
Abstract
Sociocultural context seems to influence the epidemiology, phenotype, treatment, and course of psychosis. However, data from low- and middle-income countries is sparse. This research is part of a multidisciplinary and multimethod study on possible mental disturbances, including hallucinations, among (apprentice) traditional health practitioners (THPs) who have experienced the “ancestral calling to become a THP” in rural KwaZulu-Natal, South Africa. The aim of the current article is to examine whether the calling-related experiences can be assessed according to a psychiatric taxonomy. We included individuals who were identified with the calling and who were undergoing training to become a THP (ukuthwasa). IsiZulu-speaking formal mental health practitioners conducted thorough psychiatric interviews that measured psychological experiences with and without distress using the Community Assessment of Psychic Experiences, and psychiatric symptoms and disorders using the Schedule for Clinical Assessment in Neuropsychiatry. Of the 48 individuals who participated, 92% had psychotic experiences (PE), causing distress in 75%; and 23% met DSM-5 criteria for an unspecified psychotic disorder (15%) or mood disorder (8%). In conclusion, in rural KwaZulu-Natal, the ancestral calling may resemble phenomena that psychiatry would understand in the context of psychosis, ranging from subclinical PE to clinical psychotic disorder. Ukuthwasa might have a beneficial influence on the course of psychotic symptoms in some individuals, potentially because it reduces stigma and promotes recovery. Further multidisciplinary research is needed to investigate the psychopathology of the apprentice THPs and the underlying processes of ukuthwasa.
Keywords
Introduction
Growing evidence suggests that sociocultural factors may influence key aspects of schizophrenia spectrum disorders and other psychotic disorders (March et al., 2008; Myers, 2011; Veling, Hoek, Wiersma, & Mackenbach, 2010), including their epidemiology (Bourque, Van Der Ven, & Malla, 2011; Goldner, Hsu, Waraich, & Somers, 2002; Kirkbride et al., 2006; McGrath et al., 2004; Saha, Chant, Welham, & McGrath, 2005; Veling et al., 2007, 2008), phenomenology, course (Harrison et al., 2001), and recovery (Jääskeläinen et al., 2013). This potential influence can best be illuminated by transdisciplinary research, conducted within and across contexts with sharply contrasting cultural and socioeconomic environments (Susser & Martínez-Alés, 2018; Susser & Patel, 2014). To date, however, the vast majority of studies on psychosis have focused on developed, high-income nations. Data on psychosis from low- and middle-income countries (LMICs) remain sparse and have mostly been based on samples of individuals who visit mental health services, which is generally a minority of persons with psychosis in LMICs (Bekele, Flisher, Alem, & Baheretebeb, 2009; Burns & Tomita, 2015; Gureje et al., 2015; Morgan et al., 2015).
The present paper is an add-on to an epidemiological study of first episode psychosis in a rural area in KwaZulu-Natal (KZN), South Africa (Psychotic Disorders in an African Setting: Incidence, Early Course and Treatment Pathways; FEP-INCET study; Veling et al., 2019). The current research is part of a multidisciplinary, multimethod study (see also Van der Zeijst et al., 2020) on psychopathology, including experiences that psychiatric nosology might characterize as psychotic phenomena, among a sample of (apprentice) traditional health practitioners (THPs). This follows an ethnographic study in which the phenomenology, course, local healing processes, and emic perspective of the “ancestral calling to become a THP” are described (Van der Zeijst et al., 2020). In that study, some individuals in rural KZN mentioned the ancestral calling as a potential cause for mental disturbances, such as certain kinds of hallucinatory experiences, confusion, anxiety, fear of “losing their mind”, and sleeping problems. Although the concept of the calling is locally regarded as a gift from the ancestors and not as a pathological phenomenon, at its onset, the mental disturbances that accompany the calling are usually experienced as very disturbing, recognized as mental illness by patients and the people around them, and – together with physical symptoms – constitute a motive to seek help from formal healthcare, THPs, or both. We found indications that the ancestral calling runs in certain families. In the worldview of the Zulu, it is believed that the ancestral calling is handed down from generation to generation; at the same time, a genetic aetiology cannot be ruled out. Individuals who are identified with the ancestral calling by THPs are prescribed an apprenticeship as an apprentice THP; a process that is called ukuthwasa in isiZulu, the language of the Zulu. The apprentice THPs undergoing the process of ukuthwasa are called amathwasa. Our ethnographic results suggest that, in this particular group of people, ukuthwasa might result in recovery from the calling illness and its related distress and dysfunction – but not from the hallucinations, since the apprentice THPs and mature THPs intercede with the ancestors as part of their healing profession (Van der Zeijst et al., 2020).
