
Abstract
Elevated levels of depressive and somatic symptoms have been documented among college students. Over the past two decades, there has been an increase in the number of Bedouin Arab students studying at institutions of higher education in southern Israel. To date, research on coping and mental health problems among students who are members of this ethnic minority has been limited. This study examined the role of three aspects of perceived social support – availability, satisfaction, and the ability to get emotional support – in predicting depressive and somatic symptoms among Jewish Israeli and Bedouin Arab college students. A total of 89 Bedouin and 101 Jewish first-year students participated in this study, which involved two assessment waves 12 to 14 months apart. Participants completed questionnaires assessing depressive symptoms, somatic complaints, three aspects of perceived social support, and demographics. At Time 1, Bedouin students exhibited higher levels of depressive and somatic symptoms and lower levels of all three aspects of social support. Regression analyses showed that level of emotional support was a prospective predictor of somatization at Time 2. Moreover, when levels of emotional support were low, ethnic group predicted depression at Time 2; emotional support predicted depression only among Bedouin Arabs. The present study highlights the importance of the use of emotional support in predicting somatic complaints and depressive symptoms specifically among Bedouin Arab students. Clinical implications on intervention programs for ethnic minority students will be discussed.
Keywords
Elevated levels of depressive and somatic complaints have repeatedly been found among young adults in general and among college students in particular. Over the past 15 years, the incidence of depression has doubled among the college/university student population. In a survey carried out among American college students, 32.5% of females and 25.4% of males reported that, within the last 12 months, they had felt depressed to the point that they found it difficult to function (American College Health Association, 2012). Moreover, the 12-month prevalence of somatic complaints among college students worldwide has been found to range from 15–60% (El Ansari, Oskrochi, & Haghgoo, 2014; El Ansari, Oskrochi, & Stock, 2013; Stock et al., 2008). Somatization is the translation of emotional distress into physical symptoms that have no identifiable physical cause.
The prevalence of these mental health problems (i.e., depression and somatization) is particularly noteworthy among Arab young adults worldwide (Kaplan, Glasser, Murad, Atamna, Alpert, Goldbourt, & Kalter-Leibovici, 2010) and Arab college students, in particular (Thomas & Altareb, 2012). Al Khatib (2013) surveyed 547 undergraduate students from Al Ain University of Science and Technology in the United Arab Emirates and found that 20.3% of those students reported having experienced mild depression over the past month and 33.8% reported having experienced major/clinical depression over the same period. A recent study has shown that, in Israel, Bedouin Arab students reported higher levels of depressive symptoms that indicate a risk of clinical depression as compared to Jewish students (Abu-Kaf & Braun-Lewensohn, 2015; Abu-Kaf & Priel, 2008). The tendency for individuals to somaticize distress is common among people from non-Western collectivistic cultures, such as Arabs (Consedine, Chentsova-Dutton, & Krivoshekova, 2014; Hamdi, Amin, & Abou-Saleh, 1997; Kleinman, 2004). A study of the prevalence of somatic complaints among Arab students from nine Libyan universities found that the majority of the surveyed students (62%) reported having experienced three or more symptoms of depression sometimes or very often over the last 12 months (El Ansari, Khalil, & Stock, 2014). Another study conducted among college students in Egypt found one-year prevalence rates of 22% for gastrointestinal complaints and 60% for aches and pains; these prevalence figures are higher than those observed among college students in England (El Ansari, Oskrochi et al., 2014).
The demographic composition of Israel provides an interesting opportunity to examine the role of social support in predicting depression and somatization in several different ethnic contexts. The current study sought to examine the cross-sectional and prospective relationships between different social support indices, depression, and somatic complaints in two different ethnic groups (i.e., Bedouin Arab and Jewish).
