
Abstract
Eating disorders (EDs) have been documented in various cultural settings. A continuous increase in ED’ rates among non-Western cultures (e.g., Arab cultures and East-Asian cultures) has been reported. We aimed to investigate the relations among culture, ED symptoms, and psychological features that are highly relevant in EDs through a cultural comparison of three groups. The groups included female university students in Israel with varying levels of exposure to Westernization: 118 Jewish students, 132 Arab students studying at a mixed university with a Jewish majority, and 111 Arab students studying at Sakhnin College, a college for Arab students only. The groups differed significantly on the Conservation Value dimension from the Short Portrait Values Questionnaire. Four psychological features were examined as predictors of ED symptoms: Interoceptive-deficits, Ineffectiveness, Asceticism, and Maturity-fear. The results revealed a comparable prevalence of self-reported ED symptoms among Arabs and Jews, with a small exception for bulimic symptoms, which were less prevalent among those in the Sakhnin group, who also scored lower on Ineffectiveness and higher on asceticism than the other groups. Testing the relations between the four psychological features and ED symptoms revealed that culture played a moderating role in predicting the strength of ineffectiveness and maturity-fear. Ineffectiveness was not a predictor among the Sakhnin group, whereas maturity-fear was not a predictor in the least conservative Jewish group. Asceticism and interoceptive-deficits predicted ED symptoms across all study groups. Our findings indicate that the problem of EDs may be similar among Arab and Jewish women in Israel. Moreover, despite some similarities in the relevance of some ED-related psychological features, other features are moderated by culture.
Keywords
Research in cross-cultural psychopathology has identified ways in which culture shapes distress and disorders (Kirmayer & Ryder, 2016). Specifically, studies have shown a rise in Eating Disorders (EDs) prevalence in non-Western cultures (Hoek, 2016; Melisse et al., 2020; Pike & Dunne, 2015). Research on EDs reveals a complex dynamic of cultural and psychological factors ranging from idealizing thinness and media influence (Keel & Klump, 2003) to personality correlates underlying the development and maintenance of EDs (Skårderud & Fonagy, 2012; Treasure & Schmidt, 2013). The purpose of the present study was to examine and compare the relationship between ED symptoms and relevant psychological features across different cultural groups within Israeli society, specifically Jewish and Arab women. By doing so, our overarching aim was to promote a culture-sensitive approach to this psychopathology, both in general and specifically in the Israeli context.
EDs and culture
Out of the four main categories of EDs (DSM-5; American Psychiatric Association, 2013), we focused on symptoms pertaining to anorexia nervosa (AN) and bulimia nervosa (BN). Both AN and BN are characterized by a pathological desire to reduce body weight, a compulsive obsession with weight, disordered perception of body shape, and undue influence of body shape on self-evaluation. AN entails difficulties maintaining a minimal normal weight for age and height, whereas BN is characterized by recurrent and uncontrollable episodes of bingeing large quantities of food followed by purging behaviors. Contrary to AN, in BN body weight remains at a normal or above-normal level (American Psychiatric Association, 2013).
A large body of research on EDs found that both sociocultural and psychological factors generate cognitive and emotional susceptibility to body and weight disturbances (Polivy & Herman, 2002). Most of these studies were conducted in Western societies, yet interest is increasing in examining cultural differences in ED symptoms and the psychological features related to the existence and maintenance of EDs.
One of the main sociocultural risk factors for developing EDs in Western countries is the emphasis on weight and physical appearance as indices of success, with thinness, beauty, and dieting symbolizing health and happiness (Swami et al., 2009). This conception is culturally bounded. In some Arab cultures, plumpness in women was valued and thought to symbolize femininity, fertility, and good health (Melisse et al., 2020; Shuriquie, 1999). Accordingly, EDs were less prevalent in Arab cultures (Melisse et al., 2020), yet today their general prevalence is increasing (e.g., Melisse et al., 2020; Zeeni et al., 2017). For example, Lebanese female students were found to avoid particular foods and exhibited a prevalent desire to become thinner (Khawaja & Afifi-Soweid, 2004; Zeeni et al., 2017). Similarly, 24% of the students in a university sample from the United Arab Emirates (UAE) scored above the cut-off on the Eating Attitude Test (EAT-26), indicating disordered eating attitudes and high risk to develop EDs (Thomas et al., 2010).
The previous sociocultural perspectives on EDs concluded that EDs may be culture-specific as they occur more frequently in Western-European cultures, and influenced by body ideals present in these cultures. Accordingly, the increase in disordered eating in non-Western societies has been attributed to excessive exposure to Western media and lifestyle, which idealize thinness (e.g., Mousa et al., 2010; Thomas et al., 2010). Others have posited that it is not Westernization per se but rather processes of industrialization and urbanization unfolding now due to globalization throughout some non-Western cultures that play a role in the development of EDs among young women in these societies (Van Son et al., 2006). Beyond some positive dimensions, cultural change and urbanization, which bring about new lifestyles and gender roles, constitute risk factors for EDs among some women. Women living in cultures in transition may develop EDs as a reaction to new expectations and ambitions that may clash with more traditional gender roles (Katzman & Lee, 1997; Pike & Dunne, 2015). These sociocultural factors may translate into psychological factors relevant to EDs.
