
Abstract
In this article, an anthropologist and a psychiatrist examine a Sufi shrine-based concept of affliction known as asrat (an “effect” in Hindi-Urdu, “difficulty” in Arabic) and related practices of healing in urban north India. Rather than being located in an individual body, asrat afflictions are shared, most often within a household or kinship group. Through surveys, clinical assessments, and ethnographic work, we track three different ways in which afflictions move between bodies, and the mechanisms at work in asrat healing processes. Rather than a “collectivist” concept of the psyche, we suggest that a key role of shrine-based therapeutic processes is to manage a “suspicion system,” related to experiences of psychic and economic injuries and conflict between intimates and kin. Through a multi-sited research design that moves across a leading Sufi shrine, an urban poor neighborhood in Delhi, and one of India's leading psychiatric facilities, we argue that within asrat-related processes, psychic vulnerabilities are addressed by “re-combining” relations through forms of inter-subjective attunement within a smaller segment of the kin group, potentially making symptoms and the burden of care and conflict more livable. We suggest that shrine-based concepts and practices may be cross-culturally significant, even for secular understandings of the inter-subjective dimensions of mental illness.
We begin with an excerpt from a conversation recorded at Badaun, a Sufi shrine in north India renowned for the treatment of maansik rog (mental/psychic afflictions). A Hindu couple from Delhi whom we will call Madhavi and Raj had been observing our research team, which included an anthropologist (Singh, co-author), a Sufi healer from Delhi (Sufiji), and a team of psychiatrists (led by Sharan, co-author). The couple expressed an interest in discussing their journey to Badaun: Singh: What kind of problem did you have? When did it begin?
Madhavi: It began 12 years ago, Mooh tedha ho jaana. Haath per tedhe ho jaana, gussa aana [My face, hands, feet got contorted, I would get angry].
[From her purse, Madhavi takes out tablets and outdated prescriptions of Clonazepam and Lithium, prescribed at different points of time by psychiatrists at the Institute for Human Behavior and Allied Sciences (IHBAS), a leading psychiatric facility in Delhi].
Madhavi: I had these medicines regularly. This one for six months and this other one for eight months, but it made no difference. They called me to IHBAS for lots of interviews, they helped as much as they could, and asked about all kinds of things from my childhood. Then they told me that there is nothing wrong with you.
Singh: Have you ever been to any other shrines? Balaji?
Raj: Yes, we went to Balaji. But there was no peshi [witnessing/healing] there.
Sufiji [interjects in a judicial idiom]: Balaji is a high court. This is a Supreme court. I have many cases [at the Badaun shrine] who are returnees from Balaji.
Raj [doesn't agree or disagree]: Because of Balaji …
Madhavi [completes the sentence]: A peshi [trance] did first happen at home.
Raj: But finally here at the Sarkars, the thing revealed itself fully, who did it, what it was.
Singh: So it was an asrat?
Raj: Yes, it was someone from home. It is always someone from home, never an outsider. The nearer they [relatives] are, the more dangerous they are.
Introduction: Asrat as a transcultural conceptual problem
In this article we, an anthropologist and a psychiatrist, return to a longstanding question at the intersection of our disciplines, namely religious healing. 1 Rather than being a culturally “bound” phenomenon, 2 we argue that the healing practice we investigate offers conceptual issues that are also relevant for secular, global understandings of mental illness. The ethnographic excerpt above contains the key issues we address in this article: the uncertain movement between treatment systems, which we trace through a multi-sited research design; the hierarchy of shrines (“Balaji is a high court, Badaun is a Supreme court”); the concept of affliction (“So it was an asrat?”); and the suspicion of proximates (“the nearer they are, the more dangerous they are”). Rather than analytically distancing these experiences as “sorcery” or rendering them too quickly legible in the language of faith, we seek to foreground the significance of a Sufi shrine-based concept of affliction known as asrat (an “effect” in Hindi-Urdu, “difficulty” in Arabic) and related practices of healing in north India.
We hope that our experience-near rendering of asrat in this article will contribute to emerging discussions of “cultural concepts of distress.” Like biomedical modes of classification, such concepts may be seen as having their own forms of rigor, consistency, and replicability (Lewis-Fernández and Kirmayer, 2019, p. 787). As outlined ahead, the concept of asrat includes a mode of etiological understanding, linked to particular practices and techniques of care and treatment that are replicated over time, often across large geographical distances in disparate shrines. As with current developments in psychiatric neuroscience in which disease categories are being fundamentally questioned and revised (Lewis-Fernández and Kirmayer, 2019, p. 790), “cultural concepts” too might exert pressure in contesting, revising, and refining biomedical understanding.
Perhaps the central aspect of the concept of asrat is that rather than being located solely in an individual body or brain, the affliction is conceived as transferrable across bodies, most often a household or a kinship group. Through surveys, clinical assessments, and ethnographic instances, we demonstrate three distinct modes of sharing an asrat affliction. 3 Firstly, through the movement of symptoms of mental illness between kin in ways that are also psychiatrically real; second, in the sharing of misfortunes that might include but are not limited to forms of mental illness; and third, in related but distinct illness trajectories within a household.
Crucially, we do not see these modes of sharing an affliction as entirely explained by the idea of non-western “porous dividuals,” 4 or as an expression of a distinctly collective “Indian” psyche (Kakar, 1982) as opposed to “western” individuality. Instead, we propose a more complex psychic mechanism at work in the practices surrounding asrat. An asrat, as we describe through instances below, often begins with a threat to existence arising from a disorder of intimate otherness, which may initially appear as a shaq (doubt/suspicion) or a kind of certainty in the perception of psychic and economic injuries and conflicts with intimates such as spouses, siblings, neighbors, kin, or business associates. “The nearer they are, the more dangerous they are,” as Raj puts it above.
How are asrat afflictions addressed? The answer we offer is in two parts, each of which involves understanding Sufi shrines as an “ecology of mind” (Bateson, 1972). As Bateson (1972) famously argued, an “ecology of mind” is best understood not through its boundaries but through its “arcs of circuits” (p. 145). In recent years, anthropologists have argued for the importance of thinking about mental illness as existing in biological and social circuits (Raikhel and Garriott 2013; Schull, 2006), for instance, an “institutional circuit,” as Kim Hopper calls it, that often forms in so-called advanced industrial democracies, between homelessness, supported housing, hospital, and jail, that creates a chronic condition of “social defeat” (Luhrmann, 2007) in ways that may serve to intensify symptoms. In our research context, our opening contention, as with Madhavi and Raj above, is that the circuit of treatment-seeking for mental health in contemporary India moves between hospitals, homes, neighborhoods, and shrines, often in no particular order. Within this ontologically discontinuous circuit, each point may have its own threats and possibilities for patients and caregivers, as emphasized in our examples below. Circuits can be religious and secular. Sufi shrines are often institutionally organized through genealogical networks linked to other shrines. 5 Further, shrines remain connected to rural and urban neighborhoods through healers and shrine representatives like Sufiji. Approaching a healer does not preclude simultaneous forays into biomedical care.
As such, rather than focusing solely on shrines, our research design aimed to investigate the conceptual and experiential implications of asrat, as this was expressed at different points in the circuit of mental health care: (1) in the psychiatry ward of a leading hospital in Delhi, where one of the co-authors (Sharan) is a clinician and faculty member; (2) in an urban poor neighborhood in east Delhi where Singh has been doing ethnographic work for the last three years, in particular living with a Muslim spiritual healer in this neighborhood; and (3) in a leading north Indian Sufi shrine of Badaun (in Uttar Pradesh, 5 h away from Delhi) renowned for the treatment of asrat. An asrat may express itself within a household in the form of pagalpan (madness), mansik rog (psychic affliction), shaq (suspicion), vehem (an unfounded doubt) pareshani (distress), chinta (worry), udasi (sadness), tenshun (tension), and other related terms.
