
Abstract
Research on mental health in specific communities requires careful attention to cultural context and language. Studies on global mental health have increasingly analyzed idioms of distress, or culturally situated ways of conceptualizing, experiencing, and expressing distress. This study examines how idioms of distress are used and understood in Arcahaie, Haiti. The goal was to enrich current understanding of mental health conceptualization and communication by exploring the heterogeneity of common idioms of distress. Interviews with community members (N = 47) explored meanings and perceived causations of 13 idioms of distress. Major themes included pervasiveness of poverty, ruminative thinking, effects of Vodou and Christian belief systems, embodied distress, and the behavior of “crazy” people (moun fou). The findings suggest some specific pathways for potential community engagement projects, including training lay-leaders in cognitive behavioral therapy using existing socioreligious infrastructure and expanding access to social engagement activities. This research contributes to a small but growing body of literature on mental illness in Haiti and to methods for studying idioms of distress.
Introduction
Understanding mental health is a complex endeavor because it involves familiarity with the biological, psychological, and cultural components of how people think of themselves and others. Biomedical psychiatry has developed complex, manualized heuristics for categorizing mental illnesses and their causes (Charlson et al., 2017; Lewis-Fernández & Kirmayer, 2019). Global mental health, despite focusing on expanding mental health care to low-income settings, is heavily influenced by etiologic systems developed in high-income countries (Charlson et al., 2017). However, fruitful engagement with local ethnopsychologies to create effective mental health interventions requires attunement to the ways distress is approached in a local context, which is often alien to biomedical systems.
Studying idioms of distress provides insight into a cultural group’s means of expressing and experiencing distress. The term “idioms of distress” was coined by Mark Nichter (1981) in his article on Havik women in South India. It was defined as “socially and culturally resonant means of experiencing and expressing distress in local worlds. They are evocative … [and] express personal and interpersonal distress beyond that associated with universal disease processes” (Nichter, 2010, p. 405; cf. Hinton & Lewis-Fernández, 2010; Nichter, 1981). Idioms of distress are effective and often non-stigmatized means of expressing distress (Kaiser et al., 2015; Nichter, 2010).
By arguing for the utility of idioms of distress, Nichter (1981) was also arguing against methods of cultural study that were primarily deductive and theoretical. Instead, idioms of distress offer an inductive and practical methodology. They permit culture-specific understandings of concepts like psychopathology (Den Hertog et al., 2016; Desai & Chaturvedi, 2017; Hinton & Lewis-Fernández, 2010) by emphasizing the importance of being attuned to the cultural context of mental health (Desai & Chaturvedi, 2017; Kaiser et al., 2015; Nichter, 2010). Careful study of idioms of distress can also yield “local conceptual frameworks” that allow for proper understanding of existing treatments (Kohrt & Hruschka, 2010, p. 323) and potentially yield novel approaches as well. This also prevents researchers from committing an “error of decontextualization,” which arises from discussing idioms of distress stripped of their cultural background (Den Hertog et al., 2016, p. 385; Hinton & Good, 2015). One example of this error occurred following a civil war in Liberia: many foreigners conflated the idiom of distress open mole with the diagnosis of posttraumatic stress disorder found in the Diagnostic and Statistical Manual of Mental Disorders (DSM) of the American Psychiatric Association (Abramowitz, 2010). 1
It is important to consider the relationship between idioms of distress and DSM diagnoses. For example, in a study of the Khwe of South Africa, the idiom of distress “thinking a lot” was shown to convey a variety of meanings, not all of which indicated pathology (Den Hertog et al., 2016). This finding suggests two points of caution. First is the risk of producing a “pidgin psychiatry” by incorporating these idioms of distress into clinical settings, meaning a psychiatry that is adapted for biomedical clinical contexts yet tied to its original context in name only (Abramowitz, 2010, p. 354; Den Hertog et al., 2016; Kaiser et al., 2014, 2015). Idioms of distress could become a laundry list devoid of deeper meaning (Kaiser et al., 2014; Kohrt & Hruschka, 2010).
Second is the fallacy of thinking that an idiom of distress is equivalent to a discrete diagnostic category (Den Hertog et al., 2016). On the contrary, a single idiom of distress can carry a variety of meanings even within a culture, depending on the setting (Kaiser et al., 2015; Mendenhall et al., 2019; Lewis-Fernández & Kirmayer, 2019). Recognizing the heterogeneity of idioms of distress is crucial for appreciating the varied meanings of those idioms of distress and understanding the way users of those idioms of distress approach mental illness. The recognition of heterogeneity and interpretation of a singular idiom of distress also helps to avoid exoticization and reification, which are common threats in research on cultural concepts of distress (Lewis-Fernández & Kirmayer, 2019). Other scholars have also noted problems with simplifying idioms of distress by claiming that they have one fixed meaning, a pitfall that risks conflating them with psychiatric syndromes (Abramowitz, 2010, p. 354; Den Hertog et al., 2016; Kaiser et al., 2014, 2015; Keys et al., 2012).
Researchers have demonstrated how idioms of distress can be successfully incorporated into clinical settings. Some have noted that idioms of distress can be useful as screening tools for identifying individuals in need of care (Hinton & Lewis-Fernández, 2010; Kohrt et al., 2016; Rasmussen et al., 2015; Weaver, 2017). In some instances, they might be sensitive for detecting signs of mental distress, although they are not diagnostically specific (Kaiser et al., 2014, 2015). Additionally, clinicians can use idioms of distress to communicate issues in a non-stigmatizing manner (Kaiser et al., 2015; Nichter, 2010; Weaver, 2017). For example, researchers noticed greater success in communicating with Nepali respondents using idioms of distress to discuss trauma associated with a recent civil war, while minimizing the stigma associated with such conversations, especially compared to biomedical terminology (Kohrt & Hruschka, 2010).
