
Abstract
Cross-national epidemiological studies show that prevalence rates of common mental disorders (i.e. depression, anxiety disorders, and PTSD) vary considerably between countries, suggesting cultural differences. In order to gather evidence on how culture relates to the aetiology and phenomenology of mental disorders, finding meaningful empirical instruments for capturing the latent (i.e. non-visible) construct of ‘culture’ is vital. In this review, we suggest using value orientations for this purpose. We focus on Schwartz's value theory, which includes two levels of values: cultural and personal. We identified nine studies on personal values and four studies on cultural values and their relationship with common mental disorders. This relationship was assessed among very heterogeneous cultural groups; however, no consistent correlational pattern occurred. The most compelling evidence suggests that the relationship between personal values and mental disorders is moderated by the cultural context. Hence, assessing mere correlations between personal value orientations and self-reported symptoms of psychopathology, without taking into account the cultural context, does not yield meaningful results. This theoretical review reveals important research gaps: Most studies aimed to explain how values relate to the aetiology of mental disorders, whereas the question of phenomenology was largely neglected. Moreover, all included studies used Western instruments for assessing mental disorders, which may not capture culturally-specific phenomena of mental distress. Finding systematic relationships between values and mental disorders may contribute to making more informed hypotheses about how psychopathology is expressed under different cultural circumstances, and how to culturally adapt psychological interventions.
Keywords
Introduction
The global prevalence of common mental disorders such as depression, anxiety disorders and posttraumatic stress disorder (PTSD) is substantial (Kessler & Ustun, 2008), and depression is among the leading causes of disability worldwide (Whiteford et al., 2013). However, the World Mental Health Surveys (WMHS) showed that prevalence rates varied considerably across countries: statistically significant higher rates were found in high-income countries (i.e., the USA, New Zealand, France, and the Netherlands) than in low- and middle-income countries (e.g., China, Nigeria, Mexico, or India). For PTSD, documented prevalence rates in Nigeria and China were even close to zero (Kessler et al., 2007).
In the WMHS, not only did the prevalence rates differ across countries, but their correlates did as well. Kessler and Bromet (2013) found that the relationship between income and the lifetime prevalence of depression was stronger in high-income countries than in low- and middle-income countries. Regarding education, an even more complex pattern of associations emerged: In some non-Asian countries (Israel, the US, Mexico and Ukraine), low education was associated with higher rates of depression. In Pondicherry (India), respondents with the lowest education were 14 times as likely to have depression, whereas in Japan and Shenzhen (China), the least educated had the lowest risk of depression (Kessler & Bromet, 2013). One possible interpretation of this finding is that education per se is not related to mental health outcomes, but rather the extent to which education and achievement are valued in society.
Hence, findings from the WMHS indicate cultural differences regarding the prevalence rates and the correlates of common mental disorders. Such cultural differences most likely relate to the aetiology and phenomenology of mental disorders (Kirmayer, Lemelson, & Cummings, 2015). Aetiology refers to the factors that foster or undermine mental illness, thus to the actual underlying prevalence rates. By contrast, phenomenology refers to variations in how psychological distress and mental illness are expressed across different cultures. Different terms have been used to describe such cultural variations regarding the phenomenology of mental disorders, such as idioms of distress (Nichter, 1981, 2010) or culture-bound syndromes (American Psychiatric Association, 1994). In an extensive literature review, Kohrt et al. (2014) compiled evidence from 45 studies which described such ‘cultural concepts of distress’ (CCD). The authors assessed the methodological quality of included studies and examined associations between CCD and psychiatric disorders. Associations became lower with increasing epidemiological rigour of the study. The authors concluded that “More rigorous and culturally appropriate studies … may represent studies that describe CCD more accurately and thus capture the uniqueness from psychiatric categories” (p. 400). Hence part of the variation in prevalence rates possibly results from the category fallacy (Kleinman, 1987), which refers to “the reification of a nosological category developed for a particular cultural group that is then applied to members of another culture for whom it lacks coherence and its validity has not been established” (p. 452).
Research has still not answered the question whether CCD are actually unique, or to what extent systematic relationships can be found between specific cultural patterns and the prevalence and expression of mental distress. Similar patterns of distress were found in disparate cultural settings (e.g., Jilek & Jilek-Aall, 1985; Kirmayer & Minas, 2000), but these studies did not systematically look at similarities regarding the cultural context in which such patterns of distress emerged. In order to reveal systematic relationships between culture and psychopathology, finding meaningful empirical instruments for capturing the latent (i.e. non-palpable) construct of ‘culture’ is vital.
This review suggests using value orientations (Schwartz, 1994a, 1994b) for this purpose. Value orientations facilitate and structure personal and cultural spheres and serve as behavioural and motivational guides for individuals, institutions, and nations (Boer & Fischer, 2013; Fischer & Boer, 2011). Societies develop their culturally-specific value orientations in response to their very specific economic and ecological living-conditions, and values are transmitted to the next generations via socialisation. Evidence suggests that certain circumstances (e.g., greater opportunities in life) lead to similar value orientations (e.g., importance given to self-realisation) across cultures, even if qualitative differences exist with regard to how these values are expressed (Fischer, 2013). In this sense, value orientations make culture measurable to some extent.
The present review compiles evidence on whether and how value orientations are associated with the prevalence and expression of mental disorders, and critically examines this evidence from a theoretical perspective. Several research groups have attempted to find relationships between values and mental disorders, but from our point of view, a critical theoretical reflection on the nature of this relationship is still lacking. We argue that a strictly theoretical approach will be needed in order to reveal systematic patterns of relationships between values and mental disorders, if they exist. Therefore, we first outline Schwartz's theory on cultural and personal value orientations (Schwartz, 2006) and explain the difference between these two levels. Thereafter, existing evidence on value orientations and mental disorders will be integrated into this theoretical framework and conclusions will be drawn for future research. Finding systematic relationships between values and mental disorders may contribute to making more informed hypotheses about how psychopathology may present under different cultural circumstances, and how to culturally adapt psychological interventions (Bernal & Sáez-Santiago, 2006).
