
Abstract
Causal attributions of mental illness have received substantial attention given their influence on help-seeking patterns of individuals and the level of engagement with health services. Few studies, however, have examined caregivers’ perspectives of their relatives’ illness. The current study aimed to examine caregivers’ causal attributions of their relatives’ mental illness and its association with perceived stigma in a multi-ethnic Asian sample. Primary caregivers (N = 350) of psychiatric outpatients were recruited from a psychiatric hospital. The attribution and stigma sections of the Family Interview Schedule (FIS) were utilized to obtain caregivers’ causal report of their relatives’ illness and stigma perception. Logistic regressions were performed to examine the socio-demographic and diagnostic correlates of the four categories of causal attributions (psychosocial, biological, drug-/substance use-related, supernatural). The majority of caregivers identified psychosocial causes, followed by biological, supernatural, and lastly drug-/substance use-related causes for their relatives’ illness. Marital status, religion, employment status and the diagnosis of depressive disorders were significant correlates of biological attributions. Ethnicity and not knowing their relatives' diagnosis were significantly associated with psychosocial attributions. For drug-/substance use-related attributions, ethnicity was the only significant correlate. Supernatural attributions did not yield any significant associations. Caregivers who endorsed drug-/substance use-related reasons also reported significantly higher stigma than caregivers who did not endorse these attributions. A tendency to endorse biological and psychosocial causes for their relative’s illness was noted among caregivers. Further research on caregivers’ causal attributions is warranted to account for and replicate current study findings.
Introduction
Extensive research has explored the causal attributions that individuals associate with their illness. According to Ajzen and Fishbein's (1977) theory of reasoned action, understanding the attitude and beliefs that caregivers and individuals have with regard to the cause of a mental illness is important given that this will likely influence their decision to seek out specific health care services for their condition (i.e., help-seeking patterns). Furthermore, aligning patients' causal attributions of their illness with those of the service providers' is important as the level of congruence between patients' and health professionals' explanatory models of illness is likely to affect their engagement rates with mental health services (Arthur & Whitley, 2015; Elkin et al., 1999; Saravanan et al., 2007) and their compliance with treatment (Elliott, Maitoza, & Schwinger, 2011).
Qualitative and quantitative studies to identify the causal explanations of illness have been predominantly conducted among the public and patient populations and less so among caregivers (e.g., Arthur & Whitley, 2015; Polenick & Martire, 2013; Yang et al., 2015). Clarke and Couchman (2012), for instance, found caregivers of youths with psychosis frequently endorsed biological and substance use factors as well as psychological and stress-related factors, whereas Esterberg and Compton (2006) found family members of African Americans hospitalized with schizophrenia primarily endorsed biological causes (e.g., disturbance of brain chemistry, heredity, drug or alcohol abuse, brain infection). Hinton, Franz, Yeo, and Levkoff (2005) on the other hand, found 54% of caregivers of dementia patients from four ethnic groups (African-American, Anglo European-American, Asian-American, Latino) to hold mixed explanatory models; with many attributing Alzheimer's disease and related dementias to normal aging or psychosocial stress.
With regard to studies conducted in an Asian context, Yang and Wonpat-Borja (2012) found general social causes (i.e., common environmental factors such as stress, and work pressure) to be the most frequently endorsed beliefs among relatives of Chinese immigrants with psychosis, followed by indigenous Chinese beliefs (e.g., narrow-mindedness, mystical causes, effect of past lives) and physical/biological causes (e.g., brain-related disorder, physical problem, infectious disease). Likewise, Phillips, Li, Stroup, and Xin (2000) found 84% of Chinese relatives to endorse social, interpersonal, and psychological explanations (e.g., conflict in non-family relationships and stress) as causes of schizophrenia with less than 12% endorsing physical/biological and spiritual factors.
