
Abstract
As forced displacement and migration reach unprecedented levels globally, the ways in which parents communicate stories of trauma, displacement, and post-migration adversities to their children offer unique insight into how these experiences affect forcibly displaced families. The present study aimed to explore how mothers communicate with their children about their experiences of trauma, displacement, and mental health whilst seeking International Protection in Ireland. Semi-structured qualitative interviews were conducted with 19 mothers who had children aged between four and 17 years. All mothers were applicants for, or recipients of, International Protection in Ireland. Data were analyzed using thematic analysis. Two superordinate themes were developed from the analysis. ‘Guarding communication’ occurred when mothers used strategies including avoiding certain topics of conversation, silencing their children, and withholding information from their children. ‘Grappling with communication’ occurred when mothers sought to be child centred yet doubted themselves and were inconsistent in how they communicated with their children. Mothers do not adopt one strategy for communicating with their children. Rather, communication was fluid and dynamic as mothers oscillated between silence and narration. The findings show how difficult it can be for mothers to tell their narratives to their children, and have implications for the provision of therapeutic support for parents and families. What matters most may be to support mothers’ agency in choosing the manner, timing, and content of their communication with their children.
Introduction
Forcibly displaced individuals are at an elevated risk of trauma exposure across pre-, peri-, and post-migration landscapes—also known as the triple-trauma paradigm (Miller & Rasco, 2004). Pre-migration settings include exposure to war and persecution; the peri-migration period may involve exposure to sexual violence, poverty, and prolonged stays in refugee camps experienced along the migration route; and post-migration contexts can include exposure to punitive asylum protocols, racism and discrimination, loss of culture, and enduring acculturation stressors after arrival in the host country (Císse et al., 2020; Porter & Haslam, 2005). The types, severity, duration, and accumulation of traumatic experiences across these migration landscapes are associated with post-traumatic stress disorder (PTSD) and other adverse mental health outcomes (Blackmore et al., 2020; Bogic et al., 2015). The risk of elevated negative mental health outcomes also extends to child and adolescent refugees (Kevers et al., 2022). This risk is attributed to direct experiences of war, the strain associated with migration and post-migration transitions and acculturation challenges (Fazel et al., 2012; Hodes & Vostanis, 2019), as well as indirect influences through parental PTSD, harsh parenting, and parenting stress (Bryant et al., 2018; Eruyar et al., 2018). Considerable research has been devoted to understanding the transmission of trauma across generations, often using samples of survivors of the Holocaust and their children (Kellerman, 2001; Solkoff, 1992). One key finding emerging from this research is that survivors and their children are often resilient to the effects of trauma, and in light of this, the trauma transmission paradigm has been criticized for needlessly pathologizing survivors (Sagi-Schwartz et al., 2003). Such critique has also led to attempts to explicate processes that exacerbate or protect against trauma transmission, often focusing on quality of attachment and parenting (Bosquet et al., 2014; Field et al., 2013).
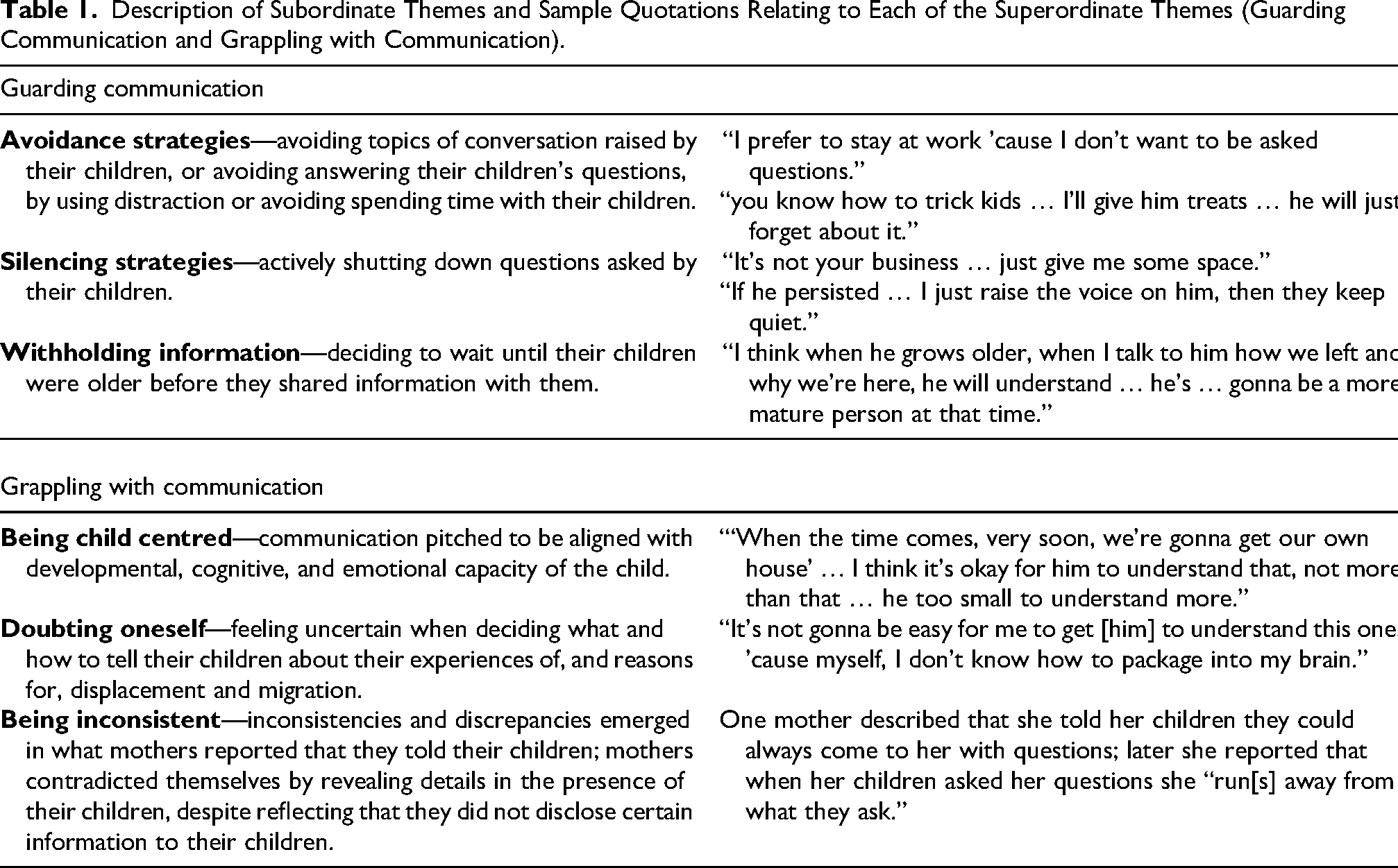
Description of Subordinate Themes and Sample Quotations Relating to Each of the Superordinate Themes (Guarding Communication and Grappling with Communication).
