
Abstract
This study investigates the pattern of use of traditional and alternative healers among psychiatric patients in Nelson Mandela Metropole. An interview schedule was applied to 254 subjects at six sites, enquiring about consultations with traditional and alternative healers in the past year. Multivariate analysis was performed to determine predictors of consultation. Overall, 78 (31%) of respondents had consulted a healer in the past year. The ethnic distribution was: 156 (61%) Black, 53 (21%) Coloured (Mixed Race), 42 (17%) White and three (1%) Indian. The male to female ratio was 119 (46.85%):135 (53.14%). The healers gave no advice about psychiatric medication to 48 (61.5%) of consulters, 23 (29.5%) were told to continue their medication, four (5.1%) told to stop, and one (1.3%) told to stop and restart later. In multivariate models, predictors of consultation were being Black and of lower education. Although 45 (58%) of the consulters indicated that medical treatment was more helpful than the healer’s, 45 (58%) intended to consult again. Overall, 22% of consulters reported abuse by the healer.
Keywords
Introduction
South African studies show that 70% to 84% of patients with different ailments consult traditional healers (THs) at some time (Koen, Niehaus, Muller, & Laurent, 2003; National Progressive Primary Health Care Network Summary Brief, 1997; Robertson, 2006). The South African Stress and Health study (SASH) reported that only 5.7% of persons with a mental disorder had received any conventional mental health care in the preceding 12 months (Stein, Williams & Kessler, 2009). In comparison, 5.8% of the general population had accessed a TH or alternative/complementary medicine practitioner, and a further 6.6% had used services from social or religion-based practitioners during the preceding 12 months. Patients who consult traditional, religion-aligned and complementary or alternative healers (TAH) in South Africa are frequently prescribed a variety of interventions that may contain herbal, animal, homeopathic, and allopathic ingredients (World Health Organization Traditional Medicine Strategy, 2005, p. 1). Mental health practitioners (MHPs) often do not know the ingredients of these prescriptions. They also have little knowledge of their potential pharmacological actions, side effects or interactions, because many potions are untested, and their use is not monitored (World Health Organization Traditional Medicine Strategy, 2005, p. 1). Thus, it is important for MHPs to know more about how people use TAHs and their interventions.
Some studies have found that TAH in other African countries recognize symptoms of severe mental illness but strongly believe the cause is supernatural (Abbo, 2011). This in turn influences their interventions. Another study conducted in Uganda found that over 80% of the participants who had accessed a TAH for symptoms of psychosis had also used biomedical services for the same symptoms during the study period (Abbo, 2012). The potential role of TAHs in mental health care has been debated in the literature on global mental health, with little consensus on the way forward. Patel (2011) identifies the mutual suspicion between the two health care systems and concerns about the ‘unscientific’ and unorthodox practices of TAHs as obstacles to such collaboration.
Use of traditional medicine in the South African setting
South African clinicians frequently deal with patients from different cultural backgrounds. Patients who use traditional or alternative remedies do not always inform their treating clinician. The widespread use of TAHs by patients in South Africa thus requires clinicians to become knowledgeable about this subject in order to better serve the patients they treat. If a health practitioner is uninformed about the use of traditional or alternative medicines, this may impede medical treatment or even negatively affect allopathic interventions. For example, Callilepis laureola, a South African traditional herbal medicine (known as “impila” in Zulu), is cytotoxic (Popat et al., 2001) and may result in hepatic necrosis (Wainwright & Schonland, 1977).
In a study of Xhosa-speaking patients with schizophrenia, 84% of the patients reported having used TAH treatment because of their symptoms (Babb et al., 2007). This number is similar to the percentage of HIV-infected individuals in another South African study, where 84% reported using a TAH (Koen et al, 2003). Participants in the Babb et al. study (2007) spent between £4 and £27 per month on traditional medicines in 2007 (i.e., R56 to R380 based on the Rand/GBP exchange rate in 2007). At Hlabisa Hospital in KwaZulu Natal, 80% of patients admitted with a snake bite had used traditional medicine prior to admission and 62.5% had consulted a TH prior to admission (Sloan, Dedicoat & Lalloo, 2007). The median time of consulting the healer after the injury was 15 minutes, compared to seven hours 15 minutes until admission to hospital. These studies, which focused on mainly THs, highlight that across South Africa a significant number of patients who consult health practitioners also chose to consult THs outside of the medical field. In addition, the study at Hlabisa Hospital raises concerns about accessibility to medical or health care, i.e., if one compares the number of TAHs to the number of medical doctors in South Africa, is the time difference between accessing care from a healer and care from the hospital a question of accessibility and preference rather than patient preference alone?
Nxumalo, Alaba, Harris, Chersich and Goudge (2011) reported that the use of THs appeared to decline with an increase in wealth. In their sample of 4762 respondents, the most frequently cited reasons for using THs were: a) the perception that treatment was effective (52.6% of respondents); b) THs offered continuity of care (for 37.2%); and, to a lesser extent, c) THs offered respectful treatment, proximity, and availability of medicines.
