
Abstract
Previous research has demonstrated that without the use of professional interpreters, language barriers interfere with patient care. The literature recommends documenting the presence of language barriers in medical charts. To our knowledge, this mixed methods study is the first to examine language documentation practices in a Canadian inpatient psychiatry setting. The research team interviewed 122 patients admitted to a tertiary care psychiatry ward in Montreal, Canada between 2016−2017 to assess their ability to communicate in the healthcare establishment's languages (English/French). Nineteen participants identified as having a language barrier were selected for a qualitative analysis of the retrospective audit of their medical charts. The presence of a language barrier was reflected in 68% of these charts. When a language barrier was documented, professional interpreters were never used. Our qualitative analysis, informed by literature on medical discourse, aimed to provide clinical, administrative, and organizational recommendations to optimize the utilization of interpreting services in psychiatric wards. Documentation of language data was inconsistently collected, often vague, and shed light on the clinical challenges involved in differentiating language barriers from psychopathology. Normalization of limited care for language diverse patients was reflected in the clinical notes. Findings show that a change of organizational culture is imperative to provide optimal care to language diverse patients. We recommend clinician education and standardization of documentation practices, along with institutional policies supporting the systematic use of professional interpreters in mental healthcare settings, to maximize human rights and patient safety, and to bring medical practices to an acceptable standard of care.
Introduction
In the context of globalization and increasing immigrant diversity, the Canadian population has come to speak more languages in recent decades (Statistics Canada, 2017), which has made healthcare more complex. A substantial body of literature has established that language barriers between clinicians and patients increase the risk of misdiagnoses and medication errors, and negatively impact healthcare access, adherence to treatment, and patient satisfaction (Bowen, 2015).
A “language barrier” has been defined in several ways, including: language discordance between patient and clinician (Okrainec et al., 2014); self-reported language proficiency in the mainstream language rated as less than “very well” (Dorsey et al., 2014); limited self-reported ability to communicate with caregivers (Karliner et al., 2008); and a language preference in which to receive health services that differs from the establishment's main language (Gee et al., 2010). Okrainec et al. (2014) suggest that these definitions of the term “language barrier” cannot be used interchangeably and should all be measured in clinical practice. For the purposes of this study, language barrier refers to patients with limited proficiency in French and English, the two common languages of the hospital from which the study participants were recruited.
In mental health, effective communication is essential given that language serves as the principal diagnostic tool to assess thought content, cognition, complex emotions, and thought disorder. When patients express themselves in their own language, they articulate their experiences in a more nuanced manner, which ultimately improves the accuracy of their psychiatric assessment and diagnosis (Kirmayer et al., 2008). The literature recommends systematically working with qualified interpreters during psychiatric assessments of individuals with limited mainstream language proficiency (Skammeritz et al., 2019) and discourages the use of ad hoc interpreters who may fail to recognize nuanced patterns of speech with clinical relevance, such as disordered thought processes (Elkington & Talbot, 2016). Indeed, informal interpreters are at higher risk of committing translation mistakes with clinical consequences (Flores et al., 2003). Furthermore, the use of family members as interpreters may limit the patient's disclosure as it compromises confidentiality, and vulnerable individuals, such as victims of domestic violence, may be put in danger when family members interpret for them (Ho, 2008). Despite the fact that substantial evidence has demonstrated the effectiveness of professional interpreters, they remain underutilized in most clinical settings (Bauer & Alegría, 2010).
Addressing language barriers on a clinical and organizational level involves multidimensional strategies. The literature recommends collecting and documenting patients’ preferred spoken language and their proficiency level in the language used by the healthcare establishment (Chong et al., 2019; Nerenz et al., 2009). Collection of these data can identify disparities that lead to targeted interventions (Hasnain-Wynia et al., 2006). In the last two decades, a sizable body of research, mostly in the U.S., has examined the documentation practices of language barriers in medical charts. Most of these studies have been performed in medical settings, such as the emergency room (Taira & Orue, 2019). Research suggests that language data recorded in medical charts are often lacking or inaccurate, and collected in an inconsistent way (Bowen, 2015). To our knowledge, no studies have explored documentation strategies of mainstream language proficiency in Canadian psychiatric settings.
The aim of this exploratory study is to describe how language barriers are documented in clinical records of patients admitted to the inpatient psychiatry ward of a tertiary care hospital in Montreal, Canada. Our analysis will focus on providing clinical, administrative, and organizational recommendations to optimize the utilization of interpreter services on psychiatry wards and, ultimately, to improve the quality of care for language diverse patients. In the context of this study, “language diverse” patients are defined as patients with limited proficiency in either French or English, which are the main languages of communication within the institution.
The medical notes contain observations, evaluations, and clinical information written by various practitioners. This information tracks ongoing care by the clinical team and plays a role in treatment planning and accountability. Many progress notes are filled out by nurses who report daily functioning and behavior, or are written by medical students as part of their training and professional socialization (Hobbs, 2004).
The content of medical records informs and shapes clinical decisions. Determining which information is worthy of being recorded is at the core of clinical practice (Atkinson, 1977; Buus, 2009). In this study, we examine whether awareness of language barrier is a recognized component of clinical assessment. Indeed, we are interested to know how language barrier is described in the medical record, and how reading and writing progress notes transform clinical knowledge and practice regarding patients with limited or no mainstream language proficiency.
Theoretical framework
Drawing on the medical discourse literature, we study the medical record as a genre (Berkenkotter, 2008; Coker, 2003; Hobbs, 2004; Schryer, 1993). A genre is a conventional mode of communication shared by members of a community and which is formed by the social purposes it serves (Bakhtin, 1986; Fairclough, 1992). A genre is not static, it is open to innovation, manipulation, and change (Schryer, 1993). Evaluation of the medical record as a genre arose in modern Europe during the historical epistemological shift towards scientific rationality. It has been shaped by multiple influences over time (Schryer, 1993), informed by assumptions and epistemologies that validate, frame, and constitute what counts as clinical knowledge. Medical records were standardized in the 1980s (Berkenkotter, 2008; Class, 2014; Coker, 2003; Wilce, 2009), during a time in which experiential narratives were becoming increasingly acknowledged (Hunter, 2021). Currently, evidence-based and patient-centered care coexist in medical records and are not mutually exclusive. Evidence-based care stems from a positivistic medical model, and patient-centered care from medical humanities and discourse-based research (Roberts et al., 2004).
Methods
This is a secondary data analysis study which relies on qualitative data collection methods, specifically, semi-structured interviews and participant observation notes. According to Heaton (2008), one method of carrying out secondary analysis involves researchers re-using their own self-collected data in order to investigate new or additional questions. This applies to our study, where the participant selection process was based on secondary analysis of pre-existing data drawn from a larger previous mixed methods study conducted in a tertiary care hospital in Montreal, Quebec, Canada from July 2016 to May 2017.
