
Abstract
The DSM-IV Outline for Cultural Formulation (OCF) was a framework for assessment based on principles of cultural psychiatry. The Cultural Formulation Interview (CFI) for DSM-5 provided a tool enabling wider use of cultural formulation in clinical cultural assessment. Validation to justify the inclusion of the CFI in DSM-5 involved quantitative analysis of debriefing interviews of patients and clinicians for feasibility, acceptability and clinical utility. We now further examine qualitative field trial data from the CFI interviews and the debriefing interviews in Pune, India. Administration of the CFI was followed by routine diagnostic assessment of 36 psychiatric outpatients—11 found to have severe mental disorders (SMD) and 25 with common mental disorders (CMD). Domain-wise thematic analyses of the CFI and debriefing interviews identified recurrent themes based on cultural identity, illness explanatory models, stressful and supportive social relationships, and the impact of political, economic, and cultural contexts. A tendency to elaborate accounts, rather than simply name their problem, and more diverse past help-seeking distinguished CMD from SMD groups. Patients valued the CFI more than clinicians did, and most patients did not consider cultural background differences of clinician-patient relationships to be relevant. Qualitative analysis of CFI data and critical analysis of domain mapping of CFI content to the structure of OCF domains indicated the value of revising the dimensional structure of the OCF. A proposed revision (OCF-R) is expected to better facilitate clinical use and research on cultural formulation and use of the CFI.
Keywords
Introduction
The Outline for Cultural Formulation (OCF) introduced in Appendix I of the DSM-IV was an important step towards acknowledging the relevance of culture in the practice of mainstream psychiatry (APA, 1994). The Cultural Formulation Interview (CFI) published in the text of the DSM-5 provided an operational formulation of the OCF, thereby making essential features of cultural psychiatry more accessible to mainstream practitioners (APA, 2013). Although the structure of the OCF, an assessment framework, was modified for the CFI (Lewis-Fernández et al., 2014), which is an assessment tool, the domain structure of both the OCF and CFI address common priorities, including questions about cultural identity, emic ideas about illness, social relationships (including the relationship between the patient and clinician), and the influence of stressful and supportive societal settings.
An important step in the development of the CFI involved assessment of its feasibility, acceptability, and clinical utility in India and in all participating sites of the multi-site international field trials (Lewis-Fernández et al., 2017; Paralikar et al., 2015). The CFI has been shown to enhance medical communication (Aggarwal, DeSilva, Nicasio, Boiler, & Lewis-Fernández, 2015) and to have value for use with patients’ relatives (Hinton et al., 2015). Barriers to wider use of the CFI have been reported (Aggarwal, Nicasio, DeSilva, Boiler & Lewis-Fernández, 2013). These studies of the perceived value of the CFI based on pilot-study experience, however, have not examined the clinical data from CFI interview content, and such consideration is relevant and needed.
Filling that gap, this study analysed clinical cultural data from CFI interviews in the field trial at the collaborating site in Pune, India. We examined domain-wise findings from both qualitative CFI assessment data and the perceived value of the CFI by patients and clinicians in subsequent debriefing interviews. To examine the effect of psychopathology on cultural assessment and cultural formulation, we also compared CFI clinical data of patients with common mental disorders (CMD) and serious mental disorders (SMD).
Methods
Setting
The study was conducted in the context of CFI field trials at the site in urban Pune, India. The city has a rich cultural heritage and opportunities for employment that attract migrants from surrounding rural areas, including the Konkan coast of Western Maharashtra and other regions of India. The research was conducted in the psychiatry outpatient department of the King Edward Memorial Hospital (KEM), a multi-speciality charitable trust hospital with 650 beds serving a lower- middle-class population that pays for low-cost services.
Instruments
Structure of the field trial version of the CFI used in multi-centre validation studies and revision published in DSM-5.
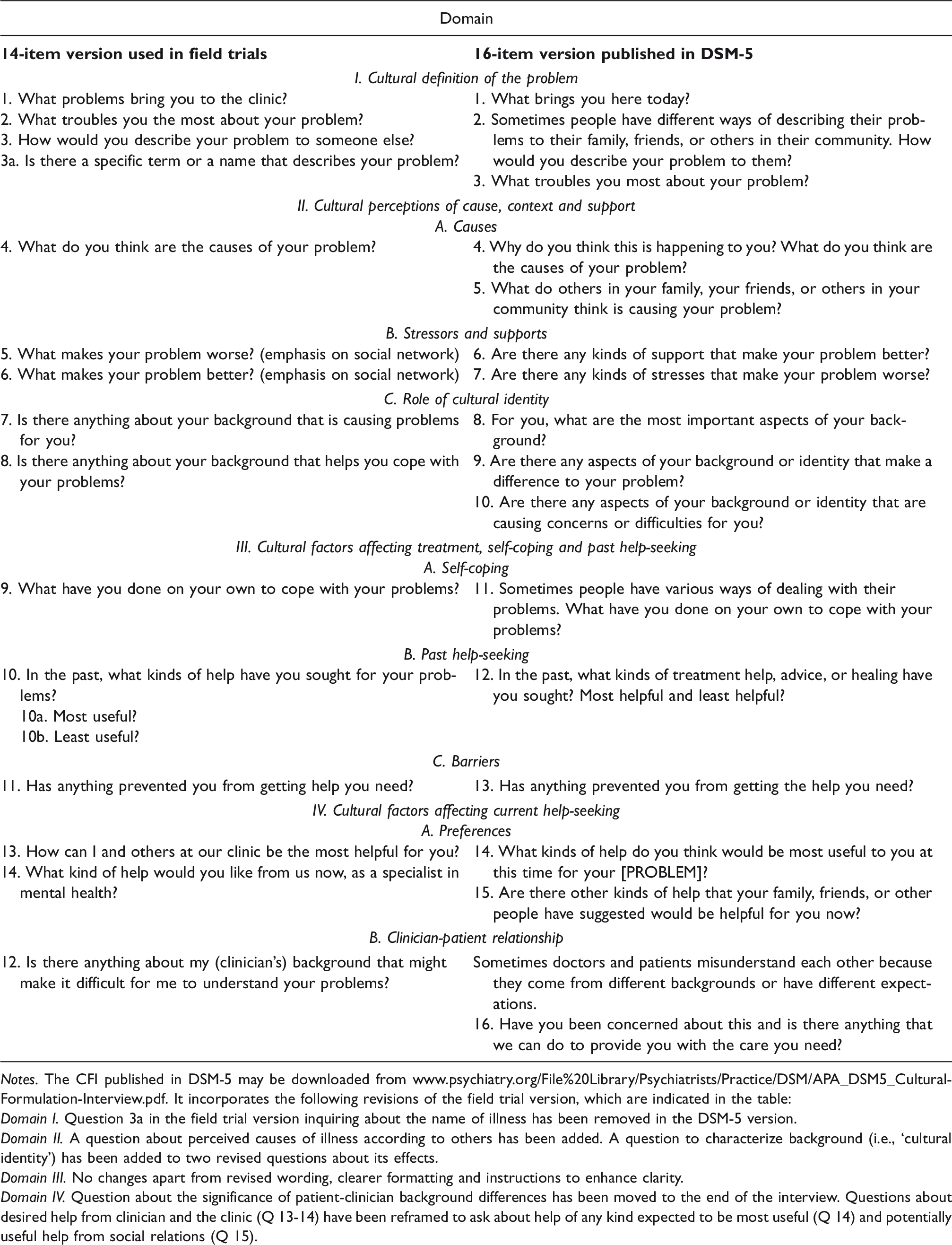
Notes. The CFI published in DSM-5 may be downloaded from www.psychiatry.org/File%20Library/Psychiatrists/Practice/DSM/APA_DSM5_Cultural-Formulation-Interview.pdf. It incorporates the following revisions of the field trial version, which are indicated in the table:
Domain I. Question 3a in the field trial version inquiring about the name of illness has been removed in the DSM-5 version.