This is particularly important where idioms of distress emphasize social origins and resolution of distress, rather than transferring responsibility onto individual sufferers (Kaiser & Weaver, 2019). For example, the idiom of distress tension in North India locates the source of distress within a social situation (Weaver, 2017). Similarly, in Haiti’s Central Plateau, reflechi twòp (thinking too much) is a form of distress that can be tied to structural violence (Kaiser et al., 2014).
Study context
Haiti is a low-income country that occupies the western third of the Caribbean island of Hispaniola/Ayiti. A former French colony, it declared independence in 1804 after a slave revolt (Barthélémy, 1990). However, its sovereignty has been challenged since independence, and its internal affairs influenced by an influx of Christian missionaries, foreign governments and agencies (including the United Nations), and nongovernmental organizations (NGOs; Pierre et al., 2010). A major spike in NGOs followed the earthquake in January 2010 (James, 2011; Schuller, 2016). Most groups were dedicated to assisting recovery efforts and sometimes included a mental health component (Pierre et al., 2010).
There are few psychiatric services in Haiti. The closest professional mental health facility to our area of study was in Port-au-Prince, a two-hour drive. However, there is a broader culture and history of how Haitians understand and respond to psychological distress. These frameworks are influenced by biomedical psychiatry but also contain elements derived from Vodou and Christian belief systems. Vodou is a syncretic belief system that stems from West African and Roman Catholic traditions. It has dominated Haitian thought since the colonial era, when slaves incorporated practices from their homelands into the faith imposed upon them by French masters (Brown, 1991; Deren, 1953; Métraux, 1972). Various groups have attacked and stigmatized Vodou (Desrosiers & St Fleurose, 2002; Farmer, 1992; Métraux, 1972; Pierre et al., 2010; Vonarx, 2007). Vodou priests have been important leaders, as well as targets for persecution by anti-Vodou forces (Hurbon, 1979).
Vodou beliefs and rituals have long been mediated through a history of colonialism and continue to respond to different forms of imperialism. For example, the Rara street festival celebrates the ti nèg (“little guy”) who opposes domestic and foreign elites through Vodou and Christian symbolism (McAlister, 2002). Similarly, illness is sometimes believed to be caused by curses sent by others to torment victims (Brodwin, 1996; Vonarx, 2007). The attacker is often motivated by envy of another’s socioeconomic privilege, which is exacerbated by Haiti’s precarious economy. The image of a country rife with interpersonal disputation and violence feeds outsiders’ perception of Haiti as a barbaric place. That perception has been used by outsiders to justify (neo)colonial subjugation, thereby exacerbating the very conditions of structural violence that motivate curses (Kaiser & Fils‐Aimé, 2019; Vonarx, 2007).
Aims
This study extends work on idioms of distress in Haiti by exploring cross-regional consistency and variability of Haitian ethnopsychology vis-à-vis idioms of distress. Keys et al. (2012) demonstrated the utility of studying idioms of distress in the context of mental distress in Haiti. Their team interviewed community members in the Central Plateau region of Haiti about how they understood, used, and responded to different idioms of distress. Keys et al. (2012) noted how patients and clinicians differed in how they interpreted idioms of distress. For example, patients tended to invoke a mixture of cognitive-emotional and socially-based etiologies for some idioms of distress, while clinicians generally suggested literal interpretations and biomedical explanations of patients’ conditions (Keys et al., 2012).
The present study focuses on several communities in the Arcahaie arrondissement, a coastal district northwest of Port-au-Prince and home to several foreign religious NGOs. The goal is to compare local perceptions of idioms of distress in terms of causation, manifestation, and treatment. This study emphasizes the heterogeneity of idioms of distress both between different regions (i.e., in comparison to Keys et al., 2012) and within the same locale. Previous investigators have attempted to avoid simplifying narratives by conducting thorough multi-site studies that highlight the varying meanings of idioms of distress between sites (e.g., Kaiser et al., 2015). This study is motivated by a similar endeavor to compare findings between interviews in Arcahaie and others conducted in the Central Plateau by Keys et al. (2012). Further, this study contributes to this project by highlighting the within-site heterogeneity of idioms of distress, thus furthering understanding of how idioms of distress are used in different ways to describe psychological distress. A deeper and richer portrait of these idioms of distress can facilitate improved communication of mental health issues, which can help create effective interventions to address mental distress in Haitian communities.
Methods
We interviewed community members in villages in the Arcahaie arrondissement in partnership with Haiti Children, a US-based nonprofit orphanage and school with a large campus in Arcahaie. We conducted interviews in four locations: (1) the Haiti Children site; (2) Williamson, a town adjacent to the main highway that runs along Haiti’s western coast; (3) Doco 1; and (4) Doco 2, two villages in the mountains overlooking Williamson. The interviews took place during June 13–July 24, 2016.
Sampling intentionally targeted key informants such as teachers, pastors, nurses, social workers, other community leaders, and selected laypeople. All encounters were conducted with the aid of a local Kreyòl interpreter and in the presence of two American investigators. The interpreter provided real-time translations for questions asked by investigators and answers provided by participants. Participants were recruited via contacts from Haiti Children, the interpreter, and other participants, with an emphasis on recruiting community leaders.