This broader ethnographic study consisted of participant observation in the inpatient psychiatry ward, attendance in weekly clinical meetings, and semi-structured qualitative interviews with patients and clinicians. The Institutional Review Board of the CIUSSS West-Central Montreal, where participant recruitment took place, provided ethics approval for this study.
Setting
The study setting was a mid-sized tertiary care teaching hospital affiliated with an English language university, located in a multicultural area of Montreal, Quebec, Canada. At the time the data for this study were collected, the mother tongue of 79.1% of the Quebec population was French, 8.9% English, and 14.5% other languages (Statistics Canada, 2019). However, a survey study of 1000 participants performed at this hospital in 2010 showed that 65% of patients had a mother tongue other than French or English (Okrainec et al., 2014). Under the laws of Quebec, all health institutions in the province are obliged to offer services in French. In recognized bilingual institutions such as the hospital where the study was conducted, Quebec laws also guarantee the right of patients to receive services in English on demand. In practice, English is the dominant language of communication in this institution. There is no legal obligation to monitor linguistic barriers and ensure that health and social services are accessible to patients who are not fluent in either French or English. The only context in which access to an interpreter is mandatory is before the courts. At the hospital where this study was conducted, medical notes were handwritten, scanned, and uploaded to the electronic medical record, and clinical documentation was often the responsibility of the junior medical staff. Also, professional interpreters paid by the public health care system were available at this healthcare establishment on demand.
Participant recruitment and selection
Participant recruitment is illustrated in Figure 1. All 164 patients admitted to the psychiatry ward from July 2016 to May 2017 were approached for the larger mixed methods study. Patients were eligible to participate in the study if they were aged 18 years or older and considered clinically stable and competent enough by the treating clinician to participate. Participants who provided consent (N = 122) were interviewed by the research team during hospitalization.
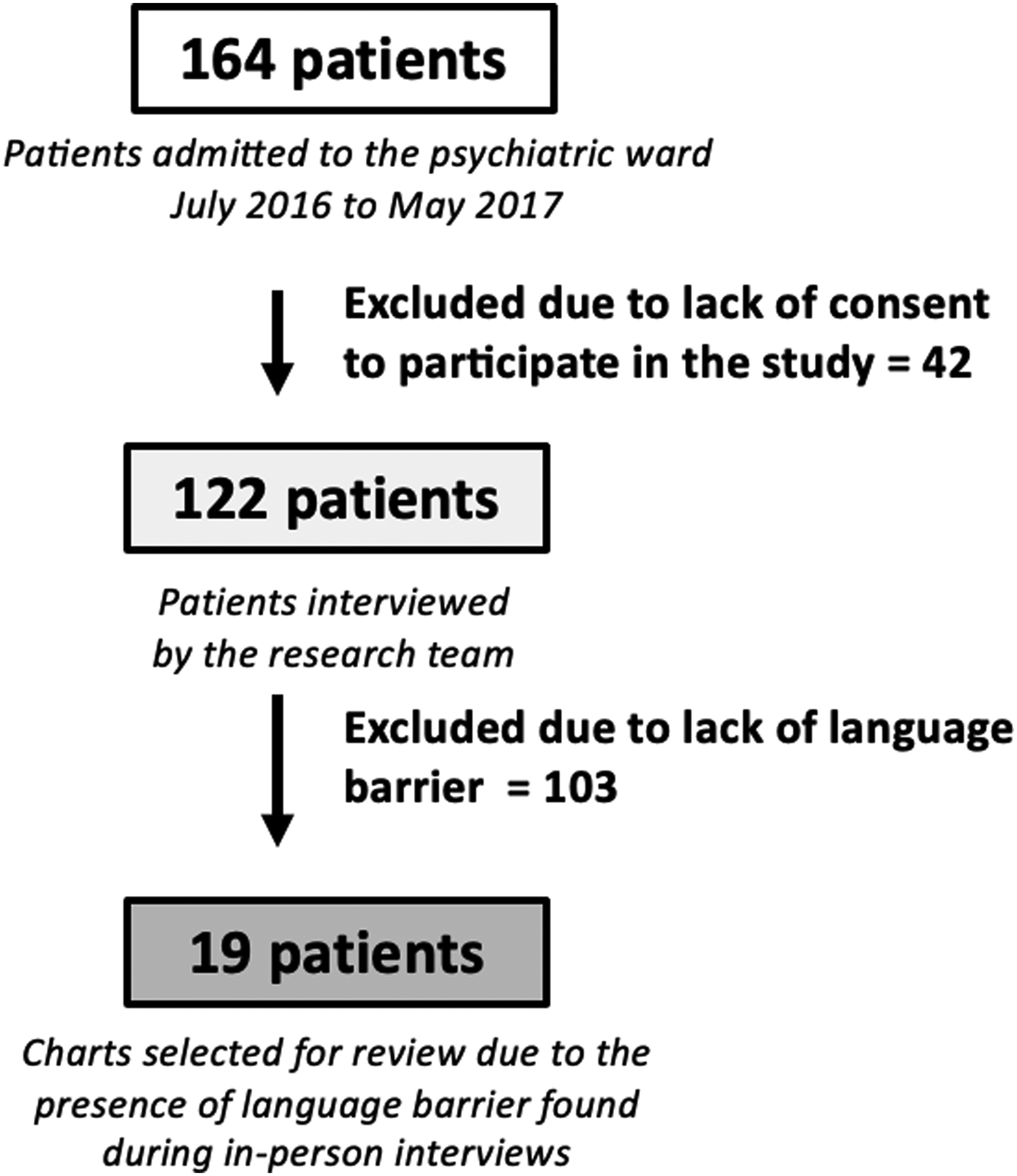
Participant recruitment and selection process.
Data for this article were gathered from participants in which a language barrier was deemed present because they fulfilled at least one of the following criteria: 1) The research team's impression was that there was a language barrier based on clinical weekly meetings and their observations while interviewing the patient; 2) The patient's self-assessment of their French and English proficiency was “basic” or less, and 3) When interviewed by the research team, the patient voiced interest in having an interpreter present when speaking with a physician. Nineteen patients met at least one of these criteria and were included in the final sample of participants whose medical charts were reviewed. For six of these patients there was no explicit mention of language barrier in the charts, but evidence of language barrier was noted during the interviews.
Measures/instruments
Data were collected via retrospective review of medical charts and of transcripts of direct interviews with patients. The patient interviews were semi-structured and guided by questionnaires that inquired about sociodemographic characteristics, as well as language history, preference and proficiency. Questions were mostly open-ended to permit maximum freedom of expression. When patients were asked to describe their English and French proficiency levels, answers were divided into the categories “excellent,” “good,” “basic,” and “none” (“none” meaning that the patient did not speak the language at all). Demographic and interview data were entered into a secure SPSS database.