Value Orientations: A Taxonomy to Delineate the Latent Concept of Culture
Different psycho-cultural value theories exist and have been studied extensively over the last few decades. Hofstede (1980) describes societies according to the dimensions collectivism vs. individualism, along other dimensions. Inglehart (1997; Inglehart & Baker, 2000) suggested a distinction between materialist and postmaterialist values, arguing that people's values change in the process of modernisation. And Schwartz presented a value theory which encompasses value orientations at the personal and cultural level (Schwartz, 2006, 2014; Schwartz & Bilsky, 1990). The three value theories are based on theoretical assumptions and empirical data from large, cross-national studies, some of which are repeatedly applied in order to enhance validity and draw conclusions about the stability vs. variability of values (e.g., the World Values Survey). Schwartz (1994a) defined values in terms of conscious goals, or “responses to three universal requirements with which all individuals and societies must cope: needs of individuals as biological organisms, requisites of coordinated social interaction, and requirements for the smooth functioning and survival of groups” (p. 22).
One of Schwartz's (1994a, 1994b) core theoretical assumptions is the circular structure of values, which distinguishes his theory from other value theories. This circular structure reflects relationships between values: Adjacent values in the circular structure are similar, i.e. share motivational content, whereas opposed values conflict with one another and cannot be pursued at the same time without causing motivational conflicts. Values can be thought of in terms of what they share with adjacent values, but also in terms of their opposite pole. Hence individuals and cultures can be described regarding their giving importance to either one or the other pole of different value dimensions.
Schwartz's conceptual differentiation between the cultural and personal level is unique among current value theories and offers a useful theoretical framework for the purpose of this review. Cultural value orientations use the country or region as the unit of analysis, whereas personal value orientations use the individual person as the unit of analysis (Schwartz, 2006). Since the two levels and the interaction between them already provide a sophisticated background for examining cultural differences in mental health, no other value theories were included in the present review, in order to reduce complexity.
The second dimension refers to the maintenance of social order, which is reflected in the contraposition of hierarchy vs. egalitarianism. Hierarchy refers to the legitimacy of an unequal distribution of power, roles, and resources. By contrast, egalitarianism encompasses equality and social justice. The third dimension describes people's relations to the natural and social world, which is reflected in the conflict between harmony vs. mastery. Harmony is defined in terms of “fitting into the world as it is, trying to understand and appreciate rather than to change, direct, or to exploit” (Schwartz, 2006, p. 141), whereas mastery comprises values such as daring, being successful, ambitious, and capable. Over the past two decades, Schwartz found support for his theory on cultural values in analysing teacher and student samples from 73 countries (Schwartz, 2006).
Theoretical model of Schwartz's personal values (Schwartz, 1992, printed with permission).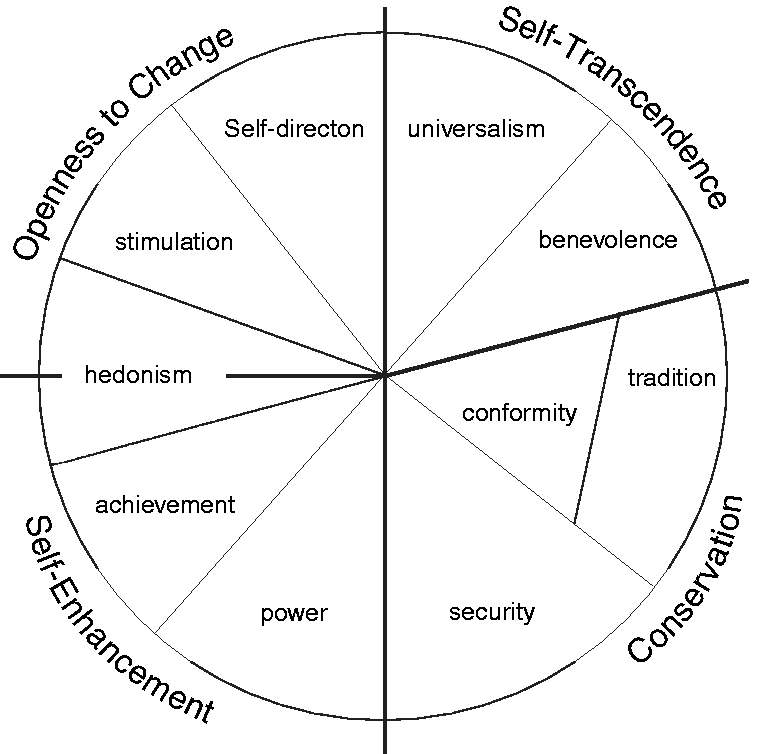
Categorizations of Schwartz's individual values.
