
Abstract
While food insecurity and poverty worsen mental health outcomes among people living with HIV/AIDS (PLHIV), few intervention studies have targeted poverty and food insecurity as a way to improve mental health. Among HIV-positive patients, addressing such upstream determinants may prove crucial to ensure better mental health and HIV clinical outcomes. We integrated longitudinal, qualitative research into a randomized trial of a livelihood intervention to understand processes and mechanisms for how the intervention may affect mental health among HIV-infected Kenyan adults. In-depth interviews were conducted with intervention participants (n = 45) and control participants (n = 9) at two time-points (after intervention start and upon intervention end). Interviews (n = 85) were translated, double-coded, and analyzed thematically using an inductive-deductive team approach. Participants reported numerous mental health improvements post-intervention including reduced stress, fewer symptoms of anxiety, improved mood, lower depressive symptoms, fewer repetitive and ruminating thoughts, and more hopefulness for the future. Improvements in mental health appear to occur via several mechanisms including: 1) better food security and income; 2) increased physical activity and ability to create fruitful routines around farm work; and, 3) improved sense of self as an active member of the community. Qualitative, longitudinal interviews may help identify intervention mechanisms for improved mental health, but additional research is required to confirm self-reports of mental health changes. These findings suggest that livelihood interventions may improve mental health in multi-faceted ways, and help PLHIV better integrate with their communities.
Introduction
Common mental health disorders, such as anxiety and depression, are important contributors to disability-adjusted life years in resource-constrained countries (Steel et al., 2014). People living with HIV/AIDS (PLHIV), in particular, have a high burden of mental illness, which can worsen both physical and mental health outcomes (Chibanda, Benjamin, Weiss, & Abas, 2014). In sub-Saharan Africa (SSA), pooled analysis suggests that one in three HIV-positive patients exhibit depressive symptomology, and 13-18% report major depression (Nakimuli-Mpungu et al., 2012; Tsai, 2014). Depression among PLHIV, in turn, is associated with higher viral loads (Evans et al., 2002), faster disease progression and mortality (Antelman et al., 2007).
It is well-documented that food insecurity, socio-economic status and financial stress are related to common mental disorders (Lund et al., 2010). In the general population, poverty and food insecurity are associated with worse mental health functioning (Subbaraman et al., 2014). Among HIV-positive patients, longitudinal and cross-sectional studies have highlighted an association between food insecurity and depression in SSA (Hadley & Patil, 2006; Hadley et al., 2008; Tesfaye et al., 2016; Tsai et al., 2012). Household food insecurity is also associated with lower mental health-related quality of life scores among HIV-positive patients in SSA (Palermo, Rawat, Weiser, & Kadiyala, 2013; Tesfaye et al., 2016; Weiser et al., 2012).
Practitioners and scholars increasingly recognize that mental health is unlikely to adequately improve unless structural barriers, such as food insecurity, poverty, and social exclusion are addressed (Burgess, 2015; Kidia et al., 2015; Nakimuli-Mpungu et al., 2014).Theoretically, this aligns with the “social causation” hypothesis, which suggests that poverty underscores mental health outcomes due to the strong links between economic resources and stress, social exclusion, and exposure to other social dynamics such as violence (Flisher et al., 2007; Patel & Kleinman, 2003). A renewed emphasis on poverty being intertwined with mental health is also an extension of the biospychosocial model, which positions mental health within social drivers such as socio-economic status (Hatala, 2012). Given this relationship between poverty and mental health, livelihood programs that aim to improve food insecurity may improve mental health symptoms concurrently. However, in a recent review of mental health interventions for PLHIV, none were focused on structural drivers of mental health (Sikkema et al., 2015). Interventions that focus specifically on nutrition, without structurally addressing livelihoods or food security, have found mixed results. A food basket program in Uganda improved household food security and physical quality of life compared to a matched comparison group receiving otherwise similar HIV care (Rawat, Faust, Maluccio, & Kadiyala, 2014), but made no measureable difference on mental health (Maluccio, Wu, Rokon, Rawat, & Kadiyala, 2016). In South Africa, no differences were noted in general quality of life (a measure comprised of both physical and mental health) between recipients and non-recipients of nutrition support services (Oketch, Paterson, Maunder, & Rollins, 2011).
There have, on the other hand, been an increasing number of studies on economic interventions and their impact on the mental health of non-HIV-infected populations. A systematic review found mixed evidence for the effect of poverty alleviation programs on mental health outcomes (Lund et al., 2011). Since publication of Lund et al.’s review, several additional trials have been completed. In Kenya and Mexico, cash transfers reduced depressive symptoms among participants (Kilburn, Thirumurthy, Halpern, Pettifor, & Handa, 2016; Ozer, Fernald, Weber, Flynn, & VanderWeele, 2011). These quantitative findings align with qualitative research suggesting cash transfers can reduce stress, anxiety and depression in varied populations (Owusu-Addo, Renzaho, & Smith, 2018). However, in Nicaragua and Zambia, women participating in cash transfers had no difference in depressive symptoms or perceived stress (Macours, Schady, & Vakis, 2012).