Domain II. A question about perceived causes of illness according to others has been added. A question to characterize background (i.e., ‘cultural identity’) has been added to two revised questions about its effects.
Domain III. No changes apart from revised wording, clearer formatting and instructions to enhance clarity.
Domain IV. Question about the significance of patient-clinician background differences has been moved to the end of the interview. Questions about desired help from clinician and the clinic (Q 13-14) have been reframed to ask about help of any kind expected to be most useful (Q 14) and potentially useful help from social relations (Q 15).
Debriefing interviews for clinician (DIC) interviewers and patients (DIP) queried the perceived value and relevance of the CFI. They included both categorical and narrative questions about experience with CFI, the value of content elicited, effects on rapport, and relevance for diagnosis and treatment planning. The DIC was supplemented with an enhanced version for additional detail in the first and third interviews. Both the DIC and DIP invited suggestions to improve the instrument.
Design
Adult patients 18–80 years of age were eligible for recruitment. After explaining the study to potential participants, their capacity to consent was assessed and consent was obtained. Patients were excluded if acutely suicidal, intoxicated, or symptomatic for drug withdrawal, dementia, mental retardation, or florid psychosis that impaired their capacity to complete the interview. Patients completed a demographic information form with assistance from the research team, if required. The CFI was administered by a clinician who had not previously seen that patient. Debriefing interviews were administered to each clinician and patient after the CFI interview by another clinician.
Clinicians were trained to use the CFI, and each completed between three and seven CFI interviews, as required in the multi-centred field trial. Each patient was interviewed only once. All CFI and debriefing interviews were audio-recorded. After administering the CFI, the same clinician conducted a routine clinical diagnostic interview to make a DSM-IV-TR diagnosis. Based on that diagnosis, patients were classified as either CMD (mainly anxiety and depressive disorders) or SMD (psychotic disorders and/or multiple comorbidities).
Data management and approach to analysis
Audio recordings of the CFI and the debriefing interviews were translated into English. First-level thematic codes were derived from the structure of the instruments (i.e., questions of the CFI and debriefing interviews). Narrative content of the CFI and the debriefing interviews was imported from MS Word into MAXQDA and coded with the autocoding feature based on formatting by interview item. The dataset was read and re-read to identify and manually code content from questions of each domain that was relevant for other domains of the CFI, mindful of the fact that a patient’s response to any one question might be more relevant to the interests of another question. Manual coding involved a process of repeated immersion in the data set and mapping of thematic content across domains of the CFI and with reference to domains of the OCF. We first analysed the aggregate sample and then compared CMD and SMD patients.
Results
Patient sample and clinician interviewers
CFI and diagnostic interviews were completed by eight psychiatrists for 36 patients (14 women and 22 men). Fourteen debriefing interviews were conducted by three of these psychiatrists and 22 by two psychologists. The mean age of study patients was 38.3 years (standard deviation (SD), 12.46), and the mean of their years of education was 13 years (SD, 4.03). Most patients were married (21/36), 12 were never married, and three were divorced or separated. Most patients were unemployed or dependent (28/36), and all patients were from low or middle-income economic strata. CMD diagnoses (25) were more frequent than SMD (11).
Among clinicians, seven were women and three were men. Their mean age was 39.1 years; Marathi was the first language for nine and English for one. All were fluent in Hindi. Mean years of clinical experience was 13.3 years (SD, 7.36; median, 13 years; range, three to 32 years).
Domain I: Cultural definition of the problem
CFI domain-specific content, diagnostic distinctiveness and perceived relevance.

*See Table 3 for elaboration of causes and contexts.
CMD patients were more likely to elaborate on their problems than SMD patients. The North Indian man mentioned above explained his problem: I wasn’t taking treatment, and I thought I could survive it without meds … However, currently, my confidence level goes low, especially when I have to give an interview or meet new people. My tongue starts stammering and I don’t like it. I don’t think I will be able to survive this competitive world.
Debriefing evaluation
Patients and most clinicians appreciated the first few questions of the CFI because they provided space to elaborate details of problems and family contexts. Clinicians valued clinical insights from these first questions, which helped formulate differential diagnosis and treatment priorities. Patients typically found it difficult to immediately provide a name, and clinicians noted difficulty trying to elicit a name from them. Two clinicians suggested removing this question.
Domain II: Cultural perceptions of cause, context and support
Causes, and stressors and supports
Due to bad habits like gambling, one loses money and you go bankrupt. You regret becoming bankrupt, you feel depressed, sadness comes and you feel guilty. Due to bankruptcy, you are unable to do anything. When there is mental weakness (mana-durbalta), I gamble. In my opinion, mental weakness increases due to sexual urges (laingikta). If one continuously has sex, it causes weakness … Having sex every day is inappropriate and harmful, but I am unable to control the urge. I feel like having sex all the time … I told her [his brother’s wife] some made-up story and forced her to have sexual relations with me. I felt a lot of guilt, and I repent about what I did with my sister-in-law. But I could not control myself.