An additional focus of research has been on the construction of trauma narratives and communication about traumatic experiences within the family unit (De Haene et al., 2020; McFarlane & Kaplan, 2012). This is important for several reasons. First, it has been suggested that the manner of disclosure of war trauma to children within their families may be related to their well-being (Measham & Rousseau, 2010), with some studies finding greater disclosure associated with higher child symptomatology (Angel et al., 2001) and others finding the opposite (Montgomery et al., 1992). Second, the trauma narrative is a central reparative element in treatment models for refugee populations (De Haene et al., 2012). According to De Haene et al. (2020), refugee families construct “unique strategies of narration or silence around their family trauma history” (p. 151) and often there is a continuous tension between disclosure and silencing of painful memories.
The relative value of disclosure versus silencing has been the subject of theoretical debate, particularly as more research on non-Western refugee populations has emerged. Originally parents’ silence and emotional withdrawal was believed to be negative and to result in the unconscious displacement of emotional issues onto the child. Thus, open communication and disclosure of family secrets were promoted (Dalgaard & Montgomery, 2015) while silencing was seen as less adaptive (Dalgaard et al., 2016). However, communication is a culturally embedded practice, and attention needs to be paid to cultural idioms of distress, defined as “socially and culturally resonant means of experiencing and expressing distress in local worlds” (Nichter, 2010, p. 405).
For example, in their exploration of trauma communication among Cambodian refugees in the United States, Lin et al. (2009) found that views of what constitute culturally appropriate communication about past atrocities may inhibit sharing of traumatic family histories across generations. Based on interviews with children in the United States who had either left Cambodia while they were very young or whose parents had arrived in the United States prior to their birth, Lin et al. reported that many parents avoided talking about the genocide within Cambodia with their child as a means to cope with the trauma. This often gave rise to alienation from their children or a misunderstanding on the children's part of the experiences of older generations. While silencing may have adverse outcomes, it may be protective for parents. Furthermore, when it is culturally embedded to be silent about feelings, it may undermine mental health to suddenly become open and communicative.
Lin et al. (2009) also found that children received glimpses of their parents’ past trauma, through overhead conversations, via seemingly casual conversations, or during emotional outbursts. According to the study, these partial and indirect communications about past trauma often resulted in children being unable to form a coherent and meaningful narrative about their parents’ histories, and led children themselves to engage in avoidance, discomfort, and a perpetuation of silence around past parental trauma.
These findings point to how parents can oscillate between disclosure and silencing, and that disclosure can take different forms and can arise in different contexts. Resonating with these findings, Measham and Rousseau (2010) identified three forms of trauma communication based on interviews with parents: avoidance, modulated disclosure, and unmodulated disclosure. Avoidant narratives were ones where parents did not divulge much information about family history of trauma or indicated that trauma had a minimal effect on their child. Modulated disclosure was characterized by parents talking about traumatic events in a subtle manner, without the disclosure of graphic details about the trauma. Finally, unmodulated disclosure referred to situations where parents indicated that their children had been affected by their experiences, and either could not discuss these experiences with their children, or else discussed these events only, at the expense of being able to discuss non-traumatic aspects of the family's past. This latter form of disclosure was evident in all families who presented with clinical problems. The authors concluded that the timing and manner of disclosure is what matters, and that the manner of disclosure needs to account for the child's developmental status in addition to the family's reunion status and the meaning of the trauma narrative in the family (Measham & Rousseau, 2010).
Extending this work, Dalgaard et al. (2016) also identified modulated disclosure as a communication strategy in which parents talk to their children about their traumatic past in a manner that is attuned to the emotional needs and developmental status of the child. Further, Dalgaard et al. (2016) also describe unfiltered speech whereby parents talk about their trauma histories in the presence of their children, but not directly to their children. This creates an incongruence between what parents believe their children know and what their children actually know. Dalgaard et al. (2016) reported an association between children's insecure attachment and this unfiltered communication.
