
Abstract
Previous studies have documented a high prevalence of psychological distress and mental illness among older immigrants from the former Soviet Union (FSU) in Israel. Yet, this population rarely seeks help from mental health providers. The present study aimed to identify beliefs and attitudes about depression and anxiety among older immigrants from the FSU treated in primary care, and among their primary care physicians, who were also FSU immigrants. The study used focus group (FG) interviews with primary care patients (n = 12) and physicians (n = 23). The interviews were transcribed and analyzed using open thematic coding. Three main themes were identified: a) avoidance of discussion of mental health and stigma regarding mental illness; b) expectations to control one's mental state; and c) limited opportunities to acquire knowledge about Western mental health. Primary care physicians recognized the barriers facing their older immigrant patients concerning mental health diagnosis and treatment. Yet, due to work overload, their ability to assist older immigrants was limited. The findings suggest that older immigrants from the FSU might benefit from mental health information and exchange of ideas about Western mental health.
Introduction
The present study explores beliefs and attitudes regarding the nature of depression and anxiety among patients and physicians who migrated to Israel from the former Soviet Union (FSU) over two decades ago, and the ways of coping they consider appropriate for these conditions. We focused on depression and anxiety as these two conditions are most often treated in primary care (Roy-Byrne & Wagner, 2004) and are part of the work requirement of primary care physicians (PCPs) (Arroll Khin, & Kerse, 2003).
When examining attitudes towards mental illness, it is important to recognize that perceptions of normal versus abnormal behaviors are culturally constructed (Kirmayer, 2001; Yamada & Marsella, 2013). Normative practices related to the appraisal of and response to subjective feelings vary with cultural models. Emotional disturbances result in deviations from these normative cultural practices (Mesquita & Walker, 2003). Hence, the diagnosis of psychopathology requires assessing patient's symptoms and experiences as abnormal within the context of his or her cultural group (American Psychiatric Association, 2000). However, the definition of the immigrants' current “cultural group” is often ambiguous. Acculturation, which is defined as cultural and psychological changes following continuous contact and interaction between individuals from different cultures, is a dynamic process (Berry, 1997; Redfield, Linton, & Herskovits, 1936), which can result in differential manifestations of mental illness in immigrant populations. Immigrants often adopt parts of the host culture's perspectives regarding normal versus abnormal behaviors. Coping mechanisms and resources used to mediate stressors may also be culturally bound (Marsella & Yamada, 2010). These mechanisms and resources may be absent in the host culture, thus, putting immigrants at a heightened risk for mental health problems. Moreover, immigrants are often exposed to multiple stressors (Kirmayer et al., 2011), which can place them at a greater risk for mental illness.
The present study concerns immigrants from the former Soviet Union (FSU) to Israel, who currently comprise one sixth of the Israeli population (CBS, 2010). FSU immigrants arrived in Israel as part of a large wave, with over one million people during the 1990s and early 2000s (CBS, 2010). Immigration began following the collapse of the Soviet Union, which brought great fear of the unknown future, accompanied by a severe economic crisis, and high levels of anti-Semitism (Remennick, 2007). A major motivation for immigration to Israel was the relatively simple procedures involved, due to the Israeli Law of Return (Horowitz & Leshem, 1998), which allows entry and immediate citizenship to Jews, their children, and grandchildren, unrelated to their country of birth or residence.
The immigrants that arrived by the mid-1990s were a relatively homogeneous group. Mostly were highly educated Jews from urban areas, who chose to settle in Israel. Since the mid-1990s, the FSU immigration to Israel has become more heterogeneous, with a higher proportion of non-Jews, and less-educated individuals, from diverse geographic regions. Many of these new immigrants have suffered from personal and family difficulties. Their choice of Israel as a destination was primarily due to a strong desire to leave the FSU and limited opportunities to immigrate anywhere else (Kimmerling, 2004; Rosenbaum-Tamari & Demian, 2003). Despite their heterogeneity, FSU immigrants in Israel are thought to share cultural similarities, due to their common background as Jews (Remmenick, 1998), as well as their Soviet background, and subsequent experiences as immigrants in Israel (Mirsky, Baron-Draiman, & Kedem, 2002; Remennick, 2007). Despite the relatively high level of education and professional experience of FSU immigrants in Israel (CBS, 2006), their integration in Israel has faced various challenges, primarily due to underemployment (Gorodzeisky & Semyonov, 2011), limited social networks that consist of mainly FSU immigrants (Leshem, 2009), and a preference for the Russian language and culture (Lissitsa, 2007). Yet, FSU immigrants, particularly the younger generation, have gone through a constant process of integration into Israeli society and culture (Amit 2012; Gorodzeisky & Semyonov 2011; Leshem, 2009; Lissitsa, 2007). Nevertheless, compared with other Israelis,FSU immigrants report greater distress and psychiatric problems (Mirsky, 2009; Mirsky, Kohn, Levav, Grinshpoon, & Ponizovsky 2008; Ritsner, Ponizovsky, Kurs, & Modai, 2000; Zilber, Lerner, Eidelman, & Kertes, 2001) and their use of psychiatric medications is significantly higher (Ayalon et al., 2011). Therefore, there is a need to understand FSU immigrants' current cultural attitudes and practices regarding mental health in order to provide culturally appropriate services and interventions.