Semi-structured interview questions explored 13 idioms of distress, delving into the nature of the idiom of distress, its etiology, behavioral and cognitive features, how sufferers are treated in the community, and the ideal means of alleviating the sufferer’s distress. The original list of idioms of distress was based on those studied by Keys et al. (2012). Pèdi bon anj (to lose one’s good angel) was dropped in the present study because it was deemed unfamiliar to most people in Arcahaie. Pèdi fey (to lose one’s leaves) and tèt pa dwat (head not straight) were removed because they were mostly used in a joking manner, rather than as a sign of mental distress. Kè bat fò (heart beating strong) was changed to the equivalent batman kè (heartbeat) since the interpreter determined that the latter term was more commonly used in Arcahaie. Two or three idioms of distress were chosen for each interview by a random number generator. Most interviews lasted for about 30 minutes, with a range of 19–65 minutes.
All interviews were audio-recorded and coded for major themes. The interpreter’s live translations of each interview were transcribed, with review and transcription of the original Kreyòl as needed to aid in interpretation. The idioms of distress and other key Kreyòl phrases were maintained in Kreyòl in the transcriptions. Codes were developed through reviewing transcripts until no new themes arose. Coders discussed how to code the interviews before independently coding each transcript. Codes were subsequently discussed to reach consensus.
Before interviews, all interviewees were informed of the purpose, content, risks, and benefits of the project, and any questions were addressed. Consent was obtained either by signing a Kreyòl consent form or by verbal affirmation. The research protocol was deemed exempt by the institutional review board of the Icahn School of Medicine at Mount Sinai and was approved by the mayor of Arcahaie (we sought out local counsel who determined that the mayor’s approval would suffice for a non-interventional study carrying minimal risk to participants). Following conversations with the interpreter and several trial interviews, the consent script, list of idioms of distress, and the survey questions were modified to better fit the local cultural context. This included modifications to decrease stigmatization that could accompany discussion of mental distress.
Results
Most participants were male and lived in Williamson (Table 1). A plurality of participants worked in education. Almost all identified their religion as some form of Protestantism. A minority had received some form of psychological counseling training; these were typically pastors and seminary students who received some counseling training in seminary.
Demographic characteristics of participants (N = 47).
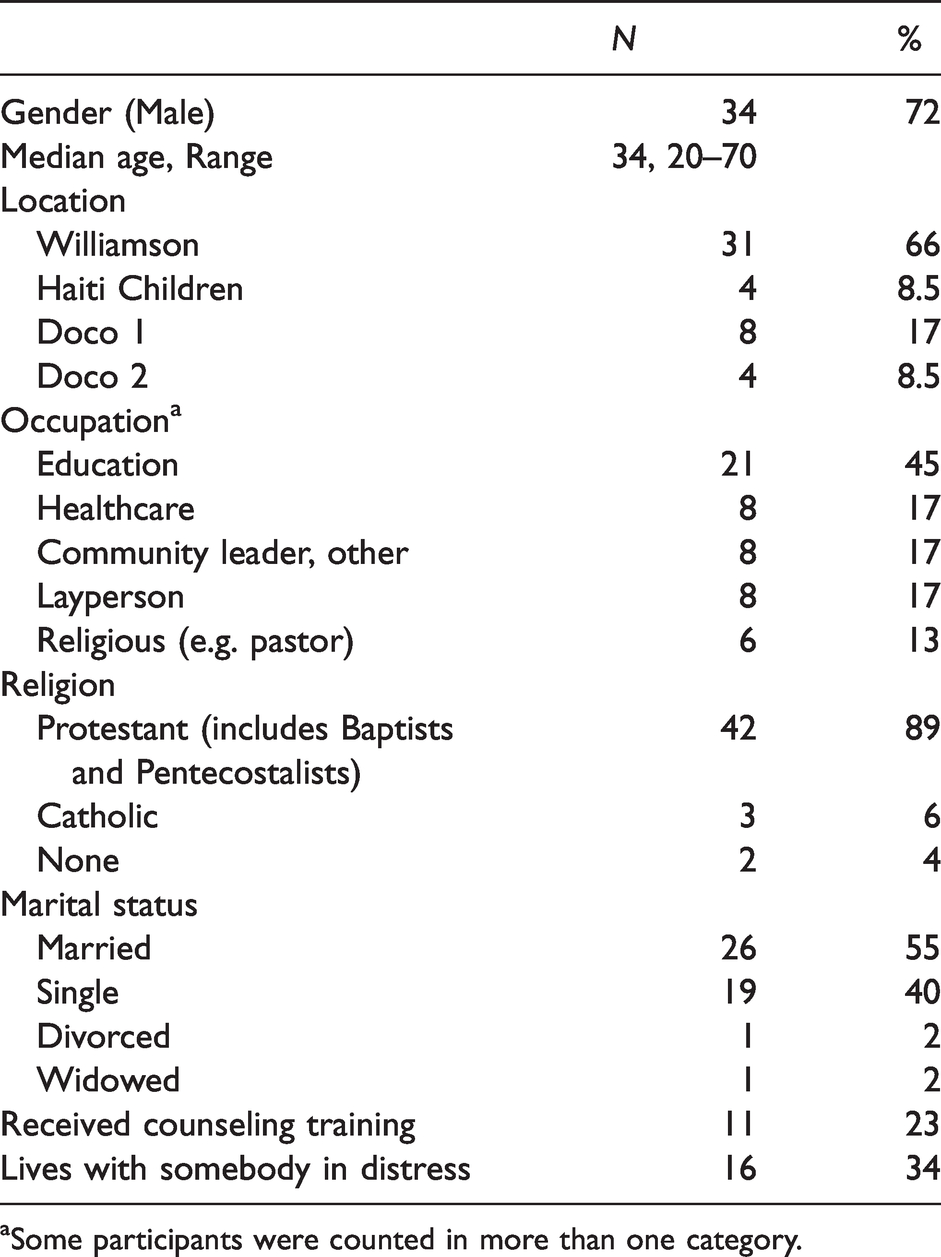
aSome participants were counted in more than one category.