EDs, psychological features, and culture
A vast body of literature suggests that several psychological features are catalysts for developing and maintaining EDs and thus are important in their prevention and treatment (Polivy & Herman, 2002). Our study focused on features that may differ between cultures: interoceptive-deficits and ineffectiveness, which have been shown to be key predictors of EDs in Western cultures (Olatunji et al., 2018), as well as asceticism and maturity-fear, assumed to be important ED predictors in non-Western cultures. These features are taken from the EDI-2, a widely used self-report questionnaire which measures psychological features commonly related to EDs.
Interoceptive-deficits, a key psychological feature among ED patients, manifest in an inability to identify and understand one's internal bodily cues and emotions (Fassino et al., 2004; Olatunji et al., 2018). Difficulties in differentiating between physical and emotional states and in understanding one's own emotional experiences may lead to ED-related behaviors, used as a concrete means of representing and enacting one's feelings and thoughts (Bleiberg, 2001). Indeed, progress on interoceptive-deficits during treatment corresponds with a decrease in symptoms (Matsumoto et al., 2006). The second feature, ineffectiveness, involves feelings of inadequacy, insecurity, low self-esteem, and worthlessness (Garner, 1991). This feature has long been linked with EDs (Bruch, 1962), as individuals with EDs were found to exhibit higher ineffectiveness and negative self-perception than healthy controls (Fassino et al., 2004).
Are these features similarly linked with EDs in non-Western societies? Evidence suggests that interoceptive-deficits may be relatively low in non-Western cultures (Ma-Kellams, 2014; Tsai et al., 2004), given the greater attendance to contextual rather than internal cues when evaluating the self and others (Kanagawa et al., 2001; Ma-Kellams et al., 2012). Cultural differences in ineffectiveness may be linked to collectivistic versus individualistic socialization practices, correspondingly leading to the development of interdependent versus independent self-construal (Markus & Kitayama, 1991). Individuals with interdependent selves may emphasize complying with group norms and tend to fit in more than those characterized by self-effectiveness, whereas the opposite is true for people with independent selves. According to this view, self-effectiveness is more important in Western than in non-Western cultures.
Other features may be especially important in predicting EDs in non-Western cultures. In this study, we investigated two features from this group: asceticism and maturity-fear. Studies investigating AN in non-Western countries (Hong Kong, India, and Ghana) revealed that AN was motivated by religious beliefs and ascetic values (Bennett et al., 2004; Lee et al., 2001) and that it pertained to heightened religiosity and pursuit of spiritual ideals such as self-discipline, self-denial, and control over bodily needs. Heightened religiosity and ascetic beliefs, which are more prevalent in traditional, non-Western cultures (Saroglou, 2011; Tessler, 2010), were associated with symptoms of EDs among Muslim-Arab women from the UAE (Thomas et al., 2018).
Maturity-fear is the fear of sexual maturity and adulthood. This fear has been acknowledged as a psychological feature in the phenomenology of EDs (Holland et al., 2013; Nakai, 1997; Svenaeus, 2013), as thinness may reflect fear of maturation and a desire to remain in prepubescent stages (Moore et al., 2016; Svenaeus, 2013). Such fears maybe more prevalent among women in patriarchal traditional societies who must confront many gendered social expectations and regulations, such as early marriage, sexual modesty, and accepting the authority of men over women (James-Hawkins et al., 2017; Sharabi, 1988). Maturity-fear was indeed found to be higher among Saudi-Arabian compared to Canadian girls (Al-Subaie et al., 1996), among Asian female students compared to American White and Black female students (Rosen et al., 1988), and among Japanese women with different ED subtypes compared to Western ED patients (Pike & Mizushima, 2005).
It appears, then, that ED-related psychological features may differ in prevalence or levels between cultures. Yet, so far, the possible differential relevance of these features to ED symptoms has not been studied. The present study seeks to fill this gap by investigating the above four psychological features as predictors of EDs in the culturally diverse context of Israel.
The Israeli context
Israel is a multicultural country. According to Israel's Central Bureau of Statistics (ICBS, 2021), 74.2% of Israeli citizens are Jewish and 20.9% are native Arabs of Palestinian descent. Palestinian Arabs and Jews in Israel are relatively segregated in terms of residence (there are only few mixed cities) and the educational system. The hegemonic mainstream group of Israeli Jews tends to be secular, individualistic, and Western-oriented (Lavee & Katz, 2003), whereas Palestinian Arabs are gradually experiencing a transition from a conservative society to a modern liberal one. While the majority of Arab society in Israel maintains a traditional lifestyle (Barak & Golan, 2000; Dwairy, 2004; Smooha, 2010), some Arab subgroups are more exposed to Western ideals through media consumption or integration into the Israeli-Jewish society (e.g., in higher education or work settings) and may adopt more Western views.