The present study seeks to contribute to this limited body of literature by exploring intra-family communication styles in forcibly displaced families who are seeking International Protection in Ireland. Specifically, the present study asks the question “How do mothers who are seeking International Protection in Ireland speak to their children about their experiences of displacement, mental health and seeking asylum, and what are their motivations and strategies for communication?” This study is conducted in Ireland, where in 2019, the year during which fieldwork for the present study was conducted, there were 4,781 new applications for International Protection, representing a 30.2% increase on figures from 2018. At the end of 2019 there were 7,330 pending applications, and the median processing time for applications was 15.6 months. Of the 1,870 decisions made at the first stage of the application process in 2019, 52% were positive decisions (Irish Refugee Council, 2019; Sheridan, 2020). In Ireland, the reception system for those who are seeking International Protection is commonly referred to as Direct Provision, as the state directly provides applicants with bed, board, and medical care. The delivery of these services commonly occurs through a system of residential institutions or Direct Provision centres, which, since their advent in 2000, have amassed national and international criticism for offering overcrowded, sub-standard living conditions which foster dependency and social exclusion (Doras, 2020).
Method
Design
A cross-sectional qualitative research design (Willig, 2012) using semi-structured interviews and thematic analysis (Braun & Clarke, 2006, 2012) was employed in the present study.
Recruitment Process
Participation was open to mothers and fathers who were applicants for (asylum-seekers) or recipients of (refugees) International Protection in Ireland. A refugee was defined as an individual who has been recognized as meeting the terms of the 1951 Refugee Convention, or as someone who has received subsidiary protection or permission to remain in Ireland by the Minister for Justice and Equality. An asylum-seeker was defined as an individual who has applied to Ireland's International Protection Office and who is seeking to be recognized as a refugee under the terms of the 1951 Refugee Convention (Government of Ireland, 2015). Mothers and fathers were required to be 18 years old with at least one child aged between four and 17 years. Parents and children were required to be living together. Individuals with acute mental health difficulties, learning difficulties, communication difficulties, and cognitive impairment were excluded from the present study. Parents were recruited between May and December 2019.
Participants were recruited through a partner organization—Spirasi—which is the National Centre for the Rehabilitation of Victims of Torture in Ireland. Spirasi was founded in 1999, after Ireland signed the UN Convention again Torture (UNCAT). This Convention was ratified in 2000 via the Criminal Justice Act (2000) (Government of Ireland, 2000), wherein the State is mandated to enact Article 14 of UNCAT, to provide as full as possible rehabilitation for victims of torture. The services provided by Spirasi range from therapeutic, legal, and medical to the psychosocial and educational.
Initially, the second author approached four clients, all mothers, within Spirasi who met the study inclusion criteria, based on the assessment of their therapists. Of these, three agreed to participate. Two of these parents offered to help recruit additional participants in their respective Direct Provision centres, and the remaining participants were thereafter recruited via snowball sampling. A further 22 mothers showed interest and provided their contact details so that the second author could contact them regarding participation. All potential participants received an information leaflet and consent form which detailed information about the aims of the research, inclusion criteria, confidentiality and limits to confidentiality of the data, benefits and risks of involvement, data storage, and right to withdraw information. Participants were then given seven days to decide if they would like to participate, during which they could contact the second author with any research-related queries. Of the 22 mothers who registered interest, 17 went on to contact the researcher, who confirmed their suitability to participate in terms of the criteria. Thus, we had a final sample of 20 participants. In one instance, the sound quality of the audio recording was too poor to be transcribed and therefore this interview was not included in the final analysis, resulting in 19 participants in this study.
Participants
Participants were 19 mothers living in Direct Provision centres in Ireland. Mothers ranged in age from 29 to 46 years (M = 36.63; SD = 5.04). Sixteen mothers were seeking asylum and three mothers had permission to remain in Ireland. The length of time spent living in Direct Provision ranged from three to 36 months (M = 19.79, SD = 10.72). Six mothers had one child, seven mothers had two children, three mothers had three children, two mothers had four children, and one mother had five children. Eighteen mothers were from African countries including Zimbabwe, Nigeria, and South Africa and one mother was from Southeast Asia (countries of origin of only one participant were not identified to protect their identity).
Data Collection
Ethical approval was obtained from the Ethics Committees at the Department of Psychology, Southern University Denmark and the School of Psychology, Trinity College Dublin. Semi-structured interviews were conducted with mothers, ranging in duration from 20 to 67 min (M = 40.70, SD = 11.70). Interviews were conducted by the second author, who worked as a co-facilitator of education and therapy sessions within the Spirasi centre and had received training in conducting qualitative research and working with vulnerable groups. In all but one instance, mothers were interviewed in the Direct Provision centre in which they resided; in the remaining case, the interview was conducted in a nearby restaurant at the request of the participant. In all cases, the interviewer and interviewee were visible to others (for example, through a closed door with a glass panel, or in a quiet corner of a public space). All participants chose to conduct the interview in English but were offered the services of an interpreter if they wished to complete the interview in their native language. All interviews were audio recorded. The interviewer also recorded fieldnotes after each interview to document her observations, details about who was present, emotional responses of participants, etc.
Prior to the commencement of the interview, a demographics questionnaire was used to record mother's age (measured in years); country of origin; protective status (asylum-seeker v. refugee); time spent living in Direct Provision (measured in months); and number, age, and sex of children. Following completion of this, the interview began. Participants were reminded that they did not have to answer questions unless they wished, and that they could terminate the interview at any point. The interview schedule was designed to address the question: How do mothers talk to their children about experiences of displacement and asylum seeking? Mothers were asked to describe how they talked to their children about their past and current situation (e.g., “How do you talk to your child about the reasons you left your home country?”; “How do you talk to your child about family who are still in [country of origin]?”; “How do you talk to your child about your childhood and growing up in your home country?”; “Do you talk to your children about how you are feeling? … If so, how?”; “How do you think your ongoing asylum-seeking process has affected the way in which you interact with your child, if at all?”). Questions were adapted, elaborated upon, or omitted dependent on the individual context.
