
Abstract
The mental health of asylum seekers has attracted significant interest and examination. Quantitative studies have consistently indicated that asylum seekers experience mental distress at a higher rate than both host populations and their refugee counterparts. Qualitative insight into asylum seekers’ embodied experience of mental distress is limited. This qualitative narrative study aimed to explore African asylum seekers’ everyday embodied experiences of mental distress. Sixteen semi-structured one-to-one interviews were conducted with African asylum seekers who had experienced mental distress and were receiving mental health care services in Ireland. Narrative data were analysed using a holistic analysis framework of narrative form and content. Participants described their everyday endurance of relentless rumination, shame, self-loathing, anger, and mistrust, and of becoming demoralised and hopeless. Study findings indicate that asylum seekers’ mental distress interweaves the physical, psychological, emotional, and social realms, thus impacting on the whole of their being. Consequences for asylum seekers include feeling anaesthetised, having a severely diminished capacity to connect and interact with their external surroundings and other people, and, for some, efforts to end their life.
Examinations of, and responses to, asylum seekers’ mental distress must delve beyond the confines of diagnostic categorisations and codifications of symptomology. To achieve heightened understanding and efficacious interventions, we must empathetically listen and engage with asylum seekers’ narratives of distress and the socio-cultural and socio-political context they inhabit.
Introduction
As the search for safety, acceptance, freedom, democracy, and human rights continues, the United Nations High Commissioner for Refugees (UNHCR) estimates the number of forcibly displaced persons around the globe to be at a record high of 70.8 million (UNHCR, 2018). By the end of 2018, the Republic of Ireland had received 13,336 forcibly displaced individuals, 7,196 of whom were asylum seekers (UNHCR, 2018). The number of people seeking asylum is forecast to increase to approximately 7,700 people by the end of 2019 (Department of Justice, 2019). In Ireland, asylum seekers await the outcome of their asylum application in reception centres known as Direct Provision (DP). The DP system facilitates their access to housing in one of 39 geographically dispersed accommodation sites and provides a weekly allowance of €38.80 per adult and €29.80 per child, daily meals, and access to healthcare.
Figures supplied in September 2019 indicate that, due to wider issues pertaining to housing supply in Ireland, while 6,056 people seeking asylum are being accommodated in dedicated asylum accommodation centres, there are 1,363 people seeking asylum who are living in emergency accommodation locations (e.g., sharing rooms in hotels and B&Bs). The median processing time for a first instance decision on asylum applications is reportedly 14.3 months and as of June 2019, 5,727 cases awaited processing (Department of Justice, 2019). Prior to 2017/2018, asylum seekers were prohibited from entering the labour force and their access to university education was financially prohibitive. Six Irish universities have since been granted the status of ‘University of Sanctuary’, enabling them to waive fees and/or provide scholarships to a small number of eligible asylum seekers each year. In addition, the European Communities (Reception Conditions) Regulations 2018 came into effect in Ireland on 30 June 2018, permitting access to the labour market for a specific cohort of eligible international protection applicants. People who do not receive a first instance recommendation within nine months from the date when their protection application was lodged can now apply for a labour market access permission from the Minister for Justice and Equality.
However, commentators have highlighted the many prohibitive barriers that challenge eligible individual’s ability to secure employment, including their lack of access to bank accounts and driving licences, the remote locations of DP centres, which make it difficult to gain employment in the locality, and a lack of awareness on the part of employers regarding the right to work for people seeking asylum (Irish Refugee Council, 2019). In addition, asylum seekers must reapply for permission to work every six months. Consequently, the temporary nature of the permission to work can act as a deterrent for potential employers. Reports of unsuitable and poor living conditions, child protection concerns, as well as inefficient and opaque legal procedures have also attracted the concerns of national and international human rights organisations (Irish Refugee Council, 2013, 2019; Working Group on the Protection Process on Improvements to the Protection Process, including Direct Provision and Supports to Asylum Seekers, 2015; United Nations Committee on the Elimination of Racial Discrimination, 2016; United Nations Committee against Torture, 2017; Arnold, 2012; Shannon, 2012).