Bedouin Arabs in Israel belong to the Arab minority in the country. They comprise 27% of the population of the Negev (southern Israel). This society is characterized by a young population (over 60% are under age 19) and high levels of poverty (Israel Central Bureau of Statistics, 2015; RHA Center for Bedouin Studies and Development, 2010). Over the past few decades, this Bedouin society has undergone a rapid process of modernization. Over this period, there has been an increase in the number of Bedouin Arab students studying at institutions of higher education in Israel. In the 2007–2008 academic year, 672 Bedouin Arab students were enrolled in undergraduate studies. In 2013–2014, the number of Bedouin Arab students increased to 1107 (Hendin & Ben Rabi, 2016; RHA Center for Bedouin Studies and Development, 2010). In contrast, Jewish individuals are part of the majority culture that is more individualistic and less authoritarian than Bedouin Arab society and also emphasizes separation, independence, personal development, and achievement more than Bedouin Arab society (Hofstede & Hofstede, 2005).
Research on stress and coping has shown that one of the most effective means by which individuals cope with stressful events is social support (Cohen, 2004; Cohen & Wills, 1985). Social support is defined as information that leads people to believe that they are cared for and loved, esteemed and valued, and members of a network of communication and mutual obligation (Cobb, 1976). Since the 1970s, social support has been the focus of significant research interest. Overall, this research has shown that “social support is a valuable social commodity and those who are endowed with social support are better off in most instances than those who are not” (Hobfoll & Vaux, 1993, p. 685).
Social support has long been known to buffer against the adverse effects of stress, enhance well-being, reduce the severity of illness, and speed recovery from medical disorders when they do occur (Cohen & Wills, 1985; Dalgard, Thapa, Hauff, McCubbin, & Syed, 2006; Thoits, 1995; Uchino, 2004). Researchers have argued that social support is an important determinant of psychological well-being and academic adjustment among college students (Hinderlie & Kenny, 2002; Rodriguez, Mira, Myers, Morris, & Cardoza, 2003).
Different researchers investigating social support have applied the construct in different ways: as the number of people in the participant's network, as an index of overall satisfaction with social support, the availability of several forms or types of support (informational/emotional, tangible, affectionate support, and positive social interaction), and the ability to get instrumental and emotional support as coping strategies. There is substantial evidence showing the benefits of many forms of social support for both mental and physical health (Rodriguez et al., 2003; Thoits, 1995).
Despite the salient evidence of the positive impact of social support, many factors may influence the extent to which people perceive, seek, and use/get social support. Along with gender and personality, culture is considered an important factor. Recent research has shed light on cultural differences in the utilization and perception of different types of social support. The vast majority of research on this topic has been conducted among Asians and Asian-Americans. Those studies have consistently found that Asian and Asian-American participants explicitly seek support less frequently (Taylor, Sherman, Jarcho, Takagi, & Dunagan, 2004), find support to be less helpful (Kim, Sherman, Ko, & Taylor, 2006; Kim, Sherman, & Taylor, 2008; Wang, Shih, Hu, Louie, & Lau, 2010), and experience the explicit use of support as more psychologically and biologically stressful (Taylor, Welch, Kim, & Sherman, 2007). These results led researchers to the idea that individuals from non-Western–collectivistic/interdependent cultures may tend to use and benefit from different types and forms of social support as they attempt to manage stress. Taylor and her colleagues (2007) distinguished between explicit social support according to the conventional Western definition of the social support: “[…] as the advice, instrumental aid, or emotional comfort one can recruit from social networks… implicit social support as the emotional comfort one can obtain from social networks without disclosing or discussing one’s problems vis-á-vis specific stressful events. Implicit support can take the form of reminding oneself of close others or being in the company of close others without discussing one’s problems” (Taylor et al., 2007, p. 832).
A number of studies have found that Asians benefit more than Americans from implicit social support; whereas Americans derive more benefit from explicit social support (Kim et al., 2008; Taylor et al., 2007; Yang, Leu, Simoni, Chen, Shiu, & Zhao, 2015).
In using this form of emotional support, the individual may enjoy the benefits of emotional support without concerns of losing face or exposing vulnerability. Over the last two decades, a limited number of studies have been conducted to examine social support among Arab students in Arab countries and in Israel. Those studies have yielded several interesting findings. First, Arabs reported significantly more often than Jews that they would turn to “no one” for support (Kaplan et al., 2010; Pines & Zaidman, 2003). Second, in cases in which Arab students do decide to turn to others for help, they tend to turn to family members (i.e., spouse, mother, father, and siblings) more often than friends or professionals (Kaplan et al., 2010; Pines & Zaidman, 2003). Perceived social support from one’s family was a better predictor of whether a life event would be perceived of as a stressful situation (as compared to perceived social support from friends) (Khallad & Jabr, 2016; Hamdan-Mansour & Dawani, 2008).