Within the Israeli community of immigrants from the FSU, older immigrants comprise a unique group. Unlike younger immigrants, many of the older immigrants still have a limited command of Hebrew (Remennick, 2003, 2004). Most have experienced underemployment and low wages, and many live on welfare allowances and part-time jobs (Litwin & Leshem, 2008; Remennick, 2003).
Mental distress in the form of anxiety, depression or somatization is high among immigrants of various age groups from the FSU (Jurcik, Chentsova-Dutton, Solopieieva-Jurcikova, & Ryder, 2013; Mirsky et al., 2008; Ron, 2007; Leipzig, 2006), even after they have lived in Israel for several years (Lerner, Kertes, & Zilber, 2005). The rates of mental distress and psychiatric disorders are higher among older compared to younger immigrants from the FSU (Mirsky, 2009; Zilber et al., 2001), and they are also more likely to somatize their distress (Ritsner et al., 2000). The mental difficulties of older immigrants have been attributed to the effects of immigration on their lives (Ritsner & Ponizovsky, 2003; Ron, 2007; Zilber et al., 2001) and to their poor state of physical health (Lerner et al., 2005). Social support has shown to moderate distress among this population, and its absence is a risk factor for mental distress (Ritsner & Ponizovsky, 2003).
Studies have found that in the early 1990s, immigrants who arrived from the FSU tended to have limited acquaintance with the topic of mental health, which was highly stigmatized, and had negative views on seeking professional mental help. This was associated with a lack of information about mental health, lack of experience in seeking formal help from mental health services, and mistrust of professional help (Leipzig, 2006; Auslander, Soskolne, & Ben-Shahar, 2005; Levav, Kohn, Flaherty, Lerner, & Aisenberg, 1990). In the Soviet Union, psychiatry was an outdated and abuse-ridden medical field. Psychiatric hospitals were often used to lock up political prisoners, there were no psychological or social services, and general mistrust of authorities prevented people from seeking confidence-based formal help for mental distress (Levav et al., 1990).
Studies conducted during the first decade of the 21st century found that FSU immigrants' willingness to seek help was low, both in Israel (Shor, 2007; Soskolne, Auslander, & Ben-Shahar, 2006) and in the US (Polyakova & Pacqulao, 2006). The percentage of immigrants from the FSU who sought mental health assistance was significantly lower than that of the rest of the Jewish population in Israel (Auslander et al., 2005; Ritsner et al., 2000). Lack of trust was a predominant explanation for the immigrants’ reluctance to seek formal help (Shor, 2007; Leipzig, 2006). At times of distress, immigrants from the FSU mostly chose to carry on without any help, or to seek informal help from family members and close friends (Lerner et al., 2005; Slonim-Nevo, Sharaga, & Mirsky, 1999). The formal help they favored was that of their PCPs (Polyakova and Pacqulao, 2006; Ritsner et al., 2000), who are the main gatekeepers for mental health services in North America and Israel (Thombs et al., 2012; Tabenkin & Gross, 2000). The preference to consult with PCPs might be linked with the immigrants' propensity to somatize their mental distress (Ritsner et al., 2000).
Research has shown that primary care immigrant patients from the FSU prefer being treated by a Russian-speaking PCP (Eger-Dreyfuss, 2005; Menachem, Zlichin, Zlichin, & Schwatzman, 2008). This may be especially important to the older population, whose have difficulty overcoming language barriers. Research has shown that PCPs who themselves had immigrated from the FSU catered to the needs of their FSU patients better than other PCPs, because they shared their language and culture, and were acquainted with the needs and expectations of their patients (Eger-Dreyfuss, 2005).
Despite the fact that PCPs tend to serve as gatekeepers in the case of mental health problems, they have been shown to have difficulties in treating mental illness because of a tendency to normalize and trivialize mental illness in comparison to other chronic medical conditions (Coventry et al., 2011). In Israel, PCPs identified multiple barriers associated with the management of depression and anxiety in primary care, including patient-level barriers, i.e., the diagnosis and treatment of mental illness in primary care, and system-level barriers, i.e., the limited time available for patient visits and the inadequate informal and formal support available for patients and providers alike (Ayalon, Karkabi, Bleichman, Fleischmann, & Goldfracht, 2016).