Beliefs about the causes of mental illness have been found to be influenced by various socio-demographic characteristics including educational qualifications, age, ethnicity and culture (Adewuya & Makanjuola, 2008; Arthur & Whitley, 2015; Bignall, Jacquez, & Vaughn, 2015; Caplan et al., 2011). Higher education has generally been associated with a higher endorsement of biological and psychosocial causes (Adewuya & Makanjuola, 2008; Caplan et al., 2011; Saravanan et al., 2007), while older age has been linked to a greater tendency to endorse supernatural factors (Adewuya & Makanjuola, 2008). Cultural and ethnic differences have also been noted in the endorsement of causal attributions (e.g., Angermeyer & Matschinger, 2005). Karasz, Garcia, and Ferri (2009) found African Americans and Hispanic Americans to be less likely than European Americans to endorse a “biopsychiatric” model of depression (e.g., chemical imbalance, personality characteristics) and more likely to view their depression as originating from psychosocial causes (i.e., social and financial challenges). A similar finding was noted by Furnham and Chan (2004) who found Chinese participants to be more likely than British participants to endorse the sociological explanatory model (i.e., external or societal problems) as compared to the biological model. Bignall et al. (2015), on the other hand, found ethnic minorities (e.g., Hispanics, Asian Americans) to consistently endorse spirituality and normalization causes as opposed to White participants; compared to 11% of Hispanics who endorsed spiritual reasons for mental illness, only 3% of Whites endorsed these. In contrast, Yang et al. (2015) found no significant association between caregiver characteristics (age, gender, education), patient characteristics (marital and employment status) and causal beliefs of psychiatric illness among Chinese immigrant relatives.
Causal beliefs concerning mental illness and its association with stigma have received considerable attention over the years (Bignall et al., 2015; Karasz et al., 2009). Stigma associated with mental illness not only leads to discrimination and rejection but also presents a potential problem for rehabilitation and reintegration of people with mental illness back into society (Charles, Manoranjitham, & Jacob, 2007). While some studies have shown biological models to increase tolerance (i.e., less stigma) towards those with mental illness by reducing ascriptions of responsibility and blame towards the person (e.g., Phelan & Link, 2004), others have found biological causes to contribute to perceptions of unpredictability and dangerousness which in turn results in stronger rejection of those with mental illness (Angermeyer, Holzinger, Carta, & Schomerus, 2011; Arthur & Whitley, 2015; Pescosolido et al., 2010; Read & Law, 1999; Walker & Read, 2002). Whereas the aforementioned studies have mainly focused on public stigma (i.e., public opinions of individuals with mental illness), stigma experienced by family caregivers of individuals with mental illness has received less attention. This form of stigma, also known as affiliate or associative stigma, has been suggested to have an effect on the distress and burden perceived by caregivers (e.g., Mak & Cheung, 2012). Mak and Cheung (2012), for instance, found Chinese caregivers of family members with schizophrenia, bipolar disorder, and major depressive disorder who had a greater concern about “saving face” to have a higher tendency to internalize stigma (i.e., affiliate stigma), which in turn was associated with greater caregiver distress and subjective burden. While concern about “saving face” remained significantly related to caregiver distress even after the inclusion of affiliate stigma (i.e., partial mediation), it was no longer significantly related to subjective burden once affiliate stigma was entered into the equation (i.e., full mediation) (Mak & Cheung, 2012). Chang, Yen, Jang, Su, and Lin (2017), on the other hand, found affiliate stigma to vary depending on diagnosis for Taiwanese caregivers of relatives with schizophrenia expressing a higher level of affiliate stigma than those with depressive disorders.
Given that existing studies have focused extensively on explanatory models of illness among the clinical and general population, and have been conducted primarily in a Western context, it is unclear how these findings would translate to a multi-ethnic Asian society in which family bonding and filial piety play a central role (Chien & Chan, 2004). In view of the aforementioned gaps in the literature, the current study sought to explore the causal beliefs about mental illness among caregivers in a multi-ethnic Asian sample. In particular, the aims of the study were two-fold: 1) to examine the socio-demographic correlates of caregivers’ causal beliefs of their relatives’ mental illness (early psychosis, chronic schizophrenia, depressive disorder, anxiety disorder, dementia) and 2) to examine the association between caregivers’ causal beliefs and stigma.