Palestinian Arab women in Israel face various challenges, both as an ethnic minority in Israel and as women living in a patriarchal traditional society (Elnekave & Gross, 2004). There is a considerable disparity between Palestinian Arab women and Jewish women in Israel, with Jewish women generally more empowered and enjoying more independence and freedom (Abu-Kaf, 2019; Abu-Rabia-Queder & Arar, 2011). Arab women face a duality between conservative and modern values, which may vary in strength among different subgroups (Zaatut & Haj-Yahia, 2016).
Research on EDs in Israel has generally concentrated on the Jewish mainstream group, revealing EDs’ rates that are typical to some Western countries worldwide (e.g., Western Europe and the United States; Latzer & Tzischinsky, 2005). In contrast, research on EDs in Arab cultures in Israel is scarce. Data collected during the previous decade showed that ED referral rates to public clinics among Arabs were still extremely low compared to Jews: out of 1700 referrals to the largest ED ambulatory service in northern Israel, only two AN and eight BN patients were Arabs (Latzer et al., 2008). The posited explanation was that Arabs in Israel hold more traditional attitudes regarding ideal body image that protected them from EDs (Apter et al., 1994; Shuriquie, 1999). Nevertheless, the number of teenaged Arabs in nonclinical settings reporting abnormal eating attitudes is on the rise (Latzer et al., 2007, 2014). These studies ascribed the level of pathological eating behaviors among Arab teenagers to their degree of exposure to Western ideals and media influence (Apter et al., 1994; Latzer et al., 2007). These studies did not look into the relevance of psychological features to EDs in Arab culture in Israel—one of our goals in this study.
The present study
The study goals were: (1) to examine whether cultural differences exist in a) the prevalence of ED symptoms and b) the links between ED symptomatology and psychological features; and 2) to offer further evidence of the role of exposure to Western ideals in predicting the prevalence and psychological profile of EDs in non-Western cultures. As a specific case study, we distinguished between two Arab groups in Israel that differ in their exposure to the Westernized majority group. One is a group of students from Sakhnin College, an all-Arab institution where the studies are in Arabic (hereafter, Sakhnin-Arabs). The other is a group of Arab students studying at the University of Haifa, an institution with a Jewish majority where the studies are in Hebrew (hereafter, Haifa-Arabs). Thus, Haifa-Arabs are more intensely exposed to a Western-oriented culture through their education at a Hebrew university compared to Sakhnin-Arabs. We assumed that their differential exposure would be reflected in differences in their values. We used Schwartz's framework of cultural values to test possible differences between the studied groups. Values are desirable trans-situational goals that vary in their importance as guiding principles in people's lives. Schwartz's value theory (Schwartz, 1992) originally identified 10 central values organized in a circular structure that reflects the conflicts and compatibility among them. The circle represents two bipolar dimensions: openness-to-change versus conservation, and self-transcendence versus self-enhancement. Support for this structure emerges in research among more than 200 samples from over 70 countries (e.g., Fischer & Schwartz, 2011). In the present study we will use only conservation values, as it best captures the differences between the relevant groups. We expect that the Sakhnin-Arab group would be the most conservative and the Jewish group would be the least conservative. We assumed that their differential exposure would be reflected in differences in their values, so that the Sakhnin-Arab group would be the most conservative and the Jewish group would be the least conservative. We examined potential differences among the three student groups (Sakhnin-Arabs, Haifa-Arabs, and Jews) with respect to a) ED symptom prevalence, b) level of four psychological features related to EDs, and c) relations between ED symptoms and psychological features. The vast cultural differences within Israel provide a unique opportunity to examine the role of culture in EDs.
Specifically, we hypothesized that:
H1. The three groups would differ in psychological features related to EDs such that (a) interoceptive-deficits and (b) ineffectiveness would be lower among Jews than among Sakhnin-Arabs and (c) asceticism and (d) maturity-fear would be higher among Sakhnin-Arabs than among Jews. We expected the Haifa-Arab group to fall between the two on all four features.
H2. Psychological features related to EDs: (a) interoceptive-deficits, (b) ineffectiveness, (c) asceticism, and (d) maturity-fear would predict ED symptoms across cultures.
H3. A moderating role of culture would be found, such that (a) interoceptive-deficits and (b) ineffectiveness may exhibit a stronger relationship to ED symptoms among Jews than among Sakhnin-Arabs, while (c) asceticism and (d) maturity-fear may exhibit a stronger relationship to ED symptoms among Sakhnin-Arabs than among Jews. We aimed to study these relations as open questions among Haifa-Arabs.
We also planned to test between groups differences in prevalence of ED symptoms as an open question, as the available data is not decisive.