To date, it remains unclear how the mental disturbances that are associated with the ancestral calling can be conceptualized from a psychiatric point of view. In the literature on ancestral calling among Nguni tribes – to which the Zulu belong – the ancestral calling has most often been related to psychotic disorders like schizophrenia (Buhrmann, 1982; Edwards et al., 1983; Niehaus et al., 2004; Shezi & Uys, 1997; Sorsdahl, Flisher, Wilson, & Stein, 2010), and to a lesser extent, to mood disorders and anxiety disorders (Ensink & Robertson, 1996; Sorsdahl et al., 2010). However, the literature is sparse and often dated, and to the best of our knowledge, no psychiatric or psychological studies have been conducted directly among apprentice THPs.
This article focuses on data derived from thorough psychiatric interviews that were conducted among amathwasa. We sought to determine whether their mental disturbances would be construed as representing psychopathology according to psychiatric taxonomy. Based on the thick descriptive data from our qualitative study as well as the literature, we expected to find all of the following represented among the apprentice THPs: 1) psychological experiences with and without distress using a self-report questionnaire (the Community Assessment of Psychic Experiences – CAPE); 2) psychiatric symptoms using a semi-structured psychiatric diagnostic interview (Schedules for Clinical Assessment in Neuropsychiatry – SCAN); and 3) psychiatric disorders using the SCAN. By using these instruments, we aimed to assess the degree to which each was represented, focusing on psychosis and mood-related disorders. Furthermore, by combining our quantitative and qualitative results, we aimed to make inferences that would illuminate how we should think about the psychological manifestations of the apprentice THPs and the process of ukuthwasa in particular, and on the role of social context in relation to psychosis in general.
Methods
Study site
This study was conducted in Vulindlela, a rural communal area in KZN that is situated approximately 150 km north-west of the city of Durban in South Africa. Vulindlela, with about 250,000 residents, has five traditional councils, each of which is headed by an Inkosi (tribal chief) who is involved in community life along with formal government authorities (Labys, Susser, & Burns, 2016). The area is characterized by widespread poverty and unemployment. The HIV prevalence in KZN is the highest in the country, with 60% of the women and 40% of the men in the age group 25–40 years affected (De Oliveira et al., 2017). In Vulindlela, there are nine public sector primary health care clinics. The closest psychiatric referral hospital is Town Hill psychiatric hospital in Pietermaritzburg. In the province of KZN, approximately 25% of the beds that are required to provide adequate in-patient psychiatric care are available (Burns, 2014). Community mental health services are even more sparse, especially in rural areas, such as Vulindlela. In these areas, a significant proportion of health care is delivered by the THPs practising in the region.
Participants
Individuals who were identified by a THP as having the ancestral calling and who were accepted by the THP to undergo ukuthwasa – the training to become a THP – were included between September and December 2013. THPs base the identification of the ancestral calling on the presence of certain signs and symptoms, including powerful ancestral dreams (Van der Zeijst et al., 2020). The only exclusion criterion that we defined was being aged under 21 and above 48. Written informed consent was obtained in each participant’s first language.
Procedures and instruments
The present research was conducted as an add-on study to a mixed-methods preparatory study for the investigation of the incidence, early course, and treatment pathways of psychotic disorders in a rural South African setting (FEP-INCET study; Veling et al., 2019). The study was approved by the regional chairperson Zulu Inkosi and his Traditional Council. Ethical approval was obtained from the University of KwaZulu-Natal Biomedical Research Ethics Committee (file number BEO68/11) and Columbia University Institutional Review Board (file number IRB-AAAI1536).
The FEP-INCET study has been working with a progressive association of THPs known as uMwelela Kweliphesheya. This association signed a memorandum of understanding with the Nelson Mandela School of Medicine of the University of KwaZulu-Natal in 2003, and agreed to collaborate on issues of research, education, and training. In order to become a THP, the individual must have followed ukuthwasa successfully and be initiated as THP. In order to practice as a THP, an individual should be registered as a THP with the tribal authority. For the FEP-INCET study, 50 THPs were recruited who were all verified by tribal authorities as authentic THPs, who consented to participate in the study, and who committed to participate in training (Veling et al., 2019). For this sub-study, the local project manager (EM), who is a psychiatric nurse and has worked closely with traditional leadership and THP groups in the region for many years, selected from these 50 original recruits the THPs who were training amathwasa. These THPs were provided with information about the sub-study, and were, after they agreed to participate, requested to refer all their apprentice healers to our study, and not to make any selection if they were training more than one apprentice. In the end, five THPs contributed to this study.