The psychological wellbeing of forcibly displaced populations is an enduring concern, as an established body of research has reached the consensus that they experience mental health difficulties at a comparatively higher rate than host country populations (Fazel, Wheeler, & Danesh, 2005; Lindert, Ehrenstein, Priebe, Mielck, & Brähler, 2009; Ryan, Kelly, & Kelly, 2009; Gerritsen et al., 2006; Momartin et al., 2006; Steel et al., 2009). Asylum seekers are particularly vulnerable in that they experience even poorer mental health outcomes than their refugee counterparts, including increased rates of post-traumatic stress disorder (PTSD), depression, anxiety, suicide, and suicidal behaviour (Ryan et al., 2009; Gerritsen et al., 2006, Iverson & Morken, 2004; Momartin et al., 2006; Richter et al., 2018). Studies highlight how concomitant aspects of the asylum seeking phase, such as the protracted procedures of seeking asylum, insecurity regarding legal status in a host country, living in detention, threats of repatriation, challenging refugee determination procedures, restricted access to services, and lack of opportunities to work or study, insidiously combine to generate this higher risk of mental distress (Li, Liddell, & Nickerson, 2016; Laban, Gernaat, Komproe, Schreuders, & De Jong 2004; Laban, Gernaat, Komproe, van der Tweel, & De Jong, 2005; Lamkaddem, Essink-Bot, Devillé, Gerritsen, & Stronks, 2015; Mueller, Schmidt, Staeheli, & Maier, 2011; Ryan et al., 2009; Silove, Sinnerbrink, Field, Manicavasagar, & Steel, 1997; Silove, Steel, & Watters, 2000; Silove et al., 2007).
From a research perspective, the aforementioned corpus of research has predominantly employed quantitative methodologies to determine prevalence and has framed or codified asylum seekers mental health within the confines of diagnosable mental health conditions. Further, Li and colleagues (2016) contend that extant research that explores the determinants of asylum seekers’ mental health has tended to focus on quantitatively determining which aspect of the asylum seekers pre- and/or post-migratory stressors most strongly impact upon their psychological wellbeing. These strands of research provide relatively limited insight into how mental distress is subjectively experienced on a daily basis in the post-migratory context of seeking asylum. While a body of qualitative research is emerging, its focus has predominantly explored asylum seekers’ experiences’ of post-migratory conditions (Barnes, 2003; Brekke, 2004; Burchett & Matheson, 2010; Coffey, Kaplan, Sampson, & Tucci, 2010; Murphy, Keogh., and Higgins, 2018) and their experience of seeking mental health support (Sundvall, Titelman, & Bäärnhielm, 2018; Chase & Rousseau, 2017). To our knowledge, there remains a paucity of research that explores asylum seekers’ first-person accounts of how they experience their mental distress whilst awaiting their asylum outcome.
Exploring first-person accounts is important because people who experience mental health difficulties have an intimate, in-depth knowledge of why and how their mental distress manifests, the meaning they ascribe to their distress, how it affects their life, how treatments and interventions may impair or improve their life, and what paths they wish to pursue to restore a meaningful and productive life (Davidson, 2016). It is this expertise that originally inspired the implementation of recovery-oriented care in mainstream mental health policy and practice. Mental health practitioners were once viewed as the sole experts, but they are now encouraged to afford parity of esteem, engage with service users, and incorporate into their practice this other valid source of experiential expertise (Davidson, 2016). Further, in the current era of globalisation, mental health service providers are challenged to understand, address, and provide services that acknowledge and incorporate the complexity and interdependence of a person’s many social identities (race, ethnicity, gender, etc.) and the systemic inequalities and structural forces which shape a person’s experiences (DelVecchio Good & Hannah, 2015; Fisher-Borne, Cain, & Martin, 2015). It is within this context of recovery-oriented care and of demand for enhanced cultural competence and humility that bearing witness to the personal narratives of asylum seekers can help challenge embedded understandings of, and responses to, their mental distress, inspire compassion and empathy, and promote enhanced validation of their experiences. Contextualising asylum seekers’ embodied experience of distress within their socio-cultural and socio-political environments has the added benefit of ensuring that adaptive and meaningful therapeutic responses are curated and implemented with potentially increased efficacy as a result.
This paper presents a selection of findings from a narrative study that was designed to explore the mental health and mental health care experiences of African asylum seekers in Ireland. It focuses specifically on African asylum seekers’ embodied experiences of enduring mental distress while awaiting a decision from their asylum application.
Methods
A qualitative narrative study design was conducted that used semi-structured face-to-face interviews. Participant recruitment was accomplished through a convenience purposeful sample, which was facilitated by staff members at two mental health support services. Acting as gatekeepers, staff members identified individuals who fulfilled the study eligibility criteria, which required participants to: 1) originate from an African country; 2) be seeking asylum at the time of data collection; 3) have experience of attending a mental health service; 4) feel well enough to partake in the study and; 5) have capacity to consent to the interview. Individuals’ attainment of a prescribed diagnosis was not an inclusion criterion. This study focused on participants’ subjective appraisals of their mental health and their access to mental health support services. To assert a prescribed diagnosis as an inclusion criterion would reaffirm the framing and categorisation of asylum seekers’ mental health experiences within a pathologizing lens and consequently conflict with the remit of the study.