Method
Participants and procedure
The sample included 361 female college students recruited from three different sources. The first group consisted of 111 Sakhnin-Arab students, the second consisted of 132 Haifa-Arab students and the third group consisted of 118 Jewish students, also from the University of Haifa. Students participated in the study voluntarily or in exchange for course credit. Questionnaires were distributed online to University of Haifa students (Jewish and Arab) on an online university platform, as well as in Facebook groups that host students from Haifa university. Moreover, questionnaires were printed out and distributed in classrooms to Sakhnin-Arabs at the Arab college in Sakhnin. Participants filled in the questionnaire in their native language, after giving their informed consent. This research was approved by the ethics committee at the University of Haifa (IRB approval: 059/17) as well as at Sakhnin College.
Measures
Personal details. Participants reported on their age, ethnicity, religion, and socioeconomic status (self-report on a 4-point scale) and answered questions regarding their height and weight. Their Body Mass Index (BMI) was calculated based on these reports.
For the internal consistencies of all the scales described below, see Table 1.
Cronbach’s alpha, means, SDs for EDs symptoms and psychological features related to EDs in three cultural groups.

Note. Means marked with the same letter are not statistically different.
*p < .05. **p < .01. †= p < .10.
Conservation value dimension. Items of tradition, security, and conformity taken from the Short Portrait Values Questionnaire
The Eating Attitudes Test (EAT-26; Garner et al., 1982) is a 26-item, 6-point scale depicting symptoms and concerns characteristic of EDs. It is widely used for screening and measuring eating problems in large non-clinical populations. The Hebrew version revealed good construct validity that was significantly related to body image (r = .43) and dieting frequency (r = .55). The Arabic version was significantly related to body image and BMI (Al-Subaie et al., 1996; Mousa et al., 2010; Nasser, 1986).
Other scales assessing ED symptoms or psychological characteristics typical to ED were taken from the EDI-2 (Garner, 1991) and all have a Likert-type 6-point answering scale. We did not use the EDI-3 because, to the best of our knowledge, it has not been administered to Arabs in Israel and thus its reliability and validity have not been determined. The EDI-2 was previously translated and administered in Hebrew and Arabic, yielding good internal consistency ranging between 0.67 and 0.93 (Latzer et al., 2007).
Drive for Thinness (DFT) includes seven items measuring attitudes and behaviors that indicate excessive preoccupation with dieting, weight, and extreme pursuit of thinness. Items reflect both a strong wish to lose weight and a fear of weight gain (e.g., “I am terrified of gaining weight”).
Bulimia subscale includes seven items assessing the tendency toward episodes of uncontrollable overeating (bingeing) that may be followed by the impulse to engage in self-induced vomiting (e.g., “I have thought about trying to vomit in order to lose weight”).
Interoceptive-deficits, as measured via the Interoceptive-Awareness scale, which includes 10 items assessing one's lack of confidence in recognizing and identifying emotions and sensations of hunger or satiety in oneself (e.g., “I get confused about what emotion I am feeling”).
Ineffectiveness. This 10-item scale assesses general feelings of inadequacy, insecurity, and worthlessness (e.g., “I feel ineffective as a person”).
Asceticism. This scale contains eight items assessing the tendency to pursue spiritual ideals such as self-discipline, self-denial, self-limitations, hyper-control over bodily needs, and self-sacrifice (e.g., “Denial of my physical needs helps me feel spiritually strong”). Two items were omitted to improve internal consistencies (“I try hard to have fun”; “Suffering toughens a person”). Removing these two items improved internal consistency in all three culture groups from α = .68, α = .62, α = .43 to α = 71, α = .70, α = .60 for the Jewish, Haifa-Arab, and Sakhnin group respectively.
Maturity-fear. This scale contains eight items assessing one's desire to retreat to the security of prepubescent years due to the overwhelming demands of adulthood (e.g., “I wish I could return to the security of childhood”).
Results
First, we conducted a comparison between groups on demographic variables. The majority of the Arabs were Muslim (67% in Haifa and 75% in Sakhnin—the rest were Christians, Druze, or “other”). The groups differed in age, F(2,377) = 54.53, p < .0001: the Jewish group was older (M = 23.16, SD = 1.62) than the Arab groups (M = 21.78, 20.67, SD = 2.41; 1.84, among Sakhnin and Haifa students, respectively). Socioeconomic status significantly differed between all the cultures, F(2,377) = 19.90, p < .001: Jews (M = 2.40, SD = .53) > Haifa-Arabs (M = 2.19, SD = .50) > Sakhnin-Arabs (M = 2.03, SD = .38). Both age and socioeconomic status were covariates in the main analyses. BMI significantly differed between groups, F(2,377) = 5.99, p < .05, and was highest among the Sakhnin-Arabs (M = 23.12, SD = 3.76) and lowest among the Haifa-Arabs (M = 21.48, SD = 3.76). Jews were ranked in the middle (M = 22.65. SD = 4.25). The average BMI for all groups was in the same normal weight range.