The amathwasa underwent two separate interviews that were completed blind to the results of the other. The first interview included the sociodemographic characteristics and the CAPE. The second interview consisted of the SCAN. Both interviews were conducted on the same day at Town Hill psychiatric hospital in Pietermaritzburg. Interviewees were compensated in cash for their time with 200 South African rand.
CAPE
The CAPE is a 42-item questionnaire developed to assess the prevalence of subclinical psychotic experiences in the general population (Konings, Bak, Hanssen, Van Os, & Krabbendam, 2006). We translated the questionnaire into isiZulu according to the WHO guidelines of forward-translation, back-translation, and adaptation (World Health Organization, 2010). Originally, the CAPE is a self-report questionnaire, but because of the high level of illiteracy in Vulindlela, the CAPE was administered by trained, isiZulu-speaking students in psychology. The CAPE assesses three symptom dimensions: positive experiences, negative experiences, and depressive experiences, with 20, 14, and 8 items, respectively. Each item assesses frequency and distress associated with the experience, both on a 4-point Likert scale ranging from “never” to “nearly always” (frequency) and “not” to “very” (distress). An experience was rated as present if the frequency was “often” or “nearly always”. Distress was rated as present if the score was “quite” or “very” for symptoms with a frequency of at least “often”. The positive dimension measuring psychotic experiences (PE) was further divided into three subdimensions: perceptual anomalies, bizarre experiences, and delusional ideation (Mark & Toulopoulou, 2016).
SCAN
The SCAN is a semi-structured diagnostic interview to assess psychiatric symptoms and diagnoses (Wing et al., 1990). The SCAN was conducted by three local isiZulu-speaking psychiatrists who were fluent in both isiZulu and English, and who were familiar with the Zulu culture. The psychiatrists received a formal SCAN training from two experienced clinical psychiatrists (WV and HWH) to conduct this clinical diagnostic interview. We conducted version 2.0 of the SCAN, limited to sections relevant for mood disorders and for psychotic disorders, asking for present state symptoms (up to six weeks prior).
In the SCAN, the clinical severity of a symptom is measured by assessing the duration and frequency of the symptom and the degree to which symptoms interfere with mental functions (intensity). Some items have their own individual rating scales, while other items – usually related to specific symptoms – are rated on a standard 4-point scale. For reasons of clarity in the presentation of symptoms, we mainly used the items to which these standard rating scales are applied – unless otherwise noted. For mood-related symptoms, this scale consisted of: “absent”, “present in minor degree”, “present in moderate severity during most of the period”, and “present in severe form during most of the period”. For psychotic symptoms, clinical intensity was measured according to either frequency or duration and no attempt was made to define mild, moderate, and severe intensity. The scale that was used for these items consisted of: “absent”, “present, but uncommon or transitory”, “present on multiple occasions or part of the time”, and “present, more or less continuously”. In the section of the SCAN that inquired about delusions, it is noted that this standard rating scale may not directly reflect the clinical status of delusional beliefs; nevertheless, the interviewer is asked to rate delusions by using this standard scale.
In order to assess psychiatric diagnoses, all SCAN interviews were reviewed one by one, and a diagnostic classification according to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) was made for each participant during a consensus meeting with four psychiatrists. In case of incongruence, the final decision was made by the senior psychiatrist (JKB).
Data analysis
Data from the CAPE and SCAN were entered and analysed using the Statistical Package for Social Sciences (SPSS), Version 23.0. Descriptive statistics were performed for group characteristics. Sample means and percentages were calculated, and simple frequency distribution for different variables was generated.
Results
In total, 48 apprentice THPs were included in this study. We were able to complete the interviews for the entire study group. The sociodemographic characteristics of the amathwasa are shown in Table 1. All participants identified themselves as Zulu. There were more female than male participants, slightly more than half of them were in their 20s, and the majority were single. All but one reported a religious affiliation, all related to Christianity. Christian denominations that involve traditional African rituals and customs (such as Shembe and Zion) were reported more often than denominations in which these traditions are not, or to a lesser extent, incorporated (such as Presbyterian, Methodist, and Catholic religion). Most participants were undergoing ukuthwasa on a full-time basis and had no other occupation.
Sociodemographic characteristics of the amathwasa (n = 48).
