreed that the Vietnamese population should only selectively use the phrase tâm thần [mental]. One participant shared that, In our Vietnamese society, when someone knows that your family has a person who has bệnh tâm thần [mental illness], they will start thinking that there is something wrong with your family bloodline. Because of this, people tend to hide their sick family members and do not take them to get treatment.
Participants discussed at length which term could best replace tâm thần [mental], debating between the terms tâm lý [psychological] or tâm trí [mind]. Finally, they decided that tâm trí [mind] is the best choice and suggested using this term to avoid the negative connotations of tâm thần [mental]. To support the use of the term tâm trí [mind], one participant stated: … to confirm the phrase we should use: illness that is related to mind (tâm trí), so whether the person has a severe mental illness or just a mild mental problem, we will still use the same term that is not harsh or negative.
It is important to note that several participants reported acculturation-related challenges such as language barriers and lack of information about resources, in addition to stigma-related barriers to seeking help. However, these challenges were only shared by a couple of participants and even though the moderator sought to explore this topic further with other participants, participants naturally went back to discussing their daily responsibilities in caring for a person with SMI. A similar situation occurred when the moderator specifically asked participants about any positive aspects of caregiving.
Discussion
This study offers insights into Vietnamese immigrant caregivers’ views on mental illness and their caregiving experiences. In line with a previous study (Pharr, Francis, Terry, & Clark, 2014), participants in our study reported following longstanding family-oriented traditions of mutual support and familism/family obligation. The findings suggest that the key cultural values of family responsibility and obligation lead many family members to endure difficulties and make necessary sacrifices to become primary caregivers.
We found that participants attribute a critical role to religion in influencing their attitudes and behaviors toward mental illness and the caregiving experience. More specifically, caregivers reported utilizing religion often to cope with distress, sustain their caregiving motivation, and maintain hope for the recovery of their charges. Some caregivers relied on the Buddhist concept of karma as an existential explanation for their suffering. Catholic worshipping activities also served as a source of emotional sustenance to enable caregivers to cope with caregiving stress and burden. Core moral orientations and spiritual values of Christianity/Catholicism direct worshippers to perform compassionate acts, to embrace the need to make sacrifices, and to reach emotional acceptance of caregiving hardships (Hinton et al., 2008). As Miltiades and Pruchno (2002) have pointed out, while religious/spiritual participation may not directly reduce caregivers’ emotional burden and stress level, regardless of denomination, religion served as a critical coping strategy.
As with previous studies reporting that Vietnamese caregivers suffer feelings of frustration, worry, and emotional burden (Caqueo-Urízar, et al., 2012), participants in this study experienced negative effects of caregiving on their wellbeing and social life. Our findings are consistent with prior research (MacNeil & Jaggers, 2013) suggesting the caregiving process negatively impacted FCs’ social relationships and professional lives (National Alliance for Caregiving and AARP, 2015). A recent study estimates that 70% of caregivers in the USA encounter challenges in maintaining employment due to their dual responsibilities (National Alliance for Caregiving and AARP, 2015). In our study, seven out of 21 caregivers (33.3%) were not employed, and those who did work reported struggles arranging their work or study schedules to accommodate their caregiving duties at home. The disruptive behaviors of persons with SMI and dislike of social situations prevented FCs from fulfilling their personal, social and professional needs and this may elevate caregivers’ risk of developing social isolation and depression (Caqueo-Urízar et al., 2012; Shah et al., 2010; Zauszniewski & Bekhet, 2014). Our study indicates the need for interventions to support caregivers such as the psychoeducational interventions focusing on problem-solving skills and coping techniques that have been shown to have a strong positive effect on caregivers in other populations (Gallagher-Thompson et al., 2000). Caregivers in this study suggested that a support group may also help to support their emotional wellbeing. Some of these caregivers in this current study previously attended a Vietnamese support group, but due to different factors (e.g., uninteresting group discussions, inconvenient time), many participants ceased attending and the program disbanded.