To verify our assumptions about the differences between the three cultures, we compared them regarding their conservative values. An analysis of variance yielded a significant effect, with Sakhnin-Arabs the most conservative, followed by Haifa-Arabs, and Jews being the least conservative (see Table 1), confirming our assumptions. Next we compared the groups for symptoms of EDs. A one-way MANCOVA was conducted to compare the groups on EAT-26, DFT, and bulimia. Age and socioeconomic status were used as covariates. A multivariate effect of cultural group was found, Hotelling's T = .04, F(6,706) = 2.72, p < .05; η²=.02. None of the univariate tests reached significance, but differences in bulimia were marginally significant (see Table 1), with Sakhnin-Arabs exhibiting somewhat lower bulimic tendencies. The findings imply that the three groups are quite similar in their level of reported ED symptoms.
The first hypothesis predicted cultural differences in the level of psychological features related to EDs. A MANCOVA was conducted, with culture as the predictor and maturity-fear, asceticism, ineffectiveness, and interoceptive-deficits as the dependent variables. Age and socioeconomic status were covariates. As hypothesized, a significant multivariate effect was found, Hotelling's T = .21, F(8,708) = 9.39, p < .001; η²=.09. The univariate tests showed a significant culture effect for asceticism and ineffectiveness, though the effect size was small (see Table 1). Bonferroni post-hoc analyses showed that asceticism was highest among Sakhnin-Arabs and ineffectiveness was lowest in this group, while Haifa-Arabs and Jews did not differ on either scale. Contrary to the hypothesis, no significant cultural differences were found for maturity-fear and interoceptive-deficits.
