
Abstract
Between 16 and 20% of perinatal women in low- and middle-income countries experience depression. Addressing postpartum depression (PPD) requires an appreciation of how it manifests and is understood in different cultural settings. This study explores postpartum Mongolian women's perceptions and experiences of PPD. We conducted interviews with 35 postpartum women who screened positive for possible depression to examine: (1) personal experiences of pregnancy/childbirth; (2) perceived causes and symptoms of PPD; and (3) strategies for help/support for women experiencing PPD. Unless extreme, depression was not viewed as a disease but rather as a natural condition following childbirth. Differences between a biomedical model of PPD and local idioms of distress could explain why awareness about PPD was low. The most reported PPD symptom was emotional volatility expressed as anger and endorsement of fear- or anxiety-related screening questions, suggesting that these might be especially relevant in the Mongolian context. Psychosocial factors, as opposed to biological, were common perceived causes of PPD, especially interpersonal relationship problems, financial strain, and social isolation. Possible barriers to PPD recognition/treatment included lack of awareness about the range of symptoms, reluctance to initiate discussions with providers about mental health, and lack of PPD screening practices by healthcare providers. We conclude that educational campaigns should be implemented in prenatal/postnatal clinics and pediatric settings to help women and families identify PPD symptoms, and possibly destigmatize PPD. Healthcare providers can also help to identify women with PPD through communication with women and families.
Introduction
Even before the COVID-19 pandemic, mental health disorders posed a significant burden worldwide; in fact, in 2019, depression was the second leading cause of disability globally (IHME, 2021). While depression may not be associated with high mortality, the chronic morbidity it can cause is staggering. Studies suggest that mental and behavioral disorders are among the leading causes of disability and lost years of health globally (Patel et al., 2016; Rehm & Shield, 2019).
Approximately 16% of pregnant women and 20% of postpartum women in low- and middle-income countries (LMICs) experience clinical depression (WHO, 2015). Postpartum depression (PPD) is defined as major depressive disorder with symptom onset during pregnancy or within four weeks (DSM-5) to six weeks (WHO) after childbirth (American Psychiatric Association, 2013; WHO, 2016). The diagnostic criteria specify that five or more associated symptoms must be present nearly every day for at least two weeks. These include depressed mood, loss of interest or pleasure in activities that are normally enjoyable, change in appetite, insomnia or hypersomnia, psychomotor agitation or retardation, fatigue/decreased energy, and feelings of worthlessness or excessive/inappropriate guilt, among others (WHO, 2016). The risk factors for PPD can be grouped into five main categories—physical/biological, obstetric/pediatric, sociodemographic, psychological, and cultural—with the relative influence of each risk factor varying based on person and context. All women can develop PPD, but poverty, migration, extreme stress, exposure to violence, and low social support generally increase the risk (WHO, 2015).
PPD can negatively impact women's everyday functioning as well as interpersonal relationships. Mother–infant interactions essential for children's normal development, and basic needs can be critically disrupted. Some studies have found strong correlations between maternal depression and poor infant/child health outcomes, including impaired infant emotional, cognitive, and motor development, as well as negative impacts on breastfeeding practices, child growth, sleep habits, and child healthcare utilization (Almond, 2009; Chen et al., 2021; Farias-Antunez et al., 2018; Hanlon, 2013; Letourneau et al., 2012; Surkan et al., 2011; Tsai & Tomlinson, 2012).
Although effective PPD treatment options exist (Leight et al., 2010), the proportion of those untreated is very high. The WHO has estimated a shortage of 1.18 million mental health care specialists in LMICs and the “treatment gap,” estimated at 76–85% (Scheffler & The World Health Organization, 2011), is attributed to differing public health priorities, a lack of mental health policy and legislation, and a lack of financial and human resources, among other factors (Kakuma et al., 2011; Patel et al., 2007).
An important part of treating PPD is appreciating how it is conceptualized by women, families, and health professionals, including mental health professionals but also primary care physicians and other types of providers. The field of transcultural psychiatry teaches that although some similarities may exist across cultures, psychological conditions often manifest in dramatically different ways in different places and among different populations (Kirmayer & Pedersen, 2014). People may exhibit divergent beliefs in terms of how they understand and experience health and illness (i.e., their explanatory models) and how they express psychological distress (i.e., their idioms of distress). A nuanced understanding of how manifestations of mental illness such as PPD can be both individually and culturally determined is critical to promoting mothers’ and children's health.