Once identified, staff members offered eligible participants a brief verbal description of the study, detailed written information, and the opportunity to meet with the researcher. On meeting with the researcher (first author), eligible participants received in-depth verbal information about the study and answers to questions raised. Prospective participants were encouraged to appraise the study information and to contact the researcher at a later date should they wish to proceed with being interviewed.
The interviews were conducted with consenting participants at a time and place of their choosing. With the assistance of an interview guide, participants were initially asked three open ended ‘grand tour’ questions (Spradley, 1979) that were designed to elucidate their experiences in relation to seeking asylum in Ireland, their mental health difficulties, and their interactions with mental health services: (1) Can you tell me about your experience of seeking asylum in Ireland? (2) Can you tell me about your experience of mental health difficulties? (3) Can you tell me about your experience of seeking support for your mental health difficulties?. While these three questions were used, participants were supported to maintain control over ordering, pacing, inclusion/exclusion of content, and emotional intensity of their narratives. Prompted by participants’ narratives, additional probing questions were then asked for clarity and to promote detailed, rich descriptions of the events recounted or appraisals proffered. Their narratives in relation to the open question on the content and impact of the distress they experienced are presented in this paper.
Consent and ethics
This study adhered to best practice guidelines for conducting research with forced migrants (Palmer, 2008, Hugman, Pittaway, & Bartolomei, 2011). Participants with limited literacy in English were provided with translated written materials and interpreters in the language of their choice. Further, an iterative process of verbal consent was adopted, in which participants were asked to provide verbal consent for each stage of the research process, including the location of the interview, the presence of their chosen interpreter, the topics of discussion, and which parts of the discussion were and were not audio-recorded. The study also adhered to standard ethical practices of confidentiality and safety by anonymising all data at the source, by allocating pseudonyms to all participants, and by securing the storage of data in accordance to data protection legislation. In addition, the well-being of participants was safeguarded by pre-planned safety protocols and efficient referrals to participants’ named mental health support service in the event that they became distressed over the course of the research process. Ethical approval for the study was granted by the Trinity College Dublin’s Faculty of Health Science Ethics Committee (App#8) and by the Research Advisory Committees of the two mental health support services.
Study sample
In total, 16 African asylum seekers were interviewed: nine were female and seven were male (Table 1). The African asylum seeker population was chosen in light of the large representation of African nationalities amongst asylum seekers in Ireland at the time of data collection. Of the 16 participants, their countries of origin included Democratic Republic of Congo (n = 6), Zimbabwe (n = 2), Sudan (n = 2), Nigeria, Somalia, Ethiopia, Togo, South Africa, and Cameroon (n = 1 each). The duration of their time awaiting a decision on their asylum application ranged from 15 months to nine years. All the participants resided in direct provision accommodation and all were accessing mental health support services. All but one participant consented to their interview being audio-recoded.
Participant profile.

Data analysis
Lieblich and colleagues’ (1998) holistic-content approach to data analysis was used as a guiding analytical framework. NVivo (Version 10, 2014) was used as an assistive coding mechanism to data analysis. Global themes were first identified through repeated readings of transcribed interviews, which were then comparatively appraised for consistency within and across each participant’s narrative. Overall impressions of the text were documented and initial themes and foci highlighted. Instances of contrast, exceptions, and contradictions to the global themes were identified and informed a recategorization of themes and subthemes. Interpretative bias was reduced via in-depth discussions of the themes and data with the second and third authors throughout the analytical process.
Results
Data analysis identified four overarching themes in participants’ descriptions of their mental distress: (1) relentless rumination; (2) shame and self-loathing; (3) anger and mistrust; and (4) becoming hopeless and demoralised. Tables 2 to 5 present selections of participants’ statements from the interview that most effectively capture and articulate these themes. The authors reached consensus on the inclusion of these quotes as representative of the themes.
Relentless rumination.

Shame and Self-loathing.

Anger and Mistrust.
Becoming hopeless and demoralised.
Relentless rumination
Relentless rumination and its impact on the physical and mental well-being was a core aspect of the participants’ daily experiences. Many of the participants spoke of how their thoughts, actions, and behaviours were consumed and controlled by an unstoppable and uncontrollable sequence of negative thought patterns. The content of their rumination included reliving their traumatising past (A.1 and A.2) and worry about their insecure present and uncertain futures (A.4 and A.5). Subjected to extreme trauma in their home countries, many of the participants recalled how these experiences were etched into their memories and repeated over and over in their minds (A.1). The re-experiencing of traumatic memories was at times prompted by external stimuli that were associated with past events, such as seeing a policeman or other figures of authority (A.2). Their excessive rumination was also fuelled by uncertainty about the safety of family and friends who remained back in their home countries. Unable to contact them, participants described how their concern for them and about what may have happened to them enveloped their thoughts every day (A.3). Further compounding their rumination were overwhelming worries about their precarious present situation (A.4) and uncertain futures (A.5). Having received deportation orders and/or watching the sudden deportation of their peers, participants described the anxiety that they experienced, living in fear of being deported, visualising various permutations of negative events that might occur on their return home, and surmising the detrimental consequences for their families.