Microfinance interventions have similarly had mixed impacts on mental health. While several studies suggest that microfinance improves mental health (Becchetti & Conzo, 2010; Mohindra, Haddad, & Narayana, 2008; Pronyk et al., 2008), others show no significant impact or mixed results (Ahmed, 2005; Christy-McMullin, Shobe, & Wills, 2009; Han, Grinstein-Weiss, &Sherraden, 2009; Karlan & Zinman, 2010; Kayser, Lombe, Newransky, Tower, & Raj, 2010; Masud Ahmed & Chowdhury Abbas, 2001). In addition, one RCT suggests declines in mental health following access to microfinance (Fernald, Hamad, Karlan, Ozer, & Zinman, 2008). Some analyses suggest a relationship between microfinance and increased rates of suicide, particularly among men (Ashta, Khan, & Otto, 2015). This literature highlighting the immense stress of loan repayment have led some practitioners to develop refined forms of microfinance, including flexible loan repayment (Field, Pande, Papp, & Park, 2012) and a new emphasis on savings over credit (Ssewamala, Neilands, Waldfogel, & Ismayilova, 2012).
Distinct from cash transfers and microfinance are livelihood interventions, which focus on building skills or capital over time. Few studies to date have rigorously tested through randomized control trials the impact of livelihood interventions on mental health. In one study, women receiving livestock assets in Democratic Republic of Congo had decreased depressive symptoms over time (Glass, Perrin, Kohli, & Remy, 2014). However, it is less clear how and why such livelihood interventions may lead to mental health changes, specifically from the perspective of local communities and stakeholders in which such interventions are embedded (Jain & Orr, 2016). We examined how a multi-sectoral livelihood intervention affected mental health for HIV-positive farmers in Kenya. Using qualitative methodology, we explored participant definitions of mental health, perceived changes in mental health due to the intervention, and mechanisms through which the intervention may have influenced mental health outcomes.
Methods
Setting
The study was conducted in Migori County in the former Nyanza region of Kenya where the vast majority of individuals are food insecure (Kenya National Bureau of Statistics, 2008). This region has the highest HIV prevalence in Kenya, at 15.1% (Kenya National Bureau of Statistics and ICF Macro, 2010), and is a region that has a high burden of depression (Ngui, Khasakhala, Ndetei, & Roberts, 2010). Details of the Shamba Maisha (meaning “farming life” in Kiswahili) study design have been previously described (Cohen et al., 2015). In brief, we conducted a pilot randomized controlled trial in two communities to explore whether Shamba Maisha improved food security and HIV clinical outcomes among farmers.
The two sites selected for this study were chosen based on similarities in clinic size and agricultural characteristics (access to water, size of homesteads). The two sites were randomly assigned to either intervention or control conditions by a biostatistician who was not involved in fieldwork. Participants were recruited through organized meetings held at each health facility and announcements at patient support group sessions. Individuals who expressed interest were screened for eligibility and consented. Inclusion criteria for the trial and hence the current qualitative study included: HIV-infected and receiving ART, ages 18- to 49-years old, having access to farmland and surface water, being moderately or severely food insecure at baseline or malnourished during the year preceding enrollment, and participating in or being willing to join a patient support group. Participants were enrolled starting in August 2012 and followed for one year.
A cross-disciplinary team of experts on agriculture, development and HIV-related health designed the intervention, intended to sustainably improve food insecurity and HIV clinical outcomes (including mental health). The Shamba Maisha intervention was comprised of three components, delivered as a package to intervention participants (Cohen et al., 2015): 1) “Money Maker” Hip Pump, a low-cost micro-irrigation water pump, which enabled farmers to irrigate their crops year-round, avoiding dependence on seasonal rainfall thus capitalizing on higher crop prices in the marketplace; 2) training on sustainable farming practices and financial management delivered to groups of participants in eight didactic and practical demonstration sessions; and 3) loan program of vouchers (worth ∼$150 USD) to purchase the irrigation hip pump, seeds, fertilizers, and other farming implements. Study participants were expected to repay the loan in full by the end of two harvest seasons, but were not required to forfeit personal belongings (other than the hip pump) if they failed to repay the loan. Trainings and loan repayment occurred in the context of patient support groups.
Data collection
We integrated a longitudinal qualitative study into the pilot trial, aiming to unpack the mechanisms behind intervention impacts (Zakaras et al., 2016). The purpose of the current manuscript is to explore the mental health impacts of the intervention. We developed a ‘theory of change’ to explain how livelihoods intervention may work towards improvements in multiple aspects of participant lives, and that improvements in mental health may be on the causal pathway towards improved HIV outcomes (Figure 1). Our goal was to use longitudinal qualitative data to assist with refining the theory of change.