Three research assistants carefully reviewed the 19 medical charts for every mention of a language barrier or use of an interpreter. Notes related to communication difficulties encountered by the team or an observed patient behavior that might be related to a language barrier were also included. The types of notes that were analyzed were emergency triage notes, emergency room notes, initial psychiatry consultation notes, progress notes, social worker notes, and discharge summaries. These qualitative data were entered into a secure database, where the following information with respect to each note was included: the verbatim note, its writer's role (doctor, nurse, social worker, medical student), chart location, and date recorded.
Data analysis
Qualitative methodology was informed by thematic and discourse analysis. Charting entries were analyzed for thematic content (Joffe, 2012) and a document summary form was created for each chart. Discourse analysis strategies were used to contextualize the meanings implicit in the themes. A dual deductive–inductive approach was considered the most appropriate to allow the generation of new ideas (Bernard, 2011; Bradley et al., 2007; Braun & Clarke, 2006).
The 19 medical records were evaluated and divided into two subgroups: 1) patients for whom a language barrier was documented at least once in their medical charts (n = 13), and 2) patients for whom a language barrier was never documented (n = 6). A documented language barrier was defined as an explicit reference to a patient's limited proficiency in the mainstream language (either English or French). For example, the clinician note ‘'Patient had problem speaking English fluently'’ was considered a documented language barrier.
All research assistants read the entries to get a general sense of the data before coding. Meetings took place to discuss differences and similarities in the codes that emerged. Based on these codes, we identified a preliminary list of major themes. Subsequent re-analysis of the data yielded additional major themes and sub-themes. During this process, codes were fractured, combined, and reorganized to develop conceptual categories. A select number of excerpts were chosen as examples to be cited in the article, and for each subtheme, a condensate was constructed to summarize the entries it contained.
Results
Participants
Participant socio-demographic and clinical characteristics are reported in Table 1. All participants were immigrants, except for one patient who was born in Canada, raised in a different country, and returned to Canada as an adult. The participants predominantly arrived in Canada as adults. Their first languages were diverse: Russian (1), Gujarati (1), Italian (2), Spanish (2), Tagalog (1), Mandarin (1), Polish (2), Cantonese (2), Romanian (1), Armenian (1), Farsi (1), Arabic (2), Tamil (1), and Greek (1).
Patient characteristics (N = 19).
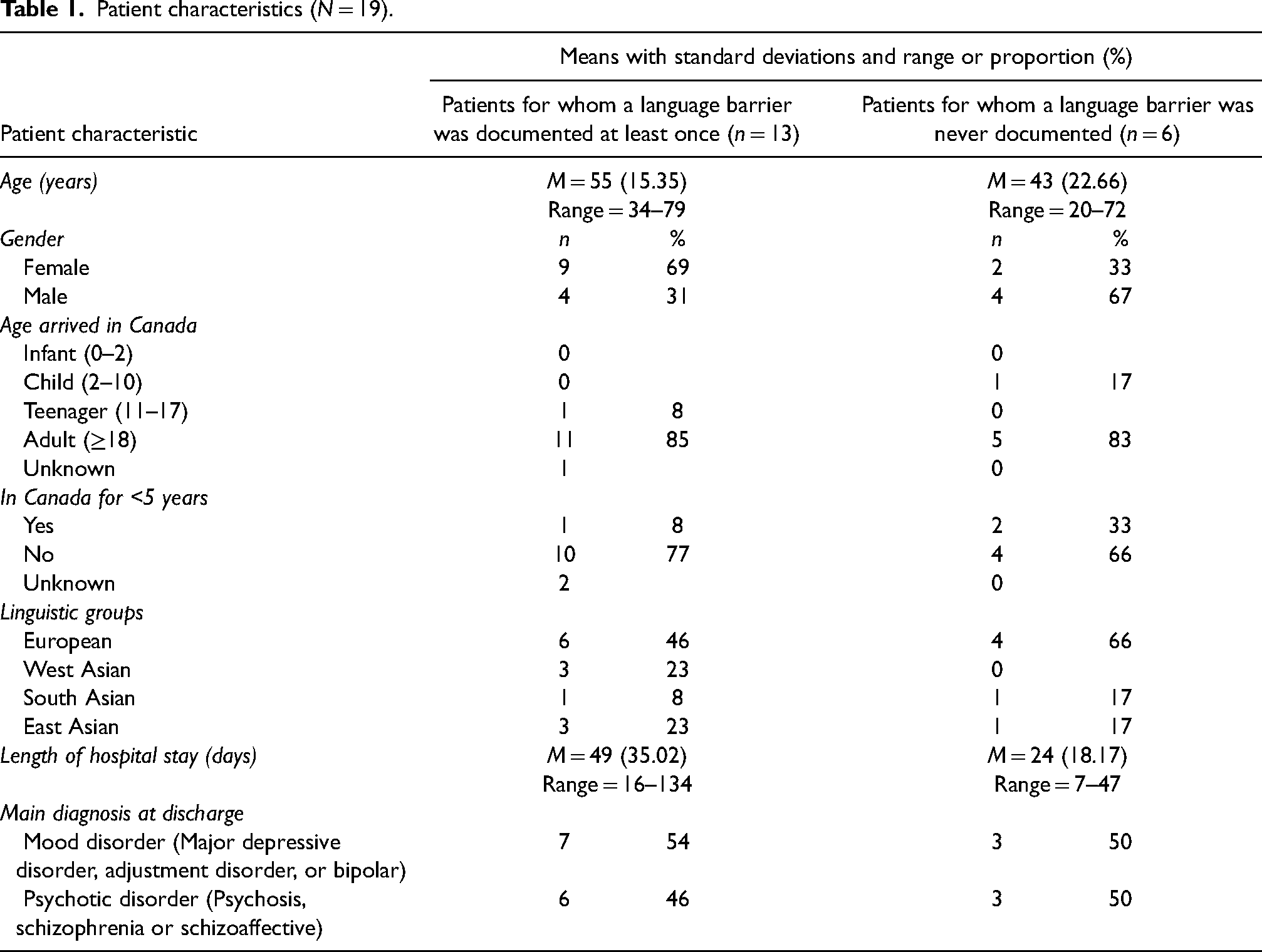
Table 1 also compares the characteristics of the following subgroups: 1) patients for whom a language barrier was documented at least once, and 2) patients for whom a language barrier was never documented. Table 2 provides an overview of participant proficiency in French and English. Given our small sample size, these tables are only meant to describe our sample without looking for statistically significant differences between the groups.