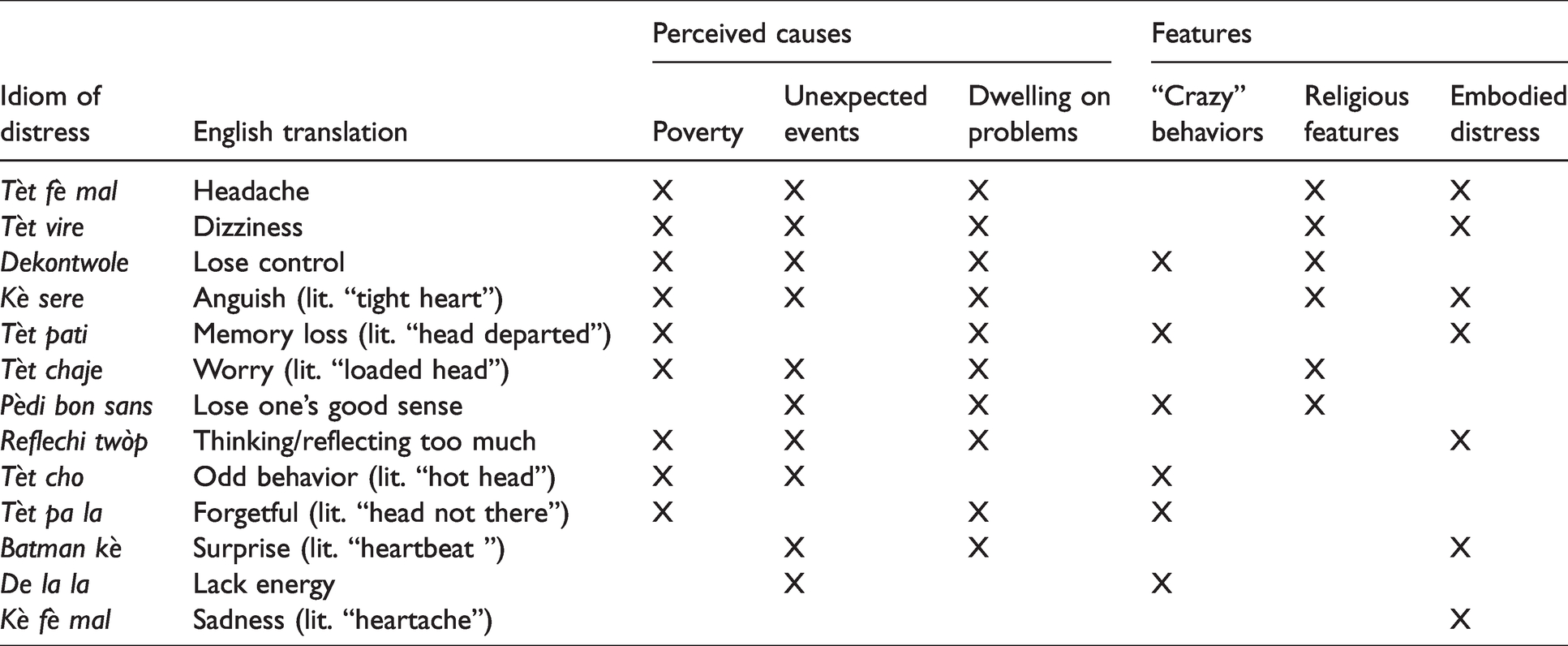
Themes derived from qualitative data focused largely on causation and features of mental distress, along with treatment. Table 2 summarizes major conceptual associations of idioms of distress in terms of their perceived causes and features. It demonstrates the heterogeneity of responses regarding possible causes by highlighting how each idiom of distress can convey a variety of meanings. For example, dekontwole is sometimes thought to be caused by poverty, unexpected events, or dwelling on problems. It was also associated with both symptoms of moun fou (“crazy person”) and religious features. Table 2 also demonstrates the overlapping features among many idioms of distress, showing how they defy neat classification. For example, many idioms of distress can be caused by poverty, unexpected events, and dwelling on problems. Behaviors associated with moun fou were given as features for many different idioms of distress. Below, we describe idioms of distress within these categories, as well as findings regarding appropriate treatment.
Idioms of distress: Heterogeneity of their perceived causes and features described in interviews (N = 47).
Causes of mental distress
Poverty
The adverse effects of poverty were described in association with most idioms of distress. Frequently a participant would say that “economic problems” could cause an individual to experience that form of distress. The most common example given was unemployment which resulted in hunger, inability to pay for their children to attend school, and inability to see a doctor or buy medicines. In some interviews, participants noted that reflechi twòp (thinking too much) is a form of distress that is widespread in their community and throughout Haiti due to poverty. One 60-year-old farmer from Doco 2 was asked if there was any way for individuals who experience reflechi twòp to get better. In response he said: You want a job, and you don’t find [one]. There is nothing for you to use to make money. Here in this community, people work for a day for 50 gourdes [1 USD]. That’s nothing. That causes the people in the community to reflechi twòp, almost everybody. Sometimes they don’t even have this kind of job to have 50 gourdes.
When participants described poverty as being the root cause of distress, they usually identified jobs or money as the most helpful things for alleviating distress. Other remedies included community members pooling their resources to help someone in financial trouble. Because the cause of distress was economic in nature, it was suggested that only an economic solution could provide any help, both for reflechi twòp and tèt fè mal.