In the first part of this article, we describe our anthropological and clinical findings moving across the contexts of clinic, neighborhood, and shrine. Within this movement, we retain the conceptual centrality of asrat, as the traversal of affliction across kin, and the healing ecology that a Sufi shrine offers, as the guiding theme of this article. Our multi-sited research design allows us to better understand how shrine-based healing may continue outside of shrines, in returning to an unsettled home, and further, how traces of the relational problem named by asrat may also be expressed in a psychiatric context.
Alongside circuits, a second conceptual link between asrat and the idea of an ecology of mind lies in “oikos” (dwelling space), the root word of ecology, resonant with our claim that asrat expresses and addresses disorders of intimacy within households and networks of relations, variably configured, rather than individual affliction. After outlining the three coordinates of the circuit, in the second half of the article we explore specific dynamics of affliction and healing more closely, through three ethnographic instances of treatment-seeking households, moving across different points in the circuit of mental health care. Through these three instances, we argue that shrine-based healing offers ways of managing doubt, suspicion, intimate injury, and periods of florid symptoms through a combination of cognitive, embodied, and emotional mechanisms that seek to bolster and “re-combine” relations (Strathern, 1992) through what we call inter-subjective attunement, typically within a smaller segment of the kin group. Further, we argue that rather than a one-off “cure,” shrine-based therapeutics are particularly attuned to the often long-drawn-out, relapsing, remitting tempos of mental illnesses, in ways that potentially make periods of florid symptoms and the burden of care and conflict more livable. That said, ours is not a simple affirmation of the efficacy of shrine-based cures. We remained equally interested in the experiences of treatment-seekers who reported failed visits to shrines, and movements back into psychiatric care, or movements between systems, as with Madhavi and Raj above.
The existing literature on shrine-based healing in India: Comparisons and emerging insights
This is an exciting moment in the study of shrine-based healing for mental illness, particularly in the case of India. There is by now a strong scholarly literature on several healing shrines across India, in some cases with repeat studies across generations of some of the best-known shrines such as the Balaji temple in Rajasthan (Dwyer, 2003; Kakar, 1982; Pakaslahti, 1998; Quack, 2014; Sax, 2014; Sood, 2016), the Mahanubhav temple in Maharashtra (Ranganathan, 2015; Skultans, 1987), as well as Muslim shrines and healing practices across India and Pakistan (Basu, 2014; Bellamy, 2011; Ewing, 1997; Flueckiger, 2006; Taneja, 2017).
A key point of consensus within the recent literature is an argument against modernizing assumptions that healing shrines are becoming any less important in contemporary India as spaces of mental health care. As Helene Basu (2014) challengingly asks, “from whose perspective is psychiatry, and from whose perspective is religious healing perceived as dominant?” (p. 166). As one of our key interlocutors in this article, a Muslim healer from east Delhi, popularly known as “Sufi-ji” (“ji” being a common suffix of respect in India),
6
put it to us one evening in the Sufi healing shrine of Badaun with a rhetorical flourish: Imagine if all the asylums and psychiatry wards in India were full at one time. How many patients do you think could be accommodated? 30,000 maybe, at most?
7
Badaun has more visitors than that on a single day. And then think of how many Dargahs there are all over India.
As such, one of our starting points is that the role of shrine-based healing is not necessarily waning in contemporary India, even as such spaces are increasingly policed and enfolded into secular regimes of power and knowledge (Basu, 2014; Sax, 2014, Sood, 2016). 8 Further, most of the current literature has turned away from varied forms of “marginalization theses” (Basu, 2014: 167) of such spaces as providing care solely for the poor who have no recourse to biomedical facilities or as enabling a “performance” of hysteria, often assumed to be a primarily feminine mode of suffering. Demographic analyses of treatment-seekers have found fairly even distributions of sex, caste, and class. 9
While religious healing is a canonical theme within anthropology, Indian psychiatrists too have not necessarily ignored or dismissed shrine-based healing as a form of superstition. The Indian Journal of Psychiatry, for instance, published since 1948, has had longstanding conversations on Indian concepts of mental illness, including a significant body of research on religious healing. Psychiatric investigations of healing shrines do not necessarily negate such spaces even within the terms of biomedicine. For instance, a landmark study conducted by the National Institute of Mental Health and Neurosciences (NIMHANS, Bengaluru), a leading center for mental health research in India, published in the British Medical Journal, followed a cohort of 31 mentally ill treatment-seekers at the Muthuswamy temple in Tamil Nadu over a three-month period, and showed that the mean brief psychiatric rating scale dropped significantly by the time of departure from the temple, with 22 subjects improving and three recovering fully (Raghuram et al., 2002, p. 39).
Even as quantitative accounts of improvements are illuminating, a more complex and unresolved question emerges: through what processes might such improvements be said to occur? Some authors have argued against an overemphasis on “efficacy” or “cure” (Ranganathan, 2015), arguing that the end result of treatment is not necessarily to be symptom-free, since shrines primarily work as a space of refuge and safe sociality during the phase when symptoms are, in psychiatric terms, florid. Others, building on Csordas and Kapferer's canonical arguments on the “rhetoric of transformation” (Csordas 1983) and the “negation and reconstruction of the self” (Kapferer, 1979), conceive of healing rituals as forms of “folk psychotherapy” (Csordas, 1983, p. 338), with spirits taken as metaphors “condensing fields of stressful experience” (1983, p. 359), a mode of analysis that has been applied to healing shrines in India as well (Pakaslahti, 1998, p. 164).
Our contribution departs from models of “folk” psychotherapy and catharsis to instead focus on two essential features of asrat; firstly, the sharing of the affliction, and second, the management of suspicions not through “counter-sorcery” (Nabokov, 2000) but rather through forms of inter-subjective attunement. Before we turn to specific instances, we outline our research design, as well as the ethnographic and clinical context, moving between the ecology/circuit of hospital, neighborhood/home, and shrine.
Research design and initial findings
The Sufi shrine of Badaun: Anthropological and clinical perspectives
Anthropological contexts: Ritual, circuits, and the ecology of the Badaun shrine
Spatial and temporal relatedness within Sufism is most often organized through saintly genealogies. As such, consider a Sufi map of India (Figure 2) within which Badaun is located. As most scholars and devotees would agree, the most prestigious Sufi shrine in India is that of the founding Pir (saint) Moinuddin Chisti in Ajmer (Rajasthan)

Sufi Ansar Ahmed (“Sufiji”) Healer, Trilokpuri, Delhi.

Leading Sufi Shrines of North India.
Alongside saintly genealogies, as treatment-seekers put it, shrines are often divided by their healing specialties, “like hospitals” as many jokingly add. What they are referring to is a key difference made by healers between shrines for saints who are jamali (associated with reham or compassion) and those for saints who are jalali (associated with heat and righteous anger). The most prestigious Sufi shrines in India—Ajmer, Mehrauli, and Nizamuddin—are jamali. Supplicants go to these shrines for a mannat (a request, for instance, for success in an exam or in business). For an asrat, the appropriate treatment route is to go to a saint who is jalali, associated with a different kind of court, described not as a darbar (royal court) like the compassionate courts of Ajmer or Mehrauli but rather as an adalat (the Persianate Hindu-Urdu term for secular legal courts).