The second hypothesis pertained to the prediction of three different ED symptoms (EAT-26, DFT, Bulimia) by ED-related psychological features. Three multiple regression analyses were computed. In all of them the predictors were culture (dummy coded as D1 for Haifa-Arabs – Jews contrast, and D2 for Sakhnin-Arabs – Jews contrast), the four psychological features (interoceptive-deficits, ineffectiveness, asceticism, and maturity-fear), and the interaction terms between D1/D2 and each of the psychological features. The four psychological features were standardized. Age and socioeconomic status were included as covariates.
All models were significant (see Table 2). As in previous analyses, age was not a significant predictor, but socioeconomic status significantly predicted EAT-26 and DFT. The groups did not differ in EAT-26 or DFT, but Sakhnin-Arabs were significantly lower than Jews on bulimia, a difference that was only marginally significant in the ANCOVA (probably due to more predictors in the regression model).
Standardized regression coefficients predicting EDs symptoms (N = 363).
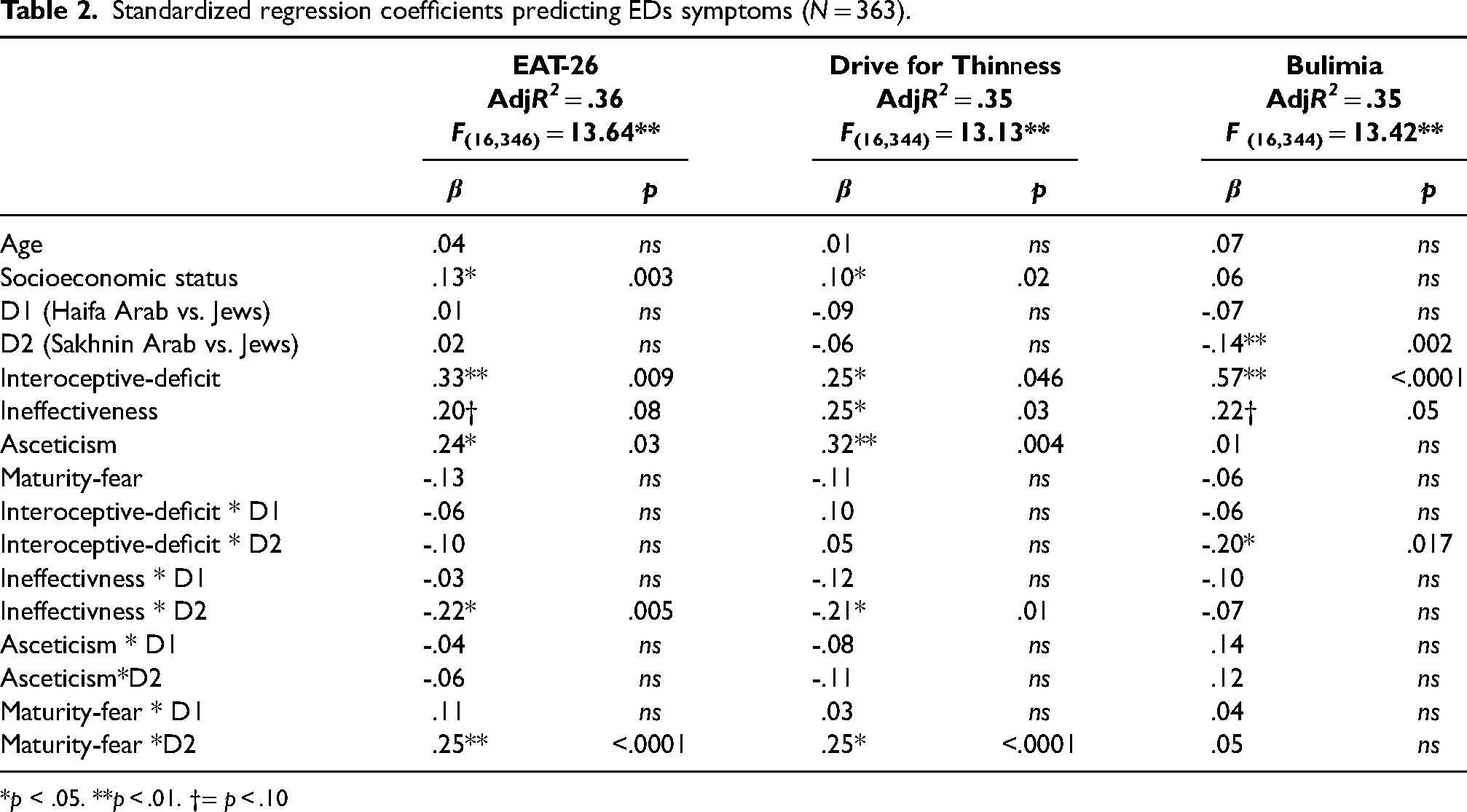
*p < .05. **p < .01. †= p < .10
Interoceptive-deficit was the most consistent predictor. It was significant in all three models and was the strongest predictor of EAT-26 and bulimia, supporting H2(a). It did not interact with culture for EAT-26 and Drive for Thinness, but a significant interaction emerged between Sakhnin Arab – Jewish comparison and interoceptive-deficit. Simple slope analysis showed that interoceptive-deficit was a stronger predictor of bulimia among Jews than among Sakhnin-Arabs (see Figure 1). H3(a) was for the most part not supported. It was supported only for bulimia, but only regarding the strength of prediction and not for the existence of meaningful relations across all tested groups.
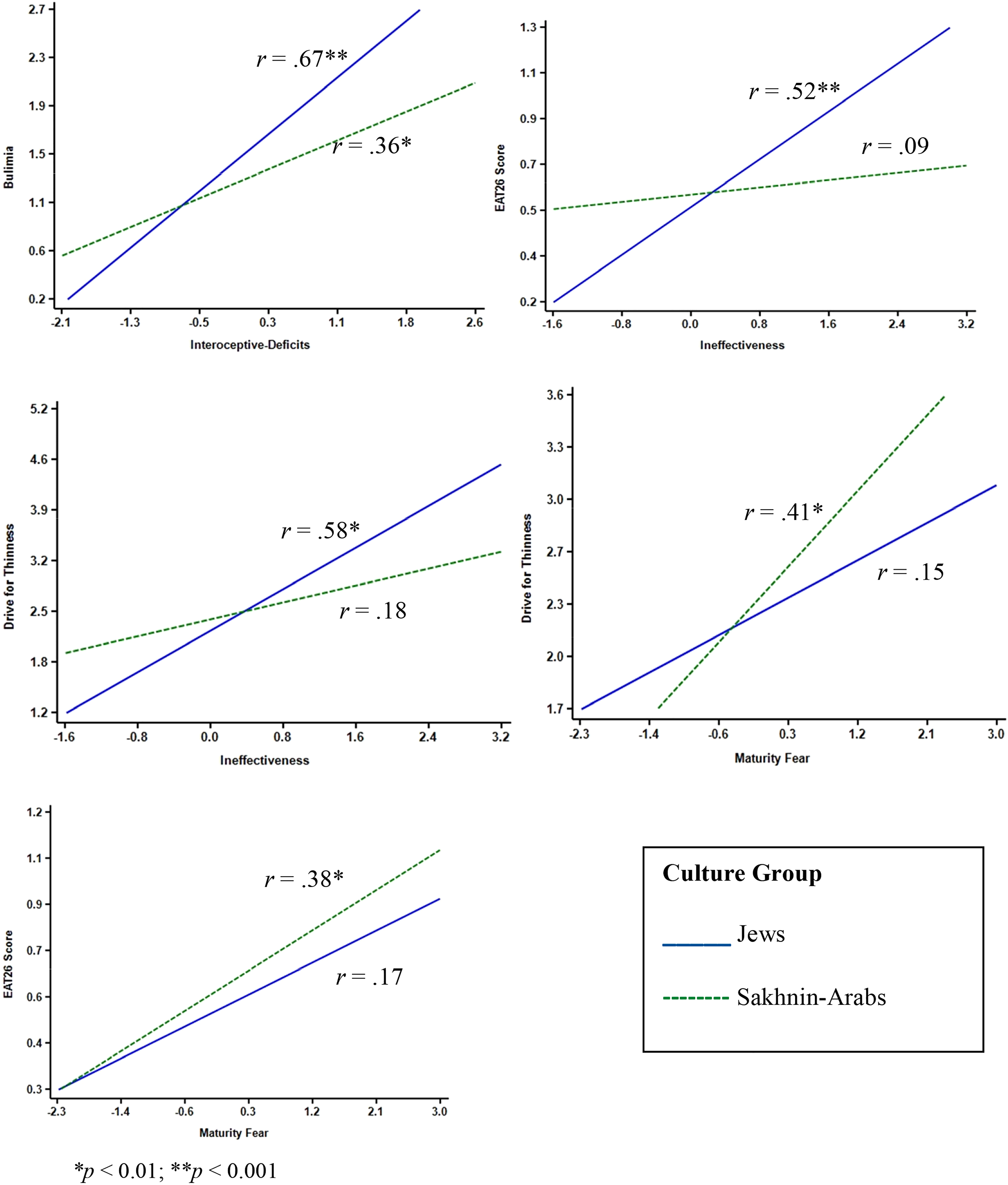
Psychological features predicting EDs symptoms by group.