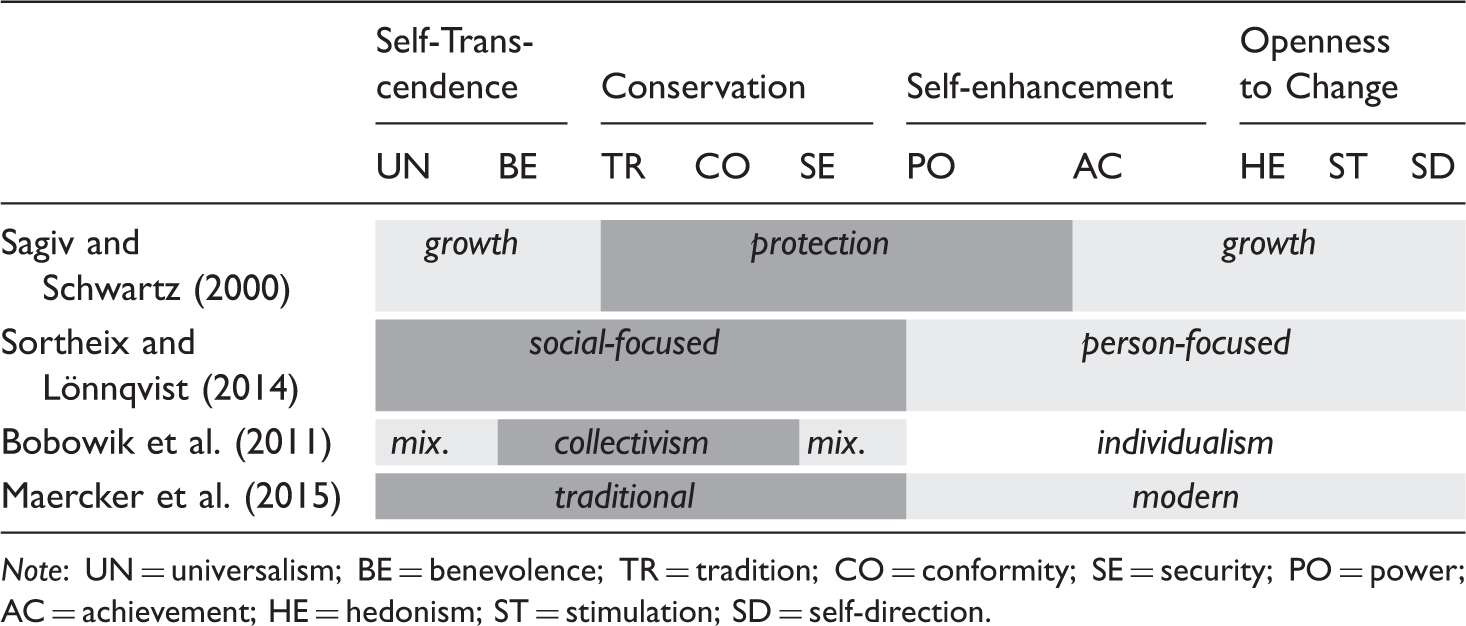
Note: UN = universalism; BE = benevolence; TR = tradition; CO = conformity; SE = security; PO = power; AC = achievement; HE = hedonism; ST = stimulation; SD = self-direction.
Although the different classifications of values were done based on very different theoretical backgrounds and assumptions, they seem to overlap to a large extent. This is not surprising, given Schwartz's conceptualisation of a circular structure, in which adjacent values are more similar than opposed values. It seems that for examining the relationship between values and mental health, looking separately at ten values seems overly complex, and most researchers saw the need for reducing this complexity.
Culture, Values and Mental Illness
In cultural clinical psychology, two traditional approaches of etic and emic research (Berry, 1989) have delivered different kinds of insights which complement each other: The WMHS are etic in nature because they used the same diagnostic categories and algorithms across cultures. Differences in prevalence rates were analysed using the same, cross-culturally applicable variables, such as income or education. On the other hand, emic research has brought forward very rich and diverse descriptions of how cultural factors relate to the phenomenology and aetiology of common mental disorders among very specific cultural groups, e.g. Cambodian refugees in the US (Hinton, Pich, Marques, Nickerson, & Pollack, 2010), Nepali survivors of trauma (Kohrt & Hruschka, 2010), or people suffering from ataque de nervios in Puerto Rico (Guarnaccia, Lewis-Fernández, & Marano, 2003).
The present review aims to examine to what extent cultural and personal value orientations can be used to bridge existing evidence from etic and emic research on mental disorders. The following example illustrates this assumption: Guarnaccia et al. (2003) describe the syndrome of ataque de nervios among Puerto Rican people, which is characterised by acute emotionality (e.g. fear, rage, or grief), combined with a felt loss of control. Affected people often describe their struggling with overwhelming emotions prior to releasing the accumulated tension. Lewis-Fernández and Aggarwal (2015) refer to the Cuban literary critic Benítez-Rojo (1992) to explain this phenomenon against the historical background in Puerto Rico and the Caribbean region in general, which was characterised by tremendous structural violence created by genocide, slavery, and colonial despotism. Emic research indicates the centrality of being controlled and ‘in equanimity’ in Caribbean societies, in order to preserve social harmony. Even in extraordinary situations, it is vital that people remain within the appropriate cultural bounds of emotional expression. Strong emotions are considered as dangerous, and Caribbean people have tended to adopt a non-confrontational stance in order to cope with strong emotions.
What the authors describe here is the process of a cultural value (i.e. social harmony) being developed as a response to historical challenges, and a psychiatric syndrome which relates to this particular cultural value. Thus, a very detailed and thorough understanding of a particular context has elucidated how a particular cultural value affects both the aetiology and phenomenology of a psychiatric syndrome. However, the same cultural value (social harmony) can be found in a completely different context, e.g., China. Zhai and Qu (2001) found in a survey study that, despite far-reaching social and economic change in China, guanxi (interpersonal relations) and he xie (harmony) remained the core value orientations throughout Chinese history until the present. One further important aspect is the cultural value of mianzi (one's face) in order to preserve social harmony. These cultural values relate directly to how mental disorders are perceived and expressed in China. Yang, Kleinman, Link, Phelan, Lee, Good (2007) describe the far-reaching consequences of losing one's face due to mental illness in China, which affects not only the individual person affected by a mental disorder, but the entire family. Having a mental illness “threatens to break the vital connections (‘quanxi wang’) that link the person to a social network of support, resources, and life chances” (p. 1529). As a consequence, depression is expressed through somatic rather than psychological symptoms in China (Ryder, Yang, Zhu, Yao, Yi, Heine, & Bagby, 2008), which might explain the low prevalence rates of ‘conventional’ depressive syndromes found in the WMHS (Kessler & Ustun, 2008).