Given the discrepancy between the mental difficulties of older immigrants from the FSU in Israel, their infrequent use of mental health services, and their common use of psychiatric medications, the present study aimed to examine the perceptions of older immigrants from the FSU regarding depression and anxiety, and the ways they cope with these conditions. We specifically targeted primary care patients and PCPs in order to gain a more clinically relevant view of these issues.
Method
This is a qualitative study, based on indepth focus group interviews with two populations: (a) older immigrants from the FSU currently treated in primary care (not necessarily for mental illness); and (b) PCPs who are immigrants from the FSU. We expected the perspective of the PCPs to complement that of the older immigrants. The study was funded by a grant from the Israel National Institute for Health Policy Research. This paper reports specific findings from a larger study funded by this grant (see Ayalon, Karkabi, Bleichman, Fleischmann, & Goldfracht, 2015; Ayalon et al., 2016).
Participants
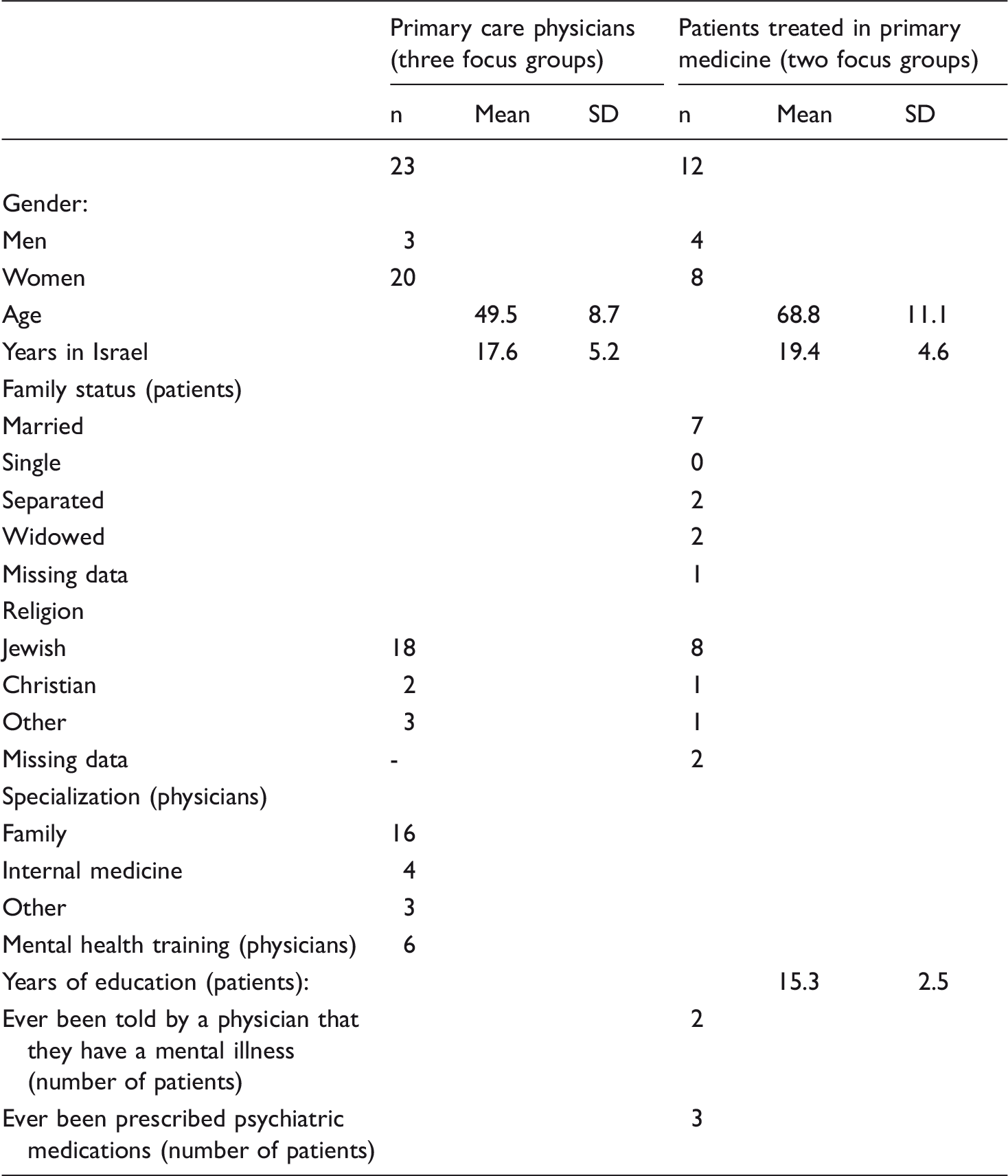
Participants were PCPs and older primary care patients; both PCPs and patients immigrated to Israel after 1990. Three groups were held with PCPs, in three Israeli towns. The first included 10 female PCPs, three of whom had mental health training. The second group included seven PCPs, five women and two men, two of whom had mental health training. The third group included six PCPs, five women and one man, one of whom had mental health training. The reference to mental health training means training that is more extensive than the basic training provided to all PCPs. It is important to note, however, that since July 2015, Israel has begun implementing a Mental Health Reform, in which mental health services are transferred to primary care (Nakash, Razon, & Levav, 2015). Therefore, mental health training has become compulsory for PCPs.