Descriptions of headaches and disturbed sleep patterns were particularly frequent in participants’ narratives (A.6 and A.7). They recalled the embodied physical and emotional anguish that they would feel because of painful headaches, with one participant describing this experience as his brain feeling so hot and full of worries that he felt as if it was boiling over with thoughts (A.6), and another stating that the overwhelming pain induced in her a desire to die (A.7). Many of the participants recounted that their relentless rumination did not stop at night-time, but instead seeped into their dreams in the form of nightmares and flashbacks (A.9, A.10 and A.11). As a result, they described their difficulties in achieving regular sleeping patterns and the physical and mental exhaustion they consequently endured (A.8, A.9 and A.10). Participants also recalled that they often felt so distracted and disoriented because of their relentless rumination that their ability to do anything or talk to anyone was compromised. They recalled that they felt anesthetised to the outside world and oblivious to their external surroundings. As a result, some of the participants often found themselves in locations with no recollection of how they got there or had stepped out on the road in front of oncoming traffic (A.11 and A.12). For the vast majority of participants, their relentless rumination became so all-encompassing that they began to vocalise aloud their worries repeatedly, some for hours on end (A.13, A.14 and A.15).
Shame and self-loathing
The participants’ narratives indicated that they were experiencing feelings of shame and self-loathing. They believed that they were unwanted, unworthy, and devalued to the community and, as such, experienced extremely low self-esteem and negative self-perception. Many of the participants expressed feelings of guilt for the situation in which they found themselves, harshly criticized themselves, and seemed unreasonably angry with themselves. For example, some displayed intense shame regarding their asylum seeker status and their limited capacity to achieve life goals and/or improve their quality of life in Ireland (B.1). Others chastised themselves for being away from family and for not being able to assist them (B.2). Many of the participants also implemented self-imposed isolation. They recalled that they often endured long periods during which they did not leave their hostel room and did not talk to or see anyone (B.3). For some, their self-imposed isolation appeared to be influenced by a desire to avoid interactions in which their negative self-perception would be reaffirmed. These participants spoke of their desire to avoid the judgement, negativity, and glare of the outside world and of their belief that they no longer fitted in with society (B.4 and B.5). For others, interactions with people outside of direct provision acted as reminders of what their life could have been, particularly in relation to family life and career opportunities. In these instances, they carefully orchestrated their interaction with the outside world to short periods of time, after which they swiftly retreated back to their direct provision residence (B.6).