The healer in the South African context
In countries with limited access to allopathic medicine, traditional medicine is often the main source of health care (World Health Organization, 2012). The discrepancy between the biomedical conceptualization of disease and the patient’s perception and experience of illness may be further magnified by cultural differences between the patient and the health practitioner (Putsch & Joyce, 1990). In the case of TAHs, they may be able to bridge this gap because they often share the same background as their patients and may therefore have a clearer understanding of patients’ views of their symptoms and the attributed cultural meaning (Mufamadi, 2001). According to Ndetei (2007) some of the postulated reasons why patients consult TAHs may be related to shared beliefs between the healer and the patients: “the healer understands the significance of ancestral spirits, he shares the belief in supernatural forces and he identifies with the reality of witches.” Robertson (2006) also argued that “many consider TAHs to provide more holistic care than medical practitioners, to be more accessible, and have an approach that is more appropriate and therefore more acceptable to the community.” Likewise, Mufamadi (2001) states that the TAHs’ view of the disease is usually more in line with the patient’s beliefs than the Western medical conception of disease is.
Pinkoane, Greeff and Williams (2005) looked at the patient relationship and therapeutic techniques of South Sotho TAHs. They concluded that the process of interaction between the TAH and the patient is built on a relationship consisting of various phases and based on mutual respect and understanding of each other’s cultural views and beliefs. De Villiers and Ledwaba (2003), in their paper on TAHs and paediatric care, state that TAHs have good communication skills, are readily available in all areas, and manage the patient, the family, and social problems. This implies that they are holistic in their approach. This supports the argument that TAHs’ interventions may be tailored to suit the patient’s and family’s needs and their understanding of the health problem, and that proposed solutions may be more acceptable to the patient and family. There is thus a need for MHPs to recognise that the acceptability of interventions suggested to patients may have important implications for treatment adherence. MHPs need to have a good understanding of their patients’ view of their problems and symptoms, despite not being of the same culture.
Legislation governing traditional healing in South Africa
In 1995 South Africa had around 200,000 practising TAHs, compared to 25,000 doctors (Kale, 1995). In 2007, there was an estimated 190,000 TAHs as reflected in the Traditional Health Practitioners (THP) Act No. 22 of 2007 (Republic of South Africa, 2008). This Act is far removed from the Witchcraft Suppression Act of 1957 and the Witchcraft Suppression Amendment Act of 1970, which outlawed the practice of traditional healing during that period. There was no formal regulation of traditional healing practices in South Africa until the advent of the THP Act. It aims to regulate the practice of TAHs through the Traditional Health Practitioners Council of South Africa (THPC). It provides the regulatory framework intended to ensure efficacy, safety, and quality of traditional health services through the management and control of registration, training, and conduct of TAHs. This required traditional practitioners such as diviners (amagqirha or izangoma), herbalists (amaxhwele or izinyanga), traditional surgeons (iingcibi), and traditional birth attendants to register with the THPC by May 1, 2015. The THPC consists of TAHs from the nine different provinces, a representative from the Department of Health, a medical doctor, and a pharmacist. The council was established to promote public health awareness, protect and serve the interests of members of the public who use or are affected by the services of traditional health practitioners, and to ensure that traditional health practice complies with universally accepted health care norms and values. There have been teething problems with the implementation of the regulation because it is often difficult for the TAH to access to the information required to register.
Another legal development relates to sick notes issued by TAHs in South Africa to excuse workers or students who needed an absence when they were ill. Sick notes issued by TAHs were not recognized as legitimate in the past. A court challenge was mounted, culminating in the Supreme Court of Appeal (Bloemfontein) making the ruling in November 2013 that a sick note from a TH must be seen in the same light as one issued by a qualified medical doctor, in the Basic Conditions of Employment Act (De Wet, 2013). Furthermore, in a submission to the parliamentary monitoring group made in August 2013 on behalf of the Eastern Cape Provincial Legislature on the Mental Health Care Amendment Bill, it was proposed that TAHs “must be given room to assist with the treatment of mental illness where scientific Western medical interventions fail” (Eastern Cape Provincial Legislature, 2013). This submission further suggested that room be given for “traditional exorcisms where psychiatric doctors fail”; subject to the rights enshrined in the Constitution to refuse any form of interventions should a patient wish to do so. One might question why this submission should be applied to mental illness alone instead of the rest of the medical field if it is meant to represent a genuine attempt to accommodate TAHs within the medical field. It does nevertheless raise a question about the role of TAHs in the South African medical field and where they fit into health services.