Despite the growing number of cross-cultural studies focused on social support, little is known about social support outside of Western cultures. In particular, very little is known about the different types and forms of social support among people in Middle Eastern cultures and Bedouin Arab students, in particular.
The current study
We designed a two-wave longitudinal study to test the predictions of three different forms of social support concerning the prospective relationships with depressive symptoms and somatic complaints among Bedouin Arab and Jewish students. During the first month of the students' first year of university/college, the students completed self-report questionnaires in their native language (Time 1). Twelve to 14 months later (Time 2), the same students completed the self-report questionnaires once again.
Several research questions were examined in this study: a) will Bedouin Arab and Jewish students report different levels of social support, depressive symptoms, and somatic complaints?; b) which social support indices are negatively associated with depressive symptoms and somatic complaints among Jewish and Bedouin Arab students?; and c) which social support indices prospectively predict depressive symptoms and somatic complaints among Bedouin Arab and Jewish samples?
Method
Participants
Two hundred and seventeen students participated at Time 1 (110 Jewish student and 107 Bedouin Arab students). Attrition rates were 8% (nine students) and 17% (18 students) among the Jewish and Bedouin Arab students, respectively. Attrition from the current study was related to students moving and changing their phone numbers, which meant that they could not be contacted (4% and 4% among the Jewish and Bedouin Arab students, respectively); students leaving the university (2% and 9% among the Jewish and Bedouin Arab students, respectively); students refusing to participate at the second assessment time (2% and 2% among the Jewish and Bedouin Arab students, respectively), and students transferring to a foreign university (0% and 2% among the Jewish and Bedouin Arab students, respectively). Cross-tabulation analyses were conducted to examine the relations between attrition status and demographic variables, cultural context and gender. We found a statistically significant relationship between attrition status and cultural context: χ2 (1, 216) = 4.39, p < .05. More of the Bedouin Arab students dropped out of the study, as compared to the Jewish students. However, we did not find any statistically significant relationship between attrition and gender: χ2 (1, 216) = 0.12, ns.
Demographic characteristics: Differences between Bedouin Arab and Jewish students.

p < .05. ***p < .001.
Measures
To measure satisfaction with social support, the Social Support Questionnaire-6 (SSQ-6) was used (Sarason, Sarason, Shearin, & Pierce, 1987). The SSQ-6 is comprised of six items that address different problems (e.g., who can you really count on to help you feel more relaxed when you are under pressure or tense?; who can you really count on to be dependable when you need help?). Each item has two parts. The first part of each item assesses the number of people to whom the individual feels he or she can turn when this problem occurs and the second part of each item measures the individual's degree of satisfaction with the perceived support available in each situation on a six-point Likert scale (ranging from very dissatisfied to very satisfied), to yield a satisfaction score (SSQS-6). This scale has been shown to have high internal reliability (Sarason et al., 1987). In the present study, we used only the satisfaction score from the Arabic and Hebrew versions (Hobfoll, Canetti-Nisim, & Johnson, 2006). The internal reliability score (Cronbach’s alpha) for this scale was .86 among the Bedouin Arab sample and .70 among the Jewish sample.
The MOS Social Support Survey (MOS) was used to assess the availability of social support (Sherbourne & Stewart, 1991). The MOS is a 19-item self-report questionnaire used to assess the perceived availability of support, if needed. Respondents were asked to indicate how often different types of support are available if needed on a five-point Likert scale ranging from 1 (never) to 5 (all of the time). Examples of items include “someone to help you if you were confined to bed”; “someone to confide in or talk to about yourself or your problems”, and “someone to share your most private worries and fears with”. In Sherbourne and Stewart’s (1991) study, the instrument was tested among adults in different geographic locations and the reliability and validity of the instrument were established. In the current study, the Arabic and the Hebrew (Schwartz & Frohner, 2005) versions of this instrument were used. The Cronbach’s alpha coefficients for the scale were .91 and .72 among the Bedouin Arab and Jewish students, respectively.