Several studies have examined predictors of PPD in Asian settings. Nisar et al.'s (2020) systematic review on perinatal depression in Mainland China found that lower socioeconomic status, poor physical health, anxiety about pregnancy, and reduced social support were major risk factors, while better living conditions and a higher level of education were protective factors for perinatal depression. Dadi et al.'s (2020) meta-analysis of 64 studies on antenatal depression in LMICs found that pregnant women with a history of economic difficulties, poor marital relationships, common mental disorders, poor social support, poor obstetric history, and exposure to violence were more likely to report antenatal depression. Similarly, Klainin and Arthur's (2009) review on PPD in 64 studies from 17 Asian countries found that psychological risk factors for PPD included anxiety, past psychiatric history, stressful life events, childcare stress, negative affect, low self-esteem, poor self-image, and negative attitudes toward employment. Socio-demographic risk factors included economic difficulties, being a homemaker, domestic violence, and a lack of emotional support and/or dissatisfaction with support from husband, parents, and parents-in-law. Oates et al. (2004) examined perspectives of PPD across 11 Asian countries and found contributing factors included tiredness, marital and family conflict, and lack of social support. There was a seemingly universal recognition of PPD as a primarily psychosocial phenomenon. The healthcare professionals who participated in the study recommended increasing mental health service provision, whereas mothers and families viewed the solution within the personal and psychosocial realm, illustrating disparities in the way that providers, women, and families characterize PPD, and the importance of cultural context.
Further research on the perspectives of Mongolian mothers is integral to inform PPD education, screening, and treatment (Almond, 2009; Oates et al., 2004). To date, no other known study has been conducted on Mongolian mothers’ perspectives on PPD and only two other studies have been conducted on PPD in Mongolia. Pollock et al. (2006) examined the validity and internal reliability of two screening tools for PPD in detecting depression in Mongolian women of reproductive age. Pollock et al. (2009) assessed PPD prevalence and risk factors among 1,044 women in the capital city and found an estimated prevalence rate of 9.1%, with marital relationships, food insecurity, dissatisfaction with pregnancy, maternal health problems since birth, and concern about the baby's behavior as risk factors (Pollock et al., 2009). The dearth of studies on Mongolian women's explanatory models and idioms of distress in the context of PPD contributes to the limited understanding of PPD, its manifestation, and the interplay of risk factors as they relate to mothers’ lived experiences within Mongolian society. This study addressed this deficit by exploring the ways in which PPD manifests in postpartum Mongolian women, with resulting implications for how to best identify and treat it.
Methods
This mixed-methods study was conducted at the National Center for Maternal and Child Health (NCMCH) in the capital city of Ulaanbaatar, which serves a diverse patient population from both urban and rural areas. The four study objectives were to: (1) determine the prevalence of PPD among a sample of postpartum women who had recently given birth at the NCMCH; (2) identify potential predictors of PPD; (3) explore how women understand and experience PPD; and (4) identify ways to improve identification and treatment of PPD. A mixed-methods study design seemed most appropriate, given the lack of information available on this topic and the importance of appreciating the cultural nuances around this topic. A combination of data collection methods allowed us to survey a larger sample on questions that were easily answered with multiple choice responses versus exploring the more nuanced.
Health professionals at the NCMCH invited all eligible mothers to participate in the study. Eligible mothers were those who: (1) had given birth within the last six weeks; (2) had a postpartum visit at the NCMCH during the study period; (3) were willing and able to give informed consent; (4) spoke Mongolian; and (5) had given birth to a healthy baby without complications. Participants were given a short survey with questions on demographic characteristics (age, marital status, education, and income), and pregnancy and birth history.
At the approximately four weeks postpartum health check, women were screened for PPD using two screening tools: the Edinburgh Postnatal Depression Scale (EDPS) and the WHO 20-item Self-Reporting Questionnaire (SRQ-20). Both tools have been validated and widely used, including by Pollock et al. (2006) in Mongolia. We used both tools in order to examine whether one tool would be more culturally relevant in this setting. The EDPS has 10 questions (maximum score of 30) assessing symptoms over the last seven days. The SRQ-20 has 20 questions (maximum score of 20). Women with scores of ≥8 on the SRQ-20 and/or ≥11 on the EPDS (as used by Pollock et al., 2006) were referred immediately for evaluation by the NCMCH psychologist. Anyone who later expressed suicide ideation during the study was also immediately referred to a psychologist who was available 24/7 for the study.
All women who screened positive during the first six weeks of the study were invited to participate in follow-up interviews. The one-on-one interviews, lasting about 30–60 min each, were conducted within two weeks of the screening. They were conducted in the Mongolian language in a private space in the clinic by a Mongolian obstetrician-gynecologist trained in qualitative methods. A loosely structured question guide was developed based on the literature and our previous research on PPD in Mongolia (Trop et al., 2018). The questions covered four key domains: (1) Sociocultural context of pregnancy/childbirth; (2) Women's perinatal mental health; (3) Personal experiences of pregnancy/childbirth; and (4) Life before and after the baby. Participants received US$10 compensation. The interviews were audio recorded, transcribed, and translated into English. Using a thematic analysis approach, the transcripts were reviewed at least three times independently by three research team members to develop a coding scheme and identify emergent themes. We then applied the codes during the coding phase, refining the codes as necessary through group discussions. We also conferred with the larger local Mongolia team to ensure accurate interpretation of the results. Discrepancies in coding were discussed and resolved among all team members. Representative quotes were extracted to illustrate these themes, with pseudonyms used to protect privacy. All participants gave written informed consent. Ethics approval was received from the University of Southern California and the national Ethics Review Board of Mongolia.