Upon completion of data collection, participants were provided with a debriefing sheet summarizing the aims of the research and containing contact details of the second author. All participants were offered a session with a trained therapist from the Spirasi centre in the event that the interview was distressing for them. Interviews were transcribed verbatim and pseudonyms were assigned to participants. Identifying information was redacted from transcripts.
Analysis
Thematic analysis (TA) was selected as it could accommodate varied and contextualized data and offer pragmatic flexibility in the exploration of context-specific, culturally informed patterns of communication. Moreover, TA is not bound by a singular epistemological or theoretical framework and was therefore deemed most appropriate and in keeping with the study's research question. Braun and Clarke's (2006) six-phase approach to TA was used to analyse the data.
Phase 1 comprised familiarization with the data wherein transcripts were read and re-read multiple times. Phase 2 involved generating initial codes, with 318 codes being produced. Most codes were specific to communicative information, e.g., child asking questions and mother keeping negative things from the child, with additional codes generated for non-communicative information, e.g., maternal reports of traumatic experiences and parenting difficulties specific to direct provision.
Only the codes relating to communication are presented in the present paper. The interview data were coded in a primarily inductive, data-driven manner, with all data being coded and all codes defined. Data segments were coded inclusively and coded to more than one code where appropriate. For example, the data extract … because she talks [about] anything and then I would find it that no, I can’t explain some of the things further, because it's too big for her. But she would come with big questions. Then, I think if I open up, yeah, I think this thing is too big for her. So, I would tell her, “Wait. I’ll tell you when you’re 18.”
was coded to several codes including child asking questions, concern for child, being child centred, developmental capacity of child, parental decision making and future conversations. However, coding of the data was also informed by a deductive approach, whereby concepts that existed within the literature were drawn upon to inform the analysis. For example, the code ‘being child centred’ aligns closely with characteristics of ‘modulated disclosure’ described by Dalgaard et al. (2016).
Phase 3 involved searching for themes. Codes were categorized, collated, merged, and reorganized into communication themes with sub-themes, for example the codes mother treating their child as an individual, mother trying to provide child with age-appropriate answers, and mother imagining effects of disclosure on child were categorized together and merged under the theme of being child centred. In phase 4, themes were reviewed, refined, and reordered under three superordinate themes; for example, avoidance strategies, silencing strategies, and withholding information were reordered under the same superordinate theme (guarding communication). Phase 5 entailed themes being defined and named; for example, the superordinate theme of guarding communication was defined as communication in which the mother employed strategies to avoid engaging with certain topics of conversation. The final report was produced in Phase 6.
Research Trustworthiness
After the second author had coded all interviews, the first, third, and final authors were provided with the codebook with definitions of all codes and were asked to code extracts from a total of five randomly selected interviews. They were asked to use the codebook when applicable, but also to produce new codes or categories if they saw something not included in the codebook. For each interview, they read the entire transcript and coded extracts within each interview. The coding and its principles were then discussed, and codes were changed, merged, or elaborated upon if questioned within the team.
Results
Two superordinate themes—Guarding Communication and Grappling with Communication—each with subordinate themes, were developed from the analysis of the data, each of which captured the strategies and motivations underlying how mothers communicated with their children about their experiences (See Table 1).
Guarding Communication
All participants discussed how maternal communication—or lack of it—was shaped by the enduring effects of pre-migratory trauma and forced displacement. In reporting trauma and trauma sequelae, and in navigating cultural transitions and evolving political and policy spheres in the context of Direct Provision, communication was highly guarded. The theme of guarding communication was represented by three subordinate themes, namely: avoiding certain topics of conversation, silencing their children, and withholding information from their children.
Avoidance Strategies
Sixteen mothers reported using avoidance as a strategy when their child broached topics of conversation which mothers found difficult. The mode of presentation varied across participants and appeared to be guided by the age of the child. For example, mothers of younger children frequently described avoidance techniques which involved changing the topic of conversation or distracting the child. For example, Primrose described how she changed the topic of conversation when her six-year-old child asked her questions which she did not want to answer: “I’ll always try to dismiss it … then I’ll find a way of coming out, like changing the subject.” Similarly, Maureen described avoiding answering questions about her husband who remained in their country of origin by distracting her five-year-old son: “you know how to trick kids … I’ll give him treats … he will just forget about it.”
Mothers of older children also reported using avoidance strategies as a way of dealing with difficult questions or topics of conversation which they perceived as triggering. Victoria, a single mother of three children, came to Ireland with her youngest child and was later followed by her two older children. During this interim period, Victoria described not answering her phone when her children called her so that she could avoid being asked questions about their journey to Ireland: “I just didn’t want them like to call all the time … every time … they were asking me, ‘Mommy, when are you taking us?’ … And so, I was just avoiding that.” Primrose also described avoiding difficult topics of conversation with her older children. For example, she detailed that she would send her older daughter to a friend's house: “she’ll go and play, play, play until late, come back and then she’ll bath, eat, and sleep … just to avoid her saying things.” Or she would take on more shifts at work: “I prefer to stay at work ’cause I don’t want to be asked questions.”