Shamba Maisha intervention theory of change.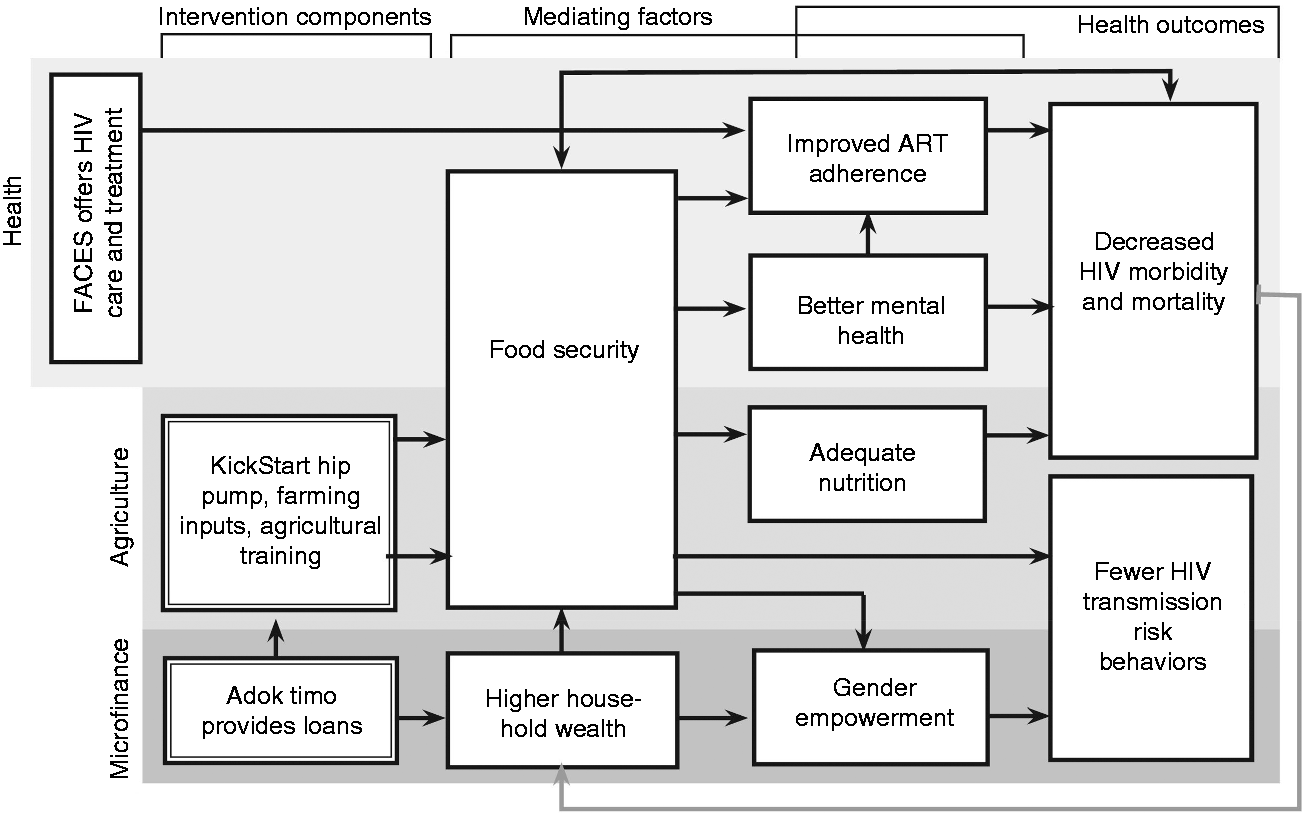
Overall, 85 in-depth interviews were conducted. We interviewed a purposive sample of intervention participants (n = 45) and a subset of control participants (n = 9) with the aim to recruit a wide range of ages, and both male and female participants. Our purpose in interviewing control participants was to ascertain whether the impacts and mechanisms described by intervention participants were related to the intervention or to study participation more broadly. All participants approached for the qualitative sub-study agreed to participate.
A subset of 31 intervention participants were followed longitudinally, with one interview early in the intervention (at 3 to 5 months after enrollment) and a second at intervention end (12 months after the start of the intervention). The longitudinal approach to data collection allowed a better understanding of intervention effects over time. Control participants were interviewed at the intervention end only, or 12 months after enrollment.
Interviews were conducted by four local researchers (two male, and two female) who were fluent in local languages (Dholuo and Kiswahili) and English. Researchers held either bachelor or master's degrees and were trained extensively on qualitative research techniques. This training included interviewing in an exploratory, non-judgmental, non-leading way and probing for rich descriptions of participants' experiences (Bernard, 2006; Patton, 2002). We carried out mock and pilot interviews to standardize techniques within and across interviewers. In addition to undergoing extensive training, study investigators (AMH, SLD, SDW) reviewed early transcripts to provide feedback on interview and probing style.
Each interview took place in a private location of the participants' choosing such as their home or the study office. Interviewers were gender-matched with participants. Interviews lasted between 45 minutes and 2.5 hours and were digitally recorded. Only the researcher and respondent were present during the interviews, and none of the interviewers were previously known to study participants to encourage an unbiased accounting of positive and negative experiences with the intervention. Researchers were hired specifically for qualitative research and were managed separately from the team delivering the Shamba Maisha intervention.
The interview guides at baseline aimed to elicit feedback about particular topics in the daily lives of participants, such as household composition, food, healthcare, partner dynamics, and farming decisions. To explore mental health, participants were asked about whether they had felt down, anxious, or sad and what causes sadness or stress in their lives. Follow-up interviews with the same participants addressed the same set of questions at a new time-point 7-9 months later. Interviewers at follow-up asked about any changes (positive or negative) related to mood, stress, anxiety, or sad emotions, with specific emphasis on asking participants to describe their own views on mental health. Participants were asked whether feelings of stress, sadness or anxiety had changed at all in the previous year. They were also asked to describe the reasons underlying any changes in these feelings.
Data analysis
Interviewers transcribed and translated their own interviews into English. Each transcript was reviewed by a co-investigator to ensure clarity of the translation. This step also served as a training technique, since the co-investigator could identify areas where further probing might be warranted. Individual transcripts were labeled based on the location, age, and gender of the participant. Each transcript was given a pseudonym to ensure anonymity and to link participants from the two interview timepoints.
Data were managed using Dedoose (Sociocultural Research Consultants, 2013), a qualitative software that allows for real-time access to a secured database by a number of people in an analysis team. Several co-authors developed a thematic coding framework based on the topics covered in interview guides. The framework was shared with other co-investigators and data collectors and revised through a series of teleconferences. Once the framework was established, all codes and their definitions were imported into Dedoose to aid a first round of coding. This first round of coding focused on highlighting large chunks of data and placing them within one or more relevant “broad codes”.
Themes and analytical constructs.