Unexpected and traumatic events
Another precipitant of distress was unexpected bad news or a traumatic event. The most common type mentioned was the death of a loved one. Other types that were frequently invoked were getting into an accident, losing a job, and receiving a bill from a child’s school that cannot be paid.
One notable adverse event that was mentioned multiple times was the 2010 earthquake, often referred to as “January 12.” Many participants knew people, or knew of people, who were severely affected by the earthquake. Five idioms of distress were described as associated with the earthquake: de la la (lack energy), tèt pati (memory loss), tèt pa la (forgetful), pèdi bon sans (lose one’s good sense). Referring to a possible cause of pèdi bon sans, a 32-year-old teacher in Williamson said: “After January 12 there were many people who pèdi bon sans because they didn’t function the way they used to before.” When that teacher was asked about how he would respond to someone who was exhibiting the signs of pèdi bon sans, he said he would refer that person to a psychologist, although he acknowledged that he did not know where the nearest psychologist was. He also added that others in the community might mock such a person.
Ruminating on problems
Many idioms of distress were associated with dwelling on problems afflicting an individual. The idiom of distress most obviously associated with this problem was reflechi twòp, (thinking/reflecting too much). However, reflechi twòp was sometimes the cause of other forms of distress as well. For example, a 43-year-old pastor from Williamson described the physical manifestations of tèt pati as follows: “When that person reflechi twòp about [being] jobless, that problem [tèt pati] can act in his body. In that time, you see that person has lost weight; he’s become thin, bony.”
Other times, a form of distress was said to have been caused by rumination without explicitly referring to reflechi twòp. For example, a 33-year-old nurse from Williamson said she could identify someone with kè sere (anguish) by seeing “that person sits somewhere, and that person is like miles away,” which is also a typical description of reflechi twòp.
Obsessive thinking was often described as when an individual intensely thinks about their specific stressor and wonders how they will cope. Other participants suggested that a state of deep thinking was caused by hearing unexpected bad news. Some participants associated deep thinking with the state of mind of a moun fou. These characteristics were sometimes causally linked: an individual may hear unexpected bad news, which causes her to experience reflechi twòp, which in turn causes her to become fou.
When asked how these individuals could be helped, participants often advised establishing dialogue with them, ensuring they have a social support network, and providing means of relaxation through hobbies or communal activities. The express aim of these interventions was to distract the individual from dwelling on their problems, thereby alleviating their mental distress.
Some participants suggested that anyone could establish dialogue with a sufferer. Others thought that community members should be specifically trained in how to counsel their peers. Many participants said that if the community had more resources, sending individuals to see a psychologist would be the best way to help those individuals because psychologists are ideally suited to analyze individuals’ problems and help them with their mental distress. The suggestion that a sufferer should see a psychologist was not more common among any subgroup of participants.
Many participants called for building a community center where everyone can engage in activities to relieve stress. Some examples were playing soccer, taking trips to the beach, or hobbies to help individuals relax. Many participants also suggested that having a hobby or establishing easily accessible communal activities could prevent mental distress.
Features of mental distress
Embodied distress
A common theme voiced by participants across many idioms of distress was the way in which a form of distress manifests with physical symptoms. The reverse was also common: physical ailments were frequently blamed for causing mental distress. Someone who is de la la may feel that they are physically weak. Kè fè mal (heartache) could be a sign of heart or stomach disease but also a sign of sadness. Tèt pati (literally, head departed) was often associated with high blood pressure. Tèt fè mal could be interpreted as gloominess or as a symptom of another disease. Someone who reflechi twòp sometimes shows signs of weight loss. Tèt vire (dizziness) was described as a type of weakness associated with vertigo, high blood pressure, and headache (one participant said it was like tèt fè mal, but with less severe pain). Batman kè was described by different participants as a variety of physical symptoms: rapid heartbeat, shortness of breath, pain, high blood pressure, weight loss, weakness, and even a heart attack. Kè sere (literally, tight heart), primarily described as occurring when someone is sad or anxious, was also associated with weight loss. There was little consistency among participants over whether an idiom of distress was primarily a physical symptom that caused mental distress or a mental problem that manifests as physical symptoms. The exception was kè fè mal, which most participants described as primarily a physical ailment.
Kè fè mal merits special mention as the only idiom of distress that was described by many participants in positive terms. Many interviewees associated it as sympathy, or pity, for the less fortunate in their community. Far from being a sign of distress, kè fè mal was sometimes described as a virtue. A 38-year-old nurse from Williamson described it as, “It’s like when something touches your heart, you feel sorry for something.”
“Crazy” symptoms
Many participants associated idioms of distress with a moun fou. Characteristics of a moun fou included strange behavior, throwing rocks at passers-by, rudeness, walking in the streets without clothes, crossing the street without looking, inability to control themselves, acting without knowing why, and inability to listen to advice. These features were consistent between participants describing different idioms of distress associated with moun fou. Respondents did not distinguish between mou fou-associated idioms of distress in terms of severity.
When asked how community members treated a moun fou, participants frequently reported that those individuals were harassed and teased by community members. Some community members were reported to take pity on those individuals, but those sympathetic responses were described as atypical. Some participants noted that harassment usually worsened the condition of the moun fou.
When an idiom of distress was associated with moun fou, the participant expressed that there was no way to help that individual. Some said only God could cure a moun fou. When asked how the community might help those individuals if the community had more resources, a common suggestion was to place those individuals in a restricted space where they could be supervised. Other participants identified such a space as a psychiatric center.