Results
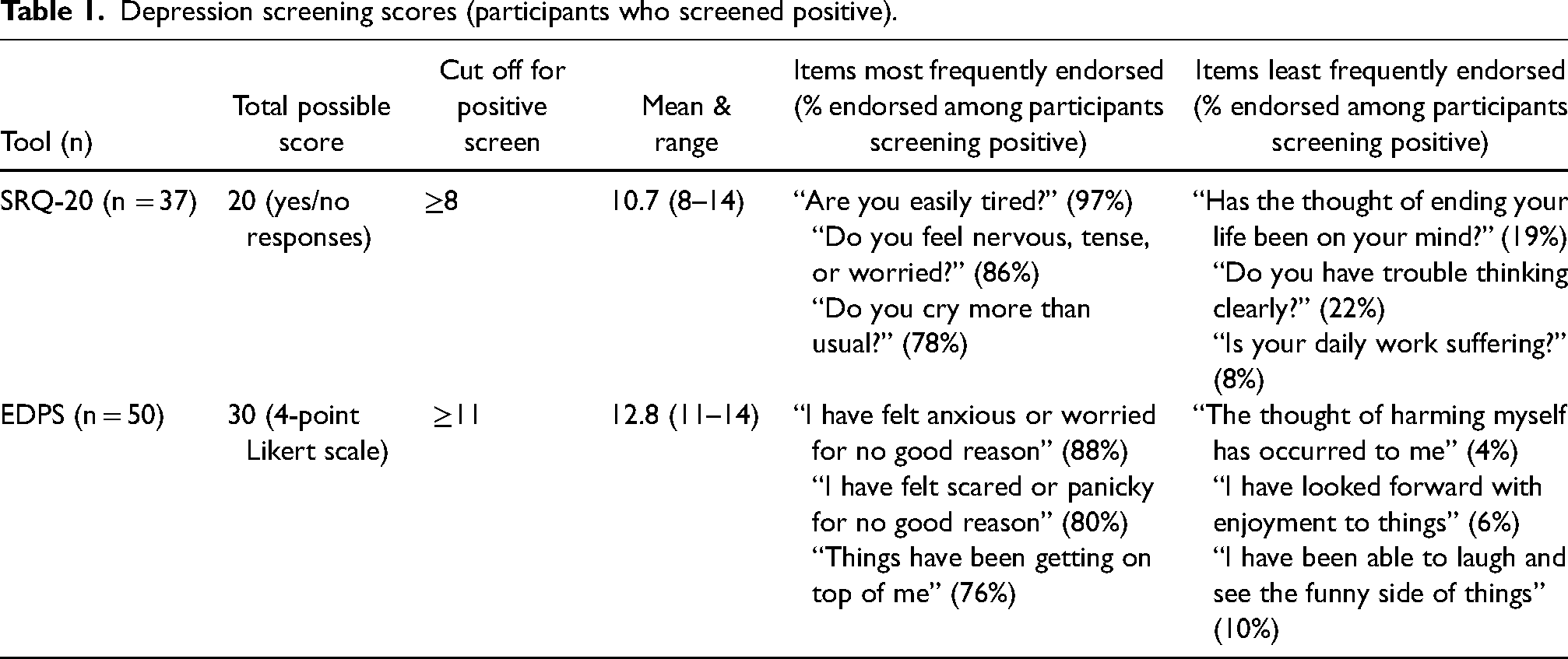
In total, 349 women were screened for PPD; 61 scored positive, suggesting a PPD prevalence of 17.5%. Of those 61, 37 were positive on the SRQ-20, 50 were positive on the EDPS, and 25 screened positive on both. As seen in Table 1, for the SRQ-20 (n = 37), the range of scores was 8–17, with a mean and median of 10.4 and 10.0, respectively. The questions with the highest number of “yes” responses were: “Are you easily tired?”, “Do you feel nervous, tense, or worried?”, and “Do you cry more than usual?” The questions with the fewest “yes” responses were: “Has the thought of ending your life been on your mind?”, “Do you have trouble thinking clearly?”, and “Is your daily work suffering?” In terms of the EDPS (n = 50), the range was 11–17, with a mean and median of 12.5 and 12.8, respectively. The questions that received the highest number of positive responses were: “I have been anxious or worried for no good reason,” “I have felt scared or panicky for no good reason,” and “Things have been getting on top of me.” The questions with the lowest agreement were: “The thought of harming myself has occurred to me,” “I have looked forward to enjoyment with things,” and “I have been able to laugh and see the funny side of things.”