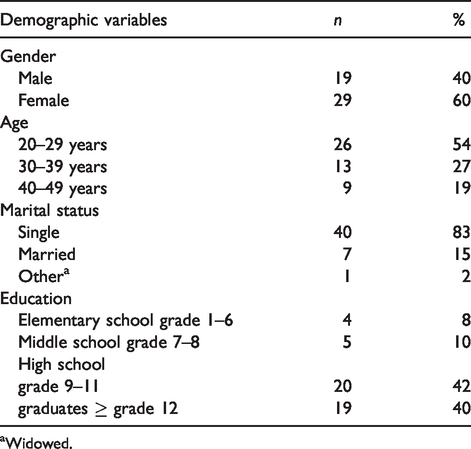
Widowed.
Psychological experiences as measured with the CAPE
The vast majority (94%) of participants in the study group (n = 48) endorsed at least one experience on the positive, negative, or depressive dimension of subclinical psychotic experiences. The average was nearly nine experiences per apprentice THP. These experiences caused distress in 81% of the group, with an average of 5.7 distressing experiences per participant. Of the three CAPE dimensions, experiences of the positive dimension were most often reported and were most often associated with distress. Within the positive dimension, delusional ideations were reported more often than bizarre experiences and perceptual anomalies (90% versus 67% and 46%, respectively), and were more often associated with distress (71% versus 42% and 33%, respectively). On the negative dimension, experiences were endorsed as present by 73% and as distressful in 60% of the cases, and on the depressive dimension, this was 58% and 48%, respectively (see Table 2).
Presence and distressfulness of psychological experiences as measured with the CAPE (n = 48).
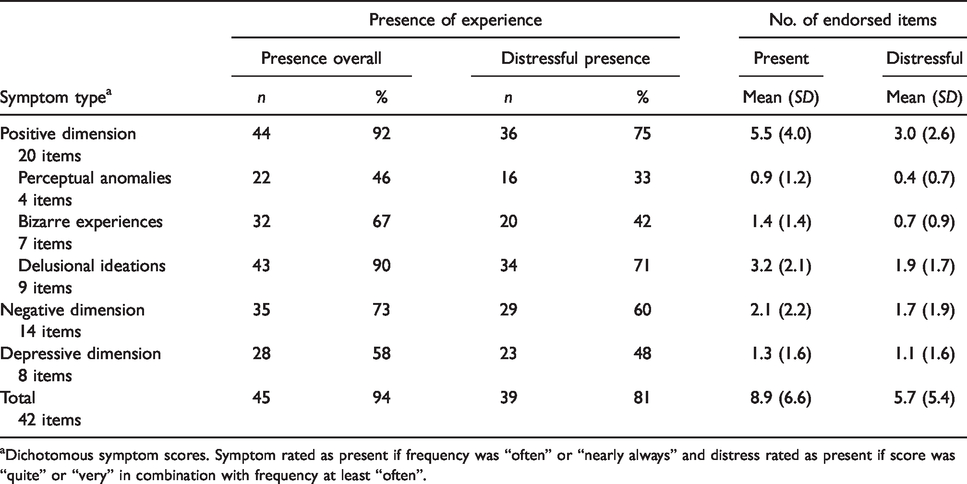
Dichotomous symptom scores. Symptom rated as present if frequency was “often” or “nearly always” and distress rated as present if score was “quite” or “very” in combination with frequency at least “often”.
Psychiatric symptoms as measured with the SCAN
In Table 3, an overview of the prevalence of psychotic and mood-related symptoms in the study group is shown. Of the psychotic symptoms, hallucinations were more prevalent than delusions. Seventy-three percent of the group had verbal auditory hallucinations. “Being spied upon” was the most prevalent delusion. Except for one apprentice THP who suffered from “thoughts being read” on multiple occasions, delusions were rated as uncommon or transitory. Religious delusions and delusional paranormal explanations were present in 6% of the sample (not included in Table 3 because they are assessed with an absent/present scale only). All participants with delusions also reported hallucinations to some degree.
Frequency distribution of psychotic and mood-related symptoms identified on the SCAN (n = 48).

Items of SCAN using a different scale, converted as follows to present the symptoms in uniformity:
†“rarely” and “every week” > “transitory”; “most days” > “part of the time”; “nearly all the time” > “continuously”. ‡“voices do comment occasionally” > “transitory”; “frequent comments” > “part of the time”. §“little or no loss, but does not positively enjoy life” > “minor degree”; “marked loss” > “moderate severity, most of period”; “total loss” > “severe, most of period”. bIncluding: sensations of touch, temperature, pain and floating. cIncluding: sexual delusions, hypochondriacal delusions, familiar people impersonated, delusions of grandiose identity, delusions concerning appearance, delusion of depersonalization or realization, thought insertion, and thought commentary. dAccording to SCAN, this is a positive rating of presence, but presence to such a minor degree that it is not appropriate for use in diagnostic classification.