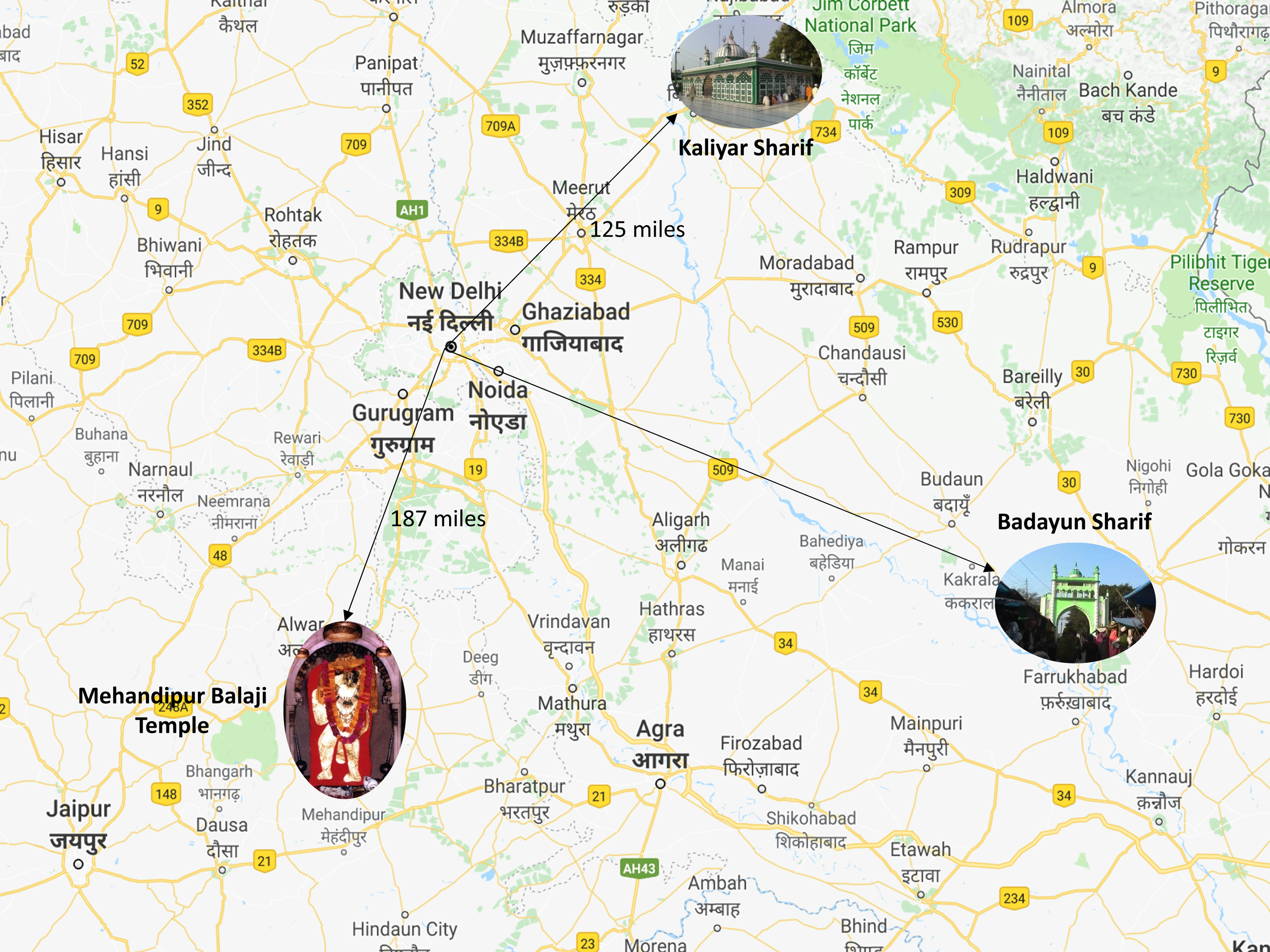
As most healers and treatment-seekers emphasize, for the treatment of asrat there are at least three major adalats in north India—the Sufi shrines of Badaun and Kaliyar Sharif, and the Hindu temple of Balaji in Mehendipur, Rajasthan (Figure 3). Interestingly, there is a specifiable reason why a Hindu temple such as Balaji is included in this geography of Sufi Muslim adalats. As many khadims (shrine caretakers), pirzadas (descendants of the saintly family), and healers at Badaun, including Sufiji, describe it, the Hindu temple of Balaji is a minor “branch” of Badaun, since the actual healing work there, they argue, is done by the Muslim Pir shrine of Divan Sarkar, present within the Balaji temple premises, who is a relative of the Badaun saints. Rather than syncretism, we might think of this as a creative extension of the Sufi logic of genealogy and network, as well as striking similarities in the legal terminology and circumambulatory form of the healing ritual (described below). With such forms of porosity and connection as a fact of South Asian religious life, in this article too we move analytically between Hindu and Muslim healing shrines.
Leading adalats (courts of healing) in north India.
Situated within this networked sacred geography, Badaun is 217 km away from Delhi, in the state of Uttar Pradesh. Singh made three visits to Badaun with Sufiji and his mareez (patients) over the course of 2015–2017, conducting repeat interviews and visiting 11 of them at home in Trilokpuri and adjacent neighborhoods, some months after their visit to Badaun. On one of these three visits, in May 2016, an eight-member team of Sharan (as team leader), three senior residents, and four AIIMS undergraduates accompanied Sufiji and Singh to Badaun. At Badaun, our team began by accompanying Sufiji and treatment-seekers to understand their daily routine, which consists of two (morning and evening) circumambulations across the 6-km radius visiting the mazhar (graves) of different buzurgs (elders), including the saintly brothers Chote and Bade Sarkar, as well as the grave-shrines of their sister Banno bua (aunt), their grandfather, Bankey mian, and three medical spirits—Doctor Pir, Hakim (herbal specialist) Pir, and the Compounder (pharmacist) Pir.
The space of the Badaun shrine (Figure 4) is conceived as an adalat headed by the Sarkar (ruler) brother-saints. Within this conception of deified/saintly sovereignty (Singh, 2012), the treatment regime over time is described through a further set of Hindi-Urdu legal terms, in ways that are strikingly similar to comparable shrines in other parts of India. 10 After arriving at Badaun, the first step for a treatment-seeking group is to present their arji (a petition outlining their problem) to the saints through a khadim in writing or verbally. They then begin a routine of haziri (attendance) through the twice-daily circumambulation. The ritually prescribed duration of stay at Badaun is 40 days, described by the Sufi term chilla (ascetic training), although people often stay for much longer. At some point during the daily rounds of haziri, a patient may begin to have a peshi (witnessing/possession) in which the afflicting spirit begins to speak and trance, which often becomes more intense during the qawwali (a Sufi musical form, now famous worldwide). If a peshi occurs and the afflicting spirit(s) begin to speak, “the case” is “open” (people use the English terms). The subordinate shrines begin to weaken the spirit(s) through kacchi phansi (preparatory hanging), by draining the spirit, as the supplicant's hand gets stuck to the shrine. A spirit may resist and restate its attachment to the body. The case is “closed” after the spirit(s) depart. This can occur voluntarily, signaled by a dream of a family member or by the spirit's testimony and promissory signature offered by placing a thumbprint at the base of the Chote Sarkar shrine. Alternatively, a defiantly settled spirit is subject to a symbolic ritualized phansi.

A rough sketch of the Badaun saintly shrine.
In consultation with Sufiji, our interview and survey design consisted of a form jointly designed by Singh and Sharan, which we call Asrat (Appendix 1). A crucial aim of this survey form was to consistently demonstrate that in an asrat it is not only a single person who is afflicted. Alongside a brief socio-demographic survey (including place of origin, religion, caste, number of household members at the shrine, duration of stay) and treatment pathways data (including hospital visits and attempts at biomedical treatment), our opening question was: “Who all in your family in your family has been affected by asrat?” Our team completed 39 asrat forms. Among these, the lowest number of family members affected was one and the highest was 11, with a mean of 2.69. Of our sample, 24 treatment-seeking groups were long stay (resident in the shrine for more than six months), 13 were short stay (less than six months), while one was seasonal. Alongside ethnographic modes of engagement with shrine administrators, healers, and patients, Sharan and his team also conducted clinical assessments within the shrine.