Depression screening scores (participants who screened positive).
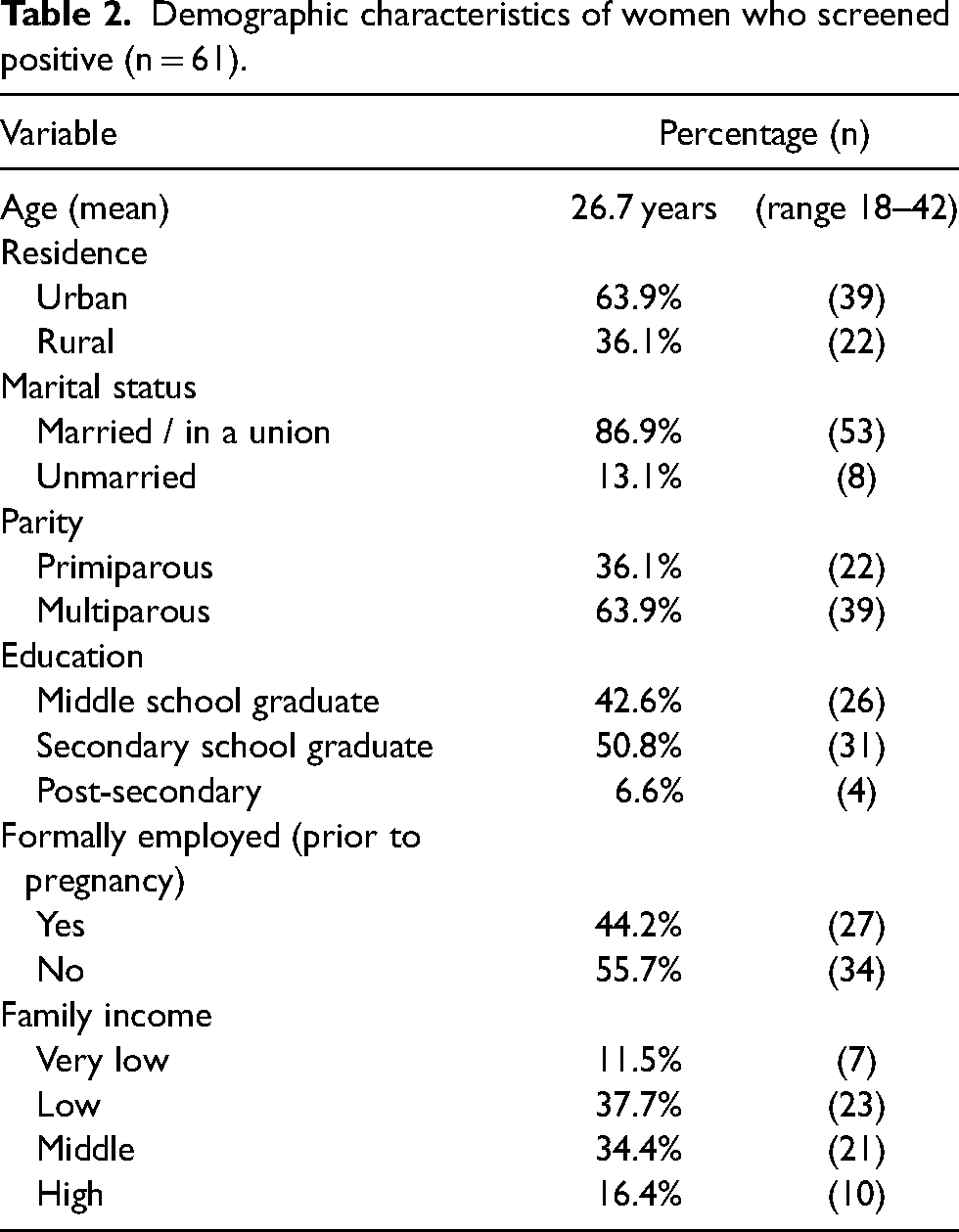
The demographic characteristics of the 61 women that screened positive are seen in Table 2. The mean age was 26.7 years (range 18–42), about 87% were married, 64% lived in the capital, and about one-third were first-time mothers. About 42% had completed middle school or less and more than one-half had not worked formally prior to becoming pregnant. Thirty-five women participated in the interviews.
Demographic characteristics of women who screened positive (n = 61).
Symptoms of PPD
In the interviews, about one-quarter of participants reported never having heard of the term “postpartum depression,” while most had heard of the term but reported having little understanding of its meaning. Only one participant openly self-identified as being depressed (and her case included suicidal ideation). The rest acknowledged experiencing PPD symptoms yet didn’t label themselves as depressed.