To assess the ability to get emotional social support, participants completed the Getting Emotional Support subscale of the shortened version of the Coping Orientations to Problems Experienced Inventory (Brief COPE) (Carver, 1997). Participants rated the two emotional support statement in terms of how frequently they used each strategy to manage stressful events, on a scale of 1 (never) to 5 (always). These items include: “I've been getting emotional support from others”; and “I've been getting comfort from someone”. In the current study, the Hebrew (Ben-Zur, Gilbar, & Lev, 2001) and Arabic (Qouta, Punamäki, & El Sarraj, 1997) versions of the instrument were used. The internal consistency coefficients of these versions of the instrument were .83 and .77 among the Bedouin Arab and Jewish students, respectively.
The Center for Epidemiological Studies Depression Scale (CES-D) was used to assess symptoms of depression (Radloff, 1977). The CES-D is a 20-item inventory of symptoms on which respondents report how frequently they experienced each symptom during the past week, using a four-point Likert scale that ranges from zero (rarely or none of the time) to 3 (most or all of the time). Examples of items include “I felt that I could not shake off the blues even with help from my family or friends” and “I thought my life had been a failure”. Scores ranged from 0 to 60 and the lenient diagnostic cut-off point for depression, based on participants’ scores on the CES-D, is 16. A stricter cut-off point of 23 is considered more reliable (Roberts, Andrews, Lewinsohn, & Hops, 1990). We used a Hebrew version of the CES-D (Blumstein et al., 2004) and an Arabic version (Ghubash, Daradkeh, Al Naseri, Al Bloushi, & Al Daheri, 2000; Kazarian & Taher, 2010). In this study, the Cronbach’s alpha coefficients for the CES-D scores at Time 1 and Time 2 among the Bedouin Arab and Jewish students ranged from .84 to .92.
Somatization was assessed using the 15-item Somatic Symptom Severity Scale (PHQ-15) from the Patient Health Questionnaire (Kroenke, Spitzer, & Williams, 2002). Respondents reported on the frequency of symptoms experienced during the past month, using a three-point Likert scale that ranged from zero (none of the time) to 2 (most of the time). Examples of items include “pain in your arms or legs or other joints”, “nausea, gas, or indigestion”, and “headaches”. The PHQ-15 has been translated into numerous languages and has been examined in different countries (such as Saudi Arabia, Germany, and others; Becker, Al Zaid, & Al Faris, 2002; Lowe et al., 2004). In this study, the Cronbach’s internal consistency alpha coefficients for the PHQ-15 scores at Time 1 and Time 2 among the Bedouin Arab and Jewish students ranged from .72 to .82.
Respondents were asked to report their ethnicity/cultural group, gender, age, and institutional affiliation.
Procedure
Approval for the study was granted by the Ethics Committee of Ben-Gurion University of the Negev. Advertisements were published in Arabic and Hebrew at the university and on websites aimed at students. Students contacted (by email or by phone) the research assistants (two Jewish research assistants and two Bedouin Arab assistants) to set up a face-to-face meeting. The questionnaires were administered in small groups of five to eight participants in a large classroom on the campus, in a standardized format. The order in which the questionnaires were presented was counterbalanced. The students were informed that the purpose of the study was to better understand their experiences during their university/college studies.
One year later, those same students were contacted (by email or by phone) and invited to participate in the second assessment wave. At Time 1, participants completed the SSQ6, MOS, the Getting Emotional Social Support subscale – Brief COPE, CES-D, PHQ-15 and demographic questionnaire in their native language (Arabic or Hebrew). At Time 2, they completed the CES-D and PHQ-15. At Time1 and Time 2, students also completed additional questionnaires concerning coping strategies and adaptation to academic life. After the second set of data was collected, participants were fully debriefed as to the purpose of the study. Among the student who initiated contact with the research assistants, 92% of the Bedouin Arab students and 89% of the Jewish students arrived to the data-collection session and completed the questionnaires.
Data analysis
A preliminary χ2 analysis was used to explore differences in sample characteristics between the two cultural groups. Four main sets of analyses were conducted. First, an attrition analysis was performed. Second, a two-way MANOVA was conducted to test for group and gender differences in levels of social support, depression, and somatization at Time 1 and Time 2. Then, zero-order correlations were computed to test the cross-sectional relationships among the study variables among Bedouin Arab students and Jewish students. Finally, two regression analyses were employed to examine the longitudinal associations between social support, somatization, and depression among the two samples.