Next, the same three researchers wrote analytical reports to describe each fine code alongside illustrative quotes. We selected quotes that were representative of the cohort, with special attention paid to divergent quotes (those in which participants' experiences differ from other participants). Lastly, the analytical reports were re-organized with an aim of generating theoretical constructs that extend the knowledge of the field (Tweed & Charmaz, 2012). All quotes presented here include participant demographics, and where possible, a longitudinal perspective is explored.
Ethical considerations
Informed, written consent was obtained by all participants. Transportation reimbursement was offered up to 800 Kenyan shillings per clinic-based interviews (∼$9.4 USD) and 400 Kenyan shillings for home-based interviews (∼$4.70). Ethics approval was obtained from Kenya Medical Research Institute (SSC #2178) and the University of California San Francisco (CHR #11-07435). This trial is registered at ClinicalTrials.gov (NCT01548599).
Results
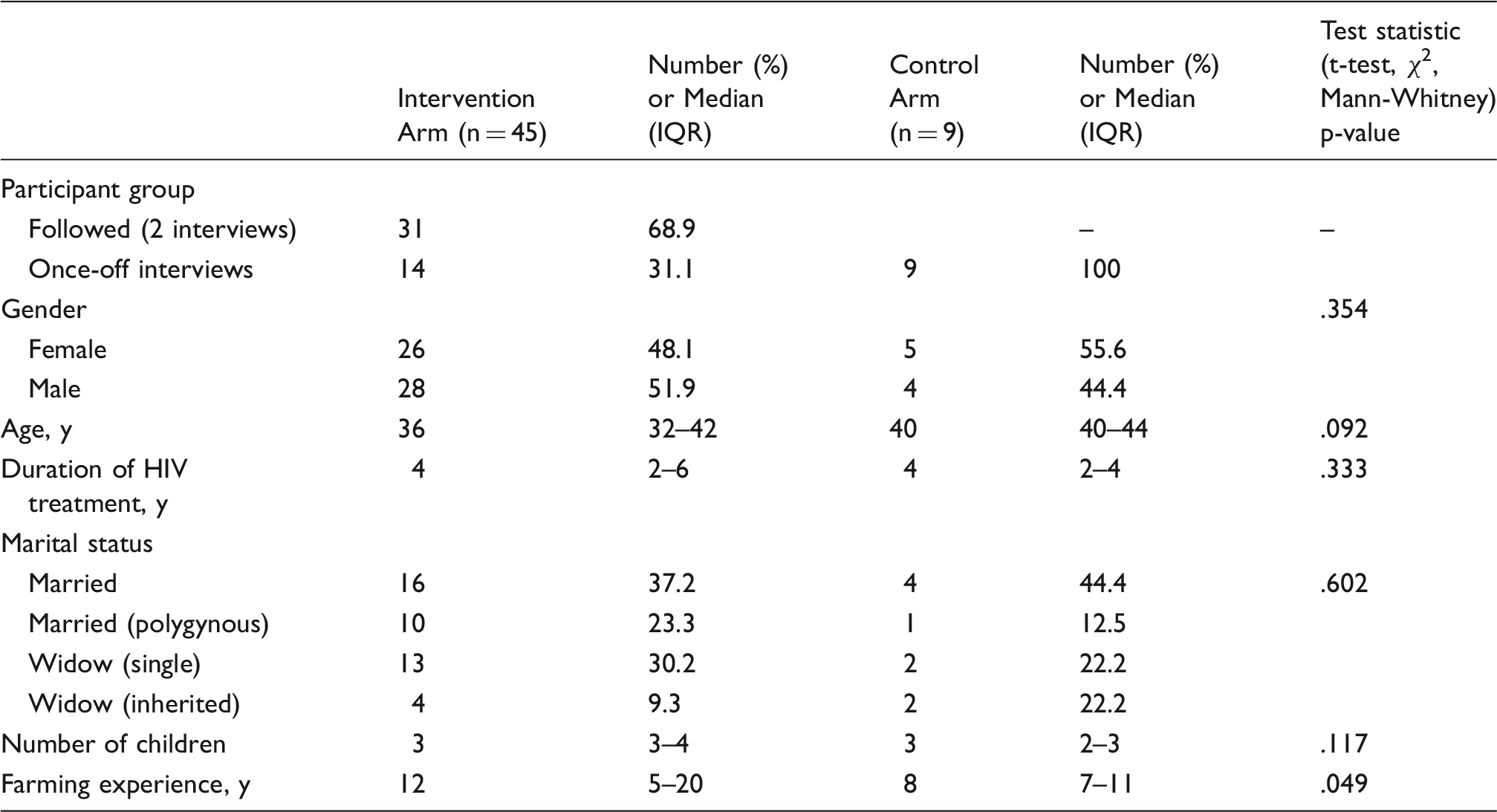
Participant characteristics
Characteristics of participants included in the study (N=54).