Interactions between healers and health practitioners in South Africa
Mbatha, Street, Ngcobo and Gqaleni (2012) argued that the World Health Organization (WHO) Traditional Medicine Strategy for 2002–2005 provided a framework to promote traditional medicine and its integration into national healthcare policies to reduce mortality and morbidity, especially in the least-developed countries. While South Africa’s TAHs are not integrated into national healthcare strategies as yet, there have been partnerships formed in different health disciplines in an effort to improve patient care. MHPs in South Africa thus operate in a changeable environment, increasing pressure on them to acknowledge the patient’s rights to choose TAHs as part of their treatment options. Clinicians therefore need to equip themselves with the knowledge and means to take informed decisions about these aspects in their everyday practice.
The limited research and information available in this field in South Africa makes it difficult for MHPs to negotiate their way when faced with a patient’s expressed needs, if such needs are in conflict with the MHP’s belief system. An example is when a still symptomatic inpatient requests to be granted “leave” from the hospital to go and consult with a healer while still under the MHP’s care. How are these decisions addressed if the MHP does not have information on the TAH’s interventions and how these interventions might affect the patient’s health?
A study conducted by pharmacy students in Port Elizabeth, Nelson Mandela Bay, investigated awareness of diabetes mellitus among African THs (Van Huyssteen et al, 2009). They used a method of three interactive workshops attended by the researchers and healers. Although each individual workshop was well attended, one of the problems the researchers had was lack of sustainability of attendance, with only three of the total 51 healers attending all three workshops. Reasons identified as possible contributors to this were that some of the healers were out of town for some of the workshops, some healers only became aware of the workshops after the first one had taken place, and the communication system between the researchers and the healers, and amongst the healers themselves, was inadequate. As a result, researchers were unable to reach the healers at crucial times. In spite of these limitations, the researchers were able to hold a feedback workshop during which the healers indicated that they were using the information gained during the previous workshops. They had also begun imparting the knowledge learned to other THs and to their apprentices. If this effect of health education can be replicated in the field of mental health, it may be possible for MHPs and THs to engage collaboratively as promoters of psychoeducation among a shared patient population.
Collaboration between TAHs and the medical and allied health professions has brought about positive change in fields such as tuberculosis (TB) and HIV treatment. Peltzer, Mngqundaniso and Petros (2006) investigated HIV/AIDS/sexually transmitted infections (STIs) and TB knowledge, beliefs, and practices of 233 THs in KwaZulu-Natal. In their sample, 29% of the healers had treated TB and 20% had treated AIDS. They found that 93% of the healers approved of distributing condoms to clients, 82% had conducted HIV/STI risk reduction counselling in the past three months and 56% indicated they had referred a patient for HIV testing in the past three months. Although THs in the study had adequate knowledge about HIV symptoms and major HIV transmission routes, their knowledge was poorer when it came to other HIV transmission routes. The researchers suggested training for THs, their clients and medical practitioners in various aspects of HIV prevention and care. The healers in the study were able to demonstrate knowledge about different aspects of HIV despite having no formal medical education. An approach similar to that recommended by Peltzer et al. (2006) could be applied to mental health services, starting with researching the practices of THs while simultaneously sharing psychoeducation information and encouraging them to instil adherence to psychiatric medication.
Another study that examined the acceptability and effectiveness of THs as supervisors of TB treatment in Hlabisa, KwaZulu-Natal, showed that 89% of patients supervised by healers completed their TB treatment, in comparison to 67% of those supervised by health clinic personnel, community health workers or lay people (Colvin, Gumede, Grimwade & Wilkinson, 2002). The mortality rate among those supervised by THs was 6% in comparison to 18% in the other group. This suggests that not only can THs provide an additional means of reaching patients, but that they may assist in improving treatment adherence and possible outcomes in chronic medical conditions. This may be another useful model to follow for possible collaboration between healers and MHPs.
Sixty-five Black patients admitted to a psychiatric ward in the Witwatersrand area were asked about their preferred health practitioner if given a choice (Farrand, 1984). Twenty-one patients (32.3%) said they would prefer to see a medical doctor (MD) only, 10 (15.4%) a faith healer (FH) only, eight (12.3%) a TH only, five (7.7%) an MD and TH combination, and five (7.7%) a combination of an MD and FH. Significantly, 16 (24.6%) expressed a preference to consult all three (i.e., MD, FH, and TH). This means that, in total, up to 40% of patients who would prefer to consult a medical practitioner also expressed a wish to consult with another healer at the same time. Kahn and Kelly (2001) explored how South African psychiatric nurses manage apparent incompatibilities between their practice of Western psychiatry and the use of traditional healing services. Such systems often coexist pluralistically in their experience. However, when questioned about possible cooperation between these systems, respondents gave views inconsistent with their pluralistic world view and promoted psychiatry’s supremacy. The nurses acknowledged the need for traditional healing systems in South Africa, but were of the view that psychiatry was superior to traditional healing.