Spirits and religion
Forms of distress associated with moun fou were often associated with supernatural causation, specifically an ekspedisyon, which is essentially a curse. The community members in these Protestant-majority villages tended to speak about Vodou priests
2
with contempt and insisted that they themselves would never consult one. A moun fou was often assumed to be the victim of a curse, which only a return to Christian faith, with the help of a pastor, could cure. Vodou priests were invariably described as someone who would, at best, steal a supplicant’s money or, at worst, exacerbate the problem.
3
A 54-year-old Protestant veterinarian in Williamson was asked how a Vodou priest would treat someone experiencing a particular idiom of distress. He responded: The Vodou priest, what he does is bad … you have a fever and you are sick … you come to him, you trust in him, he’s going to do something to help you. Instead of giving you medicine to cure you he makes it worse to have more money from you.
Many participants reported that religious beliefs could cause or explain some forms of distress. A commonly invoked cause of distress was disobeying God by not listening to the Bible, or not believing in God or Jesus. Some participants stated that heresy, or following a heretical pastor, could have a similar effect. Participants reported that disobedience and disbelief are related to several forms of distress, including tèt fe mal, dekontwole, tèt vire, pèdi bon sans, kè sere, and tèt chaje (worry). Consequently, prayer and a return to proper Christian belief were frequently offered as means to alleviate distress.
Seven participants noted that sometimes too much religion could induce mental distress. These atypical religious effects came in two forms. One was when an individual becomes confused and distraught by the competing claims of different churches, associated with tèt chaje, de la la, dekontwole (in this context meaning inability to concentrate), and kè sere. For example, a 36-year-old gardener from Doco 1 explained the religious aspect of tèt chaje as follows: “Every church has its own way of understanding the Gospel … That can cause tèt chaje because many, many people are saying different things.” Another form was religious fervor or spending too much time studying the Bible, associated with de la la, tèt pati, tèt vire, and pèdi bon sans.
Medicine and community as cures for mental distress
For each idiom of distress, participants were asked what they thought could treat that form of distress. Without exception, each idiom of distress was described by some participants as treatable by medicine prescribed by a doctor. Some participants insisted that some forms of distress—particularly those associated with moun fou, Vodou spirits, or God—were beyond medical help. In other cases, particularly when an idiom of distress was associated with moun fou, some participants stated that medicine would at least help a person “calm down.”
A common refrain among participants was a desire for a medical center where physicians and medicine could be easily accessed (none of the communities had a clinic that was open daily). Despite the frequent invocation of physician expertise for addressing mental distress, none of the participants explained idioms of distress in a manner consistent with a biomedical model of disease (except for the sole physician who was interviewed).
The most common non-medical remedies mentioned by participants were drinking tea or making a headband of tealeaves. This was suggested for kè fè mal, tèt vire, pèdi bon sans, and batman kè. For example, a 70-year-old pastor in Williamson was asked how he would advise someone who was experiencing kè fè mal, and he responded, “Go to see doctor. But if they don’t have possibility to go and see doctor, they go and get tea, take the leaves and boil it.”
A couple of pastors spoke of youth groups they founded where community members were trained in how to approach individuals who appear to be in distress. Group members were taught to counsel these individuals and seek means to address their troubles.
Discussion
This study examined how idioms of distress are understood and used in the Arcahaie region of Haiti. We found that idioms of distress were not exclusively associated with any single cause or feature of mental distress. Rather, each idiom of distress was identified with a variety of causes and features by different participants, and specific causes and features related to numerous idioms of distress, thus demonstrating the heterogeneity of each idiom of distress even within the same community. For example, some participants associated ostensibly socially-based idioms of distress with moun fou, such as when dekontwole was associated with poverty by some participants and by others with a curse that made an individual into a moun fou. Other participants noted that dekontwole may be caused by reflechi twòp. Additionally, about half of the idioms of distress were described as indicative of both mental distress and physical health problems, depending on the context. Together, these findings speak to the heterogeneity in meaning of idioms of distress in terms of individual idioms conveying multiple meanings. Scholars have argued that idioms of distress should not be reduced to psychiatric diagnoses (Abramowitz, 2010; Hinton & Lewis-Fernández, 2010; Kaiser et al., 2015; Kohrt & Hruschka, 2010). It is likewise important that these complex concepts not be oversimplified to reflect only one among a multitude of meanings.
Another significant finding from our interviews is a relative divide between descriptions of idioms of distress that could be glossed as “crazy” versus those describing other forms of distress. The first type of description of idioms of distress was associated with moun fou, and many participants thought that little could be done. There was a strong stigma against this condition: individuals with it were often seen as irksome and best avoided (cf. Kaiser et al., 2013; Keys et al., 2012). These descriptions often involved a recent curse or lapse in religious piety. In contrast, the second type of description of idioms of distress was in relation to economic or interpersonal problems whose root causes could be ascertained by carefully questioning the distressed individual. There was little stigma against such individuals. On the contrary, many participants reported that it was common for neighbors to notice those types of suffering and offer to help. Here, too, the heterogeneity of idioms of distress is highlighted by demonstrating the overlapping meanings and features of different idioms of distress.