Perceived mental health improvements
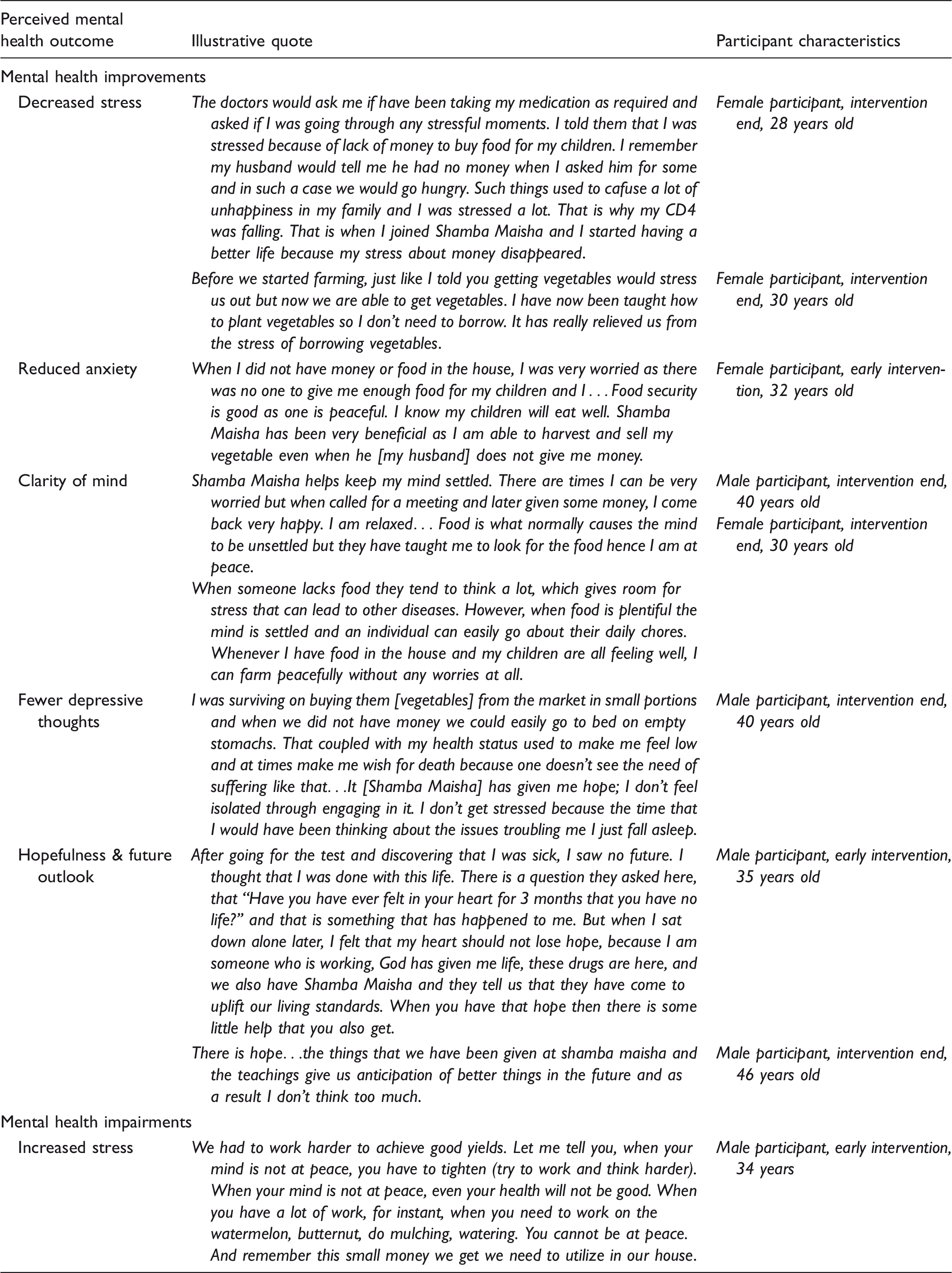
Illustrative quotes of perceived mental health changes after intervention participation.
Participants often reflected that they experienced less stress after taking part in the intervention. Several participants described that the intervention helped raise CD4 counts by decreasing stress levels. A 32-year-old man described his CD4 improving from 640 at the start of the intervention to 1000, a shift that was accompanied by a decrease in viral load. He noted that once he put his “entire mind on work and didn't have any other thoughts,” he was able to “focus all the energy (ketotekoduto)” on other matters such as taking medication on time, eating well, and staying healthy.
Multiple participants illustrated their reduction in anxiety by describing how their mind is “settled” or “clear,” an important way of articulating good mental health in this setting. One 33-year-old man explained that less anxiety around hunger helped him “have a very clear mind (bedokodparo ma liw) [because] I am not worried of sleeping on an empty stomach.” Many participants described fewer symptoms of depression after taking part in the intervention. These shifts in mental health are explored further in the following sections, which explain specific mechanisms around improved mental health.
Mechanisms towards improved mental health
Participants in our study perceived that mental health was altered through several key mechanisms, including: improved food security and ability to provide for family, more productive daily routines (thereby reducing time for and attention to persistent fears), enhanced social standing that accompanied being more active community members. Concerns over repaying loans, however, were a significant perceived negative mental health outcome of the intervention.
Improved food security reduces anxiety and depressive symptoms
Participants described that their feelings of depression and hopelessness related to difficulties accessing food and providing for their families. Hunger itself was seen as a trigger for anxiety, stress, and depression by one 30-year-old woman, who explained that “when one is full they are more rational but when one is hungry they get anxious and stressed, leading to depression.” She further articulated that, “when I do not have food, I think a lot about what I would cook at a certain meal and wonder what to do.”
Participants noted that the intervention decreased stress in the household by improving food availability. A 28-year-old mother explained that she “used to be stressed about how the children were going to eat.” Yet, when the anxiety of finding food was alleviated, she was able to “eat and laugh happily” with her family. Similarly, a 33-year-old man who reported experiencing “having no food” during the early interviews discussed how participation in Shamba Maisha improved his food situation and reduced anxiety: “I am not worried, knowing that we will eat vegetables, so it covers the part where I could have been forced to go look for food.” These examples underscore important gendered aspects of food provision, with women being predominately concerned with putting food on the table, whereas men spoke more about finding work to pay for food.