Little is known by MHPs regarding the nature of TH interventions for psychiatric illness. Collaboration between the Medical Research Council, the Traditional Medicines Research Group of the Universities of Cape Town and Western Cape, and THs, culminated in a South African Traditional Healers’ Primary Health Care Handbook first published in 1997 (Felhaber & Mayeng, 1997). This handbook covers a range of topics, including first aid, nutrition, hygiene, traditional concepts of disease, and diagnosis, as well as biomedical concepts of disease and diagnosis. It also looks at different systems and illnesses ranging from the respiratory system, cardiovascular system, gastrointestinal system, urogenital system, skin and appendages, endocrine, musculoskeletal, and ophthalmological and miscellaneous infections. It discusses alcoholism, cancer, family planning, and issues like pain management. It however lacks information on mental illness and the diagnosis and treatment thereof. Though there is a chapter on the central nervous system, this is focussed on neurological rather than psychiatric illnesses. This highlights the gap that exists in the availability of information about TH interventions for mental illness in South Africa.
Use of traditional medicine in other African Countries
Kyeyune, Nakyanzi, Nkangabwa, Kabatesi and Tusaba (2000) demonstrated improved patient care with a referral system between THs and biomedical workers in rural Uganda, where 98% of healers reported referring patients to biomedical workers one year after being trained in STIs and HIV, compared to 7% prior to the training. In a Zambian study, THs received educational sessions on HIV, malaria, TB, child health, and nutrition (Nyumbu, 2003). The healers then informed their communities about these issues and identified cases that needed referral to health clinics. This cooperation between conventional medical practitioners and THs culminated in a national training manual for THs in 2001. Another survey of 29 THs in Uganda showed that almost all the healers recognized that they were treating people with mental illness. They identified mental illness as the most common problem they encountered in practice. Investigators concluded that there were grounds for cooperation between THs and medical services, which could also help harness primary care resources more effectively (Ovuga, Boardman, & Oluka, 1999). In a cross-sectional survey of 387 adult respondents who attended TH shrines in Uganda, the prevalence of psychological distress was found to be 65.1%, while 60.2% had a diagnosable current mental illness, and 16.3% had had one disorder in their lifetime (Abbo, 2011). Of the 387 respondents, over 80% of those with psychosis used both biomedical and traditional healing systems. Those respondents who had accessed both systems of care seemingly showed better outcomes.
A Sudanese study profiled patients who sought help from THs. Sixty-one percent were aged 21 to 40 years, 62% were women, and they were generally less educated than the general population (Ahmed, Bremer, Magzoub, & Nouri, 1999). A Tanzanian study found that the prevalence of common mental disorders in patients attending THs to be double that of patients attending primary health care clinics, i.e., 48% vs. 24% (Ngoma, Prince, & Mann, 2003). Another study of psychiatric patients in Pakistan found that 73% of patients with somatoform disorders, 73% with personality disorders, 70% with schizophrenia, 68% with mood disorders, and 55% with anxiety disorders had sought traditional treatments for their mental disorders (Farooqi, 2006). These studies have been able to demonstrate some positive effects from engaging with or utilising THs in different fields of health. In an Ethiopian study, Birhan, Giday and Teklehaymanot (2011) surveyed 306 patients who visited TH clinics. The reasons given for visiting TH clinics in their sample were efficacy for 57.2% of the respondents, dissatisfaction with modern medicine for 35.6%, a combination of both reasons (i.e., dissatisfaction with modern medicine and efficacy) in 3.3%, cost for 2%, and a combination of both dissatisfaction and cost for another 2%. This implies that a number of factors influenced the respondents’ decision to consult a TH in the Ethiopian study. All these studies concur with those in South Africa: that TH use is part of the reality of help-seeking behaviour for most populations across Africa, including those who suffer from mental illness.
Based on the evidence presented, some patients in South Africa and across other parts of Africa rely not only on allopathic health interventions for their health needs, but also on traditional or alternative healing methods. This is irrespective of whether such methods are backed by scientific research or not. In Africa and Southern Africa this pattern of help-seeking behaviour seems to be repeated in an even more pronounced manner, especially for those with mental illness. This places responsibility on health care providers to familiarise themselves with both systems of health care. Researching use of traditional or alternative methods of healing and the healers who provide them could thus assist both the patient and healer, whether allopathic or traditional, in bridging the knowledge gap in this field.
Objectives
The overall aim of this study was to examine use of traditional and alternative healers in people with mental disorders in the Nelson Mandela Bay Metropolitan Municipality (the Metro: comprising Port Elizabeth, Uitenhage, and Despatch) to obtain descriptive information that could contribute to a better understanding of such use. The specific objectives were to: a) investigate the prevalence of use of TAH services by patients with mental illness in the defined cohort; and b) identify predictors of consultation with TAHs in this cohort.