Characteristics of the research participants.
Procedure
The research was approved by the Helsinki committee of the Clalit Health Services. All participants signed an informed consent form prior to joining the research.
PCPs were approached directly by the researchers. Patients were recruited by flyers distributed in clinics and directly by PCPs and nurses.
A focus group is a group of six to 10 participants, guided by a skilled moderator (Morgan, 1998). This is an effective research method in cases where the participants are not sure about their feelings concerning certain issues, as it allows them to form an opinion while listening to others. The focus group elicits different opinions over a short period of time. In addition, the method is faster and more cost-effective than personal interviews, and may also develop into a group discussion in which many nuances of the issue are revealed (Morgan, 1998). The drawbacks of the method are that dominant participants may control the discussion, and a consensus may be reached, rather than eliciting diverse opinions and stands. The present study attempted to deal with these potential limitations in the following ways: the selected moderators were experienced in enriching the focus group discussions; the groups were small, to allow the voicing of multiple opinions (Morgan, 1998); and the groups were as homogenous as possible, to facilitate nuanced expression in a relaxed atmosphere.
Homogeneity within the group was reflected in several ways, including patients' age, general health condition (e.g., not having a severe disease or severe mental disease), geographical proximity to the clinic where the focus-group had taken place, and immigration year. Within the PCPs' group, the homogeneity was reflected by the fact that all PCPs had clinical experience with immigrants from the FSU and all were FSU immigrants themselves. Gender-homogeneity was not planned; in practice, in most of the groups the majority of the participants were women. Notably, focus groups are often used in studies of this kind, and have yielded important insights in previous studies (Bradley et al., 2002).
The PCPs' focus groups were conducted in Hebrew, and those held with the patients were conducted in Russian. This is because in order to work as a physician in Israel, the physician has to have a full command of Hebrew, as licensure exams are conducted in Hebrew. This was not the case for older adults from the FSU, many of whom continue to speak their mother tongue and have limited command of Hebrew. The moderators were post-graduate social science students, who spoke both Hebrew and Russian, were experienced in working with groups, and had been trained by the co-author (L. A.). The moderators began with broad questions and gradually narrowed down their scope. Each focus group session took one to two hours. All group sessions were recorded and transcribed verbatim; the Russian transcriptions of the group sessions were translated into Hebrew as accurately as possible, to preserve the meaning of the interview (Polkinghorne, 2005).
The focus groups were given a set of questions to prompt the discussion. In the two groups of primary care patients the initial questions were: “Tell us what depression and anxiety mean”, “How does one deal with depression and anxiety?”, and “What are the advantages and disadvantages of dealing with depression and anxiety formally and informally?” In addition, self-report questionnaires were used to gather demographic information, including country of birth, age, gender, education, socioeconomic status, physical and mental illnesses, and symptoms of anxiety (GAD-7) (Spitzer, Kroenke, Williams, & Löwe, 2006) and depression (PHQ-9) (Kroenke, Spitzer, & Williams, 2001). The groups of PCPs were given the following guiding questions: “Tell us what depression and anxiety mean”, “How are depression or anxiety generally dealt with in primary care?”, “What are the advantages and disadvantages of various health services that prescribe medication or provide other types of treatment?”, and “Tell us about difficult situations you have come across with patients who suffered from depression or anxiety”. Demographic information was also gathered for the PCPs, including country of birth, specialization, age, gender, place of study, number of years in Israel, and mental health training.
Data analysis
To establish the rigor of the present research, we relied on triangulation (Cresswell, 2003) by two researchers who analyzed the findings separately and independently, and cross-checked the analysis with other PCPs who work with immigrants from the FSU. Findings are illustrated with quotes from the interviews. This makes the process that yielded the findings transparent (Polkinghorne, 2005) and allows readers to judge the proposed interpretations (Cresswell, 2003).
Two of the researchers analyzed the focus groups separately. The other researchers, all with at least two decades of experience in primary care, actively participated in coding the data. The analysis was coded in stages (Strauss & Corbin, 1998): the transcribed text of each group interview was first coded thematically; then similarities and differences between the interviews were evaluated, and themes were grouped to create broader structures (Strauss & Corbin, 1998). During analysis, comparisons were repeated between individual participants, within the groups, between groups of different types of participants (patients or physicians), and between focus groups of the same type of participants. This was done to create thematic categories that would be more comprehensively relevant to the participants (Miles, Huberman, & Saldana, 2014). The different stages of the analysis were documented in real time and used as a means of inspection of the data (Rodgers & Cowles, 1993).