Methods
Setting and sample
Singapore is a multi-ethnic country in Southeast Asia with a population of 5.6 million; Chinese constitute 74.3% of the resident population, followed by the Malays (13.4%), Indians (9.1%), and Other ethnic groups (3.2%) (Singstat, 2016). The care of people with mental illness in Singapore rests primarily on the specialized mental health services in both public and private sectors (Chong, Abdin, Vaingankar, Kwok, & Subramaniam, 2012).
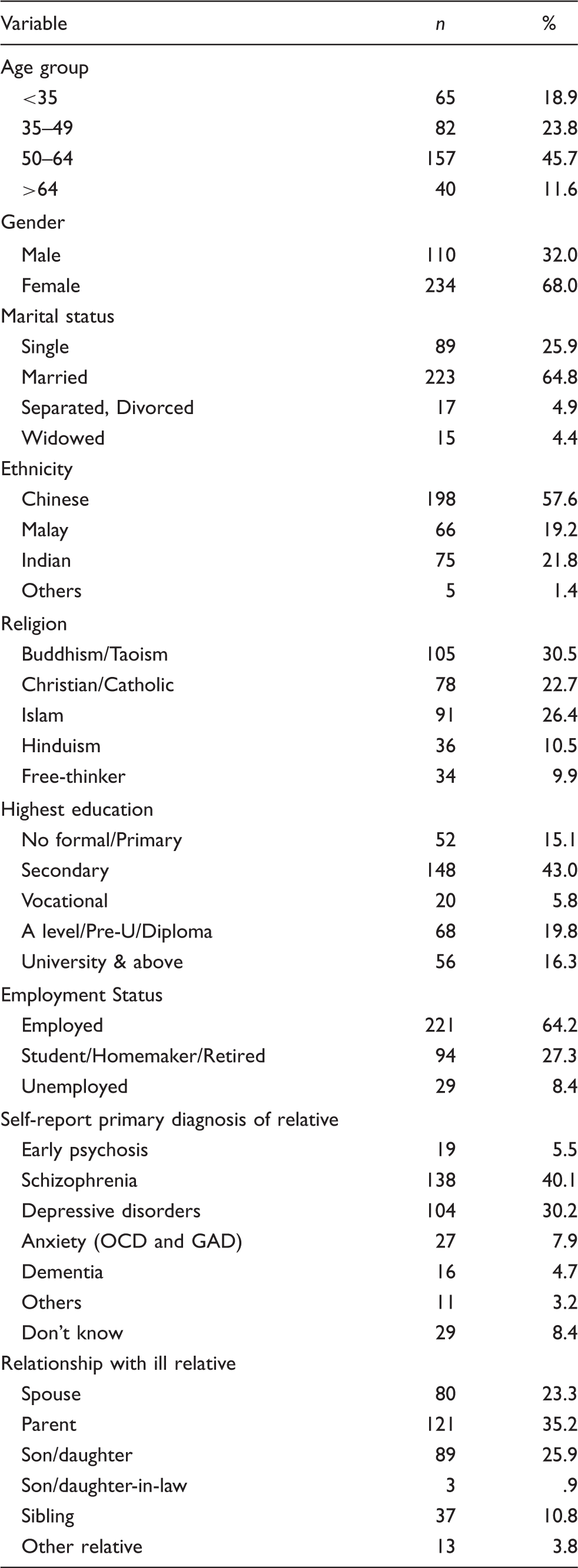
Caregiver characteristics of study sample (n = 344).
Procedure
Caregivers accompanying their ill relatives were approached at the clinic by trained research assistants. Caregivers were eligible for the study if: 1) they were a Singapore Citizen or a Permanent Resident, 2) aged 21 years and above, 3) able to read and comprehend English, Chinese, Malay or Tamil, and 4) were primary caregivers of patients with mental illnesses such as early psychosis (first episode psychosis), chronic schizophrenia (those with more than 2 years of illness were considered as having chronic schizophrenia), depressive disorders, anxiety disorders, dementia and unknown mental illness (wherein the caregiver did not know the specific name of the illness). Questionnaires and informed consent forms were translated into the three main languages (Chinese, Malay, and Tamil) by mental health professionals who were well-versed in the respective languages. Written informed consent was obtained from all caregivers in the language that they felt most comfortable speaking. The questionnaire was either self-administered or administered by a trained research assistant as per the preference of the caregiver. Participants were reimbursed for their participation upon completion of the questionnaires. The study was approved by the relevant ethics committee (i.e., National Healthcare Group Domain Specific Review Board).