Several participants described how improved food insecurity positively affected their mental health. One widowed woman who had been inherited by an extended family member explained the reduced worry and sense of calm that arose out of having sufficient food for her three children: I am calmer and happier as I am able to provide enough food for my family. I do not have to worry about what my children will eat at all. Before Shamba Maisha I had to strain to be able to buy omena [small fish] or sugar but Shamba Maisha has now brought a lot of ease because the vegetables can be sold to get money to buy these things. When my partner comes home and finds me happy, he is also happy and everything goes well. (Female participant, intervention end, 38 years old)
In the control site, several participants linked hunger to feeling “low”. In one interview, a man spoke about hunger and “wishing for death” to avoid the suffering of living in poverty and in ill-health: We even sleep hungry, and when we do not have money we could easily go to bed on empty stomachs. That coupled with my health makes me feel low (miyoabedokod) and at times makes me wish for death because one doesn't see the need of suffering like that. (Male participant, control site, 40 years old) Interviewer (I): Tell me how you feel mentally each day. Researcher (R): There are some times that I feel lonely during the day but I have since learned to be reading my bible or listening to the radio so that I keep that feeling away.
I: What brings that feeling?
R: Lack of money to buy food or for accomplishing other plans brings this kind of feeling. I: Share with me about a time when you were stressed. R: Between November and January, I was stressed because I needed school fees for my children and I also had a patient whom I was taking care of. So yes, I have had such an experience and when I went for the routine checkup my CD4 and weight was found to have reduced significantly.
I: How is the situation now?
R: I still experience a little stress.
I: What brought the stress?
R: A lack of food brings that. (Female participant, control community, 46 years) But when the Shamba Maisha came, money for these petty things became available, and these small things may be petty, yes, but they really bring about psychological torture (to gikelochandruok mar paro) which Shamba Maisha has gotten rid of.(Male participant, intervention end, 44 years old)
Productive farming routines reduced depressive and worrisome thoughts
Many participants explained that staying engaged and busy through farming and participation in Shamba Maisha helped reduce stress. A 40-year-old woman described how “something funny about stress is that if you are just seated idle is when it increases, but when you are busy doing something your thoughts are reduced and the stress also goes down.” She went on to say that when feelings of stress overwhelm her, she visits the farm as a way to stay busy and distract herself. Several other participants explained that becoming engaged in farming through Shamba Maisha helped to reduce existential worry about illness and death: After realizing that I had the virus, I worried a lot about what the state of my children would be when I am dead, but with the [Shamba Maisha] teachings, that worry has now reduced. When I first learned of my status, I could think a lot about how I got infected by the disease. I even got worried about the life of my children after my death, which I saw was very near. But I have since changed and when I am going about my duties, I do them without the feeling that I will leave them behind…I just do them well and I feel a lot more free (thuolomang'eny, literally ‘opportunity of time’). (Male participant, intervention end, 43 years)
Multiple participants described increased motivation and enthusiasm in general as they started to be more productive in the farm. One woman said that Shamba Maisha helped her stay organized and productive: I: I have seen a big change as I am more enthusiastic (kendo, literally ‘hope and optimism’) and I feel recharged to farm much better than I used to. Now I concentrate a lot more on my farming.
I: What is the source of your enthusiasm to work?
R: What has brought about this enthusiasm is the way we were trained to farm, yeah. …Sometimes I go to my farm and sing as I work, this helps me reduce the worries and have a good life. I: Tell me more about Shamba Maisha reducing your worries. R:Initially I used to be very idle; I had a lot of time and I would easily get stressed as I thought aimlessly. Shamba Maisha has made me very busy and organized. I have to plan how to do my work to fit in the available time, which has helped me progress, and I really like the life that I am now leading. (Female participant, intervention end, 48 years old) Shamba Maisha has made me very alert. Now I have a plan to cultivate 1000 heads of watermelon. I have onions ready for transplanting in 1 acre, kales in the seedbed, which has got me thinking about its transplantation. My mind is therefore very packed (pachakoroopong) all the time. For me to come here, I was called from the farm. Before I have destructive thoughts; now I think about my crops in the garden. (Male participant, early intervention, 33 years old) The only thing that stresses me a lot is dying. I normally feel that I am an already dead person who is just taking the ARVs to extend my life up to a given time and then I just die. I am mostly disturbed when I am going to bed. (Male participant, control site, 40 years old)
Reframed social identities: Future outlook and self-esteem
Taking part in Shamba Maisha helped participants to be more hopeful about their future. One man explained that his depressive thoughts lifted and he regained hope since participating in Shamba Maisha due to his new ability to work: After going for the [HIV] test and discovering that I was sick, I saw no future. I thought that I was done with this life. There is a question they asked here, that “Have you have ever felt in your heart for 3 months that you have no life?” and that is something that has happened to me. But when I sat down alone later, I felt that my heart should not lose hope, because I am someone who is working, God has given me life…. and we also have Shamba Maisha and they tell us that they have come to uplift our living standards. When you have that hope then there is some little help that you also get. (Male participant, early intervention, 35 years old)
These new livelihood opportunities led to improved feelings of self-efficacy, which were paralleled by positive changes in one's sense of self within the broader community. Intervention participants were viewed by their community as increasingly important, active members of society who were worthy of visiting and conducting business with. The change in participants' economic standing was accompanied by a change in social standing. Several participants echoed a similar theme throughout their narratives about the diminishing distance between them and the community. In this way, individual changes in mental health and self-efficacy were embedded within the social and communal aspects of mental health (e.g. respect, connectedness) that were crucial for research participants in this particular setting.