Clinical assessments at the Badaun shrine
Based on the family's account in our asrat form, an index patient was selected (specified by the family) and a psychiatric assessment was conducted with them. Twenty-nine such psychiatric assessments were conducted which, included 17 men and 12 women. Depending on the psychiatric assessment, Sharan or one of the senior residents administered the Brief Psychiatric Rating Scale (to 10 individuals with schizophrenia, unspecified psychosis, and bipolar disorder, of whom three demonstrated significant current pathology; average score 42.8 ± 12.7; range 17–58), 11 the Clinician Administered Dissociative States Scale (to six individuals with dissociative (conversion) disorder, of whom one demonstrated no pathology and others had low depersonalization, derealization, and amnesia sub-scores; average CADSS score 14.83 ± 9.6; range 0–29), 12 and the Patient Health Questionnaire (PRIME MD-PHQ; to 14 subjects, among whom five had no diagnosis, three had a somatoform disorder, seven had major depression, one had other depressive disorder, four had panic syndrome, and two had other anxiety disorder). 13 Among our asrat sample of 39, 11 patients had visited outpatient services, three had been in inpatient treatment, 10 had not visited a hospital, and biomedical treatment information could not be reliably ascertained for 15.
In psychiatric terms, in our small survey (N = 39), a wide range of ICD-10 categories—from severe mental disorders and common mental disorders, to dissociative/conversion disorder and personality disorder—were represented. Individuals were from lower to upper socioeconomic groups and different religious communities, and those who had engaged with diverse healing-medical traditions were also represented, suggesting that care in the shrine was not restricted to the poor who had no recourse to biomedical facilities.
For some, the shrine was a therapeutic ecology, as ritualized daily routines, conversations, and forms of assistance emerged between different groups of visitors. Compared to inpatient hospitalization, shrines may offer less restrictive options, particularly for treatment-seekers in partial remission, with community-based involvement, expressive cultural forms, possible gainful employment inside and outside the shrine, participation of family members, formation of social bonds, and the re-signification or containment of potential or actual violence, as with the two psychiatric vignettes below.
The re-signification of self-injury (Psychiatric Vignette 1)
Two subjects who appeared to have emotionally unstable personality disorder (impulsive type) prior to being at the shrine would commit forms of physical self-harm. Potentially violent behavior that had caused them infamy earlier was re-signified in the shrine in ritualized form, and the change seemed to provide them with prestige and solace.
Containment: Inner and outer (Psychiatric Vignette 2)
A 35-year-old engineer had been in and out of the shrine twice before: once when he had symptoms suggestive of mania and once for symptoms suggestive of depression. Biomedical treatment had apparently not worked, and his marriage had been in jeopardy in the manic episode. The family reported that, unlike at home, he did not become violent at the shrine.
Note: Two subjects with psychotic disorders also were reported to be much less violent in the shrine. Such subjects were occasionally chained by family members to trees, when the threat of violence seemed imminent or when the family members were exhausted after hours of following them as they moved around and threatened to leave the shrine complex.
Our next step in understanding the shrine as part of a wider circuit of care was to examine how a shrine like Badaun remains connected to particular neighborhoods in a metropolitan city like Delhi. Crucially, through our multi-sited research design, we could also investigate the ways in which healing work might be continued after leaving a shrine, with healers in urban neighborhoods and/or through biomedical forms of treatment-seeking or through repeat visits to the shrine (akin to “follow-up” OPD services, as shrine residents sometimes jokingly put it), in ways often necessitated by the relapsing-remitting tempos of mental illness.
The neighborhood and the healer
Since July 2015, Singh has been conducting ethnographic work in the urban poor neighborhood of Trilokpuri 14 in east Delhi, where the Department of Psychiatry of the All India Institute of Medical Sciences (AIIMS) runs a clinic oriented primarily toward Opioid Substitution Therapy. As part of a larger study on mental illness and opioid abuse among the urban poor (Singh 2021; Singh & Rao 2021), we carried out three phases of socio-demographic and psychiatric instrument-based surveys among men and women in 90 households in Trilokpuri across a period of six months (January–June 2016) to understand household economies, health-seeking behavior, and disease burdens, including but not limited to mental illness.
Within this neighborhood, Singh came to know a Muslim healer popularly known as Sufi-ji (“the venerable Sufi”) who gradually became one of his closest interlocutors in Trilokpuri. Sufiji's one-room dwelling in Block 27, a Muslim majority block in Trilokpuri, doubles as a healing space. 15 Between November 2015 and August 2016, Singh spent three nights a week staying with Sufiji, as part of a larger ethnographic project set in Trilokpuri. As a result, Singh came to know many of Sufiji's patients over time through meetings and interviews and the repeated observation of their interactions in Delhi and on trips to Badaun. Sufiji is one among a genre of healers found in several north Indian neighborhoods who work as local representatives of prestigious healing shrines like Badaun, although healers may also work independently of such affiliations.
Neighborhood representatives within Sufi networks, like Sufiji, do not necessarily have official designations from the shrine. Rather, their affiliations are most often sustained more informally through annual ritual periodicities as well as healing. Sufiji, for instance, is an important activating link between Delhi and Badaun, raising money for the annual Urs festival (the day of the saint's passing or “marriage with god”) in Badaun, ferrying treatment-seekers back and forth, running an officially registered NGO in East Delhi called the Chote Bade Sarkar Seva Samiti (the “service committee” of the Badaun saints), as well as a smartphone-based WhatsApp Group linked to this NGO, in which 200 or so members exchange texts, videos, news, and Muslim and Hindu religious images on a daily basis. Alongside the close observation of Sufiji's healing practice at home in East Delhi, a key aspect of this study, for us, was to be able to accompany Sufiji and his patients to Badaun, and then return home with them to Delhi, for repeat interviews and to observe healing processes over time, and to understand households and neighborhoods as ecologies of tension, suspicion, and rehabilitation, as described in the ethnographic instances below.
The psychiatric clinic
The third part of our study was carried out in the outpatient facility of the Psychiatry Department of the AIIMS (Delhi), one of the leading medical research and treatment facilities in India. The daily attendance at the AIIMS psychiatric outpatient services consists of about 300–400 patients, of whom 80 are first-contact cases while others are follow-up cases. Our interest in this segment of the study was to interview patients who reported failed visits to shrines, and were now in psychiatric care, at times concomitantly with continuing shrine-based forays. From March to June 2016, a senior resident in charge of reviewing and assigning patient appointments was asked to informally broach the question to first-contact and follow-up patients of whether or not they had sought alternative sources of care including shrines, vaids (practitioners of indigenous forms of medicine), and others, with the assurance that this would in no way impact their treatment at AIIMS. Those who assented met Singh or Ajmal Roshan, an AIIMS undergraduate research assistant, to fill out WHO encounter forms (used for treatment-seeking pathway studies across the world), to which we added a narrative supplement regarding the reasons for their dissatisfaction with shrine-based treatment. Thirty-five such forms were completed. Of this sample, Singh conducted open-ended, follow-up interviews ranging from 1 to 3 h with 12 of these patients/households, to further discuss their specific experiences of shrine-based healing and the reasons for their switch between different systems of care.
Inhabiting this three-point circuit, we offer three ethnographic instances that for us capture what we see as two essential elements of shrine-based healing: firstly, the sharing of the affliction between family members, and secondly, forms of doubt or suspicion within the kinship group or proximate neighborhood regarding an injury that is managed in the healing process by strengthening an intra-familial dynamic, which we describe as a form of attunement. Each of the three instances below describes specific modes in which an asrat affliction comes to be shared.