Assessment of language proficiency by chart data category (N=19)
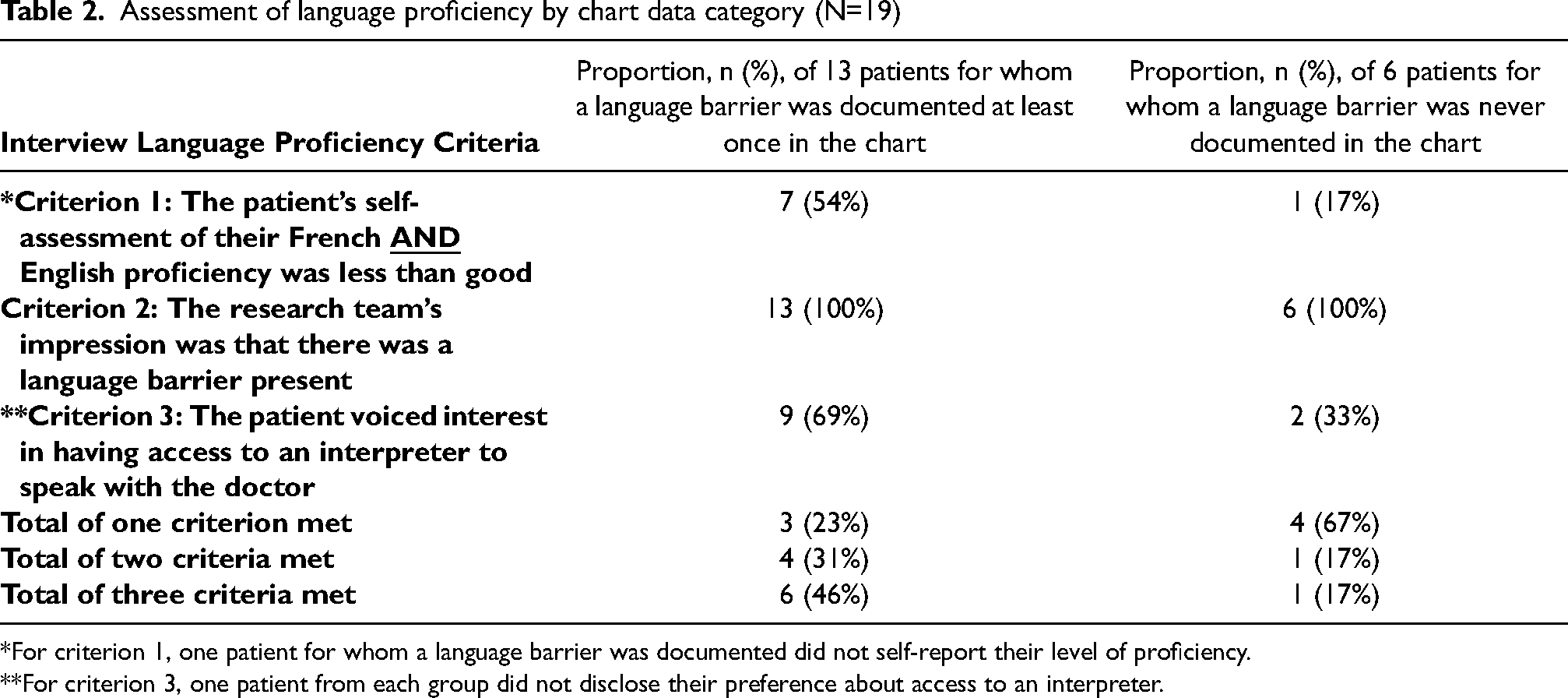
*For criterion 1, one patient for whom a language barrier was documented did not self-report their level of proficiency.
**For criterion 3, one patient from each group did not disclose their preference about access to an interpreter.
Quantifying documentation of language data
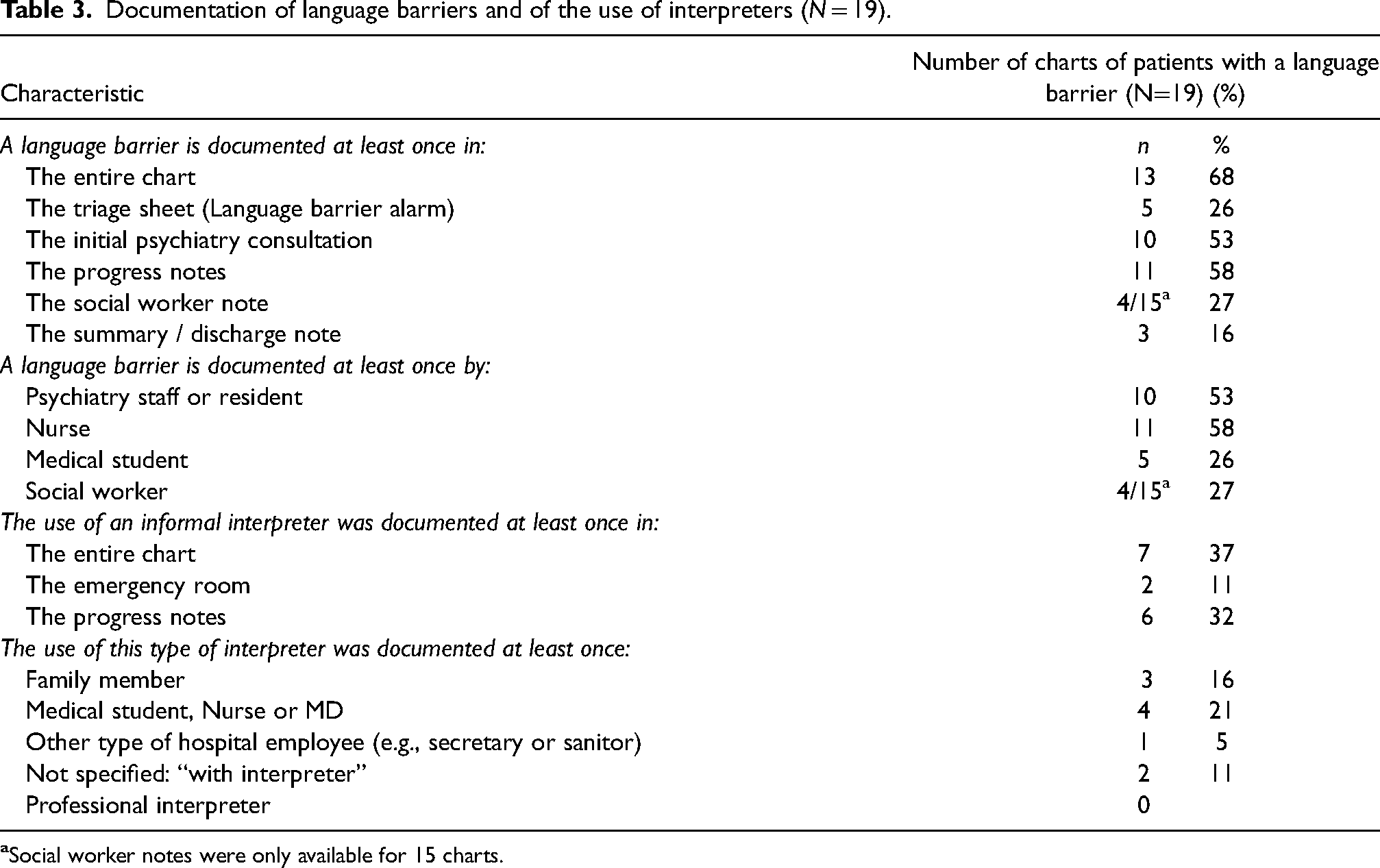
The presence of a language barrier was documented at least once in the medical charts of 68% of participants. Table 3 illustrates in which parts of the chart the presence of a language barrier was most often documented and by which healthcare professional. We found that even when language barriers were documented, no professional interpreters were contacted. When the use of interpreters was documented, they mostly consisted of patients’ relatives and healthcare professionals.