Summary of causes and contexts of presenting problems (domain II).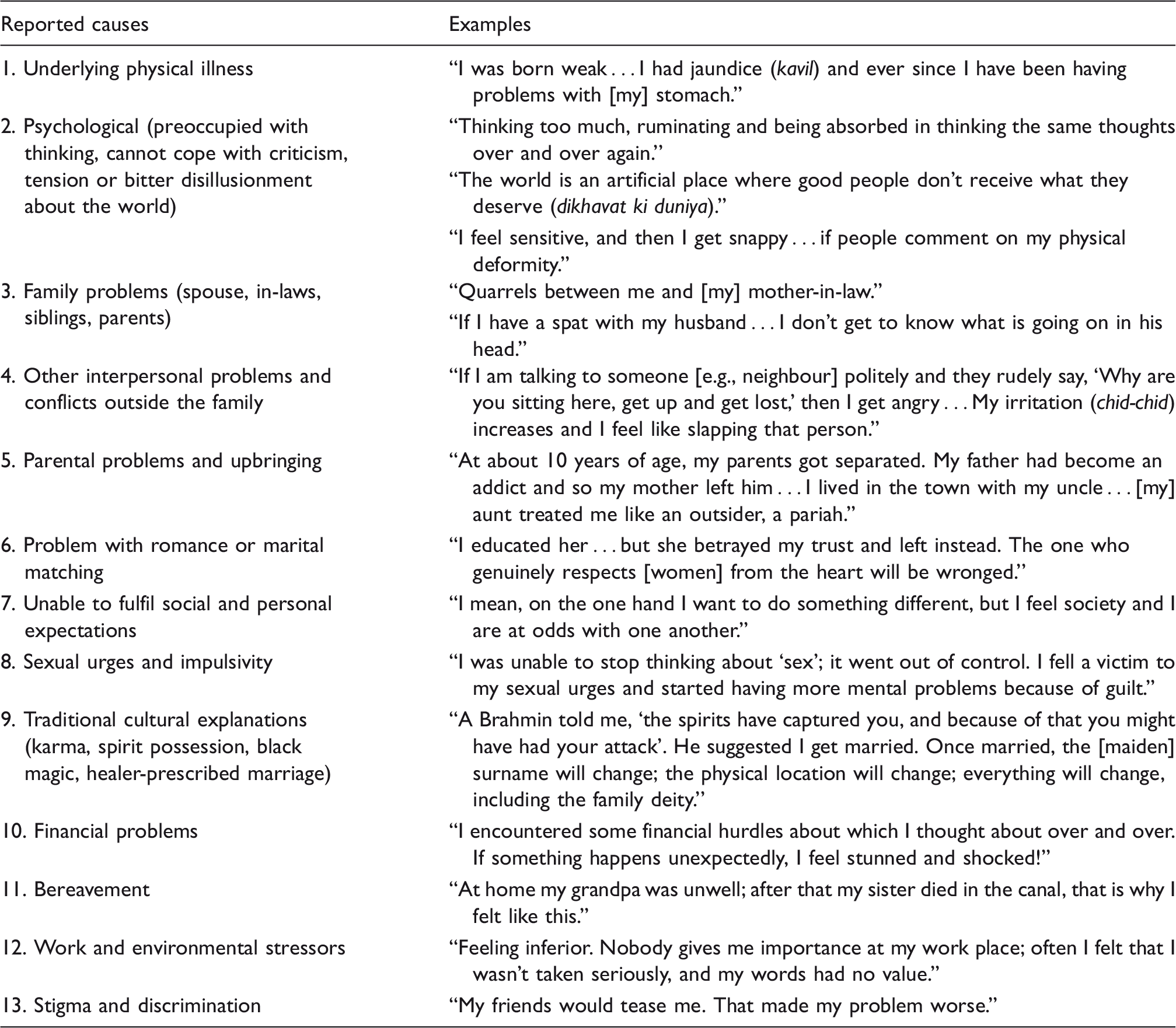
Initially I used to go to my parents’ place if such quarrels happened … My parents used to sympathetically advise me, and I felt better. It was also quite relaxing talking to my friends at work, back when I had a job … My sister-in-law is good support. She sympathetically advises everybody in our family and solves many problems. Because of her, my marriage is still intact.
Debriefing evaluation
Patients appreciated the opportunity to discuss causes and contexts. For some, responding to these questions generated valued psychological insights. For example, the North Indian patient quoted earlier explained, “I am glad that this question was asked this time. Initially I thought that these things [pressure from family and relatives] trouble me, but now having shared this information I think that even I should work on some things about myself.”
Clinicians recognized treatment implications from their better understanding of patients’ perceived causes and social supports. They also valued the process of focusing on patients’ experience because it enhanced rapport in the clinical relationship. A clinician interviewing a 54-year-old man with hallucinations explained, “I feel that the cultural perceptions of cause, context and support are important elements, along with the patient’s understanding of his problem.” In some interviews, however, clinicians were frustrated when they were unable to elicit a relevant response.
Role of cultural identity
Many patients found it difficult to talk about cultural identity in response to the two questions about its impact, which was the focus of the cultural identity questions in the field trial version of the CFI. Although only a few expressed clearly positive or negative effects, most denied its negative impact on their condition (23/36).
For those describing adverse effects, cultural identity was framed with reference to stressful conditions and contexts, such as migration, place of origin, religion, caste, social norms, and problems with their in-laws’ family. Caste-related issues were woven into the discourse, but usually explicit only on probing. Differences between SMD and CMD accounts were subtle, although SMD patients seemed less inhibited in describing the negative impact of cultural identity.
Though accounts conflated elements of personal background and difficult social conditions, migration was most frequently linked to a cultural identity contributing to distress. Migration-related cultural issues typically emphasized how hard it was to adjust. Accounts referred to migration at various levels: within-city, between-cities, rural-urban, and international migration. Explaining problems from within-city migration attributed to conflictual cultural identities, an unemployed 27-year-old non-Brahmin man described his upbringing in a Brahmin community. Although his father owned a house in a multi-caste and multi-religious community, he had rented a house in the Brahmin community, drawn by the appeal of a cultured environment. Economic problems after his father’s death compelled the patient to return to the multi-cultural neighbourhood. After moving back, he encountered discrimination and stigma by others who regarded his background in the Brahmin community as pretentious: When we moved from Sadashiv Peth (Brahmin locality) to Ganj Peth (multi-religious locality), people in Ganj Peth knew we had moved from Sadashiv Peth, and they believed that we were very snobbish. People from Sadashiv Peth are very cultured because many Brahmins live there. The life style is ‘Brahmin type’, and we would behave in the same manner … I mean our ‘level’ had become like that only. Everybody would think of us as Brahmins only, as our manners were also like theirs. My husband is from Satara and I am brought up in Pune. So I am following Pune culture, but my in-laws live in the style of Sangli, Satara, Kolhapur culture – that is, the culture of Western Maharashtra. There they harass daughters-in-law, and so many women have committed suicide by jumping in the well. We belong to the same caste, but my husband’s family has a different culture and that’s creating a problem.