Anger and mistrust
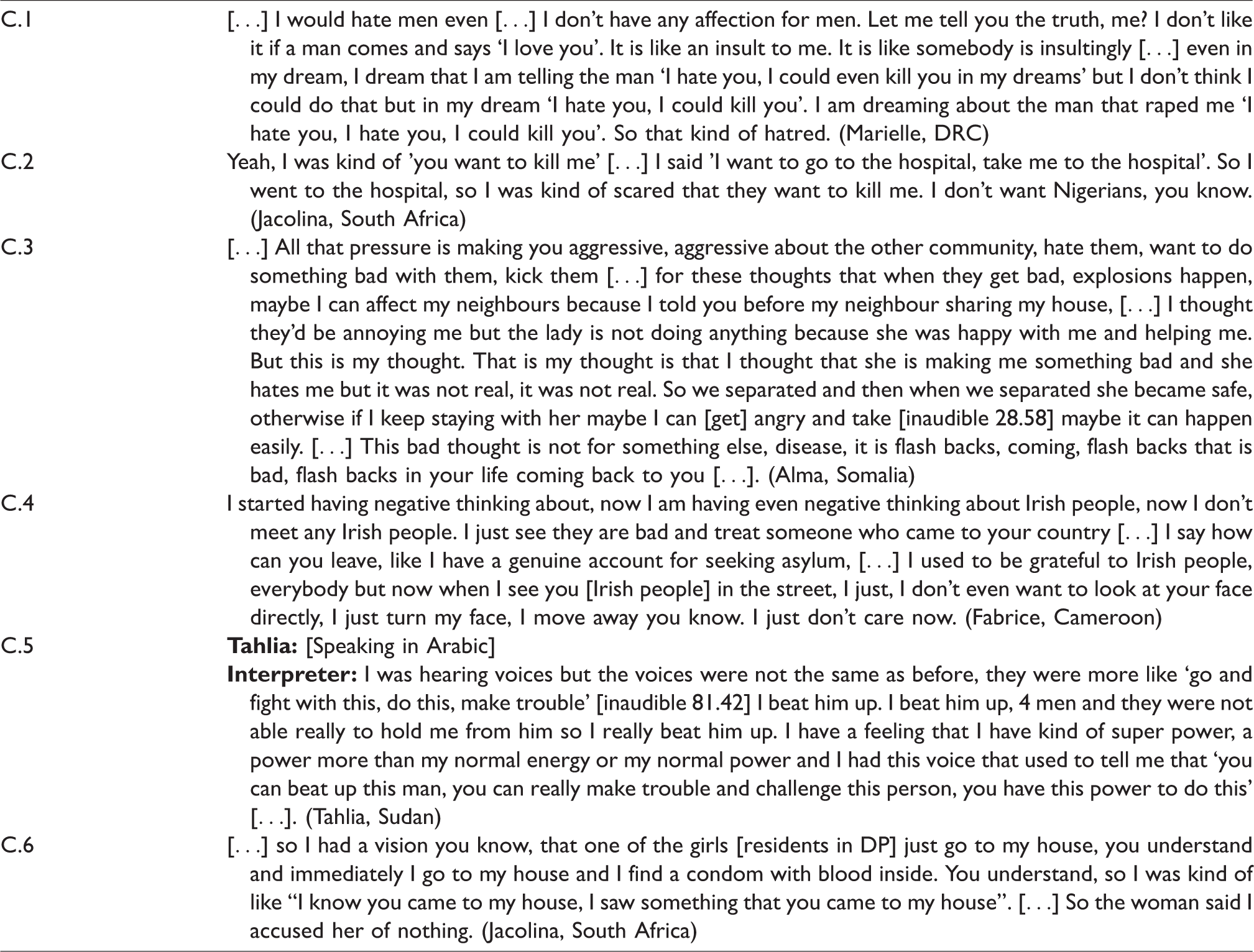
Intense feelings of anger and mistrust were also evident in the participants’ narratives. In some cases, participants’ feelings of anger and/or mistrust were apparent as they shared how their anger stemmed from events that had occurred in the past and that now appeared to have a detrimental impact on their current relationships (C.1 and C.2). For others, the pressure of post-migratory conditions in Ireland fuelled their anger and mistrust towards others (C.3 and C.4). In these instances, participants’ sense of belonging had deteriorated and, in their belief that the Irish community hated them, they began to reciprocate these feelings. For other participants, their feelings of anger and/or mistrust could be observed in the content of their perceptual and auditory experiences (C.5 and C.6). Interpersonal relationships consequently suffered, often becoming volatile, as participants’ feelings of fear and distress increasingly developed into overwhelming waves of intense frustration, anger, and suspicion.
Becoming hopeless and demoralised
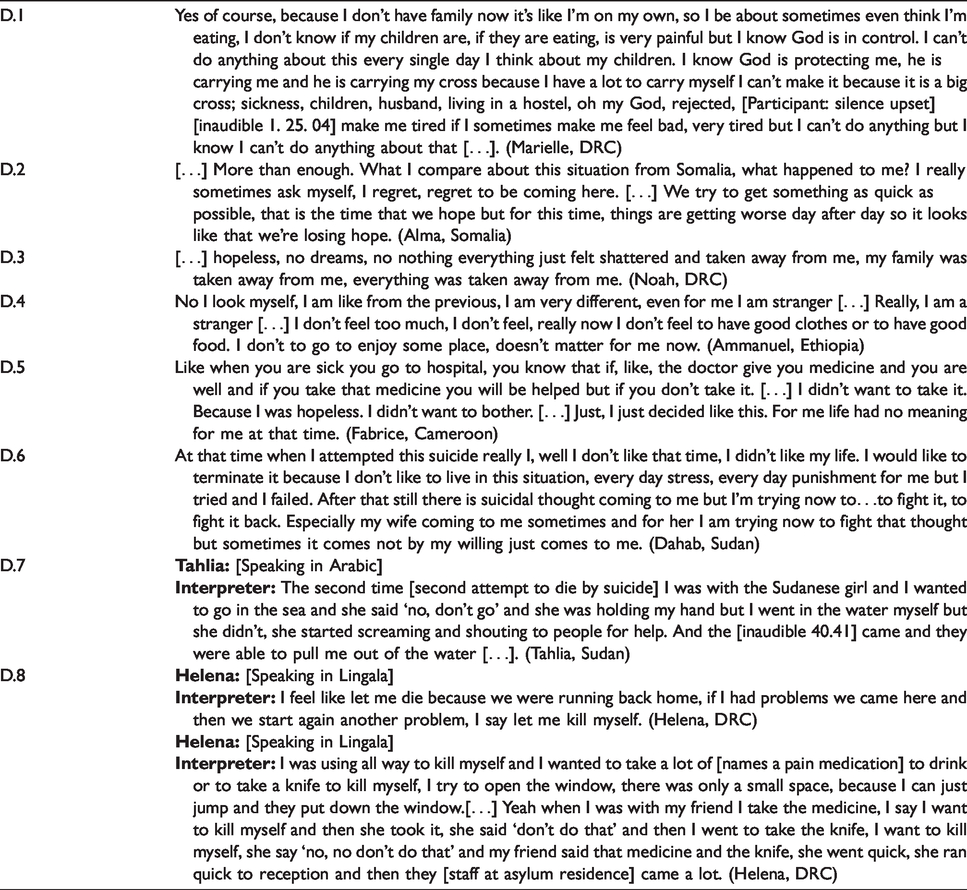
While all the participants’ narratives illustrated the depletion of their sense of hope, a noteworthy proportion of the study sample (n = 6) appeared to have reached the point of demoralisation and devastating hopelessness. Their lives, both in their home country and in Ireland, had experienced an overwhelming amount of trauma and sadness. As a result, many of the participants struggled to perceive positivity in their lives, either presently or in the future. The numerous challenges presented to them were perceived as insurmountable and participants described feeling overwhelmed and hopeless as a result (D.1, D.2 and D.3). Many of the participants had become extremely demoralised and they deemed efforts to improve the quality of their life as futile (D.4). One participant even questioned the rationale for taking the medication that had been prescribed for his mental health issue. He reasoned it illogical to attempt to feel better because he perceived his life as having little worth or meaning (D.5). Participants’ demoralised state appeared to extinguish any remaining value or worth that they ascribed to their life. They described reaching a point of utter hopelessness and consequently spoke of their attempts to end their distress by taking their own life. For many (n = 6), dying by suicide was perceived to be the only option available to them which could end their suffering (D.6, D.7, D.8 and D.9).