Results
Attrition analysis
The 18 Bedouin Arab participants lost to attrition were compared with the 89 Bedouin Arab participants who completed all of the questionnaires at Time 2. Among the Bedouin Arab students, a MANOVA was conducted with attrition status as the independent variable and social support (satisfaction with social support, Getting Emotional Support, and availability of social support) and emotional distress (depression T1 and somatization T1) as the dependent variables. We found significant differences in the ability to get emotional social support. In the Bedouin Arab sample, participants who dropped out of the study reported significantly lower levels of emotional social support (F (1, 106) = 5.5, p < .05,
Group and gender differences
Social support indices, depression, and somatization at Time 1: Means and standard deviations for each subgroup and effects of culture, gender, and culture-X-gender.
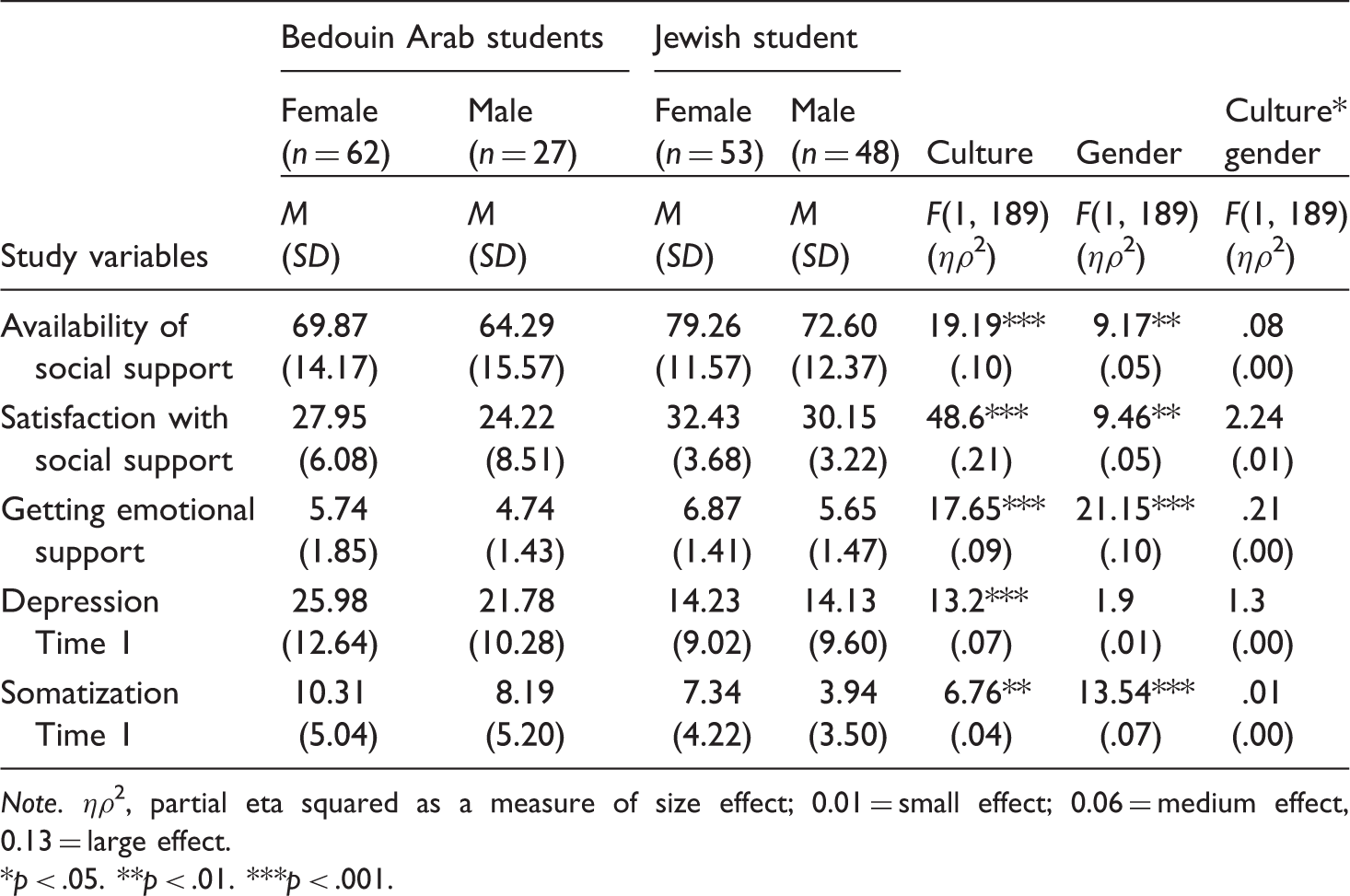
Note. ηρ2, partial eta squared as a measure of size effect; 0.01 = small effect; 0.06 = medium effect, 0.13 = large effect.