One patient explicitly associated her problem with low-caste status. The following dialogue between this 39-year-old English-speaking patient with SMD and her clinician interviewer indicates the importance of acknowledging the impact of cultural identity in establishing a therapeutic alliance. Clinician: Is untouchability still practiced? Patient: Yes. In Modi-Khana Clinician: Do you mean to say that it is still practiced there? Patient: Untouchability is still practiced everywhere … Clinician: Oh, I didn’t think it was. Patient: Where do you live? Clinician: In India, but I didn’t think it was practiced in Pune. Patient: Come with me and I will show you.
Debriefing evaluation
Some patients who understood and reflected on questions about the role of cultural identity appreciated the opportunity to talk about their faith in god; they emphasized the importance of religion, caste identity, and family values. A 50-year-old man with SMD explained, “Questions that asked me how I understand my illness and the question where I answered about attending religious programs to feel better were helpful.”
Notwithstanding initial difficulty understanding the question about the impact of cultural identity, with additional time on the topic, some came to value the question, as indicated in the following dialogue between a patient and the debriefing interviewer: Patient: At first, topics related to culture are a little difficult to understand. I even told him [the clinician]. Because I hadn't thought about how being ill may affect my family. And I realized that it actually does affect them... Clinician: What were those cultural questions? Patient: What influence does your caste have on your illness? Whether your problems increase or decrease. [The] first time it is a little difficult to understand. It seems all is okay and has no impact. Clinician: So, you have to put some thought into it? Patient: We have to think, madam, because this is the first time I am facing such questions. Before this, doctors never asked me if your background has any impact on your problems. They ask [about symptoms] and I tell them, and I get my medicines. I mean it might be helpful to others but I don’t think it applies to me. I don’t think I have a problem of that nature; therefore I don’t think that question is important. Suppose there is a Christian person living in a Hindu location, who dresses differently or doesn’t apply vermilion [kumkum, the traditional powder used by married women], then maybe people would look at them differently and talk behind their back. But because we live in a Hindu location, I don’t face these problems from the neighbours, because we all follow similar customs.
Other clinicians, however, who did not elicit useful responses remained skeptical: The patient could not understand the questions properly. We were unable to go beyond superficial issues despite much probing. The patient is illiterate. She restricted responses to symptoms and her relatives only. She was circumstantial or went off on a tangent. This could be due to the formal thought disorder … or it may be due to her being too preoccupied with her physical complaints.
Domain III: Cultural factors affecting treatment, self-coping, and past help seeking
Patients talked about several self-coping strategies, such as exercise, recreation, art, literature, religious help seeking, seeking social support, and introspection. A few patients regarded use of medicines as self-coping. Responses typically referred to self-coping measures without much reflection on how they helped. A middle-aged woman, however, was a notable exception; she explained the value of joining a self-help group for lonely people: We have a group called anand-yatra [‘happy journey,’ a group for single people]. There I can talk to my female friends who are older to me, and I seek their support. There is no hassle in letting go of loneliness for a while because they are all extremely lonely. So we come together as friends.
Some patients, however, liked non-directive empathic listening. A woman with CMD was dissatisfied with prior religious help, finding it proscriptive but unproductive. She preferred the interviewer’s empathic listening. “You, doctor, have asked me everything so calmly, and I have been able to tell everything with similar ease. Others keep telling me what to do.”
Barriers to help-seeking included treatment cost, travel time, and concerns about the effectiveness and side effects of medicine. Some CMD patients reported a lack of family support and fear of stigma were barriers to treatment. A 38-year-old man with CMD explained, “Money factor, fear of what people will say about me – that I am mentally ill. So I avoided treatment. Even though the distances were more, I continued treatment in the government hospitals as medicines were available at no cost.”
Stigma was also an explicit barrier for several other patients. The young man from North India noted earlier elaborated on the impact of stigma: Initially I didn’t want anybody to know about my treatment. In the villages people go to ojhas [magico-religious healers] and it’s acceptable. But for mental health that’s a little different. [My] family is afraid that people [will find out] about this problem. A marriage opportunity may come my way, but if they come to know about my mental disease, that will be a problem. They will say: ‘This fellow has a mental disease.’ I can't go to relatives, they will ask many questions. This information will spread like fire. I don't have a problem with that, but my mother and father will go into depression [suffer because of it]. They will avoid seeing relatives because they will ask about their son.
Debriefing evaluation
Patients appreciated the chance to express grievances with previous treatment. This was clearer from their accounts than from their remarks in debriefing. Clinicians valued information about past help-seeking and barriers to current help-seeking, both for diagnosis and treatment planning. They typically noted that benefit but without elaborating.
Domain IV: Cultural factors affecting current help seeking
The value of treatment was based on expectations that many patients described explicitly. They referred to attentive listening, understanding, advice, solutions, information, appropriate medicines, and their own anticipation of quick and complete recovery. The 37-year-old male CMD patient who had referred to an affair with his sister in-law explained that he expected benefits from making sense of a thorough analysis of his account, and he elaborated expectations as follows: My depression should be studied in detail, carefully considering each of my thoughts and words. My words and my thoughts should each be verified on the basis of what I am suffering from and why. This evaluation will yield a diagnosis. You should undertake research on my depression and provide me with the best medicine. My earlier happiness and enthusiastic nature should be restored for me, and I should behave like a good human being in society. Patient: No, not at all. Because you are a doctor, your relationship with your patients should be friendly. You should not let your background affect the relationship with a patient, so that this should not affect the treatment. Therefore I don’t think there will be any problem with you. Clinician: Suppose that I, as the doctor, was from a different culture or spoke a different language, might it then make a difference? Patient: Yes, then it might have an effect to some extent, because you would not be able to understand my problems. … I don’t think religion and language have too much of a role to play, but yes, background could possibly play a role. The family and society or community (samaj) you live in and ways of doctors’ and patients’ thinking may differ, and that could affect the treatment.