Measures
Socio-demographic information
Details such as age, gender, marital status, ethnicity, religion, educational qualifications, employment status, relationship with ill relative (i.e., biological versus non-biological), and self-report of ill relatives' primary diagnosis were collected (Table 1).
Family Interview Schedule (FIS)
The FIS was initially developed for use in the World Health Organization (WHO) Long-Term Follow-Up Study of Schizophrenia (Sartorius & Janca, 1996). Only the attribution and stigma scales from the FIS were utilized in the current study.
Causal attributions scale
Caregivers’ causal attributions of their relatives’ illness were obtained by asking caregivers “what the doctors and anyone else involved with (their relative’s care) have told them is the matter with them.” All sources of information including those from traditional healers, priests, social workers, and other service providers were encouraged. The scale lists 11 possible causes for their relatives’ illness excluding a “No explanation” option whereby the informant is unable to identify a specific cause and an “Others” option whereby the caregiver is allowed to state a cause that does not correspond to any of the 11 possible causes provided. Each of the causal explanations was coded 0 = no, 1 = yes, 8 = uncertain based on the caregiver’s report. For the purpose of the current study and in line with past studies (e.g., Arthur & Whitley., 2015), the list of causal attributions was grouped into four main categories: drug-/substance use-related (e.g., drinks too much, smokes too much), biological (e.g., heredity, faulty biological functioning), psychosocial (e.g., faulty nutritional habits, physical effects of environment, intimate interpersonal relationships, family life, character or lifestyle, social environment), and supernatural causes (e.g., bewitchment, spirits, God’s wrath).
As long as participants answered “yes” to any one of the 11 items, they were considered as endorsing that attribution and were regrouped accordingly into one of the four categories (drug-/substance use-related, biological, psychosocial, supernatural causes). Participants were allowed to endorse more than one category of attribution. While the items on the causal attributions scale were conceptually related, the scale items did not necessarily correlate with one another. As such, in accordance with Phillips et al (2000) and Yang et al. (2015), reliability statistics were not calculated for this scale.
Stigma
A list of 14-items was used to assess self-report of stigma among caregivers. Caregivers were asked to indicate the frequency of which they have experienced the list of issues since their relative developed psychiatric problems. An example of an item is “You worried that your neighbors would treat you differently.” Scores for each item ranged from “0 = not at all” to “3 = a lot,” with higher scores indicating greater stigma. Internal consistency for the stigma scale was acceptable (Cronbach’s alpha = .798).
Data analysis
Analysis in this study was performed using Statistical Package for Social Sciences (SPSS) version 21 software. Descriptive statistics were used to obtain the frequency distribution of the study sample. ANOVA was used to examine the relationship between stigma and the four categories of causal attributions. Four logistic regressions with each category of causal attribution as the outcome variable were performed to examine the socio-demographic (age, gender, ethnicity, marital status, religion, employment status, education level, relationship with ill relative) and diagnostic correlates (early psychosis, schizophrenia, depressive disorders, anxiety disorders, dementia, do not know, and others). Multicollinearity between the variables was checked for before running the regression analyses. All statistically significant results were reported at p < .05.
Results
Socio-demographic characteristics of the sample
Responses from a total of 344 caregivers were analyzed. Six participants were withdrawn from the study due to failure to complete the questionnaire.
Correlates of causal attributions
Correlates of caregivers’ causal attributions of ill relatives’ mental illness.

p < .05.