p < .05. **p < .01. ***p < .001.
We found that ethnicity affected depression at Time 1, somatization at Time 1, and the three indices of social support. The Bedouin Arab students had higher levels of depression and somatization at Time 1, as compared to the Jewish students. As shown in Table 2, the Bedouin Arab participants’ mean score on the CES-D at Time 1 was close to the stricter diagnostic cut-off point of 23 among both males and females. Among the Bedouin Arab sample, at Time 1, 13 male participants (48%) and 38 females (61%) scored above the stricter diagnostic cut-off point of 23. Moreover, Bedouin students reported lower levels of availability of social support, satisfaction with social support, and use of emotional support.
Gender had an effect on somatization at Time 1, as well as social support indices. Females reported higher levels of somatization and social support than males.
Cross-sectional relationships among the study variables
Zero-order correlations observed between the study variables.

Note. Correlations below the diagonal are for the Jewish group (n = 101) and correlations above the diagonal are for the Bedouin Arab group (n = 89). The results shown above relate to scale scores.
p < .05. **p < .01. ***p < .001, two-tailed test.
Longitudinal association of somatization and depression
Hierarchical regression analysis of predictors of depression at Time 2 (N = 190).

Note ^ p < .07 *p < .05, two-tailed test. ***p < .001, two-tailed test.
When Time 2 depression served as the outcome (see Table 4), Block 1 accounted for 38% of the variance of this outcome (adjusted R2 = .38, F [7,182] = 15.92, p < .001). Statistically significant predictors were: Time 1 depression (b = .37, SE = .08, β = .37, t = 5.46, p < .001), somatization (b = .52, SE = .17, β = .23, t = 3.00, p < .01), and ethnicity (b = 1.69, SE = .83, β = .15, t = 2.34, p < .05; a sharper increase in depression was observed among the Bedouins). Block 2 explained an additional 3% of the variance of the outcome (adjusted R2 = .41, F [13,176] = 19.02, p < .001) and this addition was marginally significant (F-change = 1.85, p < .07). Importantly, the only significant two-way interaction was observed between the use of emotional support and ethnicity (b = −1.87, SE = .90, β = −.16, t = −2. 08, p < .05). Block 3 added another 1% to the variance of the outcome explained by the regression model (adjusted R2 = .42, F [16,173] = 17.48, p < .001), but that addition was not statistically significant (F-change = .1, ns). None of the three three-way interactions between ethnicity, gender, and social indices was statistically significant.
We probed the statistically significant two-way interaction based on Aiken and West’s (1991) recommendations. We found that when levels of emotional support were low (1 SD below the mean), ethnicity prospectively predicted depression (unstandardized simple slope = 6.78, SE = 2.59; standardized simple slope = 0.29, t = 2.62, p = 001). However, this effect was not significant when levels of emotional support were high (unstandardized simple slope = 0.31, SE = 2.50; standardized simple slope = 0.01, t = 0.13, p = .90). When probing the interaction from perspective of ethnicity as a moderator, emotional support did not predict depression at Time 2 among the Jewish students (unstandardized simple slope = −0.48, SE = 0.57; standardized simple slope = −0.07, t = −0.85, p = 0.40), but was marginally significant among the Bedouin students (unstandardized simple slope = −2.69, SE = 1.43; standardized simple slope = −0.23, t = −1.89, p = .061; Figure 1).