When asked to describe how to know if someone has PPD, participants mostly mentioned severe symptoms such as suicidality, and at times even described symptoms reminiscent of psychosis. Several reported that PPD was akin to “going crazy.” Julia, a 31-year-old first-time mother from the capital, explained, “I’ve heard of it, but not much. But I think that being sad for a long time or suddenly getting very happy may change people's minds and they go crazy.”
By far the most common perceived symptom of PPD was anger. For example, Monkh Erdene, a 30-year-old mother of three from a rural area, said, “I’m easily angered, and I think that if everything is not right, I get angry easily. If I get angry, it takes us 1 h or a half hour to get me calmed down because my hands shake and my heart starts racing.” Tsetseg, a 27-year-old first-time mother from the capital, reported a similar experience: During my pregnancy I felt angry about the arguments that were going on, the problems that we were having. Before I was pregnant, I used to take everything very easy—all the problems. But during my pregnancy, I would get angry. I think I took things very seriously.
Along these lines, women with PPD were perceived to be sensitive and emotionally volatile, with difficulty controlling their emotions or behaviors. Tuya, a 21-year-old mother of two from the capital, said “During pregnancy, I think women have no control over their emotions. They get upset easily and cry easily. They get stressed easily.” Prolonged and intense sadness accompanied by uncontrollable crying were other commonly described symptoms, and those that some had experienced personally. Geriel, a 22-year-old mother of three from the capital, explained: “I became a cry baby. I used to cry when my husband told me something or my brother and sister told something. I used to cry a lot when I tried to say something.” Sadness was perceived to be a normal part of the childbirth experience.
Participants from rural areas used the term “sav khuurukh” to describe a general mental health condition with features of PPD, but did not specifically identify it as PPD. Two perceived causes of “sav khuurukh” were being surprised or shocked and a hot/cold imbalance in the body. Chimeg, a 28-year-old mother of two from a rural area, explained, “my mother-in-law said that you should not eat a lot of hot foods and you should not touch hot things. Otherwise, it makes “sav khuurukh” happen to a woman.” However, “sav khuurukh” was never discussed by women from the capital.
Causes and consequences of PPD
Psychosocial factors were often perceived to be the root causes of PPD; in fact, no one mentioned any biological causes, such as hormonal changes, obstetric or pediatric causes, or a history of mental illness. PPD was largely believed to be caused by tension or difficulties with the baby or family members, such as husbands, as opposed to issues relating to the mother herself. Several said PPD resulted from neglect by husbands. For example, when asked what makes pregnant women sad, Erhi, a 20-year-old first-time mother from the capital, answered, “The husband's absence. I was upset because he didn’t spend much time with me. Pregnant mothers are bored at home. She needs so many things from her husband.”
Participants often described their own postpartum experiences in terms of relationships. PPD both caused and exacerbated tensions in interpersonal relationships, largely due to anger, mood lability / emotional reactivity, and sleep deprivation. Nekhii, a 23-year-old mother of three from the capital, discussed this: I had lots of problems during pregnancy. I wasn’t calm at all. I was angry with my husband. When his parents came to our house and suggested something about the household or our babies, I got angry and wanted to die with my baby. I couldn’t make others understand me. I couldn’t make myself clear to my husband and family.
About 60% of participants felt that PPD negatively impacts the relationship between a mother and baby, including inhibiting women's ability to properly care for newborns. PPD was also thought to negatively affect babies’ emotional development. This relationship seemed to be reciprocal; babies’ negative emotions (e.g., crying) could in turn influence mothers’ emotional states. Women who had happy babies were perceived to have less PPD than those who had difficulties with their babies’ feeding or sleeping. Problems with breastfeeding were also reported as both a cause and consequence of PPD. Geriel explained: “Her breast won’t produce enough milk. She will be tired. Also, it’ll affect the baby; the baby will be hungry.” PPD was also commonly attributed to unintended pregnancies. Yet for the almost 60% of participants reporting that their most recent pregnancy was unintended, almost all said that they and their family members were happy upon learning about the pregnancy.
The second major perceived cause of PPD was isolation at home. About 40% of participants lived in rural areas, often quite far from the nearest neighbors, which triggered feelings of loneliness and isolation. However, many urban participants also expressed similar feelings of boredom and loneliness because of being confined to home. Geriel, a 22-year-old mother of three from the capital, discussed this: “I took care of my child for almost nine months at home. I was so bored and wanted to go out and meet my friends. I feel distant from people and that nobody cared [about] me.” Arban, a 24-year-old mother of two from the capital, described how her life had changed since having a baby, “Doing nothing at home is the worst thing that can happen …. I used to work all day. But doing nothing at home makes me sad.”
For many women, staying at home meant being unable to contribute to the household income, which caused stress and anxiety related to finances. Additionally, financial pressures due to the loss of the women's income also negatively impacted household finances. Women's lack of financial independence both contributed to the risk of PPD and amplified its impact. Sarnai, a 32-year-old mother of three from the capital, reported, “Since I’m not working anymore, one person's salary is not enough. I cannot spend money on things that I used to spend on.” Participants in the capital were more likely to report financial difficulties after having a baby than those living in rural areas.