Discussion
This is the first report from analysis of CFI interview content at a site of the DSM-5 field trials. Our qualitative analysis of interview findings with reference to domains of the framework of the version of the CFI published in the DSM-5 extends the scope of previous analysis for quantitative reports that documented the value of the instrument. The qualitative approach explains what patients and clinicians did or did not appreciate in the CFI and why. We have compared cultural formulations of patients with diagnoses of CMD and SMD, and we have also analysed patients’ and clinicians’ qualitative accounts in debriefing interviews, inquiring about their perceived relevance of the CFI. The following discussion of our findings explains what these cultural formulations tell us about the significance of culture in the problems of our patients. The discussion is relevant for practical applications of pursuing the research interests of clinical ethnography (Calabrese, 2013) and cultural epidemiology (Weiss, 2017). We are primarily concerned here, however, with the practical clinical implications of our experience in the field trial and with the implications for conceptualization and clinical use of cultural formulations derived from assessment with the CFI or by other means (Lewis-Fernàndez, Aggarwal & Kirmayer, 2016).
Value of the CFI
Our consideration of the value of the CFI based on interview content and qualitative debriefing interviews provides results similar to the positive experiences reported in earlier studies (Lewis-Fernández et al., 2017; Paralikar et al., 2015; Aggarwal et al., 2015). Questions about causes and contexts in domain II were the most appreciated by both patients and clinicians, and were most easily elaborated with perceived practical significance. Patients were surprised and appreciative of clinicians’ interest in both their illness and their cultural identity, indicating the value of reflecting on the process and findings from the assessment. Some requested more attention to questions on sexuality, thereby indicating a wish to share with the clinician intimate details they considered relevant, expecting these to contribute to complete recovery as a worthwhile human being.
Patients valued rapport with the CFI interviewer, and they were more enthusiastic than clinicians in endorsing the value of the CFI. Clinicians’ acknowledgement of the value of the CFI interview, which also has been noted in other field-site validation studies (Bäärnhielm et al., 2016; Aggarwal et al., 2013), was mitigated by concerns about the time required to administer it. Appreciation of the CFI is consistent with complementary developments in person-centred approaches to psychiatric care (Mezzich, Botbol, Christodoulou, Cloninger & Salloum, 2016; Kirmayer, Bennegadi, & Kastrup, 2016), patient-reported outcomes (Rotenstein, Huckman, & Wagle, 2017), and the increasing priority of cultural competency (Lim, Diaz, & Ton, 2016; Napier et al., 2014). Such efforts contribute to long-standing goals to realize practical benefits of clinically applied medical anthropology (Helman, 2007; Kleinman, 1983).
OCF and cultural formulation case reports
A substantial body of cultural formulation case studies has enriched the literature of cultural psychiatry. Such case studies were introduced as a regular feature of the journal Culture, Medicine and Psychiatry over more than two decades (Lewis-Fernandez, 1996). Many of these and comparable case studies published in other journals show how culture contributes to diagnosis and case management (Bäärnhielm, 2012; Bäärnhielm & Scarpinati Rosso, 2009; Bucardo, Patterson, & Jeste, 2008; Shore & Manson, 2004; Browne, 2001; Yilmaz & Weiss, 2000; O’Nell, 1998; Barrett, 1997; Lim & Lin, 1996; Manson, 1996). The presentation of these case reports is typically structured according to the five domains of the OCF presented in the DSM-IV (APA, 1994), concluding with a summary of the contributions of the cultural formulation to diagnosis and clinical management in domain V. The wording for these domains was modified slightly, but without altering the underlying framework, in an update of the OCF in DSM-5 (APA, 2013).
Reconfiguring OCF domains in the CFI
Although the OCF framework facilitated the communication of cultural formulation in case reports, clinical communication, and training, it was considered unsuitable as an operational framework for structuring questions of the CFI. The priorities of assessment were found to be fundamentally different from the priorities of conceptualizing, documenting, and communicating case formulations. As noted in the handbook on the CFI, it follows a “typical sequence in clinical interviewing” (Kirmayer, 2016). Structural adjustments are required to maintain this flow, e.g., where and how to situate questions about cultural identity, which is the topic of the first domain of the OCF, with respect to domain II of the CFI, which concerns questions about causes and contexts.
Domain II of the OCF on cultural explanations of the illness covers a wide range of illness-related interests. The four points in the DSM-IV and DSM-5 descriptions of domain II of the OCF are addressed in four different CFI domains: local illness categories are mapped to domain I; meaning of illness and patient-perceived causes are mapped to domain II; and past help-seeking experience and current plans are mapped to domains III and IV, respectively. Interests of three other domains of the OCF are embedded across domains of the CFI: questions concerning cultural identity (domain I of the OCF) are in domain II of the CFI. Cultural categories of psychosocial environment and levels of functioning (domain III of OCF) are partially addressed in domain II. But level of functioning is not directly assessed in the core CFI, although it is covered by supplementary module (SM) 2. Cultural elements of the clinician-patient relationship (domain IV of the OCF) are also addressed in domain IV of the CFI, which also includes consideration of current preferences for help and clinical care.
Future development of the cultural formulation will benefit from consideration of how it relates to interviews like the CFI, which provide the essential clinical information (Kirmayer, 2016). To better represent the cultural formulation emerging from such interviews, Kirmayer suggests a two-dimensional grid, with space for clinical information in cells at the points of intersection on two dimensions: one dimension with critical points in “course of illness” (six categories from causal factors to social response) and a second dimension for “systemic level” (eight categories on the spectrum from subpersonal to global systems) (see Table 6-4 in Kirmayer, 2016). Such a grid with 48 cells to be populated with information from clinical assessment data is too complicated for mainstream use, which remains a priority for the CFI to justify its inclusion in the DSM. Nevertheless, acknowledgement of the challenges of representing a cultural formulation highlights limitations of both the original OCF and the CFI for structuring that clinical information. It suggests a need for an updated practical framework that is feasible, acceptable, and useful for documenting and communicating cultural formulations.
Implications of findings for proposed OCF revision (OCF-R)
Based on critical consideration of the structure of the original OCF and analysis of data from our CFI interviews, we suggest further modification of the OCF in a proposed revision (OCF-R). This may better fulfil the need for a simple coherent practical framework that better clarifies and distinguishes priority interests of cultural formulation. This OCF-R is similar to the original but modifications are more conceptual and comprehensive than the revised OCF for DSM-5. By proposing a more refined and coherent structure, this proposal for an OCF-R may hopefully facilitate conceptual understanding, documentation of case records, and both clinical and research communications. Figure 1 indicates the relationship of the domain structures of the original OCF, the CFI, and OCF-R. Because OCF-R has been derived from analysis of our CFI data, it may be better suited (i.e., more feasible, acceptable, and useful) for documentation and communicating a cultural formulation.