Effect of the interaction between ethnic group and emotional support on depression at Time 2.
When Time 2 somatization served as the outcome, Block 1 accounted for 52% of the variance of that outcome (adjusted R2 = .52, F [7,182] = 47.62, p < .001). Statistically significant predictors were: Time 1 somatization (b = .58, SE = .06, β = .58, t = 8.99, p < .001), gender (b = −.66, SE = .29, β = −.16, t = −2.22, p < .05; women reported a greater increase in somatization), and getting emotional support (b = −.35, SE = .20, β = −.15, t = 1.97, p < .05). Block 2 and Block 3 each added 1% to the variance of the outcome explained by the regression model. These additions were not statistically significant (F-change = .89, ns; F-change = 1.49, ns). None of the two-way or three-way interactions was a statistically significant predictor of somatization at Time 2.
Discussion
The current study aimed to examine the ability of three different aspects of perceived social support to predict depressive symptoms and somatic complaints among Bedouin Arab and Jewish students. As expected, considerable mental health problems were found among the Bedouin Arab students. Approximately 50% of the surveyed Bedouin Arab students (males and females) scored above the stricter diagnostic cut-off point of 23, indicating severe levels of depressive symptoms. The statistics presented here are similar to previous statistics related to depressive symptoms among Arab college students (Al Khatib, 2013). Furthermore, Bedouin Arab college students face additional difficulties and challenges as they come from a disadvantaged population that is experiencing a rapid transition process and are the first generation from their families to have access to higher education (Abu-Kaf & Braun-Lewensohn, 2015). Bedouins also reported a greater increase in depression over time, in the presence of average or low levels of emotional social support. Moreover, higher levels of somatization were observed among Bedouin Arabs in their first year of college/university studies (Hamdi et al., 1997; Kleinman, 2004). In a study conducted among immigrants in the United States, individuals from collectivistic societies who were less emotionally acculturated to American culture (i.e., expressed and inhibited their emotions differently than Americans) were more likely to develop somatic symptoms (Consedine et al., 2014).
An additional interesting group difference was found in the internal consistency of many of the measurements in the current study. Higher internal consistency was found among Bedouin Arab students than among the Jewish students. This finding may be related to the fact that the research on Bedouin Arab society in general, and Bedouin Arab students in particular, is quite limited. Thus, knowing that one is taking part in one of the first studies in this field may affect one’s motivation to participate in such research. This motivation might influence the way these students completed the questionnaire (e.g., more concentration and more consistency).
Gender differences were noted for somatization levels at Time 1 and at Time 2. Women reported higher levels of somatization than men and this finding is consistent with previous research (Houghton et al., 2012). However, the present study showed no significant difference in the prevalence of depression among males as compared to females, which is contrary to the common understanding that depression is generally more common among women.
Ethnic differences in the three social support indices were found. Bedouin Arab students reported lower levels of social support, as compared to Jewish students. These findings support previous research that has demonstrated that, like Arabs, Asians and Asian-Americans use less social support for coping with stress than European-Americans or Jewish Israelis (Kim et al., 2008; Taylor, Sherman, Jarcho, Takagi, & Dunagan, 2004; Wang et al., 2010). These ethnic differences may be related to the fact that in more collectivistic cultures (e.g., Bedouin Arab culture), requesting assistance from others may involve exposing one’s vulnerability and/or incompetence, risking rejection or “losing face”, and/or fear of hurting the feelings of others and making them uncomfortable (Taylor et al., 2004).
We found a similarity in the cross-sectional relationships between social support indices, and depression and somatization among Bedouin Arab and Jewish students. We found negative associations between depression and each of the social support indices. This finding is in line with those of several studies that have shown that low levels of perceived social support are related to depressive symptoms (Cohen, & Wills, 1985; Grav, Hellzen, Romild, & Stordal, 2012). However, we found no associations between somatization and two indices (i.e., availability of social support and satisfaction with social support) among the two samples. Cultural differences were noted with regard to getting emotional social support; this variable was positively associated with somatization among the Jewish students, but not among the Bedouin students. This latter finding is consistent with Kleinman’s claim that a “presentation of personal and interpersonal distress in an idiom of physical complaints may include an adaptive coping pattern of help-seeking” (Kleinman, 1986, p. 51). Somatization in specific cultural context can yield constructive outcomes such as increased use of social support (Kleinman, 1986, 2004). Moreover, positive associations were found between somatic and depression symptoms. This finding supports those of previous studies that found that depressive symptoms and somatization are strongly associated with one another (Baune, Caniato, Garcia-Alcaraz, & Berger, 2008; Kroenke, 2003).