Social stigma also emerged as one of the main themes discussed at length by respondents. Participants repeatedly referred to negative attitudes toward mentally ill persons and to the stigma around mental illness in society in general and in the Vietnamese-American community in particular, lending support to previous research findings (Kramer et al., 2008). According to participants, stigma towards mentally ill people in the Vietnamese community originates from the presumed explanation for the origin of mental illness. Many Vietnamese would refer to “a bad family bloodline” as a root cause of families having a mentally ill member. Such beliefs substantially damage these families’ appearance and reputation in the community from which they derive self-worth. This stigma exacerbates the caregiving burden, makes the family reluctant to share information with outsiders, and prevents caregivers from seeking help due to feelings of shame and fear of losing face.
However, our findings indicate that this cultural barrier did not affect the help-seeking behaviors of caregivers in this study. In fact, caregivers seemed to exhibit pride at holding the title of người chăm sóc [caregiver]. One possible explanation for this finding is that the caregivers experienced religious fulfillment from completing their karmic obligations through providing care, which in turn assuaged the general cultural predisposition towards feelings of shame and reluctance to seek help.
Nevertheless, caregivers expressed their mutual frustration over the Vietnamese cultural stigma attached to mental health and emphasized the need to change this negative perception. For example, the term tâm thần [mental] has a benign literal meaning, but it has taken on negative connotations in everyday use. This partially stems from the historical background of mental health care in Vietnam. As previously discussed, the first psychiatric clinics, referred to in Vietnamese as bệnh viện tâm thần were built in Vietnam during the French colonial period. These hospitals initially functioned as custodial wards to imprison people rather than as treatment centers (Nguyen, 2003).
The public, in general, and Vietnamese immigrants, in particular, often refer to people receiving treatment at mental health clinics as “crazy” or “abnormal.” This severe stigma holds such societal power that the participants of the study viewed the phrase tâm thần [mental] very negatively. Caregivers could not differentiate between the stigma attached to the term by the historical trauma that persists in society to this day and the term’s actual definition, which lacks negative connotations. Thus, while tâm thần [mental] is the formally accepted term in mental health practice and research in Vietnam, caregivers proposed replacing it with the non-stigmatizing term tam tri [mind], defined literally as “mind” (Hoang et al., 1997). In mental health practice with the Vietnamese population in the USA, it may be useful and acceptable for service providers to utilize the less offensive term tâm trí [mind] to avoid the negative stigma associated with the term tâm thần [mental]. However, as these terms are not interchangeable in the Vietnamese language, to formally replace the term tâm thần [mental] with tâm trí [mind] would substantially alter the meaning of related phrases. Thus, further efforts should focus on addressing the root causes of stigma by increasing tolerance and the general population’s attitudes toward mental illness.
Limitations
First, due to the use of convenience and snowball sampling and the limited sample size, findings of this study may not be generalizable or representative of the whole population of Vietnamese-American caregivers. Second, since participants were already connected to some form of service in the community or institutional resource, the results may not be transferable to those with limited community contact or resource utilization. As such, the findings call for further research on Vietnamese caregivers in the USA. Finally, the study involved Vietnamese living in a single geographical region, which boasts the highest Vietnamese population in the USA. In light of the important contribution of ethnic density to acculturation (Ying, Han, & Tseng, 2012), which can influence help-seeking behaviors and the level of perceived stigma, future research should assess Vietnamese FCs’ experience in regions with lower ethnic density. Although several bilingual/bicultural research team members cross-checked the translated data, we did not use professional translators or blind back-translation which raises concerns for the validity of data and should be noted as another limitation of this study. Lastly, even though the participants in our study were immigrants, our research questions did not address how undergoing immigration may have shaped their experiences as caregivers. A future study is need to explore acculturation-related challenges among Vietnamese immigrant family caregivers to understand better how immigration and acculturation specifically might impact caregiving experience among Vietnamese immigrant family caregivers.
Conclusion
Consistent with previous literature, participants in this study reported negative impacts of the caregiving process on the emotional and behavioral health of caregivers. However, caregivers in this study showed a surprising openness to seeking external help for both their family members and themselves. Mental health practitioners, family physicians, and other professionals working in the community or primary care settings can respond to this need by providing information and strategies to assist FCs in coping with caregiver stress.