Findings
The present study addressed the way depression and anxiety are perceived by primary care older immigrants and by their PCPs, who are also immigrants from the FSU. Three main categories were identified: a) avoidance of discussion of mental health and stigma; b) expectations to self-control one's mental state; and c) limited opportunities to acquire new Western knowledge on mental health. In this section we use quotes from the focus group interviews to illustrate the perceptions of older immigrants about mental illness, and the factors that prevent them from acquiring new knowledge on this subject. Quotes taken from the PCPs' focus groups shed light on the matter from another angle.
“People don't speak about this often enough”: Perceptions of mental illness, avoidance, and stigma
At the beginning of the focus groups with older primary care immigrants, moderators asked the participants to explain what depression and anxiety meant. One common reply was that depression was an accumulation of external difficulties that caused high levels of mental stress. Among the difficulties mentioned were illness, financial difficulties, the security situation in Israel, and overwhelming responsibilities and concerns for family members. Depression was described as a bad mood, withdrawal from society, irritability, or apathetic behavior. Similarly, anxiety was described as internal turmoil and worries that spring from external difficulties.
The participants often had difficulties distinguishing between depression and anxiety, and used the two terms interchangeably. They also seemed to have difficulties distinguishing between depression and anxiety vs. other mental and physical conditions. For example, two of the participants (from separate groups) said: We had [at work] a worker… he began behaving improperly… shouting, cursing… it is a kind of depression. There was a child [at the school where I worked] who, I noticed, did not smile… You could not tell if he was depressed… He was always closed… The teacher later told me he had autism. Speaker 1: It is worthwhile to simply try and speak with relatives and not to hold it within, but this isn't always possible. Speaker 2: Not everyone understands… Speaker 1: [When I was depressed] I didn't want to [speak] at all. Not with my husband and not with my children. I was nervous… Speaker 3: I don't wish to involve my relatives with my problems, let alone depression. Some people feel better if they keep silent… I know people who sit silently, someone visits them and they are silent together. And this is normal… if you begin “pulling strings” you should know what for, and say what is right for you. One must search for [symptoms of mental illness] because if you don’t, they won't be found… Those who suffer from it will not speak about it, and one must look for it, there's a substantial under-diagnosis, especially among immigrant populations.
“I should manage on my own”: Expectation to be in control and handle the situation alone
A recurrent theme in the patients' focus groups was that of controlling depression and anxiety. In one group, there seemed to be a consensus that persons suffering from mental illness can and must gather strength and control their condition. For example, as two participants said: [When I became ill] I tried and made an effort not to fall into depression… I pulled myself out of this condition. [When I was in mental distress] I did not seek [help]. I should manage on my own… I knew it would pass, this is not a permanent condition. One must simply “change channels”, look at the bright side, and not withdraw into oneself. Over a period of time, if you don't succeed, you seek help… You have tried to communicate with your family, you have tried to get support, you have tried this and you have tried sports, and if, say, this didn't work… go and consult someone who can help, a doctor. Speaker 1: There are many undiagnosed cases, because people don't come to the doctors and don't tell. Speaker 2: Or come with somatization, with all sorts of somatic complaints… Speaker 1: But do not accept the diagnosis. I had always said that a Russian woman was not susceptible to depression after giving birth… There is no time for depression, no time to idle and do nothing. But after I had my second baby… I felt that no one loved me, no one loved the baby, no one wanted me and no one wanted the baby… and I didn't want anyone to help me. I can manage this on my own… [at some point] I understood I was unable to control it… to me, this kind of depressed condition brings a person, well, almost to the end, and without help one is unable to get out of it. When someone is really depressed, they no longer think: “whom should I approach”, or that they should tell their friends and family… they don't acknowledge this… they don't feel like talking at all! With no one.
“Secluded in their small apartments”: Limited opportunities to acquire new Western knowledge
The older immigrants from the FSU who participated in the focus groups did not bring up the issue of approaching mental health specialists until this topic was mentioned by the group moderator. When asked about psychotherapy, participants answered repeatedly that they could not afford this treatment, knew little about it, had no experience with it, and did not know how to locate and access this kind of service. Several participants in the all-women group said they would like a clinic that provides “psychological help” in their neighborhood. The participating PCPs explained that unlike PCPs who are accessible at the community clinics, mental health specialists usually work in distant clinics. The difficulty to access these clinics limited immigrants' opportunities to acquire knowledge about psychotherapy.