Methods
Study design
This is a cross-sectional quantitative and descriptive study utilizing an interview schedule designed by the researchers to collect information on consultation with TAHs in the 12 months preceding the study.
Setting
Subjects were drawn from six sites providing inpatient and outpatient mental health services in the Metro, the largest municipality in the Eastern Cape with a total population of 1.152 million in 2011 (Statistics South Africa, 2009). Study sites were two acute psychiatric hospitals (one private and one state hospital) and four community psychiatry settings (two private practices and two state clinics).
Ethical clearance
Approval and ethical clearance were obtained from the Fort England Research and Ethics Committee, which is aligned to the Walter Sisulu University Research and Ethics Committee. Subjects were informed of their right to withdraw from the study whenever they wished.
Subjects
Consenting subjects aged 18 years and older were recruited at the six identified sites, over a three-month period from the beginning of May 2010 to the end of July 2010. All those over 18 years of age who accessed the treatment sites during the enrolment period were requested to consider taking part. A total of 258 patients of different cultural backgrounds and ethnicity gave consent to be included in the study. Respondents at the private practice sites were mostly well educated, employed, had medical insurance, and were admitted voluntarily. Those in state-run facilities were often from deprived circumstances, unemployed, in receipt of a disability grant or pension, and were admitted involuntarily under the Mental Health Care Act no. 17 of 2002 of the Republic of South Africa.
Measures
Information on sociodemographic characteristics and use of services, including TAHs, was obtained with a structured questionnaire designed for this study (Appendix A, see online supplemental material). Demographic information includes age, sex, level of education, household income, and employment status. Other questions are about use of TAH in the last 12 months: types of healers (“African culture-aligned”, “Complementary/Alternative”, “Religion-Aligned”, and “Other”); reasons for choosing that particular healer (cultural belief, religious belief, family/friends’ recommendation, personal preferences, response to advertisement); types of treatment administered; adherence to healers’ prescribed treatment; level of satisfaction with treatment; mistreatment, assault or abuse by the healer; and likelihood to consult a TAH for mental health in the future. A list of healers classified into three categories, was provided on the back of the questionnaire for the research assistants to refer to. The categories were THs aligned to African culture, complementary and alternative practitioners (CAMPs) and religion-aligned healers (RAHs). The list and categorization were based on the researchers’ experience with previous patients and reports about the types of healers available in the region.
Procedure
Subjects were provided with information leaflets and verbal information about the study in one of three languages: Afrikaans, English, or isiXhosa. The researchers and research assistants held a consensus meeting on administration of the pre-designed interview schedule and how the subjects’ responses would be documented. The interview schedule was administered to all consenting participants by the researchers and research assistants at the different sites. Research assistants were volunteers drawn from the health practitioners who provide routine care for all patients that access the six sites for mental health services.
Data analysis
In addition to descriptive statistics, logistic regression analyses performed were of factors related to the overall likelihood of consulting a TAH, and the likelihood of the healer consulted being a TH.
Results
Of the 258 subjects, one withdrew consent and three (1%) were deemed to lack capacity to consent, for a final sample of 254. No adverse effects were reported.
Comparison of demographic characteristics of consulters vs. non-consulters

Prevalence and other characteristics associated with consultation
In all, 78 (31%) of the 254 respondents had consulted a TAH in the previous 12 months and 176 (69%) had not (see Table 1). Of those who consulted, 59 (75%) were Black, nine were White (11.5%), and nine were Mixed Race (11.5%); 47 (60%) had some form of income, either from formal employment (31) or a disability grant (16); 27 (35%) were unemployed; 54 (69%) had a household income of more than R2000 per month, equivalent to C$274 at the 2010 exchange rate. The category of healer consulted was a TH in 38 (49%) of the 78 who consulted, a RAH in 27 (35%) of respondents, and an alternative healer in three (4%) respondents, with some respondents (20 (26%)) consulting more than one category of healer. The reasons for consulting a TAH ranged from cultural belief in 32 (41%) respondents, religious in 16 (21%), and family or friend’s influence in 22 (28%), whilst only six (8%) reported the reason of personal choice.
In 57 (73%) of the 78 cases, treatment was oral or via enema and in three (4%) it was through inhaled steam. Only two (3%) received externally applied interventions (including through skin scarification). Another route was administration through a ritual in 16 (21%) cases. Combining the oral, enema, and inhaled administration shows that 60 (77%) cases had treatment administered internally.
Seventeen (22%) of the patients who consulted TAHs reported having been abused or exploited emotionally, physically, or sexually by a traditional or religious healer, but not by a complementary or alternative medicine practitioner. Despite this, absolute compliance or near-compliance with the healer’s intervention was reported by 56 (72%) and six (8%) respondents respectively, including those who claimed abuse. Near-compliance was defined as respondents who used the healer’s interventions or treatments, but with some modifications. The total reported compliance rate was thus 80%. Furthermore, 45 (58%) of respondents said that they would definitely consult a healer again and another 12 (15%) indicated they might in future, while 19 (24%) indicated they would not consult again. Concerning the patients’ medical or psychiatric treatment, healers gave no advice in 48 (62%) of cases, 23 (30%) were told to continue treatment as usual, four (5%) were advised to stop their medication permanently, and one patient was instructed to discontinue and restart later. Two respondents could not remember the advice given.