Of the mood-related symptoms, depressive symptoms were more prevalent than symptoms of expansive mood. The mood-related symptoms were mainly experienced to a minor degree. According to the SCAN, this would constitute a positive rating of presence, but to such a minor extent that it is not appropriate for use in diagnostic classification (World Health Organization, 1994).
Psychiatric diagnoses as measured with the SCAN
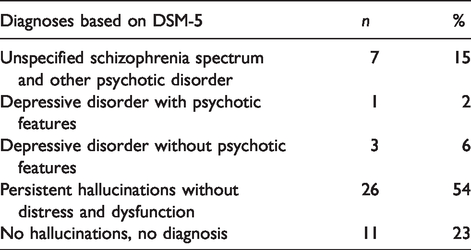
Eleven participants (23%) had a diagnosis of any psychotic or mood-related disorder. Of these participants, seven were diagnosed with a psychotic disorder and four with a mood disorder. The seven with a psychotic disorder were all assigned an “unspecified schizophrenia spectrum and other psychotic disorder”. None of the participants met the criteria for any specific psychotic disorder, such as schizophrenia, schizoaffective disorder, brief psychotic disorder, or schizophreniform disorder. All four participants with a mood disorder met the criteria for a depressive disorder, one of which with psychotic features. Thirty-seven participants (77%) did not meet the criteria for any psychotic or mood-related disorder; however, 26 participants (54%) had persistent hallucinations, most often auditory hallucinations. Because they did not suffer from any distress and dysfunction, their symptoms were not conceived as part of a DSM-5 disorder (see Table 4).
Diagnoses as measured with the SCAN based on DSM-5 (n = 48).
Discussion
In this study, we aimed to determine whether the experiences of apprentice THPs (amathwasa) could be explained from a psychiatric point of view. We assessed the degree to which psychotic and mood-related psychological experiences, psychiatric symptoms, and psychiatric diagnoses were represented among a group of amathwasa. The main findings are that, of the amathwasa: 1) nearly all had PE, most of them with distress; 2) 73% experienced verbal auditory hallucinations, while delusions on a symptom level were far less common; and 3) 23% met the criteria for a DSM-5 diagnosis, namely an unspecified schizophrenia spectrum and other psychotic disorder in 15% and a mood disorder in 8%.
There are different ways of conceptualizing the mental disturbances that are associated with the ancestral calling, and these concepts might coexist within the group of amathwasa. As we also speculated in our qualitative study (Van der Zeijst et al., 2020), their experiences might reflect one or more of the following concepts: 1) no psychopathology; 2) psychopathology recognized by psychiatric taxonomy; 3) culture-specific psychopathology that is not (yet) recognized by psychiatric taxonomy. To elaborate on these concepts, we will draw upon the descriptive data of our qualitative study (Van der Zeijst et al., 2020), as well as on the quantitative findings of the current study, because the presence or absence of psychopathology is not only determined by symptom factors like frequency and intrusiveness, but also by cultural factors, such as symptom interpretation and coping.
The concept that the calling illness of the amathwasa does not reflect psychopathology is supported by the finding that 77% of participants could not be assigned a psychotic or mood-related DSM-5 diagnosis. For example, motivation to become a THP might play a role in the occurrence of the experiences. In the anthropological literature, it has been suggested that it is one of the few ways for Zulu women to function independently in traditional, patriarchic Zulu societies; this has been given as an explanation for why there are far more female than male THPs in KZN (Hammond-Tooke, 1989; Lee, 1969; Ngubane, 1977; Ogana & Ojong, 2015). As 54% of the amathwasa had persistent hallucinations, mainly auditory, but no psychiatric diagnosis, this group could resemble a selection of healthy voice hearers, defined as “individuals who experience persistent auditory verbal hallucinations, yet have no need for clinical care and do not suffer the significant distress this experience may cause in clinical populations” (Baumeister, Sedgwick, Howes, & Peters, 2017, p. 126). This non-pathological interpretation of auditory hallucinations coheres with the findings from our qualitative study (Van der Zeijst et al., 2020), in which amathwasa and mature THPs regard their ability to communicate with their ancestors via hearing their voices as a gift and a crucial part of their healing profession – rather than as a pathological phenomenon. One additional argument for why the calling-related experiences might be non-psychopathological is that individuals who have become THPs seemed to be well-functioning individuals, with no apparent signs of mental disorders (Van der Zeijst et al., 2020).