Ineffectiveness emerged as a significant predictor of Drive for Thinness and a marginally significant predictor of EAT-26 and bulimia, mostly supporting H2(b). A significant interaction between ineffectiveness and Sakhnin-Arab – Jews contrast was found for EAT-26 and Drive for Thinness. In both cases, ineffectiveness was a stronger predictor among Jews than among Sakhnin-Arabs (see Figure 1). H3(b) was for the most part supported.
Asceticism was a significant predictor of EAT-26 and Drive for Thinness, supporting H2(c), while the relations with bulimia did not support this hypothesis. Contrary to H3(c), asceticism did not interact with culture in predicting ED symptoms.
Contrary to H2(d), maturity-fear was not a significant predictor across cultures in any of the regression models. Significant interactions with cultural group disqualified such a conclusion, as maturity-fear significantly interacted with the Sakhnin-Arab – Jews contrast for both EAT-26 and DFT. Simple slope analyses (see Figure 1) showed stronger relations for Sakhnin-Arabs than for Jews. In fact, these relations were significant for Sakhnin-Arabs but not for Jews. One interesting finding was that despite the insignificant interaction between maturity-fear and Haifa-Arab – Jews contrast, simple correlations between maturity-fear and both EAT-26 (r = .31, p < .01) and Drive for Thinness (r = .21, p < .05) were significant among Haifa-Arabs. Maturity-fear did not predict bulimia in any culture. Thus, H3(d) was generally corroborated.
Discussion & conclusion
The results of this study have implications for the main questions raised, which pertain to cultural differences in the prevalence of ED symptoms, in related psychological features, and in their relations to ED symptoms. The investigation of two Arab groups in Israel may shed further light on cultural transition processes.
Group differences in ED symptoms
Our study showed that the three studied groups were almost identical in self-reported rates of ED symptoms, with a slight difference in bulimic symptoms, which were somewhat less prevalent in the conservative Sakhnin group. The Haifa-Arabs, who did not differ in ED symptoms from the Jewish group, exhibited significantly lower BMI scores. One possible explanation is the rapid cultural change the Arab society is going through (Arar & Haj-Yehia, 2016), which is especially salient for Haifa-Arabs. This rapid change suggests two independent processes. One is extensive exposure to Western body ideals (Mansour et al., 2023), and the other is the experience of adversity rooted in exposure to conflicting norms, which puts them at risk for developing EDs (Katzman & Lee, 1997; Pike & Dunne, 2015). Higher socioeconomic status was related to elevated ED symptoms in our sample. Overall the similar rates of EDs symptomatology in our groups is consistent with findings from the literature that indicate an increase in EDs’ rates in Arab cultures (Saleh et al., 2018). The fact that differences in level of Westernization did not correspond with different rates in self-reported ED symptoms in our samples generally supports the increasing perspective on EDs as becoming less “culture-bound,” only occurring in the West or tied to Western exposure only, and more “culture-reactive,” occurring in cultures in transition (Alfalahi et al., 2022; Keel & Klump, 2003; Pike & Dunne, 2015).
Profiles of psychological features related to EDs and culture
We expected that the four psychological features would reveal different prediction profiles in the different cultural groups. This expectation was not supported for two of the features that were similar across the tested cultures: interoceptive-deficits and asceticism. The other two features, ineffectiveness and maturity-fear, revealed the expected differences in profiles across cultures.
The level of interoceptive-deficits did not differ between cultures and was significantly related to ED symptoms in all groups. Though some moderating role of culture was found, it did not diminish the meaningful relations across groups. These findings support the centrality of interoceptive-deficits in ED symptoms, consistent with the idea that being aware of emotions and body sensations may be a protective factor against EDs in diverse cultures.
As expected, asceticism was indeed higher among Arab students from Sakhnin College than among both Haifa-Arabs and Jews, probably because those in this group are more traditional and generally more influenced by religion. Nevertheless, culture did not moderate the relations between asceticism and ED symptoms, pointing to the centrality of ascetic-like behaviors in the psychological profile of EDs regardless of cultural setting. This finding corresponds with the inherent struggle for control and the self-denial of bodily needs in order to attain perfection that characterizes EDs (Fassino et al., 2004).