Up to 56% (44) of those who consulted spent R500 or less on consultation or treatment over a period of 12 months. DSM–IV (Diagnostic and Statistical Manual of Mental Disorders – Fourth Edition) diagnoses of the respondents as assessed by the treating clinician (obtained from clinical notes) ranged from schizophrenia in 29 (37%) respondents who consulted, to major depressive disorder in 16 (21%), substance induced disorders in 10 (13%), bipolar disorder in nine (12%) and adjustment disorder in seven (9%) cases. The rest were dementia, anxiety disorders, and disorders due to a general medical condition.
Perceived effect of healer’s treatment by respondents
Of those who consulted, 45 (58%) reported feeling better after the healer’s treatment, compared to seven (9%) who reported feeling worse and 18 (23%) who reported no effect. When asked which was the most beneficial treatment, 45 (58%) of the respondents who consulted indicated the medical treatment as the most beneficial while 20 (26%) thought both the medical and healer’s treatments were equally helpful. Only five (6%) thought the healer’s treatment was more beneficial than medical intervention, while four (5%) thought that neither helped. With regards to possible consulting with TAHs in future, 45 (58%) of those who consulted indicated they would most definitely consult a healer again compared to 32 (18%) of those who did not consult. The percentage of healers who advised patients to stop (5%) or interrupt (1%) their regular psychiatric medication was less than anticipated.
Interpretation of results
Logistic regression model of likelihood that a TAH was consulted
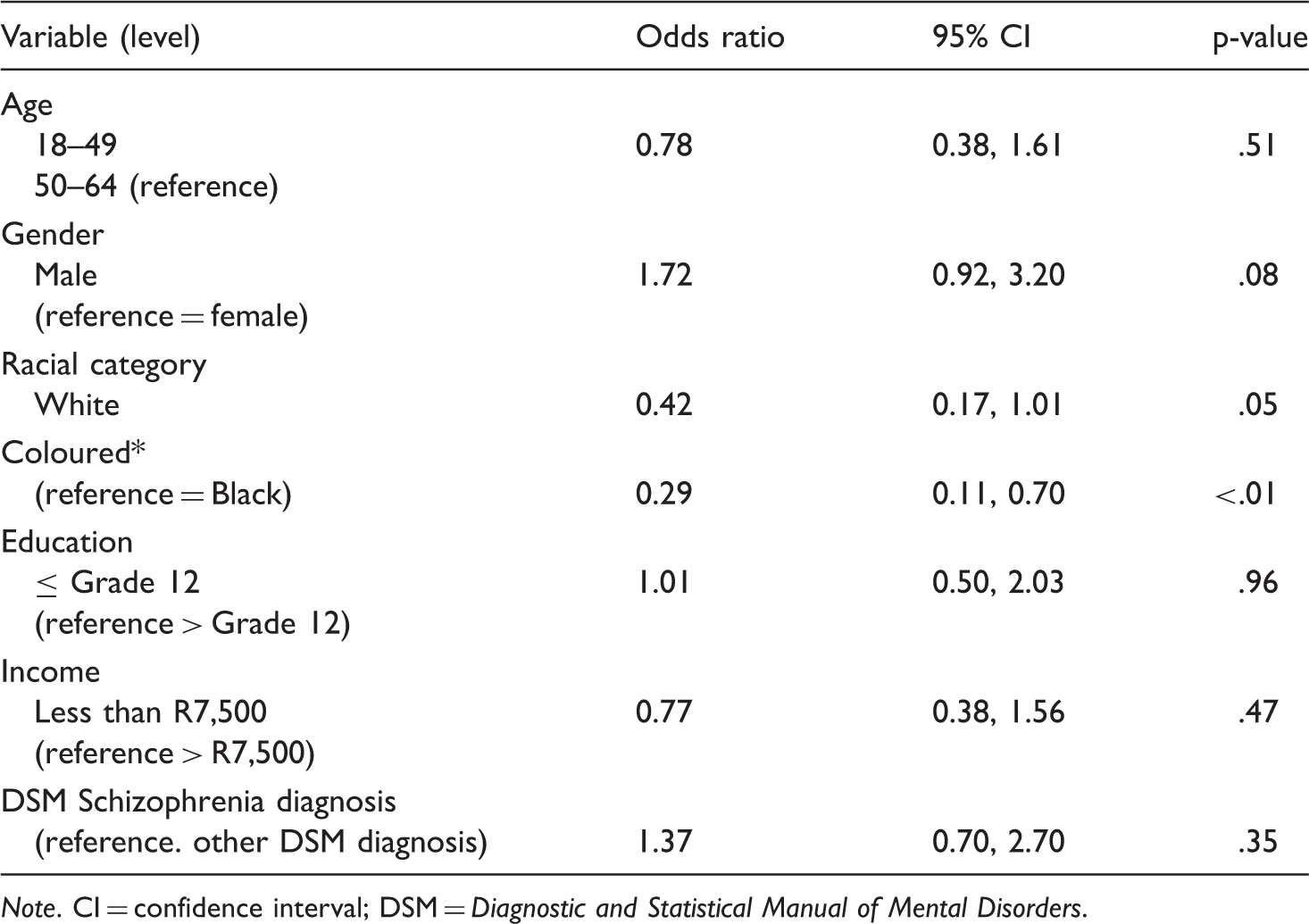
Note. CI = confidence interval; DSM = Diagnostic and Statistical Manual of Mental Disorders.