These examples show that value orientations can be used as descriptive elements which can travel across cultures to examine relationships between culture and mental health. Even if the cultural value of social harmony has developed under very different social and historical conditions in China and Puerto Rico, social harmony as a cultural value might still have similar effects on the phenomenology and aetiology of mental disorders. Cultural value orientations largely describe how a society is organised, how members of a society relate to each other, and to what extent they are encouraged to look after themselves or care for others. Kirmayer and Pedersen (2014) describe how the course and outcome of mental disorders depend “on the reactions, care, and support provided by family members and the immediate social network of community resources” (p. 767). The cultural value of embeddedness, and the personal values of benevolence and universalism, highlight these aspects. Moreover, Pickett and Wilkinson (2010) argued that social inequality affects the quality and sufficiency of social relationships, both of which affect mental health. Cultural values describe the extent to which social inequality is tolerated or even valued in a society, as opposed to culturally valuing social justice and equality.
With regard to personal values, a wealth of evidence exists on their relationship with well-being (Sagiv, Roccas, & Oppenheim, 2015). One line of research draws on self-determination theory (Deci & Ryan, 2000), arguing that ‘healthy values’ satisfy universal psychological needs (e.g., relatedness, autonomy, and competence) and therefore lead to higher well-being across cultures. A different line of research postulates that the fit between personal values and cultural values (Sagiv & Schwartz, 2000), or between personal values and the opportunities and constraints in the environment (Sortheix & Lönnqvist, 2014), are relevant for well-being. The question whether values relate to mental disorders, and not only to well-being, has been examined to a lesser extent. In the following, evidence is summarised from empirical studies on the relationship between Schwartz's personal and cultural value orientations, and common mental disorders, i.e., depression, anxiety disorders, and PTSD.
Methods
Two databases (PsychInfo and Medline) were searched, using publication type (i.e., peer reviewed journal) as a limiter. Databases were searched for articles which referred to the Schwartz values in combination with depression, anxiety disorders, stress, or PTSD. Titles and abstracts were screened, excluding studies which did not cover the topic of interest. Papers with a focus on youth and adolescents were excluded. A total of 13 studies were included: Four studies examined cultural values and nine studies focused on personal values. Some of these studies addressed two mental disorders, i.e., depression and anxiety. Correlations between personal values and mental disorders were compiled. If no correlation matrix was provided in the original article, authors were contacted and asked for their original data. All but one author replied to this request. Due to the very heterogeneous outcomes used in the original studies, no meta-analysis of correlations could be calculated.
Results
Cultural Value Orientations and Mental Disorders
Maercker (2001) analysed data from 11 countries which had been included in both a multi-centre study on cultural values (Schwartz, 1994b) and the WHO Collaborative Study on Psychological Problems in General Health Care (Üstün & Sartorius, 1995), the predecessor of the WMHS. He found a positive correlation between current depression and generalised anxiety disorder, and the cultural values of autonomy, egalitarianism, and harmony. By contrast, a negative correlation emerged for the same mental disorders with embeddedness, hierarchy, and mastery.
These findings were contrasted by two other studies, which both found a negative association between cultural autonomy and depression (Fischer & Boer, 2011; van Hemert, van de Vijver, & Poortinga, 2002), and between cultural autonomy and trait anxiety (Fischer & Boer, 2011). Trait anxiety has proven to be predictive for clinical anxiety disorders in adults (e.g., Mundy, Weber, Rauch, Killgore, Simon, Pollack, & Rosso, 2015). In the study by Fischer and Boer (2011), the association between autonomy and depression, and between autonomy and trait anxiety, was moderated by the cultural context: among the more traditional and collectivistic societies, individualism was associated with negative affect. Among more individualistic European societies, increasing individualism was associated with increasing affective well-being (i.e., less negative affect). This association, however, levelled off towards the extreme ends of individualism. The authors concluded that excessive autonomy may not be beneficial for affective well-being. With regard to trait anxiety, the strength of relationship with individualism differed across nations as well: No relationship between wealth and trait anxiety was found among the poorest societies, but among more wealthy societies, higher average income was associated with less trait anxiety.
In a secondary analysis including 25 countries, Heim, Wegmann, and Maercker (2017) replicated Maercker's (2001) original study by analysing systematic correlations between Schwartz's (1994b) cultural value orientations and prevalence rates compiled by the WMHS (Kessler & Ustun, 2008) and the Global Burden of Disease Study (Whiteford et al., 2013). Only studies with nationally representative samples were included in this study, and prevalence rates of mental disorders were assessed using the World Health Organization Composite International Diagnostic Interview (Wittchen, 1994; World Health Organization, 1990) according to the definitions and criteria of ICD-10 and DSM-IV. In accordance with Maercker (2001), lifetime prevalence of affective disorders was lower in countries with high levels of embeddedness, hierarchy, and mastery, and was higher in countries with high levels of autonomy, egalitarianism, and harmony. With regard to anxiety disorders, the strongest negative correlations were found with hierarchy and mastery, and the strongest positive correlations with egalitarianism, but the correlations were still rather weak.
Personal Value Orientations and Mental Disorders
Study characteristics.