Discussion
The aim of this paper was to explore African asylum seekers’ everyday embodied experiences of mental distress. By delving beyond the confines of diagnostic categorisations and symptomology, the findings that we report here provide detailed and holistic insight into the contextual realities of experiencing mental distress while awaiting asylum outcome. Study findings indicate that asylum seekers’ mental distress interweaves the physical, psychological, emotional, and social realms, thus impacting the whole of their being. The findings not only reaffirm the mediating impact that pre- and post-migratory conditions can have on asylum seekers’ mental health (Silove, Ventevogel, & Rees, 2017; Li et al., 2016; Carswell, Blackburn, and Barker, 2011); they also highlight the complex interplay between pre- and post-migratory traumas and their cumulative effect on asylum seekers’ mental distress.
In this study, participants recounted their reliving of pre-migratory trauma through flashbacks, hallucinations and nightmares; experiences consistent with symptomology ascribed to the diagnostic category of PTSD (American Psychiatric Association, 2013) and that have attracted significant quantitative examination in research on forced migrants (Thompson, Vidgen, & Roberts, 2018; Nosè et al., 2017; Bogic et al., 2015). Participants descriptions of somatic complaints, including weakness of body, brain heat sensations, brain pain, and headaches (Morina et al., 2017; Spiller et al., 2016), alongside the previously identified insidious elements of the post-migratory environment, such as the uncertain nature of the asylum process and the pressurised environment of reception conditions (Li et al., 2016; Laban et al., 2004, 2005; Lamkaddem et al. 2015; Mueller et al. 2011; Ryan et al. 2009; Silove et al. 1997, 2000, 2007), can also be observed in participants’ descriptions of their distress in this study. Examining each aspect of participants’ distress in isolation from one another might cause us to overlook the relationships between them and their cumulative effects on asylum seekers’ mental health in the post-migratory domain. This study’s narrative methodology has enabled us to capture a more holistic understanding of how the participants mental distress, and the complex interplay between pre-and post-migratory trauma, are experienced in the post-migratory context of seeking asylum and living in direct provision. Such a detailed understanding of the context within which asylum seekers’ trauma manifests and the pragmatic implications that are consequently experienced can contribute to the design and efficacy of therapeutic engagement and interventions.