Repayment of loans was a new source of stress
While participation in the intervention relieved stress and anxiety about food security, income and health more broadly, participation also presented a source of external stress for a few participants. Many spoke about increased stress from experiences with the microfinance loan. Loan repayment was a major concern among participants, who felt that repaying the loan presented a significant economic burden: We were given loans for the farm inputs, and at times you can get a call asking for repayment when you are really financially incapacitated and that stressed me (manonomiyaparruok, literally ‘gave me anxieties’) because I had to think about where and how I would get the money to repay the loans. That has been my source of stress since joining Shamba Maisha. (Male participant, intervention end, 41 years old) It stressed me when I cultivated the seeds that I was given which got destroyed by the hailstorm. I got worried that I was required to repay the loan but I did not have a way to repay it as my crops had been destroyed by the hailstorm. (Female participant, early intervention, 31 years old)
Discussion
Despite recognition that food security is linked to mental health, few structural livelihoods interventions exist to reduce depressive and anxious symptomology. We conducted longitudinal, qualitative research in southwestern Kenya alongside a pilot trial of an agricultural and finance intervention with HIV-positive farmers. Through our qualitative data, we found that participants perceived that their HIV-related health and mental health improved. Participants described several mechanisms through which mental health improvements took place, including: improved food insecurity and income, increased productivity, staying busy, creating fruitful routines around farm work, and shifts in identity that led them to feel as if they were active and engaged members of the community.
Our qualitative findings that increased household food security was an important mechanism towards improved mental health align with previous work from other SSA settings that demonstrated how the precarious and uncertain nature of food security can be directly tied to anxiety and depression (Hadley & Patil, 2008; Hadley et al., 2008; Tsai et al., 2012). Similarly, food insecurity has been shown to be an important contributor towards chronic stress elsewhere (Hadley & Patil, 2008; Maluccio et al., 2016). Our findings extend this work by showing how a livelihood intervention to improve household food security may reduce multiple aspects of mental health including stress, depressive symptoms and anxiety, and improve mood and hopefulness for the future. This qualitative study provides the foundation for future hypothesis-testing research by identifying the key pathways linking livelihood interventions on food insecurity towards improved mental health.
Other important mechanisms were that the livelihood intervention improved mental health when participants stayed engaged and productive through farming work, and also because the intervention helped to both restore a sense of purpose and improve their interconnectedness to others. Previous research has shown that lack of purpose in society is a driver of poor mental health among HIV-infected individuals (Litwinczuk & Groh, 2007; Lyon & Younger, 2001). This finding is supported by other studies that have shown that economic interventions help participants regain morale and vision for the future (Christy-McMullin et al., 2009; Holmes, Winskell, Hennink, & Chidiac, 2011; Karlan & Zinman, 2010). A crucial extension of this previous economic research is the way that this livelihoods intervention linked participants back to a social position of being productive, active, and healthy. In many SSA settings, the construct of mental health is deeply embedded in the social connections of a community (Kpanake, 2018), so influencing mental health necessarily requires altering an individual's interconnectedness to others.
Two other mechanisms from previous qualitative studies on the Shamba Maisha intervention are worth noting, though they are not explored in-depth here. Qualitative findings suggest that the intervention had a positive influence on gender-related power dynamics and enhanced relationship quality (Zakaras et al., 2016), all factors that may, in turn, alter the mental health of participants. Certainly, other economic interventions have seen reductions in partner conflict and domestic violence alongside decreases in psychological distress (Haushofer & Shapiro, 2016). Also, the intervention showed qualitative evidence of decreased HIV-related stigma (Tsai et al., 2017), which has similar close ties to mental health.
As Shamba Maisha may have improved mental health through a number of mechanisms, above and beyond improved food security, this may explain why our results diverge from previous null findings in food supplementation studies (Maluccio et al., 2016; Oketch et al., 2011; Rawat et al., 2014). Targeted food supplementation, while providing critical nutritional support, does not fully ameliorate food insecurity if individuals have ongoing anxiety about their food supply, or feel that it is socially unacceptable to rely on clinic-based or other programs to feed themselves or their families (Byron, Gillespie, & Nangami, 2008; Weiser et al., 2011). Similarly, direct food supplementation does little to help participants find a sense of purpose or develop skills for self-reliance, both of which may be crucial elements to attaining good mental health. For those who are stigmatised and marginalized, as those with food insecurity and HIV often are, livelihood interventions can contribute powerfully to social reintegration and reversal of status loss (Tsai, Bangsberg, & Weiser, 2013)—which may be even more important than short-term gains in food security.
Finally, through the process of carrying out this study, we also identified two local constructs of mental health, an important contribution for mental health research that aims to work transculturally (Kako, Wendorf, Stevens, Ngui, & Otto-Salaj, 2016; Mutumba et al., 2015). First, participants described that the intervention gave them a feeling of “alertness” and helped the “mind be very packed.” Several participants described that in this more positive state of mental health, they found they had little space for destructive or depressive thoughts. A more robust understanding of how participants use a “busy mind” as a coping strategy should be a focus of future work. Participants also described that when the mind is “settled” “clear,”, or “at peace” they are able to make good decisions. This interpretation of mental health aligns with findings from other SSA settings suggesting that HIV-positive patients consider poor mental health to be a state of “thinking too much” (Davies, Schneider, Nyatsanza, & Lund, 2016; Haroz et al., 2016; Kidia et al., 2015). In other studies, financial hardship has been noted as a driver of repetitive, ruminating thought patterns (Kidia et al., 2015; Lund et al., 2011), which is a well-documented symptom of both anxiety and depression (Just & Alloy, 1997; Nolen-Hoeksema, 2000). Participant rumination was decreased, suggesting that one mechanism through which livelihood interventions may influence mental health is by altering poverty, which likely serves as an underlying driver of repetitive, worrying thoughts in this population.