Marital status, employment status, religion, and the diagnosis of depressive disorders were found to be significant correlates of biological attributions. Compared to caregivers who were married, those who were divorced/separated were less likely (OR = .080, p = .032) to endorse biological attributions; those who were widowed were more likely (OR = 6.44, p = .011) to report these attributions. Individuals who were economically inactive (students, homemakers, or retired) were less likely (OR = .22, p < .001) to endorse biological attributions compared to those who were employed. Compared to caregivers who were Buddhists/Taoists, those who were Christians/Catholics were more likely (OR = 3.43, p = .004) to endorse biological attributions. Caregivers who identified their relative’s diagnosis as “depressive disorders” were also less likely (OR = .19, p = .002) to endorse biological attributions compared to those who did not.
Both ethnicity and diagnosis emerged as significant correlates of psychosocial attributions. Compared to those of Chinese ethnicity, caregivers of “Other” ethnicities were less likely (OR = .037, p = .020) to report psychosocial causes for their relatives' illness. Caregivers who reported not knowing their relatives' diagnosis were also less likely (OR = .15, p = .004) to endorse psychosocial causes. Ethnicity was the only significant correlate for drug-/substance use-related attributions. Caregivers of Indian ethnicity were more likely (OR = 23.19, p = .039) than those of Chinese ethnicity to report drug-/substance use-related causes for their relatives’ illness. No significant correlates were found in relation to supernatural attributions.
Causal attributions and stigma
Caregivers in the current study reported a mean stigma score of 7.35 (SD = 5.74; range: 0–35), with 61% scoring below this value and 39% scoring above this. ANOVA was used to examine the relationship between stigma and the four categories of causal attributions. A significant association was found between stigma and drug-/substance use-related attributions, F(1, 342) = 5.64, p = .018. Caregivers who endorsed drug-/substance use-related reasons reported significantly higher stigma scores (M = 11.36; SD = 8.4) compared to those who did not (M = 7.21, SD = 5.6).
Discussion
The current study examined the socio-demographic and diagnostic correlates of caregivers' causal attributions of their relatives’ mental illness and its association with stigma. A majority of the caregivers identified psychosocial causes followed by biological, supernatural and drug/substance-use related causes for their relatives’ mental illness. This finding was in line with past studies which have found biological (e.g., Clarke & Couchman, 2012) and psychosocial beliefs (e.g., Phillips et al., 2000; Yang & Wonpat-Borja, 2012) to be two of the most commonly reported causes of mental illness among caregivers. This tendency to endorse biological and psychosocial causes has to some extent been linked to an increase in public mental health literacy (e.g., Bartlett et al., 2006; Wang et al., 2013). For instance, Jorm, Christensen, and Griffiths (2005) noted an increase in genetic causal beliefs for both depression and schizophrenia and an increased endorsement of social causes (death of a close relative, childhood problems) for depression among Australians between 1995 and 2003–2004. Likewise, a time trend analysis based on two population surveys (in 1990 and 2001) in Germany found an increased tendency to endorse biological factors for schizophrenia among the general population (Angermeyer & Matschinger, 2005).
In addition, increasing “westernization”/acculturation has also been suggested as a possible reason for this pattern of endorsement. Yang et al. (2015) for instance, found encounters with Western psychiatric treatment and acculturation to influence the causal beliefs of psychiatric illness endorsed by Chinese immigrant relatives. Greater acculturation was shown to be associated with a greater number of causal beliefs endorsed as well as a tendency to incorporate biological/physical causes. Similar results were also observed in studies by Kung (2004) and Clarke and Couchman (2012), who noted a significant increase in caregiver endorsement of biological causes and illicit drug use, respectively, after contact with mental health services. This relationship, however, is likely bi-directional, whereby caregivers with biological and psychosocial attributions could have been more attracted to mental health services due to a match between their beliefs and those of service providers (Kung, 2004). The familiarity of caring for a family member with mental illness has also been shown to correlate with endorsements of biological and psychosocial causal factors with a “lack of personal encounter with the mentally ill” being associated with an increased endorsement of supernatural causes (Adewuya & Makanjuola, 2008, p. 340).