Social encounters can also present opportunities to acquire new knowledge about health services. However, both the patients' groups and the physicians' group described this as problematic for older immigrants from the FSU, in part because their social circle had dwindled as a result of their immigration, and also because their economic situation made them less available for socialization. One participant said: [All my friends] are extremely busy, and when you return home from work at nine o'clock, you have no energy left for anything else. In the past, seeing friends replaced a psychologist… [nowadays] when you get home you have this and that and more… You no longer want anything… you are exhausted physically. The immigrants from the FSU are intelligent people who came from a society where they used to go to concerts, lectures, or social events… here they are secluded, and don't have all of this. Sometimes they are unable to afford it financially, or have no transportation… they are secluded in their small apartments and this is very depressing… when a person has limitations – be it language, money or other matters, this certainly adds [to their depression] and sometimes this becomes the main reason for it.
The question arises whether the PCPs – who described themselves as familiar with mental health treatment (26% had designated training in this field), were available to the older immigrants, and aware of their difficulties and cultural issues – were able to assist their patients and broaden their knowledge regarding mental health. Several PCPs said they were willing to talk with patients and give them as much personal attention as possible. Other PCPs admitted that they were uncomfortable having long and complex conversations with their patients while many other patients were waiting outside. They also regarded the psychological tools they possessed as insufficient for assisting the patients. One PCP said: In many cases the family doctor does undertake to act as the patient's psychologist… We do try to use our authority to help the patient… a small tip, something… But soon enough, we must resort to medication with the patient's consent. We have no choice… there is no other solution.
Discussion
The present study examined beliefs and attitudes regarding depression and anxiety among older primary care patients and PCPs, who immigrated to Israel from the FSU. The findings show that older immigrants tend to avoid discussing this matter and expect to be able to control their mental state and cope with it on their own. Their exposure to new knowledge on the subject is very limited.
The findings indicate that the cultural background of the immigrants from the FSU plays a dominant role in their stands and beliefs on this matter. In the Soviet Union, the medical field that managed mental health was outdated, stigmatic and linked with political abuse. Consequently, the immigrants' previous acquaintance with this field was superficial and stigmatic (Auslander et al., 2005; Levav et al., 1990; Mirsky, 2009; Polyakova & Pacqulao, 2006). The findings of the present study reveal that difficulties distinguishing between various mental and physical conditions and avoidance of the subject of mental health prevail even decades after immigration (the participants' average number of years in Israel was almost 20). A study conducted in the US with older immigrants from the FSU reported similar findings (Polyakova & Pacqulao, 2006).
The normative cultural practices of subjective feelings, appraisal, and behaviors vary across cultural models and are usually functional within the particular culture (Mesquita & Walker, 2003). For instance, in the FSU, negative emotions are not always devalued. As a result, FSU immigrants might be less likely to refrain from negative feelings such as depression or low life-satisfaction, as these do not carry such a negative connotation in the FSU (Jurcik et al., 2013). In support of this claim, past research has shown that older FSU immigrants in the U.S. reported high trait levels of negative emotions: sadness, shame, fear, anger, and guilt (Consedine & Magai, 2002). Additional studies have shown that FSU immigrants in the US emphasized and focused on negative emotions in order to exemplify the emotions that were valued in their culture (Grossmann, Ellsworth, & Hong, 2012; Jurcik et al., 2013). In this context, Grossmann and Kross (2010) explained that for Russians, focusing on negative feelings is associated with a more positive value and may facilitate adaptive coping. Because coping mechanisms and resources to mediate stressors are culturally bound (Marsella & Yamada, 2010), FSU immigrants' cultural practices might be misinterpreted in the host culture.
In Israel, FSU immigrants report greater distress and psychiatric problems compared with other Israelis (Mirsky, 2009; Mirsky et al., 2008; Ritsner et al., 2000; Zilber et al., 2001) and their use of psychiatric medications is significantly higher (Ayalon et al., 2011). The rates of mental distress and psychiatric disorders in older FSU immigrants are higher than in younger ones (Mirsky, 2009; Zilber et al., 2001), and they tend to somaticize their distress (Ritsner et al., 2000). The findings of the present study show that certain circumstances related to immigration at an older age, such as economic difficulties, limited mobility (Litwin and Leshem, 2008; Remennick, 2003), and language barriers (Remennick, 2003, 2004), might result in social marginality. These immigrants have limited physical access to health services that are located at a considerable distance from their homes, and their linguistic ability to access various services and even take part in community events is no less limited. These factors hinder their socio-cultural integration and their exposure to new knowledge on the subject of mental health.
The findings also suggest that the PCPs, who are the main gatekeepers (Tabenkin and Gross, 2000), especially when it comes to immigrants from the FSU (Ritsner et al., 2000), are aware of the situation of older immigrants from the FSU in Israel. The PCPs are familiar with the typical difficulties experienced by these older immigrants, and are mostly accessible to these patients in terms of their presence in primary care clinics. However, in spite of their wish to assist patients who suffer from mental illness or distress, their workload is such that they usually have no other choice but to prescribe psychiatric medications, rather than provide empathic ongoing support and discussion (see also Ayalon et al., 2016).