Comparing domains of the OCF, CFI and proposed OCF-R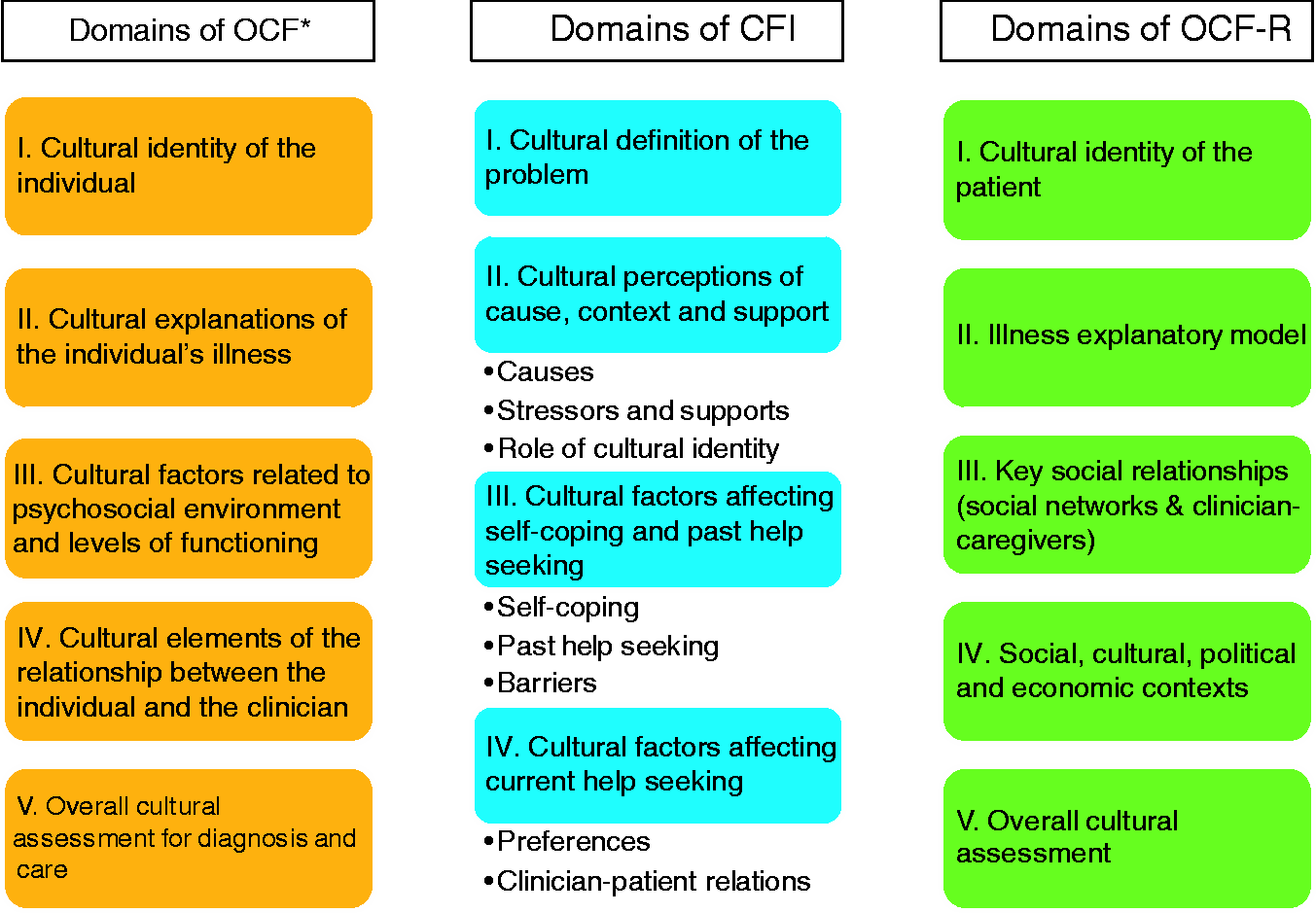
The framework of OCF-R refers to the patient, problem, social relationships, contextual settings, and overall significance of the cultural formulation. Domains of this framework are summarized in Figure 2 and elaborated below with reference to findings from the analysis of our CFI data, presented earlier as results.
Framework of proposed OCF revision (OCF-R) for documenting and communicating findings from assessment of cultural formulation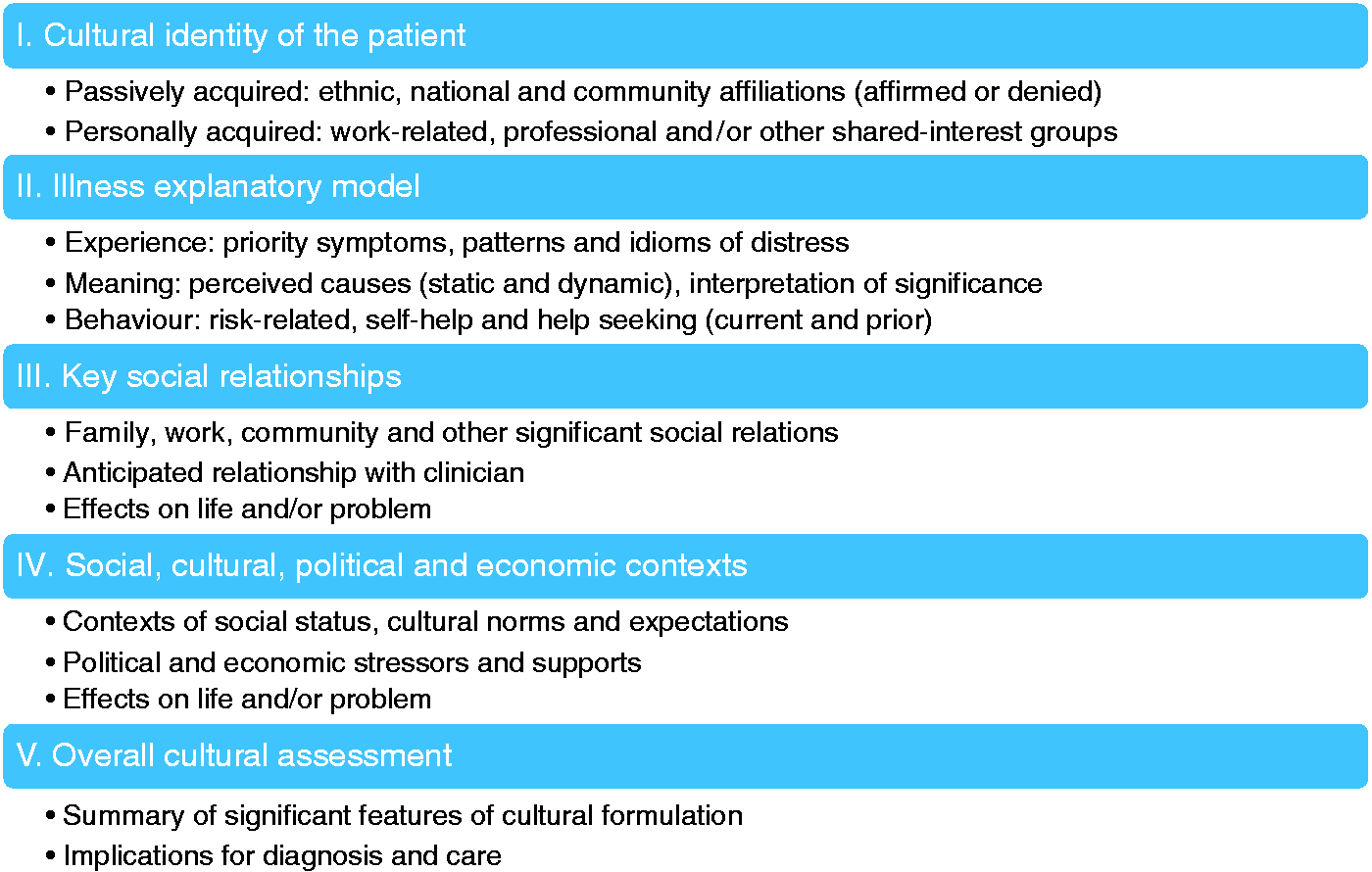
I. Cultural identity of the individual patient
Domain I, which elaborates cultural identity, remains essentially unchanged from the original OCF. It refers to a comprehensive account of a patient’s background, considering “an individual's racial, ethnic, or cultural reference group” (DSM-5) and more. Assessing cultural identity requires an interviewer to focus on a patient’s self-ascribed identity, rather than the views of others or of the clinician. Our experience in the field trial was notable for some clinicians’ difficulties eliciting – and patients’ difficulties articulating – accounts of cultural identity with a useful level of detail. This was also a problem reported at other sites in the field trials (Bäärnhielm et al., 2016). The questions of the field trial version considered only the impact of cultural identity without first adequately clarifying what it meant for the patient. Revisions in the DSM-5 published version of the CFI and development of SM (Supplementary Module) 6 on cultural identity responded to these limitations. However, further research on eliciting and evaluating the role of cultural identity is needed, and the development of the supplementary module and related efforts indicate prospects for that.
II. Illness explanatory models
Interest in cultural explanations of a patient’s illness, domain II of the original OCF, has also been an enduring feature, not only of cultural formulation but also the field of cultural psychiatry itself. The DSM-5 modification of the OCF referred to “cultural conceptualizations of distress”. Our focus on illness explanatory models is mindful of usage of the term ‘illness’ in medical anthropology, referring to an affected person’s experience of a health problem and the nature of distress. Inasmuch as the cultural formulation itself is intended for clinical use, the term ‘illness’, rather than distress or problem, is appropriate. Our recommendation for use of the term ‘illness explanatory model’, rather than ‘cultural explanation’ or ‘conceptualization’, is intended to consolidate the broad interests of the illness explanatory model in a single domain, rather than spread these illness-related interests across domains. In the CFI various aspects of illness explanatory model are covered in domains II, III, and IV to preserve the flow of the interview (e.g., past and current help-seeking each placed in separate domains).