Logistic regression model of likelihood that the TAH consulted was a traditional healer

With regard to educational level, those who had an education of Grade 12 or less were more likely to consult a TAH compared to respondents with an educational level beyond Grade 12. Diagnoses, age and income did not show any significant effect on consultation with a TAH. Although men had a higher consultation rate compared to women, this did not reach a statistical significance.
Discussion
Annual prevalence rates of consultation with healers in South Africa in previous reports have ranged from 5.7% to 38.5% depending on the ethnic group, the type of healer consulted, and the nature of the ailment (Ensink & Robertson, 1999; Gqaleni et al., 2007; Koen et al., 2003; Liverpool et al., 2004; National Progressive Primary Health Care Network, 1997; Peltzer, 2009; Robertson, 2006; Sorsdahl et al., 2009; Stein et al., 2009). The 12-month prevalence rate of 31% in the current study, although in the upper range, is nevertheless still comparable to other South African studies. Ailments in the previous studies were a variety of illnesses, including mental illness. In the Farrand et al. (1984) study, 28% of South African patients with a variety of illnesses had consulted a TAH over a 12-month period. In the 1999 study by Ensink and colleagues, the prevalence rate for consulting for mental illness ranged from 13% for diviners and 24% for herbalists to 34% for faith healers.
The prevalence rate in the current study (31%) shows that persons with mental illness in the Metro area have similar rates of accessing healer services compared to other parts of South Africa. This makes it essential for MHPs in this setting to familiarise themselves with traditional healing practices and how these may affect delivery of, and access to, mental health services. Patients with certain conditions like snake bites, mental illness and HIV infection (prior to antiretroviral treatments) tended to have a higher prevalence of consulting healers in other South African studies (Gqaleni et al., 2007).
In the present study, being Black and having a Grade 12 or lower level of education correlated with a significantly higher likelihood of consulting TAHs. Of these two factors, the one flexible to adaptation is level of education, which begs the question: Will improving the level of education in the South African population decrease the likelihood of consulting a healer? Most patients who consulted healers were unemployed, but there was no significant statistical difference between the number who held employment among those who consulted and those who did not.
The majority of people who consulted healers indicated that the healer’s intervention made them feel better (45/78 = 57.7%). This however was not reflected in the respondents’ reports about which intervention was more helpful. Paradoxically, a similar number of respondents (45/78 = 57.7%) reported that they found the medical treatment more helpful compared to the healer’s treatment and only five reported the healer’s treatment to have been more helpful. This seems to imply that the majority of respondents who consulted the healer felt better after consulting, but were still aware that medical treatment helped them more. The question this raised is: If respondents thought medical treatment was more helpful, what benefit did they perceive from the healer’s consultation that made them feel better? Also, why did a large number of those who consulted (45/78 = 57.7%) still indicate that they would definitely consult a healer again if medical treatment was perceived to be more helpful than the healer’s by a similarly large number? The answer could be that respondents perceive gain from the healer’s consultation/intervention that they may not necessarily find in standard medical interventions; this seems to be irrespective of whether the medical intervention is deemed more helpful than the healer’s intervention.
These findings pose questions regarding patient perceptions about healers and medical intervention and how these perceptions possibly influence help-seeking behaviour. Despite available scientific evidence for helpfulness of biomedical interventions for mental illness, also supported by the reported patient perceptions in this study, this does not seem to lead to abandonment of healers by those who consult them. The question is why? The answer to this question might yield clues as to the health needs of patients with mental illness and whether these may be addressed within one unified system instead of the current dual and divorced system. The greatest influence on choosing to consult a healer in this study was cultural or religious belief, followed by influence from family or friends. These two factors account for close to 70% of the reasons quoted for consulting a healer.