A moderating role of culture was found for ineffectiveness and maturity-fear in that both predicted EDs differently among Sakhnin-Arabs than in the other two groups. Counterintuitively, the Sakhnin group revealed lower ineffectiveness—a finding that may stem from the higher expectations, standards, and pressure to succeed among Jewish and Haifa-Arab students. Haifa-Arabs in particular are faced with several challenges, such as studying in a non-native language or being marginalized at times as an ethnic minority, that may increase the threat to their self-effectiveness perceptions. The finding that ineffectiveness was lower among Sakhnin-Arabs and was not related to ED symptoms may support the notion that self-reported effectiveness is probably not that threatened in this group.
The strongest moderating role of culture was found for maturity-fear. Despite the lack of mean differences between cultures, its relevance to EAT-26 and DFT differed between cultures. Particularly among Arab women, maturity may have certain costs, such as marriage at a young age and abiding by patriarchal gender roles (Azaiza et al., 2009; Ben-Ari & Azaiza, 2003). The desire to delay maturation may also serve as a way to avoid facing the conflict between traditional social expectations and exposure to changing ideals that women face in the context of rapid social change. Namely, young women in cultures undergoing transition bear the burden of meeting conflicting societal expectations, which could lead to psychological distress and loss of personal control (Abu-Baker, 2016; Haj-Yahia et al., 2019). Thus, delaying maturation through using the body may be seen as a reaction to these sociocultural conditions in the attempt to regain control over themselves. This view echoes psychoanalytic perspectives that view EDs among young women as a means to regain a sense of personal control and autonomy using their body (de Groot & Rodin, 1994; Skårderud, 2007).
Taken together, the above findings revealed a moderating role for culture in the link between maturity-fear and ineffectiveness to EDs as expected, whereas interoceptive-deficits and asceticism are linked to ED symptoms across the different cultures.
Arab groups in Israel
Whereas Sakhnin-Arabs were found to differ from the Jewish group on some of the hypothesized differences, the Haifa-Arabs were quite similar to the Jewish group. This finding raises two questions. The first is the question of why the two Arab groups differed from each other. The second and more intriguing question is why the Haifa-Arab group did not differ from the Jewish group with respect to EDs, psychological features and most of the relations between them, despite their significant differences in conservatism. The difference between the two Arab groups is not surprising considering that the Haifa-Arabs chose a Hebrew university to begin with, indicating they may be more fluent in Hebrew compared to their counterparts studying in Arabic at Sakhnin College. Their day-to-day interactions with their Jewish peers increase this exposure and may lead to some endorsement of Western values. Nevertheless, they are not as Westernized as the Jewish group, as indicated by their high conservative values, and yet they exhibited the same level of EDs, the same level of psychological features, and almost the same ED prediction profile. Perhaps as this group experiences cultural transition most strongly, it could be that for some aspects they demonstrate extreme behavior in order to resist traditional values, thus revealing responses similar to those of the Jewish group. In some cases their behavior may be even more extreme (as reflected in their BMI)—a kind of reactance reaction (Benet-Martínez et al., 2002; Sherif & Hovland, 1961). An exception, though not consistent, was found for the relations between maturity-fear and EDs. These relations among the Haifa-Arabs were ranked between those of the conservative Sakhnin-Arab group and the liberal Jewish group. This finding points to a possible perceived threat from societal expectations regarding mature women even in the liberal part of the Arab group in Israel, thus exposing this group to risk factors typical of conservative (maturity-fear) and non-conservative groups (ineffectiveness). Future studies should further investigate cultures in transition in terms of both reactance and risk factors.
Limitations and suggestions for future work
The present work does have some limitations. First, we relied on self-report measures that may be biased by social desirability. Second, the relationships between the variables are not causal. Hence, future longitudinal studies are needed to assess the psychological features contributing to EDs among Arabs in Israel. Third, our samples consisted of university students, which may not represent the population at large. Fourth, the internal consistencies of some of the scales were not satisfactory. Finally, our sample was not a clinical sample, partially due to the difficulty in recruiting clinical samples within the Arab culture where seeking mental health assistance is generally stigmatized (Latzer et al., 2008). We must note that the lack of evidence regarding current rates of diagnosed ED cases in the Arab community and the similar levels of self-reported ED symptoms among Arabs and Jews in a community sample may not necessarily indicate a similar pattern in the clinical public sector.
Despite these limitations, we can cautiously conclude that the prevalence of EDs in community samples is quite similar among Jews and Arabs in Israel. Moreover, some psychological features—asceticism and interoceptive-deficits—are robustly related to EDs in both cultures, whereas the relationships between EDs and other features—ineffectiveness and maturity-fear—are moderated by culture.
Footnotes
Acknowledgments
We would like to acknowledge the important cooperation of Sakhnin College during the recruitment process for this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.