Body image concerns also came up in multiple interviews as a cause of PPD. Baryarmaa, a 28-year old mother of two from a rural area, explained how these changes could affect women, “I’ve read a book that said that when mothers start to compare themselves to their previous selves and they are not happy about their bodies, they get some kind of disease but I don’t know what that is.”
Help for women with PPD
When asked who could provide general emotional support to pregnant or postpartum women, about one-half of participants said their mother or husband while only about 10% mentioned friends. Husbands were seen as the primary source of help and support with the baby. Naranteseg explained: If the baby is calm and well-rested and sleeping well, the mother is happy. If not, the mother will be worried or she cannot get enough rest. When the baby really cries, it feels very difficult. The husband should take care of the wife as much as possible.
Many felt that it was critical for husbands to also give more attention to their wives during pregnancy and the postpartum period. Od explained, “Husbands should take good care of the mother because if they don’t take care of her, she will feel hurt and sad.”
Several participants felt that women suffering from PPD should inform their husbands but acknowledged that Mongolian women generally do not discuss such matters with others, even partners. Mary explained why she told her husband about how she was feeling, “If I don’t tell my husband, then he will not understand me. So I need to tell him directly about the things that are happening to me, the emotions that I’m going through.” Mongolian women's reluctance to discuss mental health problems with others, especially strangers, also extended to family members. Geriel related, “I used to get angry and get upset easily. I used to keep my problems to myself by being quiet. I was not open when I interacted with people. I think I had ‘pregnancy syndrome’. I became upset.”
When asked who could potentially help a woman experiencing PPD, almost one-third suggested a formal healthcare provider, such as a physician or psychologist. First-time mothers in particular reported feeling anxious and were more likely to express a willingness to seek help from healthcare providers than multiparous women. It is important to note, however, that this help was not mental health care but information and reassurance. Despite this suggestion, more than three-quarters of women reported that they had nobody to turn to for help or support for PPD. For example, Naranteseg said, “I don’t think that there's such a place to help a woman with postpartum depression. I think that they go to their friends to ask for help or to share their emotions.” Surprisingly, no one mentioned seeking help from traditional healers or monks and only two participants mentioned psychologists as sources of help, highlighting the perceived lack of any healthcare options for PPD. Od explained, “They should go to the psychologist. But financially, it is difficult. I don’t think mothers will go there because they need to spend this money on other things.”
Many believed that healthcare providers should initiate conversations about PPD with patients, who might otherwise never broach the subject. Talk therapy was identified as desired and helpful. Enkhjargal, a 31-year-old mother of three from a rural area, said, “I wish there was a place to help women psychologically in the same way as health centers. Healthcare providers regularly conduct health checks. Similarly, they should ask about our feelings.” Geriel also mentioned that open discussions with providers would be more effective than self-administered depression screenings: Understanding and talking to them will help. Mongolians are very quiet and they like to keep things to themselves so I think mothers won’t begin conversations about their problems. Also, some people are afraid of their families knowing about it so they may fill in the screening forms incorrectly.
Discussion
This study sheds light on the perceptions and experiences of PPD among a sample of Mongolian women who screened positive for PPD. Our results on PPD prevalence aligned with both previous similar studies in Mongolia, as well as the general global prevalence of PPD. Participants generally had heard of PPD but acknowledged a lack of understanding of its range of symptoms. While most participants correctly identified some symptoms that fit the standard diagnostic criteria, especially sadness and sleeplessness, mood lability manifesting as anger was the most common perceived symptom of PPD. It is possible that anger was recognized most because it is often more visible than other PPD symptoms. It may also be that in Mongolian culture, emotional volatility manifesting predominately as anger is a culturally acceptable idiom of distress.
While participants often openly discussed their own experiences suggestive of PPD, most did not overtly identify themselves as having PPD. This could be explained by the fact that, with one exception, participants did not exhibit suicidality, which was perceived to be one of the main signs of PPD. This is concordant with our previous work with Mongolian healthcare providers (Trop et al., 2018). Hesitancy to self-identify as having PPD could be related to embarrassment or shame, or to lack of recognition of the range of PPD symptoms, especially those that are less severe. Furthermore, in this culture, until it reaches an extreme, depression may not be viewed as a disease, but rather a natural condition following childbirth, which has been documented in other studies (Hanlon, 2013). The results suggest that experiences or symptoms of depression are similar to those listed in the DSM-5 and ICD-10 scales, but that women may describe these symptoms differently and may not use the term “depression,” which may be biased toward the notion of a universal form of mental illness instead of a culturally specific, non-English language term for distress (Cork et al., 2019; Kleinman, 1977).