Throughout the narratives, mothers also revealed the motivations and factors underlying their adoption of avoidance strategies. Commonly, avoidance was framed as a way of protecting oneself from memories which were painful or traumatic, or from questions that could not be answered. Natasha explained her use of avoidance strategies by saying that “I don’t know if I can call it ‘protect myself’ or what, because I know that if he starts talking … that night I wouldn’t even sleep.” Similarly, Primrose explained: “that is the only life that I can live … ’cause I don’t have answers, what must I say? I don’t have answers.”
For other mothers, avoidance appeared to be enmeshed in their cultural frameworks of communicating with children in ways that protected them from adult concerns. Eighteen mothers were of African origin and several emphasized that within an African context, it was not common to speak to children about serious matters. Josephine noted that: “sometimes, it's the culture. That's how we were brought up … I don’t even remember one day seeing my mom cry. It's just the African culture. We are not allowed to show emotion.” Josephine went on to add that in her culture, “we try to hide our emotions … especially from our children.” The notion of mothers hiding difficult emotions, stress, and trauma sequelae from their children resonated throughout the interviews; instead, mothers reported that they would pretend to be okay or that they would explain away their reluctance to talk to their children as being due to tiredness or a headache. Esther described trying to avoid interactions with her young daughter when experiencing a depressive episode: “when she comes near me, maybe hugs me, I’ll say, ‘Please. I’m tired. I don’t want’.”
Finally, some mothers described how avoidance strategies were shaped by post-migratory environmental factors such as sharing small living spaces and/or bedrooms or not having access to childcare or a support network. Julia reported an absence of an extended family or support network to help her since her arrival to Ireland. Therefore, when she experienced acute mental health symptomology, she told her son that she was leaving their apartment despite remaining in her room: “because sometimes he doesn’t give you peace, that boy.” Another mother, Chloe, reported that she avoided dealing with her trauma sequelae and stress in the presence of her son by waiting until he was at school before processing her emotions: “you lose your own right of exercising emotion whenever you want … you kinda learn to be upset later.”
Silencing Strategies
A second subordinate theme describing a strategy of guarding communication was that of “silencing,” discussed by nine mothers. Wanting to “keep things” to oneself or the concept of “bottling things up” often preceded maternal reports of “shutting down” certain conversations or “blocking” difficult questions. This was often compounded by acute mental health symptoms and stressors relating to seeking International Protection. Deborah described instances in which she would silence her younger children by raising her voice when they asked questions which she could not answer about family members in their country of origin: “If he persisted then I-I just raise the voice on him, then they keep quiet.” Victoria described occasions in which her daughter would ask her if she is okay and she would, in turn, shut down the conversation: “I usually say, ‘It's fine. It's not your business. It's simply fine. Just give me some space’.” Primrose similarly described silencing her adolescent son when she was experiencing an accumulation of stressors and mental health symptomology. When asked what types of questions her son was asking, she replied that she did not know but that it was best “to kind of shut him off before he can open his mouth … you try always to block everything that is coming.”
Primrose reported that she was aware that this must be difficult for her son but that silencing served a self-protecting purpose: “I know it must be hard on him that ‘My mama, I can’t even ask her anything,’ but he doesn’t know what I’m going through.” Other mothers positioned silencing strategies as a means to achieve the space to process pre-migratory traumatic experiences while also allowing oneself to forget about these experiences. Thus, concepts of “wanting to forget” and “erasing” memories were invoked to explain why silencing was used. Silencing also allowed mothers to think about these traumatic experiences, but in their own time. For example, Victoria described that her “mind just wants to forget” about traumatic events in her past. However, desire to forget was also juxtaposed with having the space and time to process what she has survived and escaped from: “it only gets to me now that I’m here … I’m actually starting to think back. But, you know, sometimes, you know, I just want to forget.”
Withholding Information
A third subordinate theme, that of withholding information from children, was described by 12 mothers. This strategy ranged from providing children with vague or very limited information to completely withholding information. This communication strategy was commonly reported when mothers described dealing with questions about migration to Ireland and factors relating to their International Protection case. Withholding information was often explained by mothers as a means to protect their children from “carry[ing] heavy things” or to prevent maternal stressors from being a “weight” to the child. Mothers described waiting until their child was older and until “the time was right” to discuss more difficult or complex matters, such as disclosing the reasons for their forced displacement and the status of family members in their country of origin. Camilla described that she would “definitely” speak to her son about factors underpinning their displacement at a more age-appropriate time in the future: “I think when he grows older, when I talk to him how we left and why we’re here, he will understand … he's … gonna be a more mature person at that time.” Charity also described waiting until her children were older to speak to them about “why we are here, why we left our country.”
Mothers also withheld information from their children when they were uncertain about outcomes, such as whether they would reach their intended destination. For example, Camilla described her children asking her where they were going when they were fleeing their country of origin. She did not tell her children details about their journey as she was unsure if they would ever reach their destination: “‘You’ll see where we’re going when we get there.’ ’Cause I wasn’t sure we were gonna reach our destination. You don’t know what's gonna happen.” Ayat described that she did not tell her daughter that they were fleeing their country to Ireland via South Africa but rather told her that they were visiting South Africa: “I just say we’re visiting South Africa. Because I didn’t want the whole thing for her to know that ‘okay, now my mom is running away’.” Later, when they arrived in South Africa, Ayat told her daughter that they would visit her auntie “overseas.” Thus, information was imparted in degrees, depending upon what was going to happen next.