Many of this study’s findings are consistent with the findings in Keys et al. (2012). Among the idioms of distress that were common to both studies, respondents in both studies provided a range of physical, psychological, and social explanations for how they are used and what types of conditions they reference. Respondents in both studies also offered different ideas of how to resolve psychological distress. These similarities substantiate the heterogeneity of idioms of distress between geographical regions. One difference between our findings was that respondents in the present study placed greater emphasis on biomedical solutions, such as seeking the assistance of health care professionals or taking pharmacologic medicine. In their investigation of “thinking too much,” Kaiser et al. (2014) found few participants recommended pharmacologic therapies. Participants in the present study may have emphasized biomedical treatment because of social desirability bias: participants hoped that after an interview with foreigners they would have increased access to biomedical treatments. Another reason for the emphasis on biomedical treatments could relate to the occupations of most of our participants: Haitians working in health care and education may be more likely to recommend biomedical treatment than those in agriculture or fishing. The latter group was underrepresented in our study but is more representative of rural Haitian communities. Alternatively, the difference might reflect a regional difference in interpretation and response to idioms of distress.
Implications for interventions
Our findings suggest several areas for potential intervention to alleviate mental distress, either through prevention or treatment. One frequently invoked cause of mental distress was pervasive poverty. Another commonly invoked theme was the effect of trauma on mental distress, whether economic, interpersonal, or from a natural disaster. Many participants said that distress associated with traumatic events could not be prevented because it was impossible to predict when something bad would happen.
Nevertheless, many of those events are the predictable results of entrenched and widespread poverty. Future interventions focused on mental health may benefit from preventing adverse effects from prior or ongoing stressors to help community members avoid the downward spiral that often follows psychological trauma. Future investigators should also consider whether non-psychological efforts, such as reducing unemployment or general poverty, may be effective in alleviating mental distress. Systematic reviews indicate that efforts to reduce mental illness via poverty reduction are equivocal, while mental health interventions consistently show positive effects for poverty (Lund et al., 2011). A comprehensive approach is likely the most effective for addressing both issues.
A possible psychotherapeutic approach to addressing some idioms of distress could be cognitive behavioral therapy (CBT), a treatment modality that emphasizes the correction of maladaptive thought processes. There is some evidence that CBT may be particularly useful for reflechi twòp, an idiom of distress characterized by preoccupation or obsession with certain thoughts (Kaiser et al., 2014). Other evidence supports using CBT in addressing ataque de nervios among some Latino populations, khyâl attacks among Cambodians (Hinton et al., 2010), and heart–mind idioms of distress in Nepali and Bhutanese communities (Murray et al., 2011), and it is commonly recommended as treatment for “thinking too much” idioms of distress (Kaiser et al., 2015). Because reflechi twòp was often described in our study as a cause or feature of other idioms of distress, this might be a helpful focal point to alleviate distress associated with several idioms of distress. An additional advantage is that CBT can be administered by trained laypeople in settings such as Haiti that have few mental health professionals (Hoeft et al., 2018; Kaiser et al., 2014). We found some evidence of current efforts to train community members to act as mental health counselors in Williamson. While CBT appears to be a particularly appropriate fit in this context, we would caution against applying this therapeutic approach to all forms of distress. Instead, research grounded in understanding local concepts of distress should be used to identify the most appropriate treatment modalities in each setting.
Another approach mentioned in many interviews was community activities, often framed as distracting individuals from their suffering. This suggests an opening for community engagement projects in partnership with existing civic and religious groups that could serve as both a way to prevent distress and to alleviate existing distress. Such activities might build on the long history of community engagement through konbit, a form of collaborative community activity aimed at achieving a common goal (Keys et al., 2015). Because not all communities will have the resources to develop and sustain these approaches, they should receive funding and logistical support alongside therapeutic programs. Research from Haiti and other contexts confirms that activities aimed at distraction and social engagement are a common response to thinking too much (Kaiser et al., 2015). However, respondents elsewhere in Haiti have said that such projects bring limited relief, since the underlying causes of thinking too much (e.g., unemployment, food insecurity) remain unaddressed (Kaiser et al., 2014). This suggests that structural interventions aimed at addressing the root causes of distress are needed as a more lasting remedy for mental distress (Kaiser et al., 2014; 2015).
Another finding of these interviews is the influence of biomedical treatment modalities on participants in this study. We noted that many participants mentioned that a psychologist might help sufferers by talking to them. Our participants may have learned about clinical psychology from local NGOs (cf. McLean et al., 2015) or from the influx of mental health professionals who came to Haiti in the wake of the 2010 earthquake. Participants appeared to evince some familiarity with psychotherapy in general but not with any specific forms of psychotherapy, which could indicate that participants were sharing what they had heard from NGOs and researchers. The participants who spoke of the need for psychologists were implicitly suggesting that there was little anyone could do for most individuals suffering from severe mental distress since there were no psychologists near their villages. The deference given to specialists trained with biomedical treatment modalities also extended to medications. While many participants spoke of folk remedies for some forms of distress, none were as commonly invoked as the efficacy of medications. The frequent mention of biomedical treatment modalities could be influenced by a social desirability bias when answering questions from foreigners. Similarly, the repeated wish for a medical or psychiatric center to help community members with mental distress could reflect the hopes and aspirations that the study participants had for what would follow a visit from foreign researchers. At the same time, deference to biomedicine is widespread in Haiti, demonstrated by the colloquialism apre Bondye, se doktè (after God is the doctor).
While this study did not examine the origins of how these biomedical modalities became popularized in Arcahaie, these findings are consistent with literature on the syncretic nature of Haitian religion. Vodou has long been a point of conflict in Haiti. Its syncretism is a result of centuries of coerced foreign influences, including French colonial rule, oppressive Haitian regimes who relied on foreign powers for their own legitimacy, and Christian mission groups. To survive, Haitian culture has had to integrate disparate cultural influences into self-evolving and often conflicting identities distinct from external political and cultural powers (Barthélémy, 1990; Desrosiers & St Fleurose, 2002; Farmer, 1992; Khoury et al., 2012).