Ethnographic Instance 1: Seema and Savitri at Badaun
Mode of sharing an asrat: Movement of symptoms across bodies and the distribution of care
Here is an excerpt from Singh's field notes from June 2016: For the last two days we have been circling the Badaun shrine complex following the therapeutic process of a pair of Sufiji's patients, a mother, Savitri (aged 36), and her daughter, Seema (aged 15)16, Hindu high-caste Rajputs, from Aligarh in Uttar Pradesh. Our AIIMS team assessed Seema yesterday and found her to have a Clinician Administered Dissociative States Scale score of 31, the highest among the group of six to whom this particular clinical assessment was administered. Seema moves from one part of the shrine to another, laughing, and sometimes screaming the words of stubborn spirits: “Sultan Arifeen, do what you want, I won't leave.” During a period of lucidity Seema described to me how her mother was kamzor [weak] and so she had to take on her mother's illness. The consensus among Seema, Savitri, and Sufiji seems to be that the affliction stems from Savitri, the mother, who looks well and is smiling and talkative. She offers her account of the movement of the illness: “I had a baby and had to breastfeed him. So Seema took on the asrat” [apne upar le liya]. The baby boy, now two years old, is with them as they perform their daily haziri. Today in our seemingly routine haziri a significant transfer is occurring, enabled by Sufiji's presence, Savitri (the mother) separates herself from us and goes down on her haunches next to Seema and bellows, like an animal. As I look quizzical, Sufiji clarifies the process in a judicial idiom: “Last night I told the mother that case katne ke liye [to “end the case”] you will have to take it back on yourself. So yahaan par iska transfer ho raha hai [the case is being transferred]. For two years it has been on the daughter alone.” Seema and Savitri had been staying at the shrine for the past six months.
In a comparable study in the Mahanubhav shrine in Maharashtra, Vieda Skultans studied 40 cases of such movements of affliction over a six-month period. The most common mode of sharing according to Skultans (1987) is a movement of the afflicting spirit during trance, from husbands/sons to their wives/mothers (p. 670). Skultans (1987) calls this a form of “self-sacrifice” (p. 676). As the principal caregivers on whom the burden of care falls most significantly, Skultans (1987) argues, women take on the “redistribution of illness within families” (p. 670). While Skultans’ argument is compelling, we find the gender distribution of affliction to be more varied rather than a unidirectional movement from masculine to feminine bodies. A key insight of Skultans’ (1987) that we accept is that in relation to shrine-based healing, “mental health may be considered as a property of households and kinship groups, rather than individuals” (p. 662).
Conceptually though, we contend that this question of porosity or contagion is not explained by invocations of a “non-western” collectivist psyche secured by kinship.
17
Such a conclusion would ignore a central feature of asrat and practices of shrine-based healing, namely, the conception of threat to which the healing process most often responds. Consider an ethnographic detail that Skultans notices but leaves untheorized. As Skultans asserts, afflictions are most often understood to begin with a dispute with an intimate other. “One can plead with God, but not with an angry relative,” as one of Skultans’ (1987) interlocutors’ asserts (p. 670). To pursue this thought further, we cite an excerpt from an interview that Singh conducted with Savitri (Sa) and her daughter, Seema (Se): Singh: How did your asrat begin?
Sa: It began because of my jethani [elder sister-in-law] and saas [mother-in-law]
Singh: What problem did they have with you?
Sa: My jethani's children would die. Mine died too, because of her.
Se [daughter] adds: he [referring to her father] has gone over to their side!
Sa [in tears]: I was the ladli [darling] of my parent's house. My father is very rich. So my jethani got jealous of our property. She did something to me. She did it through a maulvi [a Muslim spiritual adept], who gave her a pot of blood, and then she had a son. Then my son was born. For two months he kept crying and then he died. Maulvis did it, so only the sarkars [the Badaun saints] will be able to cut it. They confirmed that it was my saas and jethani who did it. And Sufiji also said this was the case.
An asrat, we find, often begins with a threat to existence arising from a disorder of intimate otherness, which may initially appear as a doubt, a shaq (suspicion), which a healer like Sufiji may diffuse, as a vehem (a misplaced feeling), or treat it as real, as an issue to be lived with, that emerges in a weave of relations, particularly with neighbors and kin. In secular terms, how might we understand mental illness in relation to forms of suspicion? In their recent book Suspicious Minds: How Culture Shapes Madness, Joel and Ian Gold (2014) argue that a central component of the “social” brain is what they call a Suspicion System, “a form of cognition, directed at potentially dangerous others” (p. 163). Gold and Gold (2014) differentiate between what they call a healthy Suspicion System, that enables us to pick up evidence of “social threats” (p. 165), and a damaged Suspicion System that moves from “justified” suspicions to paranoia and other forms of delusion (p. 195). The fine line between genuine and delusional threat perception, Gold and Gold (2014) further argue, is kept in place by a parallel cognitive process, which they call the Reflective System (p. 200).
Rather than claiming a neuroscientific basis for our argument, we emphasize a different aspect of Gold and Gold's (2014) thesis, namely that “the social world affects the brain no less than a stroke or a tumor would” (p. 140). Accepting this formulation, instead of an abstractly widened conception of the social, we situate the suspicion system in relation to oikos (household/dwelling space). A household and a neighborhood, one's most proximate ecologies, may have far-reaching effects in the experience and prognosis of mental illness. A crucial step in understanding asrat as a concept and a set of practices are the ways in which mental illness is etiologically reinterpreted in relation to an oikos as a site of suspicion. These suspicions are then managed not by a Reflective system but by practices that seek to curtail the spiraling intensity of suspicions and negativity, most often by making them livable, by bolstering alternative circuits of intimacy within the oikos, such as a mother and a daughter in the instance of Seema and Savitri.
Consider a psychiatric reading of this mother–daughter dyad. In psychiatric terms, the occurrence of similar disorders in two or more family members is conceptually closest to epidemic hysteria. Epidemic hysteria has been defined as a constellation of symptoms suggestive of organic illness, but without an identifiable cause, that occurs between two or more people who share beliefs (e.g., asrat) related to those symptoms (Philen et al., 1989). Episodes may recur and can last for several years such as in demonopathy in Christian convents (Madden, 1857). Theories of epidemic hysteria include those that suggest that symptoms are produced for various (conscious as well as unconscious) reasons or due to stress and personal vulnerability.
However, the case of Seema and Savitri does not seem to be epidemic hysteria, in the sense that the affliction moves from Savitri to Seema to enable the former to breastfeed and care for the baby and then from Seema to Savitri to enable the closing of the case. The to and fro movement of the affliction is purposive in its directionality. This purposiveness is not witnessed in epidemic hysteria. In Munchhausen by proxy, symptoms are produced in the other (without the other's willing participation), but they are not shared by the one who produces the symptoms.
From a psychological perspective, the intra-psychic and the inter-personal are fundamentally entangled (Benjamin, 1998; Ettinger, 2006; Roseneil and Ketokivi, 2016). Minuchin’s (1974) Family Stress Model which is based on a systems approach to family therapy suggests that family stress depends on the way a family adapts, interacts, and transacts with a stressful event. Minuchin sees stress as a phenomenon flowing from four major sources that could be inside or outside the family system: extra-familial forces on one family member (work stress), extra-familial forces on the entire family (unemployment of the breadwinner), transitional points in the family (e.g., birth of a child), or idiosyncratic problems (e.g., family with a longstanding serious illness in a member). The family's ability to adapt will greatly determine how stress is managed by the family system. Minuchin argues that family systems that respond to this pressure by increasing the rigidity of their transactional patterns and boundaries and avoiding alternatives for solving problems are systems in need of treatment.