There were aspects of participants’ narratives, specifically their narratives around shame and anger, which are less explored in extant forced migrant mental health research and yet provide lucid additional insight into the everyday embodied experience of distress for asylum seekers. Participants’ narratives of anger, towards themselves and others, cogently illustrate the intensity and visceral manifestations of their distress, as incessant and protracted feelings of fear, rejection, and shame fuse and stimulate potential waves of volatility. Inextricably entangled, participants’ disclosures appeared to also indicate that their post-migratory lives were filled with intense feelings of shame, worthlessness, and self-directed anger with regards to their asylum seeker identity. The degree of self-loathing experienced was so intense that many participants physically, emotionally, and intellectually withdrew from society and enforced self-imposed isolation. The detailed intensity of participants’ narratives about their anger and shame have attracted limited discussion in research to date, yet the findings of this study suggest that the incessant presence of such feelings have the potential to consume asylum seekers’ wellbeing and thus significantly exacerbate their distress.
The themes of hopelessness and futility reflect what has been called ‘demoralisation syndrome’ (Hocking & Sundram, 2015). Proctor and colleagues (2018) coined ‘lethal hopelessness’ for these feelings to denote the complex web of inter-related indices informing self-harm. To date, research examining self-harm and suicide in asylum seeker populations has primarily relied on information that was originally recorded in medical and legal reports and have consequently only cited diagnostic and asylum outcome indices as primary determinants of self-harm and suicide (Joshi & Warfa, 2014; Kalt, Hossain, Kiss, & Zimmerman, 2013; Goosen et al., 2011; Cohen, 2008; Dudley, 2003; Robjant, Hassan, & Katona, 2009). Of the 16 participants in this study, six disclosed that they had thought about or attempted to take their own life. In their appraisals of the reasons for their suicidal behaviour, participants cited separation from family, hopelessness and powerlessness for the future, and demoralisation because of their uncertain and pressurised post-migratory existence. While this sample is small, their narratives indicate additional precursors of suicidal behavior amongst asylum seekers that remain unexplored and thus warrant further examination.
Implications and recommendations
Viewed through a medicalised lens, aspects of participants’ experiences and/or behaviours could be interpreted simply as attributes of psychiatric symptomology; a perspective which potentially negates opportunities to implement effective support systems both in and outside of psychiatry. In contrast, participants’ narratives offer an alternative interpretation of their distress and contextualises the distress within their interconnected pre- and post-migratory experiences. In so doing, the emphasis moves away from what Bracken and Thomas call “euro-centric notions of dysfunction and healing” and towards a space open to an alternative context-centred response to asylum seekers’ distress, which casts the connections between social, political, and cultural realities as central to our understanding of and responses to ‘madness’ (Bracken & Thomas, 2001, p. 726).
Psychological reactions to adversity and devastating events represent an extremely individualised process that is mediated by a constellation of different factors. Summerfield writes: “Psychological trauma is not like physical trauma: people do not passively register the impact of external forces […] but engage with them in an active and social way” (Summerfield, 2000, p. 321). Understanding and responding to asylum seekers’ distress in a context-centred approach counters the trauma discourse that saturates societal perceptions of, and responses to, forced migrants, and instead promotes their resiliency. It may be argued that the recommended multisector, pyramidal, and phased approach to promote all forced migrants’ mental health and psychosocial wellbeing (Sneddon, 2018; Priebe, Giacco, & El-Nagib, 2016) reflects such a resilience-informed and context-centred approach. Complimentary to the Adaptation After Persecution and Trauma (ADAPT) model (Silove et al., 2017), such an approach equitably integrates an appreciation for interventions that are designed to strengthen protective factors and to address social determinants of wellbeing (such as safety, basic physical needs, income, employment and social integration), alongside one for more specialised targeted and therapeutic interventions targeted to those with particular mental health needs. To achieve a phased, pyramidal, and holistic approach to asylum seekers’ distress, integrated partnerships between community, primary care, and tertiary mental health services are necessary, and indeed, may be integral to ensuring effective referral and communication pathways between support services.
Within and across all preventative and curative interventions, the development and genuine enactment of cultural competency (Betancourt, Green, Carrillo, & Owusu Ananeh-Firempong, 2003; Bhui, Warfa, Edonya, McKenzie, & Bhugra, 2007; Kirmayer, 2012) and other culturally responsive strategies (Slobodin, Ghane, & De Jong, 2018; Hocking, Mancuso, & Sundram, 2018; Mills, Xiao, Wolitzky-Taylor, Lim, & Lu, 2017; Groen, Richters, Laban, & Devillé, 2017; Adeponle, Thombs Groleau, Jarvis, & Kirmayer, 2012; Hinton & Jalal, 2014; Kieft, Jordans, de Jong, & Kamperman, 2008; Slobodin & de Jong, 2015; Vincent, Jenkins, Larkin, & Clohessy, 2013) will be integral to ensure that differing worldviews and explanatory models of mental distress are adequately incorporated into treatment and research. Cultural competency needs to prioritise an openness and willingness to listen to, contextualise, and empathetically engage with asylum seekers’ distress, how they describe it, and what they believe may assist to alleviate it (DelVecchio Good & Hannah, 2015; Fisher-Borne et al., 2015). It also requires a willingness to integrate health pluralism (White, Sumeet, & Giurgi-Oncu, 2014) and incorporate therapeutic approaches that originate from outside of Western biomedicine, including diverse forms of indigenous medicine and traditional healing (e.g. Ayurveda, traditional Chinese medicine, and traditional healing in Africa), which may be responsive to asylum seekers’ source of explanatory health beliefs, and their related coping or help-seeking behaviours. It is through the work of genuine engagement that the identification and provision of a holistic support system may be secured, which will increase the acceptability and engagement with support services for asylum seekers.