The widespread condemnation of Vodou practices among participants in the present study could, like the deference to biomedical treatment modalities, reflect a desirability bias to give “acceptable” responses to foreigners. This bias is likely accentuated regarding religious identity due to the stigma against Vodou from foreigners and domestic religious leaders, as well as the greater stigma among Protestants who make up almost all of our sample (Desrosiers & St Fleurose, 2002; Farmer, 1992; Keys et al., 2012; Khoury et al., 2012; Pierre et al., 2010). The representation of Protestants in our study was disproportionately high relative to Haiti’s population, where around 30% of residents identify as Protestant (Central Intelligence Agency, 2021).
Despite our overwhelmingly Protestant sample, it is important to note the central role that Vodou priests play in health and illness elsewhere in Haiti. So crucial is healing to Vodou traditions, one ethnographer wrote that “Haitian Vodou is a health care system” (Vonarx, 2011, p. 46) and priests have been known to employ a variety of rituals and rites, based in temples, to address various ailments (Brown, 1991; Deren, 1953; Khoury et al., 2012; Miller, 2000; Vonarx, 2011). Although the communities of our participants are unlikely to welcome relationships with Vodou priests, partnering with houngans elsewhere in Haiti may be helpful for community mental health projects. Vodou beliefs need not be a barrier to biomedical interventions (Khoury et al., 2012; Miller, 2000); however, planners should beware that Vodou priests may be more expensive than biomedical practitioners (Wagenaar et al., 2013).
A commonly suggested treatment in the present study for many types of distress was increased devotion to God and Jesus. However, most participants, including some pastors, believed that curses could cause genuine harm for individuals, often because a neighbor had beseeched a bòkò (sorcerer) to send a curse to that individual. Combined with the many mentions of the importance of seeing doctors and taking medicines, the culture in Arcahaie can be seen as its own syncretism of biomedical, Protestant, and Vodou belief systems. This suggests an openness to, and potentially significant role for, biomedical mental health practices in Haiti in conjunction with local understandings of mental illness.
However, clinicians and researchers must beware of the risks in relying too heavily on biomedical principles in treating Haitians. A clinician might be tempted to merely note when an idiom of distress is mentioned as signaling that a patient is experiencing a discrete form of mental distress. A researcher might directly inquire if an individual is suffering from an idiom of distress and interpret an affirmative response as evidence for the presence of a cultural syndrome, or something resembling a biomedical diagnosis. Such an approach exoticizes both the idiom of distress and the individual suffering from forms of mental distress unfamiliar to the inquirer. It decontextualizes idioms of distress since it ignores the heterogeneity of idioms of distress and the dynamic nature of how mental distress is expressed. Clinicians would do well to familiarize themselves with the language and culture of their target population to better communicate with their patients in destigmatizing and sensitive ways. Partnerships with community leaders must also be equitable to ensure that biomedical principles do not overwhelm and erase local understandings and practices related to mental distress.
Limitations
One limitation of our study is the reliance on an interpreter for translating all interviews from Kreyòl to English. This is a significant issue for an area of study where the nuances of language are crucial. We attempted to overcome this barrier by having our interpreter translate the interviews in real time and immediately discussing any issues in interpretation or understanding that arose, using Kreyòl audio recordings to develop transcripts, and retaining Kreyòl terms for idioms of distress and other key phrases in the transcripts. A different linguistic limitation is that we started with a set list of idioms of distress for this study. As a result, we may have missed some relevant idioms of distress that were not mentioned by any respondent (e.g., sezisman, seized-up-ness; James, 2011).
Another limitation is that the demographics of the participants were skewed in important ways. First, most participants were male and employed. Further, most of the participants lived in Williamson and were only familiar with the dynamics of that town. Finally, almost all participants were Protestant and all the clergy were pastors. This is a marked distinction from the rest of the country, where nearly 60% of residents identify as Catholic and/or Vodou (Pew-Templeton, 2010). Had we interviewed more women, unemployed individuals, Catholics, Vodou adherents, and their respective clergy, we may have heard different perspectives on mental distress, particularly as many of our respondents used religious reasoning and symbolism to explain different aspects of idioms of distress.
Conclusion
This study demonstrates heterogeneity in the ways people understand and respond to idioms of distress within and across regions in Haiti, which is important to attend to in mental health interventions. Our findings suggest some directions for future research: (1) continue to investigate idioms of distress and their heterogeneity across regions both within Haiti and other countries, (2) explore the feasibility and impact of training laypeople to be volunteer or paid mental health counselors using techniques such as CBT, (3) investigate what different rural communities in Haiti know about psychotherapy and how receptive they might be to psychotherapeutic interventions, (4) expand local forms of support such as youth outreach groups and church-affiliated community activities in Williamson identified through this study, and (5) further explore how religious beliefs and practices in different areas of the country affect the way communities understand and treat mental illness. Potential lines of inquiry could include conducting this study in a community where Vodou practice is dominant, examining how North American Christian communities affect how Haitians understand Vodou vis-à-vis different strains of Christianity, or further exploring how religious fervor can be a source of mental distress.
Footnotes
Acknowledgements
The authors wish to thank Sharon Barazani for assistance with preliminary research; Emma Shimony and Blean Girma for coding and analyzing interviews; the staff at Haiti Children for providing immense and crucial aid for each step of this study; and the many community members of Williamson, Doco 1, and Doco 2 for welcoming us and participating in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: BK was supported by a grant from the National Institute of Mental Health of the National Institutes of Health (grant number F32MH113288). MS and CK were supported by the Icahn School of Medicine at Mount Sinai. AL was supported by a grant from the New York County Psychiatric Society. KJ was supported by Haiti Children.