The concept that the experiences of the amathwasa indicate psychopathology, ranging from potential prodromal signs and symptoms of psychotic or non-psychotic psychiatric disorders to an actual clinical psychotic episode, is substantiated by high rates of PE (CAPE) and psychotic symptoms (SCAN) among the amathwasa. Seventy-five percent of amathwasa experienced distressing PE, whereas in their systematic review and meta-analysis, Linscott and Van Os (2013) calculated an average prevalence of PE in the general population of 7.2%. Although PE and psychotic symptoms may be related to a degree of distress and help-seeking behaviour, they do not necessarily amount to clinical psychotic disorder (Van Os, Linscott, Myin-Germeys, Delespaul, & Krabbendam, 2009). However, they do sometimes occur as part of the clinical high-risk state for psychosis, which confers an enhanced probability of later developing a psychotic episode, with a transition risk that could be as high as 32% after three years (Fusar-Poli et al., 2013; Van der Gaag et al., 2012). Our results show that 15% of the amathwasa could be diagnosed with actual psychotic disorder, which is much higher than normal population (lifetime) prevalence of approximately 3% (Van Os et al., 2009). Additionally, the findings from our qualitative study support this scenario of psychopathology for a substantial proportion of amathwasa (Van der Zeijst et al., 2020). The participants from our ethnographic study reported that the hallucinatory experiences, such as hearing the voices of their ancestors, are often associated with significant distress and impaired functioning at their onset. In combination with a set of other mental and physical disturbances, these are interpreted as serious illness by the individuals themselves and the people around them. In order to evaluate whether the apprentice THPs are in fact individuals who are in a high-risk state for psychosis, we are conducting a follow-up study.
The third possibility is that the calling illness reflects culture-specific psychopathology which is not (yet) recognized by psychiatric taxonomy. Shezi and Uys (1997) suggested that the calling illness shows similarities with shin-byung, a cultural syndrome originating from the Korean shamanistic tradition. This syndrome, which was included in the DSM-IV-TR (American Psychiatric Association, 2000) but not in the DSM-5, is the experience of possession by a god undergone by a chosen healer, which is accompanied by physical pain and psychosis that may only be cured through acceptance of, and full communion with, the spirit (Yi, 2000).
Our qualitative study informed us that the hallucinations and other mental disturbances of the amathwasa tend to follow a process, from seriously disturbing at the onset, to beneficial and positive at the outcome (Van der Zeijst et al., 2020). According to the participants, this applies only if the affected individual successfully undergoes ukuthwasa. Individuals who were later identified with the calling first sought help because they experienced distress and dysfunction from mental and physical illness. After becoming a THP, they explained, they were cured from the distress and dysfunction of their disturbances: they transformed into well-functioning and respected members of the society, with a defined occupation, role, and social status (Van der Zeijst et al., 2020). Given the fact that all amathwasa who we assessed in our quantitative study had been apprentice THPs for some time already, one can wonder whether we would have found even higher prevalence rates of PE, psychotic symptoms, and psychiatric disorders if we had assessed them in their acute phase, when they first moved in with their THP; especially the 54% with isolated hallucinations but without a psychiatric diagnosis. However, these 48 individuals were further into the process of ukuthwasa and thus might have largely recovered. As a result, they might be left only with non-disturbing auditory hallucinations as part of their healing profession. Accordingly, one could hypothesize that the amathwasa who met the criteria for a psychiatric disorder might not be far enough in the process and therefore have not recovered yet, so follow-up might show recovery in most of these. Another possible explanation for the high prevalence of psychiatric disorders among the amathwasa is that the social perception of the calling illness versus a psychiatric disorder is blurred at the boundaries. Some individuals who perhaps have a more significant disorder interpret this as calling illness and enter into ukuthwasa, but continue to experience distress and/or dysfunction despite the intervention. They may be individuals who do not respond to ukuthwasa, and for whom the calling “diagnosis” might need to be revised (Ensink & Robertson, 1996; Niehaus et al., 2004).