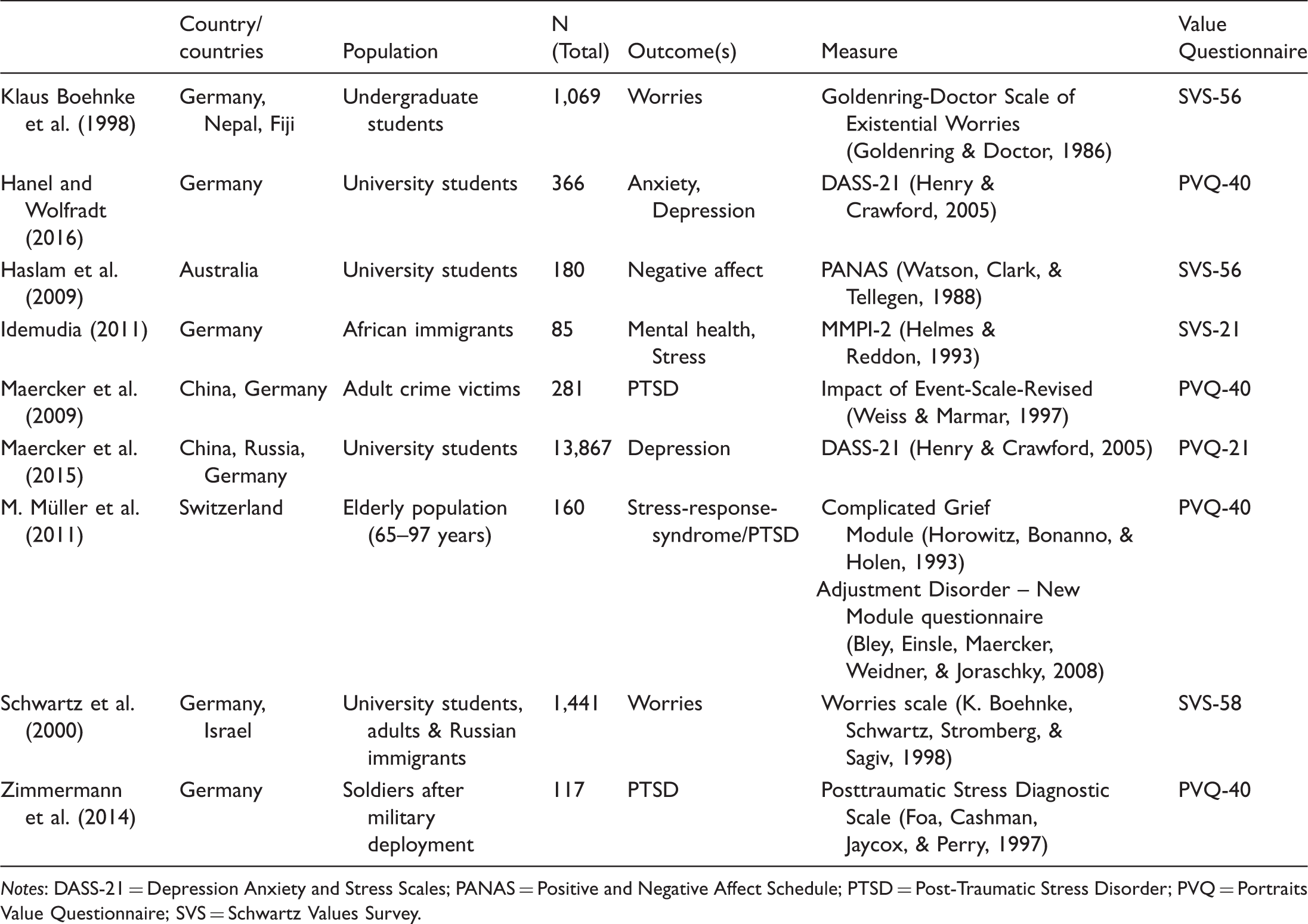
Notes: DASS-21 = Depression Anxiety and Stress Scales; PANAS = Positive and Negative Affect Schedule; PTSD = Post-Traumatic Stress Disorder; PVQ = Portraits Value Questionnaire; SVS = Schwartz Values Survey.
Correlations between personal values and common mental disorders.
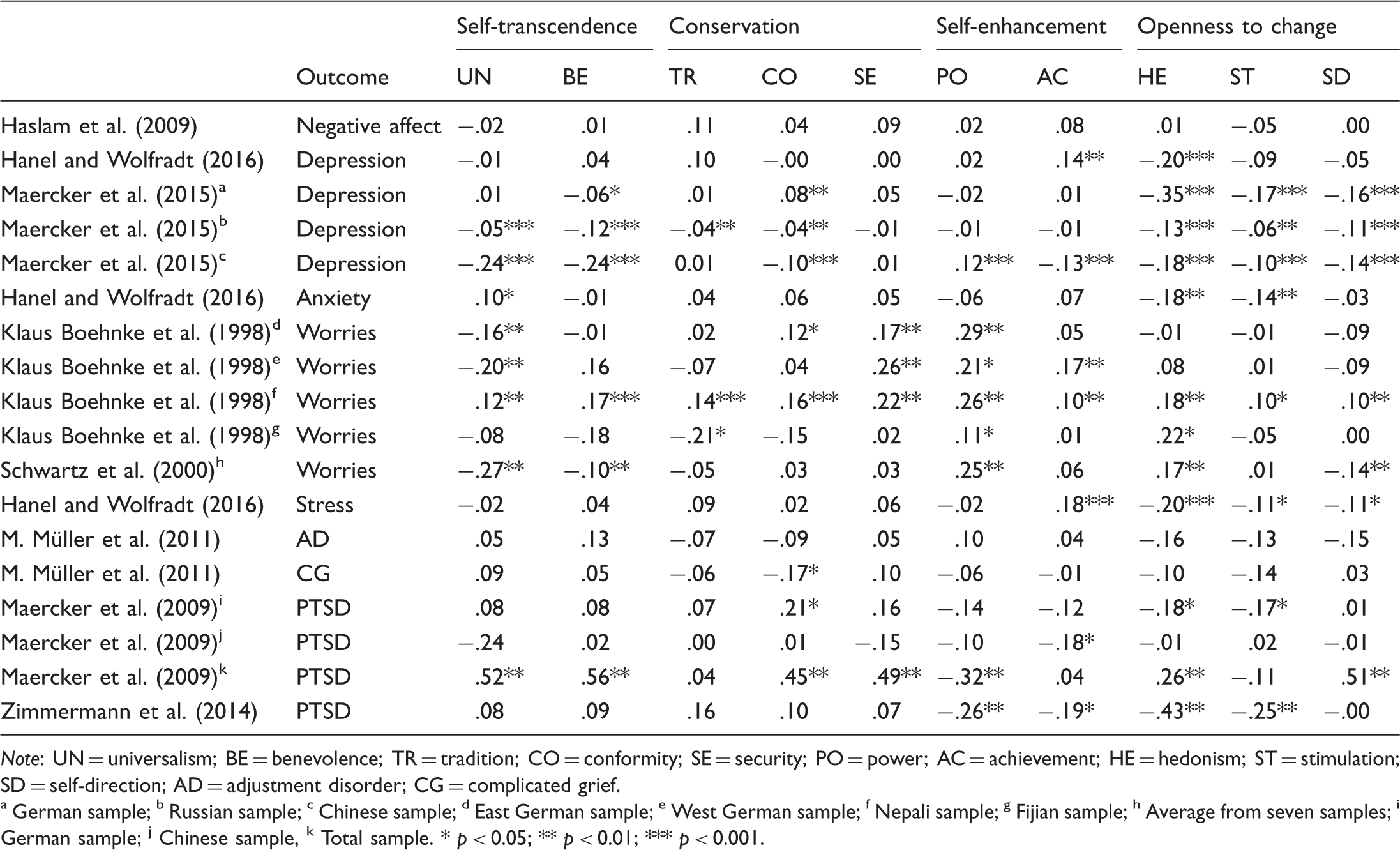
Note: UN = universalism; BE = benevolence; TR = tradition; CO = conformity; SE = security; PO = power; AC = achievement; HE = hedonism; ST = stimulation; SD = self-direction; AD = adjustment disorder; CG = complicated grief. a German sample; b Russian sample; c Chinese sample; d East German sample; e West German sample; f Nepali sample; g Fijian sample; h Average from seven samples; i German sample; j Chinese sample, k Total sample. * p < 0.05; ** p < 0.01; *** p < 0.001.
Depression
Significant correlations between personal values and depression were found in two studies (Hanel & Wolfradt, 2016; Maercker et al., 2015), with somewhat inconsistent results (see Table 3). In general, openness to change values correlated negatively with depression. Correlations with conservation and self-enhancement were low and inconsistent, e.g. achievement correlated positively with depression in a student sample in Germany (Hanel & Wolfradt, 2016), but negatively in a student sample in China (Maercker et al., 2015). And with regard to self-transcendence, significant negative correlations were found in student samples from Russia and China (Maercker et al., 2015), but not in other samples. Haslam, Whelan, and Bastian (2009) found no significant correlations at all.
Anxiety
With regard to anxiety, results were even more inconsistent, with no clear correlation pattern becoming visible. Only one study had looked at anxiety per se (Hanel & Wolfradt, 2016). The other two studies examined how personal values related to worries across multiple samples from several countries (Klaus Boehnke, Stromberg, Regmi, Richmond, & Chandra, 1998; Schwartz, Sagiv, & Boehnke, 2000). The most consistent correlations emerged between worries and power, with considerably high positive correlations across all samples. Moreover, universalism correlated with both anxiety and worries in most samples, but with inconsistent directions (i.e., positively vs. negatively). And most interestingly, the ten values correlated positively with worries only in the Nepali sample.
Stress and PTSD
Few significant correlations were found between values and different measures of stress, such as adjustment disorders and complicated grief symptoms (M. Müller, Forstmeier, Wagner, & Maercker, 2011). In one study including crime victims from Germany and China, Maercker et al. (2009) found relatively weak correlations between values and PTSD in the separate samples, but relatively high and statistically significant correlations in the total sample. The scatterplot of these correlations is displayed in Figure 2. From this figure, it is evident that most German dots are in the top right quadrant, and most Chinese dots are in the bottom left quadrant. Therefore, the correlation becomes stronger and meaningful only when combining the samples.