With regard to socio-demographic and diagnostic correlates of caregivers’ causal attributions, those who were economically inactive (students, homemakers, or retired) were less likely to endorse biological attributions compared to those who were employed. A similar result was found in Pang et al.’s (2017) study among the Singapore general population, whereby those who were unemployed (homemaker/student/retired) were less likely to endorse physical factors (i.e., a virus or other infection, an allergy or reaction) compared to those who were employed. It is possible that those who were employed/economically active had more avenues to access information on mental health (e.g., increased socialization, by word-of-mouth, exposure to mental health awareness campaigns) compared to those who were economically inactive, which could have increased their likelihood of endorsing biological causes, given some evidence linking increased mental health literacy with endorsement of these causes (e.g., Bartlett et al., 2006; Jorm et al., 2005; Wang et al., 2013). Caregivers who identified their relatives as having depressive disorders were also less likely to endorse biological attributions. This result was in accordance with studies such as Pilkington, Reavley, and Jorm (2013), who found the Australian general population to be more likely to attribute depression to psychosocial causes (e.g., problems in daily life, the death of closed ones) rather than biological causes (e.g., virus, allergic reaction).
Those who were Christians/Catholics were also more likely to endorse biological attributions compared to those who were Buddhists/Taoists. Compared to those who were married, those who were divorced/separated were less likely to endorse biological attributions, while those who were widowed were more likely to do so. These findings, however, were unique to this study and require further validation.
With regard to psychosocial attributions, caregivers who reported not knowing their relatives’ diagnosis were less likely to endorse this as a cause; those of Chinese ethnicity regardless of knowledge about their relatives’ diagnoses, on the other hand, were more likely to endorse psychosocial causes. This finding was consistent with studies such as Kung (2004), Phillips et al (2000), and Yang and Wonpat-Borja (2012), who found psychosocial explanations to be the most endorsed among those of Chinese ethnicity. This tendency was attributed to the centrality of family in the Chinese culture whereby “familial bond” and support is considered an asset (Kung, 2004) and family conflict is perceived as a potential trigger for mental illness (Kung, 2004). In the current study, association with “psychosocial causes” was examined as a single category rather than individual psychosocial causes (e.g., family conflict, stress), thus generalizability between these studies is limited.
Interestingly, Chinese caregivers were also less likely than caregivers of Indian ethnicity to report drug-/substance use-related causes for their relative's illness. While it is possible that Chinese caregivers may have felt less comfortable in reporting drug/substance use causes, this may indicate a general disposition of accounting for mental illness through psychosocial causes among individuals of Chinese ethnicity as indicated in past studies (e.g., Yang & Wonpat-Borja, 2012). It is also probable that the higher prevalence of alcohol use among the Indian population in Singapore (Subramaniam et al., 2012) could have made this causal factor more salient for this group, in turn resulting in a higher tendency to report this as a possible cause for their relatives’ illness.
Given that only a few studies have examined caregivers’ causal attributions in relation to caregiver characteristics (Polenick & Martire, 2013), more research in this area is warranted to account for and replicate current study findings. Furthermore, there exists some evidence to suggest that caregiver characteristics may be less predictive of the types of causal attributions endorsed when compared to socio-demographic and illness characteristics of patients (Clarke & Couchman, 2012). Nevertheless, studies such as Polenick and Martire (2013) have found caregivers’ relationship with their ill relative to be associated with causal attributions of illness. Spouses of older adults with depression, for instance, were found to be significantly more likely than adult children of patients to make person-centered attributions (e.g., the perception of depression being a result of deficits in motivation, self-discipline). Although these factors (i.e., age, relationship with ill relative) were not replicated in the current study, it is important to note that both the aforementioned studies used different categorical classification of causal attributions which limits translation of results.
Previous studies have yielded mixed evidence with regard to the association between stigma and causal beliefs. While some have shown biological models to be associated with less stigma (Phelan & Link, 2004), others have found biological causes to be linked to greater stigmatization (e.g., Angermeyer et al., 2011; Arthur & Whitley, 2015). Yet others have found stigma scores to be significantly associated with supernatural causes (Charles et al., 2007).