Grappling with Communication
The second superordinate theme reflected how mothers grappled with communicating with their children. Three subordinate themes were subsumed within this process. First, mothers sought to align their disclosure of information to their children in a child-appropriate manner—this sub-theme is termed ‘being child centred.’ However, being child centred was challenging for mothers, as certain pieces of information were difficult to share with their children. The second subordinate theme ‘doubting oneself’ captured these challenges as mothers questioned what they should say to their children and how. Finally, the third subordinate theme was termed ‘being inconsistent,’ reflecting that mothers’ stated communication strategy often did not align with how they actually communicated with their children.
Being Child Centred
Eighteen mothers described ways of communicating which placed the child at the core of dyadic communication. These mothers reported communicating details of their experiences to their child in a considered, child-centred manner. Communication was pitched to be aligned with the developmental, cognitive, and emotional capacity of the child. Child-centred communication involved balancing the disclosure of information whilst simultaneously not wanting to “overload,” “stress,” or “burden” the child.
For example, Esther described the difficulties in deciding how best to disclose distressing information about family members in their country of origin to her son. She described that her son knew that something was wrong, as “he saw me change, like getting thinner and thinner and weaker” and kept asking her “Mummy, what's wrong?” Esther reported that she took her time to think about how best to disclose this information: “I did think. I did take my time to think about it because I knew once I tell him, there's no coming back.” Similarly, Sasha described how she tried to explain the trajectory of seeking asylum, “getting papers,” and leaving the Direct Provision centre in a child-appropriate way: “I’ll just tell her … your friends … came first here in Ireland … that's why they got the paper. We only came like a year and half ago … maybe when you are two years or three years we might get the papers … then we will leave.”
Sasha explained that her daughter was too young to understand the concepts of the International Protection interview process and gaining refugee status: “she wouldn’t understand … It's too much for her, she's only like nine.” Charity similarly reported that communicating specific details of the asylum process to her young son was not age appropriate “‘when the time comes, very soon, we’re gonna get our own house’ … I think it's okay for him to understand that, not more than that … he too small to understand more.”
Many mothers framed being child centred as a reflection of a parenting style that was not typical of their own upbringing: “back home or African style … it's not easy for you to talk to your parent and be open.” Similarly, Nicole described that she did not have an honest relationship with her own mother and that she wanted to have a different relationship with her children: “I want to be honest with my kids … I want them to come back to me, to feel free to ask me something where they know mommy won’t … ignore the question.”
Doubting Oneself
Fifteen mothers expressed feeling uncertain when deciding what to tell their child regarding their experiences of, and reasons for, displacement and migration. Mothers of younger children additionally expressed feeling uncertain when deciding how to communicate information to their child regarding their country of origin. For example, Chloe described not knowing how to speak to her young son about the reasons for their forced displacement as these factors were embedded in a context which he does not remember: “I tend to worry that maybe I should start telling him about who he is—like why we are here … But I still don’t find an easy way to explain it to him.” Chloe further described the difficulties in speaking to her son about the factors underpinning displacement as she herself continues to find it difficult to reconcile this information: “it's not gonna be easy for me to get [him] to understand this one, 'cause myself, I don’t know how to package into my brain … and say, ‘This is how it went down’.”
Josephine described that she did not know how to discuss factors surrounding her forced migration with her adolescent son by saying that “there are some things that I can’t explain to him.” Similarly, Primrose described not knowing how to communicate details of her past traumatic experiences and the reasons underpinning the displacement to her children: “If it [disclosure] can happen, only God can know. Maybe when-when I’m on my death bed that's when I can say, ‘Listen, guys, I need to tell you a, b, c, d’.” This uncertainty was compounded by worry concerning how this type of disclosure would impact her children: “I don’t know what damage [it is] going to do to them.”
Mothers also described doubting themselves when discussing how they had talked about and kept alive their culture and background with their child. For example, Maria described her young daughter asking her “‘Mommy, what [is] my other country's name? … Mommy what's your language?’” Maria described that she felt as though she had “failed” her daughter by not communicating these details to her and that she “made a terrible mistake by switching” to English. Similarly, Chloe also reported that she felt she had “made a mistake of not teaching [her son] my language.”
Finally, mothers’ doubts also came about when children accessed information via other means, such as through social media or from other children in the Direct Provision centre, and they were forced to revisit initial decisions they had made about what information to impart to their child. Samantha described a traumatic incident in her country of origin in which a family acquaintance was murdered. She described withholding this information from her son so that she would not “unnecessarily disturb him.” However, she later reported that her son learned of this incident via the internet and became “very quiet.” Samantha then described telling him “exactly what happened because now it's there and he's reading it.” Later, Samantha reported that they “keep away the things that he shouldn’t know,” revealing an inconsistency between the information she described withholding from her son and the information he was able to access via social media.
In a similar vein, Ayat reported that she chose not to tell her daughter about the intricacies of the interview and adjudication process as part of seeking asylum. However, her daughter later found out more detailed and complex information from other children in the centre, forcing Ayat to reconsider her narrative to help her daughter reconcile this new information: “because some things … you tell yourself you are protecting your child from … [then] she would come from outside and tell you those things …” This concept of mothers questioning and revising what they told their children was experienced as a loss of autonomy of their communication choices, with Ayat reporting that “it's the women [who] lose …”
Being Inconsistent
Finally, all mothers reported communicating information which revealed inconsistencies in how they talked with their children. For example, Deborah reported that she did not speak to her children about her mental health symptomology and that they were unaware of the difficulties she was experiencing. However, the field notes of the interviewer indicated that two of her children were in the room when she later spoke about the symptoms that she was currently experiencing, therein conveying an inconsistent communication style. Moreover, Deborah described that her children would repeatedly ask her when their father is coming to join them in Ireland. Throughout the interview, Deborah reported that, at times, she would answer these questions by saying that “yes, anytime soon he will be coming,” then “oh, okay, he's coming maybe next year,” and then “that he is coming in two months.” In describing these interactions, Deborah appeared to be unaware of these contradictory statements that she was making to her children and the potential for fostering confusion.