As explained in the recent second edition of the Textbook of Cultural Psychiatry, confusion about a misleadingly narrow focus on perceived causes discourages acknowledgement of the broader scope of Kleinman’s original formulation of the illness explanatory model framework (Weiss, 2018). Kleinman proposed illness explanatory models as “notions about an episode of sickness and its treatment that are employed by all those engaged in the clinical process” (Kleinman, 1980). Consequently, the broad scope of interests implied by “notions” endorses the priority of a wider range of illness-related issues (Weiss, 2018; Lloyd et al., 1998), and the focus on illness should therefore not be limited to cultural ‘explanations’. Cultural implications of illness, its meaning, and what to do about it are all fundamental interests of the illness explanatory model framework. Cultural patterns and idioms of distress, priority symptoms, perceived seriousness, the pain of patient-perceived stigma, self-coping, past help-seeking experience, anticipated outcome, and current preferences for help are all relevant. These various facets of the illness explanatory model are therefore the designated focus of domain II of the OCF-R.
In our CFI data set, information about patients’ illness explanatory models came from questions in all domains of the CFI. Naming illnesses (CFI domain I) yielded various responses; perceived causes (CFI domain II, see Table 3) were wide-ranging and widely valued; accounts of self-coping and past help-seeking (CFI domain III) and current preferences for help (CFI domain IV) were diverse. This last point was most relevant in distinguishing patients with CMD, who had wider and more diverse past help seeking experience, from patients with SMD. Current preferences for help seeking often highlighted desires for medicines that bring quick recovery, and counselling that is directive and problem-solving in the context of a close, confiding clinical relationship that is benevolent and parent-like.
III. Key social relationships
Key elements of social relationships, acknowledging family and other interpersonal social stressors and supports, were addressed by questions in CFI domains II and III. They are consolidated in OCF-R domain III. The formulation of this domain also places the clinician-patient relationship in the broader context of social relations. The two are complementary, though fundamentally different: key interpersonal relationships elicited in the course of the CFI are for the most part elements of history and life experience that a patient brings to the interview. Asking a patient to comment on potential effects of a clinician’s cultural differences that may affect the clinician’s effectiveness is less a matter of a patient’s experience. It is more an indication of a new relationship that did not exist before the start of the assessment interview, even though past experience in clinical and other social relationships may be influential.
Key relationships with a spouse, parent or child, siblings, and in-laws were as important as expected in our patients’ accounts. Rich narratives explained interpersonal aspects of vulnerability, coping, resilience, and support; they confirmed the priority of family and neighbourhood relations, which were a substantial component of patients’ narratives.
The priority of the anticipated clinician-patient relationship had been addressed in domain IV of the CFI after questions about current help seeking preferences. Our patients uniformly denied any personal concerns about adverse effects of the clinician’s cultural background differences. Idealization of the doctor is consistent with traditional values, which are likely to limit acknowledgement of anticipated concerns about this relationship, especially in an initial assessment interview. If such concerns were to be expressed, they would probably reflect a seriously problematic prior clinical experience.