Non-adherence to medical treatment for those with mental illness is a common problem that often leads to relapse and increases the cost of care (Knapp, King, Pugner, & Lapuerta, 2004; Olfson, Marcus, Wilk, & West, 2006). The reported 80% compliance rate with healers’ interventions in this study is very similar to the 84% reported in other studies among those who have used healers. This may imply that such healers are somehow able to overcome challenges faced by MHPs when it comes to treatment adherence (Koen et al., 2003; Robertson, 2006). Contributors to nonadherence have been identified as a combination of patient-related factors like forgetting to take medication, inadequate understanding of dose and schedule, lack of engagement in treatment decisions, impaired cognition, substance abuse, and mental health conditions, as well as other factors related to the health providers or the medication itself (Neiman, et al., 2017). It is unclear what factors contribute to the reported good adherence to TAH interventions.
Limitations
Adherence to healers’ interventions relied on self reporting and not objective measurements. Reports of feeling better and helpfulness of the interventions were based on subjective reports rather than objective measurement of signs and symptoms. The smaller number of Coloured (Mixed Race), White and especially Indian subjects limits generalisability to other ethnic groups within the Metro. While a minimal number of Indian respondents could be recruited for the current study, another South African study of 200 subjects from an Indian community in Chatsworth, Durban, showed that 38% of patients with a variety of ailments (diabetes mellitus, headaches, arthritis, joint pain, stress, skin disorders, backache, hypertension, and nasal disorders) used services of alternative/complementary healers (Singh, Raidoo & Harries, 2004). Consultation rates for this ethnic group were thus similar to the rates in the current study.
There was also possible underreporting of psychiatric disorders due to general medical conditions (GMC - now classified under another medical condition in DSM5), in particular HIV, in our study. Only one patient was indicated as suffering from a psychiatric disorder due to a GMC (HIV). This is different from other South African studies of HIV infection in psychiatric patients which demonstrated HIV seroprevalence figures of 9.5% (Van Wyk, Von Brandis-Martini, Pretorius and Webber, 2004) and 29.1% (Singh, Berkman, & Bresnahan, 1997). Reasons for this difference are unclear. Possible contributory factors could be related to issues of capacity to consent, with concerns around stigma and confidentiality possibly limiting testing or disclosure of respondents’ HIV status to investigators.
The interview schedule, although generally well received by participants, was lengthy, which some respondents might have found challenging. It also included some questions that the respondents may not have felt comfortable divulging. These include the history of consultation with a healer, personal or household income, and abuse by the healer. The fact that it was structured might have limited its flexibility and the researchers addressed this partly by including a section where respondents could provide a unique response to most questions if they felt this necessary (marked “other” and “describe” in the interview schedule). It also relied on the respondent’s ability to recall events that might have occurred over a period of months to a year.
Conclusion
The 31% prevalence rate of consultation of healers by psychiatric patients in this study cohort is comparable to similar South African studies (5.7% to 38.5%) for people with mental illness and other ailments. Some predictors for consulting healers included being Black and having a lower level of education. The reported high compliance with healers’ interventions (80%) and the small percentage (5%) of healers who advised patients to stop or interrupt their regular medication may indicate potential for collaboration between healers and MHPs in encouraging medication adherence. Factors contributing to this high adherence may include patient specific factors (e.g., cultural or personal beliefs), healer specific factors, the healer intervention methods, and/or the character and quality of the relationship between patient and healer. The authors postulate that another possible factor may relate to the expected length of interventions, since healer interventions may be more time-limited compared to long-term or indefinite periods of treatment associated with managing chronic mental disorders. Researching this aspect of why THs achieve such high adherence rates to their interventions may make it possible to develop strategies to improve medication adherence among patients with mental illness.
There are many more healers in South Africa than MHPs and a large portion of the population with mental health problems make use of their services, particularly TAHs. Based on the sheer number of TAHs it is essential to research ways to make best use of TAHs within mental health services and to consider developing referral pathways between MHPs and TAHs where possible. Engaging with TAHs in a manner that promotes cooperative working in mental health services may provide an untapped opportunity to increase access to care and encourage adherence to prescribed medication in patients who access both systems of care. The subjective reports of feeling better after consulting a healer most likely contribute to the relatively high number of respondents intending to re-consult with healers in future (58%). Quantitative measures and scales to measure this aspect may yield more information about healer–patient interactions, which may provide potential insights into the role of healers in psychiatry.
Supplemental Material
Supplemental material for Use of traditional and alternative healers by psychiatric patients: A descriptive study in urban South Africa
Supplemental material for Use of traditional and alternative healers by psychiatric patients: A descriptive study in urban South Africa by Zukiswa Zingela, Stephan van Wyk and Jacques Pietersen in Transcultural Psychiatry
Footnotes
Acknowledgment
The authors wish to thank Dr Leandré Gauché, Dr Wim Esterhuysen, Dr Eleanor Carr, and Mrs Tracy Geyer for assisting with collection, capturing, and analysis of data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.