Scatterplot of the correlation between universalism and PTSD in two separate samples from Germany and China (Maercker et al., 2009, data kindly provided by the first author).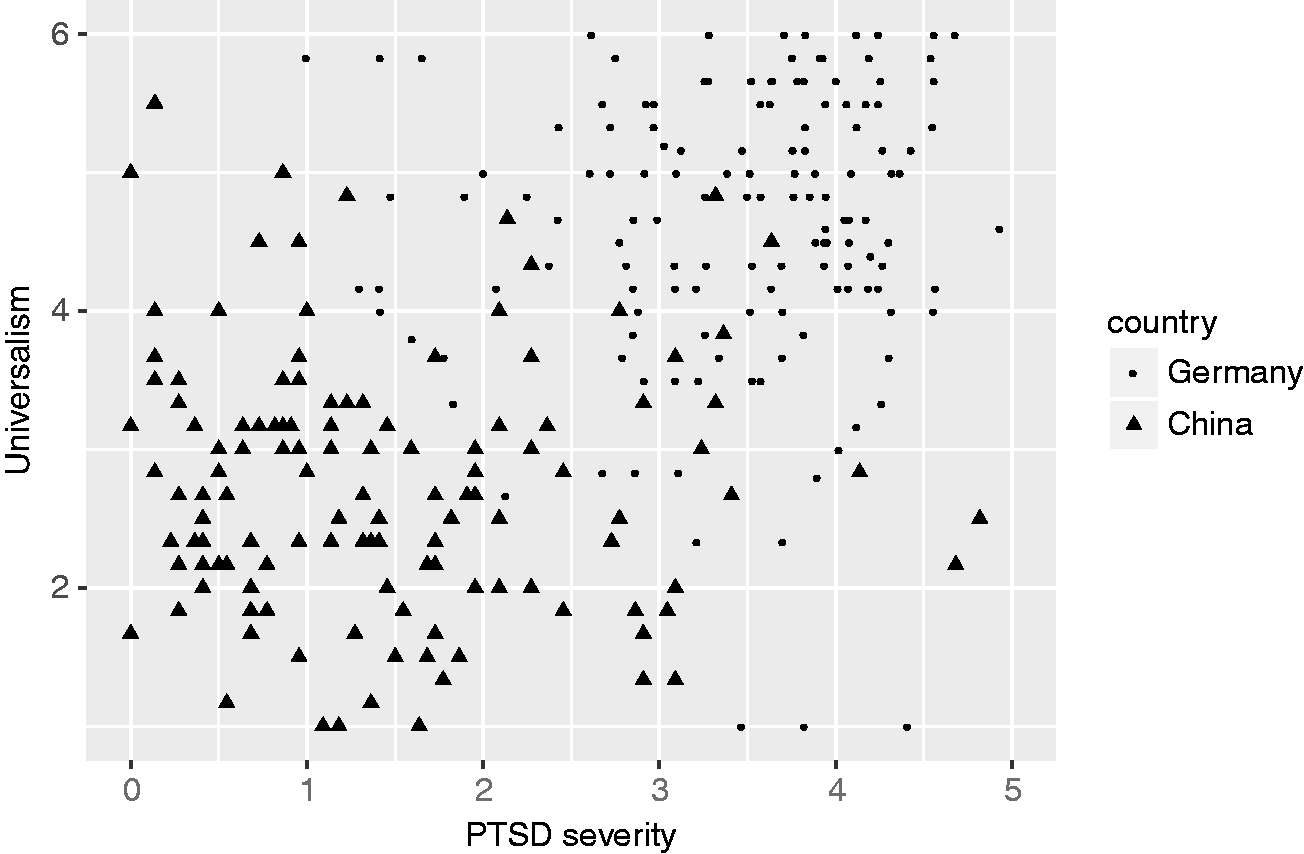
Mediator variables
Several studies looked at indirect paths between values and mental disorders, suggesting a broad range of possible mediating factors. Idemudia (2011) examined personal value orientations, acculturative stress, and mental health among African German immigrants. They found that self-transcendence (i.e., universalism and benevolence) was related to lower acculturative stress and, in consequence, to better mental health, whereas self-enhancement had the opposite effect. The authors did not specify how acculturative stress was defined or measured, which limits the conclusions that can be drawn from this result.
Maercker et al. (2015) used two mediator variables to explain the relationship between personal values and mental health: social support and resilience. In student samples from Germany, China, and Russia, results indicated that traditional values (i.e., benevolence and conformity) predicted social support, whereas self-direction (a modern value) predicted resilience; both mediator variables were associated with positive mental health and lower depression. Zimmermann, Firnkes, Kowalski, Backus, Siegel, Willmund, and Maercker (2014) studied personal value orientations and PTSD among German soldiers after military deployment and used resilience as a mediator variable, as well. In this study, power and hedonism decreased the probability for PTSD, whereas universalism was associated with a higher risk. Resilience partly mediated this relationship.
Maercker et al. (2009) and M. Müller et al. (2011) included social acknowledgement as a victim and disclosure intentions to explain the relationship between traditional and modern values and different stress-related outcomes, such as adjustment disorder, complicated grief, and PTSD in different samples. Acknowledgement as a victim was defined as the degree to which individuals feel validated and supported by their social networks following a loss or traumatic experience. Disclosure is the act of expressing oneself about upsetting experiences. On the one hand, research shows a positive effect of disclosure on well-being (Esterling, L'Abate, Murray, & Pennebaker, 1999), but at the same time, clinical samples showed elevated intentions to disclose (Gidron, Peri, Connolly, & Shalev, 1996).
Both social acknowledgement and disclosure intentions have proven to be relevant in the development of PTSD (Maercker & Müller, 2004; J. Müller, Mörgeli, & Maercker, 2008). Among middle-aged German and Chinese crime victims, disclosure intentions and social acknowledgement mediated the path between traditional values and PTSD (Maercker et al., 2009). In a sample of Swiss elderly people, only disclosure intentions mediated the path between traditional values and stress-response syndromes (i.e., adjustment disorder and complicated grief); social acknowledgement as a victim did not. The authors discussed different possible explanations for these findings. One of them was that it might be easier for elderly people with traditional values to disclose suffering resulting from grief or other stressful life events that would be relatively normal in this phase of life than it would be for middle-aged adults to disclose post-traumatic stress after a crime, which is often related to fear and shame, and thus is more difficult to talk about.
Interaction between the Cultural and Personal Level
The evidence presented above indicates that the relationship between personal values and mental disorders differs across cultures and age groups. Consequently, several authors hypothesised that the cultural and economic context moderated this relationship, a hypothesis that could be partly confirmed (e.g. Sagiv & Schwartz, 2000; Sortheix & Lönnqvist, 2014). A recent study provides further compelling evidence for this assumption: Sortheix and Schwartz (2017) used data from the sixth round of the European Social Survey (25 countries). Six items from the Center for Epidemiological Studies Depression Scale Revised (CESD-R, Radloff, 1977) were included in this survey, as well as a screening test for depression and depressive disorder. The analysis showed that benevolence, self-direction, stimulation, and hedonism were negatively associated with depression, whereas power, security, conformity, and tradition correlated positively. Correlations with universalism and achievement were not significant. More interestingly, the cultural value of egalitarianism moderated the relationship between values and depression: in less egalitarian countries, the (negative) correlation with depression was stronger for self-direction and achievement, whereas the (positive) correlation was stronger for conformity and tradition. No moderation effects were found for the other six values.