Our results underscore the need to consider the broader context of the socioeconomic and cultural environment to understand how people interpret depressive symptoms, which has been highlighted by others (Davies et al., 2016; Khanlari et al., 2019; Lasater et al., 2018; Leung et al., 2005; Patel et al., 2010; Stewart et al., 2015). Psychosocial or situational factors, as opposed to biological, were predominantly associated with PPD, which has been found in other Asian settings (Ho-Yen et al., 2007; Leung et al., 2005; Oates et al., 2004). A “situational” model that explains psychological distress in the context of social and interpersonal situations, as opposed to physiological, may be a more common explanatory strategy in this culture (Patel, 1995). Most commonly, participants felt that PPD was largely caused by interpersonal relationship tensions, which mood fluctuation and anger often exacerbated. Boredom, loneliness, isolation, and neglect by husbands were also considered primary causes, along with financial difficulties, problems with the baby's health, unintended pregnancy, and changes in the mother’s physique. One recent study in China also found that social support and interpersonal relationships with family members, especially husbands and mothers-in-law, play important roles in postpartum depression (Qi et al., 2022). Unintended pregnancy has also been associated with PPD in other studies in the USA (Abbasi et al., 2013; Mercier et al., 2013), Brazil (Brito et al., 2015), South Africa (Davies et al., 2016), Zimbabwe (Mbawa et al., 2018), and Laos (Inthaphatha et al., 2020). None of the participants identified perceived biological, obstetric, or pediatric causes for PPD. A history of mental illness, which has been associated with PPD in other settings, was also not mentioned (Beck, 2001; Josefsson et al., 2002; O’Hara & Swain, 1996).
The association of PPD, both as a cause and a consequence, with interpersonal relationship problems reflects the importance of maintaining harmonious relationships in Mongolian culture. The family plays a critical role in Mongolian society, particularly in the context of the perinatal period. The theme of isolation and loneliness featured prominently in our study. Historically, Mongolians were largely nomadic, and families lived far away from their neighbors, thereby having to rely solely on each other for support (Baatar et al., 2012; World Bank, 2016 ). In this setting, physical and social isolation can be extreme for mothers who lack a social support system. While coping and emotional support was perceived to come from family, women may not take advantage of this traditional support system because of the cultural taboos against speaking about personal mental health issues with others. This sociocultural context also has implications for treatment; our results demonstrate a preference for a personalized approach that incorporates interpersonal relationships and broadens social support networks. Establishing support groups for new mothers and educating families about how to support women experiencing PPD might be valuable in this setting, along with the use of mobile phones or tablets to increase access to care through tele-mental health. Inclusion of male partners in such programs is recommended, which concurs with other findings (Cohen & Schiller, 2017 ).
When describing their own health, participants largely discussed feelings—loneliness, isolation, sadness, and boredom—rather than physical symptoms. Several of the screening questions queried about physical conditions such as poor appetite, digestion issues, and headaches that Mongolians may not associate with PPD, thereby influencing the validity of the screening tools which may reflect a more western conceptualization of PPD. Despite being validated in two previous studies in Mongolia, low endorsement on some questions might reflect the participants’ lack of understanding about what the questions were about, such as the question “Things have been getting on top of me.” While we found that screening tools, especially the SRQ-20, were useful in identifying PPD as defined by the DSM, the addition of other culturally appropriate screening questions may be warranted. For example, queries about shock or fear might be relevant, as they are perceived to cause “Sav khuurukh,” the local idiom that seems to describe a condition similar to depression. Endorsement of fear- or anxiety-related screening questions was high (65% on the SRQ-20 and 80% on the EDPS), suggesting that this might have relevance in the Mongolian context and be linked with the western concept of PPD. Other literature has described the concept of “yadargaa,” which literally translates into “weariness” or “weakness” and seems to describe prolonged impairment and “ill health” similar to PPD which can present differently in different people depending on their circumstances (Altangerel, 1998; Kohrt et al., 2004). Other studies have explored the development of more culturally relevant screening tools for depression in Sri Lanka (Abeyasinghe et al., 2012 ), Kenya (Green et al., 2018), Democratic Republic of Congo (Bass et al., 2008), South Africa (Davies et al., 2016), and Malawi (Ng’oma et al., 2019 ). It is important to note that support should be available for women whether or not they fit the western diagnostic criteria (Coates et al., 2015). More work is needed to further clarify this in the Mongolian context.
Our results highlight the need for healthcare providers and community members to initiate discussions about PPD because women may be reluctant to broach the subject or may lack understanding about the warning signs and options for help. Such discussions can help to normalize expressions of emotions in a more open way, potentially paving the way for discussions with others, such as family members. In our previous study among providers, we found that most providers focused on directly observable manifestations of PPD (e.g., crying and not taking care of the baby) and not necessarily those that women express (e.g., feeling down, hopelessness, etc.) (Trop et al., 2018). In the previous study, we also found that most providers also believed that an integral part of identifying and treating PPD is openly talking with women. The current findings suggest that Mongolian women may be open to discussion about mental health issues when someone initiates the conversation, despite the perception that they avoid discussing personal issues.