Implications for research, intervention, and policy
Shamba Maisha adds to what is known in SSA about structural means to improve mental health interventions. Future research should explore the mechanisms through which livelihoods can improve mental health in order to refine theory and research in ways that make intervention effects more measurable. In addition to locally developed psychological interventions to target mental health and depression in SSA (Futterman et al., 2010; Kaaya et al., 2013), this research suggests that livelihood programs may be an important avenue to improve mental health. To date, few interventions have sought to improve HIV-related mental health in SSA settings (Collins, Holman, Freeman, & Patel, 2006; Sherr, Clucas, Harding, Sibley, & Catalan, 2011). A systematic review of cognitive behavioral interventions for common mental disorders within HIV-positive populations found no extant literature from SSA (Spies, Asmal, & Seedat, 2013). Since that time, group interpersonal therapy interventions have had mixed success in improving mental health in SSA settings. Interventions in Uganda and South Africa demonstrated significant decreases in depression among HIV-positive patients (Nakimuli-Mpungu et al., 2015; Petersen, Hanass Hancock, Bhana, & Govender, 2014). Yet, two other studies of group-based therapy showed no significant changes in depression among HIV-infected women (Kaaya et al., 2013; Mundell et al., 2011).
These pilot studies also highlight practical and theoretical challenges that may hinder wider scale-up. Evidence-based interventions are often designed to be delivered by skilled mental health practitioners (Mundell et al., 2011; Nakimuli-Mpungu et al., 2015). In SSA, where a single mental health professional serves roughly 70,000 people (WHO, 2015), such models may face feasibility constraints. Communities themselves may be unwilling to support ‘talking’ treatments if these approaches are unfamiliar or misaligned with social norms in the setting (Patel, Chowdhary, Rahman, & Verdeli, 2011). Retention within interventions that require multiple sessions is a challenge in settings where patients must weigh the value of clinic visits against other activities, such as income generation (Mundell et al., 2011; Patel et al., 2011; Petersen et al., 2014).Thus, the very therapies that are deemed efficacious for HIV-positive populations in resource-rich settings (Safren et al., 2009) may be infeasible to deliver in SSA settings. It is possible that group-based interventions could have a better acceptability than traditional individual mental health therapies. The group-based nature of livelihood interventions among HIV-positive patients bring benefits associated with pooling resources, providing peer social support, and instrumental support around health (Roopnaraine, Rawat, Babirye, Ochai, & Kadiyala, 2012).
There are important considerations for financial interventions and their potential to increase stress among participants. We learned from a few intervention participants that loan repayment was a source of increased stress. Others have noted that microfinance may be a stress-inducing intervention, since it asks clients to repay loans on a rigid timetable (Fernald et al., 2008). Multiple studies have shown null effects for financial interventions on mental health (Ahmed, 2005; Christy-McMullin et al., 2009; Han et al., 2009; Karlan & Zinman, 2010; Kayser et al., 2010; Masud Ahmed & Chowdhury Abbas, 2001), perhaps in part because stress-relieving aspects of increased cash flow are outweighed by the anxiety of repaying a loan. That Shamba Maisha included a microfinance program that did not require collateral for those unable to repay the loan may be a key differentiator for its impact on mental health. Moreover, Shamba Maisha offered additional agricultural training compared to other models that have been linked to mental health declines (Ashta et al., 2015; Fernald et al., 2008). It is plausible that accessing land, participating in agricultural training, growing crops, and receiving a loan to produce income was better for mental health than simply income alone.
Limitations
There were several important limitations to our study. Qualitative data can help interpret mechanisms but these data are inappropriate for determining the impact of the intervention on mental health outcomes. We did conduct this qualitative data alongside a pilot randomized control trial, but the pilot trial was not adequately powered to examine differences in mental health between the intervention and control arms. In the future, longitudinal, qualitative research should be paired with a larger randomized control trial to determine whether mental health shifts were a measurable result of the intervention. It is possible that the qualitative interview format inflated the perceived impact of the program, for example if questions were presented in a leading way. We aimed to mitigate this limitation by training researchers to ask open-ended questions and by using longitudinal data to confirm shifts in participant responses over time. Social desirability bias may have influenced the data if participants perceived that the qualitative researchers were a part of the intervention team or if participants believed that providing favorable responses would create opportunities to gain material benefit. To minimize this bias, we hired local researchers who were not involved in intervention delivery or any other aspect of the study, and assured participants that their responses would not be shared with other members of the study team. Nevertheless, it can be challenging for participants to distinguish between intervention staff and external research teams, so the potential bias for conducting qualitative interviews within an intervention cannot be completely eliminated.
Conclusion
Despite a growing consensus that food insecurity leads to worsened mental health among PLHIV, the existing literature provides little knowledge about how best to remedy this vicious cycle in practice. Our data support the hypothesis that livelihood interventions may provide an important strategy for improving mental health in SSA settings by addressing the structural and social drivers of mental health, including poverty and food security, work productivity, social connectedness and hope.
Footnotes
Acknowledgments
We gratefully acknowledge the important support of the Kenyan Medical Research Institute (KEMRI) and Family AIDS Care & Educational Services (FACES). We also thank the women and men who generously gave their time to participate in the study. We gratefully acknowledge the Director of KEMRI and the Director of KEMRI’s Centre for Microbiology for their support in conducting this research. We also thank the Kevin Kadede, Priscah Owato, Pamela Kimwele, Gina Clark, Kyle Pusateri, and Nandy Nittur for their important contributions to this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by National Institute of Mental Health (grant R34MH094215). Additional funding was provided by the World Food Programme and the Burke Family foundation. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.