An accumulation of mental health symptomology and stressors appeared to compound inconsistencies and contradictions in maternal communicative processes. Primrose described telling her children that they could come to her with any issues—“If you have got a problem, sit down with me”—but later reported that she would tell her children “I’m not in the mood of questions” when she was experiencing acute mental health symptoms. Similarly, Nicole described telling her children that they could always come to her with questions. However, when her daughters approached her with questions that she finds difficult Nicole reported that she “run[s] away from what they ask me because I don’t know how to answer them.” These findings, which are based on field notes and on analysis of inconsistencies in mothers’ subjective reporting of their communication, underlie the fact that there may be a significant gap between consciously shared strategies about communication and those which are actually employed.
Discussion
The present study set out to explore how mothers communicate with their children about their experiences of trauma, displacement, and mental health difficulties whilst seeking International Protection and living in Direct Provision centres in Ireland. Based on qualitative interviews with 19 mothers who had been in Direct Provision centres in Ireland for an average of 20 months, and thematic analysis of mothers’ narratives, two themes were developed from the data, each capturing strategies and motivations underlying how mothers communicated with their children about their experiences. The themes—guarding communication and grappling with communication—were ubiquitous across all interviews, suggesting that mothers did not adopt a singular style of communication. Rather, communication was a dynamic process underpinned by motivations to protect both oneself and one's child, as well as trying to address the child's requests for information. The interplay between guarding and grappling with communication reflects the dialectical tension between disclosure and silencing, as discussed by De Haene et al. (2020).
The first superordinate theme—guarding communication—comprised three subordinate themes, each representing strategies to maintain a silent position on their trauma narrative. This strategy was manifested through avoiding topics of conversation, silencing their children, and withholding information, and various means were employed, such as distracting their children, changing topics of conversation broached by their children, providing vague and limited information to their children, and directly telling their children to stop asking questions. Guardedness in its various manifestations was framed as a mechanism for self-preservation, as mothers simultaneously coped with mental health symptomatology, post-migration stressors, and living in Direct Provision centres.
The guarding communication theme from the present study resonates partially with the ‘avoidance’ form of communication identified by Measham and Rousseau (2010) and with the ‘silencing’ discussed by Dalgaard et al. (2016). Similar to the subordinate themes identified in the present study, for parents in the Dalgard et al. sample, silencing was manifested through not referring to traumatic experiences from the past in front of the children, distracting the children when they asked questions, or providing only minimal responses to questions (akin to withholding information in the present study). The narratives generated in the present study further illuminate that avoiding, silencing, and withholding communication were often driven by a need to protect oneself from harm, although several mothers also noted that open communication with children was not typical within their culture, or that they were striving to protect their children from being burdened by the weight of their trauma. Whatever the underlying motivation, these findings suggest that guarding one's story needs to be acknowledged as an important way of dealing with trauma. While past research may have pathologized silence and associated not talking about the trauma with a perpetuation of mental health difficulties (Dalgaard & Montgomery, 2015), these mothers appear to be distancing themselves from painful memories in order to avoid being overwhelmed by them and this may well be an adaptive response. Indeed, being given the space and permission to be silent and to possibly forget past traumas may be important for creating hope and building a future life in a new country (De Haene et al., 2020).
The second superordinate theme—grappling with communication—and its three subordinate themes—being child centred, doubting oneself, and being inconsistent—captured the challenges faced by mothers as they sought to address their children's questions and disclose information to them. Almost all of the mothers adopted a child-centred position when talking to their children about their past and current situation. They took into account their child's age and maturity level and tried to pitch their communication in accordance with what they perceived their child could cognitively and emotionally process. However, this could be challenging because it is not easy to know the capacities of the child, and mothers were left doubting themselves about how more difficult elements of their story could be talked about and worrying about how disclosure might impact negatively on their children.
The sub-theme of being child centred aligns closely with the concept of modulated disclosure (Dalgaard et al., 2016; Measham & Rousseau, 2010). These authors similarly described a child-centredness in how trauma narratives were disclosed—more detail or greater disclosure was more appropriate with older rather than younger children. Parents strove to achieve a balance between sharing age-appropriate information to help children make sense of their situation and protecting children from being burdened (De Nutte et al., 2022). However, the interviews with mothers in this study further reveal how modulated disclosure is not straightforward and can leave mothers feeling uncertain and worried. An additional consideration for mothers was how to deal with information which children sourced from outside the family, such as through social media or from other children in the Direct Provision centres. A small number of mothers in the present study described being forced to explain things to their children as a result of these external influences. De Nutte et al. (2022) similarly found that parents’ choices to disclose or be silent were shaped by their social and relational context and often had to be negotiated, and that, as was the case for mothers in the present study, their agency regarding these choices was constrained.
Finally, inconsistencies were apparent in how these conversations happened between mothers and their children. Being inconsistent was notable when mothers contradicted themselves during the interviews or disclosed information in the presence of their children, despite reflecting that they wished to withhold information or remain silent. Such inconsistencies are reflective of how challenging such stories are to tell. Dalgaard et al. (2016) similarly describe an unfiltered form of communication, where parents talk about traumatic memories in the presence of their children but not directly to their children. This results in a discrepancy between what the child knows and what the parent acknowledges the child knows, and can give rise to confusion for the child and a lack of coherence as they construct their own meaning of the situation.