While some services for caregivers are available, many participants indicated that they were unaware of these services or found them difficult to access. Service providers should focus more on developing effective outreach strategies to inform help-seeking Vietnamese caregivers about ethno-specific resources. Researchers and practitioners may explore the possibility of designing and utilizing an online platform to meet the needs of Vietnamese caregivers. Such a platform could provide a confidential chat room where caregivers can attend online support group sessions from home; foster awareness about available service providers; and enable caregivers to share their experiences with, review and rate available public and private services to enhance information dissemination to cautious or less informed caregivers.
Caregivers’ use of religion as a coping strategy highlights the importance of cultural competence in providing care. As Boykin and Thompson (2007) note, patients may derive great solace from the accepting, compassionate environments of religious institutions. Our study found that this benefit extends to patients’ caregivers, who may turn to religion as a coping strategy. Mental health practitioners and religious institutions can collaborate to develop a strengths-based community support model, inform caregivers of available resources in the community, provide emotional support through home visits and respite services, and facilitate support group meetings.
While it did not emerge as a study theme, it is worthy to note that some participants in this study strongly suggested that a support group may also help their emotional wellbeing. Some of these caregivers previously attended a Vietnamese support group, but due to different factors (e.g., uninteresting group discussions, inconvenient time), many participants ceased attending and the program disbanded.
The majority of participants mentioned the negative impacts of stigma. To address the root cause of societal stigma, mental health stigma reduction programs must work to educate the broader Vietnamese American population. In order to change people’s negative perceptions of mental illness, programs should adopt an evidence-based approach focused on improving understanding of the nature of mental illness among Vietnamese Americans. Our findings suggest that practitioners should take the connotations of linguistic terms into account when discussing mental health issues with Vietnamese patients and their families in the USA: instead of using the term tâm thần [mental], which recollects negative stigma attached to mental illness, it may be acceptable for service providers to use the term tâm trí [mind]. Community education and use of less stigmatizing language may encourage early intervention and treatment by reducing feelings of shame.
Footnotes
Acknowledgments
We would like to express our heartfelt appreciation to the National Alliance on Mental Illness Santa Clara County (NAMI SCC) and all participants who participated in the focus groups for their support, contribution, and collaboration. Especially we want to acknowledge the following partners for their dedication, support, and contribution: Kathy Forward, Thong Le, Brian Pham, Lina Huynh and Mekong Vietnamese Community Center.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Silberman Faculty Development Grant in the New York Trust Fund provided funding for this research (Grant number: P13-000547).
Quynh Nhu (Natasha) Bui is a MSW postgraduate from San José State University and formerly a senior instructor in the Hanoi National University in Vietnam. Her research focuses on mental health issues, social development, poverty, service delivery for migrant, rural and urban poor neighborhoods and international social work. Her prior work investigated the health and social conditions of young migrants and the elderly population in Vietnam.
Meekyung Han, PhD is a Professor and a co-coordinator for the Institute for Community-Partnered Research in the School of Social Work at San José State University. Dr. Han’s research includes mental health services for Asian-American and other ethnic populations. Her published works focus on issues related to mental health and general wellbeing, and enhancing culturally sensitive and competent practice with ethnic minority populations with specific emphasis on Asian Americans. She was the Principal Investigator of the research project from the Silberman Faculty Development Grant that funded the current study.
Sadhna Diwan, PhD is the Director of the Center for Healthy Aging in Multicultural Populations (CHAMP) and a Professor in the School of Social Work at San José State University. Dr. Diwan’s research focuses on understanding the use of home and community based services among older adults, and on understanding factors related to the physical and psychological wellbeing of older immigrants. Her most recent work examines stress and coping among diverse groups of caregivers of adults with serious mental illness.
Tran Dao, MSW is a social worker for Santa Clara County Department of Adult and Aging (Home Supportive Services department) and a postgraduate student in the School of Social Work at San José State University. Tran’s research focuses on understanding mental health stigma and how it affects the community. Her most recent work examines the caregiving experiences in the cultural context of the Vietnamese-American family caregivers of person with mental illness.