While idioms of distress frequently overlap with biomedical diagnostic criteria, there is a need to sensitize healthcare providers about cultural explanatory models of PPD and salient idioms of distress, especially in societies where understanding of biomedical systems is low (Davies et al., 2016; Kohrt et al., 2016; Lasater et al., 2018; Nichter, 2010). Healthcare providers should be aware that women may describe PPD in ways that are not biomedically focused (such as physical symptoms like loss of appetite or insomnia); neglecting to elicit descriptions of affective experience of PPD may result in failure to identify PPD. Therefore, providers should not rely only on screening tools but should also keep in mind culturally relevant descriptions of what might be PPD.
The results emphasize the need for community awareness campaigns, as well as provider–patient educational programs for patients and their families to increase family member understanding of PPD. Involving family could be an effective tool in identifying early signs of PPD, especially for those living in rural areas or who have limited access to postpartum follow-up care. The results also demonstrated that self-administered depression screening questionnaires may not be effective in this setting because of reluctance to complete such questionnaires accurately in the presence of family members, which may be linked to stigma. This finding again underscores the importance of providing more information to women, family members, and the community to dispel misconceptions and reduce stigma. Given that many participants preferred help for PPD through family instead of formal health providers, raising community awareness of PPD is crucial. Training of providers in both urban and rural areas is critical to reach all postpartum women. Provider-initiated screening is also needed at rural health care centers and clinics, as many women return to their hometowns very soon after giving birth. Screening by the nurse or primary care provider at well-baby visits may be an effective way to identify women with PPD who do not return for postpartum check-ups. Another approach shown to be effective in long-term prevention and treatment of PPD is community postpartum care by public health nurses (Glavin et al., 2010). In rural areas of Mongolia, primary health care, as well as antenatal and postnatal care, is largely provided by mid-level community health workers (CHWs) who have regular contact with all families in their catchment area (WHO, 2012). They represent a key link to the rural population and could help overcome the main challenges inherent in PPD detection and treatment in rural women. However, a referral process must be in place so that women who screen positive for PPD can access care from trained mental health care providers. Mongolia has a shortage of mental health specialists (Byambasuren & Tsetsegdary, 2005). Increasing the number of such professionals, especially in rural areas, may provide more accessible pathways of care and reduce the burden of PPD treatment on maternal health care providers. Several programs have also employed successful peer-delivered cognitive behavioral interventions in low- and middle-income settings (Chowdhary et al., 2014), including the Thinking Healthy Programme, which could be adapted successfully in Mongolia (Atif et al., 2017; Fuhr et al., 2019; Singla et al., 2019).
Limitations
This study has several limitations. First, our sample of women who gave birth at the NCMCH means that the results may not reflect those of women who give birth outside of the capital or rural women who returned to their homes shortly after giving birth. Women with high-risk births may have been over-represented, as they were often referred to the NCMCH. Our sample was restricted to women who screened positive for PPD and may not reflect the perspectives of women who were not depressed. Due to the sensitive nature of the topic, the results may have been affected by recall bias or social desirability bias because women's recollections about pregnancy may have been influenced after giving birth. Furthermore, only 35 out of 61 women who screened positive actually completed the interviews, which may reflect self-selection bias. The depth of participants’ responses to many questions was also limited, which could have been related to their disinclination to openly discuss this topic.
Conclusions
This study's findings confirm a range of possible barriers to recognition and treatment of PPD among Mongolian women, including the lack of awareness about the range of PPD symptoms, reluctance to initiate discussions with providers about mental health, and the lack of standardized and culturally informed PPD screening practices by healthcare providers. Potential differences between a biomedical model of PPD and local idioms of distress could also explain why awareness about PPD was low. To better inform women and families about PPD, educational campaigns should be implemented in prenatal and postnatal clinics and pediatric settings. Healthcare providers can also play an important role in identifying women with PPD through engaging in dialogue with women and their families. Mental health care services should be scaled up, especially in rural areas. Training mental health providers at various levels to provide quality care to women and their families is crucial; they could also be called upon to deliver training and support to other healthcare providers. In this context, effective treatment options may include non-specialists, such as rural community health workers and nurses, or the use of telepsychiatry, telepsychotherapy, or peer support groups. Finally, more research is needed to better understand cultural conceptual models of PPD, and to identify effective and culturally appropriate treatment approaches.
Footnotes
Acknowledgements
We wish to thank the student researchers who helped with this study, including Tautis Skorka, Kaylen Moline, Brandon Trop, Kenna Nguyen, and Briana Richardson. We would also like to express our deepest appreciation to the women for participating in our study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by the Dhablania and Kim Fellowship from USC Keck School of Medicine.