Limitations of the Study
Through qualitative interviews with a hard-to-reach and vulnerable population, rich narratives were generated which enabled the research team to identify themes relating to communication strategies adopted by mothers seeking asylum or being refugees. However, the cross-sectional nature of the study only provides a snapshot of communication at one point in time and limits our understanding of how these strategies may evolve and change over time, in response to children's developmental status, changes in the migration status of the family, and mothers’ own processing of their experiences. Future longitudinal research following families over their migration journey would shed light on these processes.
Recruitment for the present study comprised convenience and snowball sampling and it is reasonable to suggest that this style of recruitment failed to reach harder-to-access families within this sample framework, e.g., families with low levels of English proficiency, parents who have significant mental health burdens, families with a distrust of Irish organizations, and families who are socially isolated within these centres. We also acknowledge that our sample is homogeneous in some respects (only mothers, and most mothers being from Africa) and future research could strive to include greater diversity in samples of refugee parents seeking international protection. Notwithstanding this, we have a large and diverse sample from a potentially hard-to-reach group of people and they provided elaborate and nuanced narratives about their experiences.
Also, although recruitment was open to mothers and fathers, only mothers participated. The second author did not encounter any men who met study inclusion criteria through her role in the partner organization. The mothers who participated in the study were asked to inform their partners or any men in their social network about the study. However, most of the mothers who participated were single mothers and their social networks consisted primarily of other women. Thus, recruitment through snowballing did not yield any participants who were fathers. The difficulty in recruiting fathers may also be partly attributable to divergent cultural narrative strategies around openness and silence, and participating in an interview with a stranger may be at odds with these strategies (Bagilishya, 2000). Thus, the present study only provides a partial understanding of communication within these families and may be most representative of families with single mothers. In addition, some mothers in the sample had achieved refugee status, while others were still in the asylum-seeking process. Although we did not compare these groups of mothers, it may be important to consider migration status in future research when understanding mothers’ communication strategies and the motivations underlying them.
Given that family relationships play a central role in refugees’ adjustment to post-migration life and coping with traumatic life histories (De Haene et al., 2018), future research needs to explore how trauma narrations are constructed, from a systemic perspective by the inclusion of multiple perspectives, including those of fathers and those of the children. As noted by De Haene et al. (2020), in navigating the balance between silence and disclosure, and between remembering and forgetting, family members learn to relationally regulate the trauma narrative by monitoring what is safe and bearable for each other. Lin et al.'s (2009) study documented how young people upheld silence in order to protect their parents from distress. In the present study, the omission of the children's views on their mothers’ approaches to communication prevents a nuanced understanding of how silence and narration is negotiated within the parent–child relationship and how it is perceived and valued by the children. A further understanding of how this dialectical tension between silence and narration is navigated within relationships will have important implications for how care and services are delivered to refugee parents and children. Finally, the observations of the interviewer and the field notes at times yielded data that revealed inconsistencies or discrepancies between what mothers were saying and what they were doing (e.g., talking about issues in the presence of children while claiming that the children did not know anything about the issues). This suggests that observational data and self-reported data may provide different insights, and future research would benefit from the inclusion of these different types of data.
Clinical Implications
Mothers’ narratives highlighted how trauma exposure, displacement, mental health symptomology, and post-migration stressors influenced communication with their children. Communication was fluid and no one communication strategy was adopted; rather, mothers oscillated between silence and narration, and when they did communicate and strove to be child centred, they found this challenging. The findings suggest that different types of communication served different purposes, and all tried to have an adaptive function (e.g., mothers choose to be silent as a means of protecting themselves). Thus, therapeutic approaches that rely only upon openness and disclosure may be triggering and harmful (Rousseau et al., 2013). Our findings support De Haene and colleagues’ writings on creating a therapeutic space that enables remembering alongside forgetting and that facilitates silence as well as narration, as well as trauma-informed therapeutic approaches that acknowledge the “potentially reparative role of both disclosure and silence” (De Haene et al., 2020, p. 152). The inconsistencies documented in the findings reveal that there may be a significant gap between consciously shared strategies and those which are actually implemented. These inconsistencies may also become apparent during therapy and it is incumbent upon therapists to avoid a moralistic stance on these inconsistencies, instead seeking to understand what underlies the contradictions for their clients. Role play between therapist and client might be useful, wherein the therapist could model directly the communication of aspects of the story which are acceptable to the mother. This may help mothers understand the child's level of understanding and what the child may internalize from their conversations.
Although the current study did not explore how the various communication strategies might be associated with different outcomes for children, previous research has suggested that child-centred or modulated disclosure is associated with better child outcomes (Dalgaard et al., 2016). However, given that mothers do not adopt a singular strategy, it may be misguided to promote only child-centred communication—instead, what matters is supporting mothers’ agency in choosing the manner, timing, and content of their communication with their children. In addition, the fact that mothers struggled to be consistent and had many doubts about how to convey information to their children suggests that when mothers do want to use child-centred communication, they may benefit from therapeutic support in developing appropriate narratives to share with their children.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the COllaborative Network for Training and EXcellence in psychotraumatology (CONTEXT) programme from the European Union’s Horizon 2020, under the Marie Sklodowska-Curie Grant Agreement No. 722523.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.