Documentation of language barriers and of the use of interpreters (N = 19).
Qualitative analysis of charts where a language barrier was documented (n = 13)
From all entries for which language data were documented, three overarching themes emerged to describe the clinical contexts and purposes that led clinicians to document this information: A) Acknowledgment of a language barrier, B) Negative impact of language barriers on evaluation and care, and C) Attempts to mitigate misunderstanding (see Table 4).
(A) Acknowledgment of language barrier: Clinicians most often documented the presence of language discordance between the medical team and patient with vague terminology and without mentioning the patient's level of French or English fluency in their medical chart entry. In particular, the recurrent use of the expression “language barrier” was noted, often accompanied by the words “significant,” “some,” “present,” “likely,” or the symbols “++”. When the patient's French or English proficiency level was documented, the descriptive phrases used included (where X stands for French, English, or both): “No” X, “Very limited” X, “Minimal” X, “Little” X, “Small amount of” X, “A bit of” X, “Problem speaking” X, “Not understanding X too well,” “some difficulty in” X, “+/-” X, “Some” X, and “Basic” X. Regarding the patient's mother tongue, frequently, the terms “Unilingual” X, “Almost unilingual” X, or “Speaks mainly” X were used, implicitly documenting that the patient had limited French or English proficiency. Furthermore, these descriptive phrases were often inconsistently used for the same patient throughout the chart, from one clinical assessment to another. For example, these entries were all found in the chart of the same patient: “Basic English,” “spoke fine English,” “patient has problem speaking English fluently,” and “understands English.” Factors that may have contributed to this heterogenicity are the impressionistic assessments of language proficiency, the complexity of the subject matter being broached with the patient, the depth and duration of the clinical interview, and the patient's changing mental status throughout hospitalization. Frequently, the patient's mother tongue was not mentioned when the presence of a language barrier was documented. Some entries referred to the patient's first language without explicitly naming it, with expressions such as “speaks only with Indian Language” and “only speaks mother tongue.” Some clinicians documented that they did not know the patient's mother tongue while acknowledging the presence of a language barrier. An entry inaccurately documented that a patient spoke “Hindou,” which is not a language name, while the patient spoke Tamil, and not Hindi. In several entries, clinicians implicitly documented the presence of a language barrier by stating that patients switched languages during the interview or expressed themselves uniquely in their mother tongue. There was no mention of the use of an interpreter in these entries, suggesting that the patient–clinician communication was limited during these encounters. Sometimes, clinicians implicitly reported language discordance by quoting the patient or describing the patient's speech and level of observed understanding. For example, the expressions “answering simple questions” or speaking a “few words” in French or English implied a patient's limited language proficiency. The ambiguity of the clinician's impression was highlighted by the frequent use of the phrase “seems to understand.” At times, clinicians documented uncertainty regarding the presence of a language barrier and the patient's level of understanding, especially in the context of psychopathology. (B) Negative impact of language barriers on evaluation and care: Clinicians repeatedly documented that the clinical assessment of language diverse patients was limited by communication difficulties that hindered history taking, mental status examination, and differential diagnosis. They reported being “unable to” or that they “can’t” assess patients “thoroughly,” “properly,” or “fully” “due to” a language barrier. Clinicians frequently used the term “difficult” to describe their attempts to assess physical symptoms, orientation, and thought content. When documenting assessments, clinicians often conveyed that their impression was uncertain: “Seems oriented x3.” The “interactional uncertainty” (Roberts et al., 2004) experienced by clinicians in talking with multicultural and multilinguistic populations is expressed in the medical records through vagueness of terminology describing language proficiency and deficiency in patients, and through heightened difficulty assigning a diagnosis. Clinicians also documented complexities in obtaining informed consent and filling out application forms when treating some patients with language barriers. Chart entries showed that family members sometimes obtained consent from the patient for the clinical team. When one patient had to undergo a colonoscopy, nurses documented that the daughter called the patient to explain the test and “to tell her that she will have to cooperate + sign the consent form for the order to get the c-scope.” Regarding the day-to-day behavioral management of patients with language barriers, clinicians—mainly nurses—documented the need to use coercive measures in the context of communication difficulties that limited access to verbal de-escalation techniques. In the absence of an interpreter during an emotional crisis on the ward, although clinicians spent “++ time with the patient,” they reported that the patient was “not responding to reassurance” and refused oral medication, as they did not understand each other due to a language barrier. In such entries, use of urgent intramuscular medication was often documented. The use of wrist restraints was documented with an agitated patient. In this case, physicians charted that they had difficulties differentiating delirium from psychosis due to a language barrier: “Pt alert, orientation ? Unilingual (don’t know what language?) As per report confused ++, needs wrist restraints.” Clinicians also documented the negative consequences of language barriers on patient satisfaction with their doctors and their ability to socialize with other patients on the psychiatry ward. Indeed, clinicians often reported that patients self-isolated in their rooms due to language discordance and noticed that patients’ moods seemed negatively affected by communication barriers, such as a patient being “more irritable” when feeling misunderstood. On the other hand, nurses at times documented that patients positively acknowledged their efforts to improve communication. For example, a patient smiled after a nurse helped him verbalize his thoughts via prompting with a word. Poor patient–doctor communication was repeatedly documented by clinicians when caring for patients with language barriers. At times, the vocabulary used suggested frustration by showing how this reality was normalized in the healthcare system: communication was deemed difficult “as usual,” and a patient who was described as mute was considered at “baseline as speaks [X language] uniquely.” (C) Attempts to mitigate misunderstanding: Clinicians sometimes documented the use of informal interpreters, such as healthcare professionals and relatives of patients. When the use of an interpreter was charted, it was often in the context of the clinician assessing for suicidality, orientation, physical symptoms, and mood. Often, the medical charts reported that the family played the role of messenger between the team and the patient without being involved in direct translation. For example, clinicians documented that families provided collateral information or medical explanations to the patient on behalf of the team. On one occasion, the team called a patient's daughter to ask her to inform the patient that “there will be consequences when aggressive with co-pts or staff or anyone.” During acute emotional crises on the ward, especially those occurring late in the evening, nurses often documented that the family was contacted so that they could speak with the patient on the telephone and communicate the patient's thought content to the team.