Surprisingly, stigma scores only had a significant association with drug-related/substance-use causal attribution (e.g., drinks too much, smokes too much) but not with other causal explanations in the current study. Caregivers who endorsed drug-/substance use-related reasons reported greater perceived stigma than those who did not. This was in accordance with attribution theory, whereby substance use-related causes (e.g., misuse of drugs and alcohol) translated into the belief that the mental illness is self-inflicted or under an individual’s responsibility, which in turn elicits condemnation (i.e., higher stigma) rather than empathy (Adewuya & Makanjuola, 2008; Angermeyer et al., 2011; Corrigan, 2000; Subramaniam et al., 2017; Weiner, Perry, & Magnusson, 1988). One possible reason for the lack of significant findings could be due to the tendency of caregivers to endorse more than one causal belief for their relatives’ mental illness. The tendency to hold multiple, and in some instances, opposing models of illness has been shown in previous studies (e.g., Charles et al., 2007; Furnham & Chan, 2004). It is likely that endorsing more than one category could have masked the association between any particular causal attribution category and stigma.
Past studies such as Polenick and Martire (2013) and Williamson et al. (2005) have found casual attributions (particularly those attributed to the character and intention of the patient) to be associated with higher levels of burden as well as resentment among caregivers, respectively. Thus, it is possible that caregivers’ causal attributions may not be strongly associated with the perception of stigma but rather with caregivers’ burden and distress.
Current findings have important implications particularly in regard to the formulation of interventions such as psycho-education. Given the high endorsement of psychosocial factors among the study population, it is important that interventions targeted at caregivers address these factors rather than focusing exclusively on biomedical beliefs which are in line with the Western explanatory model of illness (Yang et al., 2015). Furthermore, the tendency to hold various causal beliefs about their relatives' illness should be taken into consideration when coordinating health care services for individuals given that multiple explanatory models may result in them seeking out various different treatment modalities (Charles et al., 2007; Phillips et al., 2000). This would in turn aid in enhancing responsiveness to the discussion of illness and treatment plans as well as boost therapeutic alliance (Yang et al., 2015).
Limitations
The current findings should be considered in view of the study limitations. Congruence between patients’ causal attributions and those of caregivers’ and service providers’ explanations of illness was not examined in this study. This may be crucial given that incongruence in explanatory models of illness between patients and caregivers could result in substantial burden on the part of the caregiver. Furthermore, details on the duration of caregiving, the presence of co-morbid conditions and the duration of illness of the patient were not obtained. This information might be important given that the time spent in caregiving is likely to be different for the various disorders, with the presence of co-morbid conditions resulting in more time being spent with the ill relative. Also, providing care for a relative with a longer duration of illness is likely to present a very different caregiving experience (in terms of patients’ behaviors and symptoms) compared to a shorter duration of illness (Chien & Chan, 2004). The use of self-report in obtaining the diagnosis of a participant’s ill relative may also present a potential problem in terms of accuracy of the diagnosis reported. In the current study, caregivers who were unaware of their relatives’ illness were not excluded. While this may be a potential problem, in most cases these individuals were either not given a formal diagnosis or were unable to recall the diagnosis of their relatives. However, given that the relatives of these caregivers were receiving treatment in a tertiary psychiatric institution, it was assumed that these individuals would still attribute their relatives’ illnesses to particular causes and would have experienced some form of stigma.
Conclusion
Notwithstanding its limitations, the current study is one of the few to explore caregivers’ causal attributions of their relatives' illness and how this could be related to stigma. It is reassuring that the majority of the caregivers endorsed psychosocial and biological causes over supernatural and drug/substance-use causes for their relatives’ illness given existing evidence that patients who tend to report supernatural causal beliefs are more likely to delay or replace medical treatment with alternative forms of treatment (Angermeyer et al., 2011; Saravanan et al., 2007). It is also crucial for clinicians to be aware that caregivers may hold more than one explanatory model of illness as this would enable them to tailor services that match the needs and preferences of the individual and family. Future studies should explore the relationship between caregivers’ causal attributions and health service use as this might be a crucial step to circumvent the problem of dropout and reduce treatment gap.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded through the Singapore Ministry of Health’s National Medical Research Council under the Centre Grant Programme (Grant No.: NMRC/CG/004/2013).