In the instance above, taken as an individual Seema would be diagnosed with “hysteria” or dissociative disorder. In contrast, the sharing of afflictions and the dyadic relationship seem to be approaching “family responsibilities” through open-ended processes involving explicit and implicit negotiation and conflicts within a familial context. Savitri's asrat developed in response to stress due to forces in the extended family, while the transfer of illness to Seema provided an alternative form of support at a transitional point in the family with the addition of a child, and separation from the father/husband.
Ethnographic Instance 2: Madhavi and Raj at Badaun and at home in Delhi
Mode of sharing an asrat: Joint misfortunes, intimate suspicions, and the restoration of everyday life
Three months after the conversation in Badaun with the Hindu couple Madhavi and Raj, with which we began this article, Singh went to conduct a follow-up interview with them at their home in a resettlement colony in Delhi. As we discussed the nature of the asrat in greater detail, the couple explained that in their view it began as a result of hostilities with Raj's brother, which resulted in severe financial losses and the loss of Raj's job, after which the asrat transferred to Madhavi, expressed through her symptoms. Of all the treatment-seekers we met, this couple seemed the most certain that their visits to Badaun had helped. What was the nature of the assistance? Rather than a miracle cure or a cathartic expulsion of negativity, their emphasis in describing the process of healing was on the gradual reconstitution of household routines, as Madhavi's symptoms became more manageable after the visits to Badaun. “For months I could not even cook food for my son,” Madhavi added, “he [referring to Raj] would do everything. But now it is much better. Whenever I feel an attack coming on I have the babhoot [a Hindu word for “sacred ash” ] and the pani [consecrated water] from Badaun, and I feel better.” Raj added: “Whenever we are running out, we go back to Badaun to renew our supply from the khadims. That's what we had come to do when you met us there.”
We suggest that what we have here is a twofold mechanism: the re-channeling of affect through the ingestion of substances (with the sacred ash and water working as a mood-altering substance) and a form of inter-subjective strengthening between the husband and wife, in ways that are harder to capture. Qualitatively, it felt like the couple completed each other's sentences, energies, and labors. How might we characterize this mode of strengthening if not through seemingly commonsensical but conceptually ineffable terms like love or kinship, which as we see, can also be fragile be fragile, dynamic, and even potentially toxic? What might be a beneficial response to a potentially life-negating intimate injury or suspicion?
While Sufism and South Asian popular culture more broadly has a highly developed vocabulary of love (through cognate Hindi-Urdu terms such as ishq, mohabbat, sneh, and pyar), ethnographically we did not find healers like Sufiji or khadims, or treatment-seekers at Badaun invoking a language of love as the countervailing force to asrat-related injuries. Rather than moving from doubt and suspicion to the certainty of faith or love as a fixed and predictable form, we sought a term that felt closer to the more implicit inter-subjective processes at stake, that could also be disrupted by the unpredictably relapsing remitting tempos of mental illness and healing. The conceptual term we have found most helpful is Stanley Cavell's 18 suggestion that a response to life-negating doubt or injury might not be certainty, but rather attunement, 19 a mode of relatedness to oneself and to others. Uncertain as that sounds, scientific definitions of cure may be just as a fragile. For instance, from a psychiatric perspective, as an antidote to “suspicious minds,” Gold and Gold (2014) assert, “The conclusion seems undeniable: if other people can damage your brain, they can also minister to it” (p. 225). Citing studies of supportive psychotherapy and Cognitive Behavior Therapy, Gold and Gold (2014) argue that enhancing “patients’ capacity to maintain authentic and healthy relationships” significantly impacts prognosis (p. 224). “Good relationships, it seems, are a universal therapeutic good, and may yet turn out to be the single most important ingredient of effective psychiatric care” (Bentall, cited in Gold & Gold, 2014: 225). Instead of Gold and Gold's somewhat one-dimensional categories of relatedness such as “good,” “healthy,” and “authentic,” we turn to Cavell's term attunement for two reasons.
Firstly, because the musical resonance of the term “attunement” offers a more modest expectation of relatedness, often visible or audible in clinical and ethnographic interactions, in how members of a household interact and express what Cavell (1979) calls a “mutual voicing” (p. 32), or disharmony and the “negation of voice” (1996: 47), in ways distinct from terms such as authenticity or goodness. Secondly, in relation to the study of mental illness, attunement stands alongside a set of companion concepts, as outlined by Cavell (1987) in related work, to do with degrees of intensity such as pitch, tone, and tempo (p. 98; 1994: 130), which may be useful in engaging with healing practices. For instance, a healing practice in shrines or with a healer like Sufiji, even in seemingly commonplace ritual acts like the provision of amulets or calming ritual substances, may be aiming for ends akin to a psychiatrist, such as containing the tempo of a suspicion or a rumination, to prevent it from spiraling into a more life-negating form, either by enhancing subjective fortitude through embodied mood or thought-shifting techniques, or by re-combining circuits within a kinship network and bolstering inter-subjective attunement.
From a psychological perspective, in Ethnographic Instance 2, Raj's affliction (severe financial losses and loss of his job, seemingly the effect of the conflict with his brother) is a family stressor rather than an illness. Madhavi takes the impact of the asrat on herself by developing dissociative (conversion) symptoms. As with Seema and Savitri above, “family responsibilities” such as the division of care and labor are approached through open-ended processes involving explicit and implicit negotiation.
The role of empathic attunement has been emphasized in therapeutic encounters. Barrett-Lennard (1998) argues that a more “synchronous engagement” between client and therapist involves becoming more “in tune” with each other. There is considerable evidence in support of the role of empathic attunement in promoting positive outcomes in all forms of psychotherapy (Angus et al., 2015). Ethnographic Instances 1 and 2 suggest that empathic attunement is not exclusive to formal therapeutic relationships.
Our conceptual argument may be clarified further by a negative instance, expressing the contrary of attunement, and the ways in which discordance and violence within a household might also be significant for understanding the experience of mental illness. We offer a final ethnographic example, of an asrat that failed to be treated in Badaun. This instance is drawn from the third strand of our study conducted in the AIIMS psychiatric outpatient service.
Ethnographic Instance 3: Aamir, Taha, Tamir, and their mother at the clinic
Mode of sharing an asrat: Parallel illness trajectories, shared and contested suspicions, intensifying discordance, and the lack of attunement
We initially encountered the Khan family in May 2016 in the course of our Pathways study in the AIIMS OPD. They were one of two households that reported a failed visit to Badaun. Other households within our pathways sample had either been to Balaji or had limited their treatment-seeking forays to neighborhood healers. 20 Singh subsequently conducted an open-ended interview with the Khan family, which lasted 2 h. Three members of the family— the mother and two of her sons—had reported psychopathology at different points of time in the last 15 years. There was agreement within the household as regards the starting point for their troubles, including the trajectories of mental illness. These were said to have begun after their father's death, as he was trying to re-occupy their property in Farroukhabad (in Uttar Pradesh, 3 h from Delhi) by displacing renters, including extended kin. Any next narrative step, even whether what happened subsequently could be called an asrat, broke into variably discordant disagreement.
The structuring voice in our interviews in the AIIMS OPD was the eldest brother, Aamir, although he was not a dominant voice, but rather was repeatedly interrupted by the younger brother Taha (in treatment for Bipolar Affective Disorder), who claimed that Aamir had been professionally harmed by the asrat, as badly as any of the patients in their household. We began by discussing the mother's trajectory. The father died in 2006. Some months later, the mother started talking to the walls and heard Allah reply. Taha adds: She wasn't imagining it. She actually spoke to Allah! I have now taken on her asrat.
Mother disagrees: Taha's problems are because of his unemployment.