Qualitative analysis of excerpts where a language barrier was documented.
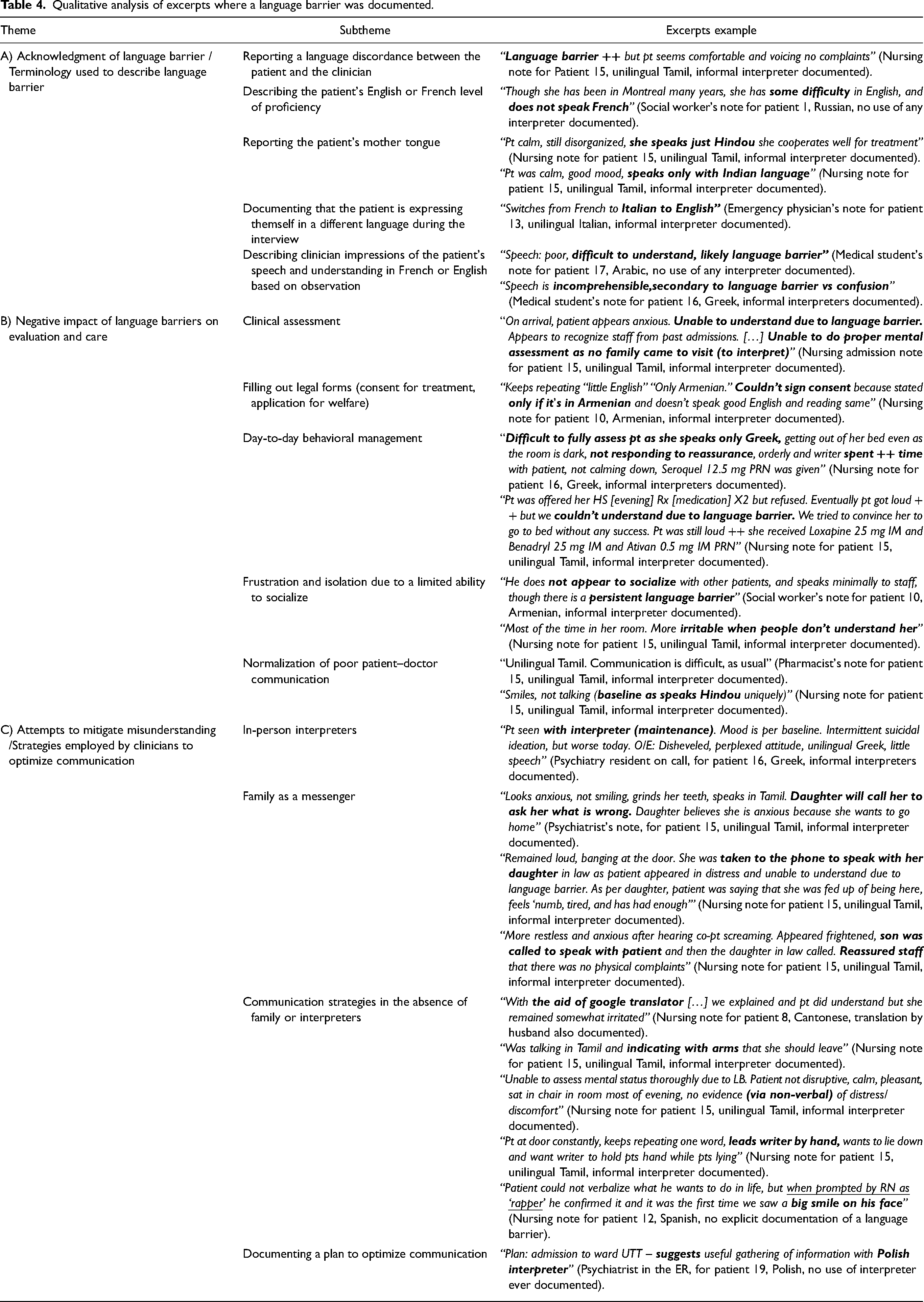
In the absence of an interpreter or family, clinicians relied on other communication strategies, such as non-verbal communication, slowed and simplified speech, or tools (e.g., Google translate) to overcome language barriers. Clinicians documented non-verbal efforts that patients made to engage with the team to be understood. Despite these efforts, clinicians described limited assessments in these entries, such as incomplete mental status evaluations.
In some notes, clinicians documented the need to plan strategies to optimize communication, such as organizing for an interpreter or calling the family. While not all entries were followed by a documented use of an interpreter, no explanations were offered as to why the plan was never implemented.
Discussion
Documentation of language data: Lacking, inconsistently collected, or inaccurate
This study found that the presence of a language barrier was documented for only 13 out of 19 patients with limited English and French proficiency. Other than the designated space for a “language barrier alarm” in the emergency triage note, which was only used for 5 out of 19 participants, no other space existed to systematically report language data in the medical chart. In the clinical notes, limited language proficiency was most often documented in the patient's identification information and mental status exam. The terminology used by clinicians to document limited language proficiency was vague and unstandardized.
Despite the fact that documenting language data improves planning for interpreting services (Nerenz et al., 2009), this study found that language data, when it was charted, was not in a form that helped clinicians to provide interpreters for patients. For example, when a language barrier alarm was activated in the triage note, the patient's preferred language was not usually indicated. Some entries included inaccurate information, such as the wrong mother tongue. These findings are consistent with previous literature indicating that language data were inconsistently collected, of questionable quality, and often inaccurate and incomplete (Bowen, 2015; Hasnain-Wynia et al., 2006; Nailon, 2007; Nerenz et al., 2009; Regenstein & Sickler, 2006; Wilson-Stronks & Galvez, 2005).
Okrainec et al. (2014) recommended documenting language preference, self-reported language proficiency, and observed language discordance. Unfortunately, in this study, healthcare professionals rarely explicitly documented patients’ self-reported language proficiency or preferred language, which suggests that they may not systematically ask these questions. Language proficiency assessment strategies were not standardized and were mostly based on clinician observations. This is suboptimal, given that Hasnain-Wynia et al. (2004) reported that patients are more likely to provide accurate information about their language than clinicians.
Factors that may contribute to a lack of documentation of language barriers
In the six charts that contained no documentation of any language barrier and no assessment of the patient's language proficiency, the patients’ limited ability to express themselves with the team was attributed entirely to the patient's psychopathology. For example, a 45-year-old woman diagnosed with bipolar disorder was described as “uncooperative with interview” and “not answering to questions, pulled blanket over her head to ignore questions.” When she did speak, it was noted that she “speaks in very few words” and she was observed “speaking Romanian to herself, ignoring people.”