There are various anthropological and historical writings on the African healing tradition. The phenomenon of the ancestral calling and the apprenticeship to become a THP is found in most African countries, for example in Uganda (Teuton, Bentall, & Dowrick, 2007), Burkina Faso (Meyer, 1991), and the Congo (Devisch, 1991). However, literature that adopts a psychological perspective is sparse, and only a few studies have indicated that ukuthwasa might be a local intervention for psychopathology (Buhrmann, 1982; Lee, 1969); for example, in terms of “reintegrating and channelling psychopathology and emotional instability” (Lamla, 1975, cited in Ensink & Robertson, 1996). Based on the findings from our qualitative study (Van der Zeijst et al., 2020), we hypothesize that the process of ukuthwasa might be considered a response to overcome the stigma of psychosis within this particular culture, because during ukuthwasa: 1) hallucinations are reframed from distressing, negative experiences to positive experiences (namely, as important and useful messages from the ancestors); 2) individuals are taught a new, constructive role as they shift from being a patient who receives treatment to being a student who receives training to become a THP; 3) the apprentice THP moves in with a THP, with whom he or she can positively identify; and 4) the disturbances are positively valued in line with local beliefs and practices. The training to become a THP gives people a social role and thereby addresses “what matters most” (Yang, Thornicroft, Alvarado, Vega, & Link, 2014, p. 496) to them. It is well known that psychotic syndromes are highly stigmatized conditions (Lasalvia et al., 2014; Yang et al., 2013), and growing evidence suggests that this stigma and discrimination have a negative impact on the psychological well-being of individuals who are at a high risk for psychosis (Rüsch et al., 2014; Yang et al., 2015). Other underlying mechanisms that may contribute to the potential beneficial role of ukuthwasa on mental disturbances, might relate to reducing poverty, social exclusion, and gender inequality, which are known to be common determinants of mental health problems (Patel, 2015). However, future investigations into the process of ukuthwasa are needed to examine whether and how this cultural process influences the course of psychotic symptoms and other mental health problems.
Strengths and limitations
A major strength of the current study is that the interviews were conducted by local mental health practitioners who have lived most of their lives in an environment steeped in Zulu culture, and who are trained in Western psychiatry. They are familiar with both the Zulu concepts and the DSM, both the emic and etic phenomenology of mental illness, and they speak both isiZulu and English fluently. Another important strength is that we had information on contextual factors via our ethnography, which helped us in the interpretation of the quantitative results. Furthermore, we conducted psychiatric assessments directly amongst individuals who were identified with the ancestral calling and who were undergoing ukuthwasa. As far as we know from the literature on ancestral calling, we are the first to have adopted this approach.
The results of the current study should be considered in light of several limitations, such as a relatively small study sample and the inclusion of amathwasa via the THPs who were also involved in the FEP-INCET study, wherein THPs were asked to refer patients with hallucinatory experiences (Veling et al., 2019). It might be possible that this influenced which amathwasa they referred to the study, namely the ones with hallucinatory experiences. However, the THPs were specifically asked to refer all their amathwasa and not to make any selection. We therefore believe that our study sample is representative of the population of apprentice THPs within the research area. Furthermore, because we assessed the amathwasa on psychotic and mood-related disorders only, there is a small chance that we missed other DSM-5 diagnoses that might provide psychiatric explanations of the calling, like dissociative trance.
An apparent discrepancy exists between the CAPE and SCAN results in our sample of amathwasa. Namely, on the CAPE, 75% of the participants had distressing PE. Yet, using the SCAN, only 17% were diagnosed with a psychotic disorder (including 2% with mood disorder with psychotic features). Fifty-four percent had persistent hallucinations, but not sufficient distress and dysfunction to meet the criteria for a psychiatric disorder. Additionally, delusional ideations were more prevalent on the CAPE than delusions on the SCAN. These discrepancies can be explained by the fact that the instruments are measuring different outcomes, with the CAPE measuring (sub)clinical psychological experiences and the SCAN measuring clinically significant psychiatric symptoms. Another important difference is the way in which the instruments were used. The CAPE interview, originally a self-reported instrument, was conducted by students in psychology who were instructed not to probe. The SCAN, on the other hand, involved probing and the interpretation of a clinically experienced and SCAN-trained psychiatrist.
Another important issue is that we used the full, validated version of the CAPE in this study, which includes the item: “Do you believe in the power of witchcraft, voodoo or the occult?” In our research area, the belief in witchcraft and the occult is culturally syntonic, meaning that a positive score on this item cannot simply be regarded as a delusional ideation. Therefore, the CAPE results of Table 2 should be interpreted with caution. The item “Do you believe in the power of witchcraft, voodoo or the occult?” was reported as present by 67% of the amathwasa, causing distress in 44% (see also Supplementary Table 1 in the Supplemental Material online). Excluding this item from our calculations would yield the following outcomes among the sample: a) total delusional ideations (based on 8 items): frequency 79%, distress 60%, mean no. of experiences 2.5 (SD 1.8), mean no. of experiences with distress 1.5 (SD 1.5); b) total positive dimension (based on 19 items): frequency 85%, distress 67%, mean no. of experiences 4.8 (SD 3.9), mean no. of experiences with distress 2.5 (SD 2.5); and c) total CAPE scores (based on 41 items): frequency 90%, distress 75%, mean no. of items 8.2 (SD 6.4), mean no. of items with distress 5.3 (SD 5.3). In the diagnostic process of the SCAN, the clinical presentation of the individual helped the psychiatrists in their decision whether the belief in witchcraft was culturally appropriate or had the characteristics of a delusion.