Aamir interrupts: At home these two become a team, like Maryam and Isa [Mother Mary and Christ]. Our house has become a nark [hell].
The mother had been in treatment at IHBAS for paranoid schizophrenia. Aamir described the difficulties her condition creates for everyday life in their joint family household, including for his marriage. Aamir: She [the mother] abuses her own brother, her daughter. She doesn't like keeping rishtedaari [the obligations of extended relations] with anyone. If someone comes from my in-laws’ place, she won't host them and will suspect them of stealing or breaking things in our house.
Mother: Whatever little we have, they’ll destroy even that.
Aamir: See, this is how it is! If anything is broken in the household, she’ll say a relative broke it. Ours used to be one of the leading families of Farroukhabad.
I turned to Aamir's younger brother Taha. After years of unemployment and a particularly painful disappointment in love with a girl in their neighborhood, Taha began to talk “fast” (tez baatein karne laga, the most common way in which delusions of grandeur and symptoms of Bipolar Affective Disorder are described in north India). Aamir clarified: Taha would say “mei collector banunga [I’m going to be a high-ranking government officer]. I belong to high society. All of you are beneath me.” He would pace until past midnight on the terrace without sleeping. I would tell him to sleep. This continued for five or six years, after which I took him for treatment to IHBAS.
Taha added: “I didn't like the mahaul [atmosphere] of IHBAS.” The youngest brother, Tamir, was the quietest. Others in the household described him as having a mota dimaag (a “slow”/“fat” brain, an Indian colloquialism for mental retardation). In contrast to the “faster” Taha, the “slower” Tamir had been employed until two years ago in an electrician's shop. Aamir clarified: “he had a salary of Rs. 4,000 per month. He was hardworking. He would leave in the morning and come back at 6 pm.” The family had begun conversations about Tamir's marriage with an older cousin in Farroukhabad (cross-cousin marriage being common among many Hindu and Muslim social groups in India). Aamir added: “One day we heard that she got married elsewhere. After that, Tamir started remaining very quiet. He stopped going to work. Now he doesn't even want to change his clothes.” Singh turned to Tamir: Singh: Everyone has spoken except you. You tell us, do you have any problem?
Tamir: I have no problem.
Singh: None?
Tamir: Headache. Pareshani [worry]. I take medicines and get okay for a while.
B: Why did you leave work?
Tamir: Dimag par bahut asar pad gaya [my brain got badly affected]. Dil kar raha tha ki aaram karein bas, aaram hi aaram [My heart felt like resting, and doing nothing else, getting lots of rest].
Conceptually these illness trajectories were not always framed as an asrat. That said, there was a basic agreement within the household that the starting point, namely, the antagonism in Farroukhabad followed by their father's death, was an asrat. Why then did Badaun “fail” this household? Our initial anthropological conjecture was that there might be a theological reason for the family's aversion to Badaun. However, in conversation it turned out that the family is Barelvi, the sect of Sunni Islam, which would not consider healing as shirk (idolatory), a derogatory term for Sufi shrine-related practices used by “reformist” and puritanical sects of Islam.
21
Rather than theology, the family's aversion to Badaun arose out of more ordinary circumstances. Here is an excerpt from our conversation about Badaun: Aamir: Three years ago, we went to Badaun Sharif. The other families explained to us. It could take 15 days. It could take two months. You’ll have to stay here.
So I said, who will stay with them? There are three people affected like this in our house. And we don't earn that much. So I had to go back to work.
Mother: Also, we were beginning to feel worse there!
Taha: I said “Allah save me! I don't want to be left here in this madhouse!” Among Dargahs I like Nizamuddin. And Haji Ali in Mumbai. And Ajmer Sharif. But not Badaun. I didn't like the mahaul [atmosphere] there. It is worse than IHBAS.
Aamir: I took them there saying that we’ll stay for three or four days. But we came back in two days.
Mother: Why should we care about such places? The children should get employed, married, end of story.
While not fixing a straightforward definition of “success” or “failure” in treatment, we might still ask what a space like Badaun could offer such a family, were the treatment to have been efficacious. We might sense a discordant, potentially detrimental family dynamic, in combination with what we could call a sense of excessive suspicion within the household. This dysfunction is expressed at times as symptoms within individual illness trajectories, for instance by the mother and by Taha. As Taha emphatically asserted to Singh: “We have received dhoka [betrayal] from every side. And found that anyone can be an enemy.” In the absence of a countervailing dynamic of attunement and re-combination within the household, an unchecked social suspicion system is expressed, not so much in a lack of “consensus” (since healthy and unhealthy disagreements are perhaps a hallmark of kinship), but in varying tempos of discordance through which tensions may escalate in pitch and tone, sometimes breaking into violence. Here is a concluding instance of escalating discordance from our conversation with the Khan family: Aamir: At times in our galli [“by-lane,” a marker of belonging within a neighborhood] they create a situation where neighbors have to dial 100 [call in the police]. He [Taha] will pick up a stone to kill our youngest brother. He has himself gotten badly hurt many times.
[…]
Mother: Taha has been beaten up so badly that his hands and feet have stopped working.
Aamir: It makes no difference!
Mother: Dimaag phat gaya tha [“His brain had burst”]
Singh (S): Who beats him up?
Mother: They [pointing to Aamir], his brothers.
Taha: I don't even want to know on whose instructions they are beating me.
Mother: I had a dream that Taha's brain is lying on the street and an elephant is picking it up with his trunk. And Taha is jumping.
Singh: In the dream?
Mother + Aamir: No, in reality!
Mother: In reality, his condition was very bad. He was jumping around everywhere.
Aamir [re-narrates mother's dream]: His brain is lying and an elephant's trunk … what was it?
Mother: An elephant is picking up Taha's brain with his trunk and putting it into a sack. At that time he was in bad shape, when I had that dream. All three brothers were beating him up.
Taha: In retaliation I read a kalma: La ilaha … and all my brothers fell down [chit ho gaye].
Aamir: He hit Ammi [our mother] on the road. He was pulling her from her hair on the road. Could we let him be? We had to hit him.
Taha: I hit Ammi for a good reason.
Aamir: Who are you to hit her? Tu baap hai [Are you the father]?
Taha: No.
Aamir: So then be quiet!
Taha: [laughs]
In this excerpt we see the lines between the normal and the pathological, the ordinary and the violent, dream and reality begin to blur. How might such a household be rejoined? From the perspective of Badaun, we are offering a set of terms for some of the modes of rejoining that such a space offers: attunement, re-combination through the bolstering of a vulnerable segment within a kin group, and ways of managing a social suspicion system. The opposite of joining or attunement would be separation, which was also an option that Aamir was suggesting: Aamir: I feel the only solution is that they [Taha and the mother] don't meet each other for one or two years. So he gets a different mahaul [atmosphere/milieu]. The three of them shouldn't be together. They need to be separated. Only then will they get better.
In Ethnographic Instance 3, the mother has been diagnosed with paranoid schizophrenia, Taha with bipolar affective disorder, and Tamir may have mild mental retardation or borderline intelligence (he has not been evaluated by a mental health professional). What is shared in this case is considerable family dysfunction caused in part by the presence of multiple mental conditions.
In psychological terms, relational disorders are defined as persistent and painful patterns of feelings, behavior, and perceptions involving two or more partners in an important personal relationship, marked by distinctive, maladaptive patterns that show little change despite a great variety of challenges and circumstances. Relational disorders have been described to occur within one generation (e.g., conflictual disorder, sexual/physical abuse, shared/induced psychotic disorder) and between generations (e.g., physical abuse or neglect, reactive attachment disorder) (Committee on the Family, Group for the Advancement of Psychiatry, 1995). In Ethnographic Instance 3, there is evidence of both intra-generational (conflict and physical abuse) and inter-generational relational dysfunction. Relational disorders have not been included in current psychiatric classificatory systems, which pertain to disorders of individuals.