Data analysis highlights the fact that language barriers exist within an ill-defined spectrum, from mild to more severe forms of communication impairment. Whereas clinicians charted the presence of severe language barriers repeatedly, milder language barriers were less readily documented. The six patients whose language data were never documented self-rated their own language barrier as milder compared to the 13 other patients for whom language data were documented at least once. As presented in Table 2, these six patients met fewer inclusion criteria, voiced less interest in having access to an interpreter, and self-rated their English as at least basic. Nonetheless, the following observations were made by researchers when they interviewed these six patients: they tended to switch from one language to another to express themselves, they seemed to be searching for their words in English and French, and they seemed to express their emotions and thoughts more calmly, and with more ease in their mother tongue when it was offered through informal interpreters.
Psychopathology may exacerbate a patient's limited ability to express themselves in a second or third language, even for individuals who have a basic and functional level of French or English when their psychiatric condition is stable. When interviewing psychiatrically unstable patients, clinicians may not recognize to what extent an underlying language barrier contributes to signs of an altered mental state, such as incoherent speech or poverty of thought. Given that language is the main diagnostic tool in psychiatry, and that basic rights can be suspended based on psychiatric assessments, more rigorous screening questions to assess for the need of an interpreter are of critical importance to patients and clinicians alike.
Underutilization of interpreters and normalization of limited patient care
Although language barriers were documented in 68% of patient charts with poor French or English proficiency, the use of an interpreter of any type was only documented 37% of the time. This is consistent with the literature, where some studies observed that despite adequate documentation of language needs, use of available interpreter services remained low (Brophy-Williams et al., 2020; Regenstein & Sickler, 2006; Regenstein et al., 2008). This suggests that the effects of documentation on quality of care may be limited, while keeping in mind that interpreter use also may be poorly documented, as suggested by previous studies (Garrett et al., 2008; Regenstein, 2007; Regenstein et al., 2009).
Although the literature recommends systematically working with qualified interpreters during psychiatric assessments of individuals with limited language proficiency (Skammeritz et al., 2019), and discourages the use of ad hoc interpreters, the use of trained interpreters was never documented in this study. When the use of interpreters was reported, it mostly consisted of patients’ relatives and healthcare professionals. In one instance, the clinician specified that a proper assessment was not possible “as no family came to visit (to interpret),” highlighting that some clinicians may consider family members to be the standard of care for translation purposes. Previous literature has demonstrated that there is an increased risk of interpreting errors when using ad hoc translators such as family members (|Flores et al., 2012). Relatives who translate are at increased risk of making communication errors such as information omission, addition, and mistranslation, which can have harmful effects on diagnosis and treatment (|Labaf et al., 2019). Furthermore, the use of a family member raises ethical concerns regarding confidentiality. According to Nielsen et al. (2020), not only is patient care compromised when family members interpret in healthcare settings, the relatives themselves are at risk of detrimental psychological consequences as a result of being involved in highly sensitive ethical dilemmas that may impair family relationships (Nielsen et al., 2020). Our study suggests that clinicians perceive professional interpreting resources to be inaccessible or lack awareness regarding the importance of trained interpreters.
Tribe and Thompson (2022) offer recent guidelines on the use of interpreters in mental health, in which they highlight the need to work with professional interpreters who have undergone a recognized language testing. In particular, qualified interpreters are strongly recommended during an initial assessment and when medication is being prescribed or an intervention offered. Professional interpreters commit less interpretation errors and improve clinical outcomes and patient satisfaction with care (Elkington & Talbot, 2016). In mental health in particular, a patient is more likely to disclose sensitive information with a trained interpreter who has developed interpersonal skills and can offer a confidential setting. Efficient collaboration with trained interpreters can also inform clinicians on cultural factors that can affect expression of emotional problems and of idioms of distress (Tribe & Thompson, 2022).
The guidelines from Tribe and Thompson (2022) also stress the need for clinicians to undertake training courses to efficiently work with professional interpreters. Some examples of practical recommendations when working with interpreters include planning more time for such assessments, avoiding using complicated technical language, avoiding the use of proverbs which may be culture-specific, favoring shorter sentences, and keeping eye contact with the patient most of the time to avoid making them feel excluded. It is preferrable to work with the same qualified interpreter if a series of meetings will take place for a same patient. Furthermore, it is recommended to plan for 10–15 min in advance of the session to brief the interpreter about the purpose of the meeting and to determine the preferred interpretation mode (e.g., word-for-word translation versus a constructionist mode by which the overall meaning is conveyed to the patient). When healthcare professionals have been formally trained to collaborate with interpreters, their willingness to participate in interpreter-assisted interventions increased (Elkington & Talbot, 2016). For example, a recent German study evaluating the feasibility of a collaborative learning module for medical and nursing students showed that the students felt that their skills working with interpreters increased after a 3-hour course (Krampe et al., 2022).
Most healthcare professionals are aware of the negative consequences that language barriers have on clinical assessment, management, hospitalization experience, and informed consent. Some entries suggest that clinicians document a language barrier to justify, for medico-legal purposes, why it was impossible to provide better care. In other scenarios, clinicians document attempts to optimize communication with patients. The strategies employed, however, are not evidence-based, inconsistently used, and have limited benefits. Sometimes healthcare professionals use desperate measures, such as calling family members late in the evening to assess patients in distress. While clinicians do their best to help patients, their clinical notes suggest that they feel unsupported when repeatedly faced with a language barrier. As a result, less than optimal patient care becomes the norm for language diverse patients.
Strategies to improve documentation practices and professional interpreter use
A growing literature recommends strategies to improve the collection of language data. Healthcare organizations should develop standardized methods of integrating language data into medical charts (Hasnain-Wynia et al., 2004). This should include designating a location within the registration system to collect language information, while implementing required fields and pop-up reminders (Regenstein et al., 2008). Tools integrated in the Emergency Medical Record (EMR) such as the Language Services Documentation Tool (LSDT) could help remind clinicians of the importance of offering interpreting services. The LSDT consists of a single-question prompt starting with “Language Needs Met By” that a provider must complete before a chart can be closed when a patient has been flagged as having a language barrier (Paradise et al., 2014).
The triage note “language barrier alarm” would be more useful if clinicians were prompted by the EMR to write the patient's mother tongue and preferred language. In an officially bilingual hospital in Quebec, we would recommend that clinical staff rate the patient's proficiency in French and English with checkboxes (excellent, good, basic, none) in the EMR. To simplify collection, previous research has recommended that each hospital develop a list of common languages used by their service population, accompanied by an open-ended response option for those whose language is not listed (Nerenz et al., 2009). The literature also suggests standardizing which healthcare professional collects this information, and when the data are collected (Hasnain-Wynia et al., 2004). Documenting language needs is imperative at the patient's initial point of contact with health services to efficiently coordinate patient-centered care (Nailon, 2007).