IV. Social, cultural, political and economic contexts
Protecting human rights of psychiatric patients and protecting the field of psychiatry itself from collusion and misuse of confinement and forced treatment for political control are well-recognized priorities of psychiatry (Freeman & Pathare, 2005). The field is less attentive, however, to the impact of social, cultural, political, and economic contexts affecting the lives of people in the world and the mental health of patients, apart from consideration of disorders defined by social or situational trauma, like post-traumatic stress disorder. Critics of the global mental health agenda have argued that additional consideration of the impact of relevant contexts and settings is required (Kirmayer & Pedersen, 2014; Cooper, 2016). Broader interest in the contexts of life around the world and their nonspecific effects on mental health problems have been acknowledged in the field of cultural psychiatry, but they are less visible in prior frameworks for cultural formulation. Sharpening the focus on this designated focus of OCF-R domain IV better acknowledges the priority of the topic.
Questions about contextual factors are included in domain II of the CFI, which is directly concerned with effects on the presenting problem of stressors and supports. Background issues associated with cultural identity in the CFI, such as the legal and financial issues that may complicate migrant status, are also relevant considerations for the proposed OCF-R domain IV. The relevance of contextual interests of this domain for the field of cultural psychiatry is acknowledged by several supplementary modules of the CFI that address key interests, including SM 4 on psychosocial stressors (Qureshi, Falgàs, Collazos & Hinton, 2016) and SM 5 on spirituality, religion, and moral traditions (Gellerman, Hinton, & Lu 2016). SM 11 for immigrants and refugees is also relevant, addressing pre-migration difficulties, migration-related losses and challenges, and how they relate to the clinical problem (Boehnlein, Westermeyer, & Scalco, 2016). SM 9 on children and adolescents (Rousseau & Guzder, 2016) and SM 10 on issues confronting older adults (Aggarwal & Hinton, 2016) similarly consider the influential contexts characterizing these two stages of life.
The impact of various relevant contextual issues is readily discernible from narrative accounts in our CFI interviews. Several study patients highlighted relevant concerns, and the structure of the OCF-R better acknowledges their relevance and priority. For example, a female artist complained bitterly about Indian culture lacking an “art mentality”. Another woman of American origin who migrated and became a resident of India acknowledged problems of the collectivist culture and the oppressive nature of caste. The Maharashtrian woman quoted in the results section on cultural identity explained the impact of cultural values affecting life with her in-laws with reference to “the Sangli-Satara-Kolhapur [regional] culture … [where] they harass daughters-in-law.” Other patients referred to the burden of cultural values that require copious spending on marriages and magico-religious beliefs that constitute barriers to rational choices for help seeking. Although some of these issues were elicited by questions on cultural identity or the illness explanatory model in the CFI, they also suggest the additional value of asking directly about aspects of political, economic, communal, terrorist, and other potentially relevant contexts of life in patients’ worlds. This may be accomplished by further revisions of the core CFI, and/or by further revising or adding one or more supplementary modules.
V. Overall cultural assessment
The final domain of the OCF-R and earlier versions involves summarizing the overall value of the cultural formulation and the relevance of the cultural formulation for diagnosis and clinical care. In that regard, reflections of the clinician on CFI findings and questions of the qualitative debriefing instruments used in the field trials may be more useful than the CFI itself. Such a debriefing question may be a worthwhile addition in a revised version of the CFI, inasmuch as experience with this instrument, like others used in psychiatry, is likely to lead to further revision.
CMD–SMD differences and study limitations
Our results show that CMD patients were more likely to elaborate patterns of distress, and they were more likely to make use of a larger network of self-help and outside sources of help. SMD patients were more likely to acknowledge the value of doctors and medicines. In many ways, however, their accounts were notably similar. This may reflect similarities between the two groups, inasmuch as SMD patients had to be recovered well enough to participate in the interview. The heterogeneity of psychopathology included in both SMD and CMD groups may also have obscured differences based on specific features of psychopathology. The SMD group included not only patients with a diagnosis of a psychotic-spectrum or mood disorder, but also patients with multiple comorbidities of CMD. Including such conditions in the CMD group may not necessarily constitute a sufficiently coherent diagnostic grouping. Furthermore, our diagnoses were based on clinical assessment by the interviewer after administering the CFI, rather than on more rigorous research criteria. Although our study design enabled comparison of CMD and SMD groups, this was not the primary consideration in recruitment and instrumentation for the CFI field trial.
Further research should pay attention to the findings and relevance of cultural formulation among various diagnostic groups, and our experience indicates a way to proceed with careful research design. Other comparative study interests, apart from diagnostic groups, would also clarify the practical implications of cultural formulations in the course of routine assessment. Such research should consider implications of gender, religion, caste, migration status, and other factors.
Conclusion
Our study describes an approach to the CFI, and presents findings from thematic analysis of interview content and qualitative assessment of the value of the CFI. Discussion of these findings highlights the value of cultural formulation in clinical practice. Our findings indicate the clinical value of the CFI in a family-centric society and the role of cultural values, livelihood, ambition, lust, and guilt. The cultural nature of marriage and family, with their strengths and weaknesses, and social interpersonal stresses, are elucidated by hopeful patients who were able to confide.
As a tool for assessment, the CFI complements the OCF as a framework for using the products of clinical cultural assessment. Each is structured according to its respective aims: the CFI is designed to assess clinical cultural data and the OCF to organize, document, and communicate a cultural formulation. The development of both is guided by critical reflection on experience and a subsequent process of revision. This process is essential for better theory, practical applicable frameworks, and useful instruments. Changes to the field trial version of the CFI in the published version of DSM-5 and our proposed revision of the OCF as OCF-R result from complementary processes and developments in the field of cultural psychiatry. Hopefully, our experience and findings, and the OCF-R may contribute to further interest, appreciation, and capacity for the productive use of cultural formulation in clinical practice.
Footnotes
Acknowledgements
Hindi translations of the CFI were provided by Dr. Smita Deshpande (Ram Manohar Lohia Hospital, Delhi) and Dr. Shubhangi Parkar (KEM Hospital, Mumbai). Dr. Vaishali Naik, and Ms. Priya Dabak assisted with translations of the Marathi and adaptation of the Hindi instruments. We thank Medha Kale, Taysir Moonim, Viplavi Joshi, Sanjeev Sarmukaddam, Aarati Puranik and Aarti Subandh for their editorial support. We acknowledge the contribution of clinician psychiatrists and psychologists of the KEM Hospital. They are Swati Joshi, Geeta Bhat, Amit Nulkar, Jyoti Shetty, Arvind Panchanadikar, Niket Kasar, Vrushali Garde-Shenoy, Mayura Bhagwat, Nishreen Saif, and Kanak Patil. We are indebted to the patients who consented to these interviews.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support of the KEM Hospital Research Centre, Pune, is gratefully acknowledged.