Conclusion: Anthropology and psychiatry, in a joined and separate key
As Gold and Gold (2014) assert: “the social world affects the brain no less than a stroke or a tumor would” (p. 140). The household, we might say, is perhaps the single most critical component in the daily habitation of the social world. And further, it is the theater in which the pressures of mental illness are often most starkly expressed, for patients, caregivers, and family members. It is this pressure point that spaces like Badaun attempt to address. As such, what would need to be studied in such spaces are both the individual trajectories of improvement, as with the NIMHANS study above, but also the concrete relations and forms and failures of joining and re-joining, as we have tried to suggest in our study of asrat. We have argued that the idea of asrat is worth considering, not only as a culturally “bound” syndrome or as a folk variant of psychotherapy, but for its religious and secular implications as regards questions of relatedness and what it means to share an illness. This question of shared burdens, suspicions, and forms of attunement might also arise and be managed or mismanaged in secular contexts, in ways that can influence prognosis and the experience of illness. We also hope that our emphasis on attunement and the “discordant” rather than the “dysfunctional” might open up considerations of how the line between the normal and the pathological might be a difference not of kind (functional vs. dysfunctional) but of degree (of pitch, intensity, tempo) within household and family dynamics.
In terms of further implications, in a recent article in the British Journal of Psychiatry, Luhrmann et al. (2015) suggest a possible answer to the famously debated “better-prognosis hypothesis,” 22 namely that in spirit-infused cultures, hearing voices and a range of other symptoms are more common and thereby perceived as less threatening, and not necessarily as signs of a violated mind. Contra Luhrmann et al., we suggest that voices in the so-called “non-West,” for almost any of the patients we interviewed, are not necessarily less of a source of terror. Rather than a “violated mind” (Luhrmann et al., 2015), perhaps what are more difficult to live with are perceived psychic injuries from relative intimates. As important perhaps as Luhrmann et al.'s notion of relationships with voices, we suggest, is the continuing and numerically significant treatment networks such as those enabled by Sufi shrines.
In investigating these networks, we do not see the biomedical and spiritual treatment systems necessarily as contraries. As we suggest, at times a healing practice and a psychotropic medication might be trying to pursue similar ends: altering a mood, allaying an anxiety, learning to live together with distress and with the kinds of shared pressures that mental illness places not only on an individual but on a household. That said, we do not claim or call for a joining of ontologies or treatment techniques. Rather, through our surveys, clinical assessments, and multi-sited ethnography, we have tried to remain true to the variability, struggles, and the uncertain movements of treatment-seekers across spaces and ontologies, in which at times the ontological, legal, and spatial distance between these nodes (Sax, 2014) might be as significant as any overlap or proximity.
The movement in a space like Badaun is not from doubt and injury to a restoration of “family” or “faith,” since symptoms may recur or a healer, shrine, or family member may remain a source of doubt. Within Trilokpuri, it was not uncommon to hear neighbors at times criticizing Sufiji: “unke haath mei shafa nahi hai” (“his cures lack certainty”). Rather than the stable elimination of doubt and injury, this form of healing, when it works, is directed toward making a negation more livable through a stitch, a rejoining, to be recombined differently, say, with one's own experiences (Psychiatric Vignettes 1 and 2), or relationally by intensifying forms of attunement within a household or kin group.
From a psychiatric perspective, the existence of a collective consciousness or mental state over and above individual consciousness is contentious (Bostock & Bostock, 2017). In psychiatric literature, this doubt is evidenced by the removal of shared delusional disorder (folie à deux) from the 5th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) and International Classification of Diseases (ICD-11), even as more complex ideas of relational selves do persist in the theoretical literature. For instance, Sedikides et al. (2011) endorse the notion that the self-concept consists of three fundamental representations: the individual self, the relational self, and the collective self. The notions of inter-subjectivity and trans-subjectivity emphasize the permeability of the boundaries of the self, and the ways in which subjects in intimate relationships assimilate (Benjamin, 1998; Ettinger, 2006; Roseneil & Ketokivi, 2016).
Current classificatory systems and the field of psychiatry in general seem to be moving toward a view that relational disorders cannot exist, on the basis that psychiatric disorders require the existence of a dysfunction within the individual. The sharing of afflictions across kinship as described in the instances above should serve as a rejoinder against the hegemonic individualist narrative, without necessarily implying a stable idea of culturally bound norms for “collective” selves, since as we have shown, kinship and intimacy can also be realms of doubt, instability, and suspicion.
Each of our ethnographic examples above aims to show how an asrat might be “resolved” or not through forms of attunement. In example 1, we witness a process that enables the dynamic redistribution of the labor of care between a mother, a daughter, and a newborn. In example 2, the husband and wife consider their case to be “resolved,” or at least managed, as functionality and daily household routines are restored. In example 3, we suggest what a counter-concept of attunement might look like, namely, discordance, and how this is expressed in the clinic (through the argumentative excerpts between the brothers and their mother) and the intensified form this lack of attunement takes within the home and the neighborhood with outbreaks of domestic violence.
As we have also indicated through the secondary literature beyond Badaun, the systems, techniques, and terminology of healing are replicated in shrines across enormous distances, in ways that remain a mystery. The mystery may not be solved by finding an original center, author, or textual code from which the system is diffused, since no such code may exist, at least as far as we have been able to track. And yet, as with many mysteries, the phenomenon offers a gripping set of questions, of how injuries traverse related bodies, in religious and secular terms, and some potential answers organized around the concept of asrat, as we have tried to indicate.
Supplemental Material
sj-pptx-1-tps-10.1177_13634615221078131 - Supplemental material for The contagion of mental illness: Insights from a Sufi shrine
Supplemental material, sj-pptx-1-tps-10.1177_13634615221078131 for The contagion of mental illness: Insights from a Sufi shrine by Bhrigupati Singh and Pratap Sharan in Transcultural Psychiatry
Supplemental Material
sj-pdf-2-tps-10.1177_13634615221078131 - Supplemental material for The contagion of mental illness: Insights from a Sufi shrine
Supplemental material, sj-pdf-2-tps-10.1177_13634615221078131 for The contagion of mental illness: Insights from a Sufi shrine by Bhrigupati Singh and Pratap Sharan in Transcultural Psychiatry
Footnotes
Acknowledgments
Drafts of this argument were presented and received the thoughtful input of colleagues at Johns Hopkins University, Princeton University, Shiv Nadar University, LMU-Munich, and Wissenschaftskolleg zu Berlin. This article would not have been possible without the sustained efforts of Ms. Anita Chopra in helping to build and analyze our project data. The authors also wish to thank Dr. Ajmal Roshan, Dr. Igam Bagra, and Dr. Ankit Gupta at AIIMS for their invaluable assistance with surveys and clinical assessments for this article, and to Sufiji for gently guiding us through the intricacies of Badaun and for introducing us to the conceptual and psychic world of shrine-based healing. The authors also wish to thank the anonymous reviewers and editors of Transcultural Psychiatry for their exacting and rigorous review process which helped to improve the article, even as its limitations remain our own.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Singh thanks the Wenner-Gren Foundation for Anthropological Research (Post PhD Research Grant), the American Institute for Indian Studies (Senior Research Fellowship), and Brown University's Center for Contemporary South Asia for research grants that enabled this phase of work at AIIMS, Badaun, and Trilokpuri; and the Wissenschaftskolleg zu Berlin (WIKO / Institute for Advanced Study, Berlin) for a writing fellowship that allowed the thoughts presented here to develop, with deeply engaged feedback and suggestions from the intellectual community at WIKO.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.