Some aspects of our findings warrant future research. Research conducted with other populations has demonstrated that the social and psychological implications of self-stigma are substantial, and include low self-esteem, low sense of empowerment, low social support, low hope, poor adherence to treatment, and low subjective quality of life (Livingston & Boyd, 2010). The incidence and/or impact of self-stigmatisation in asylum seeking populations are rarely examined and so further exploration of the drivers and impact of asylum seekers’ shame and self-loathing, in addition to potential resolutions, is warranted. The study’s findings about asylum seekers’ self-harm also indicate that future research should consider the inclusion of asylum seekers’ subjective perspectives to ensure that a comprehensive assessment, understanding, and response to self-harm suicidal behaviour while awaiting asylum outcome is achieved.
Study limitations
This study’s narrative methodology facilitated enhanced contextualisation and thus also an enhanced understanding of the content, manifestation, and impact of asylum seekers’ distress beyond the limiting confines of diagnostic categories. Further, the contemporaneous nature of data collection strengthens the reliability of participants’ narratives, as they were experiencing mental distress during the time of data collection, rather than looking back retrospectively. However, the findings need to be considered in the context of the following limitations. The non-random sampling method is a limitation. The convenient sampling of participants through gatekeepers at mental health support services may have invited response bias into the study sample. For example, individuals who were more positively disposed to recounting their experiences and/or felt that their participation could influence the outcome of their asylum application may have been more likely to consent to participation. Further, the small study sample and the inclusion of only asylum seekers who had sought the assistance of mental health support services limit the generalisability of study findings. The scope of our study’s findings may have been impeded by the chosen methodology of unstructured narrative interviews. Increased bias may have occurred as a result of our using only one interviewer. Lastly, to avoid over-burdening participants, the collection of demographic information was minimal. The collection of additional demographic details may have provided the reader with a more expansive description of the study sample, which might have enabled better interpretation of the findings.
Conclusion
Participants narratives provide rich insight into the everyday embodied experience and impact of asylum seekers’ distress. These narratives emphasise that trauma and suffering threaten the whole of the person. As Cassell writes, “because humans are of a piece – whatever happens to or is done to one part affects the whole and whatever affects the whole affects every part” (Cassell, 2010, p. 51). Focusing therapeutic resources into codifying, diagnosing, and biomedical treatment of symptomology without due cognisance of the interdependent role and impact of asylum seekers’ socio-cultural and socio-political environments may prove to be ineffective in the long-term and risks their disengagement from potentially valuable therapeutic interventions and relationships. An integrated context-centred approach may provide the necessary scope for an enhanced understanding of, and empathetic engagement with, the contextual realities of asylum seekers’ pre- and post-migratory lives and consequently inspire adaptive therapeutic approaches with effective outcomes. The sustained efficacy of any therapeutic responses to asylum seekers’ distress, whether preventative, curative, or recovery-orientated, mandates a host countries’ creation of psychosocial sanctuaries which fulfil, rather than threaten, asylum seekers’ hierarchy of needs (Murphy et al. 2018). The findings of this study, alongside a nascent body of research (Li et al., 2016; Laban et al., 2004, 2005; Lamkaddem et al., 2015; Mueller et al., 2011; Ryan et al., 2009; Silove et al., 1997, 2000, 2007; Murphy et al., 2018), indicate that the reception conditions that are provided by host countries are experienced as hostile environments and have harmful effect on asylum seekers’ wellbeing. It is crucial that the toxic post-migratory contexts be redressed, and a foundation of security and safety curated in its place. Only then can asylum seekers begin to recover from their pre-and post-migratory experiences.
Footnotes
Acknowledgements
We would like to acknowledge all the participants and thank the staff of the two participating mental health services for support with recruitment and to the Health Service Executive’s National Social Inclusion Office for providing financial assistance for the employment of interpreters.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.