These findings are highly noteworthy in terms of the older immigrants' views on depression and anxiety, given the role of the PCP in Soviet culture. In the Soviet Union, physicians belonged to one of the most respected professional groups, and enjoyed high authority and influence (Remennick & Shakhar, 2003). Comparing the Israeli medical system to the Soviet one, FSU immigrant PCPs stressed the Soviet PCPs' personal and holistic approach, and their empathy and devotion to patients (Remennick & Shtarkshall, 1997). In a similar manner, FSU older immigrants in Israel complained of impersonal attitudes of Israeli PCPs toward patients and a lack of holism in care, which they claimed to have enjoyed before immigration (Remennick & Ottenstien-Eisen, 1998). In Israel, the PCP has been the favorite formal provider to whom immigrants from the FSU could approach for help at times of mental distress (Ritsner et al., 2000). Therefore, seeing a PCP and receiving guidance on mental health in an empathic way, could have provided the immigrants from the FSU an opportunity to broaden their knowledge in this field. However, the findings of the present study suggested that an opportunity of this kind is rare.
Because of the limited exposure to new knowledge on the subject of mental health, the knowledge and cultural practices that originated in the Soviet Union are preserved. The research findings indicate that the patients who participated in the study had difficulties discussing mental health and expected to be in control of their mental state and cope with it on their own. The current findings match the findings of a study carried out with a similar population in the United States (Polyakova & Pacqulao, 2006). These findings reflect the Soviet norm of self control (Hollander, 1978). At the same time, the findings further support the reports of the PCPs concerning substantial underdiagnosis and undertreatment among this population. If so, the current research suggests a model that describes the circumstances that make current situation unchanged despite the fact that the older FSU immigrants immigrated to Israel more than two decades ago (see Figure 1 for illustration).
The suggested model.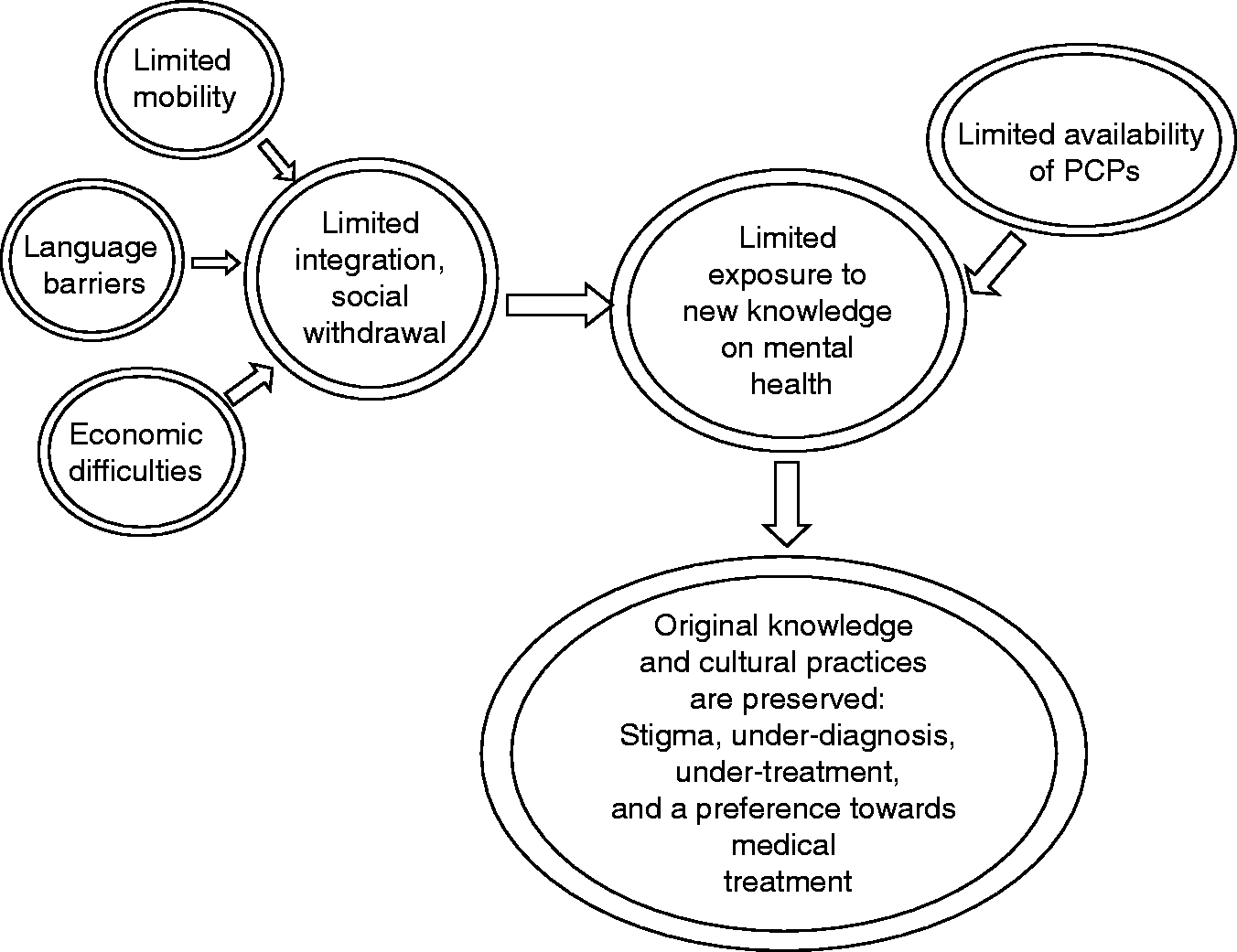
It is important to note that the research procedure used in this study (indepth focus group interviews), provides evidence for an ongoing process among older immigrants from the FSU. Whereas one group (a gender mixed group) was in consensus about the ability of individuals to control mental illness on their own, the second group (an all-women group) developed an interesting group dynamic that began with the personal story of one participant about the way she had coped with mental illness, and went on to include other personal stories. The personal stories that were told in the second group put in question the idea of self control. The intimacy that developed in the latter group appeared to have created the right atmosphere for openness and sharing, and made the participants question their cultural norms, be more receptive to new ideas, and even change their views. This process confirmed at least one advantage of the focus group technique (Morgan, 1998).