This study recommends integrating fields pertaining to language data on consent forms, such as the consent form for electroconvulsive therapy. We recommend that such forms contain a required checkbox indicating that the patient was offered access to interpreter services if there were indications that the person had limited linguistic proficiency in French and English. Not only is informed consent crucial to deliver safe, ethical, and patient-centered care, it is also legally mandatory. Performing a medical procedure without obtaining informed consent implies potential civil and criminal liability for the healthcare professionals and the institution. Data from this study, however, suggest that valid consent was compromised by language barriers. This is consistent with the findings of Schenker et al. (2007) who concluded that, despite the availability of interpreter services, hospitalized patients with a language barrier are less likely to have documentation of informed consent.
Documenting a patient's mother tongue may not translate into knowledge of a patient's language status. In one instance, a nurse wrote “language barrier ++ (but do not know which language),” when the language of the patient had been specified on many occasions in the chart. Even though direct clinical benefits of accurate documentation may be modest, language data collection should still be encouraged to guide quality improvement projects and policy changes through research (Department of Health and Human Services, 2000; Rittner et al., 2010). To increase the clinical usefulness of collecting language data, research suggests implementing strategies to link data directly with interpreting services. For example, Regenstein (2007) concluded that linking patient registration directly to professional interpreter scheduling appears to decrease wait times for interpreter services.
Clinicians may also lack training to systematically screen for language barriers and to document them. The literature demonstrates that many physicians face barriers which impede accurate language data collection including concerns about confidentiality, legality, lack of awareness of the usefulness of interpreters, difficulty recording data, fear of offending patients who may feel themselves to be victims of language discrimination, as well as a lack of adequate resources (e.g., funding, time) (Williams-Roberts et al., 2018). Research has reported considerable physician discomfort when asking patients about their race, ethnicity, and first language (Hasnain-Wynia et al., 2010).
Clinician training should teach how to ask patients about their language proficiency and preferences, and how to chart this information consistently (Hasnain-Wynia et al., 2007; Hasnain-Wynia & Baker, 2006). We suggest that the following be included in medical school teaching about the mental status examination: when assessing and describing patient speech process and thought form and content, clinicians should consistently screen for language barriers, document uncertainty about a possible language barrier, and offer an interpreter when in doubt about the quality of the clinical communication. In previous research studying patient perspectives regarding interpreting services, Schwei et al. (2018) found that participants who identified as having some basic English proficiency did not always think an interpreter was needed. We suggest that even when patients are not interested in interpreting services, clinician observations of patient's limited English and French should still be documented, especially in psychiatry, for the purpose of assessing the patient's mental status appropriately. Interpreters can be offered and available in case the patient decides to use them at some point during the interview, especially when discussing emotionally or cognitively complicated experiences.
Strengths and limitations
To our knowledge, this is the first study to describe documentation of language data in a psychiatric inpatient setting. The presence of language barriers was not defined by a single question but involved triangulation of data collected from patient self-reports of language proficiency and preference, as well the research team's impressions after interviewing patients. This made our selection process more attuned to our study setting and highlighted the complexity of defining language barriers, as well as the importance of avoiding asking a single question to assess the need for an interpreter. Our study also has local relevance for quality improvement.
However, our study is not without limitations. Given the small sample size, statistical analyses were not possible. Given that the data were collected in 2016−2017 prior to the COVID-19 pandemic, they might not reflect today's reality, as we suspect that wearing personal protective equipment such as masks may make non-verbal communication more difficult. Furthermore, our discussion does not reflect the potential impacts of language legislation known as “Bill 96” that was adopted by the Quebec National Assembly in 2022. We expect that this legislation, which strengthens the rules favoring usage of the French language when operating businesses with Quebec clients, will bring major changes to language use in the entire public sector, including the health sector.
For the qualitative analysis, some handwritten notes were illegible, and therefore could not be included. Also, one of the 19 patients did not self-report his language proficiency or comment on his interest for an interpreter, such that he was included solely based on the research team's impression that a language barrier was present based on his interview.
Given that our study has a small sample size and took place only at one site, it has some obvious built-in limitations to generalizability. Nonetheless, it highlights the importance of recognizing, documenting, and addressing language barriers in psychiatric care through the use of professional interpreters and clinician training. These fundamental aspects of patient care are applicable to any healthcare setting in which language barriers are present.
Conclusion
In conclusion, our study has explored the medical record as a genre, where evidence-based and patient-centered care coexist. Our analysis has shown that Progress Notes offer the space to combine the two modalities and express uncertainty with regard to language barriers. Overall, documentation of language data was lacking, inaccurate, or vague. Even when a language barrier was charted, professional interpreters were never used. Family members and clinical staff acted as informal interpreters to satisfy clinical expediency.
These findings show that a change of institutional culture is imperative to provide safe and equitable care to psychiatry patients with limited mainstream language proficiency. Clinician education and standardization of documentation practices could help improve the quality of language data collection. However, documenting the presence of language discordance and its negative impact on care may not lead to the use of professional interpreters or to awareness of a given patient's language status by clinicians further downstream. Compromised assessments and suboptimal care are normalized for language diverse patients, as clinicians often perceive professional interpreting services as inaccessible or impractical. Although more in-depth empirical research is needed, this study has shown that the lack of informed consent, use of restraints, and use of injectable medications are all very striking examples of the risks of psychiatric care without interpreters. These findings highlight the need for federal or provincial laws mandating access to translators in healthcare, such as the antidiscrimination provisions in the United States federal law that require health programs and clinicians to take reasonable steps to provide interpreter access to individuals with limited English proficiency (Jacobs et al., 2018). Such laws would oblige hospitals to implement a method of accessing professional interpreters. Institutional policies must also be implemented to support the systematic use of professional interpreters in mental healthcare settings and should involve clear protocols that guide clinicians when they screen for the need of interpreters, rather than relying solely on clinical impressions.
When addressing language discordance, it is essential to keep in mind that participants may have a number of challenging characteristics, such as suffering from severe mental illness, being a recently arrived immigrant, and having a low level of education and health literacy. In a complex, intersectional picture that predisposes to discrimination, individual voices may be silenced, and their rights compromised by their limited ability to advocate for themselves. In psychiatry, healthcare organizations must exercise the political will to implement policies that mandate the use of professional interpreters when patients speak the mainstream language poorly or not at all. This would protect patients by allowing them to represent themselves in the language that best portrays their cognitive abilities, emotional state and thought process, and by enabling them to safely consent to the treatment offered. These same improvements would benefit clinicians by giving them evidence-based tools to evaluate and treat patients from linguistically diverse backgrounds and challenging symptom profiles.
Footnotes
Acknowledgments
We thank the research assistants Maria Imoli, Laura Avigan and Olivier Dionne who helped with data acquisition by interviewing patients on the ward.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The project was funded by Health Canada Health Care Access for Linguistic Minorities via Dialogue McGill Project (1415-HQ-000090) PI: Dr G. Eric Jarvis.