The authors proposed a new theoretical approach for explaining these findings. They hypothesised that personal values (and their underlying motivations) interact with the cultural context and might help individuals to compensate for what the larger society or environment fail to provide. In this line of thinking, they argued that in less egalitarian societies, competitive striving is more legitimate, and fewer resources are available, which forces individuals to draw more on their own capacities and resources in order to succeed. Therefore, increased emphasis on achievement and self-direction is more protective in less egalitarian societies than it is in egalitarian societies, whereas conformity and tradition have more negative effects in these countries.
Discussion
This theoretical review compiled evidence on the relationship between cultural and personal value orientations (Schwartz, 1994a, 1994b, 2006) and mental disorders at a societal and individual level. It was suggested that cultural and personal values are useful to delineate the latent concept of ‘culture’, in order to bridge etic and emic research on the relationship between culture and mental disorders.
At the cultural level, four studies were found, and most research focused on the cultural value of autonomy. Fischer and Boer (2011) showed that among individualistic, European countries, higher levels of autonomy were related to lower levels of depression and trait anxiety (Fischer & Boer, 2011). However, in more traditional, collectivistic countries, the inverse pattern was found. A different study, which included representative samples from 25 countries (Heim et al., 2017), found that a high emphasis on embeddedness (i.e., the opposite pole of autonomy on the same value dimension) was associated with lower prevalence rates of depression and anxiety. A possible reason for these inconsistent results could be that Fischer and Boer (2011) relied on symptom scales, whereas prevalence data in Heim et al. (2017) were collected using clinical interviews. Ryder et al. (2008) showed that cross-cultural differences regarding the expression of symptoms depended on the type of symptom assessment (questionnaire vs. clinical interviews).
At the individual level, no consistent correlation pattern became evident across the nine included studies. One explanation for these inconsistent findings relates to the heterogeneous outcome measures that were used in the original studies. Outcomes included depression, anxiety, ‘worries’, adjustment disorder, complicated grief, and PTSD, all of which were measured using different symptom scales. A second explanation might be that the inconsistent findings at the individual level originate from the diversity of cultural groups included in the original studies. It goes without saying that ‘cultural groups’ do not refer to nations, but to subgroups within countries, e.g., to elderly in Germany who lost their partner (M. Müller et al., 2011), or to African immigrants in Germany (Idemudia, 2011). Since the correlation patterns differed across these groups, the universal assumption of some values being ‘healthier’ than others could not be confirmed.
Most studies presented in this review focused on aetiology, i.e., on factors that might foster or hinder the development of psychopathological symptoms. The question of how value orientations are related to the phenomenology of common mental disorders, i.e., how cultural and personal values affect the expression of emotional distress, was discussed to a lesser extent. Ryder et al. (2008) compared the expression of depression among Euro-Canadian and (Han) Chinese patients using both symptom questionnaires and structured clinical interviews. They predicted that the Chinese sample would emphasise somatic symptoms of depression more than the Euro-Canadian sample. The cultural difference with regard to the expression of somatic symptoms was strongest in clinical interviews and disappeared entirely when using symptom scales. Thus, the social context, internalised in a person's value orientations (Schwartz, 2006), may determine how emotional distress is expressed.
Moreover, all studies included in this review used established, Western instruments for measuring common mental disorders. None of the included studies looked at the relationship between value orientations and ‘cultural concepts of distress’ (CCD, Kohrt et al., 2014). Similar CCDs can be found in different cultures, e.g. tutal piensamientuwan (an excess of worrying thoughts) in rural Peru (Pedersen, Kienzler, & Gamarra, 2010) and kufungisisa (thinking too much) in Zimbabwe (Abas & Broadhead, 1997). One future line of research may look at whether and how value orientations are related to such culturally specific expressions of emotional distress. Using more culturally-sensitive measures of mental distress may reveal more meaningful patterns of relationships with value orientations. If such systematic relationships can be revealed, important implications could be derived for the cultural adaptation of psychological interventions.
Conclusion
In summary, the present review showed that Schwartz's value theory (Schwartz, 1994a, 1994b, 2006) may provide a bridging element between cross-national epidemiological research on the one hand, and very detailed descriptions of culturally-specific phenomena on the other hand. However, evidence is limited and contradictory to some extent. Implications for future research emerge from these inconsistencies. Future research should be theory-driven, and should consider Schwartz's explicit theoretical assumptions of cultural and personal values (Schwartz, 1994a, 1994b, 2006). The existing evidence indicates that looking at the mere correlation between personal value orientations and self-reported symptoms of psychopathology in one particular sample does not yield meaningful results. Several studies showed that the patterns of correlation between personal value orientations and mental health become more meaningful when considering the cultural and socio-economic context in which the data were collected (Fischer & Boer, 2011; Maercker et al., 2009; Sortheix & Schwartz, 2017). Moreover, most studies made aetiological assumptions about the relationship between values and mental disorders, but the question of how value orientations relate to the phenomenology of mental distress remains unanswered. And finally, most studies used Western measures of mental distress, which might have limited validity in diverse cultural contexts.
If future research can be streamlined, the picture of how specific cultural patterns are related with the prevalence and expression of mental distress might be complemented, with important implications for clinical practice. A better understanding of how value orientations relate to mental health in diverse contexts will hopefully allow for more culturally-sensitive interventions in order to alleviate the burden of mental diseases worldwide.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.