It is plausible to assume that the gender composition of the groups might have influenced the group processes, because women usually disclose more than men (Dindia & Allen, 1992). Therefore, due to the norm of reciprocity, in all-women groups high levels of self disclosure are expected. In all-men groups on the other hand, low levels of disclosure are expected, and in mixed gender groups the expected levels of disclosure are moderate (Fern, 2001). Another important factor of the gender-related group dynamic is the moderator's gender. In the present research, groups were moderated by a woman. According to Fern (2001), female moderators will elicit more self disclosure than male moderators if the moderator is perceived as the target, regardless of the group's gender makeup.
These findings led to the issue of a possible change in attitudes regarding mental health among older immigrants from the FSU. In a research study conducted in the early 1990s, FSU immigrants were characteristically more receptive to issues of mental health and mental assistance five years after their immigration (Lerner et al., 2005). Yet, according to the PCPs who participated in the present study, and as found in studies conducted with similar populations in the U.S. (Aroian, Khatutsky, Tran, & Balsam, 2001; Polyakova & Pacqulao, 2006), the older immigrant population has remained inflexible and was not open to change. Interestingly, the findings of the current research revealed that in the second group of patients, the focus group itself gave the participants an opportunity to broaden their knowledge in the field of mental health. This might indicate that there is a need among this population to acquire professional information, and to have an open discussion about it. It appears that in spite of their implanted Soviet norms and their socio-cultural seclusion, new ideas, such as Western mental health principles, do reach the older immigrants.
A study conducted in the U.S. with older immigrants from the FSU proposed that greater exposure to mental health services and the promotion of these services in primary care clinics would enhance older immigrants' use of these services (Polyakova and Pacqulao, 2006). This recommendation is also relevant to Israel, and has been implemented since July 2015, when the field of mental health was officially placed under the responsibility of the health insurance funds (Mizrachi, 2007; Nakash et al., 2015). But even after this change has begun, it is still necessary to investigate the accessibility of mental health services to older immigrants, as far as language, culture, and economic situations are concerned.
Limitations
Despite its strengths and significance, the study has several limitations. First, one of the basic assumptions of qualitative research is that the researchers constitute a part of the research process, and usually examine the data from their own cultural perspective (Creswell, 2003). Although the researchers in the present study belong to different subcultures within Israeli society, and two are immigrants from the FSU, the professional socialization of the researchers in Israel involves Western perspectives on the subject of mental health. Therefore, in a reflexive perspective, it is important to acknowledge a potential for cultural bias in this study. Second, the study is limited by the small sample of patients. Despite the efforts of the research team to reach this population, participation in the focus groups was limited. Perhaps, mobility difficulties of this population and sensitivity about the issue of mental health hindered recruitment. Another limitation of this study is the hypothetical discussion of beliefs and attitudes, which are not necessarily synonymous with actual behaviors.
Conclusion
The study explored attitudes and beliefs about depression and anxiety among older immigrants from the FSU to Israel. The integration of the perspectives of primary care patients and primary care providers allowed for indepth examination of the subjects of aging, migration, Soviet cultural background, and attitudes towards mental health issues, and provides a thorough understanding of the difficulties and needs experienced by older primary care immigrant patients. Results suggest the importance of providing older immigrants from the FSU with information on the subject of mental health in culture-sensitive and empathic circumstances. Engaging PCPs who work with the community might help with achieving this goal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the study was funded by the Israel National Institute for Health Policy Research.