The main aim of this study was to examine the ability of three different indices of social support to prospectively predict depressive and somatic symptoms among Bedouin Arab and Jewish students. Our results underscore the unique role of the getting emotional support (as a coping strategy) in predicting prospective somatization among both Bedouin Arab and Jewish students. In this study, greater ability to get emotional support predicted lower levels of somatic complaints one year later. However, when depressive symptoms were considered as an outcome, emotional social support was prospectively predictive only among Bedouin Arab students.
This finding supports the conceptualization of implicit and explicit social support presented by Taylor and her colleagues (2007), who claimed that people from non-Western collectivistic cultural backgrounds may utilize and benefit more from implicit social support as emotional comfort one can obtain from social networks by thinking about supportive social networks/relationships and/or spending time with significant others (particularly family members) without disclosing or discussing one’s problems or the specific stressful events. In using this form of emotional support, the individual can enjoy the benefits of emotional support while avoiding concerns about negative implications for relationships (e.g., fear of hurting loved ones' emotions, inconveniencing them, losing face or exposing vulnerability) that might otherwise be associated with the use of explicit social support. Thus, in the presence of lower levels of implicit emotional of support, Bedouin Arab individuals appear to be at risk of developing depressive symptoms.
Limitations and directions for future research
Although the two-wave, prospective design used in this study represents an advance over previous retrospective or cross-sectional studies, this study had some limitations and there are areas that warrant further attention in future research. First, our findings were based on self-report measures. Thus, further research using different methods of data collection (e.g., interview techniques, diaries, observer ratings) would be beneficial and important for the evaluation of the validity of the obtained findings. Moreover, given that social support, somatization, and depressive symptoms were all self-reported by the same individuals, there is the potential for shared reporting bias and/or reverse causation. It is likely that people experiencing depressive symptoms will view their social situation more negatively than those who are not depressed. In addition, people who are depressed can have a harder time seeking out social support. Thus, we cannot totally exclude the possibility that the associations involving these variables may be bidirectional. Third, the current study includes a relatively small and self-referred sample. Thus, individuals who sought the study team may have higher levels of distress and different attitudes and behaviors as compared to the general population of students. Future study should include larger sample of student from both cultural contexts and using different recruitment strategies. Next, the generalizability of the present results should be examined in other Bedouin Arab populations. There is a question as to how representative a sample of Bedouin Arab university students is of the Bedouin Arab culture, in general, and it can be argued that Bedouin Arab university students are more affected by Western values than the rest of the Bedouin Arab population. Future research including a non-student Bedouin Arab sample would allow for evaluation of the generalizability of the observed results.
Finally, there is a need to employ more assessment waves, to allow the sufficient evaluation of rank-ordered longitudinal changes, as well as the detection of prospective associations between different forms of social support and depression\somatic complaints.
Conclusion
The importance of this study lies in its examination of the role of different aspects of social support in predicting depressive and somatic symptoms among Jewish and Bedouin Arab college students. The present study highlights the importance of the use of emotional support in predicting somatic complaints and depressive symptoms specifically among Bedouin Arab students.
The results of the current study suggest that professionals who work with college students should design and implement interventions that focus on first-year students who are members of ethnic minority groups. Professionals providing psychological counseling in colleges and universities should be aware of the importance and the benefits of the use of emotional support for all students and for ethnic-minority students, in particular. Intervention programs should provide ethnic-minority students with appropriate and useful types of social support. Those programs should increase the chances of those students feeling more strongly affiliated with and belonging to the social network of the university/college (through the experience of being involved in relationships with significant others, particularly students from the same cultural background). Moreover, those students should be integrated into meaningful and enjoyable social activities, which should increase the implicit emotional support available to them, decrease somatic complaints, and improve their levels of functioning, all of which may have significant value for preventing future severe somatic and depressive symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.