Finally, whereas this quantitative design builds on prior qualitative work and, as a multimethod study, is suited to articulate cultural processes in relation to psychopathology, our finding that ukuthwasa might have a beneficial influence on the course of psychosis is only suggestive, as we have no record of how long the amathwasa had been undergoing the process of ukuthwasa at the time of the assessments, nor did we measure the effects of ukuthwasa quantitatively. In two feedback meetings with THPs, we presented the findings of our studies among the apprentice THPs. The THPs were given the opportunity to comment on the findings during these meetings. The THPs understood that, from a Western psychiatric perspective, the symptoms that accompany the ancestral calling can be explained within a context of psychiatric disorders, especially psychotic disorders, and they felt seen and taken seriously with the hypothesis that ukuthwasa might have a beneficial influence on the course of these symptoms, as most THPs are well functioning individuals with no signs of mental illness.
Conclusion
Our results confirm the suggestions from previous studies as well as the hypothesis from our qualitative study, namely that there is a relation between the Zulu cultural concept “ancestral calling to become a THP” and what Western psychiatry would characterize within the context of psychosis. Our data indicate that the psychotic phenomena of the amathwasa range from subclinical PE to clinical psychotic disorder. We found indications that the process of ukuthwasa might have a beneficial influence on the course of psychotic symptoms in some individuals who respond to this process, potentially because it offers a model, originated as part of the culture, for reducing stigma and promoting recovery.
Experiences can be (and are) understood within different conceptual frameworks. In this article, we have explored how the Western psychiatric perspective fits the experiences of people who sought help for distressing physical and mental experiences, which were labelled as ancestral calling by a THP.
Some people met the diagnostic criteria of a psychotic or a mood disorder. This does not imply that all amathwasa are mentally ill, nor does it devaluate the traditional healing paradigm. It does suggest that it is useful to apply a psychiatric perspective as well. This would work two ways: people with a diagnosed psychiatric disorder might benefit from psychiatric treatments, and psychiatric mental health care might learn from the healing/recovery effects of ukuthwasa in people with a diagnosable psychiatric disorder.
Our study has various other implications. Obviously, our findings warrant further consideration and development, and more multidisciplinary research is needed to investigate the psychopathology of the amathwasa and the underlying processes of ukuthwasa. Our study also offers an example of how studying psychotic illness in other cultures in LMICs is not only essential for the development of effective public health interventions locally, but also for providing new insights on risk factors for psychotic disorders, for guiding the design of early intervention studies, and for providing a foundation for ongoing research on these disorders in high-income countries.
Supplemental Material
sj-pdf-1-tps-10.1177_1363461520949672 - Supplemental material for Psychopathology among apprentice traditional health practitioners: A quantitative study from rural KwaZulu-Natal, South Africa
Supplemental material, sj-pdf-1-tps-10.1177_1363461520949672 for Psychopathology among apprentice traditional health practitioners: A quantitative study from rural KwaZulu-Natal, South Africa by Martine C.E. van der Zeijst, Wim Veling, Elliot Mqansa Makhathini, Sisanda Mtshemla, Ndukuzakhe D. Mbatha, Sinethemba S. Shabalala, Ida Susser, Jonathan K. Burns, Ezra Susser and Hans W. Hoek in Transcultural Psychiatry
Footnotes
Acknowledgments
The authors would like to thank Nokwe Mbatha and Siphumelele Nene for their assistance with translation and data collection, and Khwezi Khanyile for her assistance with data entry. We would also like to thank the traditional health practitioners who referred the amathwasa to our study, and the amathwasa themselves for contributing to this research. Finally, we are very grateful to Inkosi Zondi and his Traditional Council, who generously gave us permission to conduct this research within their community.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was an addition to a study (partly) supported by the Fogarty International Center at the U.S. National Institutes of Health (NIH), program Brain Disorders in the Developing World: Research Across the Lifespan (grant number 1R21 MH093).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.